
Prognostic Factors of Pulmonary Metastasectomy for Soft Tissue Sarcomas Arising in the Trunk Wall and Extremities

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
3.2. Surgical Information and Perioperative Complications
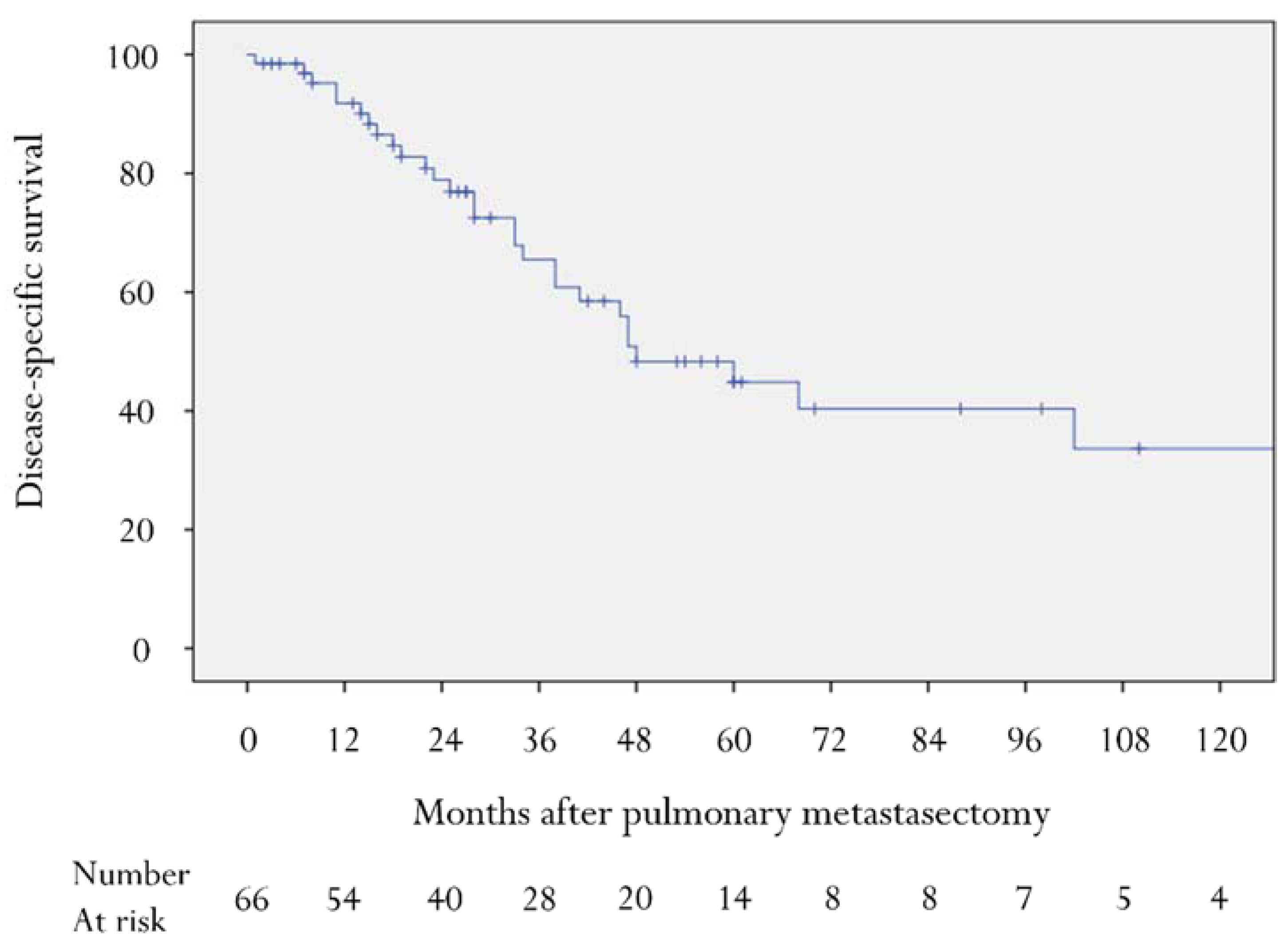
3.3. Disease-Specific Survival and Prognostic Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chudgar, N.P.; Brennan, M.F.; Munhoz, R.R.; Bucciarelli, P.R.; Tan, K.S.; D’Angelo, S.P.; Bains, M.S.; Bott, M.; Huang, J.; Park, B.J.; et al. Pulmonary metastasectomy with therapeutic intent for soft-tissue sarcoma. J. Thorac. Cardiovasc. Surg. 2017, 154, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billingsley, K.G.; Burt, M.E.; Jara, E.; Ginsberg, R.J.; Woodruff, J.M.; Leung, D.H.; Brennan, M.F. Pulmonary metastases from soft tissue sarcoma: Analysis of patterns of diseases and postmetastasis survival. Ann. Surg. 1999, 229, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Gadd, M.A.; Casper, E.S.; Woodruff, J.M.; McCormack, P.M.; Brennan, M.F. Development and treatment of pulmonary metastases in adult patients with extremity soft tissue sarcoma. Ann. Surg. 1993, 218, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Rehders, A.; Hosch, S.B.; Scheunemann, P.; Stoecklein, N.H.; Knoefel, W.T.; Peiper, M. Benefit of surgical treatment of lung metastasis in soft tissue sarcoma. Arch Surg. 2007, 142, 70–75. [Google Scholar] [CrossRef] [Green Version]
- Treasure, T.; Fiorentino, F.; Scarci, M.; Møller, H.; Utley, M. Pulmonary metastasectomy for sarcoma: A systematic review of reported outcomes in the context of Thames Cancer Registry data. BMJ Open 2012, 2, e001736. [Google Scholar] [CrossRef]
- Stamenovic, D.; Hohenberger, P.; Roessner, E. Pulmonary metastasectomy in soft tissue sarcomas: A systematic review. J. Thorac. Dis. 2021, 13, 2649–2660. [Google Scholar] [CrossRef]
- García Franco, C.E.; Algarra, S.M.; Ezcurra, A.T.; Guillén-Grima, F.; San-Julián, M.; Mindán, J.P.; Buxalleu, W.T. Long-term results after resection for soft tissue sarcoma pulmonary metastases. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.; Pak, Y.; Kraybill, W.; Kane, J.M., 3rd. Factors associated with actual long-term survival following soft tissue sarcoma pulmonary metastasectomy. Eur. J. Surg. Oncol. 2009, 35, 356–361. [Google Scholar] [CrossRef]
- Schur, S.; Hoetzenecker, K.; Lamm, W.; Koestler, W.J.; Lang, G.; Amann, G.; Funovics, P.; Nemecek, E.; Noebauer, I.; Windhager, R.; et al. Pulmonary metastasectomy for soft tissue sarcoma--report from a dual institution experience at the Medical University of Vienna. Eur. J. Cancer 2014, 50, 2289–2297. [Google Scholar] [CrossRef]
- Sardenberg, R.A.; Figueiredo, L.P.; Haddad, F.J.; Gross, J.L.; Younes, R.N. Pulmonary metastasectomy from soft tissue sarcomas. Clinics 2010, 65, 871–876. [Google Scholar] [CrossRef] [Green Version]
- Predina, J.D.; Puc, M.M.; Bergey, M.R.; Sonnad, S.S.; Kucharczuk, J.C.; Staddon, A.; Kaiser, L.R.; Shrager, J.B. Improved survival after pulmonary metastasectomy for soft tissue sarcoma. J. Thorac. Oncol. 2011, 6, 913–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toussi, M.S.; Bagheri, R.; Dayani, M.; Anvari, K.; Sheibani, S. Pulmonary metastasectomy and repeat metastasectomy for soft-tissue sarcoma. Asian Cardiovasc. Thorac. Ann. 2013, 21, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Kanzaki, R.; Kanou, T.; Ose, N.; Funaki, S.; Shintani, Y.; Minami, M.; Outani, H.; Takenaka, S.; Hamada, K.; et al. Long-term outcomes and prognostic factors of pulmonary metastasectomy for osteosarcoma and soft tissue sarcoma. Int. J. Clin. Oncol. 2019, 24, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Choong, P.F.; Pritchard, D.J.; Rock, M.G.; Sim, F.H.; Frassica, F.J. Survival after pulmonary metastasectomy in soft tissue sarcoma. Prognostic factors in 214 patients. Acta Orthop. Scand. 1995, 66, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Kawai, A.; Fukuma, H.; Beppu, Y.; Yokoyama, R.; Tsuchiya, R.; Kondo, H.; Inoue, H. Pulmonary resection for metastatic soft tissue sarcomas. Clin. Orthop. Relat. Res. 1995, 310, 188–193. [Google Scholar] [CrossRef]
- Lee, R.M.; Ethun, C.G.; Gamboa, A.C.; Turgeon, M.K.; Tran, T.; Poultsides, G.; Grignol, V.; Bedi, M.; Mogal, H.; Clarke, C.N. A novel preoperative risk score to guide patient selection for resection of soft tissue sarcoma lung metastases: An analysis from the United States Sarcoma Collaborative. J. Surg. Oncol. 2021, 124, 1477–1484. [Google Scholar] [CrossRef]
- Giuliano, K.; Sachs, T.; Montgomery, E.; Guzzetta, A.; Brock, M.; Pawlik, T.M.; Yang, S.C.; Ahuja, N. Survival Following Lung Metastasectomy in Soft Tissue Sarcomas. Thorac. Cardiovasc. Surg. 2016, 64, 150–158. [Google Scholar] [CrossRef]
- Nevala, R.; Jäämaa, S.; Tukiainen, E.; Tarkkanen, M.; Räsänen, J.; Blomqvist, C.; Sampo, M. Long-term results of surgical resection of lung metastases from soft tissue sarcoma: A single center experience. J. Surg. Oncol. 2019, 120, 168–175. [Google Scholar] [CrossRef]
- Kawamoto, T.; Hara, H.; Morishita, M.; Fukase, N.; Kawakami, Y.; Takemori, T.; Fujiwara, S.; Kitayama, K.; Yahiro, S.; Miyamoto, T.; et al. Prognostic influence of the treatment approach for pulmonary metastasis in patients with soft tissue sarcoma. Clin. Exp. Metastasis 2020, 37, 509–517. [Google Scholar] [CrossRef]
- Ohnstad, H.O.; Bruland, O.S.; Taksdal, I.; Bjerkehagen, B.; Nenadovic, M.; Sæter, G.; Jørgensen, L.H.; Hall, K.S. Response to preoperative chemotherapy in patients undergoing resection of pulmonary metastasis from soft tissue sarcoma—A predictor of outcome? Acta Oncol. 2014, 53, 1180–1187. [Google Scholar] [CrossRef] [Green Version]
- Wigge, S.; Heißner, K.; Steger, V.; Ladurner, R.; Traub, F.; Sipos, B.; Bösmüller, H.; Kanz, L.; Mayer, F.; Kopp, H.G. Impact of surgery in patients with metastatic soft tissue sarcoma: A monocentric retrospective analysis. J. Surg. Oncol. 2018, 118, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours of Soft Tissue and Bone, 5th ed.; IARC Press: Lyon, France, 2020. [Google Scholar]
- Kawai, A.; Araki, N.; Naito, Y.; Ozaki, T.; Sugiura, H.; Yazawa, Y.; Morioka, H.; Matsumine, A.; Saito, K.; Asami, S.; et al. Phase 2 study of eribulin in patients with previously treated advanced or metastatic soft tissue sarcoma. Jpn. J. Clin. Oncol. 2017, 47, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tawbi, H.A.; Burgess, M.; Bolejack, V.; Van Tine, B.A.; Schuetze, S.M.; Hu, J.; D’Angelo, S.; Attia, S.; Riedel, R.F.; Priebat, D.A.; et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): A multicentre, two-cohort, single-arm, open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1493–1501. [Google Scholar] [CrossRef]
- Thomford, N.R.; Woolner, L.B.; Clagett, O.T. The surgical treatment of metastatic tumors in the lungs. J. Thorac. Cardiovasc. Surg. 1965, 49, 357–363. [Google Scholar] [CrossRef]
- Asamura, H. Minimally invasive open surgery approach for the surgical resection of thoracic malignancies. Thorac. Surg. Clin. 2008, 18, 269–273, vi. [Google Scholar] [CrossRef]
- Clavien, P.A.; Sanabria, J.R.; Strasberg, S.M. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar] [PubMed]
- Puri, A.; Gulia, A.; Hawaldar, R.; Ranganathan, P.; Badwe, R.A. Does intensity of surveillance affect survival after surgery for sarcomas? Results of a randomized noninferiority trial. Clin. Orthop. Relat. Res. 2014, 472, 1568–1575. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Akiyama, T.; Fukushima, T.; Iwata, S.; Tsuda, Y.; Takeshita, K.; Kawai, A.; Tanaka, S.; Kobayashi, H. Prognostic factors and impact of surgery in patients with metastatic soft tissue sarcoma at diagnosis: A population-based cohort study. Jpn. J. Clin. Oncol. 2021, 51, 918–926. [Google Scholar] [CrossRef]
- Kim, S.; Ott, H.C.; Wright, C.D.; Wain, J.C.; Morse, C.; Gaissert, H.A.; Donahue, D.M.; Mathisen, D.J.; Lanuti, M. Pulmonary resection of metastatic sarcoma: Prognostic factors associated with improved outcomes. Ann. Thorac. Surg. 2011, 92, 1780–1786. [Google Scholar] [CrossRef]
- Blackmon, S.H.; Shah, N.; Roth, J.A.; Correa, A.M.; Vaporciyan, A.A.; Rice, D.C.; Hofstetter, W.; Walsh, G.L.; Benjamin, R.; Pollock, R.; et al. Resection of pulmonary and extrapulmonary sarcomatous metastases is associated with long-term survival. Ann. Thorac. Surg. 2009, 88, 877–884. [Google Scholar] [CrossRef]
- Shimizu, J.; Emori, M.; Murahashi, Y.; Sonoda, T.; Mishina, T.; Miyajima, M.; Watanabe, A.; Sugita, S.; Takada, K.; Murase, K.; et al. Pulmonary metastasectomy is associated with prolonged survival among patients with bone and soft tissue sarcoma. Mol Clin. Oncol. 2020, 12, 429–434. [Google Scholar] [PubMed]
- Hirbe, A.C.; Jennings, J.; Saad, N.; Giardina, J.D.; Tao, Y.; Luo, J.; Berry, S.; Toeniskoetter, J.; Van Tine, B.A. A Phase II Study of Tumor Ablation in Patients with Metastatic Sarcoma Stable on Chemotherapy. Oncologist 2018, 23, 760-e76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesser, T.G. Laser application enables awake thoracoscopic resection of pulmonary nodules with minimal access. Surg. Endosc. 2012, 26, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Young, R.J.; Litière, S.; Lia, M.; Hogendoorn, P.; Fisher, C.; Mechtersheimer, G.; Daugaard, S.; Sciot, R.; Collin, F.; Messiou, C.; et al. Predictive and prognostic factors associated with soft tissue sarcoma response to chemotherapy: A subgroup analysis of the European Organisation for Research and Treatment of Cancer 62012 study. Acta Oncol. 2017, 56, 1013–1020. [Google Scholar]


{kind=link}
| Variable | Patients (n = 66) (%) |
|---|---|
| Age (years, median/range) | 49 (17–82) |
| Sex | |
| Male | 38 (58) |
| Female | 28 (42) |
| Disease-free interval (months, median/range) | 17 (0–105) |
| Primary histology | |
| Synovial sarcoma | 16 (24) |
| Undifferentiated pleomorphic sarcoma | 10 (15) |
| Liposarcoma | 10 (15) |
| Dedifferentiated liposarcoma | 5 (8) |
| Pleomorphic liposarcoma | 3 (5) |
| Myxoid liposarcoma | 2 (3) |
| Myxofibrosarcoma | 7 (11) |
| Leiomyosarcoma | 6 (9) |
| Dermatofibrosarcoma protuberans | 5 (8) |
| Ewing sarcoma | 3 (5) |
| CIC-rearranged sarcoma | 2 (3) |
| Malignant peripheral nerve sheath tumor | 2 (3) |
| Sarcoma with BCOR genetic alternations | 1 (2) |
| Epithelioid sarcoma | 1 (2) |
| Extraskeletal osteosarcoma | 1 (2) |
| Alveolar soft part sarcoma | 1 (2) |
| Angiosarcoma | 1 (2) |
| Primary site | |
| Trunk wall | 34 (52) |
| Extremities | 32 (48) |
| Distribution of lung metastasis | |
| Unilateral | 58 (88) |
| Bilateral | 8 (12) |
| Number of lung metastasis (median/range) | 1 (1–12) |
| Solitary | 39 (59) |
| Multiple | 27 (41) |
| Size of largest lung lesion (mm, median/range) | 15 (1–60) |
| Type of pulmonary resection | |
| Wide wedge resection | 54 (82) |
| Segmentectomy | 7 (11) |
| Lobectomy | 5 (8) |
| Curative resection | |
| R0 | 63 (96) |
| R1 | 0 (0) |
| R2 | 3 (5) |
| Chemotherapy | |
| None | 45 (68) |
| Preoperative | 20 (30) |
| Postoperative | 4 (6) |
| Both | 3 (5) |
| Variable | n | 5-Year Survival (%) | p |
|---|---|---|---|
| Age (years) | |||
| <50 | 35 | 50 | 0.23 |
| ≥50 | 31 | 37 | |
| Sex | |||
| Male | 38 | 53 | 0.75 |
| Female | 28 | 28 | |
| Disease-free interval | |||
| <12 months | 22 | 23 | 0.001 |
| ≥12 months | 44 | 55 | |
| Primary histology | |||
| SS | 16 | 36 | 0.765 |
| Non-SS | 50 | 50 | |
| UPS | 10 | 0 | 0.001 |
| Non-UPS | 56 | 51 | |
| Liposarcoma | 10 | 57 | 0.95 |
| Non-liposarcoma | 56 | 44 | |
| MFS | 7 | 50 | 0.729 |
| Non-MFS | 59 | 44 | |
| Leiomyosarcoma | 6 | 38 | 0.369 |
| Non-leiomyosarcoma | 60 | 45 | |
| Primary site | |||
| Trunk wall | 34 | 47 | 0.40 |
| Extremities | 32 | 44 | |
| Size of primary lesion | |||
| <10 cm | 42 | 47 | 0.49 |
| ≥10 cm | 24 | 48 | |
| Distribution of lung metastasis | |||
| Unilateral | 58 | 44 | 0.536 |
| Bilateral | 8 | 50 | |
| Number of lung metastases | |||
| Solitary | 39 | 59 | 0.047 |
| Multiple | 27 | 27 | |
| Size of largest lung lesion | |||
| <20 mm | 48 | 57 | <0.001 |
| ≥20 mm | 18 | 10 | |
| Type of pulmonary resection | |||
| Partial | 44 | 51 | 0.113 |
| Anatomical | 12 | 21 | |
| Curative resection | |||
| Yes | 63 | 46 | <0.001 |
| No | 3 | 0 | |
| Preoperative chemotherapy | |||
| Yes | 20 | 24 | 0.051 |
| No | 46 | 54 | |
| Postoperative chemotherapy | |||
| Yes | 4 | 25 | 0.315 |
| No | 62 | 46 |
| Variable | HR | 95% CI | p |
|---|---|---|---|
| Disease-free interval (<12 months) | 3.544 | 1.422–8.832 | 0.007 |
| UPS | 2.882 | 0.858–9.684 | 0.087 |
| Number of lung metastasis (multiple) | 1.195 | 0.496–2.877 | 0.691 |
| Size of largest lung lesion (≥20 mm) | 3.159 | 1.117–8.930 | 0.03 |
| Non-curative resection | 12.161 | 2.011–74.817 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, S.; Kobayashi, E.; Nishio, J.; Toda, Y.; Yotsukura, M.; Watanabe, S.-I.; Yamamoto, T.; Kawai, A. Prognostic Factors of Pulmonary Metastasectomy for Soft Tissue Sarcomas Arising in the Trunk Wall and Extremities. Cancers 2022, 14, 3329. https://doi.org/10.3390/cancers14143329
Nakayama S, Kobayashi E, Nishio J, Toda Y, Yotsukura M, Watanabe S-I, Yamamoto T, Kawai A. Prognostic Factors of Pulmonary Metastasectomy for Soft Tissue Sarcomas Arising in the Trunk Wall and Extremities. Cancers. 2022; 14(14):3329. https://doi.org/10.3390/cancers14143329
Chicago/Turabian StyleNakayama, Shizuhide, Eisuke Kobayashi, Jun Nishio, Yu Toda, Masaya Yotsukura, Shun-Ichi Watanabe, Takuaki Yamamoto, and Akira Kawai. 2022. "Prognostic Factors of Pulmonary Metastasectomy for Soft Tissue Sarcomas Arising in the Trunk Wall and Extremities" Cancers 14, no. 14: 3329. https://doi.org/10.3390/cancers14143329