High Specificity of BCL11B and GLG1 for EWSR1-FLI1 and EWSR1-ERG Positive Ewing Sarcoma

 , , , , , , , , , add
Show full author list
, , , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Results
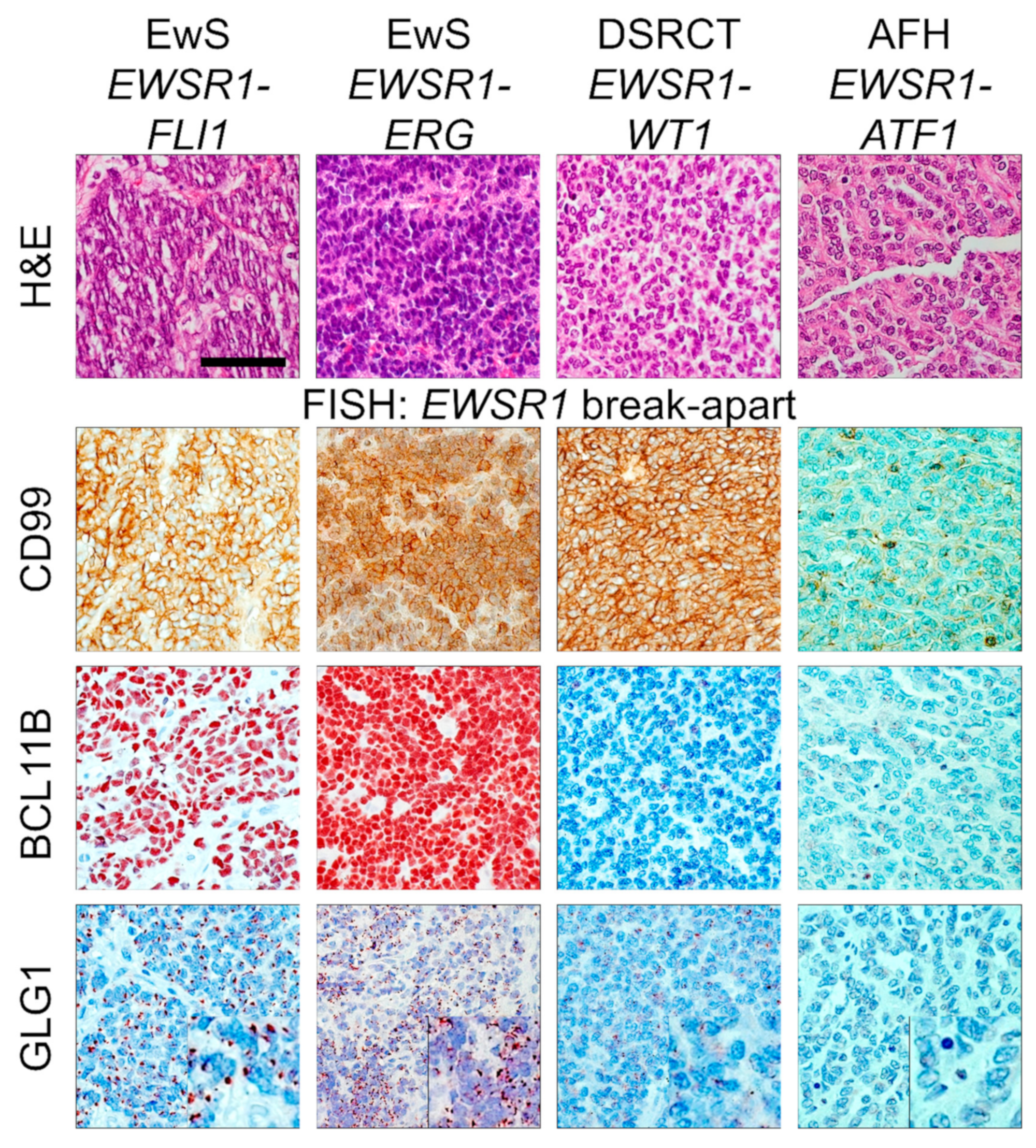
2.1. IHC for CD99 and FISH for EWSR1 Break-Apart Are Not Fully Sufficient to Diagnose EwS
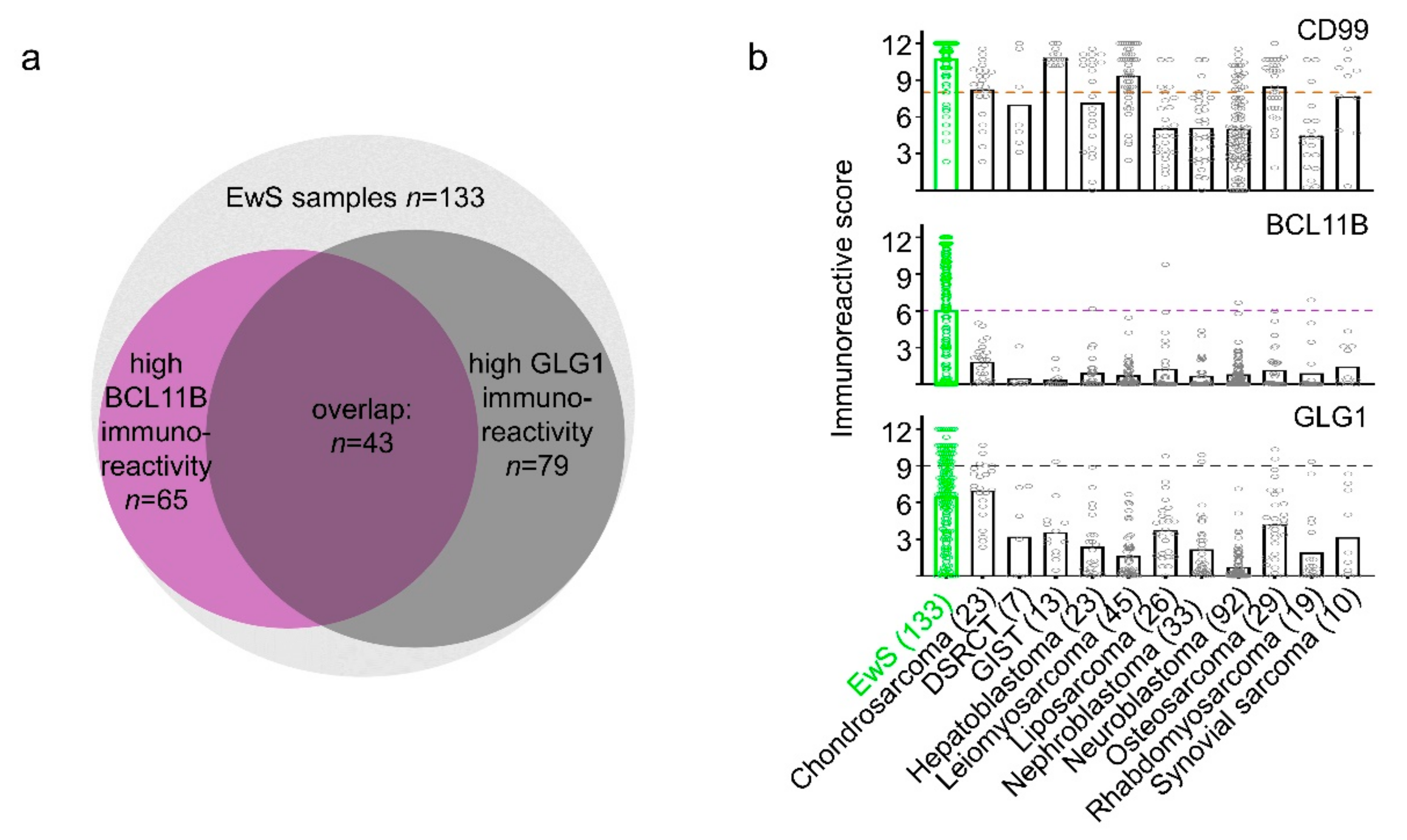
2.2. High Immunoreactivity for BCL11B and/or GLG1 Is Specific for EwS
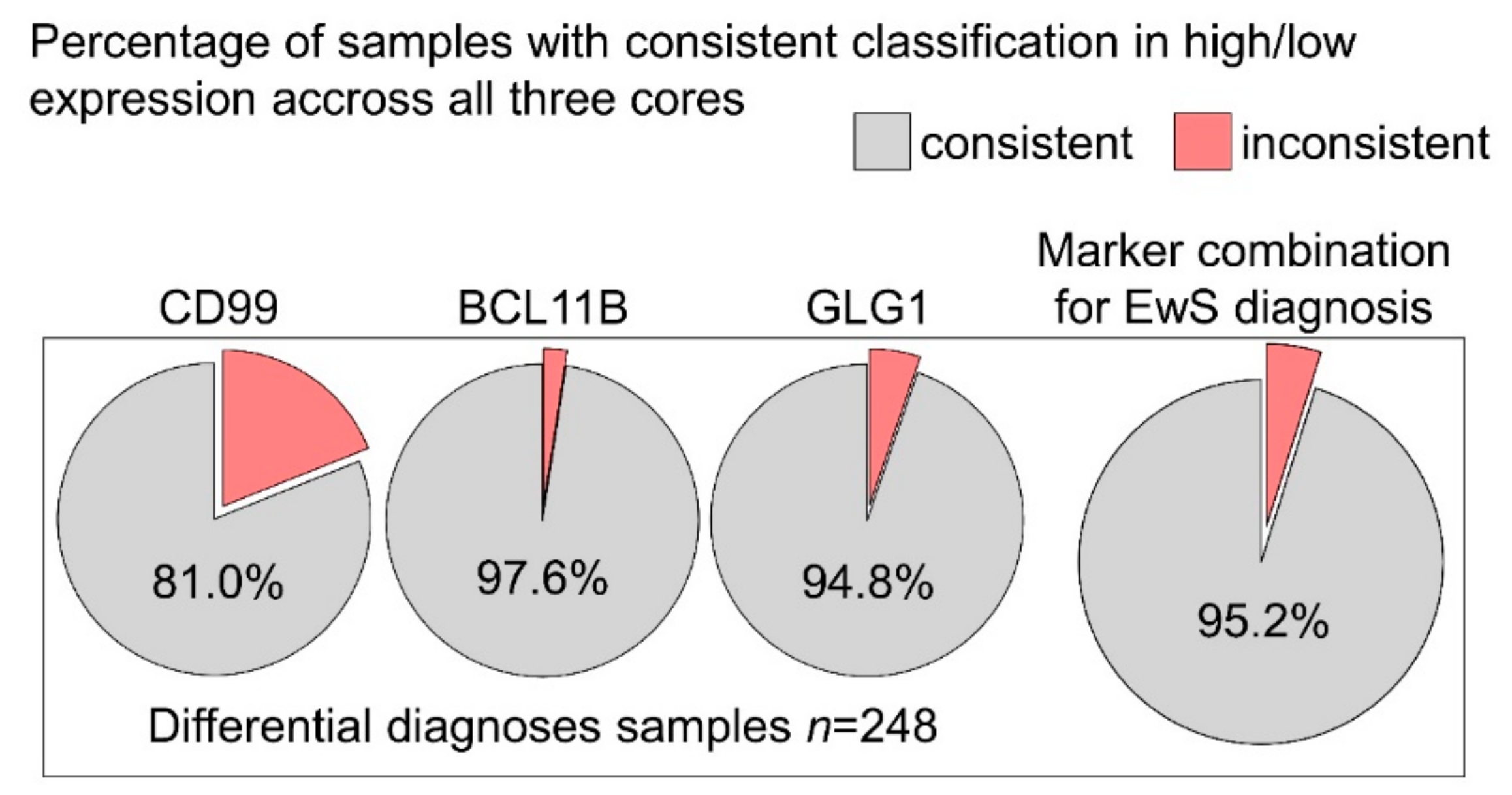
2.3. BCL11B and GLG1 Exhibit Low Intra-Tumoral Heterogeneity in Differential Diagnoses for EwS
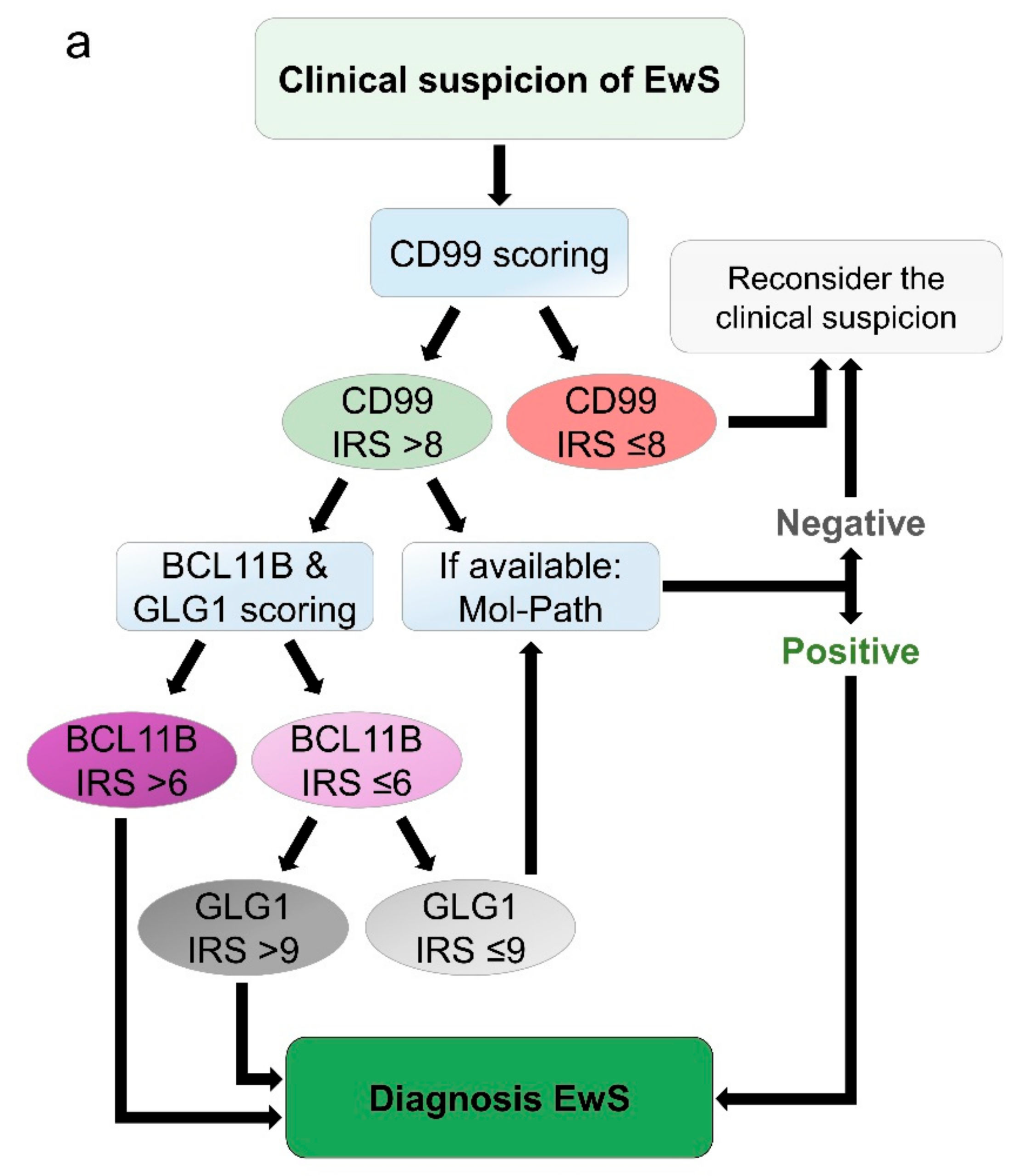
2.4. Proposed Work-Flow for Immunohistochemical Assessment of EwS
3. Discussion
4. Materials and Methods
4.1. Human Samples and Ethics Approval
4.2. Construction of Tissue Microarrays (TMA) and Immunohistochemistry (IHC)
4.3. Evaluation of Immunoreactivity and Automated Cut-Off Finding
4.4. Evaluation of Heterogeneity of Intra-Tumoral Marker Expression
4.5. RNA Extraction, Reverse Transcription, and Quantitative Real-Time PCR (qRT-PCR)
- BCL11B forward: 5′-ATGCCAGAATAGATGCCGG-3′;
- BCL11B reverse: 5′-CTCTATCTCCAGACCCTCGTC-3′;
- GLG1 forward: 5′-GTGGAGTGTAGAGATATAGTTGGC-3′;
- GLG1 reverse: 5′-ATCAGGTCCCCAGAGTCTATC-3′;
- RPLP0 forward: 5′-GAAACTCTGCATTCTCGCTTC-3′;
- RPLP0 reverse: 5′-GGTGTAATCCGTCTCCACAG-3′.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grünewald, T.G.P.; Cidre-Aranaz, F.; Surdez, D.; Tomazou, E.M.; de Álava, E.; Kovar, H.; Sorensen, P.H.; Delattre, O.; Dirksen, U. Ewing sarcoma. Nat. Rev. Dis. Primers 2018, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Kaatsch, P.; Strothotte, J.; Becker, C.; Bielack, S.; Dirksen, U.; Blettner, M. Pediatric bone tumors in Germany from 1987 to 2011: Incidence rates, time trends and survival. Acta Oncol. 2016, 55, 1145–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakata, K.; Ito, Y.; Magadi, W.; Bonaventure, A.; Stiller, C.A.; Katanoda, K.; Matsuda, T.; Miyashiro, I.; Pritchard-Jones, K.; Rachet, B. Childhood cancer incidence and survival in Japan and England: A population-based study (1993-2010). Cancer Sci. 2018, 109, 422–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochefort, P.; Italiano, A.; Laurence, V.; Penel, N.; Lardy-Cleaud, A.; Mir, O.; Chevreau, C.; Bertucci, F.; Bompas, E.; Chaigneau, L.; et al. A Retrospective Multicentric Study of Ewing Sarcoma Family of Tumors in Patients Older Than 50: Management and Outcome. Sci. Rep. 2017, 7, 17917. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, R.; Mayol, B.R.; Davis, M.; Rougraff, B.T. Extraskeletal Ewing’s sarcoma. Cancer 1999, 85, 725–731. [Google Scholar] [CrossRef]
- Duchman, K.R.; Gao, Y.; Miller, B.J. Prognostic factors for survival in patients with Ewing’s sarcoma using the surveillance, epidemiology, and end results (SEER) program database. Cancer Epidemiol. 2015, 39, 189–195. [Google Scholar] [CrossRef]
- Zhang, J.; Pan, Z.; Yang, J.; Yan, X.; Li, Y.; Lyu, J. A nomogram for determining the disease-specific survival in Ewing sarcoma: A population study. BMC Cancer 2019, 19. [Google Scholar] [CrossRef]
- Bosma, S.E.; Ayu, O.; Fiocco, M.; Gelderblom, H.; Dijkstra, P.D.S. Prognostic factors for survival in Ewing sarcoma: A systematic review. Surg. Oncol. 2018, 27, 603–610. [Google Scholar] [CrossRef]
- Gaspar, N.; Hawkins, D.S.; Dirksen, U.; Lewis, I.J.; Ferrari, S.; Le Deley, M.-C.; Kovar, H.; Grimer, R.; Whelan, J.; Claude, L.; et al. Ewing Sarcoma: Current Management and Future Approaches Through Collaboration. J. Clin. Oncol. 2015, 33, 3036–3046. [Google Scholar] [CrossRef]
- Dirksen, U.; Brennan, B.; Le Deley, M.-C.; Cozic, N.; van den Berg, H.; Bhadri, V.; Brichard, B.; Claude, L.; Craft, A.; Amler, S.; et al. High-Dose Chemotherapy Compared With Standard Chemotherapy and Lung Radiation in Ewing Sarcoma With Pulmonary Metastases: Results of the European Ewing Tumour Working Initiative of National Groups, 99 Trial and EWING 2008. J. Clin. Oncol. 2019, 37, 3192–3202. [Google Scholar] [CrossRef]
- PDQ Pediatric Treatment Editorial Board. Ewing Sarcoma Treatment (PDQ®): Health Professional Version. In PDQ Cancer Information Summaries; National Cancer Institute (US): Bethesda, MD, USA, 2002. [Google Scholar]
- Kridis, W.B.; Toumi, N.; Chaari, H.; Khanfir, A.; Ayadi, K.; Keskes, H.; Boudawara, T.; Daoud, J.; Frikha, M. A Review of Ewing Sarcoma Treatment: Is it Still a Subject of Debate? Rev. Recent Clin. Trials 2017, 12, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Andreou, D.; Ranft, A.; Gosheger, G.; Timmermann, B.; Ladenstein, R.; Hartmann, W.; Bauer, S.; Baumhoer, D.; van den Berg, H.; Dijkstra, P.D.S.; et al. GPOH-Euro-EWING99 consortium Which Factors Are Associated with Local Control and Survival of Patients with Localized Pelvic Ewing’s Sarcoma? A Retrospective Analysis of Data from the Euro-EWING99 Trial. Clin. Orthop. 2020, 478, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Whelan, J.; Le Deley, M.-C.; Dirksen, U.; Le Teuff, G.; Brennan, B.; Gaspar, N.; Hawkins, D.S.; Amler, S.; Bauer, S.; Bielack, S.; et al. High-Dose Chemotherapy and Blood Autologous Stem-Cell Rescue Compared With Standard Chemotherapy in Localized High-Risk Ewing Sarcoma: Results of Euro-E.W.I.N.G.99 and Ewing-2008. J. Clin. Oncol. 2018, JCO2018782516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Womer, R.B.; West, D.C.; Krailo, M.D.; Dickman, P.S.; Pawel, B.R.; Grier, H.E.; Marcus, K.; Sailer, S.; Healey, J.H.; Dormans, J.P.; et al. Randomized controlled trial of interval-compressed chemotherapy for the treatment of localized Ewing sarcoma: A report from the Children’s Oncology Group. J. Clin. Oncol. 2012, 30, 4148–4154. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, L.; Felgenhauer, J.L.; Bond, M.C.; Villaluna, D.; Femino, J.D.; Laack, N.N.; Ranganathan, S.; Meyer, J.; Womer, R.B.; Gorlick, R.; et al. Pilot Study of Adding Vincristine, Topotecan, and Cyclophosphamide to Interval-Compressed Chemotherapy in Newly Diagnosed Patients With Localized Ewing Sarcoma: A Report From the Children’s Oncology Group. Pediatr. Blood Cancer 2016, 63, 493–498. [Google Scholar] [CrossRef]
- Alonso, L.; Navarro-Perez, V.; Sanchez-Muñoz, A.; Alba, E. Time to diagnosis of ewing tumors in children and adolescents is not associated with metastasis or survival. J. Clin. Oncol. 2014, 4020, 32. [Google Scholar] [CrossRef]
- Brasme, J.-F.; Chalumeau, M.; Oberlin, O.; Valteau-Couanet, D.; Gaspar, N. Time to diagnosis of Ewing tumors in children and adolescents is not associated with metastasis or survival: A prospective multicenter study of 436 patients. J. Clin. Oncol. 2014, 32, 1935–1940. [Google Scholar] [CrossRef] [Green Version]
- Ewing, J. The Classic: Diffuse Endothelioma of Bone. Clin. Orthop. 2006, 450, 25–27. [Google Scholar] [CrossRef]
- Hung, Y.P.; Lee, J.P.; Bellizzi, A.M.; Hornick, J.L. PHOX2B reliably distinguishes neuroblastoma among small round blue cell tumours. Histopathology 2017, 71, 786–794. [Google Scholar] [CrossRef]
- Parham, D.M. Modern Diagnosis of Small Cell Malignancies of Children. Surg. Pathol. Clin. 2010, 3, 515–551. [Google Scholar] [CrossRef]
- Sbaraglia, M.; Righi, A.; Gambarotti, M.; Dei Tos, A.P. Ewing sarcoma and Ewing-like tumors. Virchows Arch. 2020, 476, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, W.; Mo, W.; Yang, Z. Acute lymphoblastic leukemia arising after treatment of Ewing sarcoma was misdiagnosed as bone marrow metastasis of Ewing sarcoma: A case report. Medicine (Baltimore) 2018, 97, e9644. [Google Scholar] [CrossRef] [PubMed]
- Machado, I.; Noguera, R.; Pellin, A.; Lopez-Guerrero, J.A.; Piqueras, M.; Navarro, S.; Llombart-Bosch, A. Molecular diagnosis of Ewing sarcoma family of tumors: A comparative analysis of 560 cases with FISH and RT-PCR. Diagn. Mol. Pathol. Am. J. Surg. Pathol. Part B 2009, 18, 189–199. [Google Scholar] [CrossRef]
- Fisher, C. The diversity of soft tissue tumours with EWSR1 gene rearrangements: A review. Histopathology 2014, 64, 134–150. [Google Scholar] [CrossRef] [PubMed]
- Ambros, I.M.; Ambros, P.F.; Strehl, S.; Kovar, H.; Gadner, H.; Salzer-Kuntschik, M. MIC2 is a specific marker for Ewing’s sarcoma and peripheral primitive neuroectodermal tumors. Evidence for a common histogenesis of Ewing’s sarcoma and peripheral primitive neuroectodermal tumors from MIC2 expression and specific chromosome aberration. Cancer 1991, 67, 1886–1893. [Google Scholar] [CrossRef]
- Baldauf, M.C.; Orth, M.F.; Dallmayer, M.; Marchetto, A.; Gerke, J.S.; Rubio, R.A.; Kiran, M.M.; Musa, J.; Knott, M.M.L.; Ohmura, S.; et al. Robust diagnosis of Ewing sarcoma by immunohistochemical detection of super-enhancer-driven EWSR1-ETS targets. Oncotarget 2018, 9, 1587–1601. [Google Scholar] [CrossRef] [Green Version]
- Zaccarini, D.J.; Deng, X.; Tull, J.; Maciak, C.; Valente, A.L.; Zhang, S. Expression of TLE-1 and CD99 in Carcinoma: Pitfalls in Diagnosis of Synovial Sarcoma. Appl. Immunohistochem. Mol. Morphol. AIMM 2018, 26, 368–373. [Google Scholar] [CrossRef]
- Chen, D.; Camponeschi, A.; Wu, Q.; Gerasimcik, N.; Li, H.; Shen, X.; Tan, Y.; Sjögren, H.; Nordlund, J.; Lönnerholm, G.; et al. CD99 expression is strongly associated with clinical outcome in children with B-cell precursor acute lymphoblastic leukaemia. Br. J. Haematol. 2019, 184, 418–423. [Google Scholar] [CrossRef] [Green Version]
- Kazlouskaya, V.; Malhotra, S.; Kabigting, F.D.; Lal, K.; Elston, D.M. CD99 expression in dermatofibrosarcoma protuberans and dermatofibroma. Am. J. Dermatopathol. 2014, 36, 392–396. [Google Scholar] [CrossRef]
- Richardson, A.I.; Zhang, D.; Woodroof, J.; Cui, W. p53 expression in large B-cell lymphomas with MYC extra copies and CD99 expression in large B-cell lymphomas in relation to MYC status. Hum. Pathol. 2019, 86, 21–31. [Google Scholar] [CrossRef]
- Delattre, O.; Zucman, J.; Plougastel, B.; Desmaze, C.; Melot, T.; Peter, M.; Kovar, H.; Joubert, I.; de Jong, P.; Rouleau, G. Gene fusion with an ETS DNA-binding domain caused by chromosome translocation in human tumours. Nature 1992, 359, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Zucman, J.; Melot, T.; Desmaze, C.; Ghysdael, J.; Plougastel, B.; Peter, M.; Zucker, J.M.; Triche, T.J.; Sheer, D.; Turc-Carel, C. Combinatorial generation of variable fusion proteins in the Ewing family of tumours. EMBO J. 1993, 12, 4481–4487. [Google Scholar] [CrossRef] [PubMed]
- Tirode, F.; Surdez, D.; Ma, X.; Parker, M.; Le Deley, M.C.; Bahrami, A.; Zhang, Z.; Lapouble, E.; Grossetête-Lalami, S.; Rusch, M.; et al. Genomic landscape of Ewing sarcoma defines an aggressive subtype with co-association of STAG2 and TP53 mutations. Cancer Discov. 2014, 4, 1342–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bridge, R.S.; Rajaram, V.; Dehner, L.P.; Pfeifer, J.D.; Perry, A. Molecular diagnosis of Ewing sarcoma/primitive neuroectodermal tumor in routinely processed tissue: A comparison of two FISH strategies and RT-PCR in malignant round cell tumors. Mod. Pathol. 2006, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gautam, U.; Srinivasan, R.; Rajwanshi, A.; Bansal, D.; Marwaha, R.K.; Vasishtha, R.K. Reverse Transcriptase–Polymerase Chain Reaction as an Ancillary Molecular Technique in the Diagnosis of Small Blue Round Cell Tumors by Fine-Needle Aspiration Cytology. Am. J. Clin. Pathol. 2010, 133, 633–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, T.L.; O’Sullivan, M.J.; Pallen, C.J.; Hayes, M.; Clarkson, P.W.; Winstanley, M.; Sorensen, P.H.B.; Nielsen, T.O.; Horsman, D.E. Ewing sarcoma with novel translocation t(2;16) producing an in-frame fusion of FUS and FEV. J. Mol. Diagn. JMD 2007, 9, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Deniz, K.; Sung, Y.-S.; Zhang, L.; Dry, S.; Antonescu, C.R. Ewing sarcoma with ERG gene rearrangements: A molecular study focusing on the prevalence of FUS-ERG and common pitfalls in detecting EWSR1-ERG fusions by FISH. Genes Chromosomes Cancer 2016, 55, 340–349. [Google Scholar] [CrossRef] [Green Version]
- Papp, G.; Mihály, D.; Sápi, Z. Unusual Signal Patterns of Break-apart FISH Probes Used in the Diagnosis of Soft Tissue Sarcomas. Pathol. Oncol. Res. 2017, 23, 863–871. [Google Scholar] [CrossRef]
- Baldauf, M.C.; Gerke, J.S.; Orth, M.F.; Dallmayer, M.; Baumhoer, D.; de Alava, E.; Hartmann, W.; Kirchner, T.; Grünewald, T.G.P. Are EWSR1-NFATc2-positive sarcomas really Ewing sarcomas? Mod. Pathol. 2018, 31, 997–999. [Google Scholar] [CrossRef]
- Koelsche, C.; Kriegsmann, M.; Kommoss, F.K.F.; Stichel, D.; Kriegsmann, K.; Vokuhl, C.; Grünewald, T.G.P.; Romero-Pérez, L.; Kirchner, T.; de Alava, E.; et al. DNA methylation profiling distinguishes Ewing-like sarcoma with EWSR1-NFATc2 fusion from Ewing sarcoma. J. Cancer Res. Clin. Oncol. 2019, 145, 1273–1281. [Google Scholar] [CrossRef]
- Yau, D.T.W.; Chan, J.K.C.; Bao, S.; Zheng, Z.; Lau, G.T.C.; Chan, A.C.L. Bone Sarcoma With EWSR1-NFATC2 Fusion: Sarcoma With Varied Morphology and Amplification of Fusion Gene Distinct From Ewing Sarcoma. Int. J. Surg. Pathol. 2019, 27, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.W.; Cleton-Jansen, A.-M.; Cleven, A.H.G.; Ruano, D.; van Wezel, T.; Szuhai, K.; Bovée, J.V.M.G. Molecular Analysis of Gene Fusions in Bone and Soft Tissue Tumors by Anchored Multiplex PCR-Based Targeted Next-Generation Sequencing. J. Mol. Diagn. JMD 2018, 20, 653–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koelsche, C.; Hartmann, W.; Schrimpf, D.; Stichel, D.; Jabar, S.; Ranft, A.; Reuss, D.E.; Sahm, F.; Jones, D.T.W.; Bewerunge-Hudler, M.; et al. Array-based DNA-methylation profiling in sarcomas with small blue round cell histology provides valuable diagnostic information. Mod. Pathol. 2018, 31, 1246–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, E.T.; Lui-Sargent, B.; Bell, R.; Lessnick, S.L. BCL11B is up-regulated by EWS/FLI and contributes to the transformed phenotype in Ewing sarcoma. PLoS ONE 2013, 8, e59369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mourelatos, Z.; Gonatas, J.O.; Nycum, L.M.; Gonatas, N.K.; Biegel, J.A. Assignment of the GLG1 gene for MGF-160, a fibroblast growth factor and E-selectin binding membrane sialoglycoprotein of the Golgi apparatus, to chromosome 16q22-q23 by fluorescence in situ hybridization. Genomics 1995, 28, 354–355. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Kervarrec, T.; Tallet, A.; Miquelestorena-Standley, E.; Houben, R.; Schrama, D.; Gambichler, T.; Berthon, P.; Le Corre, Y.; Hainaut-Wierzbicka, E.; Aubin, F.; et al. Morphologic and immunophenotypical features distinguishing Merkel cell polyomavirus-positive and negative Merkel cell carcinoma. Mod. Pathol. 2019. [Google Scholar] [CrossRef]
- Vaikari, V.P.; Du, Y.; Wu, S.; Zhang, T.; Metzeler, K.; Batcha, A.M.N.; Herold, T.; Hiddemann, W.; Akhtari, M.; Alachkar, H. Clinical and preclinical characterization of CD99 isoforms in acute myeloid leukemia. Haematologica 2019. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, L.C.; Soares, R.d.S.; Laurentino, T.d.S.; Lerario, A.M.; Marie, S.K.N.; Oba-Shinjo, S.M. CD99 Expression in Glioblastoma Molecular Subtypes and Role in Migration and Invasion. Int. J. Mol. Sci. 2019, 20. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, P.H.; Liu, X.F.; Delattre, O.; Rowland, J.M.; Biggs, C.A.; Thomas, G.; Triche, T.J. Reverse transcriptase PCR amplification of EWS/FLI-1 fusion transcripts as a diagnostic test for peripheral primitive neuroectodermal tumors of childhood. Diagn. Mol. Pathol. Am. J. Surg. Pathol. Part B 1993, 2, 147–157. [Google Scholar] [CrossRef]
- Paulussen, M.; Bielack, S.; Jürgens, H.; Jost, L. ESMO Guidelines Working Group Ewing’s sarcoma of the bone: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann. Oncol. 2008, 19, ii97–ii98. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.S.; Patel, R.M. Important Recently Characterized Non-Ewing Small Round Cell Tumors. Surg. Pathol. Clin. 2019, 12, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Llombart-Bosch, A.; Machado, I.; Navarro, S.; Bertoni, F.; Bacchini, P.; Alberghini, M.; Karzeladze, A.; Savelov, N.; Petrov, S.; Alvarado-Cabrero, I.; et al. Histological heterogeneity of Ewing’s sarcoma/PNET: An immunohistochemical analysis of 415 genetically confirmed cases with clinical support. Virchows Arch. 2009, 455, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Sadeghipour, A.; Abdi, N.; Babaheidarian, P. CD99: A potential Diagnostic Marker for Differentiating Sub-ependymal Giant Cell Astrocytoma from Other Mimickers: A Report of Five Cases. Iran. J. Pathol. 2017, 12, 286–290. [Google Scholar]
- Antonescu, C. Round cell sarcomas beyond Ewing: Emerging entities. Histopathology 2014, 64, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Charville, G.W.; Wang, W.-L.; Ingram, D.R.; Roy, A.; Thomas, D.; Patel, R.M.; Hornick, J.L.; van de Rijn, M.; Lazar, A.J. EWSR1 fusion proteins mediate PAX7 expression in Ewing sarcoma. Mod. Pathol. 2017, 30, 1312–1320. [Google Scholar] [CrossRef]
- Toki, S.; Wakai, S.; Sekimizu, M.; Mori, T.; Ichikawa, H.; Kawai, A.; Yoshida, A. PAX7 immunohistochemical evaluation of Ewing sarcoma and other small round cell tumours. Histopathology 2018, 73, 645–652. [Google Scholar] [CrossRef]
- Crompton, B.D.; Stewart, C.; Taylor-Weiner, A.; Alexe, G.; Kurek, K.C.; Calicchio, M.L.; Kiezun, A.; Carter, S.L.; Shukla, S.A.; Mehta, S.S.; et al. The genomic landscape of pediatric Ewing sarcoma. Cancer Discov. 2014, 4, 1326–1341. [Google Scholar] [CrossRef] [Green Version]
- Hung, Y.P.; Fletcher, C.D.; Hornick, J.L. Evaluation of NKX2-2 Expression in Round Cell Sarcomas and Other Tumors with EWSR1 Rearrangement: Imperfect Specificity for Ewing Sarcoma. Mod. Pathol. 2016, 29, 370–380. Available online: https://www-nature-com.emedien.ub.uni-muenchen.de/articles/modpathol201631 (accessed on 21 August 2019). [CrossRef]
- Tirado, O.M.; Mateo-Lozano, S.; Villar, J.; Dettin, L.E.; Llort, A.; Gallego, S.; Ban, J.; Kovar, H.; Notario, V. Caveolin-1 (CAV1) is a target of EWS/FLI-1 and a key determinant of the oncogenic phenotype and tumorigenicity of Ewing’s sarcoma cells. Cancer Res. 2006, 66, 9937–9947. [Google Scholar] [CrossRef] [Green Version]
- Magro, G.; Brancato, F.; Musumeci, G.; Alaggio, R.; Parenti, R.; Salvatorelli, L. Cyclin D1 is a useful marker for soft tissue Ewing’s sarcoma/peripheral Primitive Neuroectodermal Tumor in children and adolescents: A comparative immunohistochemical study with rhabdomyosarcoma. Acta Histochem. 2015, 117, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, R.; Matsuyama, A.; Nakamoto, M.; Shiba, E.; Kasai, T.; Hisaoka, M. The combination of CD99 and NKX2.2, a transcriptional target of EWSR1-FLI1, is highly specific for the diagnosis of Ewing sarcoma. Virchows Arch. 2014, 465, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Magro, G.; Longo, F.R.; Angelico, G.; Spadola, S.; Amore, F.F.; Salvatorelli, L. Immunohistochemistry as potential diagnostic pitfall in the most common solid tumors of children and adolescents. Acta Histochem. 2015, 117, 397–414. [Google Scholar] [CrossRef] [PubMed]
- Gangwal, K.; Sankar, S.; Hollenhorst, P.C.; Kinsey, M.; Haroldsen, S.C.; Shah, A.A.; Boucher, K.M.; Watkins, W.S.; Jorde, L.B.; Graves, B.J.; et al. Microsatellites as EWS/FLI response elements in Ewing’s sarcoma. Proc. Natl. Acad. Sci. USA 2008, 105, 10149–10154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, G.; Bittencourt, D.; Laud, K.; Barbier, J.; Delattre, O.; Auboeuf, D.; Dutertre, M. Alteration of cyclin D1 transcript elongation by a mutated transcription factor up-regulates the oncogenic D1b splice isoform in cancer. Proc. Natl. Acad. Sci. USA 2008, 105, 6004–6009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, E.; Federico, S.M.; Chen, X.; Shelat, A.A.; Bradley, C.; Gordon, B.; Karlstrom, A.; Twarog, N.R.; Clay, M.R.; Bahrami, A.; et al. Orthotopic patient-derived xenografts of paediatric solid tumours. Nature 2017, 549, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Musa, J.; Cidre-Aranaz, F.; Aynaud, M.-M.; Orth, M.F.; Knott, M.M.L.; Mirabeau, O.; Mazor, G.; Varon, M.; Hölting, T.L.B.; Grossetête, S.; et al. Cooperation of cancer drivers with regulatory germline variants shapes clinical outcomes. Nat. Commun. 2019, 10, 4128. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Entity | n |
|---|---|
| EwS | 133 |
| Chondrosarcoma | 23 |
| DSRCT | 7 |
| GIST | 13 |
| Hepatoblastoma | 23 |
| Leiomyosarcoma | 45 |
| Liposarcoma (dediff./myxoid) | 26 (17/9) |
| Nephroblastoma | 33 |
| Neuroblastoma | 92 |
| Osteosarcoma | 29 |
| Rhabdomyosarcoma | 19 |
| Synovial sarcoma | 10 |
| total | 453 |
| Cut-Off (CD99 IRS > Indicated Value) | Sensitivity (%) | Specificity (%) |
|---|---|---|
| 0 | 100.0 | 2.5 |
| 1 | 100.0 | 6.6 |
| 2 | 100.0 | 10.0 |
| 3 | 99.2 | 18.1 |
| 4 | 98.5 | 26.9 |
| 6 | 95.5 | 43.8 |
| 8 | 91.0 | 60.0 |
| 9 | 88.0 | 67.5 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orth, M.F.; Hölting, T.L.B.; Dallmayer, M.; Wehweck, F.S.; Paul, T.; Musa, J.; Baldauf, M.C.; Surdez, D.; Delattre, O.; Knott, M.M.L.; et al. High Specificity of BCL11B and GLG1 for EWSR1-FLI1 and EWSR1-ERG Positive Ewing Sarcoma. Cancers 2020, 12, 644. https://doi.org/10.3390/cancers12030644
Orth MF, Hölting TLB, Dallmayer M, Wehweck FS, Paul T, Musa J, Baldauf MC, Surdez D, Delattre O, Knott MML, et al. High Specificity of BCL11B and GLG1 for EWSR1-FLI1 and EWSR1-ERG Positive Ewing Sarcoma. Cancers. 2020; 12(3):644. https://doi.org/10.3390/cancers12030644
Chicago/Turabian StyleOrth, Martin F., Tilman L.B. Hölting, Marlene Dallmayer, Fabienne S. Wehweck, Tanja Paul, Julian Musa, Michaela C. Baldauf, Didier Surdez, Olivier Delattre, Maximilian M. L. Knott, and et al. 2020. "High Specificity of BCL11B and GLG1 for EWSR1-FLI1 and EWSR1-ERG Positive Ewing Sarcoma" Cancers 12, no. 3: 644. https://doi.org/10.3390/cancers12030644