Prospective Evaluation of Neoadjuvant Imatinib Use in Locally Advanced Gastrointestinal Stromal Tumors: Emphasis on the Optimal Duration of Neoadjuvant Imatinib Use, Safety, and Oncological Outcome

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Preoperative Management
2.2. Response Assessment
2.3. Surgical Indication
2.4. Literature Review
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
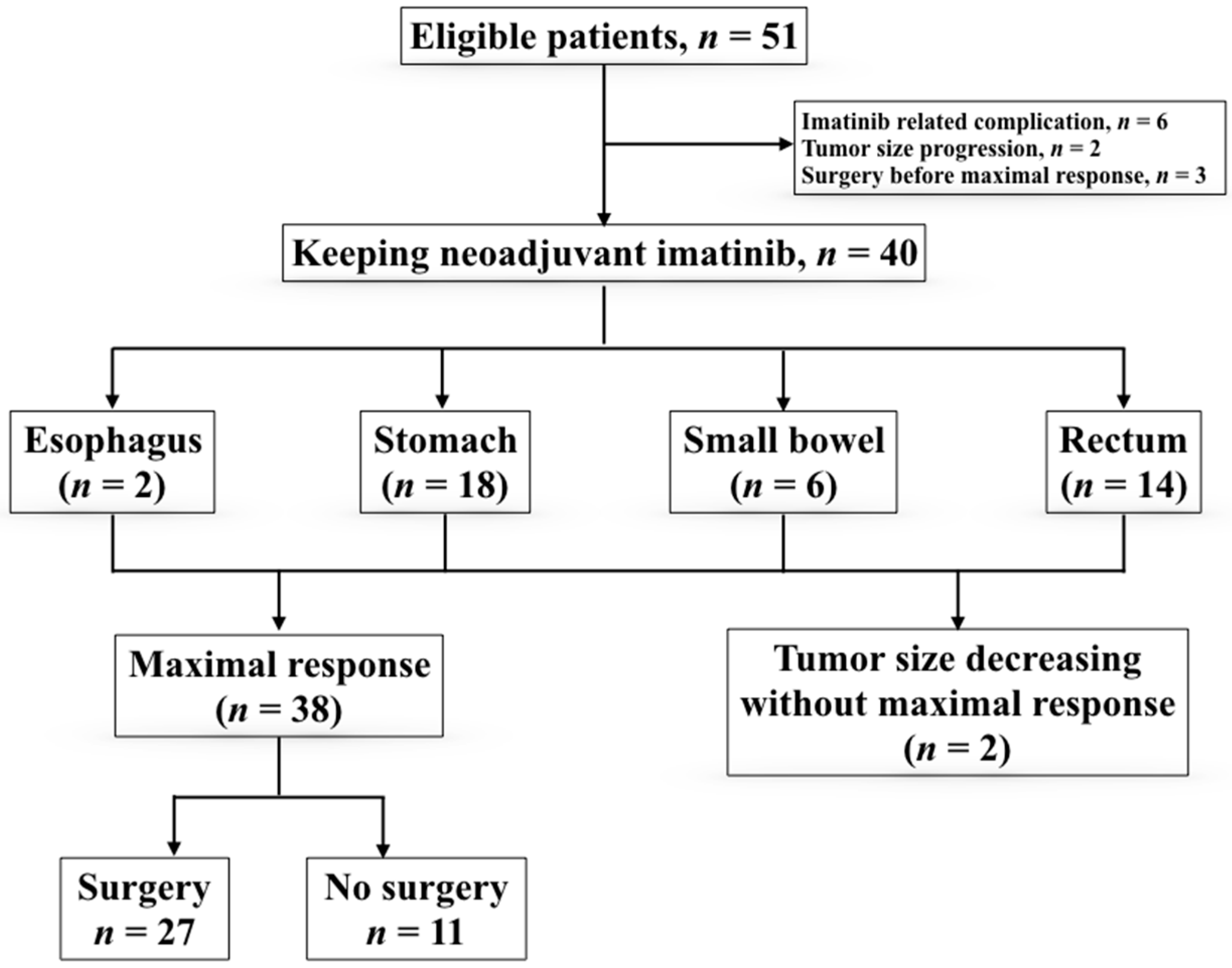
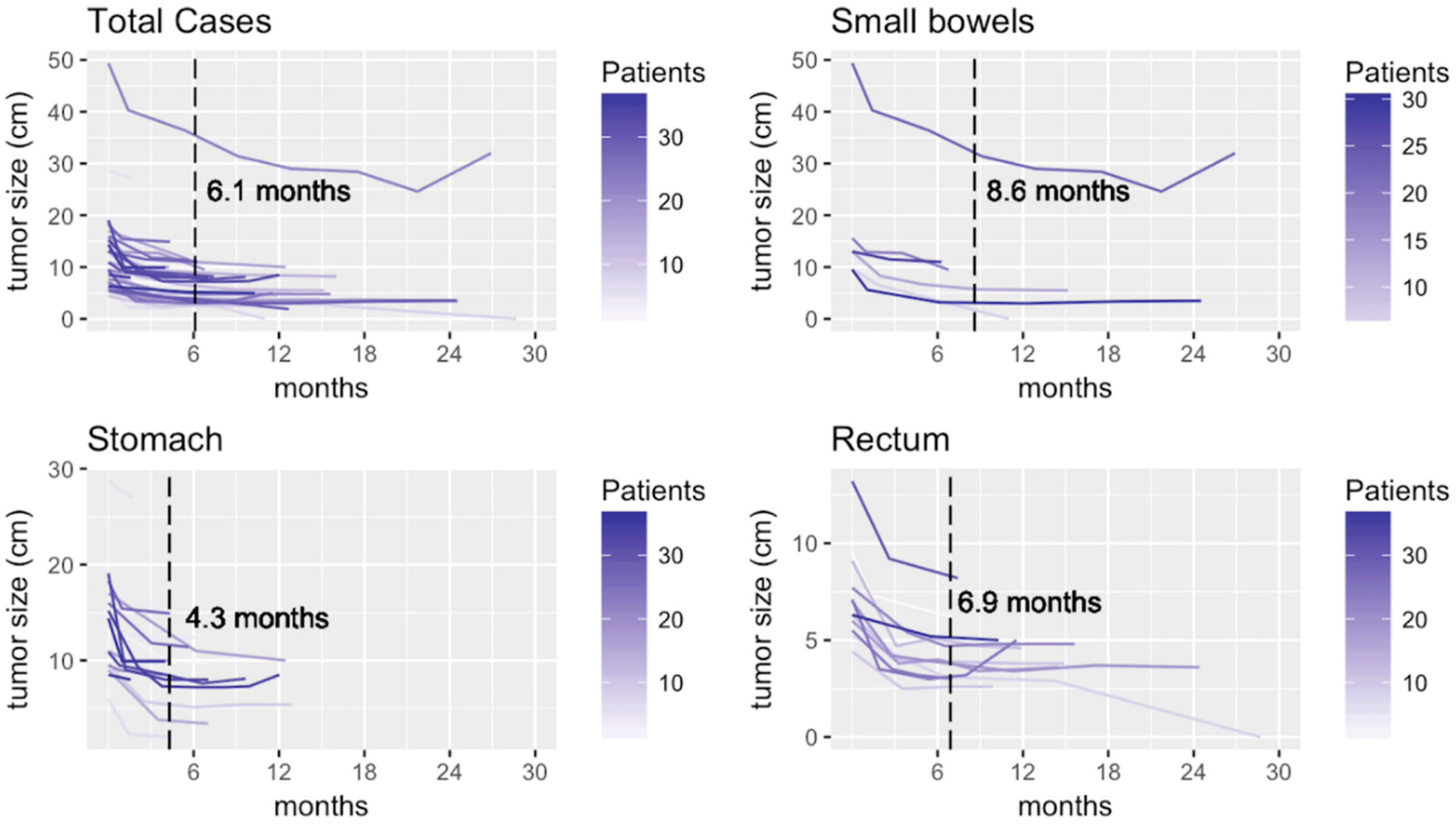
3.2. Clinical Response to Imatinib
3.3. Surgical Results
3.4. Literature Review
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Debiec-Rychter, M.; Wasag, B.; Stul, M.; De Wever, I.; Van Oosterom, A.; Hagemeijer, A.; Sciot, R. Gastrointestinal stromal tumours (GISTs) negative for KIT (CD117 antigen) immunoreactivity. J. Pathol. 2004, 202, 430–438. [Google Scholar] [CrossRef]
- Joensuu, H. [Tyrosine kinase inhibitor as a targeted therapy for GIST tumors]. Duodecim 2002, 118, 2305–2312. [Google Scholar] [PubMed]
- Heinrich, M.C.; Blanke, C.D.; Druker, B.J.; Corless, C.L. Inhibition of KIT Tyrosine Kinase Activity: A Novel Molecular Approach to the Treatment of KIT-Positive Malignancies. J. Clin. Oncol. 2002, 20, 1692–1703. [Google Scholar] [CrossRef] [PubMed]
- Von Mehren, M.; Benjamin, R.S.; Bui, M.M.; Casper, E.S.; Conrad, E.U.; DeLaney, T.F.; Ganjoo, K.N.; George, S.; Gonzalez, R.; Heslin, M.J.; et al. Soft tissue sarcoma, version 2.2012: Featured updates to the NCCN guidelines. J. Natl. Compr. Cancer Netw. 2012, 10, 951–960. [Google Scholar] [CrossRef]
- DeMatteo, R.P.; Lewis, J.J.; Leung, D.; Mudan, S.S.; Woodruff, J.M.; Brennan, M.F. Two hundred gastrointestinal stromal tumors: Recurrence patterns and prognostic factors for survival. Ann. Surg. 2000, 231, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, B.L.; Judson, I. Surgery and imatinib in the management of GIST: Emerging approaches to adjuvant and neoadjuvant therapy. Ann. Surg. Oncol. 2004, 11, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.H.; Pollock, R.E.; Munsell, M.F.; Atkinson, E.N.; Romsdahl, M.M. Prognostic factors influencing survival in gastrointestinal leiomyosarcomas. Implications for surgical management and staging. Ann. Surg. 1992, 215, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; von Mehren, M.; Antonescu, C.R.; DeMatteo, R.P.; Ganjoo, K.N.; Maki, R.G.; Pisters, P.W.T.; Raut, C.P.; Riedel, R.F.; Schuetze, S.; et al. NCCN Task Force report: Update on the management of patients with gastrointestinal stromal tumors. J. Natl. Compr. Cancer Netw. 2010, 8 (Suppl. 2), S1–S41; quiz S42–S44. [Google Scholar] [CrossRef]
- Eisenberg, B.L.; Harris, J.; Blanke, C.D.; Demetri, G.D.; Heinrich, M.C.; Watson, J.C.; Hoffman, J.P.; Okuno, S.; Kane, J.M.; von Mehren, M. Phase II trial of neoadjuvant/adjuvant imatinib mesylate (IM) for advanced primary and metastatic/recurrent operable gastrointestinal stromal tumor (GIST): Early results of RTOG 0132/ACRIN 6665. J. Surg. Oncol. 2009, 99, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Hohenberger, P.; Langer, C.; Wendtner, C.M.; Hohenberger, W.; Pustowka, A.; Wardelmann, E.; Andre, E.; Licht, T. Neoadjuvant treatment of locally advanced GIST: Results of APOLLON, a prospective, open label phase II study in KIT- or PDGFRA-positive tumors. J. Clin. Oncol. 2012, 30, 10031. [Google Scholar]
- McAuliffe, J.C.; Hunt, K.K.; Lazar, A.J.F.; Choi, H.; Qiao, W.; Thall, P.; Pollock, R.E.; Benjamin, R.S.; Trent, J.C. A Randomized, Phase II Study of Preoperative plus Postoperative Imatinib in GIST: Evidence of Rapid Radiographic Response and Temporal Induction of Tumor Cell Apoptosis. Ann. Surg. Oncol. 2008, 16, 910–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, C.; Ronellenfitsch, U.; Yuxin, Z.; Rutkowski, P.; Miceli, R.; Bylina, E.; Hohenberger, P.; Raut, C.P.; Gronchi, A. Clinical, Pathological and Surgical Characteristics of Duodenal Gastrointestinal Stromal Tumor and Their Influence on Survival: A Multi-Center Study. Ann. Surg. Oncol. 2012, 19, 3361–3367. [Google Scholar] [CrossRef] [PubMed]
- Johnston, F.M.; Kneuertz, P.J.; Cameron, J.L.; Sanford, D.; Fisher, S.; Turley, R.; Groeschl, R.; Hyder, O.; Kooby, D.A.; Blazer, D.; et al. Presentation and Management of Gastrointestinal Stromal Tumors of the Duodenum: A Multi-Institutional Analysis. Ann. Surg. Oncol. 2012, 19, 3351–3360. [Google Scholar] [CrossRef] [PubMed]
- Bonvalot, S.; Eldweny, H.; Pechoux, C.L.; Vanel, D.; Terrier, P.; Cavalcanti, A.; Robert, C.; Lassau, N.; Cesne, A.L. Impact of Surgery on Advanced Gastrointestinal Stromal Tumors (GIST) in the Imatinib Era. Ann. Surg. Oncol. 2006, 13, 1596–1603. [Google Scholar] [CrossRef] [PubMed]
- Le Cesne, A.; Van Glabbeke, M.; Verweij, J.; Casali, P.G.; Findlay, M.; Reichardt, P.; Issels, R.; Judson, I.; Schoffski, P.; Leyvraz, S.; et al. Absence of Progression as Assessed by Response Evaluation Criteria in Solid Tumors Predicts Survival in Advanced GI Stromal Tumors Treated with Imatinib Mesylate: The Intergroup EORTC-ISG-AGITG Phase III Trial. J. Clin. Oncol. 2009, 27, 3969–3974. [Google Scholar] [CrossRef] [PubMed]
- Haller, F.; Detken, S.; Schulten, H.-J.; Happel, N.; Gunawan, B.; Kuhlgatz, J.; Fuzesi, L. Surgical Management After Neoadjuvant Imatinib Therapy in Gastrointestinal Stromal Tumours (GISTs) with Respect to Imatinib Resistance Caused by Secondary KIT Mutations. Ann. Surg. Oncol. 2006, 14, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Graser, A.; Becker, C.R.; Reiser, M.F.; Stief, C.; Staehler, M. Volumetry of metastases from renal cell carcinoma. Radiologe 2008, 48, 850–856. [Google Scholar] [CrossRef]
- Schramm, N.; Englhart, E.; Schlemmer, M.; Hittinger, M.; Ubleis, C.; Becker, C.R.; Reiser, M.F.; Berger, F. Tumor response and clinical outcome in metastatic gastrointestinal stromal tumors under sunitinib therapy: Comparison of RECIST, Choi and volumetric criteria. Eur. J. Radiol. 2013, 82, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Blesius, A.; Cassier, P.A.; Bertucci, F.; Fayette, J.; Ray-Coquard, I.; Bui, B.; Adenis, A.; Rios, M.; Cupissol, D.; Perol, D.; et al. Neoadjuvant imatinib in patients with locally advanced non metastatic GIST in the prospective BFR14 trial. BMC Cancer 2011, 11, 472. [Google Scholar] [CrossRef] [PubMed]
- Shrikhande, S.V.; Marda, S.S.; Suradkar, K.; Arya, S.; Shetty, G.S.; Bal, M.; Shukla, P.J.; Goel, M.; Mohandas, K.M. Gastrointestinal Stromal Tumors: Case Series of 29 Patients Defining the Role of Imatinib Prior to Surgery. World J. Surg. 2012, 36, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zhang, Q.; Blanke, C.D.; Demetri, G.D.; Heinrich, M.C.; Watson, J.C.; Hoffman, J.P.; Okuno, S.; Kane, J.M.; von Mehren, M.; et al. Phase II Trial of Neoadjuvant/adjuvant Imatinib Mesylate for Advanced Primary and Metastatic/recurrent Operable Gastrointestinal Stromal Tumors: Long-term Follow-up Results of Radiation Therapy Oncology Group 0132. Ann. Surg. Oncol. 2011, 19, 1074–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tielen, R.; Verhoef, C.; Van Coevorden, F.; Gelderblom, H.; Sleijfer, S.; Hartgrink, H.H.; Bonenkamp, J.J.; van der Graaf, W.T.A.; de Wilt, J.H.W. Surgical treatment of locally advanced, non-metastatic, gastrointestinal stromal tumours after treatment with imatinib. Eur. J. Surg. Oncol. 2013, 39, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutkowski, P.; Gronchi, A.; Hohenberger, P.; Bonvalot, S.; Schoffski, P.; Bauer, S.; Fumagalli, E.; Nyckowski, P.; Nguyen, B.-P.; Kerst, J.M.; et al. Neoadjuvant Imatinib in Locally Advanced Gastrointestinal Stromal Tumors (GIST): The EORTC STBSG Experience. Ann. Surg. Oncol. 2013, 20, 2937–2943. [Google Scholar] [CrossRef]
- Raut, C.P.; Posner, M.; Desai, J.; Morgan, J.A.; George, S.; Zahrieh, D.; Fletcher, C.D.M.; Demetri, G.D.; Bertagnolli, M.M. Surgical Management of Advanced Gastrointestinal Stromal Tumors After Treatment with Targeted Systemic Therapy Using Kinase Inhibitors. J. Clin. Oncol. 2006, 24, 2325–2331. [Google Scholar] [CrossRef]
- Miettinen, M.; Lasota, J. Gastrointestinal stromal tumors: Pathology and prognosis at different sites. Semin. Diagn. Pathol. 2006, 23, 70–83. [Google Scholar] [CrossRef] [PubMed]
- von Mehren, M.; Randall, R.L.; Benjamin, R.S.; Boles, S.; Bui, M.M.; Conrad, E.U.; Ganjoo, K.N.; George, S.; Gonzalez, R.J.; Heslin, M.J.; et al. Soft Tissue Sarcoma, Version 2.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 758–786. [Google Scholar] [CrossRef] [Green Version]
- Casali, P.G.; Abecassis, N.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; Broto, J.M.; et al. ESMO Guidelines Committee and EURACAN Gastrointestinal stromal tumours: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv68–iv78. [Google Scholar] [CrossRef] [PubMed]
- Andtbacka, R.H.I.; Ng, C.S.; Scaife, C.L.; Cormier, J.N.; Hunt, K.K.; Pisters, P.W.T.; Pollock, R.E.; Benjamin, R.S.; Burgess, M.A.; Chen, L.L.; et al. Surgical Resection of Gastrointestinal Stromal Tumors after Treatment with Imatinib. Ann. Surg. Oncol. 2006, 14, 14–24. [Google Scholar] [CrossRef]
- Raut, C.P.; Wang, Q.; Manola, J.; Morgan, J.A.; George, S.; Wagner, A.J.; Butrynski, J.E.; Fletcher, C.D.M.; Demetri, G.D.; Bertagnolli, M.M. Cytoreductive Surgery in Patients with Metastatic Gastrointestinal Stromal Tumor Treated with Sunitinib Malate. Ann. Surg. Oncol. 2009, 17, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.N.; Chen, T.W.; Tseng, J.H.; Liu, Y.Y.; Wang, S.Y.; Tsai, C.Y.; Chiang, K.C.; Hwang, T.L.; Jan, Y.Y.; Chen, M.F. Surgical management in metastatic gastrointestinal stromal tumor (GIST) patients after imatinib mesylate treatment. J. Surg. Oncol. 2010, 102, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.N.; Wang, S.Y.; Tsai, C.Y.; Chen, Y.Y.; Liu, C.T.; Chiang, K.C.; Chen, T.W.; Liu, Y.Y.; Yeh, T.S. Surgical management of patients with progressing metastatic gastrointestinal stromal tumors receiving sunitinib treatment: A prospective cohort study. Int. J. Surg. 2017, 39, 30–36. [Google Scholar] [CrossRef]
- Fairweather, M.; Cavnar, M.J.; Li, G.Z.; Bertagnolli, M.M.; DeMatteo, R.P.; Raut, C.P. Prediction of morbidity following cytoreductive surgery for metastatic gastrointestinal stromal tumour in patients on tyrosine kinase inhibitor therapy. Br. J. Surg. 2018, 105, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Chen, C.H.; Chen, T.C.; Yeh, C.N.; Yeh, T.S. Preoperative tyrosine kinase inhibitors risks bowel anastomotic healing in patients with advanced primary and recurrent/metastatic gastrointestinal stromal tumors—A rose has its thorns. Eur. J. Surg. Oncol. 2019, 45, 153–159. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Patients (n = 51) | Esophagus (n = 2) | Stomach (n = 23) | Small Bowel (n = 9) | Colon/Rectum (n = 17) |
|---|---|---|---|---|---|
| Age, years (SD) | 59.9 (13.1) | 73.6 (9.1) | 58.3 (12.7) | 63.7 (20.2) | 58.3 (8.6) |
| Sex (M/F) | 29/22 | 2/0 | 13/10 | 4/5 | 10/7 |
| Tumor size, cm (SD) | 12.5 (7.6) | 9.3 (5.3) | 14.7 (5.9) | 17.5 (12.5) | 7.46 (2.33) |
| WBC, /μL (SD) | 6142.1 (2531.4) | 8000.0 (141.4) | 5873.6 (2629.5) | 9220.0 (2631.9) | 5407.1 (1484.5) |
| Platelets, /μL (SD) | 214.4K (83.1K) | 209.5K (91.2) | 207.7K (74.9K) | 283.6K (145.8K) | 198.7K (56.6K) |
| Bilirubin, mg/dL (SD) | 0.58 (0.32) | 0.70 (0.42) | 0.62 (0.39) | 0.45 (0.06) | 0.56 (0.26) |
| AST, U/L (SD) | 26.2 (17.0) | 34.0 (32.5) | 29.3 (21.2) | 21.5 (17.0) | 22.5 (5.9) |
| Cr, mg/dL (SD) | 0.92 (0.45) | 0.70 (0.42) | 0.88 (0.50) | 0.97 (0.50) | 0.86 (0.23) |
| AJCC Stage | |||||
| Stage I | 6 | 0 | 5 | 0 | 1 |
| Stage II | 22 | 0 | 11 | 1 | 10 |
| Stage IIIa | 6 | 0 | 1 | 4 | 1 |
| Stage IIIb | 7 | 0 | 3 | 1 | 3 |
| Undefined * | 10 | 2 | 3 | 3 | 2 |
| Clinical presentations | |||||
| Pain | 7 | 0 | 5 | 4 | 1 |
| Mass | 3 | 0 | 3 | 1 | 1 |
| GI bleeding | 11 | 0 | 6 | 1 | 5 |
| Sign of obstruction | 13 | 2 | 2 | 3 | 7 |
| Incidental finding | 5 | 0 | 4 | 0 | 2 |
| Others | 3 | 0 | 2 | 0 | 1 |
| Age/Sex | Time After Imatinib Use (Months) | Tumor Size (Median, cm) | Location | Complications after Imatinib Administration/Postoperative Condition | Resection | Mutation |
|---|---|---|---|---|---|---|
| 67M | 1.8 | 19 | Stomach | Tumor rupture, intra-abdominal hemorrhage, imatinib stopped after mutation analysis complete/expired within 1 month post-operation | R2 | PDGFRA, Exon 18 (D842V) |
| 63M | 0.4 | 18 | Stomach | Intra-abdominal hemorrhage, compartment syndrome/expired after 23 months post-operation | R2 | KIT, Exon 11 |
| 62M | 11.5 | 17.2 | Ileum | Enlarged mass with intratumor hemorrhage No recurrence after 28 months post-operation | R0 | KIT, Exon 11 |
| 64F | 0.4 | 10 | Jejunum | Necrosis of tumors, suspicion of abscess formation/no recurrence after 30 months post-operation | R0 | KIT, Exon 11 |
| 32M | 1.8 | 20 | Jejunum | Tumor rupture, intra-abdominal hemorrhage/expired after 2.1 months post-operation | R2 | KIT, Exon 11 |
| 83F | 2.3 | 10.7 | Stomach | Interstitial lung disease | No Surgery | KIT, Exon 11 |
| Characteristic | Esophagus | Stomach | Jejunum/Ileum | Rectum | Total (%) | |
|---|---|---|---|---|---|---|
| Patients with OP | 0 | 15 | 2 | 10 | 27 (67.5) | |
| Patients without OP | 2 | 3 | 4 | 4 | 13 (32.5) | |
| Time from imatinib use to op (median, months) | 8 | |||||
| Resection | R0 | 0 | 14 | 1 | 7 | 22 (81.5) |
| R1 | 0 | 1 | 0 | 3 | 4 (14.8) | |
| R2 | 0 | 0 | 1 | 0 | 1 (3.7) | |
| Organ preservation | Achieved | 0 | 12 | 0 | 7 | 19 (70.4) |
| Failed | 0 | 3 a | 2 b | 3 c | 8 (29.6) | |
| Adjuvant imatinib | Yes | 24 (88.9) | ||||
| No | 3 (11.1) | |||||
| Recurrence | 0 | 0 | 0 | 3 | 3 (11.1) | |
| Reference | Study Type | Patient Number | Conclusions/Statements |
|---|---|---|---|
| Blesius et al. 2011 [20] | Retrospective, part of the BRF14 trial | n = 25 | Only 9 patients were scheduled for later surgery. Values of overall survival and progression-free survival were close to those for localized intermediate- or high-risk GISTs (70% at 5 years). |
| Shrikhande et al. 2012 [21] | Retrospective | n = 29 | Neoadjuvant imatinib therapy for locally advanced GISTs is a safe concept for downsizing, improving resectability, and aiding organ-preserving surgery. It also improves the chance of long-term survival. |
| Wang et al. 2012 [22] | Prospective | n = 53, 31 with primary GISTs and 22 with resectable metastatic/recurrent GISTs | The long-term analysis of the patients enrolled into the RTOG 0132/ACRIN 6665 showed no significant increase in treatment complications after preoperative imatinib use in patients with resectable locally advanced GISTs. A high percentage of patients experienced disease progression after discontinuation of 2-year maintenance imatinib therapy after surgery. Further studies should focus on longer treatment with imatinib. |
| Hohenberger et al. 2012 [10] | Prospective | n = 41 | Neoadjuvant treatment with imatinib for 6 months is safe for patients with locally advanced disease. The extent of surgery can be significantly decreased after pretreatment. Even though no adjuvant treatment was foreseen, the postoperative progression-free rate at 3 years is promising. |
| Tielen et al. 2013 [23] | Retrospective | n = 57 | Imatinib in locally advanced GISTs is feasible and enables a high complete-resection rate without tumor rupture. The combination of imatinib and surgery in patients with locally advanced GISTs seems to improve overall survival and progression-free survival. |
| Rutkowski et al. 2013 [24] | Retrospective | n = 161 | Patients with locally advanced GISTs treated with neoadjuvant imatinib in routine practice show excellent long-term results of combined therapy. Postoperative imatinib therapy should be used routinely in patients considered for neoadjuvant therapy because it is highly unlikely that such tumors are very-low-risk/low-risk GISTs. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.-Y.; Wu, C.-E.; Lai, C.-C.; Chen, J.-S.; Tsai, C.-Y.; Cheng, C.-T.; Yeh, T.-S.; Yeh, C.-N. Prospective Evaluation of Neoadjuvant Imatinib Use in Locally Advanced Gastrointestinal Stromal Tumors: Emphasis on the Optimal Duration of Neoadjuvant Imatinib Use, Safety, and Oncological Outcome. Cancers 2019, 11, 424. https://doi.org/10.3390/cancers11030424
Wang S-Y, Wu C-E, Lai C-C, Chen J-S, Tsai C-Y, Cheng C-T, Yeh T-S, Yeh C-N. Prospective Evaluation of Neoadjuvant Imatinib Use in Locally Advanced Gastrointestinal Stromal Tumors: Emphasis on the Optimal Duration of Neoadjuvant Imatinib Use, Safety, and Oncological Outcome. Cancers. 2019; 11(3):424. https://doi.org/10.3390/cancers11030424
Chicago/Turabian StyleWang, Shang-Yu, Chiao-En Wu, Chun-Chi Lai, Jen-Shi Chen, Chun-Yi Tsai, Chi-Tung Cheng, Ta-Sen Yeh, and Chun-Nan Yeh. 2019. "Prospective Evaluation of Neoadjuvant Imatinib Use in Locally Advanced Gastrointestinal Stromal Tumors: Emphasis on the Optimal Duration of Neoadjuvant Imatinib Use, Safety, and Oncological Outcome" Cancers 11, no. 3: 424. https://doi.org/10.3390/cancers11030424