Prognostic Factors for Event-Free Survival in Pediatric Patients with Hepatoblastoma Based on the 2017 PRETEXT and CHIC-HS Systems

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. PRETEXT Staging System
2.3. Clinical Data Collection for CHIC-HS
2.4. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
3.2. Prognostic Values of Each Variable Used in the 2017 PRETEXT and CHIC-HS Systems
3.3. Prognostic Factors for Predicting Event-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Darbari, A.; Sabin, K.M.; Shapiro, C.N.; Schwarz, K.B. Epidemiology of primary hepatic malignancies in U.S. children. Hepatology 2003, 38, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Carceller, A.; Blanchard, H.; Champagne, J.; St-Vil, D.; Bensoussan, A.L. Surgical resection and chemotherapy improve survival rate for patients with hepatoblastoma. J. Pediatr. Surg. 2001, 36, 755–759. [Google Scholar] [CrossRef]
- Hiyama, E. Pediatric hepatoblastoma: Diagnosis and treatment. Transl. Pediatr. 2014, 3, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Aronson, D.C.; Schnater, J.M.; Staalman, C.R.; Weverling, G.J.; Plaschkes, J.; Perilongo, G.; Brown, J.; Phillips, A.; Otte, J.B.; Czauderna, P.; et al. Predictive value of the pretreatment extent of disease system in hepatoblastoma: Results from the International Society of Pediatric Oncology Liver Tumor Study Group SIOPEL-1 study. J. Clin. Oncol. 2005, 23, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Perilongo, G.; Shafford, E.; Keeling, J.; Pritchard, J.; Brock, P.; Dicks-Mireaux, C.; Phillips, A.; Vos, A.; Plaschkes, J. Pretreatment prognostic factors for children with hepatoblastoma-results from the International Society of Paediatric Oncology (SIOP) study SIOPEL 1. Eur. J. Cancer (Oxf. Eng. 1990) 2000, 36, 1418–1425. [Google Scholar] [CrossRef]
- Roebuck, D.J.; Aronson, D.; Clapuyt, P.; Czauderna, P.; de Ville de Goyet, J.; Gauthier, F.; Mackinlay, G.; Maibach, R.; McHugh, K.; Olsen, O.E.; et al. 2005 PRETEXT: A revised staging system for primary malignant liver tumours of childhood developed by the SIOPEL group. Pediatr. Radiol. 2007, 37, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Towbin, A.J.; Meyers, R.L.; Woodley, H.; Miyazaki, O.; Weldon, C.B.; Morland, B.; Hiyama, E.; Czauderna, P.; Roebuck, D.J.; Tiao, G.M. 2017 PRETEXT: Radiologic staging system for primary hepatic malignancies of childhood revised for the Paediatric Hepatic International Tumour Trial (PHITT). Pediatr. Radiol. 2018, 48, 536–554. [Google Scholar] [CrossRef] [PubMed]
- Perilongo, G.; Malogolowkin, M.; Feusner, J. Hepatoblastoma clinical research: Lessons learned and future challenges. Pediatr. Blood Cancer 2012, 59, 818–821. [Google Scholar] [CrossRef]
- Czauderna, P.; Haeberle, B.; Hiyama, E.; Rangaswami, A.; Krailo, M.; Maibach, R.; Rinaldi, E.; Feng, Y.; Aronson, D.; Malogolowkin, M.; et al. The Children’s Hepatic tumors International Collaboration (CHIC): Novel global rare tumor database yields new prognostic factors in hepatoblastoma and becomes a research model. Eur. J. Cancer (Oxf. Eng. 1990) 2016, 52, 92–101. [Google Scholar] [CrossRef]
- Meyers, R.L.; Maibach, R.; Hiyama, E.; Haberle, B.; Krailo, M.; Rangaswami, A.; Aronson, D.C.; Malogolowkin, M.H.; Perilongo, G.; von Schweinitz, D.; et al. Risk-stratified staging in paediatric hepatoblastoma: A unified analysis from the Children’s Hepatic tumors International Collaboration. Lancet Oncol. 2017, 18, 122–131. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer (Oxf. Eng. 1990) 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Ching, J.Y.L.; Ng, S.; Lam, T.Y.T.; Luk, A.K.C.; Wong, S.H.; Ng, S.C.; Ng, S.S.M.; Wu, J.C.Y.; Chan, F.K.L.; et al. The discriminatory capability of existing scores to predict advanced colorectal neoplasia: A prospective colonoscopy study of 5899 screening participants. Sci. Rep. 2016, 6, 20080. [Google Scholar] [CrossRef] [PubMed]
- Harrell, F.E., Jr.; Lee, K.L.; Mark, D.B. Multivariable prognostic models: Issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat. Med. 1996, 15, 361–387. [Google Scholar] [CrossRef]
- The R Project for Statistical Computing. Available online: www.r-project.org (accessed on 20 March 2018).
- Meyers, R.L.; Rowland, J.R.; Krailo, M.; Chen, Z.; Katzenstein, H.M.; Malogolowkin, M.H. Predictive power of pretreatment prognostic factors in children with hepatoblastoma: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2009, 53, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Maibach, R.; Roebuck, D.; Brugieres, L.; Capra, M.; Brock, P.; Dall’Igna, P.; Otte, J.B.; De Camargo, B.; Zsiros, J.; Zimmermann, A.; et al. Prognostic stratification for children with hepatoblastoma: The SIOPEL experience. Eur. J. Cancer (Oxf. Eng. 1990) 2012, 48, 1543–1549. [Google Scholar] [CrossRef]
- Allan, B.J.; Parikh, P.P.; Diaz, S.; Perez, E.A.; Neville, H.L.; Sola, J.E. Predictors of survival and incidence of hepatoblastoma in the paediatric population. HPB 2013, 15, 741–746. [Google Scholar] [CrossRef] [Green Version]
- Hata, Y. The clinical features and prognosis of hepatoblastoma: Follow-up studies done on pediatric tumors enrolled in the Japanese Pediatric Tumor Registry between 1971 and 1980. Part, I. Committee of Malignant Tumors, Japanese Society of Pediatric Surgeons. Jpn. J. Surg. 1990, 20, 498–502. [Google Scholar] [CrossRef]
- von Schweinitz, D.; Wischmeyer, P.; Leuschner, I.; Schmidt, D.; Wittekind, C.; Harms, D.; Mildenberger, H. Clinico-pathological criteria with prognostic relevance in hepatoblastoma. Eur. J. Cancer (Oxf. Eng. 1990) 1994, 30, 1052–1058. [Google Scholar] [CrossRef]
- Fuchs, J.; Rydzynski, J.; Von Schweinitz, D.; Bode, U.; Hecker, H.; Weinel, P.; Burger, D.; Harms, D.; Erttmann, R.; Oldhafer, K.; et al. Pretreatment prognostic factors and treatment results in children with hepatoblastoma: A report from the German Cooperative Pediatric Liver Tumor Study HB 94. Cancer 2002, 95, 172–182. [Google Scholar] [CrossRef]
- Perilongo, G.; Shafford, E.; Maibach, R.; Aronson, D.; Brugieres, L.; Brock, P.; Childs, M.; Czauderna, P.; MacKinlay, G.; Otte, J.B.; et al. Risk-adapted treatment for childhood hepatoblastoma. final report of the second study of the International Society of Paediatric Oncology--SIOPEL 2. Eur. J. Cancer (Oxf. Eng. 1990) 2004, 40, 411–421. [Google Scholar] [CrossRef]
- Wu, J.F.; Chang, H.H.; Lu, M.Y.; Jou, S.T.; Chang, K.C.; Ni, Y.H.; Chang, M.H. Prognostic roles of pathology markers immunoexpression and clinical parameters in Hepatoblastoma. J. Biomed. Sci. 2017, 24, 62. [Google Scholar] [CrossRef] [PubMed]
- Prokurat, A.; Kluge, P.; Kosciesza, A.; Perek, D.; Kappeler, A.; Zimmermann, A. Transitional liver cell tumors (TLCT) in older children and adolescents: A novel group of aggressive hepatic tumors expressing beta-catenin. Med. Pediatr. Oncol. 2002, 39, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Hishiki, T.; Matsunaga, T.; Sasaki, F.; Yano, M.; Ida, K.; Horie, H.; Kondo, S.; Watanabe, K.; Oue, T.; Tajiri, T.; et al. Outcome of hepatoblastomas treated using the Japanese Study Group for Pediatric Liver Tumor (JPLT) protocol-2: Report from the JPLT. Pediatr. Surg. Int. 2011, 27, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Saettini, F.; Conter, V.; Provenzi, M.; Rota, M.; Giraldi, E.; Foglia, C.; Cavalleri, L.; D’Antiga, L. Is multifocality a prognostic factor in childhood hepatoblastoma? Pediatr. Blood Cancer 2014, 61, 1593–1597. [Google Scholar] [CrossRef] [PubMed]
- Czauderna, P.; Otte, J.B.; Aronson, D.C.; Gauthier, F.; Mackinlay, G.; Roebuck, D.; Plaschkes, J.; Perilongo, G. Guidelines for surgical treatment of hepatoblastoma in the modern era--recommendations from the Childhood Liver Tumour Strategy Group of the International Society of Paediatric Oncology (SIOPEL). Eur. J. Cancer (Oxf. Eng. 1990) 2005, 41, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- D’Antiga, L.; Vallortigara, F.; Cillo, U.; Talenti, E.; Rugge, M.; Zancan, L.; Dall’Igna, P.; De Salvo, G.L.; Perilongo, G. Features predicting unresectability in hepatoblastoma. Cancer 2007, 110, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Schima, W.; Kulinna, C.; Langenberger, H.; Ba-Ssalamah, A. Liver metastases of colorectal cancer: US, CT or MR? Cancer Imaging 2005, 5, S149–S156. [Google Scholar] [CrossRef] [Green Version]
- Floriani, I.; Torri, V.; Rulli, E.; Garavaglia, D.; Compagnoni, A.; Salvolini, L.; Giovagnoni, A. Performance of imaging modalities in diagnosis of liver metastases from colorectal cancer: A systematic review and meta-analysis. JMRI 2010, 31, 19–31. [Google Scholar] [CrossRef]
- Haas, J.E.; Muczynski, K.A.; Krailo, M.; Ablin, A.; Land, V.; Vietti, T.J.; Hammond, G.D. Histopathology and prognosis in childhood hepatoblastoma and hepatocarcinoma. Cancer 1989, 64, 1082–1095. [Google Scholar] [CrossRef]
- Trobaugh-Lotrario, A.D.; Tomlinson, G.E.; Finegold, M.J.; Gore, L.; Feusner, J.H. Small cell undifferentiated variant of hepatoblastoma: Adverse clinical and molecular features similar to rhabdoid tumors. Pediatr. Blood Cancer 2009, 52, 328–334. [Google Scholar] [CrossRef] [Green Version]
- von Schweinitz, D.; Hecker, H.; Harms, D.; Bode, U.; Weinel, P.; Burger, D.; Erttmann, R.; Mildenberger, H. Complete resection before development of drug resistance is essential for survival from advanced hepatoblastoma--a report from the German Cooperative Pediatric Liver Tumor Study HB-89. J. Pediatr. Surg. 1995, 30, 845–852. [Google Scholar] [CrossRef]
- Lim, I.I.P.; Bondoc, A.J.; Geller, J.I.; Tiao, G.M. Hepatoblastoma-The Evolution of Biology, Surgery, and Transplantation. Children 2018, 6, 1. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Category | N (%) or Mean ± Standard Deviation |
|---|---|---|
| Total number of patients | 84 | |
| Age at initial diagnosis (years) | 2.9 ± 3.5 | |
| ≤2 | 56 (66.7) | |
| 3–7 | 12 (14.3) | |
| ≥8 | 9 (10.7) | |
| Sex (male:female) | 48:36 | |
| Serum AFP concentration, ng/mL | <100 | 1 (1.2) |
| 100–999 | 2 (2.4) | |
| 1000–106 | 69 (82.1) | |
| >106 | 10 (11.9) | |
| missing | 2 (2.4) | |
| PRETEXT group | I | 12 (14.3) |
| II | 29 (34.5) | |
| III | 23 (27.3) | |
| IV | 20 (23.8) | |
| Annotation factors | ||
| V (HV or IVC involvement) | Yes | 31 (36.9) |
| Tumor obliterates or encases all three HV | Yes | 9 (10.7) |
| Tumor obliterates or encases IVC | Yes | 21 (25) |
| Tumor thrombus in HV or IVC | Yes | 7 (8.3) |
| P (PV involvement) | Yes | 15 (17.9) |
| Tumor obliterates or encases both PV | Yes | 6 (7.1) |
| Tumor obliterates or encases main PV | Yes | 5 (6.0) |
| Thrombus within a first-order PV or main PV | Yes | 8 (9.5) |
| E (extrahepatic tumor extension) | Yes | 4 (4.8) |
| F (multifocality) | Yes | 32 (38.1) |
| R (tumor rupture) | Yes | 7 (8.3) |
| C (caudate involvement) | Yes | 22 (26.2) |
| N (lymph node metastasis) | Yes | 5 (6.0) |
| M (distant metastasis) | Yes | 23 (27.4) |
| One or more of V, P, E, F, or R | Yes | 46 (54.8) |
| Number of patients with an event | 19 (22.6) | |
| Number of deaths | 8 (9.5) | |
| Preoperative chemotherapy | 81 (96.4) | |
| Cisplatin/doxorubicin | 5 (5.9) | |
| Cisplatin/5-fluorouracil/vincristine | 46 (54.7) | |
| Cisplatin/5-fluorouracil/vincristine/doxorubicin | 22 (26.1) | |
| Ifosfamide/carboplatin/etoposide | 4 (4.7) | |
| Missing | 4 (4.7) | |
| Surgical resection | 54 (64.2) | |
| Orthotopic liver transplantation | 17 (20.2) | |
| Resection of pulmonary metastases | 13 (15.4) |
| Variables | EFS, Months | 3 Year EFS Rate, % | 5 Year EFS Rate, % | p-Value | ||
|---|---|---|---|---|---|---|
| Mean | 95% CI | |||||
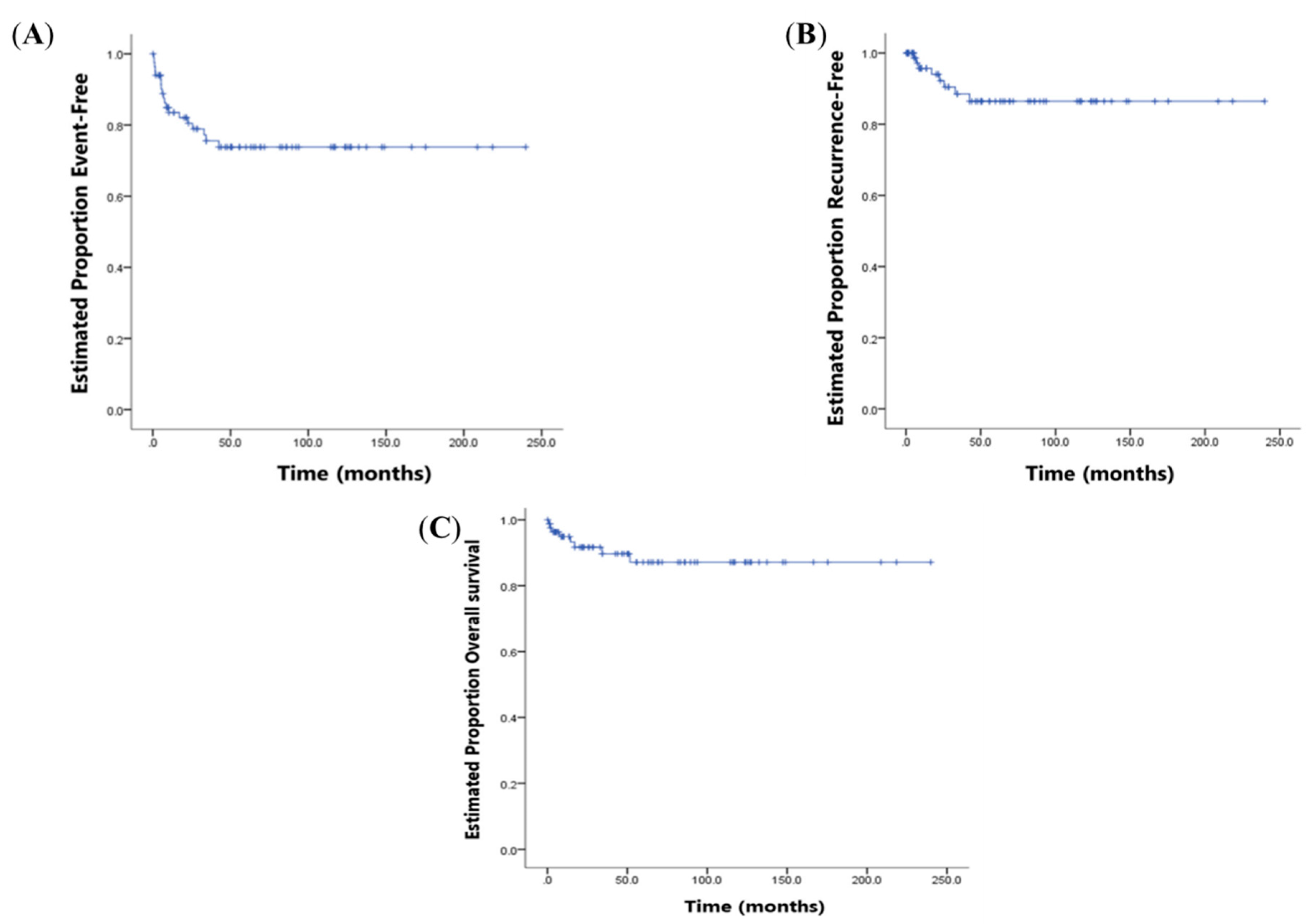
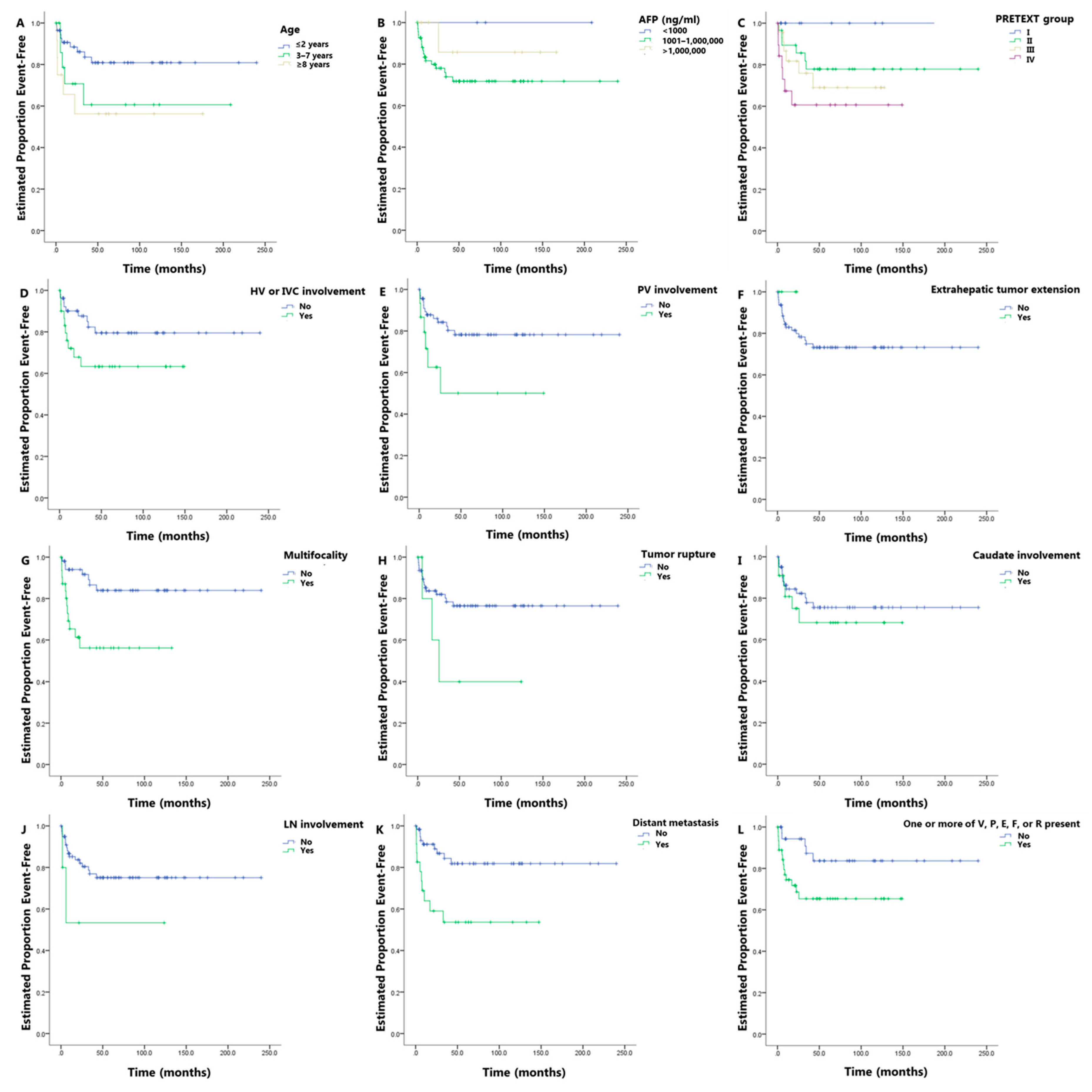
| Overall | 180.6 | 157.5–203.8 | 75.6 | 73.8 | ||
| Age at initial diagnosis (years) | ≤2 | 197.3 | 172.0–222.6 | 83.6 | 80.9 | 0.078 |
| 3–7 | 131.9 | 78.4–185.5 | 60.6 | 60.6 | ||
| ≥8 years | 102.0 | 53.3–150.8 | 56.3 | 56.3 | ||
| AFP, ng/mL | <1000 | * | * | 100 | 100 | 0.389 |
| 1000–106 | 175.9 | 149.8–202.0 | 73.9 | 71.7 | ||
| >106 | 146.3 | 109.8–182.8 | 85.7 | 85.7 | ||
| PRETEXT group | I | * | * | 100 | 100 | 0.106 |
| II | 190.7 | 155.9–222.5 | 77.9 | 77.9 | ||
| III | 93.7 | 70.7–116.6 | 75.9 | 69.0 | ||
| IV | 92.7 | 60.0–125.5 | 60.6 | 60.6 | ||
| Annotation factors | ||||||
| V (HV or IVC involvement) | No | 194.6 | 167.9–221.2 | 82.3 | 79.5 | 0.079 |
| Yes | 97.6 | 72.0–123.3 | 63.3 | 63.3 | ||
| P (PV involvement) | No | 191.0 | 167.4–214.7 | 80.3 | 78.2 | 0.030 |
| Yes | 79.9 | 38.5–121.3 | 50.1 | 50.1 | ||
| E (extrahepatic tumor extension) | No | 179.3 | 155.8–202.8 | 75.0 | 73.2 | 0.456 |
| Yes | * | * | ** | ** | ||
| F (multifocality) | No | 204.9 | 181.1–228.7 | 86.5 | 83.9 | 0.002 |
| Yes | 78.1 | 54.4–101.7 | 56.2 | 56.2 | ||
| R (tumor rupture) | No | 186.6 | 163.5–209.7 | 78.4 | 76.5 | 0.089 |
| Yes | 59.2 | 12.5–105.9 | 40.0 | 40.0 | ||
| C (caudate involvement) | No | 184.9 | 158.6–211.1 | 77.9 | 75.5 | 0.492 |
| Yes | 105.2 | 75.7–134.6 | 68.2 | 68.2 | ||
| N (lymph node metastasis) | No | 183.8 | 160.5–207.1 | 76.9 | 75.1 | 0.133 |
| Yes | 67.9 | 9.9–125.8 | 53.3 | 53.3 | ||
| M (distant metastasis) | No | 199.7 | 175.8–223.7 | 84.3 | 81.9 | 0.003 |
| Yes | 83.2 | 53.8–112.7 | 53.6 | 53.6 | ||
| One or more of V, P, E, F, or R present | No | 204.8 | 176.6–233.0 | 87.3 | 83.7 | 0.035 |
| Yes | 100.6 | 79.7–121.4 | 65.4 | 65.4 | ||
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age at initial diagnosis (years) | ||||||
| ≤2 | 1 | 0.094 | ||||
| 3–7 | 2.352 | 0.787–7.034 | 0.648 | |||
| ≥8 | 3.035 | 1.016–9.064 | ||||
| AFP, ng/mL | ||||||
| <1000 | Infinite | 0.991 | ||||
| 1000–106 | 1 | 0.568 | ||||
| >106 | 0.390 | 0.052–2.933 | ||||
| PRETEXT group | ||||||
| I | Infinite | 0.991 | ||||
| II | 1 | 0.444 | ||||
| III | 1.384 | 0.445–4.302 | ||||
| IV | 2.456 | 0.820–7.355 | ||||
| Annotation factors | ||||||
| V (HV or IVC involvement) | 2.205 | 0.895–5.435 | 0.086 | |||
| P (PV involvement) | 2.819 | 1.062–7.483 | 0.037 | |||
| E (extrahepatic tumor extension) | Infinite | 0.993 | ||||
| F (multifocality) | 3.959 | 1.564–10.135 | 0.004 | 2.908 | 1.061–7.972 | 0.038 |
| R (tumor rupture) | 2.789 | 0.811–9.597 | 0.104 | |||
| C (caudate involvement) | 1.400 | 0.532–3.688 | 0.495 | |||
| N (lymph node metastasis) | 2.939 | 0.671–12.875 | 0.153 | |||
| M (distant metastasis) | 3.566 | 1.448–8.786 | 0.006 | 2.416 | 0.918–6.354 | 0.074 |
| One or more of V, P, E, F, or R present | 2.879 | 1.034–8.018 | 0.043 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, H.M.; Hwang, J.; Kim, K.W.; Namgoong, J.-M.; Kim, D.Y.; Koh, K.-N.; Kim, H.; Cho, Y.A. Prognostic Factors for Event-Free Survival in Pediatric Patients with Hepatoblastoma Based on the 2017 PRETEXT and CHIC-HS Systems. Cancers 2019, 11, 1387. https://doi.org/10.3390/cancers11091387
Yoon HM, Hwang J, Kim KW, Namgoong J-M, Kim DY, Koh K-N, Kim H, Cho YA. Prognostic Factors for Event-Free Survival in Pediatric Patients with Hepatoblastoma Based on the 2017 PRETEXT and CHIC-HS Systems. Cancers. 2019; 11(9):1387. https://doi.org/10.3390/cancers11091387
Chicago/Turabian StyleYoon, Hee Mang, Jisun Hwang, Kyung Won Kim, Jung-Man Namgoong, Dae Yeon Kim, Kyung-Nam Koh, Hyery Kim, and Young Ah Cho. 2019. "Prognostic Factors for Event-Free Survival in Pediatric Patients with Hepatoblastoma Based on the 2017 PRETEXT and CHIC-HS Systems" Cancers 11, no. 9: 1387. https://doi.org/10.3390/cancers11091387