
Percutaneous Hepatic Perfusion (PHP) with Melphalan in Liver-Dominant Metastatic Uveal Melanoma: The German Experience

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
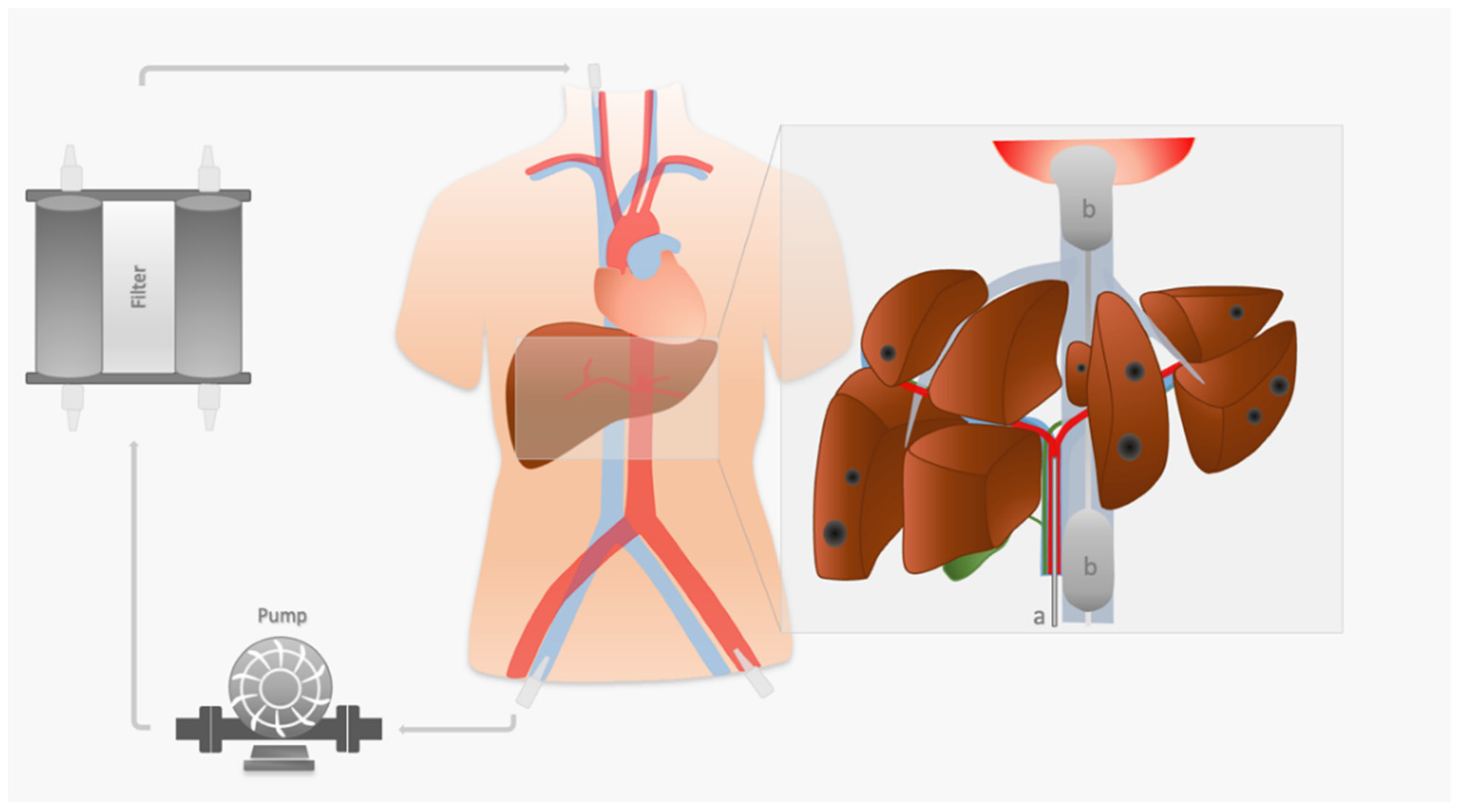
2.2. PHP Procedure
2.3. Assessment of Side Effects
2.4. Assessment of Response
2.5. Assessment of Survival
2.6. Statistical Analysis
3. Results
3.1. Patient and Interventional Data
3.2. Toxicity
3.3. Intra- and Postinterventional Complications
- One case of left cerebral artery occlusion; despite immediate thrombectomy, the patient remained with persistent neurological symptoms.
- One case of basilar artery thrombosis, most likely due to ne novo auricular fibrillations. Prompt thrombectomy and pharmaceutical cardioversion were performed. The same patient developed pulmonary embolism subsequent to deep vein thrombosis (treated with anticoagulation).
- Two minor strokes without sequelae.
- One case of central pulmonary embolism with good response to conservative treatment (anticoagulation).
3.4. Response
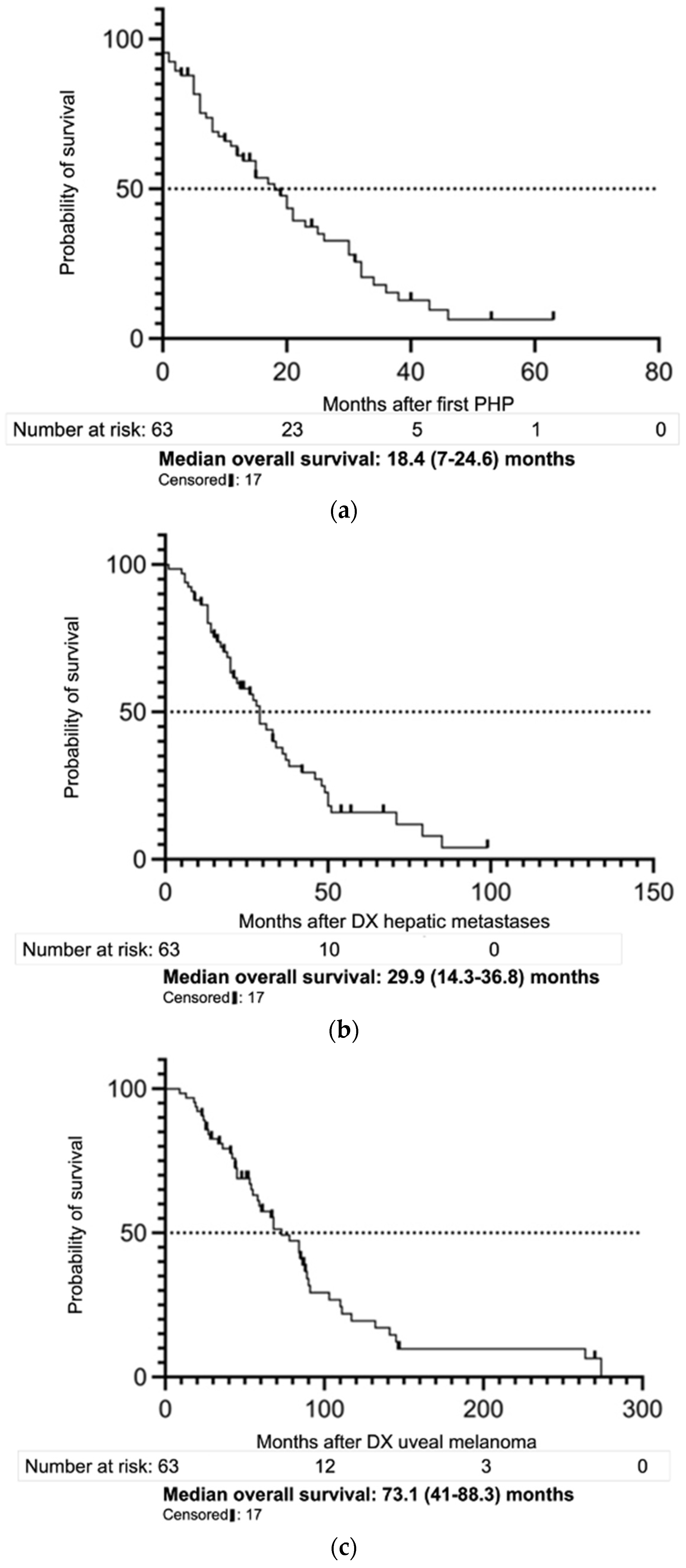
3.5. Survival
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chattopadhyay, C.; Kim, D.W.; Gombos, D.S.; Oba, J.; Qin, Y.; Williams, M.D.; Esmaeli, B.; Grimm, E.A.; Wargo, J.A.; Woodman, S.E.; et al. Uveal melanoma: From diagnosis to treatment and the science in between: Uveal Melanoma Review. Cancer 2016, 122, 2299–2312. [Google Scholar] [CrossRef]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, M.J.; Shields, C.L.; Cebulla, C.M.; Abdel-Rahman, M.H.; Grossniklaus, H.E.; Stern, M.-H.; Carvajal, R.D.; Belfort, R.N.; Jia, R.; Shields, J.A.; et al. Uveal melanoma. Nat. Rev. Dis. Primers. 2020, 6, 24. [Google Scholar] [CrossRef]
- Hughes, M.S.; Zager, J.; Faries, M.; Alexander, H.R.; Royal, R.E.; Wood, B.; Choi, J.; McCluskey, K.; Whitman, E.; Agarwala, S.; et al. Results of a Randomized Controlled Multicenter Phase III Trial of Percutaneous Hepatic Perfusion Compared with Best Available Care for Patients with Melanoma Liver Metastases. Ann. Surg. Oncol. 2016, 23, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- Damato, B. Progress in the management of patients with uveal melanoma. The 2012 Ashton Lecture. Eye 2012, 26, 1157–1172. [Google Scholar] [CrossRef] [Green Version]
- Agarwala, S.S.; Eggermont, A.M.M.; O’Day, S.; Zager, J.S. Metastatic melanoma to the liver: A contemporary and comprehensive review of surgical, systemic, and regional therapeutic options. Cancer 2014, 120, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Mariani, P.; Piperno-Neumann, S.; Servois, V.; Berry, M.G.; Dorval, T.; Plancher, C.; Couturier, J.; Levy-Gabriel, C.; Lumbroso-Le Rouic, L.; Desjardins, L.; et al. Surgical management of liver metastases from uveal melanoma: 16 years’ experience at the Institut Curie. Eur. J. Surg. Oncol. 2009, 35, 1192–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvajal, R.D.; Schwartz, G.K.; Tezel, T.; Marr, B.; Francis, J.H.; Nathan, P.D. Metastatic disease from uveal melanoma: Treatment options and future prospects. Br. J. Ophthalmol. 2017, 101, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Vidal, C.; Fernandez-Diaz, D.; Fernandez-Marta, B.; Lago-Baameiro, N.; Pardo, M.; Silva, P.; Paniagua, L.; Blanco-Teijeiro, M.J.; Piñeiro, A.; Bande, M. Treatment of Metastatic Uveal Melanoma: Systematic Review. Cancers 2020, 12, 2557. [Google Scholar] [CrossRef]
- Nathan, P.; Cohen, V.; Coupland, S.; Curtis, K.; Damato, B.; Evans, J.; Fenwick, S.; Kirkpatrick, L.; Li, O.; Marshall, E.; et al. Uveal Melanoma UK National Guidelines. Eur. J. Cancer 2015, 51, 2404–2412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, E.; Romaniuk, C.; Ghaneh, P.; Wong, H.; McKay, M.; Chopra, M.; Coupland, S.E.; Damato, B.E. MRI in the detection of hepatic metastases from high-risk uveal melanoma: A prospective study in 188 patients. Br. J. Ophthalmol. 2013, 97, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Chadha, V.; Cauchi, P.; Kincaid, W.; Schipani, S.; Waterston, A.; Cram, O.; Ritchie, D.; Salvi, S.; Nathan, P.; Blair, R. Consensus Statement on Metastatic Surveillance for Uveal Melanoma in Scotland 2019, Endorsed by National Services Division (NSD), Scotland. Available online: https://www.nhsggc.org.uk/media/256054/consensus_full_paper_final_version.pdf (accessed on 2 October 2021).
- Gonsalves, C.F.; Adamo, R.D.; Eschelman, D.J. Locoregional Therapies for the Treatment of Uveal Melanoma Hepatic Metastases. Semin Interv. Radiol. 2020, 37, 508–517. [Google Scholar] [CrossRef]
- Jovanovic, P.; Mihajlovic, M.; Djordjevic-Jocic, J.; Vlajkovic, S.; Cekic, S.; Stefanovic, V. Ocular melanoma: An overview of the current status. Int. J. Clin. Exp. Pathol. 2013, 6, 1230–1244. [Google Scholar] [PubMed]
- Diener-West, M.; Reynolds, S.; Agugliaro, D.; Caldwell, R.; Cumming, K.; Earle, J.; Hawkins, B.; Hayman, J.; Jaiyesimi, I.; Jampol, L.; et al. Development of Metastatic Disease after Enrollment in the COMS Trials for Treatment of Choroidal Melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2006, 123, 1639–1643. [Google Scholar] [CrossRef]
- Fachgesellschaften, A.D.W.M. S3—Leitlinie zur Diagnostik, Therapie und Nachsorge des Melanoms. JDDG J. Der. Dtsch. Dermatol. Ges. 2020, 18. [Google Scholar] [CrossRef]
- Khoja, L.; Atenafu, E.G.; Suciu, S.; Leyvraz, S.; Sato, T.; Marshall, E.; Keilholz, U.; Zimmer, L.; Patel, S.P.; Piperno-Neumann, S.; et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: An international rare cancers initiative (IRCI) ocular melanoma study. Ann. Oncol. 2019, 30, 1370–1380. [Google Scholar] [CrossRef]
- Abbott, A.M.; Doepker, M.P.; Kim, Y.; Perez, M.C.; Gandle, C.; Thomas, K.L.; Choi, J.; Shridhar, R.; Zager, J.S. Hepatic Progression-free and Overall Survival After Regional Therapy to the Liver for Metastatic Melanoma. Am. J. Clin. Oncol. 2018, 41, 747–753. [Google Scholar] [CrossRef]
- Karydis, I.; Gangi, A.; Wheater, M.J.; Choi, J.; Wilson, I.; Thomas, K.; Pearce, N.; Takhar, A.; Gupta, S.; Hardman, D.; et al. Percutaneous hepatic perfusion with melphalan in uveal melanoma: A safe and effective treatment modality in an orphan disease. J. Surg. Oncol. 2018, 117, 1170–1178. [Google Scholar] [CrossRef] [Green Version]
- Schönfeld, L.; Hinrichs, J.B.; Marquardt, S.; Voigtländer, T.; Dewald, C.; Koppert, W.; Manns, M.P.; Wacker, F.; Vogel, A.; Kirstein, M.M. Chemosaturation with percutaneous hepatic perfusion is effective in patients with ocular melanoma and cholangiocarcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 3003–3012. [Google Scholar] [CrossRef]
- Vogel, A.; Gupta, S.; Zeile, M.; von Haken, R.; Brüning, R.; Lotz, G.; Vahrmeijer, A.; Vogl, T.; Wacker, F. Chemosaturation Percutaneous Hepatic Perfusion: A Systematic Review. Adv. Ther. 2016, 33, 2122–2138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijer, T.S.; Burgmans, M.C.; Fiocco, M.; de Geus-Oei, L.-F.; Kapiteijn, E.; de Leede, E.M.; Martini, C.H.; van der Meer, R.W.; Tijl, F.G.J.; Vahrmeijer, A.L. Safety of Percutaneous Hepatic Perfusion with Melphalan in Patients with Unresectable Liver Metastases from Ocular Melanoma Using the Delcath Systems’ Second-Generation Hemofiltration System: A Prospective Non-randomized Phase II Trial. Cardiovasc. Interv. Radiol. 2019, 42, 841–852. [Google Scholar] [CrossRef] [Green Version]
- Dewald, C.L.A.; Meine, T.C.; Winther, H.M.B.; Kloeckner, R.; Maschke, S.K.; Kirstein, M.M.; Vogel, A.; Wacker, F.K.; Meyer, B.C.; Renne, J.; et al. Chemosaturation Percutaneous Hepatic Perfusion (CS-PHP) with Melphalan: Evaluation of 2D-Perfusion Angiography (2D-PA) for Leakage Detection of the Venous Double-Balloon Catheter. Cardiovasc. Interv. Radiol. 2019, 42, 1441–1448. [Google Scholar] [CrossRef] [PubMed]
- Moeslein, F.M.; McAndrew, E.G.; Appling, W.M.; Hryniewich, N.E.; Jarvis, K.D.; Markos, S.M.; Sheets, T.P.; Uzgare, R.P.; Johnston, D.S. Evaluation of Delcath Systems’ Generation 2 (GEN 2) Melphalan Hemofiltration System in a Porcine Model of Percutaneous Hepatic Perfusion. Cardiovasc. Interv. Radiol. 2014, 37, 763–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Struck, M.F.; Kliem, P.; Ebel, S.; Bauer, A.; Gössmann, H.; Veelken, R.; van Bömmel, F.; Dennecke, T.; Stehr, S.N.; Girrbach, F.F. Percutaneous hepatic melphalan perfusion: Single center experience of procedural characteristics, hemodynamic response, complications, and postoperative recovery. PLoS ONE 2021, 16, e0254817. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brüning, R.; Tiede, M.; Schneider, M.; Wohlmuth, P.; Weilert, H.; Oldhafer, K.; Stang, A. Unresectable Hepatic Metastasis of Uveal Melanoma: Hepatic Chemosaturation with High-Dose Melphalan—Long-Term Overall Survival Negatively Correlates with Tumor Burden. Radiol. Res. Pr. 2020, 2020, 5672048. [Google Scholar] [CrossRef] [PubMed]
- Dewald, C.L.A.; Hinrichs, J.B.; Becker, L.S.; Maschke, S.; Meine, T.C.; Saborowski, A.; Schönfeld, L.J.; Vogel, A.; Kirstein, M.M.; Wacker, F.K. Chemosaturation with Percutaneous Hepatic Perfusion: Outcome and Safety in Patients with Metastasized Uveal Melanoma. Rofo 2021, 193, 928–936. [Google Scholar] [CrossRef]
- Steeb, T.; Hayani, K.M.; Förster, P.; Liegl, R.; Toussaint, F.; Schlaak, M.; Berking, C.; Heppt, M.V. Guidelines for uveal melanoma: A critical appraisal of systematically identified guidelines using the AGREE II and AGREE-REX instrument. J. Cancer Res. Clin. Oncol 2020, 146, 1079–1088. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Manson, D.K.; Marr, B.P.; Carvajal, R.D. Treatment of uveal melanoma: Where are we now? Adv. Med. Oncol. 2018, 10, 175883401875717. [Google Scholar] [CrossRef]
- Rantala, E.S.; Hernberg, M.; Kivelä, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef]
- Nathan, P.; Hassel, J.C.; Rutkowski, P.; Baurain, J.-F.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. N. Engl. J. Med. 2021, 385, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Wessely, A.; Steeb, T.; Erdmann, M.; Heinzerling, L.; Vera, J.; Schlaak, M.; Berking, C.; Heppt, M.V. The Role of Immune Checkpoint Blockade in Uveal Melanoma. Int. J. Mol. Sci. 2020, 21, 879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triozzi, P.L.; Singh, A.D. Adjuvant Therapy of Uveal Melanoma: Current Status. Ocul. Oncol. Pathol. 2015, 1, 54–62. [Google Scholar] [CrossRef] [Green Version]
- Carr, M.J.; Sun, J.; Cohen, J.B.; Liu, J.; Serdiuk, A.A.; Stewart, S.R.; Doobay, N.; Duclos, A.; Seal, D.A.; Choi, J.; et al. Over 12 Years Single Institutional Experience Performing Percutaneous Hepatic Perfusion for Unresectable Liver Metastases. Cancer Control. 2020, 27, 1073274820983019. [Google Scholar] [CrossRef] [PubMed]
- Zager, J.S.; Orloff, M.; Ferrucci, P.F.; Glazer, E.S.; Ejaz, A.; Richtig, E.; Ochsenreither, S.; Lowe, M.C.; Reddy, S.A.; Beasley, G.; et al. Percutaneous hepatic perfusion (PHP) with melphalan for patients with ocular melanoma liver metastases: Preliminary results of FOCUS (PHP-OCM-301/301A) phase III trial. J. Clin. Oncol. 2021, 39, 9510. [Google Scholar] [CrossRef]
- Artzner, C.; Mossakowski, O.; Hefferman, G.; Grosse, U.; Hoffmann, R.; Forschner, A.; Eigentler, T.; Syha, R.; Grözinger, G. Chemosaturation with percutaneous hepatic perfusion of melphalan for liver-dominant metastatic uveal melanoma: A single center experience. Cancer Imaging 2019, 19, 31. [Google Scholar] [CrossRef] [Green Version]
- Estler, A.; Artzner, C.; Bitzer, M.; Nikolaou, K.; Hoffmann, R.; Hepp, T.; Hagen, F.; Eigentler, T.; Forschner, A.; Grözinger, G. Efficacy and tolerability of chemosaturation in patients with hepatic metastases from uveal melanoma. Acta Radiol. 2021, 1–9. [Google Scholar] [CrossRef]
- Xing, M.; Prajapati, H.J.; Dhanasekaran, R.; Lawson, D.H.; Kokabi, N.; Eaton, B.R.; Kim, H.S. Selective Internal Yttrium-90 Radioembolization Therapy (90Y-SIRT) Versus Best Supportive Care in Patients with Unresectable Metastatic Melanoma to the Liver Refractory to Systemic Therapy: Safety and Efficacy Cohort Study. Am. J. Clin. Oncol. 2017, 40, 27–34. [Google Scholar] [CrossRef]
- Gupta, S.; Bedikian, A.Y.; Ahrar, J.; Ensor, J.; Ahrar, K.; Madoff, D.C.; Wallace, M.J.; Murthy, R.; Tam, A.; Hwu, P. Hepatic Artery Chemoembolization in Patients with Ocular Melanoma Metastatic to the Liver: Response, Survival, and Prognostic Factors. Am. J. Clin. Oncol. 2010, 33, 474–480. [Google Scholar] [CrossRef]
- Heppt, M.V.; Heinzerling, L.; Kähler, K.C.; Forschner, A.; Kirchberger, M.C.; Loquai, C.; Meissner, M.; Meier, F.; Terheyden, P.; Schell, B.; et al. Prognostic factors and outcomes in metastatic uveal melanoma treated with programmed cell death-1 or combined PD-1/cytotoxic T-lymphocyte antigen-4 inhibition. Eur. J. Cancer 2017, 82, 56–65. [Google Scholar] [CrossRef]
- Heppt, M.V.; Amaral, T.; Kähler, K.C.; Heinzerling, L.; Hassel, J.C.; Meissner, M.; Kreuzberg, N.; Loquai, C.; Reinhardt, L.; Utikal, J.; et al. Combined immune checkpoint blockade for metastatic uveal melanoma: A retrospective, multi-center study. J. Immunother. Cancer 2019, 7, 299. [Google Scholar] [CrossRef] [PubMed]
- Piulats, J.M.; Espinosa, E.; de la Cruz Merino, L.; Varela, M.; Alonso Carrión, L.; Martín-Algarra, S.; López Castro, R.; Curiel, T.; Rodríguez-Abreu, D.; Redrado, M.; et al. Nivolumab Plus Ipilimumab for Treatment-Naïve Metastatic Uveal Melanoma: An Open-Label, Multicenter, Phase II Trial by the Spanish Multidisciplinary Melanoma Group (GEM-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef]
- Kirstein, M.M.; Marquardt, S.; Jedicke, N.; Marhenke, S.; Koppert, W.; Manns, M.P.; Wacker, F.; Vogel, A. Safety and efficacy of chemosaturation in patients with primary and secondary liver tumors. J. Cancer Res. Clin. Oncol. 2017, 143, 2113–2121. [Google Scholar] [CrossRef]
- Barker, C.A.; Salama, A.K. New NCCN Guidelines for Uveal Melanoma and Treatment of Recurrent or Progressive Distant Metastatic Melanoma. J. Natl. Compr. Canc. Netw. 2018, 16, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Dewald, C.L.A.; Becker, L.S.; Maschke, S.K.; Meine, T.C.; Alten, T.A.; Kirstein, M.M.; Vogel, A.; Wacker, F.K.; Meyer, B.C.; Hinrichs, J.B. Percutaneous isolated hepatic perfusion (chemosaturation) with melphalan following right hemihepatectomy in patients with cholangiocarcinoma and metastatic uveal melanoma: Peri- and post-interventional adverse events and therapy response compared to a matched group without prior liver surgery. Clin. Exp. Metastasis 2020, 37, 683–692. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | % |
|---|---|---|
| Male | 30 | 45 |
| Female | 36 | 55 |
| Age (years) 1 | 58 (51–67) | |
| Tumor load (%) prior to PHP 1,2 | 5 (1–12) | |
| Tumor mass (cm3) prior to PHP 1,2 | 70 (21–276) | |
| LDH prior to PHP 1 (U/L) | 284 (212–438) | |
| Previous local liver therapy | 25 | 38 |
| Previous systemic therapy | 12 | 18 |
| PHP as 1st therapy line | 34 | 52 |
| PHP as 2nd therapy line | 17 | 26 |
| PHP as 3rd and 4th therapy line | 15 | 23 |
| Parameter | Median | IQR |
|---|---|---|
| Melphalan dose (mg) | 182 | 153–207 |
| Intervention time (min) | 185 | 174–229 |
| Number of PHP per patient | 2 | 1–3 |
| AEs after 1st PHP n = 66 | AEs after Any PHP % per Patient n = 66 | AEs after Any PHP % per PHP n = 145 | |
|---|---|---|---|
| Thrombopenia | |||
| Grade 3 | 10 (15.2%) | 27 (40.9%) | 27 (18.6%) |
| Grade 4 | 5 (7.6%) | 9 (13.6%) | 9 (6.2%) |
| Grade 3 + 4 | 15 (22.7%) | 36 (54.5%) | 36 (24.8%) |
| Leucopenia | |||
| Grade 3 | 0 (0%) | 1 (1.5%) | 1 (0.7%) |
| Grade 4 | 4 (6.1%) | 5 (7.6%) | 5 (3.5%) |
| Grade 3 + 4 | 4 (6.1%) | 6 (9.1%) | 6 (4.1%) |
| Anemia | |||
| Grade 3 | 7 (10.6%) | 17 (25.8%) | 17 (11.7%) |
| Grade 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Grade 3 + 4 | 7 (10.6%) | 17 (25.8%) | 17 (11.7%) |
| AST increase | |||
| Grade 3 | 6 (9.1%) | 9 (13.6%) | 9 (6.2%) |
| Grade 4 | 1 (1.5%) | 2 (3%) | 2 (1.4%) |
| Grade 3 + 4 | 7 (10.6%) | 11 (16.7%) | 11 (7.6%) |
| ALT increase | |||
| Grade 3 | 4 (6.1%) | 8 (12.1%) | 8 (5.5%) |
| Grade 4 | 0 (0%) | 2 (3%) | 2 (1.4%) |
| Grade 3 + 4 | 4 (6.1%) | 10 (15.2%) | 10 (6.9%) |
| Hyperbilirubinemia | |||
| Grade 3 | 3 (4.5%) | 5 (7.6%) | 5 (3.5%) |
| Grade 4 | 0 (0%) | 1 (1.5%) | 1 (0.7%) |
| Grade 3 + 4 | 3 (4.5%) | 6 (9.1%) | 6 (4.1%) |
| Hypoalbuminemia | |||
| Grade 3 | 2 (3%) | 6 (9.1%) | 6 (4.1%) |
| Grade 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Grade 3 + 4 | 2 (3%) | 6 (9.1%) | 6 (4.1%) |
| Complication (Treatment) | n = | % |
|---|---|---|
| Active bleeding at puncture site with subsequent hemorrhagic shock (surgery) | 1 | 0.7 |
| Ulcer bleeding (surgical care) | 1 | 0.7 |
| NSTEMI (PTCA) 1 | 1 | 0.7 |
| Tumor lysis syndrome | 1 | 0.7 |
| Acute kidney failure | 1 | 0.7 |
| Sepsis | 1 | 0.7 |
| Tachyarrhythmia absoluta | 1 | 0.7 |
| Variable | β | S.E. | Wald Z | Pr (>|Z|) | Difference | Odds Ratio | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|---|---|---|---|
| Number of therapy lines prior to PHP | 0.6707 | 0.2799 | 2.40 | 0.0166 | 1 | 1.956 | 1.130 | 3.385 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dewald, C.L.A.; Warnke, M.-M.; Brüning, R.; Schneider, M.A.; Wohlmuth, P.; Hinrichs, J.B.; Saborowski, A.; Vogel, A.; Wacker, F.K. Percutaneous Hepatic Perfusion (PHP) with Melphalan in Liver-Dominant Metastatic Uveal Melanoma: The German Experience. Cancers 2022, 14, 118. https://doi.org/10.3390/cancers14010118
Dewald CLA, Warnke M-M, Brüning R, Schneider MA, Wohlmuth P, Hinrichs JB, Saborowski A, Vogel A, Wacker FK. Percutaneous Hepatic Perfusion (PHP) with Melphalan in Liver-Dominant Metastatic Uveal Melanoma: The German Experience. Cancers. 2022; 14(1):118. https://doi.org/10.3390/cancers14010118
Chicago/Turabian StyleDewald, Cornelia L. A., Mia-Maria Warnke, Roland Brüning, Martin A. Schneider, Peter Wohlmuth, Jan B. Hinrichs, Anna Saborowski, Arndt Vogel, and Frank K. Wacker. 2022. "Percutaneous Hepatic Perfusion (PHP) with Melphalan in Liver-Dominant Metastatic Uveal Melanoma: The German Experience" Cancers 14, no. 1: 118. https://doi.org/10.3390/cancers14010118