
Treatment Costs of Colorectal Cancer by Sex and Age: Population-Based Study on Health Insurance Data from Germany

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Study Population
- Subjects newly diagnosed with CRC;
- Subjects who died of CRC.
2.3. Analysis of Cost Positions
3. Results
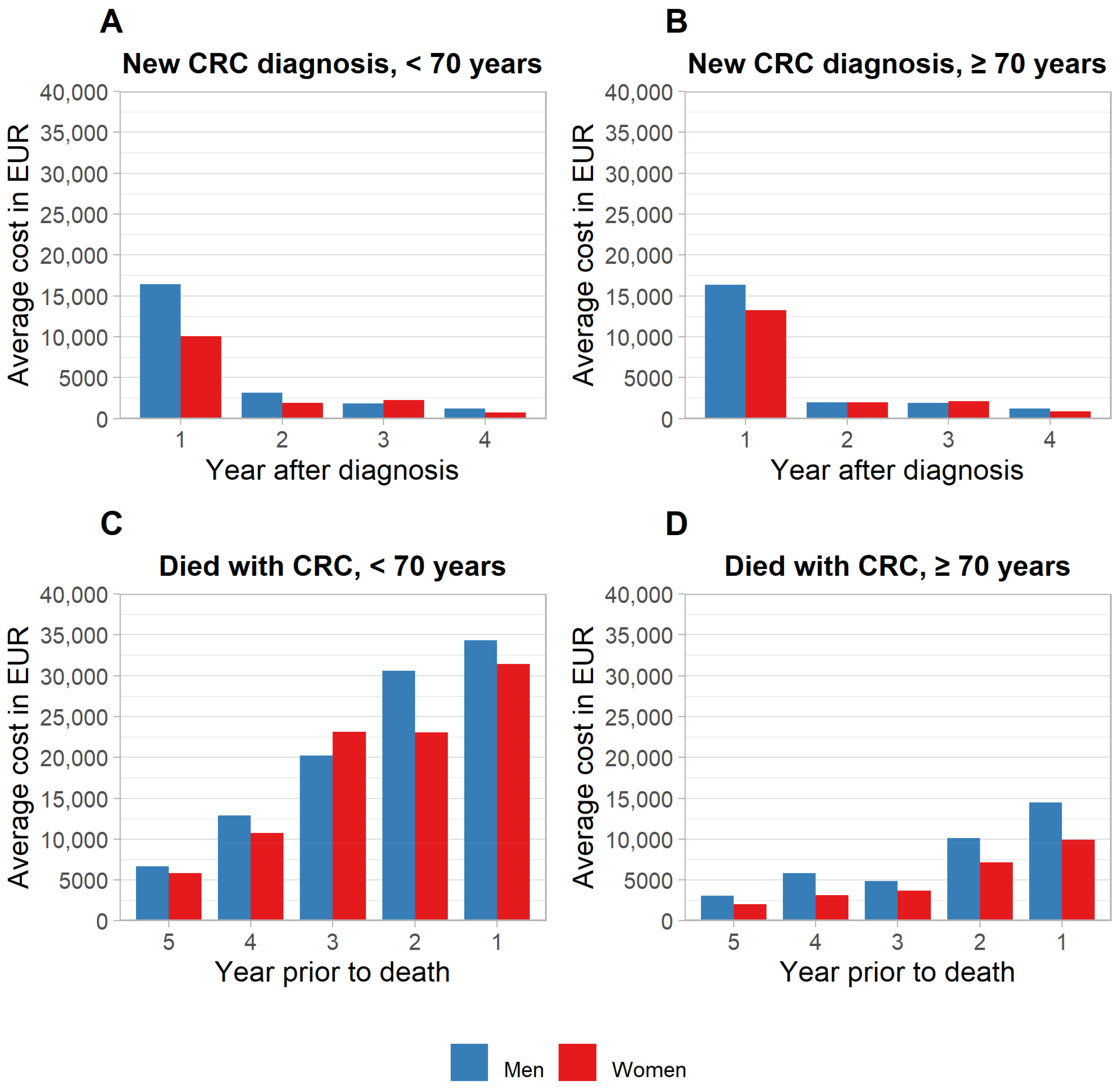
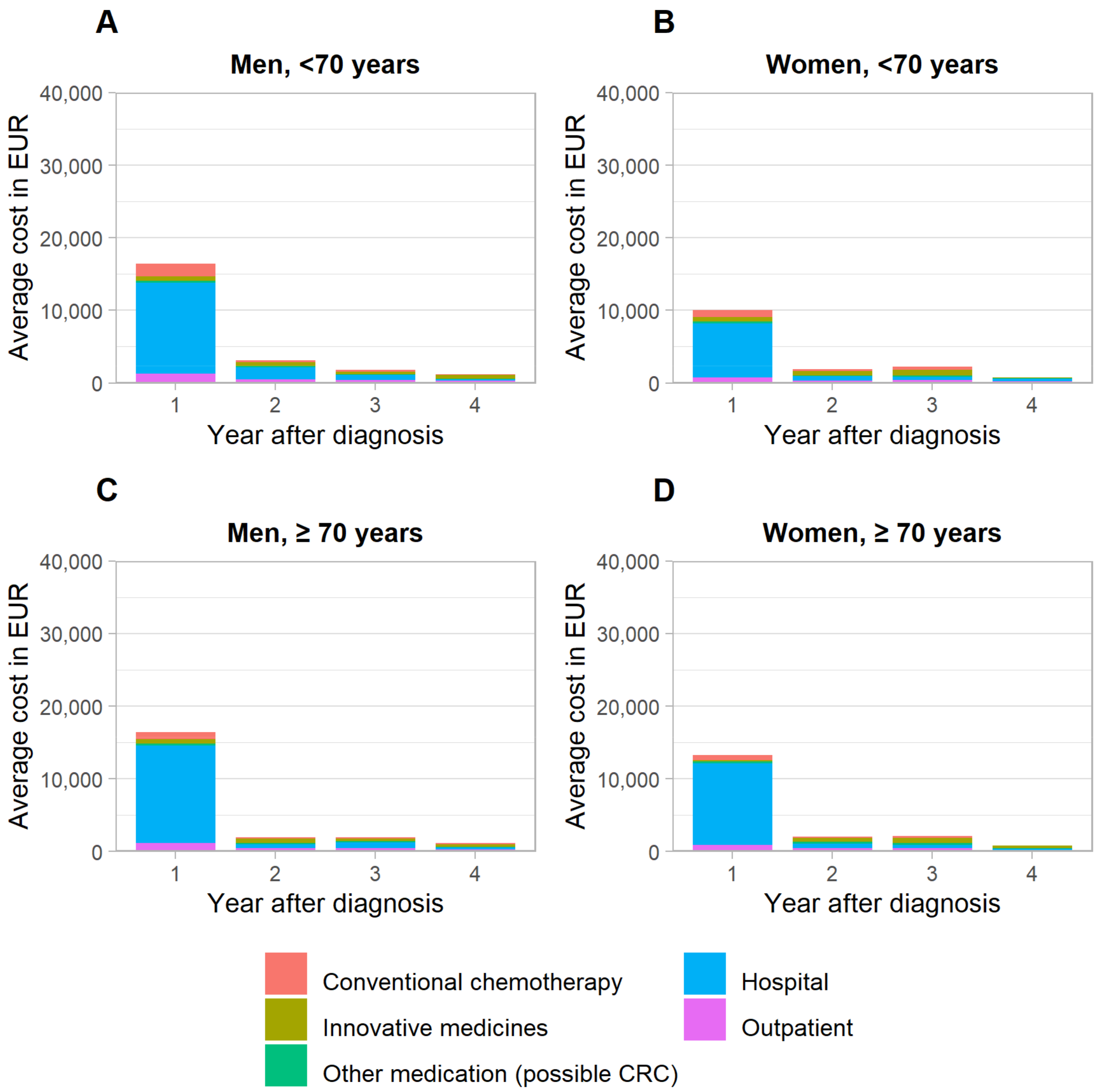
3.1. Initial Phase of Care
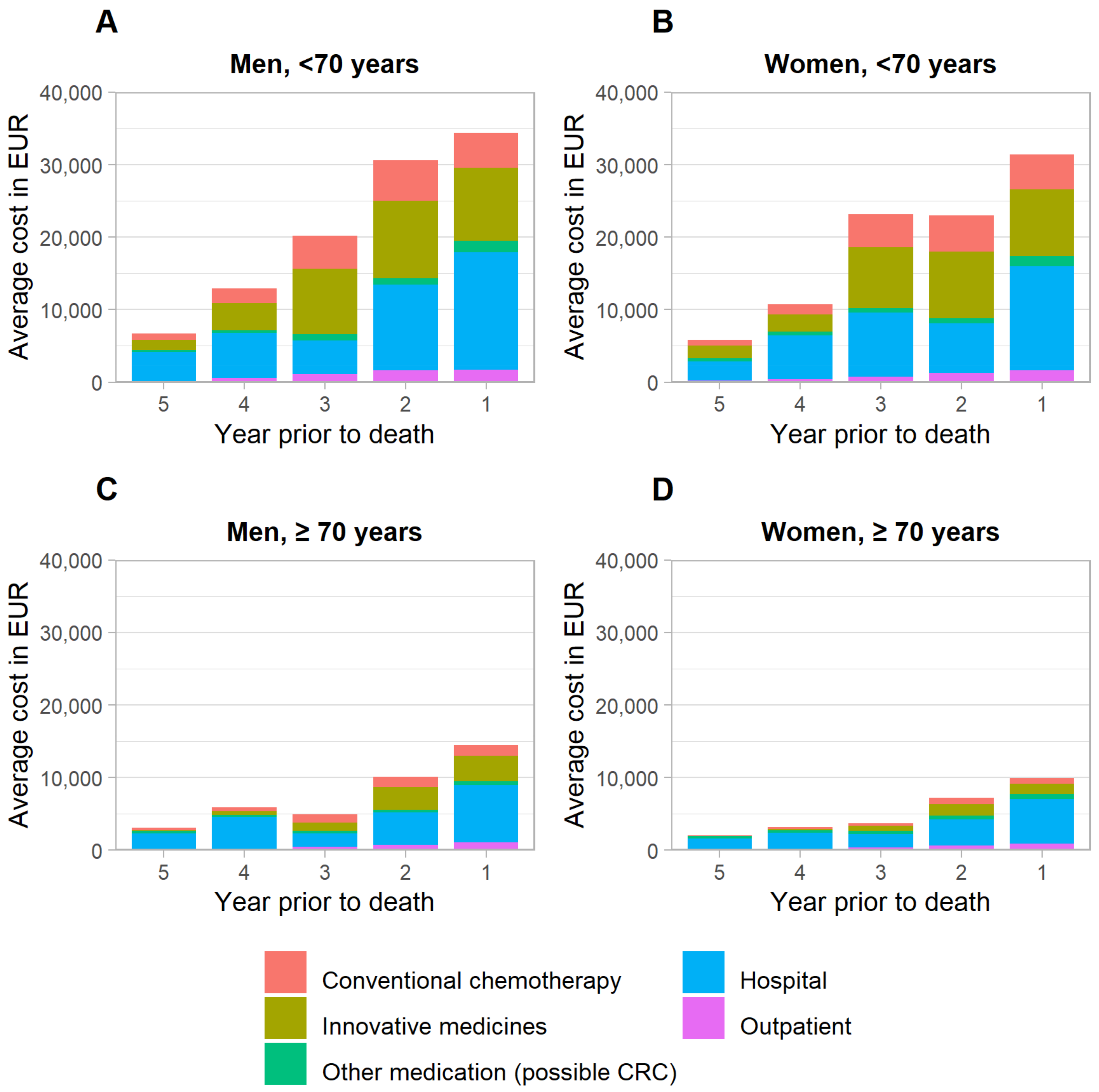
3.2. Terminal Phase of Care
4. Discussion
5. Findings in Context
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cardoso, R.; Zhu, A.; Guo, F.; Heisser, T.; Hoffmeister, M.; Brenner, H. Incidence and Mortality of Proximal and Distal Colorectal Cancer in Germany. Dtsch. Ärzteblatt Int. 2021, 118, 281–287. [Google Scholar] [CrossRef]
- Robert-Koch-Institut; Gesellschaft der Epidemiologischen Krebsregister in Deutschland e.V. Krebs in Deutschland Für 2015/2016 (Robert-Koch-Institute and the Society of Epidemiological Cancer Registries in Germany: Cancer in Germany for 2015/2016). Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/krebs_in_deutschland_inhalt.html (accessed on 20 July 2022).
- Brenner, H.; Jansen, L.; Ulrich, A.; Chang-Claude, J.; Hoffmeister, M. Survival of Patients with Symptom- and Screening-Detected Colorectal Cancer. Oncotarget 2016, 7, 44695–44704. [Google Scholar] [CrossRef] [Green Version]
- Sieg, A.; Brenner, H. Cost-Saving Analysis of Screening Colonoscopy in Germany. Z. Gastroenterol. 2007, 45, 945–951. [Google Scholar] [CrossRef] [Green Version]
- Ladabaum, U.; Alvarez-Osorio, L.; Rösch, T.; Brueggenjuergen, B. Cost-Effectiveness of Colorectal Cancer Screening in Germany: Current Endoscopic and Fecal Testing Strategies versus Plasma Methylated Septin 9 DNA. Endosc. Int. Open 2014, 2, E96–E104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.-Y.; Datzmann, T.; Hernandez, D.; Schmitt, J.; Schlander, M. Do Certified Cancer Centers Provide More Cost-Effective Care? A Health Economic Analysis of Colon Cancer Care in Germany Using Administrative Data. Int. J. Cancer 2021, 149, 1744–1754. [Google Scholar] [CrossRef]
- Haug, U.; Engel, S.; Verheyen, F.; Linder, R. Estimating Colorectal Cancer Treatment Costs: A Pragmatic Approach Exemplified by Health Insurance Data from Germany. PLoS ONE 2014, 9, e88407. [Google Scholar] [CrossRef] [PubMed]
- Yabroff, K.R.; Lamont, E.B.; Mariotto, A.; Warren, J.L.; Topor, M.; Meekins, A.; Brown, M.L. Cost of Care for Elderly Cancer Patients in the United States. J. Natl. Cancer Inst. 2008, 100, 630–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bugge, C.; Brustugun, O.T.; Sæther, E.M.; Kristiansen, I.S. Phase- and Gender-Specific, Lifetime, and Future Costs of Cancer. Medicine 2021, 100, e26523. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, C.; Pataky, R.; Bremner, K.E.; Rangrej, J.; Chan, K.K.W.; Cheung, W.Y.; Hoch, J.S.; Peacock, S.; Krahn, M.D. Phase-Specific and Lifetime Costs of Cancer Care in Ontario, Canada. BMC Cancer 2016, 16, 809. [Google Scholar] [CrossRef] [Green Version]
- Mariotto, A.B.; Warren, J.L.; Zeruto, C.; Coughlan, D.; Barrett, M.J.; Zhao, L.; Yabroff, K.R. Cancer-Attributable Medical Costs for Colorectal Cancer Patients by Phases of Care: What Is the Effect of a Prior Cancer History? J. Natl. Cancer Inst. Monogr. 2020, 2020, 22–30. [Google Scholar] [CrossRef]
- Murphy, C.C.; Harlan, L.C.; Lund, J.L.; Lynch, C.F.; Geiger, A.M. Patterns of Colorectal Cancer Care in the United States: 1990–2010. J. Natl. Cancer Inst. 2015, 107, djv198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabroff, K.R.; Mariotto, A.; Tangka, F.; Zhao, J.; Islami, F.; Sung, H.; Sherman, R.L.; Henley, S.J.; Jemal, A.; Ward, E.M. Annual Report to the Nation on the Status of Cancer, Part 2: Patient Economic Burden Associated With Cancer Care. J. Natl. Cancer Inst. 2021, 113, 1670–1682. [Google Scholar] [CrossRef] [PubMed]
- Hofmarcher, T.; Lindgren, P.; Wilking, N.; Jönsson, B. The Cost of Cancer in Europe 2018. Eur. J. Cancer 2020, 129, 41–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision). Available online: https://icd.who.int/browse11/l-m/en (accessed on 15 July 2020).
- Arora, V.; Moriates, C.; Shah, N. The Challenge of Understanding Health Care Costs and Charges. AMA J. Ethics 2015, 17, 1046–1052. [Google Scholar] [CrossRef] [Green Version]
- Kriza, C.; Emmert, M.; Wahlster, P.; Niederländer, C.; Kolominsky-Rabas, P. Cost of Illness in Colorectal Cancer: An International Review. Pharmacoeconomics 2013, 31, 577–588. [Google Scholar] [CrossRef]
- Laudicella, M.; Walsh, B.; Burns, E.; Smith, P.C. Cost of Care for Cancer Patients in England: Evidence from Population-Based Patient-Level Data. Br. J. Cancer 2016, 114, 1286–1292. [Google Scholar] [CrossRef] [Green Version]
- Kaye, D.R.; Min, H.S.; Herrel, L.A.; Dupree, J.M.; Ellimoottil, C.; Miller, D.C. Costs of Cancer Care Across the Disease Continuum. Oncologist 2018, 23, 798–805. [Google Scholar] [CrossRef] [Green Version]
- Sorich, M.J.; Wiese, M.D.; Rowland, A.; Kichenadasse, G.; McKinnon, R.A.; Karapetis, C.S. Extended RAS Mutations and Anti-EGFR Monoclonal Antibody Survival Benefit in Metastatic Colorectal Cancer: A Meta-Analysis of Randomized, Controlled Trials. Ann. Oncol. 2015, 26, 13–21. [Google Scholar] [CrossRef]
- Heinemann, V.; Rivera, F.; O’Neil, B.H.; Stintzing, S.; Koukakis, R.; Terwey, J.-H.; Douillard, J.-Y. A Study-Level Meta-Analysis of Efficacy Data from Head-to-Head First-Line Trials of Epidermal Growth Factor Receptor Inhibitors versus Bevacizumab in Patients with RAS Wild-Type Metastatic Colorectal Cancer. Eur. J. Cancer 2016, 67, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF) S3-Leitlinie Kolorektales Karzinom (Guideline Program Oncology (German Cancer Society, German Cancer Aid, AWMF): S3-Guideline Colorectal Cancer). Available online: http://www.leitlinienprogramm-onkologie.de/leitlinien/kolorektales-karzinom/ (accessed on 6 January 2021).
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.A.; Kasi, P.M.; Wallace, M.B. Colorectal Cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef]
- Cutsem, E.V.; Cervantes, A.; Adam, R.; Sobrero, A.; Krieken, J.H.V.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO Consensus Guidelines for the Management of Patients with Metastatic Colorectal Cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Ran, T.; Cheng, C.Y.; Misselwitz, B.; Brenner, H.; Ubels, J.; Schlander, M. Cost-Effectiveness of Colorectal Cancer Screening Strategies—A Systematic Review. Clin. Gastroenterol. Hepatol. 2019, 17, 1696–1981.e15. [Google Scholar] [CrossRef] [PubMed]
- Ladabaum, U.; Dominitz, J.A.; Kahi, C.; Schoen, R.E. Strategies for Colorectal Cancer Screening. Gastroenterology 2020, 158, 418–432. [Google Scholar] [CrossRef]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of Screening Sigmoidoscopy and Screening Colonoscopy on Colorectal Cancer Incidence and Mortality: Systematic Review and Meta-Analysis of Randomised Controlled Trials and Observational Studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [Green Version]
- Guo, F.; Chen, C.; Holleczek, B.; Schöttker, B.; Hoffmeister, M.; Brenner, H. Strong Reduction of Colorectal Cancer Incidence and Mortality After Screening Colonoscopy: Prospective Cohort Study From Germany. Am. J. Gastroenterol. 2021, 116, 967–975. [Google Scholar] [CrossRef]
- Heisser, T.; Hoffmeister, M.; Brenner, H. Model Based Evaluation of Long-Term Efficacy of Existing and Alternative Colorectal Cancer Screening Offers: A Case Study for Germany. Int. J. Cancer 2022, 150, 1471–1480. [Google Scholar] [CrossRef]
- Breckenkamp, J.; Spallek, J.; Kraywinkel, K.; Krieg, V.; Schwabe, W.; Greiner, W.; Damm, O.; Hense, H.; Razum, O. Linkage of data of the medical service of the health insurances with data of a cancer registry. Gesundheitswesen 2012, 74, e52–e60. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Year after Diagnosis | No of Patients | Median Age (Years) | Average CRC-Related Costs in EUR | Average Total Healthcare Costs in EUR | |||
|---|---|---|---|---|---|---|---|
| Hospital | Ambulatory | Medication | Total Costs | ||||
| Men | |||||||
| <70 age | |||||||
| 1 | 486 | 59 | 12,566 | 1235 | 2648 | 16,450 | 20,245 |
| 2 | 336 | 60 | 1677 | 449 | 1022 | 3147 | 6435 |
| 3 | 119 | 61 | 634 | 437 | 738 | 1809 | 3879 |
| 4 | 79 | 62 | 208 | 287 | 708 | 1203 | 2374 |
| ≥70 age | |||||||
| 1 | 360 | 75 | 13,399 | 1187 | 1789 | 16,375 1 | 21,210 |
| 2 | 285 | 76 | 493 | 491 | 1014 | 1998 | 6240 |
| 3 | 120 | 77 | 815 | 470 | 635 | 1920 | 5832 |
| 4 | 94 | 78 | 273 | 323 | 598 | 1195 | 3450 |
| Women | |||||||
| <70 age | |||||||
| 1 | 411 | 58 | 7519 | 716 | 1836 | 10,071 2 | 13,109 |
| 2 | 283 | 59 | 589 | 324 | 986 | 1900 | 3938 |
| 3 | 91 | 59 | 451 | 375 | 1399 | 2226 | 4831 |
| 4 | 55 | 62 | 331 | 201 | 233 | 766 | 2211 |
| ≥70 age | |||||||
| 1 | 491 | 78 | 11,177 | 913 | 1160 | 13,250 3,4 | 17,728 |
| 2 | 371 | 78 | 635 | 449 | 925 | 2009 | 6392 |
| 3 | 173 | 78 | 447 | 481 | 1195 | 2122 | 5477 |
| 4 | 131 | 79 | 110 | 244 | 487 | 841 | 2574 |
| Year before Death | No of Patients | Median Age (Years) | Average CRC-Related Costs in EUR | Average Total Healthcare Costs in EUR | |||
|---|---|---|---|---|---|---|---|
| Hospital | Ambulatory | Medication | Total | ||||
| Men | |||||||
| <70 age | |||||||
| 5 | 35 | 62 | 4007 | 152 | 2538 | 6696 | 12,265 |
| 4 | 64 | 61 | 6197 | 557 | 6137 | 12,892 | 16,566 |
| 3 | 70 | 61 | 4633 | 1124 | 14,436 | 20,193 | 26,804 |
| 2 | 117 | 60 | 11,852 | 1607 | 17,150 | 30,609 | 38,094 |
| 1 | 165 | 60 | 16,174 | 1736 | 16,441 | 34,351 | 45,460 |
| ≥70 age | |||||||
| 5 | 108 | 81 | 2182 | 109 | 779 | 3070 | 6652 |
| 4 | 176 | 80 | 4328 | 236 | 1310 | 5874 | 10,174 |
| 3 | 191 | 81 | 1831 | 443 | 2632 | 4907 | 10,563 |
| 2 | 303 | 81 | 4447 | 743 | 4919 | 10,109 | 15,462 |
| 1 | 393 | 81 | 7870 | 1073 | 5520 | 14,463 1 | 25,387 |
| Women | |||||||
| <70 age | |||||||
| 5 | 15 | 64 | 2668 | 187 | 2980 | 5835 | 9073 |
| 4 | 23 | 62 | 6007 | 436 | 4317 | 10,759 | 15,040 |
| 3 | 25 | 63 | 8845 | 742 | 13,564 | 23,151 | 26,426 |
| 2 | 56 | 62 | 6821 | 1296 | 14,924 | 23,041 | 30,168 |
| 1 | 90 | 60 | 14,397 | 1603 | 15,417 | 31,417 2 | 45,312 |
| ≥70 age | |||||||
| 5 | 121 | 82 | 1514 | 109 | 415 | 2038 | 4864 |
| 4 | 199 | 83 | 2179 | 212 | 757 | 3148 | 6496 |
| 3 | 215 | 84 | 1874 | 353 | 1465 | 3692 | 7579 |
| 2 | 345 | 84 | 3589 | 663 | 2927 | 7180 | 11,819 |
| 1 | 469 | 84 | 6138 | 917 | 2875 | 9930 3,4 | 19,259 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heisser, T.; Simon, A.; Hapfelmeier, J.; Hoffmeister, M.; Brenner, H. Treatment Costs of Colorectal Cancer by Sex and Age: Population-Based Study on Health Insurance Data from Germany. Cancers 2022, 14, 3836. https://doi.org/10.3390/cancers14153836
Heisser T, Simon A, Hapfelmeier J, Hoffmeister M, Brenner H. Treatment Costs of Colorectal Cancer by Sex and Age: Population-Based Study on Health Insurance Data from Germany. Cancers. 2022; 14(15):3836. https://doi.org/10.3390/cancers14153836
Chicago/Turabian StyleHeisser, Thomas, Andreas Simon, Jana Hapfelmeier, Michael Hoffmeister, and Hermann Brenner. 2022. "Treatment Costs of Colorectal Cancer by Sex and Age: Population-Based Study on Health Insurance Data from Germany" Cancers 14, no. 15: 3836. https://doi.org/10.3390/cancers14153836