Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia
by
 , , , and
, , , and
Pernille B. Elming
1, 
Brita S. Sørensen
1,
Arlene L. Oei
2,
Nicolaas A.P. Franken
2,
Johannes Crezee
2 ,
,
Jens Overgaard
1 and
Michael R. Horsman
1,* 1
Department of Experimental Clinical Oncology, Aarhus University Hospital, DK-8000 Aarhus C, Denmark
2
Department of Radiation Oncology, Amsterdam University Medical Centers, University of Amsterdam, 1105AZ Amsterdam, The Netherlands
*
Author to whom correspondence should be addressed.
Cancers 2019, 11(1), 60; https://doi.org/10.3390/cancers11010060
Submission received: 12 November 2018
/
Revised: 14 December 2018
/
Accepted: 29 December 2018
/
Published: 9 January 2019
(This article belongs to the Special Issue New Developments in Radiotherapy)
Abstract
:Regions of low oxygenation (hypoxia) are a characteristic feature of solid tumors, and cells existing in these regions are a major factor influencing radiation resistance as well as playing a significant role in malignant progression. Consequently, numerous pre-clinical and clinical attempts have been made to try and overcome this hypoxia. These approaches involve improving oxygen availability, radio-sensitizing or killing the hypoxic cells, or utilizing high LET (linear energy transfer) radiation leading to a lower OER (oxygen enhancement ratio). Interestingly, hyperthermia (heat treatments of 39–45 °C) induces many of these effects. Specifically, it increases blood flow thereby improving tissue oxygenation, radio-sensitizes via DNA repair inhibition, and can kill cells either directly or indirectly by causing vascular damage. Combining hyperthermia with low LET radiation can even result in anti-tumor effects equivalent to those seen with high LET. The various mechanisms depend on the time and sequence between radiation and hyperthermia, the heating temperature, and the time of heating. We will discuss the role these factors play in influencing the interaction between hyperthermia and radiation, and summarize the randomized clinical trials showing a benefit of such a combination as well as suggest the potential future clinical application of this combination.
1. Introduction
Hypoxia is a hallmark of solid tumors [1,2]. It occurs because the tumor neo-vasculature that develops from the host vascular supply via angiogenesis [3] is a primitive and chaotic system that is unable to meet the oxygen demands of the growing tumor mass [2,4]. As a consequence, cells that are distant from the blood vessels and at the limit of the diffusion distance of oxygen become chronically hypoxic [2,4]. Flow through tumor vessels is also unstable and periodically fluctuates and this can give rise to transient or acute hypoxia [2,4]. Regardless of the type of hypoxia, both pre-clinical and clinical studies show that its presence in tumors is a major factor influencing malignant progression and response to treatment, especially radiation therapy [2,5]. These observations have led to extensive pre-clinical and clinical attempts during the last 5 decades or so to try to specifically target this hypoxia and thereby improve patient outcome [6,7]. Examples of the approaches used are listed in Table 1. They include improving oxygen availability, increasing the radio-sensitivity of the hypoxic cells, killing the hypoxic population, or modifying the radiation treatment either by increasing the dose to the hypoxic areas (dose painting) or utilizing radiation of a higher LET (linear energy transfer) in which the oxygen enhancement ratio (OER) is reduced. It is interesting that hyperthermia (heat treatments of 39–45 °C) actually induces many of these effects and as such may have the potential to be one of the best agents for eliminating hypoxia.
The concept of using heat to treat cancer is actually not a new idea. In fact, it is probably one of the oldest documented treatments, since the Edwin Smith Surgical papyrus dating back to 3000 years B.C. describes a patient with a tumor in the breast treated with heat in the form of red-hot irons [8]. Early Greek (Hippocrates 400 B.C.) and Roman (Galen 200 A.D.) translations similarly recorded the use of heat treatments [9]. After the 17th Century, there were numerous reports of tumor regression in patients suffering with infectious diseases, which ultimately led to the application of fever-induced treatment with Coley’s toxin to control tumors at the end of the 19th Century [9]. Fever-induced treatments typically required temperatures of around 40 °C for several days. Later studies utilized primitive external heating techniques to achieve higher temperatures for shorter time-periods [9]. What is novel is that today we have new developments in technology (i.e., electromagnetic, ultrasound, infrared, and nano-technology based techniques) available to us [10,11]. We can thus select the appropriate technique for the specific tumor location and size, and with support from thermometry and quality assurance, we can now apply reproducible and uniform high quality hyperthermia treatments [11,12,13]. As a result, there have been numerous clinical studies showing the potential of hyperthermia to improve radiotherapy outcome [14,15,16,17]. In this review, we will discuss the different ways in which hyperthermia has been combined with radiation therapy, focusing on why this approach is selective for hypoxia, and suggest the clinical potential of this therapeutic combination to significantly improve patient outcome.
2. Combining Hyperthermia with Radiation
Tumor response to the combination of radiation and hyperthermia is dependent on the time interval between the two modalities, the heating temperature, and the time of heating [15,18,19], as illustrated in Figure 1. For the C3H mammary carcinoma model, shown in this example, the greatest enhancement of radiation response by heat occurs when both treatments are given simultaneously (Figure 1A). However, if any interval is introduced between the two modalities then the enhancement decreases with this decrease becoming greater as the time interval increases, eventually reaching a plateau as shown. A recent clinical study in patients with cervical cancer confirms the superior benefit of using a short rather than long interval between the radiation and hyperthermia treatments [20]. For the example shown in Figure 1A, the decreased response as the time interval increases is independent of whether heating is applied before or after irradiating, and this seems to be a general result for other tumor models [15]. Also shown in Figure 1A, is the effect of combining radiation and heat in a normal tissue. A simultaneous application of radiation with heat results in an enhanced effect that is identical to that seen in tumors. However, unlike the tumors, the drop-off is steeper when there is an interval and the final plateau reached is lower. For heat given after irradiating, this drop-off actually reaches a value where no enhancement occurs, but when heat is applied prior to irradiating, a residue enhancement remains. Again, the trends seen with the model shown in Figure 1A has been reported for other normal tissues [15,21].
The heating temperature and time of heating also influence the enhancement (Figure 1B). Generally, the higher the temperature and the longer the heating period, the greater the enhancement [15,18,19]. This is true regardless of the interval between the two modalities [15,18,19]. Although, as shown in Figure 1B, the degree of enhancement does depend on whether the radiation and heat are applied simultaneously or if there is an interval.
3. Radio-Sensitization by Hyperthermia
The consensus opinion is that the enhancement of radiation response by hyperthermia, when both treatments administered simultaneously, reflects radio-sensitization. This decreases as the interval between the two modalities increases ultimately disappearing when the interval is long enough (around 4 h in Figure 1A). The remaining enhancement seen as the plateau in Figure 1A is simply the result of heat killing hypoxic cells. Since the effects of a simultaneous treatment occurs in both the tumor and normal tissue, it would suggest that sensitization does not involve hypoxia. However, the normal tissue shown in Figure 1A is skin and that is known to be somewhat hypoxic [22,23] and found to have an increased radiation sensitivity when treated with classical nitro-aromatic hypoxic cell sensitizers [24]. Similar peak enhancements have been reported by others in skin and other normal tissues in which hypoxia is even absent [15,21], although in those studies no comparison was made with tumor response under similar conditions, so it is impossible to state whether the peak normal tissue response was equivalent to that for tumors or actually lower. What is interesting is that the radio-sensitization seen with hyperthermia administered in the temperature range of 40.5–42.5 °C at the same time as irradiating is as good as, or even better than, that found using nitro-aromatic drugs that specifically sensitize hypoxic cells to radiation (Figure 2). However, unlike the nitro-aromatic radio-sensitizers in which there is only a small effect in normal tissues [24] with hyperthermia one sees exactly the same effect in normal tissues and tumors [15,18,19], thus there is no therapeutic benefit for sensitization unless the heat and radiation treatments specifically target the tumor.
Interestingly, the enhancement of radiation response by hyperthermia can be further increased by simply combining the radiation and heat treatment with the radio-sensitizer misonidazole [25,26,27]. This additional benefit was seen with both a simultaneous and sequential radiation and heat treatment, and increased with temperature and drug dose [27]. Misonidazole specifically targets hypoxic cells [5,6] and if we assume that this is also true for hyperthermia, then it suggests that they may be acting on different hypoxic subpopulations. In fact, one study clearly showed that combining nicotinamide with hyperthermia was an effective approach to improve radiation response by reducing hypoxia [28] and that since nicotinamide only affected acute hypoxia the additional benefit of heat must have been through a reduction in chronic hypoxia.
Two different mechanisms are believed to account for the radio-sensitization by hyperthermia. The first involves an improvement in oxygen delivery to the tissue. Over two decades ago, it was proposed that the clinical benefit of hyperthermia was the result of mild hyperthermia temperatures (less than 42 °C) improving radiation response by increasing tumor oxygenation status, resulting in a corresponding decrease in radiation resistant hypoxia [29]. Pre-clinical data clearly shows that mild heat temperatures can improve tumor oxygenation [30,31,32,33,34] and this is most likely the result of changes in tumor blood flow [32,33,34,35], perhaps mediated through a decrease in interstitial fluid pressure [33,34] causing an increase in perfused vessels [34,36]. Interestingly, the improvement in tumor oxygenation and radiation response observed with mild temperature hyperthermia, could be further increased if animals were allowed to breathe carbogen gas immediately after heating and during the radiation period [37]. Studies have generally shown that at mild heat temperatures tumor blood flow and oxygenation status temporarily increases during the heating period but returns to normal values afterwards [31,32,35,38]. However, the radio-sensitization by heat increases with temperature and while temperatures above 42 °C might produce a very transient increase in oxygenation during the heating period, immediately after heating there is a rapid induction of vascular damage that would be expected to significantly increase the level of hypoxia and thus radio-protect tumors [32,35,38]. Cellular oxygen utilization may play a role here. This actually increases at low temperatures but decreases at high temperatures [32]. However, the increase at low temperatures of around 41 °C is only transient and with time will actually drop [39]. Any decrease in oxygen consumption, if it occurs in tumors, can actually increase the diffusion distance of oxygen, thus improving oxygen availability to hypoxic regions and so decreasing the level of hypoxia [40,41], even at the high temperatures. The situation is made even more complicated by studies from one group reporting improved tumor oxygenation that lasted for 1–2 days after heating at mild temperatures [30,42,43,44,45], an effect that is difficult to explain. Clinical studies, in which the oxygenation status of soft tissue sarcomas [46] or locally advanced breast cancer [47] was measured with oxygen electrodes after heating, also seemed to indicate that mild temperature hyperthermia improved tumor oxygenation. However, in the sarcoma study the improvement in oxygenation correlated with the degree of necrosis found in resected specimens [46], suggesting that the apparent oxygenation effects simply reflected the damage caused by higher temperatures. Indeed, an additional pre-clinical study in which tumors treated with high thermal temperatures, known to induce physiological changes that cause a significant decrease in tumor perfusion and oxygenation [1], resulted in substantial tumor control [48] while actually reporting apparent improvements in tumor oxygenation 1–2 days after applying the heat. This suggests that the apparent improvements in oxygenation were not the result of improved oxygen delivery. Clearly, the role of heat-induced effects of tumor oxygenation status accounting for radio-sensitization is somewhat controversial and unclear. What is clear from rapid-mix studies is that the improved oxygen levels are only beneficial if they are present at the time of irradiation or within a few milliseconds after irradiating [49,50]. Yet the enhancement of radiation by heat is the same whether the heat is applied long before or after irradiating (Figure 1).
An alternative explanation for radio-sensitization by hyperthermia involves potential effects on radiation-induced DNA damage repair. Ionizing radiation causes different DNA lesions that include base damage, single strand breaks (SSBs) and double strand breaks (DSBs), the latter being produced either directly by an ionizing event or indirectly when SSBs are produced close to each other on both DNA strands [51] or indirectly when problems occur during DNA replication [52,53]. DNA DSBs are potentially the most toxic DNA lesions to cancer cells, repairable by two major pathways, non-homologous end joining (NHEJ) or homologous recombination (HR) [54,55]. NHEJ rejoins the broken ends of the DNA without the need for homology or a repair template and is active through the cell cycle [56,57], whereas HR does require a template thus is only active during the S and G2 phases of the cell cycle [56,58]. When a DSB occurs, kinases initially recognize the DNA break, and accumulate together with other kinases around the location of the break and attract other DNA repair proteins to repair the break [58]. During this process, histone H2AX (γ-H2AX) is phosphorylated; which explains its use as a marker for the induction and repair of DSBs [59]. Many studies demonstrated increased levels of γ-H2AX after combined treatment with ionizing radiation and mild hyperthermia as compared with ionizing radiation alone at 24 h after treatment, indicating that the number of residual DSBs was increased [60,61]. Moreover, after heat treatment, decreased levels are reported of BP53 and Rad51; these proteins are involved in recruiting other repair proteins of NHEJ and HR to the DNA break ends, suggesting that hyperthermia interferes with both DNA repair mechanisms [62]. How the DNA repair pathways are affected is only partially known. Multiple groups reported that hyperthermia affects NHEJ pathway-specific proteins. Hyperthermia is suggested to affect NHEJ by heat-mediated inactivation of Ku, decreased activity of DNA-PK and decreased levels of KU70, KU80, and Ligase IV [62]. Hyperthermia has also been found to temporarily degrade the BRCA2 protein and reduce BRCA1, thereby inhibiting the homologous recombination DNA repair pathway [63]. Interestingly, as a result of the poor supply of oxygen and nutrients, hypoxic cells often exist in a quiescent state [64]; these quiescent cells are less sensitive to ionizing radiation because they have the time to repair the DNA properly, as well as the known resistance due to the lower level of oxygenation. Hyperthermia can push cells out of this quiescent state and make them more susceptible to ionizing radiation [65].
4. Hyperthermia as a Cytotoxic Agent
Hyperthermia can also kill hypoxic cells either directly or indirectly. Direct cell killing is strongly dependent on the heating temperature and the time of heating; the higher the temperature and the longer the heating period, the greater the effect [66,67,68]. Typically, temperatures below 42 °C actually have little effect on cell killing, unless long exposure times are utilized [66,67,68], certainly longer than a typical heating period of 1 h when combined with radiation [14,15,16,17]. The killing seen with temperatures above 42 °C increases significantly if the cells are maintained under conditions of oxygen deprivation and/or low pH [69,70]. Such adverse micro-environmental conditions are those typically found in hypoxic tumor regions [1,2] and the ability of heat to actually kill hypoxic cells in tumors has been demonstrated [28,71]. The Overgaard study actually suggested that this heat-killing effect was primarily in chronically hypoxic rather than acutely hypoxic cells [71]. This seemed to be confirmed in the other study [28] and is supported by in vitro data, since long periods of hypoxic exposure were necessary to obtain cell killing [69,70]. In tumors, it is also the chronically hypoxic cells, rather than acutely hypoxic, that will be more likely associated with nutrient deprived conditions that also give rise to heat sensitive low pH. Preferential killing of radio-resistant hypoxic cells probably explains the plateau effect seen when heat and radiation are separated by greater than 4 h (Figure 1A). Analysis of the time-temperature cell survival curves also suggest that the slopes of the curves were very different above or below 42.5 °C [66,67,68], either reflecting different cell killing mechanisms or that with the longer heating times the cells developed resistance to heat, often referred to as thermo-tolerance [72]. Interestingly, the time-temperature response curves for tumors in vivo also shows different slopes above and below 42.5 °C [73] suggesting similar thermo-tolerance mechanisms as in vitro. However, additional studies suggest that thermo-tolerance in vivo may also be vascular mediated resulting from the induction of vessel normalization [74], a process that involves a decrease in micro-vessel density and increase in pericyte coverage [75], and causes a decrease in tumor hypoxia [76].
Heat kills cells by a variety of mechanisms, including necrosis, apoptosis and modes related to mitotic catastrophe [77,78,79,80]. The biological effects of heating cells include chromosomal aberrations, mitotic dysfunction, cytoskeletal damage, changes in membrane fluidity and transport, and metabolic changes [81]. But the most likely rate limiting step for killing by hyperthermia is protein denaturation since this in a similar time-temperature relationship as for cell killing, especially at temperatures of 42.5 °C and above, although some effects do occur with long heating times at lower temperatures [82]. At temperatures around 43 °C and below apoptosis appears to predominate with necrosis seen at higher temperatures [77,80], but whether these effects are mediated via denaturation of proteins associated with the cytosol, membrane, or nucleus, is unclear [77,79]. However, the fact that cell killing is substantially increased if cells are heated under low pH conditions [69,70] would seem to support the cell membrane as the primary target. Measurement of intracellular pH (pHi) and extracellular pH (pHe) show that cells can maintain a neutral pHi even when pHe is acidic [1]). Increasing extracellular acidity would put more stress on the membrane pumps responsible for maintaining neutral intracellular pH and thus be more susceptible to heat damage.
Whatever the mechanism, one can significantly increase heat killing in vivo using agents that decrease tumor blood flow and, thus, increase the adverse environmental conditions, especially hypoxia, within tumors. This has been achieved using physiological modifiers, such as hydralazine, sodium nitroprusside, or glucose [83]; the effects are often transient and hard to predict, yet have been shown to enhance tumor response to heat [83]. More consistent, longer-maintained changes are seen with so-called vascular disrupting agents (VDAs) that damage the established tumor vascular supply [83,84,85]. Many of these VDAs, including tumor necrosis factor, chemotherapeutic drugs (e.g., arsenic trioxide and vinblastine), flavonoid compounds (e.g., flavone acetic acid and vandremycin) and tubulin-binding agents (e.g., combretastatin and its analog OXi4503), have been combined with hyperthermia to enhance the anti-tumor response [85]. Additional benefits were observed when VDAs and hyperthermia were combined with radiation [15,85]. Moreover, such combinations were extremely effective when using mild temperature heat treatments; the radiation induced tumor control reported after systemic treatment of mice with VDAs and local tumor heating at 41.5 °C was as good as, if not better than, that seen with 43 °C alone [15,85].
Hyperthermia itself can also induce vascular damage and, as a result, will kill tumor cells indirectly. Although higher heat temperatures may transiently increase tumor blood flow during the heating period, immediately after the cessation of heating a rapid decrease in tumor blood flow is seen that is often prolonged (Figure 3), although the effects are tumor and temperature dependent. This rapid and prolonged vascular collapse following heating is similar to that seen after treatment with the drug based VDAs [84,85]. For such drugs, the target is the vascular endothelial cells [86], which when damaged undergo a rapid shape change and eventually undergo apoptosis [86]. The initial effects will cause an increase in vessel permeability and as fluid leaks out of the tumor vessels it will cause a rise in interstitial fluid pressure that then collapses the vessels [86]. This is likely to be transient, but would initiate a number of other effects such as reduced blood flow, increased blood viscosity and red cell stacking, and these would cause coagulation and thus responsible for the prolonged effect. The result of the vascular shutdown will deprive tumor cells downstream of the blockage of essential oxygen and nutrients, resulting in rapid and widespread tumor necrosis and ischemia [84,87]. The cells that die first are likely to be those that already exist under deprived conditions, especially hypoxic cells. Interestingly, despite the massive necrosis induced by VDAs their potential as stand-alone therapeutic agents is limited and for their full clinical potential to be realized they need to be combined with more conventional therapies, especially radiotherapy [84,87]. This is exactly the same situation with hyperthermia and is another strong argument for combining heat and radiation [15].
5. Hyperthermia and Alternative Radiation Approaches
The only category in Table 1 where hyperthermia is not listed is the use of novel radiation-based approaches to overcome hypoxia. These involve either increasing the radiation dose to the hypoxic areas identified from imaging analysis (dose painting) or utilizing high LET radiation (i.e., carbon ions) leading to a lower OER. Dose painting approaches [89] have generally been limited because they typically involve positron emission tomography (PET) based imaging technology that fails to represent the hypoxic distributions within tumors [4,7], thus non-hypoxic areas could receive a higher dose of radiation, while regions with hypoxia are missed. However, a recent pre-clinical study [90] suggests that oxygen images obtained using electron paramagnetic resonance could identify hypoxic tumor regions to which radiation was boosted to improve local tumor response. On the other hand, effective application of hyperthermia should target all hypoxic cells regardless of where they are located, thus making dose painting redundant.
There is clear pre-clinical evidence that as LET increases the OER decreases [91,92]. At sufficiently high LET, as seen with heavy ions such as carbon ions, the OER is extremely low so hypoxia becomes less of an issue, but in a clinically obtainable LET range hypoxia is not entirely eliminated. The advantage of using heavy ions is the improved dose distribution to the tumor thus reducing normal tissue complications. Unfortunately, there are currently only 11 heavy ion facilities in the world (almost half located in Japan) [93]. Interestingly, proton facilities are for more common (there are currently some 70 facilities operational around the world with other facilities in development) [93] and even though protons have a LET that is significantly lower than carbon ions, thus hypoxia is still a significant problem, protons and carbon ions actually share similar physical advantages. It has been suggested that the combination of hyperthermia and protons may mimic carbon ion therapy [94] and as a result a clinical trial (HYPOSAR) of hyperthermia and protons in sarcoma patients is already underway [94]. This trial will involve applying heat temperatures of 41.5–42.5 °C for 60 min some 90–150 min prior to the first of five daily irradiations given each week over a seven-week period. However, this is a new concept based on theory and limited in vitro cell survival data [95], so whether the planned tumor temperatures and time interval will be as effective as carbon ions is unclear. Clearly, detailed in vivo studies looking at the combination of hyperthermia and protons are required, but studies with photons and hyperthermia may give some idea of the potential success of this approach. From single dose studies in murine tumors, we know that carbon ions are 1.4–2.4 times more effective than photons [96]. Similar enhancement ratios are shown in Figure 1A with heating at 42.5 °C for 60 min at time intervals ranging from 0 to 240 min, and has also been seen with other tumor models [15], supporting the use of this temperature and proposed time intervals in the clinical study. At a lower temperature of 41.5 °C, reduced enhancement ratios have been reported [97], decreasing from 1.7 with a simultaneous heat and radiation treatment to 1.2 with an interval of only 120 min. This suggests that for the selected time intervals between heating and irradiating, the lower temperature of 41.5 °C may be close to the limit of benefit. However, since protons have an increased relative biological effectiveness (RBE) compared to photons [98], with a RBE of 1.1 currently generically applied for clinical use, the effect of protons at 41.5 °C may actually be somewhat higher than predicted from photon studies. Obviously, pre-clinical testing of protons and hyperthermia, using a range of temperatures and time intervals is required to support the planned clinical studies.
Interestingly, there appear to be radiobiological differences between photon and proton irradiation [99,100]. Although the initial number of DNA damage foci increases with LET [101,102], the actual number are comparable between photons and protons when irradiating with protons using therapeutic beams with relatively low LET [103,104]. What has been found to be different is the residual number of unrepaired DSBs [102,104,105,106] suggesting that the repair processes are different following photon and proton irradiation, which may be part of the RBE of 1.1 for proton irradiation. It has been suggested that DSBs induced by high LET radiation, are preferentially repaired by HR [107,108], possibly because the short DNA fragments induced by the high-LET clustered DNA damage are unable to bind the Ku heterodimer. Several studies suggest this may also be the situation with protons [103,109,110], although data from at least one study has indicated that NHEJ also plays an important role in repairing DSBs induced by protons [108]. Interestingly, an in vitro study using cells with normal repair capacity, or deficient in either NHEJ or HR, investigated the effect of heating (42.5 °C for 1 h) immediately after irradiating with X-rays or protons [111]. The authors reported an enhancement of radiation-induced cell killing in the normal or NHEJ deficient cells, but not in the HR deficient, thus if HR is the principal repair mechanism after proton irradiation it adds further support to the potential combination of heat and proton irradiation. The authors also showed the same effect for carbon ions. This taken together with other studies showing the benefit of combining hyperthermia with high LET radiation [112,113,114,115], and the fact that hypoxia is less of an issue with high LET radiation [91,92], suggest that the combination of high LET and hyperthermia may be the ultimate approach for totally eliminating tumor hypoxia.
6. Clinical Relevance
Hyperthermia has been combined with radiation in a large number of clinical trials [14,15,16,17]. A meta-analysis of trials in which the patients were randomized to receive radiation alone or radiation and heat is summarized in Figure 4 [116,117,118,119,120,121,122,123,124,125,126,127,128,129]. Most of the studies involved conventional fractionated radiation therapy although one study with cervix cancer patients applied brachytherapy [119]. The planned heat treatment was typically 42–43 °C, for a period of 30–60 min, although in the brachytherapy study the aim was for a slightly lower temperature of around 41 °C [119]. Hyperthermia was applied either once or twice weekly after radiotherapy in all the studies, but with a time interval between the radiation and heat that varied from a few minutes up to 4 h. The endpoint for these studies was complete response/local tumor control, which is understandable because the heat and radiation were applied locally to the primary tumor, with sometimes a few local lymph nodes being treated. Some of the studies also reported survival data [117,118,119,122,123] but the significance of this when using local treatments is questionable. When considering tumor site, the analysis showed a significant improvement in local tumor control when hyperthermia was combined with radiation for all sites except lung. This lung study was an International Atomic Energy Agency trial in non-small cell lung cancer patients [124] and the failure to show any benefit may simply reflect poor quality control resulting from poor communication infrastructure in developing countries rather than any biological basis. Even including the results of this trial in the overall analysis, there was still a highly significant better response for radiation and heat compared to radiation alone.
Today, patients typically receive chemotherapy with radiation as part of the standard treatment, so one could question the validity of combining heat and radiation. Several studies have actually shown that including hyperthermia in the radiation/chemotherapy schedule can improve outcome [14,16]. Interestingly, a recent study in which patients with locally advanced cervical cancer were randomized to radiotherapy + hyperthermia or radiotherapy + cisplatin, reported comparable outcome and toxicity between the two treatment arms [131], suggesting hyperthermia might have a role to play as an alternative treatment if chemotherapy tolerance issues arise. Furthermore, hypoxia is often a source of resistance to many clinically used chemotherapeutic agents. This can be a consequence of hypoxia per se, but could also be due to hypoxic cells being distant from blood vessels; thus, creating a drug delivery problem, or because hypoxic cells are generally non-cycling and exist at low pH, both of which can influence drug activity [2,5]. Thus, including hyperthermia in a treatment schedule involving radiation and chemotherapy would seem to be a logical choice.
7. Future Perspectives
The future of hyperthermia involves technical developments and improved approaches for applying current methodology that allows for better and homogeneous tumor heating or being able to reduce the interval between the heat and radiation to the point where a truly simultaneous radiation and heat treatment occur. However, there are a number of biological issues, which have recently become hot topics, in which hypoxia and hyperthermia may play critical roles [132]. The first of these involves immune response. Numerous reviews have addressed the issue of immune modulatory effects of hyperthermia [133,134,135] and different mechanisms have been suggested that involve both the innate and adaptive immune system. When heat is applied to tumor cells they respond by producing heat shock proteins (HSPs) which when become extracellular act as danger signals for the adaptive and innate immune systems [136]. These released HSPs activate NK cells and antigen presenting cells (APCs) and thereby increase the cytotoxic T-cell response [135]. Heat itself can also cause cellular damage and this will lead to the release of damage-associated molecular patterns (DAMPs) which basically has the same effect as the HSPs [133]. There is evidence that immune cells, such as NK cells, CD8+ T-cells, and dendritic cells already in the tumor also become activated when heated [135]. Finally, immune cell trafficking into the tumor can be improved as a result of the vascular effects of heating [134]. More recent studies have shown that the combination of hyperthermia and radiation can further enhance the immune response, probably by the induction of a greater proportion of immunogenic cell death in the tumor [137,138]. The significance of hypoxia in this issue comes from the finding that hypoxia in tumors can have a negative effect on immunogenicity by altering the function of immune cells and/or increasing resistance of tumor cells to the cytolytic activity of immune effectors [139,140]. The elimination of hypoxia by hyperthermia adds to its already established immune modulatory effects. These effects on immune response will not only impact the primary tumor, but should also induce an abscopal effect. Indeed, anti-tumor activity in contralateral tumors that are not actually heated has been reported [141,142], but whether the same applies to truly metastatic disease is not known. Clearly, additional studies into the role of hypoxia in the immune response and its targeting by hyperthermia should be undertaken. Furthermore, these studies should be extended to consider what happens when heat and radiation are combined.
Successful cancer therapy requires targeting both the primary tumor and metastases. The cells within a tumor generally consist of non-stem cells that have a limited proliferative capacity but constitute the bulk of the cancer cells and a subset of cancer stem cells (CSCs) that can both expand the CSC population and differentiate into the various tumor cell populations [143,144]. CSCs are not only important for the growth of the primary tumor, they also play a major role in influencing metastatic spread [145,146]. Evidence exists that such CSCs are also an important factor in influencing response to treatment [144,146]. This is especially true for radiation in which studies have shown that the higher the proportion of CSCs, the greater the level of radiation resistance [147,148]. Part of this resistance may be due to intrinsic factors, such as greater repair capacity, and protection from reactive oxygen species-induced damage [149,150]. However, it is now becoming clear that additional extrinsic factors can influence resistance, especially the micro-environmental parameter of hypoxia [144,145,146]. Although an association between CSCs and hypoxia has been identified, the exact details of this relationship are unclear. It is not known whether CSCs and hypoxia simply co-exist, or whether hypoxia causes recruitment of non-stem cells in to the CSC pool. There is also the issue of how CSCs and hypoxia influence treatment resistance and malignant progression. Studies have reported that CSCs are more radiation resistant than non-stem cells [149], and hypoxia is definitely a critical factor in influencing resistance to radiation [2,5]. However, hypoxia may also increase radiation resistance by preventing cell differentiation and thus maintaining tumor cells in a more resistant undifferentiated “stem-cell-like” state [146,151].
It is also not clear as to how CSCs and hypoxia can influence malignant progression. Undifferentiated cells are more malignant [146,151], and with the hypoxic microenvironment contributing to the undifferentiated state of CSCs, this could partially explain how hypoxia and CSCs increase metastatic spread. Proteases, especially cathepsins (CTSs), are functionally involved in cancer progression including tumor invasion and metastases [152]. CTS expression, especially for CTS-L and K, have been associated with CSCs [153,154]. Such expression is also elevated under hypoxic conditions [155]. Clearly, targeting hypoxia using hyperthermia could be a novel approach for dealing with CSCs and thereby influencing both local response to radiation as well as malignant progression [156].
8. Conclusions
Figure 5 summarizes the critical issues in this review. Hypoxia is a characteristic feature of solid tumors that is a clinically relevant problem because it is a major resistance factor for conventional therapy, especially radiotherapy, and plays a significant role in malignant progression. Effectively decreasing hypoxia would clearly improve response to therapy and reduce the likelihood of metastatic spread. Despite numerous pre-clinical and clinical studies since the 1970s, only one agent has been established as a treatment option against hypoxia, and that is the radio-sensitizer nimorazole and only for treating head and neck patients with radiotherapy in Denmark. Since hyperthermia can effectively target hypoxia via a variety of different mechanisms, and has been shown to improve radiotherapy treatment in a number of tumor sites, it would suggest the application of heat to combat hypoxia should be adopted on a much wider basis, and even established as part of standard cancer therapy.
Author Contributions
The concept for this review was developed by P.B.E. with help from M.R.H. The manuscript was written by P.B.E. with help from M.R.H., B.S.S., A.L.O., N.A.P.F., J.C., and J.O.
Funding
This research was funded by the Danish Cancer Society, grant number R40-A2022-11-S2 and the Danish Council for Independent Research: Medical Sciences, grant number DFF-4004-00362.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Vaupel, P.; Kallinowski, F.; Okunieff, P. Blood flow, oxygen and nutrient supply, and metabolic microenvironment of human tumors: A review. Cancer Res. 1989, 49, 6449–6465. [Google Scholar] [PubMed]
- Horsman, M.R.; Vaupel, P. Pathophysiological basis for the formation of the tumor microenvironment. Front. Oncol. 2016, 6, 66. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. How is blood vessel growth regulated in normal and neoplastic tissue? G.H.A. Clowes memorial Award lecture. Cancer Res. 1986, 46, 467–473. [Google Scholar] [PubMed]
- Horsman, M.R.; Mortensen, L.S.; Petersen, J.B.; Busk, M.; Overgaard, J. Imaging hypoxia to improve radiotherapy outcome. Nat. Rev. Clin. Oncol. 2012, 9, 674–687. [Google Scholar] [CrossRef] [PubMed]
- Siemann, D.W.; Horsman, M.R. Modulation of the tumor vasculature and oxygenation to improve therapy. Pharmacol. Ther. 2015, 153, 107–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overgaard, J.; Horsman, M.R. Modification of hypoxia induced radioresistance in tumours by the use of oxygen and sensitizers. Semin. Radiat. Oncol. 1996, 6, 10–21. [Google Scholar] [CrossRef]
- Horsman, M.R.; Overgaard, J. The impact of hypoxia and its modification of the outcome of radiotherapy. J. Radiat. Res. 2016, 57 (Suppl. 1), 90–98. [Google Scholar] [CrossRef]
- Breasted, J.H. The Edwin Smith surgical papyrus. In Therapeutic Heat and Cold, 2nd ed.; Licht, S., Ed.; Waverly Press: Baltimore, MD, USA, 1930; pp. 196–211. [Google Scholar]
- Storm, K.F. (Ed.) Early history. In Hyperthermia in Cancer Therapy, 1st ed.; G. K. Hall Medical Publishers: Boston MA, USA, 1983; pp. 1–8. [Google Scholar]
- Dewhirst, M.; Stauffer, P.R.; Das, S.; Craciunescu, O.I.; Vujaskovic, Z. Hyperthermia. In Clinical Radiation Oncology, 4th ed.; Gunderson, L.L., Tepper, J.E., Eds.; Elsevier: Philadelphia, PA, USA, 2016; pp. 381–398. ISBN 978-0-323-24098-7. [Google Scholar]
- Trefná, H.D.; Crezee, J.; Schmidt, M.; Marder, D.; Lamprecht, U.; Ehmann, M.; Nadobny, J.; Hartmann, J.; Lomax, N.; Abdel-Rahman, S. Quality assurance guidelines for superficial hyperthermia clinical trials: I. Clinical requirements. Int. J. Hyperth. 2017, 33, 471–482. [Google Scholar] [CrossRef]
- Crezee, H.; van Leeuwen, C.M.; Oei, A.L.; Stalpers, L.J.; Bel, A.; Franken, N.A.; Kok, H.P. Thermoradiotherapy planning: Integration in routine clinical practice. Int. J. Hyperth. 2016, 32, 41–49. [Google Scholar] [CrossRef]
- Bruggmoser, G.; Bauchowitz, S.; Canters, R.; Crezee, H.; Ehmann, M.; Gellermann, J.; Lamprecht, U.; Lomax, N.; Messmer, M.; Ott, O. Guideline for the clinical application, documentation and analysis of clinical studies for regional deep hyperthermia. Strahlenther. Onkol. 2012, 188, 198–211. [Google Scholar] [CrossRef]
- Wust, P.; Hildebrandt, B.; Sreenivasa, G.; Rau, B.; Gellermann, J.; Riess, H.; Felix, R.; Schlag, P. Hyperthermia in combined treatment of cancer. Lancet Oncol. 2002, 3, 487–497. [Google Scholar] [CrossRef]
- Horsman, M.R.; Overgaard, J. Hyperthermia: A Potent Enhancer of Radiotherapy. Clin. Oncol. 2007, 19, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Cihoric, N.; Tsikkinis, A.; van Rhoon, G.; Crezee, H.; Aebersold, D.M.; Bodis, S.; Beck, M.; Nadobny, J.; Budach, V.; Wust, P. Hyperthermia-related clinical trials on cancer treatment within the ClinicalTrials.gov registry. Int. J. Hyperth. 2015, 31, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Peeken, J.C.; Vaupel, P.; Combs, S.E. Integrating hyperthermia into modern radiation oncology: What evidence is necessary? Front. Oncol. 2017, 7, 132. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, J.; Nielsen, O.S.; Lindegaard, J.C. Biological basis for rational design of clinical treatment with combined hyperthermia and radiation. In Phisics and Technology of Hyperthermia; Field, S.B., Franconi, C., Eds.; Springer: Dordrecht, The Netherlands, 1987; pp. 54–79. ISBN 978-94-010-8109-2. [Google Scholar]
- Overgaard, J. The design of clinical trials in hyperthermia. In Phisics and Technology of Hyperthermia; Field, S.B., Franconi, C., Eds.; Springer: Dordrecht, The Netherlands, 1987; pp. 598–620. ISBN 978-94-010-8109-2. [Google Scholar]
- Van Leeuwen, C.M.; Oei, A.L.; Chin, K.W.; Crezee, J.; Bel, A.; Westermann, A.M.; Buist, M.R.; Franken, N.A.; Stalpers, L.J.; Kok, H.P. A short time interval between radiotherapy and hyperthermia reduces in-field recurrence and mortality in women with advanced cervical cancer. Radiat. Oncol. 2017, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Field, S.B.; Bleehen, N.M. Hyperthermia in treatment of cancer. Cancer Treat. Rev. 1979, 6, 63–94. [Google Scholar] [CrossRef]
- Hendry, J.H.; Sutton, M.L. Care with radiosensitizers. Br. J. Radiol. 1978, 51, 927–928. [Google Scholar] [CrossRef]
- Hendry, J.H. Quantitation of the radiotherapeutic importance of naturally-hypoxic normal tissues from collated experiments with rodents using single doses. Int. J. Radiat. Oncol. Biol. Phys. 1979, 5, 971–976. [Google Scholar] [CrossRef]
- Murata, R.; Tsujitani, M.; Horsman, M.R. Enhanced local tumour control after single or fractionated radiation treatment using the hypoxic cell radiosensitizer doranidazole. Radiother. Oncol. 2008, 87, 331–338. [Google Scholar] [CrossRef]
- Porschen, W.; Gartzen, J.; Geweher, K.; Mühlensiepen, H.; Weber, H.-J.; Feinedegen, L. In vivo assay of the radiation sesnitivity of hypoxic tumour cells; influence of γ-rays, cyclotron neutrons, misonidazole, hyperthermia and mixed modalities. Br. J. Cancer 1978, 37 (Suppl. III), 194–197. [Google Scholar]
- Stone, H.B. Enhancement of local tumour control by misonidazole and hyperthermia. Br. J. Cancer 1978, 37 (Suppl. III), 178–183. [Google Scholar]
- Overgaard, J. Effect of misonidazole and hyperthermia on the radiosensitivity of a C3H mouse mammary carcinoma and its surrounding normal tissues. Br. J. Cancer 1980, 41, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Horsman, M.R.; Overgaard, J. Combination of nicotinamide and hyperthermia to eliminate radioresistant chronically and acutely hypoxic tumour cells. Cancer Res. 1990, 50, 7430–7436. [Google Scholar] [PubMed]
- Oleson, J.R. Eugene Robertson Special Lecture: Hyperthermia from the clinic to the laboratory: A hypothesis. Int. J. Hyperth. 1995, 11, 315–322. [Google Scholar] [CrossRef]
- Iwata, K.; Shakil, A.; Hur, W.; Makepeace, C.; Griffin, R.; Song, C. Tumour pO2 can be increased markedly by mild hyperthermia. Br. J. Cancer 1996, 74 (Suppl. XXVII), S217–S221. [Google Scholar]
- Horsman, M.R.; Overgaard, J. Can mild hyperthermia improve tumour oxygenation? Int. J. Hyperth. 1997, 13, 141–147. [Google Scholar] [CrossRef]
- Vaupel, P.W.; Kelleher, D.K. Pathophysiological and vascular characteristics of tumours and their importance for hyperthermia: Heterogeneity is the key issue. Int. J. Hyperth. 2010, 26, 211–223. [Google Scholar] [CrossRef]
- Sen, A.; Capitano, M.L.; Spernyak, J.A.; Schueckler, J.T.; Thomas, S.; Singh, A.K.; Evans, S.S.; Hylander, B.; Repasky, E.A. Mild elevation of body temperature reduces tumor interstitial fluid pressure and hypoxia and enhances efficacy of radiotherapy in murine tumor models. Cancer Res. 2011, 71, 3872–3880. [Google Scholar] [CrossRef]
- Winslow, T.B.; Eranki, A.; Ullas, S.; Singh, A.K.; Repasky, E.A.; Sen, A. A pilot study of the effects of mild systemic heating on human head and neck tumour xenografts: Analysis of tumour perfusion, interstitial fluid pressure, hypoxia and efficacy of radiation therapy. Int. J. Hyperth. 2015, 31, 693–701. [Google Scholar] [CrossRef]
- Song, C.W. Effect of local hyperthermia on blood flow and microenvironment: A review. Cancer Res. 1984, 44, 4721–4730. [Google Scholar]
- Xu, Y.; Choi, J.; Hylander, B.; Sen, A.; Evans, S.S.; Kraybill, W.G.; Repasky, E.A. Fever-range whole body hyperthermia increases the number of perfused tumor blood vessels and therapeutic efficacy of liposomally encapsulated doxorubicin. Int. J. Hyperth. 2007, 23, 513–527. [Google Scholar] [CrossRef] [PubMed]
- Griffin, R.J.; Okajima, K.; Barrios, B.; Song, C.W. Mild temperature hyperthermia combined with carbogen breathing increases tumor partial pressure of oxygen (pO2) and radiosensitivity. Cancer Res. 1996, 56, 5590–5593. [Google Scholar] [PubMed]
- Song, C.W.; Patten, M.S.; Chelstrom, L.M.; Rhee, J.G.; Levitt, S.H. Effect of multiple heatings on the blood flow in RIF-1 tumours, skin and muscle of C3H mice. Int. J. Hyperth. 1987, 3, 535–545. [Google Scholar] [CrossRef]
- Durand, R.E. Potentiation of radiation lethality by hyperthermia in a tumor model: Effects of sequence, degree, and duration of heating. Int. J. Radiat. Oncol. Biol. Phys. 1978, 4, 401–405. [Google Scholar] [CrossRef]
- Ansiaux, R.; Baudelet, C.; Jordan, B.F.; Crokart, N.; Martinive, P.; DeWever, J.; Grégoire, V.; Feron, O.; Gallez, B. Mechanism of reoxygenation after antiangiogenic therapy using SU5416 and its importance for guiding combined antitumor therapy. Cancer Res. 2006, 66, 9698–9704. [Google Scholar] [CrossRef] [PubMed]
- Zannella, V.E.; Dal Pra, A.; Muaddi, H.; McKee, T.D.; Stapleton, S.; Sykes, J.; Glicksman, R.; Chaib, S.; Zamiara, P.; Milosevic, M. Reprogramming metabolism with metformin improves tumor oxygenation and radiotherapy response. Clin. Cancer Res. 2013, 19, 6741–6750. [Google Scholar] [CrossRef] [PubMed]
- Shakil, A.; Osborn, J.L.; Song, C.W. Changes in oxygenation status and blood flow in a rat tumor model by mild temperature hyperthermia. Int. J. Radiat. Oncol. 1999, 43, 859–865. [Google Scholar] [CrossRef]
- Song, C.W.; Park, H.; Griffin, R.J. Improvement of tumor oxygenation by mild hyperthermia. Radiat. Res. 2001, 155, 515–528. [Google Scholar] [CrossRef]
- Song, C.W.; Shakil, A.; Osborn, J.L.; Iwata, K. Tumour oxygenation is increased by hyperthermia at mild temperatures. Int. J. Hyperth. 2009, 25, 91–95. [Google Scholar] [CrossRef]
- Vujaskovic, Z.; Song, C.W. Physiological mechanisms underlying heat-induced radiosensitization. Int. J. Hyperth. 2004, 20, 163–174. [Google Scholar] [CrossRef]
- Brizel, D.M.; Scully, S.P.; Harrelson, J.M.; Layfield, L.J.; Dodge, R.K.; Charles, H.C.; Samulski, T.V.; Prosnitz, L.R.; Dewhirst, M.W. Radiation therapy and hyperthermia improve the oxygenation of human soft tissue sarcomas. Cancer Res. 1996, 56, 5347–5350. [Google Scholar] [PubMed]
- Jones, E.L.; Prosnitz, L.R.; Dewhirst, M.W.; Marcom, P.K.; Hardenbergh, P.H.; Marks, L.B.; Brizel, D.M.; Vujaskovic, Z. Thermochemoradiotherapy improves oxygenation in locally advanced breast cancer. Clin. Cancer Res. 2004, 10, 4287–4293. [Google Scholar] [CrossRef] [PubMed]
- Hetzel, F.W.; Chopp, M.; Dereski, M.O. Variations in pO2 and pH response to hyperthermia: Dependence on transplant site and duration of treatment. Radiat. Res. 1992, 131, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Howard-Flanders, P.; Moore, D. The time interval after pulsed irradiation within which injury in bacteria can be modified by dissolved oxygen. I. A search for an effect of oxygen 0.002 seconds after pulsed irradiation. Radiat. Res. 1958, 9, 422–437. [Google Scholar] [CrossRef] [PubMed]
- Michael, B.; Adams, G.; Hewitt, H.; Jones, W.; Watts, M. A post-effect of oxygen in irradiated bacteria: A submillisecond fast mixing study. Radiat. Res. 1973, 54, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Cannan, W.J.; Pederson, D.S. Mechanisms and Consequences of Double-Strand DNA Break Formation in Chromatin. J. Cell. Physiol. 2016, 231, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Lydeard, J.R.; Lipkin-Moore, Z.; Sheu, Y.-J.; Stillman, B.; Burgers, P.M.; Haber, J.E. Break-induced replication requires all essential DNA replication factors except those specific for pre-RC assembly. Genes Dev. 2010, 24, 1133–1144. [Google Scholar] [CrossRef] [Green Version]
- Kuzminov, A. Single-strand interruptions in replicating chromosomes cause double-strand breaks. Proc. Natl. Acad. Sci. USA 2001, 98, 8241–8246. [Google Scholar] [CrossRef] [Green Version]
- Takata, M.; Sasaki, M.S.; Sonoda, E.; Morrison, C.; Hashimoto, M.; Utsumi, H.; Yamaguchi-Iwai, Y.; Shinohara, A.; Takeda, S. Homologous recombination and non-homologous end-joining pathways of DNA double-strand break repair have overlapping roles in the maintenance of chromosomal integrity in vertebrate cells. EMBO J. 1998, 17, 5497–5508. [Google Scholar] [CrossRef] [Green Version]
- Jackson, S.P. Sensing and repairing DNA double-strand breaks. Carcinogenesis 2002, 23, 687–696. [Google Scholar] [CrossRef] [Green Version]
- Fleck, O.; Nielsen, O. DNA repair. J. Cell Sci. 2004, 117 Pt 4, 515–517. [Google Scholar] [CrossRef] [Green Version]
- Davis, A.J.; Chen, D.J. DNA double strand break repair via non-homologous end-joining. Transl. Cancer Res. 2013, 2, 130–143. [Google Scholar] [CrossRef] [PubMed]
- Jasin, M.; Rothstein, R. Repair of strand breaks by homologous recombination. Cold Spring Harb. Perspect. Biol. 2013, 5, a012740. [Google Scholar] [CrossRef] [PubMed]
- Kuo, L.J.; Yang, L.-X. Gamma-H2AX—A novel biomarker for DNA double-strand breaks. In Vivo 2008, 22, 305–309. [Google Scholar] [PubMed]
- El-Awady, R.A.; Dikomey, E.; Dahm-Daphi, J. Heat effects on DNA repair after ionising radiation: Hyperthermia commonly increases the number of non-repaired double-strand breaks and structural rearrangements. Nucleic Acids Res. 2001, 29, 1960–1966. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, C.; Oei, A.; Ten Cate, R.; Franken, N.; Bel, A.; Stalpers, L.; Crezee, J.; Kok, H. Measurement and analysis of the impact of time-interval, temperature and radiation dose on tumour cell survival and its application in thermoradiotherapy plan evaluation. Int. J. Hyperth. 2018, 34, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Ihara, M.; Takeshita, S.; Okaichi, K.; Okumura, Y.; Ohnishi, T. Heat exposure enhances radiosensitivity by depressing DNA-PK kinase activity during double strand break repair. Int. J. Hyperth. 2014, 30, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Krawczyk, P.M.; Eppink, B.; Essers, J.; Stap, J.; Rodermond, H.; Odijk, H.; Zelensky, A.; van Bree, C.; Stalpers, L.J.; Buist, M.R.; et al. Mild hyperthermia inhibits homologous recombination, induces BRCA2 degradation, and sensitizes cancer cells to poly (ADP-ribose) polymerase-1 inhibition. Proc. Natl. Acad. Sci. USA 2011, 108, 9851–9856. [Google Scholar] [CrossRef] [Green Version]
- Gilbertson, R.J.; Rich, J.N. Making a tumour’s bed: Glioblastoma stem cells and the vascular niche. Nat. Rev. Cancer 2007, 7, 733–736. [Google Scholar] [CrossRef]
- Zölzer, F.; Streffer, C.; Pelzer, T. Induction of quiescent S-phase cells by irradiation and/or hyperthermia. II. Correlation with colony forming ability. Int. J. Radiat. Biol. 1993, 63, 77–82. [Google Scholar] [CrossRef]
- Dewey, W.C.; Hopwood, L.E.; Sapareto, S.A.; Gerweck, L.E. Cellular responses to combinations of hyperthermia and radiation. Radiology 1977, 123, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, O.S.; Henle, K.J.; Overgaard, J. Arrhenius analysis of survival curves from thermotolerant and step-down heated L1A2 cells in vitro. Radiat. Res. 1982, 91, 468–482. [Google Scholar] [CrossRef] [PubMed]
- Roizin-Towle, L.; Pirro, J.P. The response of human and rodent cells to hyperthermia. Int. J. Radiat. Oncol. 1991, 20, 751–756. [Google Scholar] [CrossRef]
- Overgaard, J.; Bichel, P. The Influence of Hypoxia and Acidity on the Hyperthermic Response of Malignant Cells In Vitro. Radiology 1977, 123, 511–514. [Google Scholar] [CrossRef] [PubMed]
- Gerweck, L.E.; Nygaard, T.G.; Burlett, M. Response of cells to hyperthermia under acute and chronic hypoxic conditions. Cancer Res. 1979, 39, 966–972. [Google Scholar] [PubMed]
- Overgaard, J. Effect of hyperthermia on the hypoxic fraction in an experimental mammary carcinoma in vivo. Br. J. Radiol. 1981, 54, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Field, S.B.; Anderson, R.L. Thermotolerance: A review of observations and possible mechanisms. Natl. Cancer Inst. Monogr. 1982, 61, 193–201. [Google Scholar]
- Lindegaard, J.C.; Overgaard, J. Factors of importance for the development of the step-down heating effect in a C3H mammary carcinoma in vivo. Int. J. Hyperth. 1987, 3, 79–91. [Google Scholar] [CrossRef]
- Dings, R.P.; Loren, M.L.; Zhang, Y.; Mikkelson, S.; Mayo, K.H.; Corry, P.; Griffin, R.J. Tumour thermotolerance, a physiological phenomenon involving vessel normalization. Int. J. Hyperth. 2011, 27, 42–52. [Google Scholar] [CrossRef]
- Jain, R.K. Normalizing tumor vasculature with anti-angiogenic therapy: A new paradigm for combination therapy. Nat. Med. 2001, 7, 987–989. [Google Scholar] [CrossRef]
- Winkler, F.; Kozin, S.V.; Tong, R.T.; Chae, S.S.; Booth, M.F.; Garkavtsev, I.; Xu, L.; Hicklin, D.J.; Fukumura, D.; di Tomaso, E.; et al. Kinetics of vascular normalization by VEGFR2 blockade governs brain tumor response to radiation: Role of oxygenation, angiopoietin-1, and matrix metalloproteinases. Cancer Cell 2004, 6, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Harmon, B.V.; Corder, A.M.; Collins, R.J.; Gobé, G.C.; Allen, J.; Allan, D.J.; Kerr, J.F. Cell death induced in a murine mastocytoma by 42–47 °C heating in vitro: Evidence that the form of death changes from apoptosis to necrosis above a critical heat load. Int. J. Radiat. Biol. 1990, 58, 845–858. [Google Scholar] [CrossRef] [PubMed]
- Kampinga, H.H. Thermotolerance in mammalian cells: Protein denaturation and aggregation, and stress proteins. J. Cell Sci. 1993, 104, 11–17. [Google Scholar] [PubMed]
- Roti Roti, J.L.; Kampinga, H.H.; Malyapa, R.S.; Wright, W.D.; vanderWaal, R.P.; Xu, M. Nuclear matrix as a target for hyperthermic killing of cancer cells. Cell Stress Chaperones 1998, 3, 245–255. [Google Scholar] [CrossRef]
- Vertrees, R.A.; Das, G.C.; Coscio, A.M.; Xie, J.; Zwischenberger, J.B.; Boor, P.J. A mechanism of hyperthermia-induced apoptosis in ras-transformed lung cells. Mol. Carcinog. 2005, 44, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Lepock, J.R. Cellular effects of hyperthermia: Relevance to the minimum dose for thermal damage. Int. J. Hyperth. 2003, 19, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Heacock, C.S.; Brown, S.L.; Bamburg, J.R. In vitro inactivation of actin by heat. Natl. Cancer Inst. Monogr. 1982, 61, 73–75. [Google Scholar]
- Horsman, M.R. Tissue physiology and the response to heat. Int. J. Hyperth. 2006, 22, 197–203. [Google Scholar] [CrossRef]
- Horsman, M.R.; Siemann, D.W. Pathophysiological effects of vascular targeting agents and the implications for combination with conventional therapies. Cancer Res. 2006, 66, 11520–11539. [Google Scholar] [CrossRef]
- Horsman, M.R. Angiogenesis and vascular targeting: Relevance for hyperthermia. Int. J. Hyperth. 2008, 24, 57–65. [Google Scholar] [CrossRef]
- Tozer, G.M.; Kanthou, C.; Baguley, B.C. Disrupting tumour blood vessels. Nat. Rev. Cancer 2005, 5, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Siemann, D.W.; Chaplin, D.J.; Horsman, M.R. Realizing the potential of vascular targeted therapy: The rationale for combining vascular disrupting agents and anti-angiogenic agents to treat cancer. Cancer Investig. 2017, 35, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Horsman, M.R.; Aarhus University, Aarhus, Denmark. Personal communication, 2018.
- Ling, C.C.; Humm, J.; Larson, S.; Amols, H.; Fuks, Z.; Leibel, S.; Koutcher, J.A. Towards multidimensional radiotherapy (MD-CRT): Biological imaging and biological conformality. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 551–560. [Google Scholar] [CrossRef]
- Epel, B.; Maggio, M.C.; Barth, E.D.; Miller, R.C.; Pelizzari, C.A.; Krzykawska-Serda, M.; Sundramoorthy, S.V.; Aydogan, B.; Weichselbaum, R.R.; Tormyshev, V.M.; et al. Oxygen-guided radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2018. [Google Scholar] [CrossRef] [PubMed]
- Barendsen, G.W. Responses of cultured cells, tumours and normal tissues to radiations of different linear energy transfer. Curr. Top. Radiat. Res. Q. 1968, 4, 293–356. [Google Scholar]
- Wenzl, T.; Wilkens, J.J. Modelling of the oxygen enhancement ratio for ion beam radiation therapy. Phys. Med. Biol. 2011, 56, 3251–3268. [Google Scholar] [CrossRef] [PubMed]
- Particle Therapy Facilities in Clinical Operation (Last Update: January 2019). Available online: https://www.ptcog.ch/index.php/facilities-in-operation (accessed on 7 January 2019).
- Datta, N.R.; Puric, E.; Schneider, R. Could hyperthermia with proton therapy mimic carbon ion therapy? Exploring a thermo-radiobiological rationale. Int. J. Hyperth. 2014, 30, 524–530. [Google Scholar] [CrossRef]
- Gerner, E.W.; Leith, J.T. Interaction of hyperthermia with radiations of different linear energy transfer. Int. J. Radiat. Biol. 1977, 31, 283–288. [Google Scholar] [CrossRef]
- Karger, C.P.; Peschke, P. RBE and related modelling in carbon-ion therapy. Phys. Med. Biol. 2018, 63, 01TR02. [Google Scholar] [CrossRef]
- Horsman, M.R. The therapeutic potential of using the vascular disrupting agent OXi4503 to enhance mild temperature thermoradiation. Int. J. Hyperth. 2015, 31, 453–459. [Google Scholar] [CrossRef]
- Lühr, A.; von Neubeck, C.; Pawelke, J.; Seidlitz, A.; Peitzsch, C.; Bentzen, S.M.; Bortfeld, T.; Debus, J.; Deutsch, E.; Langendijk, J.A.; et al. “Radiobiology of Proton Therapy”: Results of an international expert workshop. Radiother. Oncol. 2018, 128, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Ray, S.; Cekanaviciute, E.; Lima, I.P.; Sørensen, B.S.; Costes, S.V. Comparing Photon and Charged Particle Therapy Using DNA Damage Biomarkers. Int. J. Part. Ther. 2018, 5, 15–24. [Google Scholar] [CrossRef]
- Willers, H.; Allen, A.; Grosshans, D.; McMahon, S.J.; von Neubeck, C.; Wiese, C.; Vikram, B. Toward A variable RBE for proton beam therapy. Radiother. Oncol. 2018, 128, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Suetens, A.; Konings, K.; Moreels, M.; Quintens, R.; Verslegers, M.; Soors, E.; Tabury, K.; Grégoire, V.; Baatout, S. Higher Initial DNA Damage and Persistent Cell Cycle Arrest after Carbon Ion Irradiation Compared to X-irradiation in Prostate and Colon Cancer Cells. Front. Oncol. 2016, 6, 87. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, F.; Campa, A.; Esposito, G.; Giardullo, P.; Belli, M.; Dini, V.; Meschini, S.; Simone, G.; Sorrentino, E.; Gerardi, S.; et al. Induction and Repair of DNA DSB as Revealed by H2AX Phosphorylation Foci in Human Fibroblasts Exposed to Low- and High-LET Radiation: Relationship with Early and Delayed Reproductive Cell Death. Radiat. Res. 2015, 183, 417–431. [Google Scholar] [CrossRef] [PubMed]
- Grosse, N.; Fontana, A.O.; Hug, E.B.; Lomax, A.; Coray, A.; Augsburger, M.; Paganetti, H.; Sartori, A.A.; Pruschy, M.; et al. Deficiency in homologous recombination renders mammalian cells more sensitive to proton versus photon irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.; Marshall, T.I.; Currell, F.J.; Kacperek, A.; Schettino, G.; Prise, K.M. Variations in the Processing of DNA Double-Strand Breaks Along 60-MeV Therapeutic Proton Beams. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Hojo, H.; Dohmae, T.; Hotta, K.; Kohno, R.; Motegi, A.; Yagishita, A.; Makinoshima, H.; Tsuchihara, K.; Akimoto, T. Difference in the relative biological effectiveness and DNA damage repair processes in response to proton beam therapy according to the positions of the spread out Bragg peak. Radiat. Oncol. 2017, 12, 111. [Google Scholar] [CrossRef]
- Kavanagh, J.N.; Currell, F.J.; Timson, D.J.; Savage, K.I.; Richard, D.J.; McMahon, S.J.; Hartley, O.; Cirrone, G.A.; Romano, F.; Prise, K.M.; et al. Antiproton induced DNA damage: Proton like in flight, carbon-ion like near rest. Sci. Rep. 2013, 3, 1770. [Google Scholar] [CrossRef]
- Wang, H.; Wang, X.; Zhang, P.; Wang, Y. The Ku-dependent non-homologous end-joining but not other repair pathway is inhibited by high linear energy transfer ionizing radiation. DNA Repair 2008, 7, 725–733. [Google Scholar] [CrossRef]
- Gerelchuluun, A.; Manabe, E.; Ishikawa, T.; Sun, L.; Itoh, K.; Sakae, T.; Suzuki, K.; Hirayama, R.; Asaithamby, A.; Chen, D.J.; et al. The Major DNA Repair Pathway after Both Proton and Carbon-Ion Radiation is NHEJ, but the HR Pathway is More Relevant in Carbon Ions. Radiat. Res. 2015, 183, 345–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontana, A.O.; Augsburger, M.A.; Grosse, N.; Guckenberger, M.; Lomax, A.J.; Sartori, A.A.; Pruschy, M.N. Differential DNA repair pathway choice in cancer cells after proton- and photon-irradiation. Radiother. Oncol. 2015, 116, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ghosh, P.; Magpayo, N.; Testa, M.; Tang, S.; Gheorghiu, L.; Biggs, P.; Paganetti, H.; Efstathiou, J.A.; Lu, H.M.; et al. Lung Cancer Cell Line Screen Links Fanconi Anemia/BRCA Pathway Defects to Increased Relative Biological Effectiveness of Proton Radiation. Int. J. Radiat. Oncol. 2015, 91, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Maeda, J.; Fujii, Y.; Fujisawa, H.; Hirakawa, H.; Cartwright, I.M.; Uesaka, M.; Kitamura, H.; Fujimori, A.; Kato, T.A. Hyperthermia-induced radiosensitization in CHO wild-type, NHEJ repair mutant and HR repair mutant following proton and carbon-ion exposure. Oncol. Letts. 2015, 10, 2828–2834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, P.Y.; Tobias, C.A.; Blakely, E.A. Protein synthesis modulates the biological effectiveness of the combined action of hyperthermia and high-LET radiation. Radiat. Res. 1992, 129, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Kinashi, Y.; Masunaga, S.I.; Suzuki, M.; Ono, K.; Ohnishi, T. Hyperthermia enhances thermal-neutron-induced cell death of human glioblastoma cell lines at low concentrations of 10B. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 1185–1192. [Google Scholar] [CrossRef]
- Takahashi, A.; Ohnishi, K.; Wang, X.; Kobayashi, M.; Matsumoto, H.; Tamamoto, T.; Aoki, H.; Furusawa, Y.; Yukawa, O.; Ohnishi, T. The dependence of p53 on the radiation enhancement of thermosensitivity at different let. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 489–494. [Google Scholar] [CrossRef]
- Takahashi, A.; Ohnishi, K.; Ota, I.; Asakawa, I.; Tamamoto, T.; Furusawa, Y.; Matsumoto, H.; Ohnishi, T. p53-dependent thermal enhancement of cellular sensitivity in human squamous cell carcinomas in relation to LET. Int. J. Radiat. Biol. 2001, 77, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Huilgol, N.G.; Gupta, S.; Sridhar, C.R. Hyperthermia with radiation in the treatment of locally advanced head and neck cancer: A report of randomized trial. J. Cancer Res. Ther. 2010, 6, 492–496. [Google Scholar] [CrossRef]
- Datta, N.R.; Bose, A.K.; Kapoor, H.K.; Gupta, S. Head and neck cancers: Results of thermoradiotherapy versus radiotherapy. Int. J. Hyperth. 1990, 6, 479–486. [Google Scholar] [CrossRef]
- Valdagni, R.; Amichetti, M. Report of Long-term follow-up in a randomized trial comparing radiation therapy and radiation therapy plus hyperthermia to metastatic lymphnodes in stage IV head and neck patients. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 163–169. [Google Scholar] [CrossRef]
- Harima, Y.; Nagata, K.; Harima, K.; Ostapenko, V.V.; Tanaka, Y.; Sawada, S. A randomized clinical trial of radiation therapy versus thermoradiotherapy in stage IIIB cervical carcinoma. Int. J. Hyperth. 2001, 17, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Van der Zee, J.; González, G.D. The Dutch Deep Hyperthermia Trial: Results in cervical cancer. Int. J. Hyperth 2002, 18, 1–12. [Google Scholar]
- Franckena, M.; Stalpers, L.J.; Koper, P.C.; Wiggenraad, R.G.; Hoogenraad, W.J.; Van Dijk, J.D.; Wárlám-Rodenhuis, C.C.; Jobsen, J.J.; van Rhoon, G.C.; van der Zee, J. Long-term improvement in treatment outcome after radiotherapy and hyperthermia in locoregionally advanced cervix cancer: An update of the Dutch Deep Hyperthermia Trial. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Van Der Zee, J.; González, D.G.; van Rhoon, G.C.; van Dijk, J.D.P.; van Putten, W.L.J. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Vernon, C.C.; Hand, J.W.; Field, S.B.; Machin, D.; Whaley, J.B.; van der Zee, J.; van Putten, W.L.; van Rhoon, G.C.; van Dijk, J.D.; González González, D.; et al. Radiotherapy with or without hyperthermia in the treatment of superficial localized breast cancer: Results from five randomized controlled trials. International Collaborative Hyperthermia Group. Int. J. Radiat. Oncol. Biol. Phys. 1996, 35, 731–744. [Google Scholar] [CrossRef] [PubMed]
- Mitsumori, M.; Zeng, Z.F.; Oliynychenko, P.; Park, J.H.; Choi, I.B.; Tatsuzaki, H.; Tanaka, Y.; Hiraoka, M. Regional hyperthermia combined with radiotherapy for locally advanced non-small cell lung cancers: A multi-institutional prospective randomized trial of the International Atomic Energy Agency. Int. J. Clin. Oncol. 2007, 12, 192–198. [Google Scholar] [CrossRef]
- Overgaard, J.; Gonzalez Gonzalez, D.; Hulshof, M.C.; Arcangeli, G.; Dahl, O.; Mella, O.; Bentzen, S.M. Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. Lancet 1995, 345, 540–543. [Google Scholar] [CrossRef]
- Jones, E.L.; Oleson, J.R.; Prosnitz, L.R.; Samulski, T.V.; Vujaskovic, Z.; Yu, D.; Sanders, L.L.; Dewhirst, M.W. Randomized Trial of Hyperthermia and Radiation for Superficial Tumors. J. Clin. Oncol. 2005, 23, 3079–3085. [Google Scholar] [CrossRef]
- Berdov, B.A.; Menteshashvili, G.Z. Thermoradiotherapy of patients with locally advanced carcinoma of the rectum. Int. J. Hyperth. 1990, 6, 881–890. [Google Scholar] [CrossRef]
- Egawa, S.; Tsukiyama, I.; Watanabe, S.; Ohno, Y.; Morita, K.; Tominaga, S.; Onoyama, Y.; Hashimoto, S.; Yanagawa, S.; Uehara, S.; et al. A randomized clinical trial of hyperthermia and radiation versus radiation alone for superficially located cancers. J. Jpn. Soc. Ther. Radiol. Oncol. 1989, 1, 135–140. [Google Scholar] [CrossRef]
- Perez, C.A.; Pajak, T.; Emami, B.; Hornback, N.B.; Tupchong, L.; Rubin, P. Randomized phase III study comparing irradiation and hyperthermia with radiation alone in superficial measureable tumors. Am. J. Clin. Oncol. 1991, 14, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, J.; Aarhus University, Aarhus, Denmark. Personal communication, 2018.
- Lutgens, L.C.; Koper, P.C.; Jobsen, J.J.; van der Steen-Banasik, E.M.; Creutzberg, C.L.; van den Berg, H.A.; Ottevanger, P.B.; van Rhoon, G.C.; van Doorn, H.C.; Houben, R.; et al. Radiation therapy combined with hyperthermia versus cisplatin for locally advanced cervical cancer: Results of the randomized RADCHOC trial. Radiother. Oncol. 2016, 120, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Lee, C.-T.; Ashcraft, K.A. The future of biology in driving the field of hyperthermia. Int. J. Hyperth. 2016, 32, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Frey, B.; Weiss, E.M.; Rubner, Y.; Wunderlich, R.; Ott, O.J.; Sauer, R.; Fietkau, R.; Gaipl, U.S. Old and new facts about hyperthermia-induced modulations of the immune system. Int. J. Hyperth. 2012, 28, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Repasky, E.A.; Evans, S.S.; Dewhirst, M.W. Temperature matters! And why it should matter to tumor immunologists. Cancer Immunol. Res. 2013, 1, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Toraya-Brown, S.; Fiering, S. Local tumour hyperthermia as immunotherapy for metastatic cancer. Int. J. Hyperth. 2014, 30, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Multhoff, G.; Pockley, A.G.; Streffer, C.; Gaipl, U.S. Dual role of heat shock proteins (HSPs) in anti-tumor immunity. Curr. Mol. Med. 2012, 12, 1174–1182. [Google Scholar] [CrossRef]
- Finkel, P.; Frey, B.; Mayer, F.; Bösl, K.; Werthmöller, N.; Mackensen, A.; Gaipl, U.S.; Ullrich, E. The dual role of NK cells in antitumor reactions triggered by ionizing radiation in combination with hyperthermia. Oncoimmunology 2012, 5, e1101206. [Google Scholar] [CrossRef]
- Werthmöller, N.; Frey, B.; Rückert, M.; Lotter, M.; Fietkau, R.; Gaipl, U.S. Combination of ionising radiation with hyperthermia increases the immunogenic potential of B16-F10 melanoma cells in vitro and in vivo. Int. J. Hyperth. 2016, 32, 23–30. [Google Scholar] [CrossRef]
- Barsoum, I.B.; Koti, M.; Siemens, D.R.; Graham, C.H. Mechanisms of hypoxia-mediated immune escape in cancer. Cancer Res. 2014, 74, 7185–7190. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, S.M.; Kjaergaard, J.; Lukashev, D. Immunological mechanisms of the antitumor effects of supplemental oxygenation. Sci. Transl. Med. 2015, 7, 277ra30. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, L.; Shi, Y.; Javidiparsijani, S.; Wang, G.; Li, X.; Ouyang, W.; Zhou, J.; Zhao, L.; Wang, X.; et al. Abscopal antitumor immune effects of magnet-mediated hyperthermia at a high therapeutic temperature on Walker-256 carcinosarcomas in rats. Oncol. Lett. 2014, 7, 764–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoopes, P.J.; Mazur, C.M.; Osterberg, B.; Song, A.; Gladstone, D.J.; Steinmetz, N.F.; Veliz, F.A.; Bursey, A.A.; Wagner, R.J.; Fiering, S.N. Effect of intra-tumoral magnetic nanoparticle hyperthermia and viral nanoparticle immunogenicity on primary and metastatic cancer. Proc SPIE Int. Soc. Opt. Eng. 2017. [Google Scholar] [CrossRef]
- Clarke, M.F.; Dick, J.E.; Dirks, P.B.; Eaves, C.J.; Jamieson, C.H.; Jones, D.L.; Visvader, J.; Weissman, I.L.; Wahl, G.M. Cancer stem cells—Perspectives on current status and future directions: AACR workshop on cancer stem cells. Cancer Res. 2006, 66, 9339–9344. [Google Scholar] [CrossRef] [PubMed]
- Baumann, M.; Krause, M.; Hill, R. Exploring the role of cancer stem cells in radioresistance. Nat. Rev. Cancer 2008, 8, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Hill, R.P.; Marie-Egyptienne, D.Y.T.; Hedley, D.W. Cancer stem cells, hypoxia and metastasis. Semin. Radiat. Oncol. 2009, 19, 106–111. [Google Scholar] [CrossRef]
- Marie-Egyptienne, D.T.; Lohse, I.; Hill, R.P. Cancer stem cells, the epithelial to mesenchymal transition (EMT) and radioresistance: Potential role of hypoxia. Cancer Lett. 2013, 341, 63–72. [Google Scholar] [CrossRef]
- Hill, R.P.; Milas, L. The proportion of stem cells in murine tumors. Int. J. Radiat. Oncol. Biol. Phys. 1989, 16, 513–518. [Google Scholar] [CrossRef]
- Yaromina, A.; Krause, M.; Thames, H.; Rosner, A.; Krause, M.; Hessel, F.; Grenman, R.; Zips, D.; Baumann, M. Pre-treatment number of clonogenic tumour cells and their radiosensitivity are major determinants of local tumour control after fractionated irradiation. Radiother. Oncol. 2007, 83, 304–310. [Google Scholar] [CrossRef]
- Bao, S.; Wu, Q.; McLendon, R.E.; Hao, Y.; Shi, Q.; Hjelmeland, A.B.; Dewhirst, M.W.; Bigner, D.D.; Rich, J.N. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 2006, 444, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Diehn, M.; Cho, R.W.; Lobo, N.A.; Kalisky, T.; Dorie, M.J.; Kulp, A.N.; Qian, D.; Lam, J.S.; Ailles, L.E.; Wong, M.; et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature 2009, 458, 780–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.; Lin, Q.; Glazer, P.M.; Yun, Z. Hypoxic tumor microenvironment and cancer cell differentiation. Curr. Mol. Med. 2009, 9, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Verbovsek, U.; van Noorden, C.J.F.; Lah, T.T. Complexity of cancer protease biology: Cathepsin K expression and function in cancer progression. Semin. Cancer Biol. 2015, 35, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Hira, V.V.; Ploegmakers, K.J.; Grevers, F.; Verbovšek, U.; Silvestre-Roig, C.; Aronica, E.; Tigchelaar, W.; Turnšek, T.L.; Molenaar, R.J.; Van Noorden, C.J. CD133+ and nestin+ glioma stem-like cells reside around CD31+ arterioles in niches that express SDF-1α, CXCR4, osteopontin and cathepsin K. J. Histochem. Cytochem. 2015, 63, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Long, L.; Wang, L.; Tan, C.; Fei, X.; Chen, L.; Huang, Q.; Liang, Z. Knockdown of cathepsin L promotes radiosensitivity of glioma stem cells both in vivo and in vitro. Cancer Lett. 2016, 371, 274–284. [Google Scholar] [CrossRef]
- Sudhan, D.R.; Siemann, D.W. Cathepsin L inhibition by the small molecule KGP94 suppresses tumor microenvironment enhanced metastasis associated cell functions of prostate and breast cancer cells. Clin. Exp. Metastasis 2013, 30, 891–902. [Google Scholar] [CrossRef] [Green Version]
- Oei, A.L.; Vriend, L.E.; Krawczyk, P.M.; Horsman, M.R.; Franken, N.A.; Crezee, J. Targeting therapy-resistant cancer stem cells by hyperthermia. Int. J. Hyperth. 2017, 33, 419–427. [Google Scholar] [CrossRef]
Figure 1.
(A) Influence of time interval and sequence between radiation and hyperthermia (42.5 °C; 60 min) on tumor control in C3H mammary carcinomas (●) or moist desquamation in normal skin (○). (B) Effect of heating time and temperature on the thermal enhancement ratio (TER) for tumor control in a C3H mammary carcinoma when radiation and hyperthermia were given either simultaneously (solid symbols) or tumors irradiated and then heated 4 h later (open symbols); the heat temperatures are indicated. For both figures the TERs were determined from full radiation dose-response curves and represent the ratio of the radiation dose for radiation alone to that for radiation + heat to produce a response in 50% of animals. (Modified from [18,19]).
Figure 1.
(A) Influence of time interval and sequence between radiation and hyperthermia (42.5 °C; 60 min) on tumor control in C3H mammary carcinomas (●) or moist desquamation in normal skin (○). (B) Effect of heating time and temperature on the thermal enhancement ratio (TER) for tumor control in a C3H mammary carcinoma when radiation and hyperthermia were given either simultaneously (solid symbols) or tumors irradiated and then heated 4 h later (open symbols); the heat temperatures are indicated. For both figures the TERs were determined from full radiation dose-response curves and represent the ratio of the radiation dose for radiation alone to that for radiation + heat to produce a response in 50% of animals. (Modified from [18,19]).

Figure 2.
The radio-sensitizing effect of nitro-aromatic drugs and hyperthermia in a C3H mammary carcinoma. The sensitizer enhancement ratios (SERs) were calculated from full radiation dose-response curves of tumor control and represent the ratio of the radiation dose for radiation alone to that for radiation + sensitizer to produce a response in 50% of animals. The drug treatments were misonidazole (○), nimorazole (□), and doranidazole (△), with different drug doses administered as a single intraperitoneal (misonidazole and nimorazole) or intravenous (doranidazole) injection 30 min prior to irradiating (Modified from [24]). The dashed lines represent the SER levels when tumors were irradiated in the middle of a 60-min heating period at the indicated temperatures and are taken from Figure 1B.
Figure 2.
The radio-sensitizing effect of nitro-aromatic drugs and hyperthermia in a C3H mammary carcinoma. The sensitizer enhancement ratios (SERs) were calculated from full radiation dose-response curves of tumor control and represent the ratio of the radiation dose for radiation alone to that for radiation + sensitizer to produce a response in 50% of animals. The drug treatments were misonidazole (○), nimorazole (□), and doranidazole (△), with different drug doses administered as a single intraperitoneal (misonidazole and nimorazole) or intravenous (doranidazole) injection 30 min prior to irradiating (Modified from [24]). The dashed lines represent the SER levels when tumors were irradiated in the middle of a 60-min heating period at the indicated temperatures and are taken from Figure 1B.

Figure 3.
Effect of heating on perfusion in RIF-1 fibrosarcomas (A) or C3H mammary carcinomas (B). Tumors were heated for 1 h (shown by the black bars) at the indicated temperatures and blood perfusion in the tumors measured at different times before, during, or after heating by intravenously injecting radioactive rubidium chloride; tumors were excised 90–120 min later and tracer uptake measured on a gamma counter. Points are means (±1 S.E.) with the pre-treatment control values shown by the open symbols (Modified from [38,88]).
Figure 3.
Effect of heating on perfusion in RIF-1 fibrosarcomas (A) or C3H mammary carcinomas (B). Tumors were heated for 1 h (shown by the black bars) at the indicated temperatures and blood perfusion in the tumors measured at different times before, during, or after heating by intravenously injecting radioactive rubidium chloride; tumors were excised 90–120 min later and tracer uptake measured on a gamma counter. Points are means (±1 S.E.) with the pre-treatment control values shown by the open symbols (Modified from [38,88]).

Figure 4.
Meta-analysis of all trials in which patients were randomized to receive radiation alone (RAD) or radiation + hyperthermia (RAD + HEAT). The endpoint in each trial was complete response (CR) measured by loco-regional control and shows the calculated Odds ratio with 95% confidence intervals (95% CI). Data from [116,117,118,119,120,121,122,123,124,125,126,127,128,129] and observations from Overgaard, J. [130].
Figure 4.
Meta-analysis of all trials in which patients were randomized to receive radiation alone (RAD) or radiation + hyperthermia (RAD + HEAT). The endpoint in each trial was complete response (CR) measured by loco-regional control and shows the calculated Odds ratio with 95% confidence intervals (95% CI). Data from [116,117,118,119,120,121,122,123,124,125,126,127,128,129] and observations from Overgaard, J. [130].

Figure 5.
Hypoxia in tumors causes resistance to conventional treatments (i.e., radiotherapy of chemotherapy) and enhanced malignant progression (i.e., more aggressive growth of primary tumors or metastatic spread). Attempts to decrease hypoxia, and thereby improve tumor response to therapy as well as decrease the formation of metastases, have utilized a variety of different “traditional” approaches, as listed in Table 1. Hyperthermia can also decrease tumor hypoxia by a variety of mechanisms equivalent to all those seen with the more traditional methods.
Figure 5.
Hypoxia in tumors causes resistance to conventional treatments (i.e., radiotherapy of chemotherapy) and enhanced malignant progression (i.e., more aggressive growth of primary tumors or metastatic spread). Attempts to decrease hypoxia, and thereby improve tumor response to therapy as well as decrease the formation of metastases, have utilized a variety of different “traditional” approaches, as listed in Table 1. Hyperthermia can also decrease tumor hypoxia by a variety of mechanisms equivalent to all those seen with the more traditional methods.


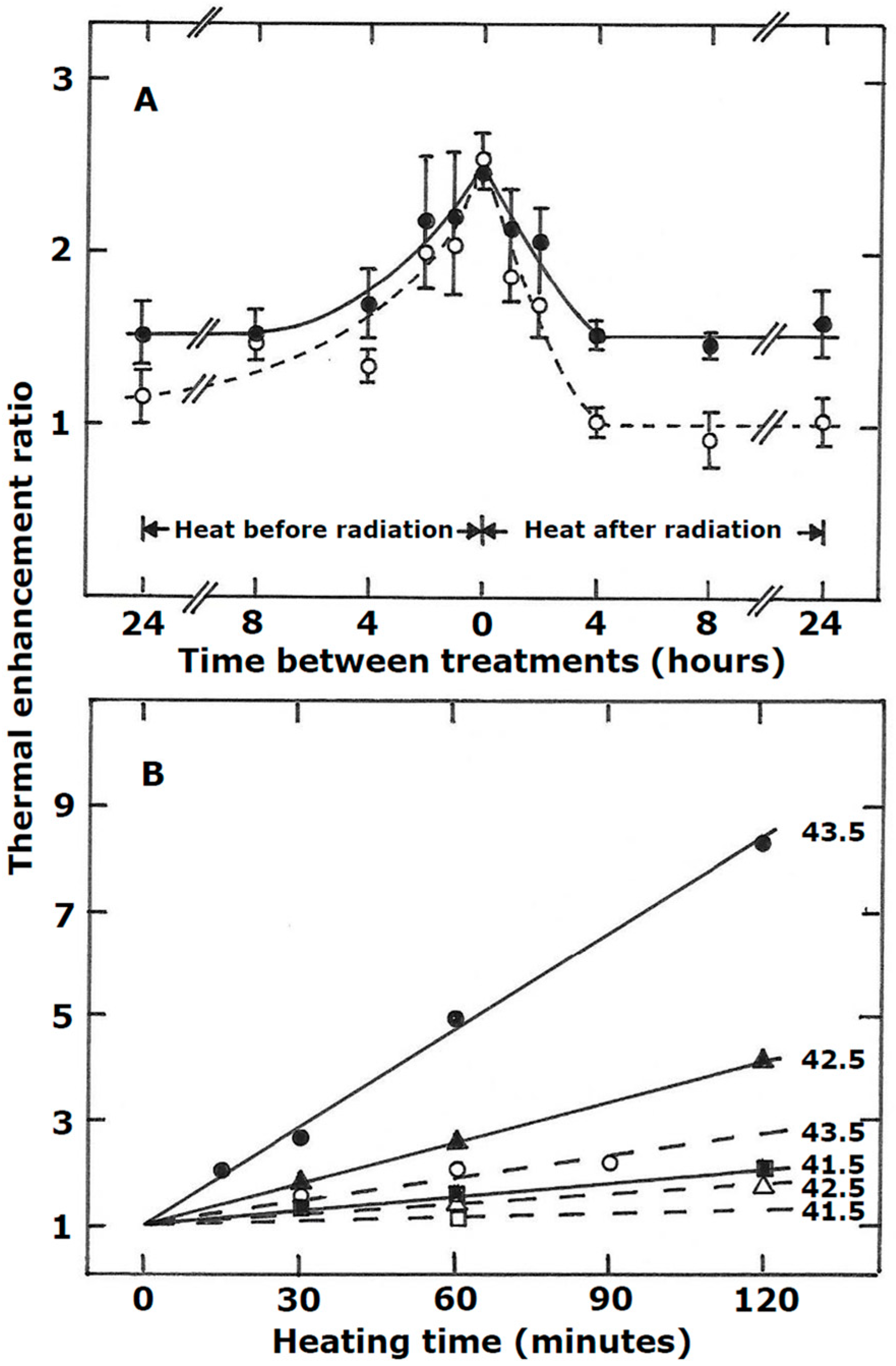{kind=link}
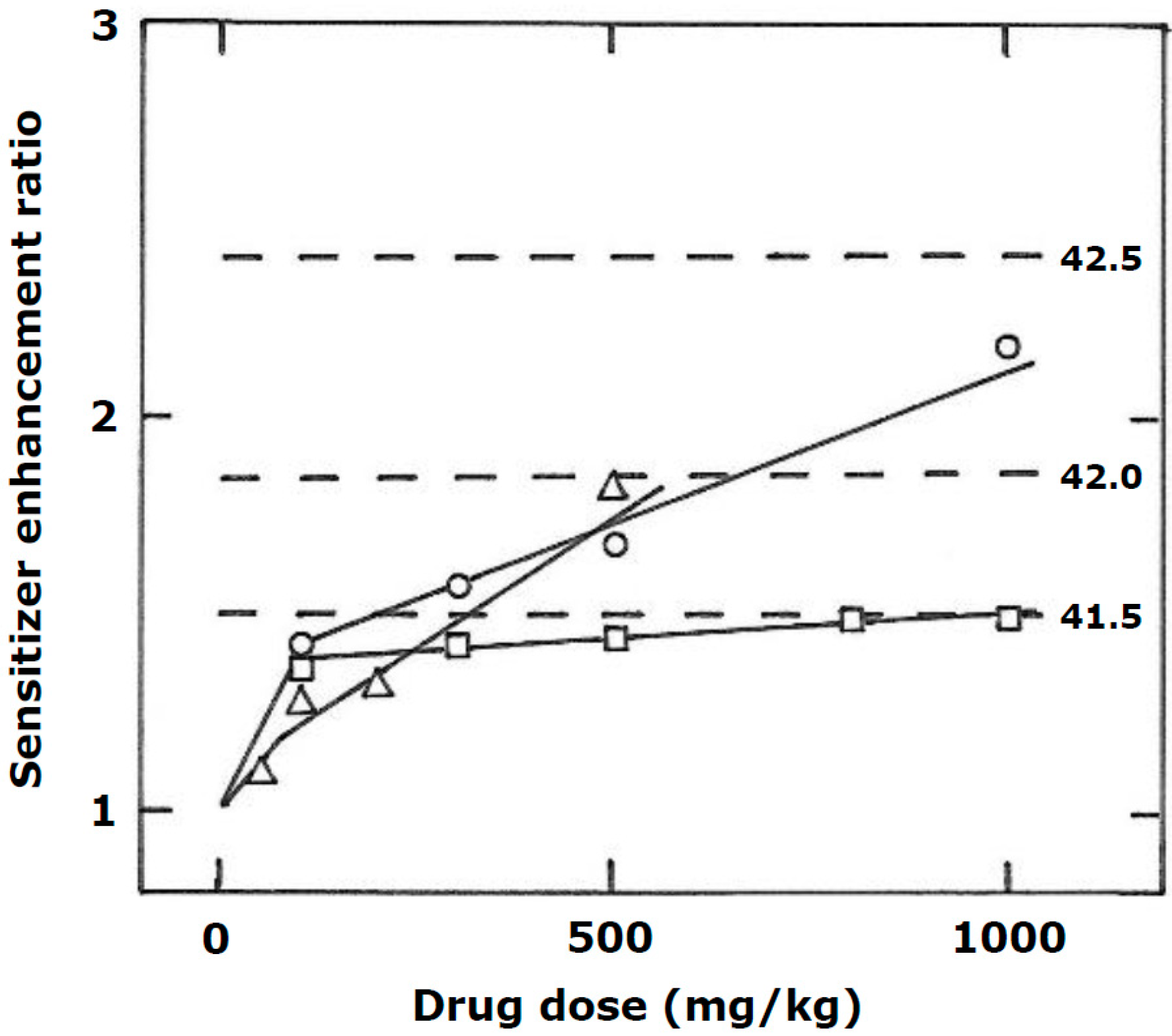{kind=link}
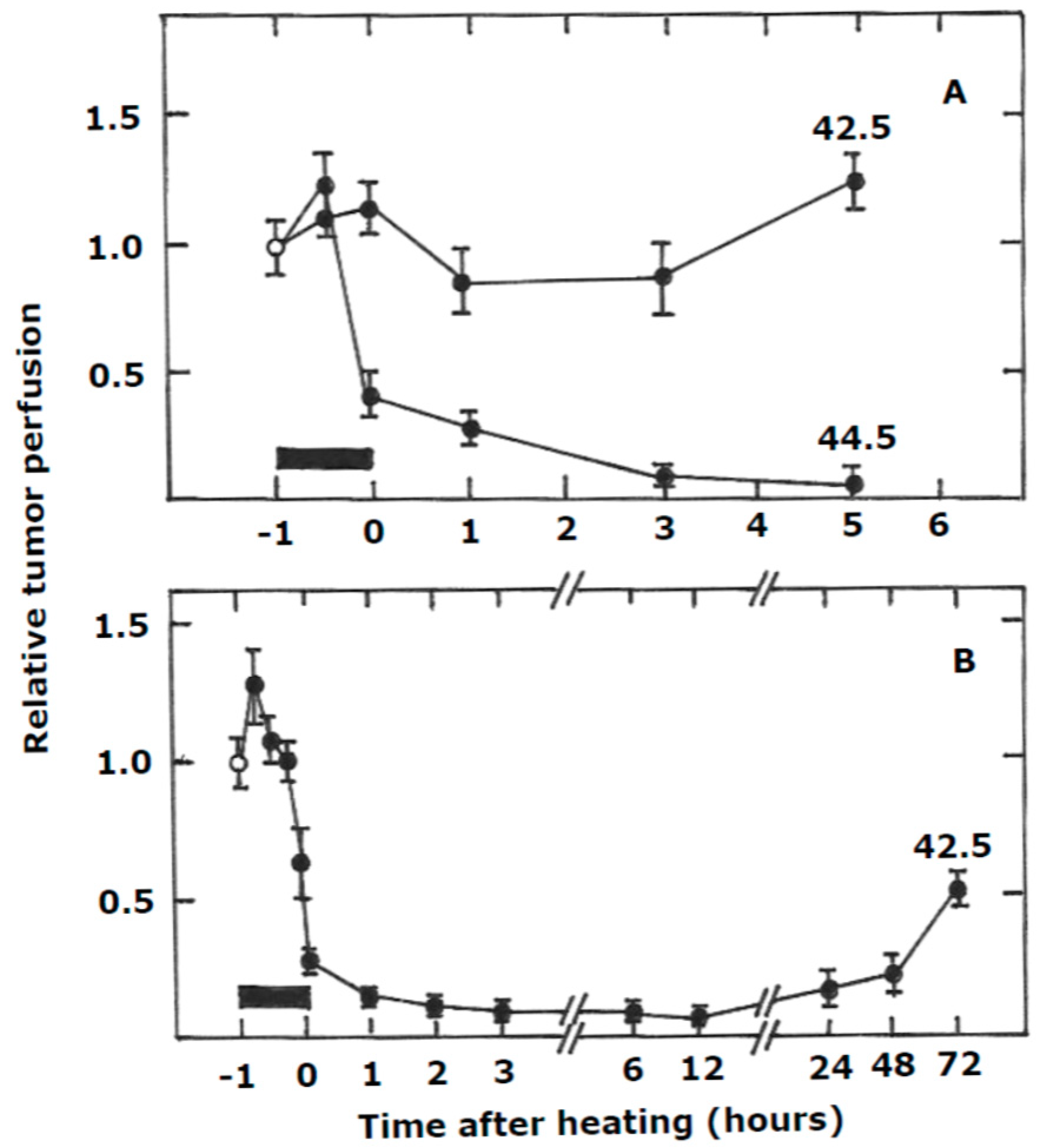{kind=link}
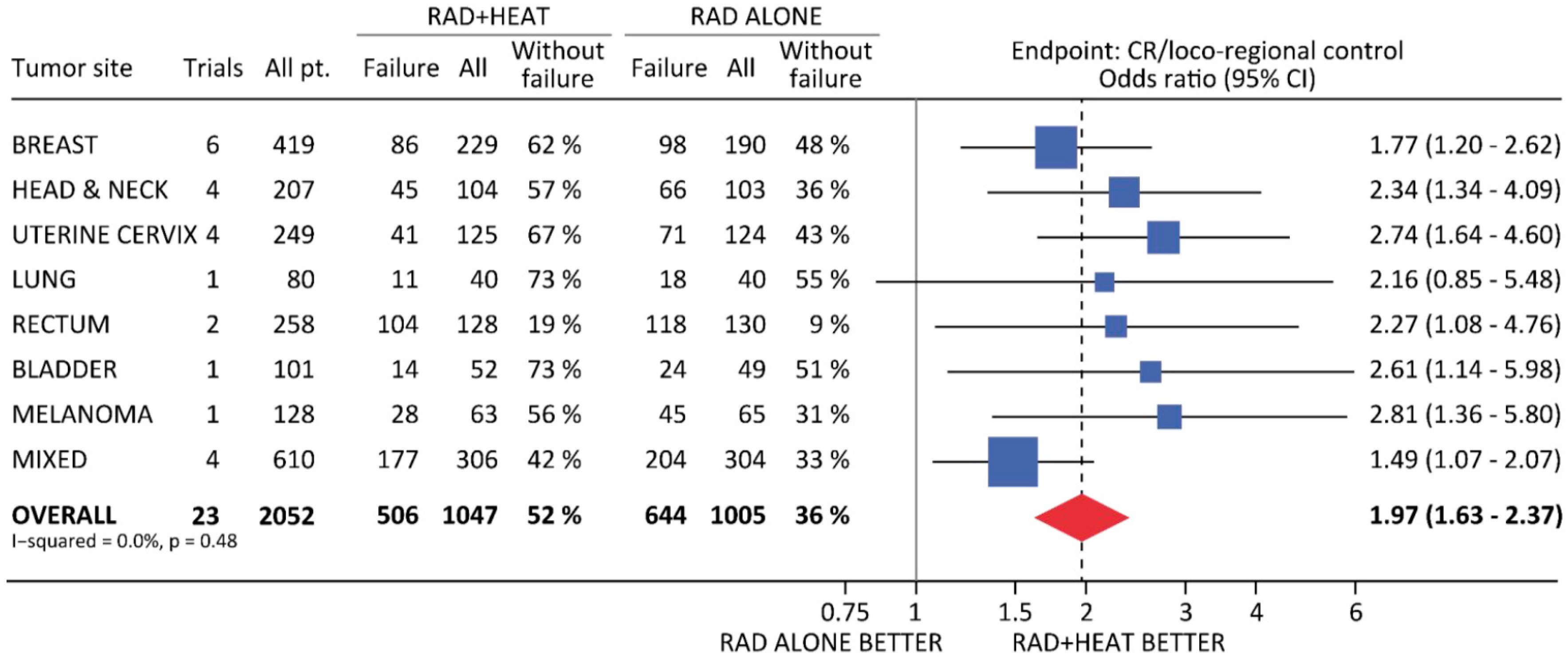{kind=link}
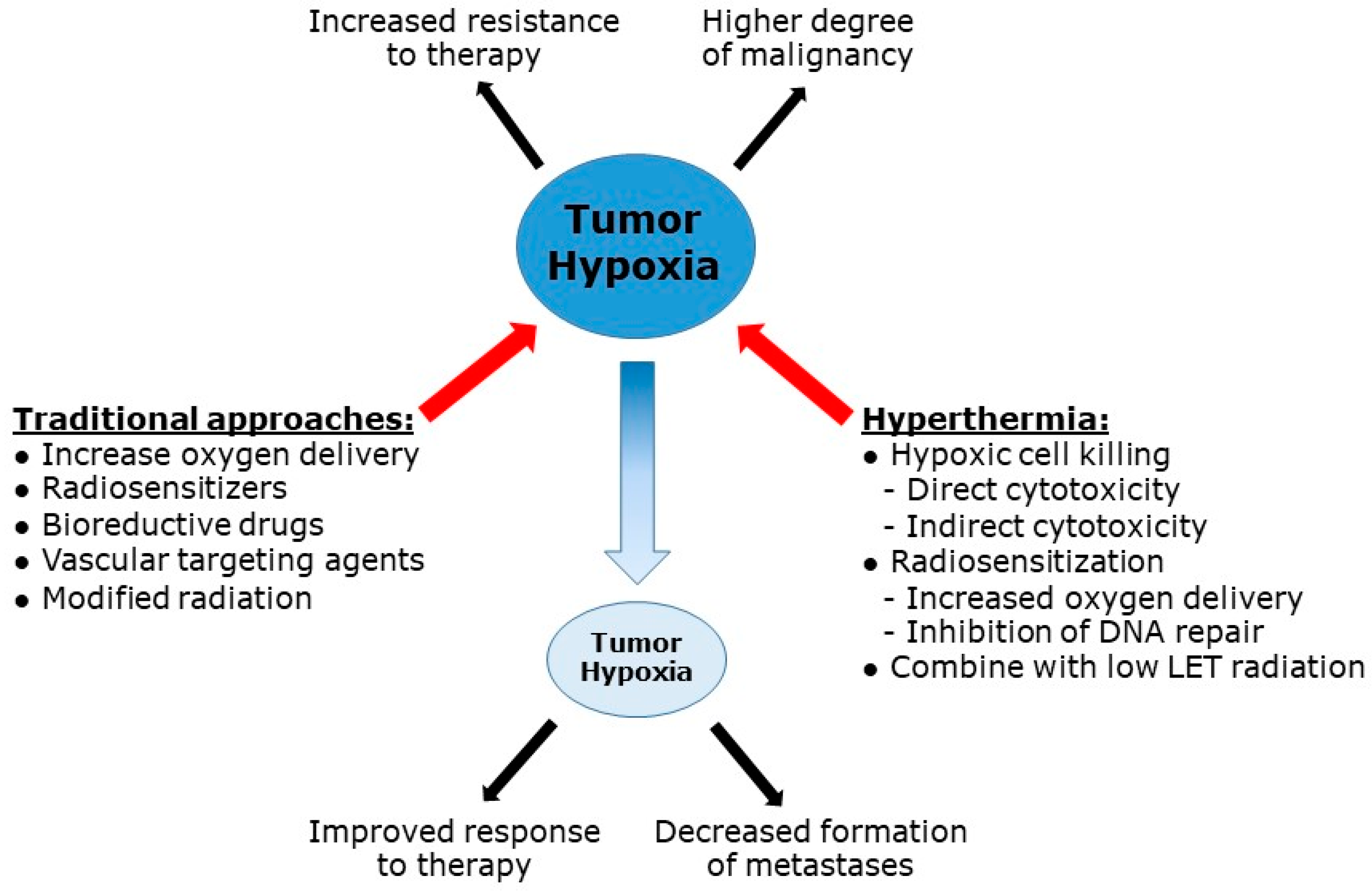{kind=link}
Table 1.
Approaches for dealing with hypoxia.
|
|
|
|
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Elming, P.B.; Sørensen, B.S.; Oei, A.L.; Franken, N.A.P.; Crezee, J.; Overgaard, J.; Horsman, M.R. Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia. Cancers 2019, 11, 60. https://doi.org/10.3390/cancers11010060
AMA Style
Elming PB, Sørensen BS, Oei AL, Franken NAP, Crezee J, Overgaard J, Horsman MR. Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia. Cancers. 2019; 11(1):60. https://doi.org/10.3390/cancers11010060
Chicago/Turabian StyleElming, Pernille B., Brita S. Sørensen, Arlene L. Oei, Nicolaas A.P. Franken, Johannes Crezee, Jens Overgaard, and Michael R. Horsman. 2019. "Hyperthermia: The Optimal Treatment to Overcome Radiation Resistant Hypoxia" Cancers 11, no. 1: 60. https://doi.org/10.3390/cancers11010060
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.