
Combination of Sorafenib and Transarterial Chemoembolization in Selected Patients with Advanced-Stage Hepatocellular Carcinoma: A Retrospective Cohort Study at Three German Liver Centers

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
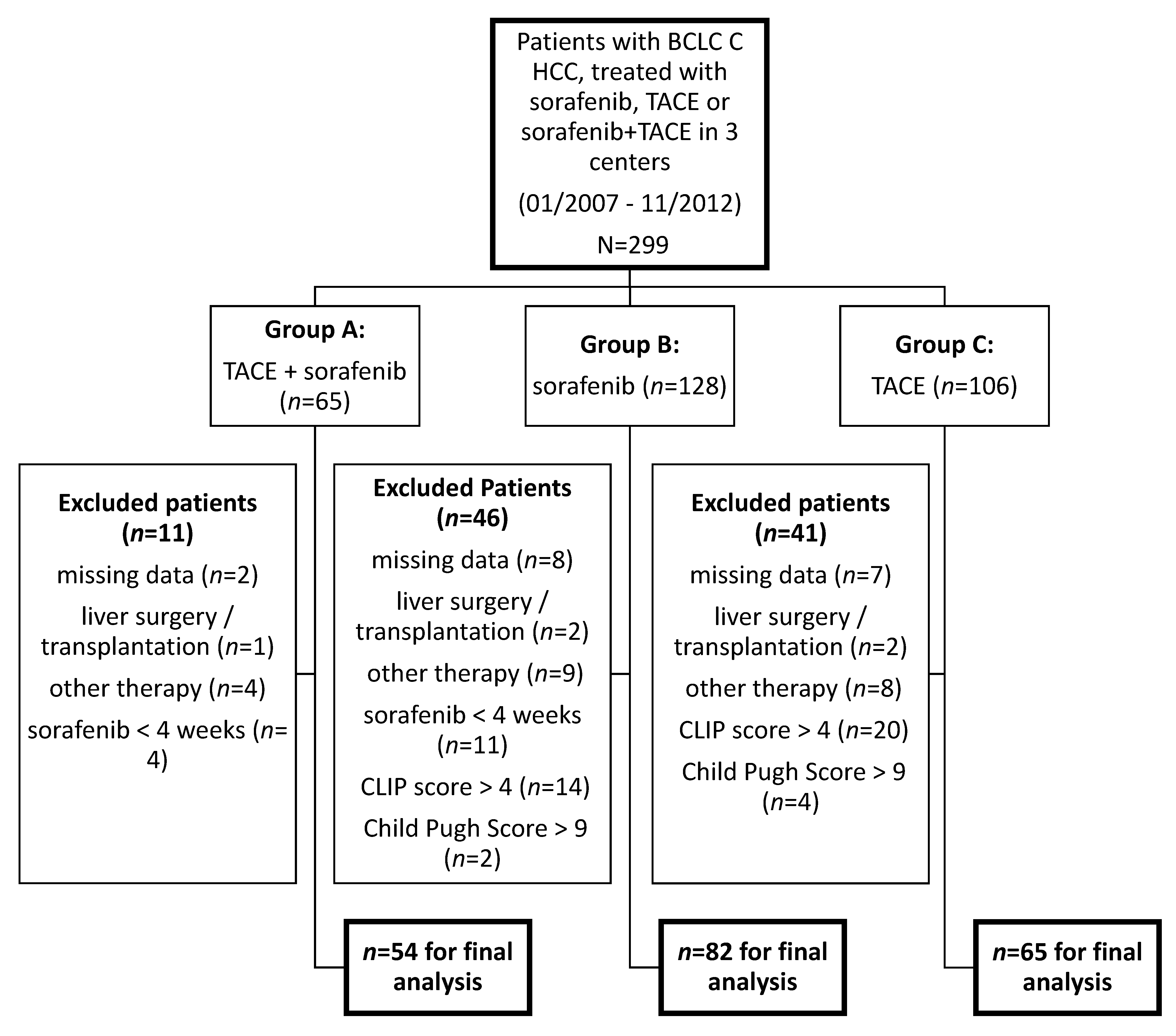
2. Patients and Methods
3. Statistical Analyses
4. Results
4.1. Patients
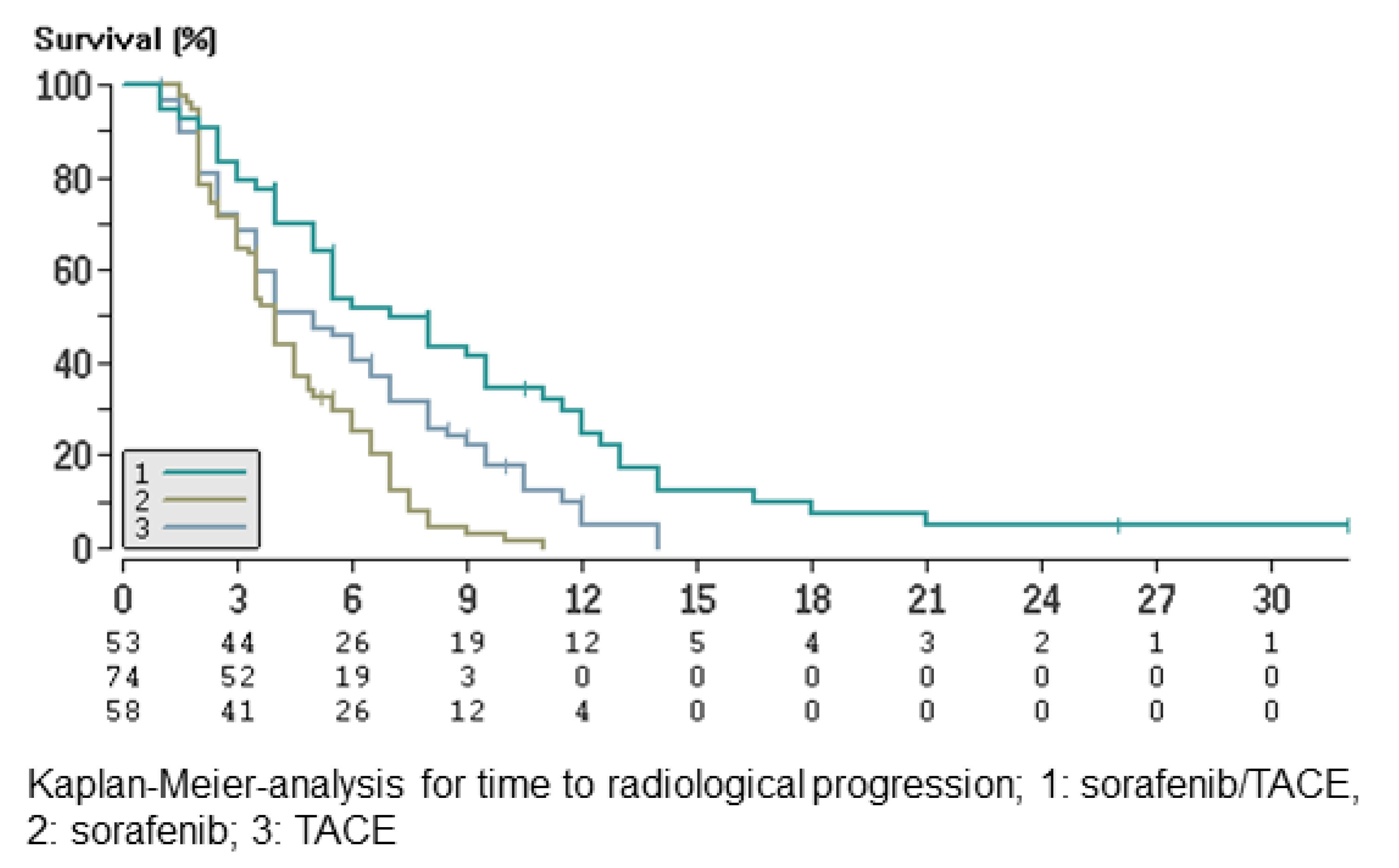
4.2. Radiologic Response
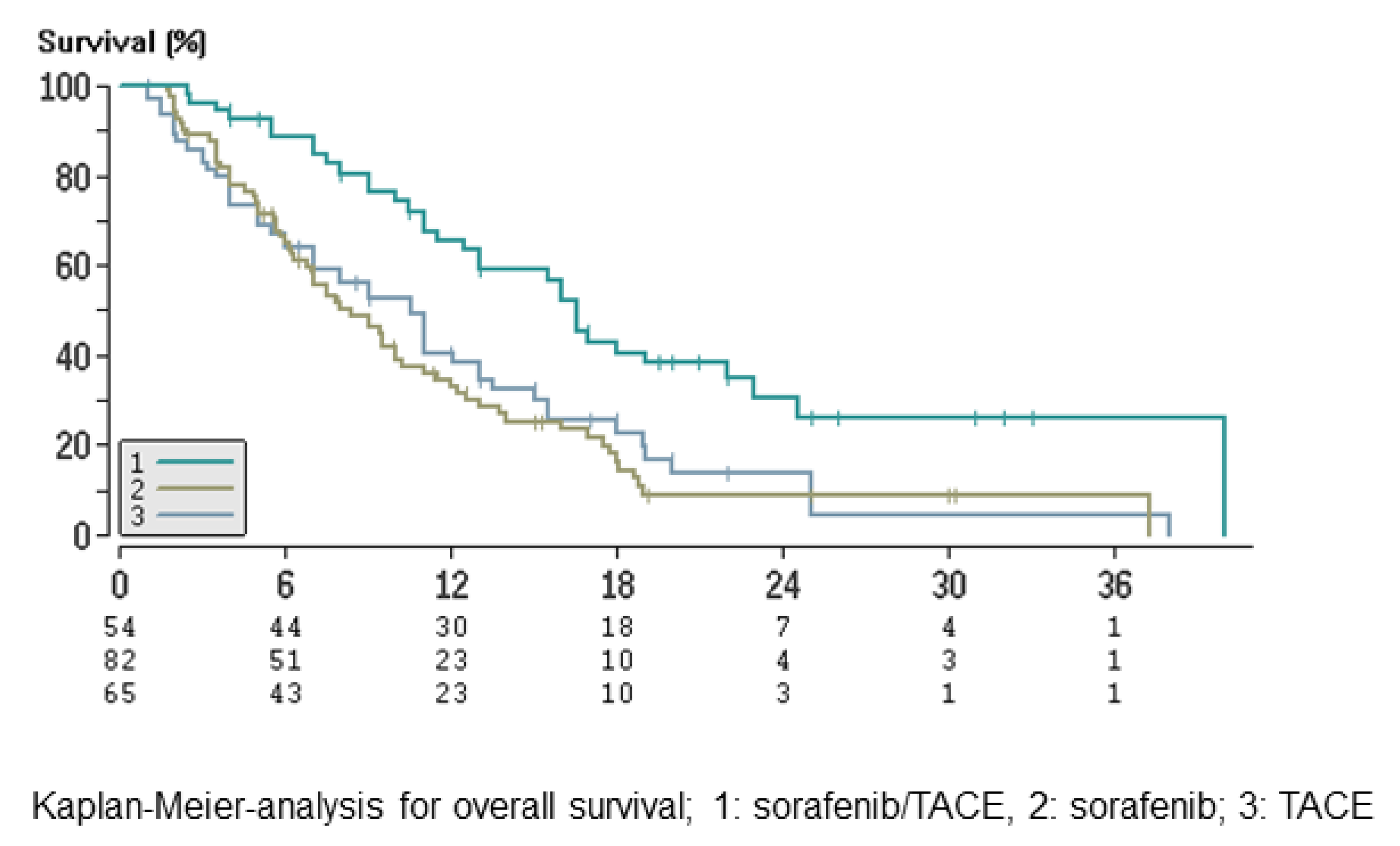
4.3. Survival Times
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. Available online: https://pubmed.ncbi.nlm.nih.gov/21296855/ (accessed on 20 November 2020). [CrossRef] [Green Version]
- El-Serag, H.B. Hepatocellular Carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–337. Available online: https://pubmed.ncbi.nlm.nih.gov/10518312/ (accessed on 20 November 2020). [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. Available online: https://pubmed.ncbi.nlm.nih.gov/21374666/ (accessed on 20 November 2020). [CrossRef] [PubMed]
- Llovet, J.M.; Ducreux, M.; Lencioni, R.; Di Bisceglie, A.; Galle, P.; Dufour, J. European Association for the Study of the Liver: European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar]
- Llovet, J.M.; Bruix, J. Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 2003, 37, 429–442. Available online: https://pubmed.ncbi.nlm.nih.gov/12540794/ (accessed on 20 November 2020). [CrossRef]
- Han, G.; Berhane, S.; Toyoda, H.; Bettinger, D.; Elshaarawy, O.; Chan, A.W.; Kirstein, M.; Mosconi, C.; Hucke, F.; Palmer, D.; et al. Prediction of Survival Among Patients Receiving Transarterial Chemoembolization for Hepatocellular Carcinoma: A Response-Based Approach. Hepatology 2020, 72, 198–212. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. Available online: https://pubmed.ncbi.nlm.nih.gov/18650514/ (accessed on 20 November 2020). [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Uka, K.; Aikata, H.; Takaki, S.; Shirakawa, H.; Jeong, S.C.; Yamashina, K.; Hiramatsu, A.; Kodama, H.; Takahashi, S.; Chayama, K. Clinical features and prognosis of patients with extrahepatic metastases from hepatocellular carcinoma. World J. Gastroenterol. 2007, 13, 414–420. Available online: https://pubmed.ncbi.nlm.nih.gov/17230611/ (accessed on 20 November 2020). [CrossRef]
- Yoo, D.J.; Kim, K.M.; Jin, Y.J.; Shim, J.H.; Ko, G.Y.; Yoon, H.K.; Sung, K.B.; Lee, J.L.; Kang, Y.K.; Lim, Y.S.; et al. Clinical outcome of 251 patients with extrahepatic metastasis at initial diagnosis of hepatocellular carcinoma: Does transarterial chemoembolization improve survival in these patients? J. Gastroenterol. Hepatol. 2011, 26, 145–154. Available online: https://pubmed.ncbi.nlm.nih.gov/21175808/ (accessed on 20 November 2020). [CrossRef]
- Pinter, M.; Hucke, F.; Graziadei, I.; Vogel, W.; Maieron, A.; Königsberg, R.; Stauber, R.; Grünberger, B.; Müller, C.; Kölblinger, C.; et al. Advanced-stage hepatocellular carcinoma: Transarterial chemoembolization versus sorafenib. Radiology 2012, 263, 590–599. Available online: https://pubmed.ncbi.nlm.nih.gov/22438359/ (accessed on 20 November 2020). [CrossRef] [PubMed] [Green Version]
- Georgiades, C.S.; Hong, K.; D’Angelo, M.; Geschwind, J.F.H. Safety and efficacy of transarterial chemoembolization in patients with unresectable hepatocellular carcinoma and portal vein thrombosis. J. Vasc. Interv. Radiol. 2005, 16, 1653–1659. Available online: https://pubmed.ncbi.nlm.nih.gov/16371532/ (accessed on 20 November 2020). [CrossRef]
- Schicho, A.; Hellerbrand, C.; Krüger, K.; Beyer, L.P.; Wohlgemuth, W.; Niessen, C.; Hohenstein, E.; Stroszczynski, C.; Pereira, P.L.; Wiggermann, P. Impact of different embolic agents for transarterial chemoembolization (TACE) procedures on systemic vascular endothelial growth factor (VEGF) levels. J. Clin. Transl. Hepatol. 2016, 4, 288–292. Available online: https://pubmed.ncbi.nlm.nih.gov/28097096/ (accessed on 17 April 2021). [PubMed] [Green Version]
- Greten, T.F.; Korangy, F.; Manns, M.P.; Malek, N.P. Molecular therapy for the treatment of hepatocellular carcinoma. Br. J. Cancer 2009, 100, 19–23. Available online: https://pubmed.ncbi.nlm.nih.gov/19018262/ (accessed on 17 April 2021). [CrossRef]
- Bai, W.; Wang, Y.J.; Zhao, Y.; Qi, X.S.; Yin, Z.X.; He, C.Y.; Li, R.J.; Wu, K.C.; Xia, J.L.; Fan, D.M.; et al. Sorafenib in combination with transarterial chemoembolization improves the survival of patients with unresectable hepatocellular carcinoma: A propensity score matching study. J. Dig. Dis. 2013, 14, 181–190. Available online: https://pubmed.ncbi.nlm.nih.gov/23324079/ (accessed on 20 November 2020). [CrossRef]
- Zhao, Y.; Wang, W.J.; Guan, S.; Li, H.L.; Xu, R.C.; Wu, J.B.; Liu, J.S.; Li, H.P.; Bai, W.; Yin, Z.X.; et al. Sorafenib combined with transarterial chemoembolization for the treatment of advanced hepatocellular carcinoma: A large-scale multicenter study of 222 patients. Ann. Oncol. 2013, 24, 1786–1792. Available online: http://www.ncbi.nlm.nih.gov/pubmed/23508822 (accessed on 18 June 2019). [CrossRef]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Duran, R.; Chapiro, J.; Sohn, J.H.; Sahu, S.; Fleckenstein, F.; Smolka, S.; Pawlik, T.M.; Schernthaner, R.; Zhao, L.; et al. Transarterial Chemoembolization for the Treatment of Advanced-Stage Hepatocellular Carcinoma. J. Gastrointest. Surg. 2016, 20, 2002–2009. Available online: https://pubmed.ncbi.nlm.nih.gov/27714643/ (accessed on 28 December 2020). [CrossRef] [Green Version]
- Lv, W.-F.; Liu, K.C.; Lu, D.; Zhou, C.Z.; Cheng, D.L.; Xiao, J.K.; Zhang, X.M.; Zhang, Z.F. Transarterial chemoembolization for hepatocellular carcinoma combined with portal vein tumor thrombosis. Cancer Manag. Res. 2018, 10, 4719–4726. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30410405 (accessed on 20 November 2020). [CrossRef] [Green Version]
- Schütte, K.; Schinner, R.; Fabritius, M.P.; Möller, M.; Kuhl, C.; Iezzi, R.; Öcal, O.; Pech, M.; Peynircioglu, B.; Seidensticker, M.; et al. Impact of Extrahepatic Metastases on Overall Survival in Patients with Advanced Liver Dominant Hepatocellular Carcinoma: A Subanalysis of the SORAMIC Trial. Liver Cancer 2020, 9, 771–786. Available online: https://pubmed.ncbi.nlm.nih.gov/33442545/ (accessed on 17 April 2021). [CrossRef]
- Lencioni, R.; Llovet, J.M.; Han, G.; Tak, W.Y.; Yang, J.; Guglielmi, A.; Paik, S.W.; Reig, M.; Chau, G.Y.; Luca, A.; et al. Sorafenib or placebo plus TACE with doxorubicin-eluting beads for intermediate stage HCC: The SPACE trial. J. Hepatol. 2016, 64, 1090–1098. Available online: https://pubmed.ncbi.nlm.nih.gov/26809111/ (accessed on 21 December 2020). [CrossRef] [Green Version]
- Liu, K.C.; Hao, Y.H.; Lv, W.F.; Jia, W.D.; Ji, C.S.; Zhou, C.Z.; Cheng, D.L.; Xu, S.B.; Gao, Z.G.; Su, M.X.; et al. Transarterial chemoembolization combined with sorafenib in patients with BCLC stage C hepatocellular carcinoma. Drug Des. Dev. Ther. 2020, 14, 3461–3468. Available online: https://pubmed.ncbi.nlm.nih.gov/32904650/ (accessed on 22 December 2020). [CrossRef] [PubMed]
- Lee, S.W.; Lee, T.Y.; Peng, Y.C.; Yang, S.S.; Yeh, H.Z.; Chang, C.S. The therapeutic benefits of combined sorafenib and transarterial chemoembolization for advanced hepatocellular carcinoma. J. Dig. Dis. 2020, 21, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.; Kedarisetty, C.K.; Venkataraman, J.; Srinivasan, V.; Deepashree, T.; Uthappa, M.C.; Ilankumaran, K.; Govil, S.; Reddy, M.S.; Rela, M. Combination of TACE and sorafenib improves outcomes in BCLC stages B/C of hepatocellular carcinoma: A single centre experience. Ann. Hepatol. 2017, 16, 247–254. Available online: https://pubmed.ncbi.nlm.nih.gov/28233748/ (accessed on 17 April 2021). [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, multicentre prospective trial of transarterial chemoembolisation (TACE) plus sorafenib as compared with TACE alone in patients with hepatocellular carcinoma: TACTICS trial. Gut 2020, 69, 1492–1501. Available online: https://pubmed.ncbi.nlm.nih.gov/31801872/ (accessed on 29 December 2020). [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Shimose, S.; Iwamoto, H.; Tanaka, M.; Niizeki, T.; Shirono, T.; Noda, Y.; Kamachi, N.; Okamura, S.; Nakano, M.; Suga, H.; et al. Alternating lenvatinib and trans-arterial therapy prolongs overall survival in patients with inter-mediate stage hepatocellular carcinoma: A propensity score matching study. Cancers 2021, 13, 160. Available online: https://pubmed.ncbi.nlm.nih.gov/33466496/ (accessed on 15 February 2021). [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Cheng, A.L.; Hsu, C.; Chan, S.L.; Choo, S.P.; Kudo, M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J. Hepatol. 2020, 72, 307–319. Available online: https://pubmed.ncbi.nlm.nih.gov/31954494/ (accessed on 15 February 2021). [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | Sorafenib/TACE (Group A) n = 54 | Sorafenib (Group B) n = 82 | TACE (Group C) n = 65 | p-Value |
|---|---|---|---|---|
| Median age (range) | 64.0 (34–77) | 65.9 (28–85) | 67.0 (41–80) | 0.13 |
| Male sex | 87% | 88% | 82% | 0.56 |
| Alcohol abuse | 31% | 28% | 38% | 0.41 |
| Viral hepatitis | 43% | 35% | 34% | 0.56 |
| NASH | 7% | 6% | 8% | 0.88 |
| Cryptogenic/other causes | 19% | 31% | 20% | 0.21 |
| BCLC stage C | 100% | 100% | 100% | 1.0 |
| Child–Pugh A | 74% | 74% | 77% | 0.94 |
| Child–Pugh B | 26% | 26% | 23% | |
| ECOG PS ≥ 1 | 70% | 55% | 62% | 0.19 |
| Tumor burden ≥50% liver involvement | 15% | 22% | 15% | 0.86 |
| Portal vein infiltration (grade 1–3) | 33% | 33% | 38% | 0.77 |
| Extrahepatic spread | 41% | 46% | 34% | 0.31 |
| α-Fetoprotein ≥400 ng/dL | 34% | 36% | 38% | 0.89 |
| CLIP score (range) | 2.1 ± 1.0 (1.0–4.0) | 2.1 ± 0.8 (1.0–4.0) | 2.1 ± 0.8 (1.0–4.0) |
| 6-Month Radiologic Evaluation (RECIST 1.1) | Sorafenib/TACE (n = 53) * | Sorafenib (n= 74) * | TACE (n= 58) * | p-Value |
|---|---|---|---|---|
| Complete response | 0 (0%) | 0 (0%) | 0 (0%) | 1.0 |
| Partial response | 8 (15%) | 2 (3%) | 5 (9%) | 0.0187 |
| Stable disease | 20 (38%) | 15 (20%) | 17 (29%) | 0.1423 |
| Progression of disease | 25 (47%) | 57 (77%) | 36 (62%) | 0.0024 |
| Disease control rate ± | 28 (53%) | 17 (23%) | 22 (38%) | 0.0024 |
| Objective response rate ¶ | 8 (15%) | 2 (3%) | 5 (9%) | 0.0187 |
| Treatment Group | mOS (Months) | 1-Year Survival Rate (%) | 2-Year Survival Rate (%) | Survival at Data Closure (%) |
|---|---|---|---|---|
| Group A: all patients liver only metastases | 16.5 | 56% | 13% | 39% |
| 16.1 | ||||
| 19.0 | ||||
| Group B: all patients liver only metastases | 8.4 | 28% | 5% | 20% |
| 8.4 | ||||
| 7.5 | ||||
| Group C: all patients liver only metastases | 10.5 | 37% | 6% | 19% |
| 10.5 | ||||
| 10.5 | ||||
| All patients | 11.0 | 38% | 7% | 24% |
| Predictor | HR | 95% CI | p-Value |
|---|---|---|---|
| Sorafenib/TACE | 0.34 | 0.23–0.53 | <0.001 |
| Child–Pugh score | 0.48 | 0.31–0.71 | <0.001 |
| ECOG PS | 0.56 | 0.37–0.83 | 0.002 |
| AFP ≥ 400 ng/mL | 1.79 | 1.25–2.5 | 0.006 |
| CLIP score 1–2 | 0.91 | 0.56–1.42 | 0.68 |
| Zhao risk score < 11.5 | 0.87 | 0.56–1.42 | 0.53 |
| Adverse events | Sorafenib/TACE (Group A) n = 50 | Sorafenib (Group B) n = 78 |
|---|---|---|
| Any adverse event | 86% | 80% |
| Adverse events ≥ grade 3 | 34% | 32% |
| Sorafenib dose reduction | 66% | 60% |
| Diarrhea | 26% | 22% |
| Hand–foot skin reaction | 24% | 17% |
| Fatigue | 6% | 8% |
| Sorafenib interruption | 38% | 35% |
| Hand–foot skin reaction | 12% | 10% |
| Diarrhea | 10% | 10% |
| Fatigue | 6% | 5% |
| Termination of sorafenib | 12% | 15% |
| Hand–foot skin reaction | 4% | 4% |
| Diarrhea | 2% | 3% |
| Fatigue | 2% | 3% |
| Adverse Events, n (%) | Sorafenib + TACE (n = 37) | TACE (n = 38) |
|---|---|---|
| Postembolization syndrome * | 11 (30%) | 13 (34%) |
| Abdominal pain | 14 (41%) | 17 (45%) |
| Nausea | 12 (33%) | 13 (34%) |
| Fever in absence of infection | 10 (27%) | 10 (26%) |
| Vomiting | 5 (14%) | 6 (16%) |
| New ascites | 9 (24%) | 8 (21%) |
| Fatigue | 8 (22%) | 5 (13%) |
| Liver dysfunction | 6 (16%) | 4 (11%) |
| Anorexia | 5 (14%) | 4 (11%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, C.; Göller, M.; Schott, E.; Waidmann, O.; op den Winkel, M.; Paprottka, P.; Zangos, S.; Vogl, T.; Bechstein, W.O.; Zeuzem, S.; et al. Combination of Sorafenib and Transarterial Chemoembolization in Selected Patients with Advanced-Stage Hepatocellular Carcinoma: A Retrospective Cohort Study at Three German Liver Centers. Cancers 2021, 13, 2121. https://doi.org/10.3390/cancers13092121
Koch C, Göller M, Schott E, Waidmann O, op den Winkel M, Paprottka P, Zangos S, Vogl T, Bechstein WO, Zeuzem S, et al. Combination of Sorafenib and Transarterial Chemoembolization in Selected Patients with Advanced-Stage Hepatocellular Carcinoma: A Retrospective Cohort Study at Three German Liver Centers. Cancers. 2021; 13(9):2121. https://doi.org/10.3390/cancers13092121
Chicago/Turabian StyleKoch, Christine, Markus Göller, Eckart Schott, Oliver Waidmann, Mark op den Winkel, Philipp Paprottka, Stephan Zangos, Thomas Vogl, Wolf Otto Bechstein, Stefan Zeuzem, and et al. 2021. "Combination of Sorafenib and Transarterial Chemoembolization in Selected Patients with Advanced-Stage Hepatocellular Carcinoma: A Retrospective Cohort Study at Three German Liver Centers" Cancers 13, no. 9: 2121. https://doi.org/10.3390/cancers13092121