Systematic Analysis of Accuracy in Predicting Complete Oncological Resection in Pancreatic Cancer Patients—Proposal of a New Simplified Borderline Resectability Definition

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
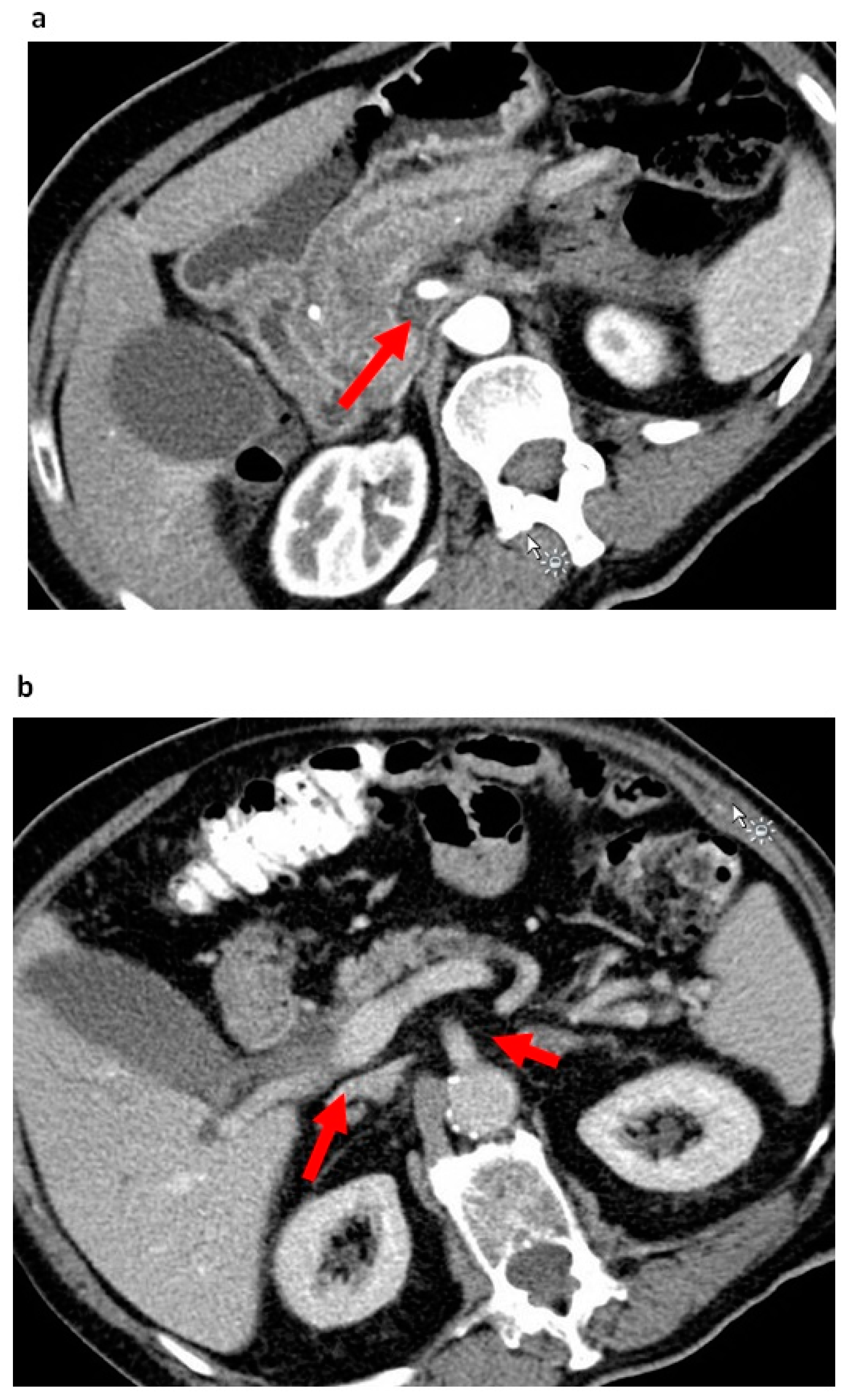
2.1. Baseline Parameters and Perivascular SMA Stranding
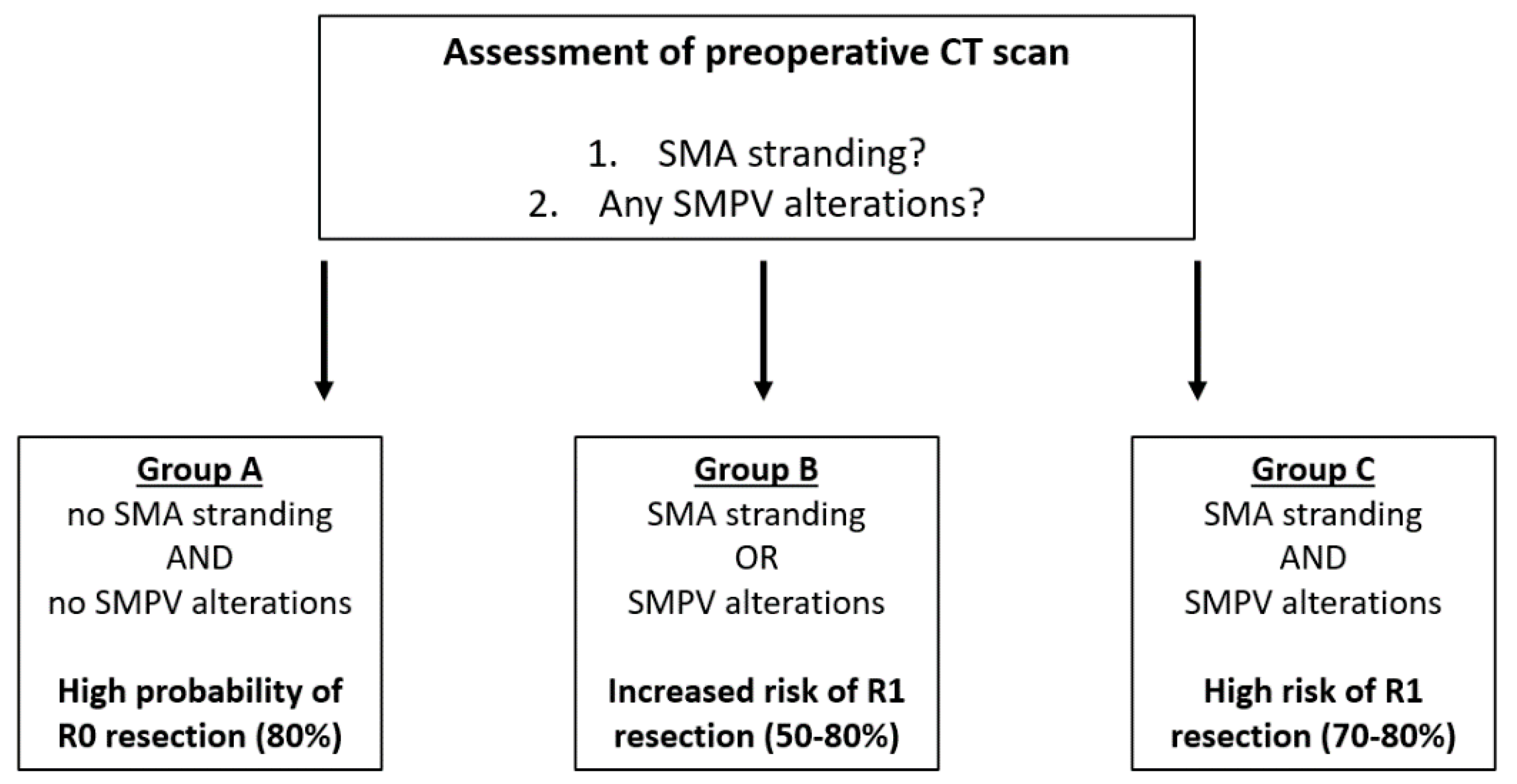
2.2. Borderline Resectability Definitions and Accuracy in the Prediction of R Status
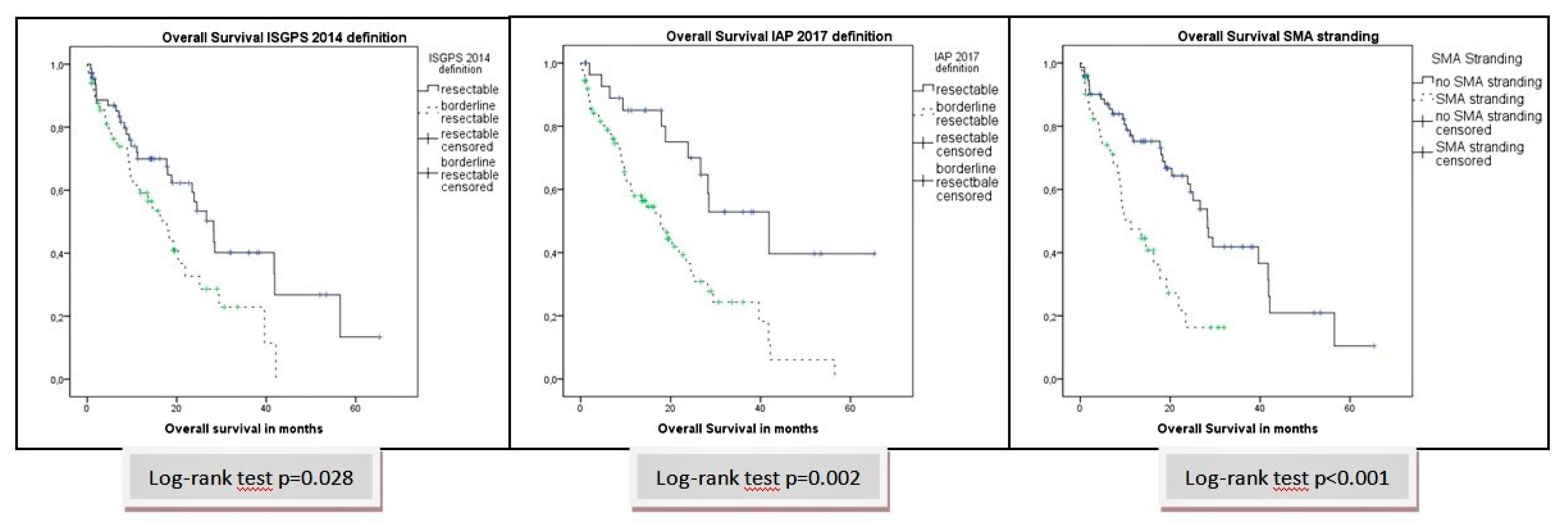
2.3. Survival Analysis Total Cohort
3. Discussion
4. Materials and Methods
4.1. Patients and Study Parameters
4.2. Tests of the Diagnostic Accuracy of the Borderline Resectability Criteria
4.3. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lillemoe, K.D.; Yeo, C.J.; Cameron, J.L. Pancreatic cancer: State-of-the-art care. CA Cancer J. Clin. 2000, 50, 241–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlader, N.; Noone, A.; Krapcho, M.; Garshell, J.; Miller, D.; Altekruse, S. SEER Cancer Statistics Review, 1975–2012; National Cancer Institute: Bethesda, MD, USA, 2015. [Google Scholar]
- Barugola, G.; Partelli, S.; Crippa, S.; Capelli, P.; D’Onofrio, M.; Pederzoli, P.; Falconi, M. Outcomes after resection of locally advanced or borderline resectable pancreatic cancer after neoadjuvant therapy. Am. J. Surg. 2012, 203, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.; Marsh, R.; Herman, J.M.; Shi, Q.; Collison, E.; Venook, A.P.; Kindler, H.L.; Alberts, S.R.; Philip, P.; Lowy, A.M.; et al. Borderline resectable pancreatic cancer: Need for standardization and methods for optimal clinical trial design. Ann. Surg. Oncol. 2013, 20, 2787–2795. [Google Scholar] [CrossRef] [PubMed]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Büchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 155, 977–988. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, Z.; Liu, Y.; Li, B.; Xu, D. Pancreatectomy Combined with Superior Mesenteric Vein–Portal Vein Resection for Pancreatic Cancer: A Meta-analysis. World J. Surg. 2012, 36, 884–891. [Google Scholar] [CrossRef] [Green Version]
- Worni, M.; Castleberry, A.W.; Clary, B.M.; Gloor, B.; Carvalho, E.; Jacobs, D.O.; Pietrobon, R.; Scarborough, J.E.; White, R.R. Concomitant Vascular Reconstruction During Pancreatectomy for Malignant Disease: A Propensity Score–Adjusted, Population-Based Trend Analysis Involving 10 206 Patients. JAMA Surg. 2013, 148, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Mollberg, N.; Rahbari, N.N.; Koch, M.; Hartwig, W.; Hoeger, Y.; Büchler, M.W.; Weitz, J. Arterial resection during pancreatectomy for pancreatic cancer: A systematic review and meta-analysis. Ann. Surg. 2011, 254, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Seufferlein, T.; Porzner, M.; Becker, T.; Budach, V.; Ceyhan, G.; Esposito, I.; Fietkau, R.; Follmann, M.; Friess, H.; Galle, P.; et al. S3-guideline exocrine pancreatic cancer. Z. Gastroenterol. 2013, 51, 1395–1440. [Google Scholar]
- Li, H.; Zeng, M.S.; Zhou, K.R.; Jin, D.Y.; Lou, W.H. Pancreatic adenocarcinoma: The different CT criteria for peripancreatic major arterial and venous invasion. J. Comput. Assist. Tomogr. 2005, 29, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, Y.; Yamashita, Y.; Kadota, M.; Takahashi, M.; Kanemitsu, K.; Hiraoka, T.; Hirota, M.; Ogawa, M.; Takeya, M. Vascular encasement by pancreatic cancer: Correlation of CT findings with surgical and pathologic results. J. Comput. Assist. Tomogr. 2001, 25, 337–342. [Google Scholar] [CrossRef]
- Joo, I.; Lee, J.M.; Lee, E.S.; Son, J.-Y.; Lee, D.H.; Ahn, S.J.; Chang, W.; Lee, S.M.; Kang, H.J.; Yang, H.K. Preoperative CT Classification of the Resectability of Pancreatic Cancer: Interobserver Agreement. Radiology 2019, 293, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Isaji, S.; Mizuno, S.; Windsor, J.A.; Bassi, C.; Fernández-del Castillo, C.; Hackert, T.; Hayasaki, A.; Katz, M.H.G.; Kim, S.W.; Kishiwada, M.; et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology 2018, 18, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Finkelstein, D.M.; Thayer, S.P.; Muzikansky, A.; Fernandez-del Castillo, C.; Warshaw, A.L. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J. Clin. Oncol. 2006, 24, 2897–2902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, J.G.; Bois, J.P.; Sarr, M.G.; Wood, C.M.; Qin, R.; Thomsen, K.M.; Kendrick, M.L.; Farnell, M.B. Predictive and prognostic value of CA 19-9 in resected pancreatic adenocarcinoma. J. Gastrointest. Surg. 2009, 13, 2050–2058. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, W.; Strobel, O.; Hinz, U.; Fritz, S.; Hackert, T.; Roth, C.; Büchler, M.W.; Werner, J. CA19-9 in potentially resectable pancreatic cancer: Perspective to adjust surgical and perioperative therapy. Ann. Surg. Oncol. 2013, 20, 2188–2196. [Google Scholar] [CrossRef] [PubMed]
- Tas, F.; Sen, F.; Odabas, H.; Kilic, L.; Keskin, S.; Yildiz, I. Performance status of patients is the major prognostic factor at all stages of pancreatic cancer. Int. J. Clin. Oncol. 2013, 18, 839–846. [Google Scholar] [CrossRef]
- Kato, Y.; Yamada, S.; Tashiro, M.; Sonohara, F.; Takami, H.; Hayashi, M.; Kanda, M.; Kobayashi, D.; Tanaka, C.; Nakayama, G.; et al. Biological and conditional factors should be included when defining criteria for resectability for patients with pancreatic cancer. HPB (Oxford) 2019, 21, 1211–1218. [Google Scholar] [CrossRef]
- Kato, T.; Ban, D.; Tateishi, U.; Ogura, T.; Ogawa, K.; Ono, H.; Mitsunori, Y.; Kudo, A.; Tanaka, S.; Tanabe, M. Reticular pattern around superior mesenteric artery in computed tomography imaging predicting poor prognosis of pancreatic head cancer. J. Hepatobiliary Pancreat. Sci. 2020, 27, 114–123. [Google Scholar] [CrossRef]
- Wellner, U.F.; Krauss, T.; Csanadi, A.; Lapshyn, H.; Bolm, L.; Timme, S.; Kulemann, B.; Hoeppner, J.; Kuesters, S.; Seifert, G.; et al. Mesopancreatic stromal clearance defines curative resection of pancreatic head cancer and can be predicted preoperatively by radiologic parameters: A retrospective study. Medicine 2016, 95, e2529. [Google Scholar] [CrossRef]
- Gasparini, G.; Pellegatta, M.; Crippa, S.; Lena, M.S.; Belfiori, G.; Doglioni, C.; Taveggia, C.; Falconi, M. Nerves and Pancreatic Cancer: New Insights into a Dangerous Relationship. Cancers 2019, 11, 893. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, M.; Mihaljevic, A.L.; Probst, P.; Heckler, M.; Klaiber, U.; Heger, U.; Büchler, M.W.; Hackert, T. Meta-analysis of recurrence pattern after resection for pancreatic cancer. Br. J. Surg. 2019, 106, 1590–1601. [Google Scholar] [CrossRef] [PubMed]
- Liang, D.; Shi, S.; Xu, J.; Zhang, B.; Qin, Y.; Ji, S.; Xu, W.; Liu, J.; Liu, L.; Liu, C.; et al. New insights into perineural invasion of pancreatic cancer: More than pain. Biochim. Biophys. Acta 2016, 1865, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Nakao, A.; Kanzaki, A.; Fujii, T.; Kodera, Y.; Yamada, S.; Sugimoto, H.; Nomoto, S.; Nakamura, S.; Morita, S.; Takeda, S. Correlation between radiographic classification and pathological grade of portal vein wall invasion in pancreatic head cancer. Ann. Surg. 2012, 255, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Hirono, S.; Kawai, M.; Okada, K.; Miyazawa, M.; Shimizu, A.; Kitahata, Y.; Ueno, M.; Yamaue, H. Pancreatic neck cancer has specific and oncologic characteristics regarding portal vein invasion and lymph node metastasis. Surgery 2015, 159, 426–440. [Google Scholar] [CrossRef] [PubMed]
- Kaissis, G.A.; Lohofer, F.K.; Ziegelmayer, S.; Danner, J.; Jager, C.; Schirren, R.; Ankerst, D.; Ceyhan, G.O.; Friess, H.; Rummeny, E.J.; et al. Borderline-resectable pancreatic adenocarcinoma: Contour irregularity of the venous confluence in pre-operative computed tomography predicts histopathological infiltration. PLoS ONE 2019, 14, e0208717. [Google Scholar] [CrossRef]
- Niesen, W.; Hank, T.; Buchler, M.; Strobel, O. Local radicality and survival outcome of pancreatic cancer surgery. Ann. Gastroenterol. Surg. 2019, 3, 464–475. [Google Scholar] [CrossRef]
- Butturini, G.; Stocken, D.D.; Wente, M.N.; Jeekel, H.; Klinkenbijl, J.H.; Bakkevold, K.E.; Takada, T.; Amano, H.; Dervenis, C.; Bassi, C.; et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: Meta-analysis of randomized controlled trials. Arch. Surg. 2008, 143, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Wellner, U.F.; Makowiec, F.; Bausch, D.; Höppner, J.; Sick, O.; Hopt, U.T.; Keck, T. Locally advanced pancreatic head cancer: Margin-positive resection or bypass? ISRN Surg. 2012, 2012, 513241. [Google Scholar] [CrossRef] [Green Version]
- Menon, K.V.; Gomez, D.; Smith, A.M.; Anthoney, A.; Verbeke, C.S. Impact of margin status on survival following pancreatoduodenectomy for cancer: The Leeds Pathology Protocol (LEEPP). HPB (Oxford) 2009, 11, 18–24. [Google Scholar] [CrossRef] [Green Version]
- Wittekind, C.; Compton, C.; Quirke, P.; Nagtegaal, I.; Merkel, S.; Hermanek, P.; Sobin, L.H. A uniform residual tumor (R) classification: Integration of the R classification and the circumferential margin status. Cancer 2009, 115, 3483–3488. [Google Scholar] [CrossRef]
- Chandrasegaram, M.D.; Goldstein, D.; Simes, J.; Gebski, V.; Kench, J.G.; Gill, A.J.; Samra, J.S.; Merrett, N.D.; Richardson, A.J.; Barbour, A.P. Meta-analysis of radical resection rates and margin assessment in pancreatic cancer. Br. J. Surg. 2015, 102, 1459–1472. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Kwon, J.; Kim, K.; Chie, E.K. Impact of Resection Margin Distance on Survival of Pancreatic Cancer: A Systematic Review and Meta-Analysis. Cancer Res. Treat. 2017, 49, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Silvestris, N.; Brunetti, O.; Vasile, E.; Cellini, F.; Cataldo, I.; Pusceddu, V.; Cattaneo, M.; Partelli, S.; Scartozzi, M.; Aprile, G.; et al. Multimodal treatment of resectable pancreatic ductal adenocarcinoma. Crit. Rev. Oncol. Hematol. 2017, 111, 152–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestris, N.; Longo, V.; Cellini, F.; Reni, M.; Bittoni, A.; Cataldo, I.; Partelli, S.; Falcini, M.; Scarpa, A.; Brunetti, O.; et al. Neoadjuvant multimodal treatment of pancreatic ductal adenocarcinoma. Crit. Rev. Oncol. Hematol. 2016, 98, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kang, C.M.; Bang, S.M.; Choi, J.Y.; Seong, J.S.; Hwang, H.K.; Choi, S.H.; Lee, W.J. The role of neoadjuvant chemoradiation therapy in patients with borderline resectable pancreatic cancer with isolated venous vascular involvement. Medicine 2015, 94, e1233. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.; Fleming, J.B.; Bhosale, P.; Varadhachary, G.; Lee, J.E.; Wolff, R.; Wang, H.; Abbruzzese, J.; Pisters, P.W.; Vauthey, N.J.; et al. Response of borderline resectable pancreatic cancer to neoadjuvant therapy is not reflected by radiographic indicators. Cancer 2012, 118, 5749–5756. [Google Scholar] [CrossRef] [PubMed]
- Boone, B.A.; Steve, J.; Krasinskas, A.M.; Zureikat, A.H.; Lembersky, B.C.; Gibson, M.K.; Stoller, R.G.; Zeh, H.J.; Bahary, N. Outcomes with FOLFIRINOX for borderline resectable and locally unresectable pancreatic cancer. J. Surg. Oncol. 2013, 108, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Katz, M.H.G.; Shi, Q.; Ahmad, S.A.; Herman, J.M.; Marsh R de, W.; Collisson, E.; Schwartz, L.; Frankel, W.; Martin, R.; Conway, W.; et al. Preoperative Modified FOLFIRINOX Treatment Followed by Capecitabine-Based Chemoradiation for Borderline Resectable Pancreatic Cancer: Alliance for Clinical Trials in Oncology Trial A021101. JAMA Surg. 2016, 151, e161137. [Google Scholar] [CrossRef] [Green Version]
- Katz, M.H.G.; Ou, F.-S.; Herman, J.M.; Ahmad, S.A.; Wolpin, B.; Marsh, R.; Behr, S.; Shi, Q.; Chuong, M.; Schwartz, L.H.; et al. Alliance for clinical trials in oncology (ALLIANCE) trial A021501: Preoperative extended chemotherapy vs. chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas. BMC Cancer 2017, 17, 505. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [Green Version]
- Broders, A.C., Sr. Malignant neoplasia of normally situated and heterotopic lymphoid tissue and its numerical microscopic grading. Tex. State J. Med. 1953, 49, 234. [Google Scholar] [PubMed]
- Raut, C.P.; Tseng, J.F.; Sun, C.C.; Wang, H.; Wolff, R.A.; Crane, C.H.; Hwang, R.; Vauthey, J.N.; Abdalla, E.K.; Lee, J.E.; et al. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann. Surg. 2007, 246, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Parameters SMA Stranding | No SMA Stranding | Positive SMA Stranding | |
|---|---|---|---|
| Total n | 75 | 43 | |
| Parameter | n (%)/median (range) | n (%)/median (range) | p-value |
| Age | |||
| < 68 | 39 (52.0) | 20 (46.5) | |
| > 68 | 36 (48.0) | 23 (43.5) | 0.702 |
| Sex | |||
| male | 31 (41.3) | 26 (60.5) | |
| female | 44 (58.7) | 17 (39.5) | 0.060 |
| ASA Score | |||
| 0–2 | 38 (50.7) | 15 (34.9) | |
| 3–4 | 37 (49.3) | 28 (65.1) | 0.125 |
| Serum CA 19-9 | |||
| >40 U/L | 22 (66.7) | 20 (80.0) | 0.375 |
| Borderline ISGPS 2014 Definition | |||
| BR- | 52 (69.3) | 16 (37.2) | |
| BR+ | 23 (30.7) | 27 (62.8) | 0.001 |
| Borderline IAP 2017 Definition | |||
| BR- | 26 (34.7) | 4 (9.3) | |
| BR+ | 49 (65.3) | 39 (90.7) | 0.002 |
| Any SMPV alterations | |||
| no | 51 (68.0) | 14 (32.6) | |
| yes | 24 (32.0) | 29 (67.4) | 0.001 |
| PVR | |||
| no | 50 (66.7) | 30 (69.8) | |
| yes | 25 (33.3) | 13 (30.2) | 0.839 |
| Multivisceral resection | |||
| no | 70 (93.3) | 38 (88.4) | |
| yes | 5 (6.7) | 5 (11.6) | 0.494 |
| T stage | |||
| T1/2 | 17 (22.7) | 10 (23.3) | |
| T3/4 | 58 (77.3) | 33 (76.7) | 1.000 |
| N stage | |||
| N0 | 29 (38.7) | 8 (18.6) | |
| N+ | 46 (61.3) | 35 (81.4) | 0.025 |
| M | |||
| M0 | 72 (96.0) | 41 (95.3) | |
| M1 | 3 (4.0) | 2 (4.7) | 1.000 |
| LNR | |||
| < median 0.08 | 43 (57.3) | 17 (39.5) | |
| > median 0.08 | 32 (42.7) | 26 (60.5) | 0.085 |
| Grading | |||
| G 1/2 | 53 (71.6) | 32 (84.2) | |
| G 3/4 | 21 (28.4) | 6 (15.8) | 0.167 |
| Lymphovascular invasion | |||
| L0 | 45 (60.0) | 26 (60.5) | |
| L1 | 30 (40.0) | 17 (39.5) | 1.000 |
| Vascular invasion | |||
| V0 | 59 (78.7) | 28 (65.1) | |
| V1 | 16 (21.3) | 15 (34.9) | 0.130 |
| Perineural invasion | |||
| Pn0 | 20 (26.7) | 4 (9.5) | |
| Pn1 | 55 (73.3) | 38 (90.5) | 0.032 |
| Adjuvant therapy | |||
| no | 35 (46.7) | 26 (60.5) | |
| yes | 40 (53.3) | 17 (39.5) | 0.182 |
| Borderline Resectability Definitions and Prediction of R Status | ||||||||
|---|---|---|---|---|---|---|---|---|
| UICC/AJCC R Status | ||||||||
| R0 | R+ | |||||||
| n/median | %/range | n/median | %/range | p-value | Sensitivity | NPV | ||
| total n | 73 | 61.9 | 45 | 38.1 | ||||
| Borderline ISGPS 2014 Definition | BR- | 47 | 64.4 | 21 | 46.7 | 0.084 | 48% | 64% |
| BR+ | 26 | 35.6 | 24 | 53.3 | ||||
| Borderline IAP 2017 Definition | BR- | 23 | 31.5 | 7 | 15.6 | 0.081 | 43% | 31% |
| BR+ | 50 | 68.5 | 38 | 84.4 | ||||
| Any SMPV alterations | no | 44 | 60.3 | 21 | 46.7 | 0.183 | 45% | 60% |
| yes | 29 | 39.7 | 24 | 53.3 | ||||
| SMA Stranding | no | 53 | 72.6 | 22 | 48.9 | 0.011 | 53% | 73% |
| yes | 20 | 27.4 | 23 | 51.1 | ||||
| Borderline novel Definition | BR- | 59 | 80.8 | 29 | 64.4 | 0.040 | 53% | 81% |
| BR+ | 14 | 19.2 | 16 | 35.6 | ||||
| Leeds/Wittekind R status | ||||||||
| R0 wide | R0 narrow/R1 | |||||||
| n/median | %/range | n/median | %/range | p-value | Sensitivity | NPV | ||
| total n | 38 | 32.2 | 80 | 67.8 | ||||
| Borderline ISGPS 2014 Definition | BR- | 23 | 60.5 | 45 | 56.3 | 0.695 | 60% | 60% |
| BR+ | 15 | 39.5 | 35 | 43.7 | ||||
| Borderline IAP 2017 Definition | BR- | 11 | 28.9 | 19 | 23.8 | 0.652 | 69% | 29% |
| BR+ | 27 | 71.1 | 61 | 76.2 | ||||
| Any SMPV alterations | no | 23 | 60.5 | 42 | 52.5 | 0.436 | 70% | 60% |
| yes | 15 | 39.5 | 38 | 47.5 | ||||
| SMA Stranding | no | 29 | 76.3 | 46 | 57.5 | 0.036 | 80% | 76% |
| yes | 9 | 23.7 | 34 | 42.5 | ||||
| Borderline novel Definition | BR- | 30 | 78.9 | 58 | 72.5 | 0.505 | 73% | 79% |
| BR+ | 8 | 21.1 | 22 | 27.5 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolm, L.; Mueller, K.; May, K.; Sondermann, S.; Petrova, E.; Lapshyn, H.; Honselmann, K.C.; Bausch, D.; Zemskov, S.; Bronsert, P.; et al. Systematic Analysis of Accuracy in Predicting Complete Oncological Resection in Pancreatic Cancer Patients—Proposal of a New Simplified Borderline Resectability Definition. Cancers 2020, 12, 882. https://doi.org/10.3390/cancers12040882
Bolm L, Mueller K, May K, Sondermann S, Petrova E, Lapshyn H, Honselmann KC, Bausch D, Zemskov S, Bronsert P, et al. Systematic Analysis of Accuracy in Predicting Complete Oncological Resection in Pancreatic Cancer Patients—Proposal of a New Simplified Borderline Resectability Definition. Cancers. 2020; 12(4):882. https://doi.org/10.3390/cancers12040882
Chicago/Turabian StyleBolm, Louisa, Katharina Mueller, Katharina May, Stefan Sondermann, Ekaterina Petrova, Hryhoriy Lapshyn, Kim Christin Honselmann, Dirk Bausch, Sergii Zemskov, Peter Bronsert, and et al. 2020. "Systematic Analysis of Accuracy in Predicting Complete Oncological Resection in Pancreatic Cancer Patients—Proposal of a New Simplified Borderline Resectability Definition" Cancers 12, no. 4: 882. https://doi.org/10.3390/cancers12040882