Favorable Outcome in Patients with Pheochromocytoma and Paraganglioma Treated with 177Lu-DOTATATE

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Patient Characteristics
2.2. Treatment and Toxicity
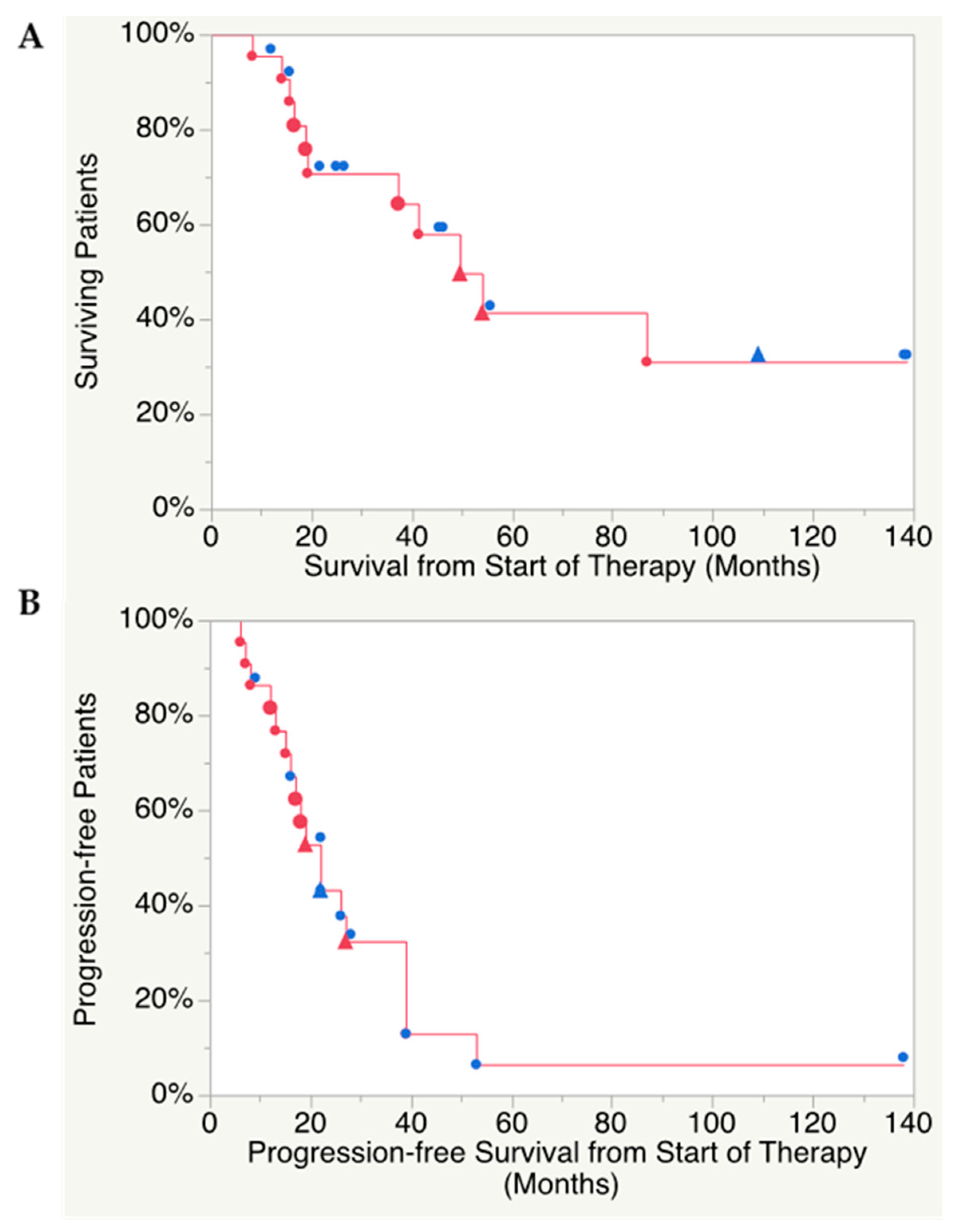
2.3. Therapy Outcome and Response Assessment
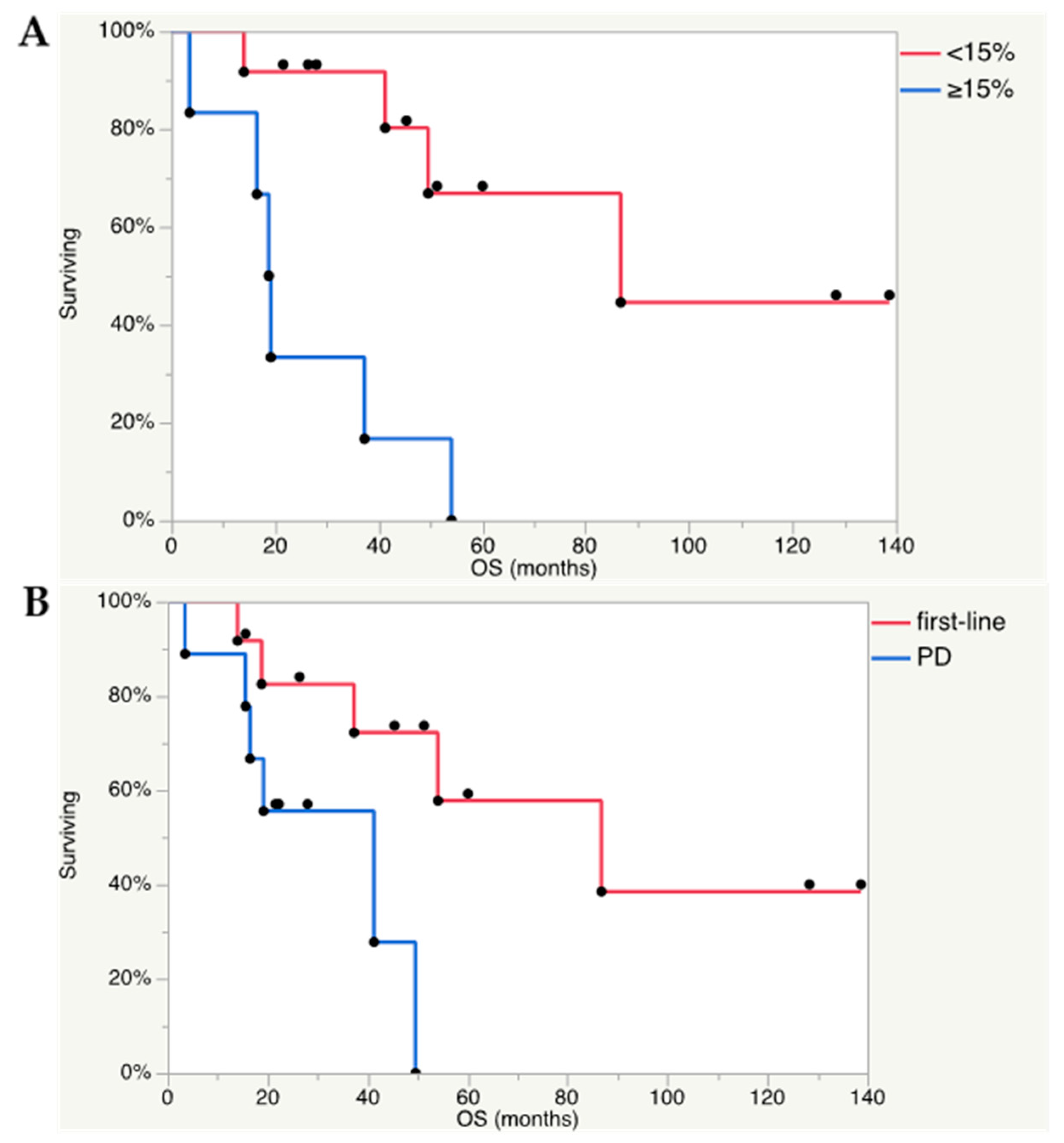
2.4. Predictors of Outcome
3. Discussion
4. Materials and Methods
4.1. PRRT Treatment Protocol
4.2. Evaluations
4.3. Response Assessment
4.4. Toxicity
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lenders, J.W.; Eisenhofer, G.; Mannelli, M.; Pacak, K. Phaeochromocytoma. Lancet 2005, 366, 665–675. [Google Scholar] [CrossRef]
- Fishbein, L.; Leshchiner, I.; Walter, V.; Danilova, L.; Robertson, A.G.; Johnson, A.R.; Lichtenberg, T.M.; Murray, B.A.; Ghayee, H.K.; Else, T.; et al. Cancer Genome Atlas Research Network, Pacak K, Nathanson KL, Wilkerson MD. Comprehensive Molecular Characterization of Pheochromocytoma and Paraganglioma. Cancer Cell. 2017, 31, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Crona, J.; Lamarca, A.; Ghosal, S.; Welin, S.; Skogseid, B.; Pacak, K. Genotype-phenotype correlations in pheochromocytoma and paraganglioma. Endocr. Relat. Cancer 2019. [Google Scholar] [CrossRef]
- Hamidi, O.; Young, W.F., Jr.; Gruber, L.; Smestad, J.; Yan, Q.; Ponce, O.J.; Prokop, L.; Murad, M.H.; Bancos, I. Outcomes of patients with metastatic phaeochromocytoma and paraganglioma: A systematic review and meta-analysis. Clin. Endocrinol. 2017, 87, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Lenders, J.W.; Duh, Q.Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.P.; Grebe, S.K.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F., Jr. Endocrine Society. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef]
- Gonias, S.; Goldsby, R.; Matthay, K.K.; Hawkins, R.; Price, D.; Huberty, J.; Damon, L.; Linker, C.; Sznewajs, A.; Shiboski, S.; et al. Phase II study of high-dose [131I] metaiodobenzylguanidine therapy for patients with metastatic pheochromocytoma and paraganglioma. J. Clin. Oncol. 2009, 27, 4162–4168. [Google Scholar] [CrossRef]
- Huang, H.; Abraham, J.; Hung, E.; Averbuch, S.; Merino, M.; Steinberg, S.M.; Pacak, K.; Fojo, T. Treatment of malignant pheochromocytoma/paraganglioma with cyclophosphamide, vincristine, and dacarbazine: Recommendation from a 22-year follow-up of 18 patients. Cancer 2008, 113, 2020–2028. [Google Scholar] [CrossRef]
- Joshua, A.M.; Ezzat, S.; Asa, S.L.; Evans, A.; Broom, R.; Freeman, M.; Knox, J.J. Rationale and evidence for sunitinib in the treatment of malignant paraganglioma/pheochromocytoma. J. Clin. Endocrinol. Metab. 2009, 94, 5–9. [Google Scholar] [CrossRef]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Mäcke, H.R.; Rochlitz, C.; Müller-Brand, J.; Walter, M.A. Response, survival, and long-term toxicity after therapy with the radiolabelled somatostatin analogue [90Y-DOTA]-TOC in metastasised neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef]
- Kwekkeboom, D.J.; Bakker, W.H.; Kam, B.L.; Teunissen, J.J.; Kooij, P.P.; de Herder, W.W.; Feelders, R.A.; van Eijck, C.H.; de Jong, M.; Srinivasan, A.; et al. Treatment of patients with gastro-entero-pancreatic (GEP) tumours with the novel radiolabelled somatostatin analogue [(177)Lu-DOTA(0), Tyr(3)] octreotate. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 417–422. [Google Scholar] [CrossRef]
- Brabander, T.; van der Zwan, W.A.; Teunissen, J.J.M.; Kam, B.L.R.; Feelders, R.A.; de Herder, W.W.; van Eijck, C.H.J.; Franssen, G.J.H.; Krenning, E.P.; Kwekkeboom, D.J. Long-Term Efficacy, Survival, and Safety of [177Lu-DOTA0, Tyr3] octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors. Clin. Cancer Res. 2017, 23, 4617–4624. [Google Scholar] [CrossRef] [PubMed]
- Forrer, F.; Riedweg, I.; Maecke, H.R.; Mueller-Brand, J. Radiolabeled DOTATOC in patients with advanced paraganglioma and pheochromocytoma. Q. J. Nucl. Med. Mol. Imaging 2008, 52, 334–340. [Google Scholar] [PubMed]
- Van Essen, M.; Krenning, E.P.; Kooij, P.P.; Bakker, W.H.; Feelders, R.A.; de Herder, W.W.; Wolbers, J.G.; Kwekkeboom, D.J. Effects of therapy with [177Lu-DOTA0, Tyr3] octreotate in patients with paraganglioma, meningioma, small cell lung carcinoma, and melanoma. J. Nucl. Med. 2006, 47, 1599–1606. [Google Scholar]
- Kong, G.; Grozinsky-Glasberg, S.; Hofman, M.S.; Akhurst, T.; Meirovitz, A.; Maimon, O.; Krausz, Y.; Godefroy, J.; Michael, M.; Gross, D.J.; et al. Highly favourable outcomes with peptide receptor radionuclide therapy (PRRT) for metastatic rectal neuroendocrine neoplasia (NEN). Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.P.; Ballal, S.; Bal, C. Concomitant 177Lu-DOTATATE and capecitabine therapy in malignant paragangliomas. EJNMMI Res. 2019, 9, 13. [Google Scholar] [CrossRef]
- Demirci, E.; Kabasakal, L.; Toklu, T.; Ocak, M.; Şahin, O.E.; Alan-Selcuk, N.; Araman, A. 177Lu-DOTATATE therapy in patients with neuroendocrine tumours including high-grade (WHO G3) neuroendocrine tumours: Response to treatment and long-term survival update. Nucl. Med. Commun. 2018, 39, 789–796. [Google Scholar] [CrossRef]
- Sandström, M.; Garske, U.; Granberg, D.; Sundin, A.; Lundqvist, H. Individualized dosimetry in patients undergoing therapy with (177) Lu-DOTA-D-Phe (1)-Tyr (3)-octreotate. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 212–225. [Google Scholar] [CrossRef]
- Sandström, M.; Garske-Román, U.; Granberg, D.; Johansson, S.; Widström, C.; Eriksson, B.; Sundin, A.; Lundqvist, H.; Lubberink, M. Individualized dosimetry of kidney and bone marrow in patients undergoing 177Lu-DOTA-octreotate treatment. J. Nucl. Med. 2013, 54, 33–41. [Google Scholar] [CrossRef]
- Garske-Román, U.; Sandström, M.; Fröss Baron, K.; Lundin, L.; Hellman, P.; Welin, S.; Johansson, S.; Khan, T.; Lundqvist, H.; Eriksson, B.; et al. Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): Feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 970–988. [Google Scholar] [CrossRef]
- Taïeb, D.; Timmers, H.J.; Hindié, E.; Guillet, B.A.; Neumann, H.P.; Walz, M.K.; Opocher, G.; de Herder, W.W.; Boedeker, C.C.; de Krijger, R.R.; et al. European Association of Nuclear Medicine. EANM 2012 guidelines for radionuclide imaging ofmphaeochromocytoma and paraganglioma. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1977–1995. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pat. No. | Age at PRRT Start | Sex | Tumor Type | Primary Tumor Localization | Ki-67 Index | Genotype | Indication for PRRT | Metastases | Previous Therapy | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgery | RT | 131I-MIBG | ChT | |||||||||
| 1 | 61 | F | PGL | Retroperitoneum | 5% | SDHB | Sympt | Retroper lgll, Liver, Bone | + | + | - | - |
| 2 | 33 | F | PGL | Urinary bladder | 10% | SDHD | NA | Mediast lgll, Neck, Heart | + | - | - | - |
| 3 | 24 | M | PGL | Retroperitoneum | <2% | Sporadic | Sympt | Retroper lgll, Bone | + | + | + | - |
| 4 | 67 | M | PGL | Aortic bifurcation | 15% | SDHB | PD | Bone | - | + | + | - |
| 5 | 53 | F | PCC | 2% | Sporadic | Sympt | Liver | + | - | - | - | |
| 6 | 25 | M | PGL | Retroperitoneum | NA, 4/10HPF | NA | PD | Bone | + | + | - | + |
| 7 | 56 | M | PCC | 12% | NA | PD | Retroper lgll, Bone | + | + | - | - | |
| 8 | 71 | F | PGL | Liver | 25% | Sporadic | NA | Bone | + | - | - | - |
| 9 | 70 | F | PGL | Kidney | 20% | NA | PD | Bone | + | + | + | - |
| 10 | 25 | M | PGL | Retroperitoneum | 25% | SDHB | NA | Liver, Bone, Lung | - | - | - | - |
| 11 | 56 | F | PCC | 30% | NF1 | PD | Liver, Bone | + | - | - | - | |
| 12 | 59 | F | PGL | Retroperitoneum | NA | NA | PD | Bone, Mediastinal lgll | + | + | + | - |
| 13 | 55 | M | PCC | 22% | NA | Sympt | Bone | - | + | - | - | |
| 14 | 65 | F | PGL | Cauda equina | 13% | Sporadic | PD | 0 | + | + | - | - |
| 15 | 62 | M | PCC | <1% | NA | Sympt | Liver, Bone, Lung | + | + | - | - | |
| 16 | 67 | M | PGL | Aortic bifurcation | 5% | NA | PD | Liver, Bone | + | - | - | - |
| 17 | 80 | M | PCC | <1% | SDHA | Sympt | Retroper lgll. Liver, Lung, Bone | + | - | + | - | |
| 18 | 39 | F | PCC | 3% | SDHB | NA | Retroper and mediastinal lgll, Lung | - | + | - | - | |
| 19 | 72 | M | PCC | 1% | NA | NA | Liver, Bone | + | - | - | - | |
| 20 | 63 | M | HNPGL | Bilateral neck | NA | SDHD | Sympt | 0 | - | + | - | - |
| 21 | 79 | M | PCC | NA | NF1 | PD | Bone | + | + | + | - | |
| 22 | 31 | M | HNPGL | Bilateral neck | NA | NA | Sympt | Liver, Bone | - | + | - | - |
| Patient No. | No. PRRT Cycles First Treatment | No. PRRT Cycles Salvage Treatment | No. PRRT Cycles in Total | Hematological Toxicity | ||
|---|---|---|---|---|---|---|
| Trbc Toxicity Grade | RBC Toxicity Grade | WBC Toxicity Grade | ||||
| 1 | 3 | 3 | 0 | 1 | 1 | |
| 2 | 4 | 4 | 0 | 0 | 0 | |
| 3 | 4 | 4 | 0 | 2 | 0 | |
| 4 | 4 | 4 | 0 | 0 | 0 | |
| 5 | 4 | 3 | 7 | 0 | 0 | 2 |
| 6 | 4 | 4 | 0 | 0 | 0 | |
| 7 | 6 | 4 | 10 | 0 | 1 | 0 |
| 8 | 4 | 4 | 0 | 0 | 2 | |
| 9 | 3 | 3 | 0 | 0 | 0 | |
| 10 | 8 | 3 | 11 | 0 | 0 | 2 |
| 11 | 3 | 3 | 1 | 1 | 0 | |
| 12 | 5 | 5 | 0 | 2 | 0 | |
| 13 | 6 | 6 | 0 | 1 | 0 | |
| 14 | 3 | 2 | 5 | 0 | 2 | 0 |
| 15 | 4 | 4 | 0 | 0 | 0 | |
| 16 | 5 | 4 | 0 | 0 | 0 | |
| 17 | 5 | 4 | 0 | 1 | 0 | |
| 18 | 4 | 2 | 6 | 0 | 1 | 0 |
| 19 | 3 | 3 | 1 | 0 | 1 | |
| 20 | 5 | 5 | 0 | 1 | 0 | |
| 21 | 3 | 3 | 0 | 1 | 0 | |
| 22 | 4 | 4 | 0 | 1 | 1 | |
| Sum | 94 | 14 | 108 | n = 2 grade 1 | n = 9 grade 1 n = 3 grade 2 | n = 3 grade 1 n = 3 grade 2 |
| Patient No. | NM Response ≥50% | Best Response RECIST 1.1 (%) | Best Response RECIST 1.1 (Category) | Time to BR RECIST 1.1 (Months) | OS (Months) | PFS (Months) | Catecholamine Response | CgA Response |
|---|---|---|---|---|---|---|---|---|
| 1 | NA | −17 | SD | 6.7 | 86.8 | 6.7 | −48% * | NA |
| 2 | NA | 0 | SD | 128.4 | 138.2 | 138.2 | Normal | Normal |
| 3 | NA | 0 | SD | 45.2 | 139.2 | 53 | −43% * | −61 |
| 4 | Yes | −13 | SD | 4.7 | 8.2 | 8.2 | Normal | −21 |
| 5 | Yes | −18 | SD | 15.2 | 109.4 | 22.5 | −28% | −35 |
| 6 | No | 0 | SD | 6.5 | 21.6 | 21.6 | Normal | Normal |
| 7 | Yes | −2 | SD | 15.0 | 49.6 | 27 | −38% * | −5 |
| 8 | Yes | 0 | SD | 12.0 | 37.3 | 16.7 | Normal | −51 |
| 9 | No | −14 | SD | 11.3 | 19.2 | 5.6 | −14% | 164 |
| 10 | No | −29 | SD | 13.8 | 54.1 | 18.8 | Normal | −85 |
| 11 | No | −15 | SD | 9.8 | 16.5 | 11.8 | Normal | NA |
| 12 | Yes | −65 | PR | 10.5 | 15.6 | 14.6 | −81% | −15 |
| 13 | No | −6 | SD | 15.6 | 18.8 | 18.3 | −43% | −52 |
| 14 | Yes | −18 | SD | 15.0 | 41.3 | 38.9 | Normal | Normal |
| 15 | Yes | −50 | PR | 9.5 | 14 | 12.7 | −29% | −6 |
| 16 | Yes | −6 | SD | 15.8 | 55.6 | 39.1 | 315% | 138 |
| 17 | No | −7 | SD | 20.0 | 45.4 | 28 | −53% | −56 |
| 18 | No | 0 | SD | 8.2 | 26.4 | 26.4 | Normal | −14 |
| 19 | Yes | 0 | SD | 32.8 | 46.2 | 38.8 | −13% | −55 |
| 20 | No | −7 | SD | 15.5 | 15.6 | 15.6 | Normal | Normal |
| 21 | No | −15 | SD | 16.4 | 24.9 | 22.3 | −89% * | −1 |
| 22 | No | −15 | SD | 8.6 | 11.9 | 8.6 | Normal | Normal |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vyakaranam, A.R.; Crona, J.; Norlén, O.; Granberg, D.; Garske-Román, U.; Sandström, M.; Fröss-Baron, K.; Thiis-Evensen, E.; Hellman, P.; Sundin, A. Favorable Outcome in Patients with Pheochromocytoma and Paraganglioma Treated with 177Lu-DOTATATE. Cancers 2019, 11, 909. https://doi.org/10.3390/cancers11070909
Vyakaranam AR, Crona J, Norlén O, Granberg D, Garske-Román U, Sandström M, Fröss-Baron K, Thiis-Evensen E, Hellman P, Sundin A. Favorable Outcome in Patients with Pheochromocytoma and Paraganglioma Treated with 177Lu-DOTATATE. Cancers. 2019; 11(7):909. https://doi.org/10.3390/cancers11070909
Chicago/Turabian StyleVyakaranam, Achyut Ram, Joakim Crona, Olov Norlén, Dan Granberg, Ulrike Garske-Román, Mattias Sandström, Katarzyna Fröss-Baron, Espen Thiis-Evensen, Per Hellman, and Anders Sundin. 2019. "Favorable Outcome in Patients with Pheochromocytoma and Paraganglioma Treated with 177Lu-DOTATATE" Cancers 11, no. 7: 909. https://doi.org/10.3390/cancers11070909