
Hepatobiliary Scintigraphy and Glass 90Y Radioembolization with Personalized Dosimetry: Dynamic Changes in Treated and Nontreated Liver

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Radioembolization Work-Up
2.3. Y90 Microsphere Injection and IMAGING
2.4. Hepatobiliary Scintigraphy (Morpho-Functional Imaging)
2.5. Tumor Assessment
2.6. Statistical Analysis
3. Results
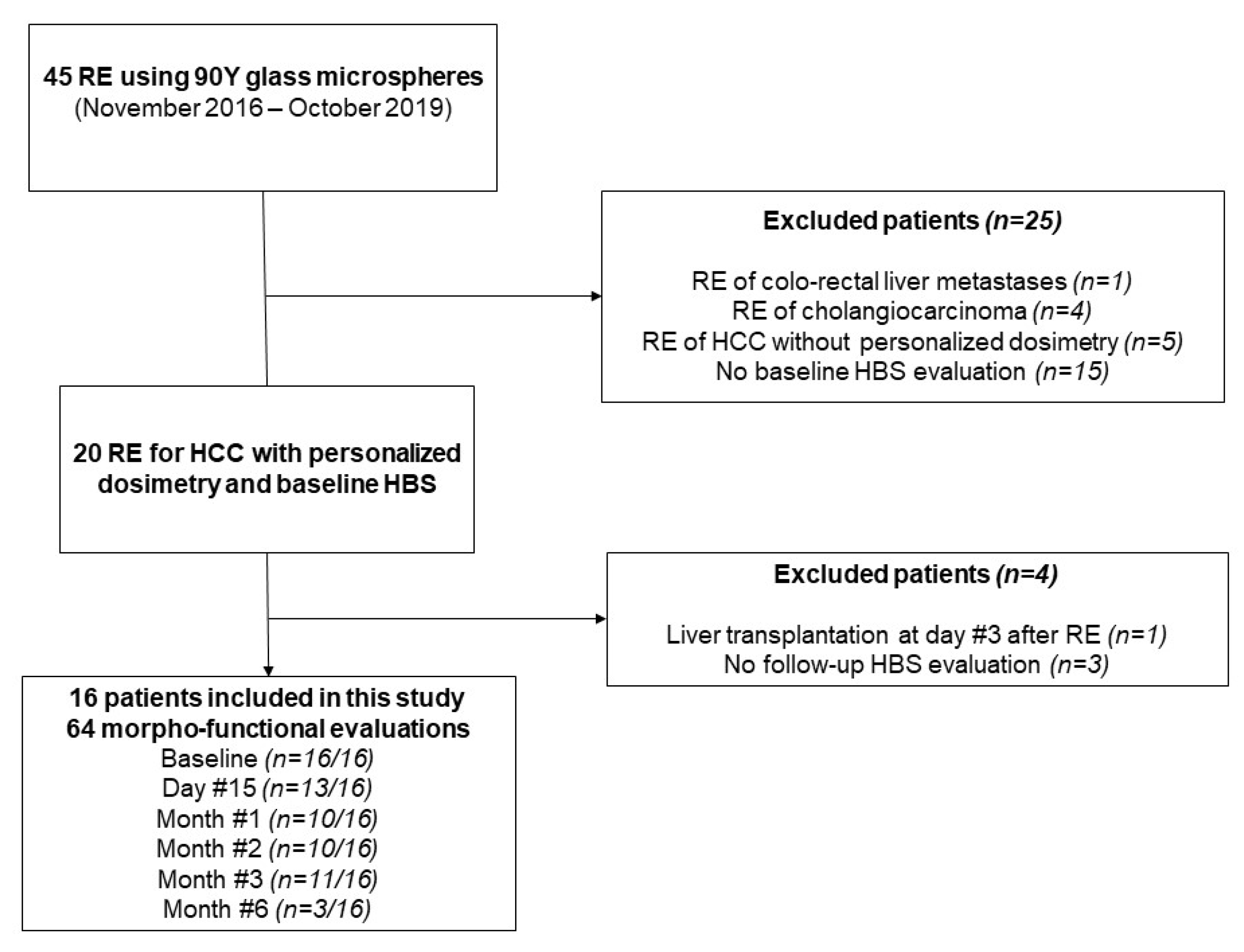
3.1. Population
3.2. Tumor Assessment
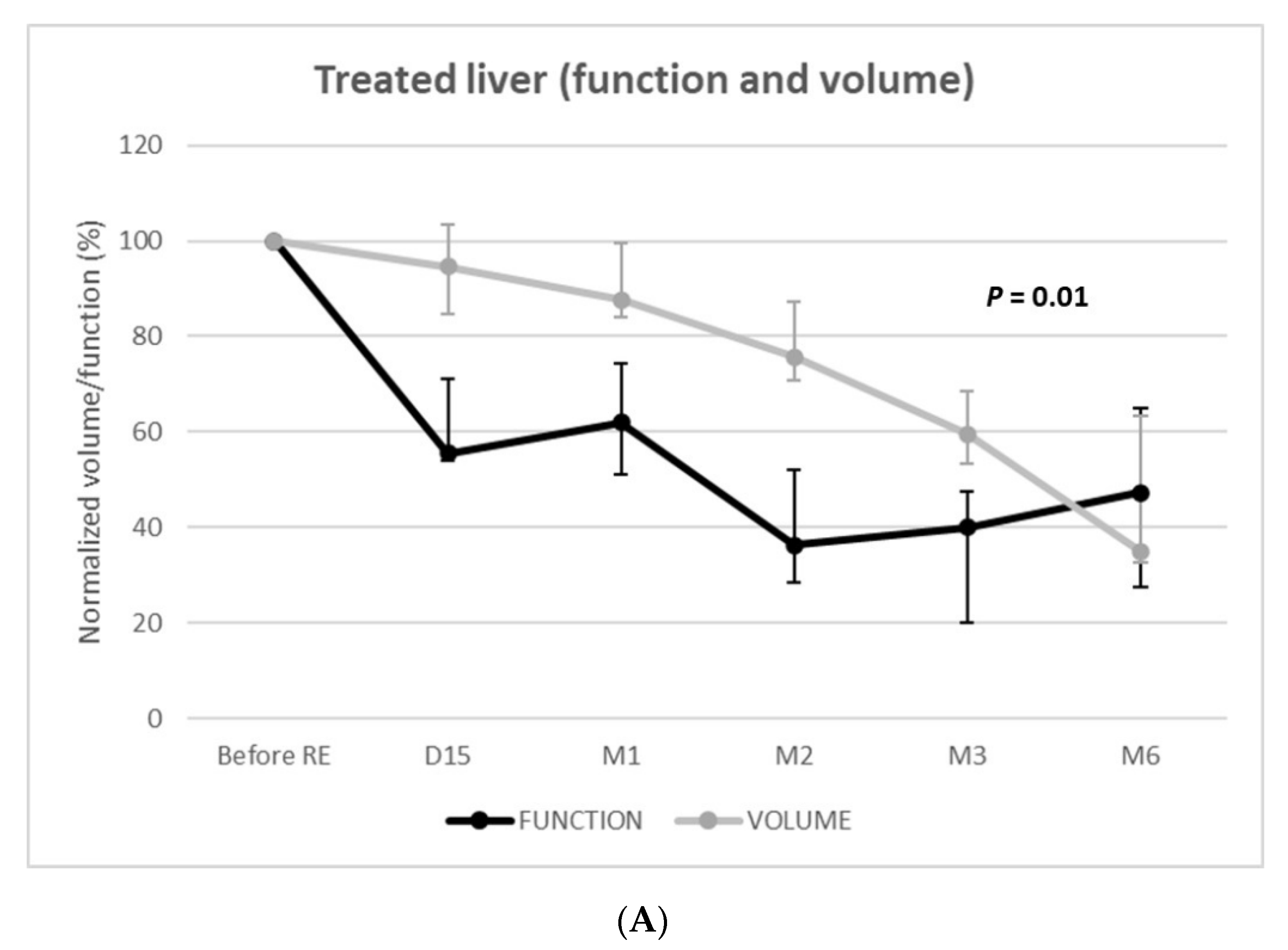
3.3. Function and Volume Changes
3.4. Comparison Using Linear Mixed Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F.H.; et al. Y90 Radioembolization Significantly Prolongs Time to Progression Compared With Chemoembolization in Patients With Hepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163.e2. [Google Scholar] [CrossRef] [Green Version]
- Campigotto, M.; Giuffrè, M.; Colombo, A.; Visintin, A.; Aversano, A.; Budel, M.; Masutti, F.; Abazia, C.; Crocé, L.S. Comparison between hepatocellular carcinoma prognostic scores: A 10-year single-center experience and brief review of the current literature. World J. Hepatol. 2020, 12, 1239–1257. [Google Scholar] [CrossRef] [PubMed]
- Chow, P.K.H.; Gandhi, M.; Tan, S.-B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients With Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Ricke, J.; Klümpen, H.J.; Amthauer, H.; Bargellini, I.; Bartenstein, P.; De Toni, E.N.; Gasbarrini, A.; Pech, M.; Peck-Radosavljevic, M.; Popovič, P.; et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J. Hepatol. 2019, 71, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.-P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef]
- Garin, E.; Palard, X.; Rolland, Y. Personalised Dosimetry in Radioembolisation for HCC: Impact on Clinical Outcome and on Trial Design. Cancers 2020, 12, 1557. [Google Scholar] [CrossRef] [PubMed]
- Hermann, A.L.; Dieudonné, A.; Ronot, M.; Sanchez, M.; Pereira, H.; Chatellier, G.; Garin, E.; Castera, L.; Lebtahi, R.; Vilgrain, V. Relationship of Tumor Radiation-absorbed Dose to Survival and Response in Hepatocellular Carcinoma Treated with Transarterial Radioembolization with (90)Y in the SARAH Study. Radiology 2020, 296, 673–684. [Google Scholar] [CrossRef]
- Salem, R.; Padia, S.A.; Lam, M.; Bell, J.; Chiesa, C.; Fowers, K.; Hamilton, B.; Herman, J.; Kappadath, S.C.; Leung, T.; et al. Clinical and dosimetric considerations for Y90: Recommendations from an international multidisciplinary working group. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1695–1704. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; De Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Terroir-Cassou-Mounat, M.; et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): A randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol. Hepatol. 2020, 6, 17–29. [Google Scholar] [CrossRef]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Martinez-Cuesta, A.; Viudez, A.; Chopitea, A.; Iñarrairaegui, M.; Arbizu, J.; Bilbao, J.I. Liver disease induced by radioembolization of liver tumors. Cancer 2008, 112, 1538–1546. [Google Scholar] [CrossRef]
- Garin, E.; Rolland, Y.; Pracht, M.; Le Sourd, S.; Laffont, S.; Mesbah, H.; Haumont, L.A.; Lenoir, L.; Rohou, T.; Brun, V.; et al. High impact of macroaggregated albumin-based tumour dose on response and overall survival in hepatocellular carcinoma patients treated with (90) Y-loaded glass microsphere radioembolization. Liver Int. 2017, 37, 101–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapelle, T.; De Beeck, B.O.; Huyghe, I.; Francque, S.; Driessen, A.; Roeyen, G.; Ysebaert, D.; De Greef, K. Future remnant liver function estimated by combining liver volumetry on magnetic resonance imaging with total liver function on 99m Tc-mebrofenin hepatobiliary scintigraphy: Can this tool predict post-hepatectomy liver failure? HPB 2016, 18, 494–503. [Google Scholar] [CrossRef] [Green Version]
- Cieslak, K.P.; Bennink, R.J.; de Graaf, W.; Van Lienden, K.P.; Besselink, M.G.; Busch, O.R.; Gouma, D.J.; van Gulik, T.M. Measurement of liver function using hepatobiliary scintigraphy improves risk assessment in patients undergoing major liver resection. HPB 2016, 18, 773–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaf, W.; Van Lienden, K.P.; Dinant, S.; Roelofs, J.J.T.H.; Busch, O.R.C.; Gouma, D.J.; Bennink, R.J.; Van Gulik, T.M. Assessment of Future Remnant Liver Function Using Hepatobiliary Scintigraphy in Patients Undergoing Major Liver Resection. J. Gastrointest. Surg. 2009, 14, 369–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaf, W.; Van Lienden, K.P.; Van Gulik, T.M.; Bennink, R.J. (99m)Tc-mebrofenin hepatobiliary scintigraphy with SPECT for the assessment of hepatic function and liver functional volume before partial hepatectomy. J. Nucl. Med. 2010, 51, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Erdogan, D.; Heijnen, B.H.; Bennink, R.J.; Kok, M.; Dinant, S.; Straatsburg, I.H.; Gouma, D.J.; Van Gulik, T.M. Preoperative assessment of liver function: A comparison of 99mTc-Mebrofenin scintigraphy with indocyanine green clearance test. Liver Int. 2004, 24, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Bennink, R.J.; Cieslak, K.P.; Van Delden, O.M.; Van Lienden, K.P.; Klümpen, H.-J.; Jansen, P.L.; Van Gulik, T.M. Monitoring of Total and Regional Liver Function after SIRT. Front. Oncol. 2014, 16, 152. [Google Scholar] [CrossRef] [Green Version]
- Braat, M.N.G.J.A.; De Jong, H.W.; Seinstra, B.A.; Scholten, M.V.; Bosch, M.A.A.J.V.D.; Lam, M.G.E.H. Hepatobiliary scintigraphy may improve radioembolization treatment planning in HCC patients. EJNMMI Res. 2017, 7, 2. [Google Scholar] [CrossRef] [Green Version]
- Labeur, T.A.; Cieslak, K.P.; Van Gulik, T.M.; Takkenberg, R.B.; Van Der Velden, S.; Lam, M.G.E.H.; Klümpen, H.-J.; Bennink, R.J.; van Delden, O.M. The utility of 99mTc-mebrofenin hepatobiliary scintigraphy with SPECT/CT for selective internal radiation therapy in hepatocellular carcinoma. Nucl. Med. Commun. 2020, 41, 740–749. [Google Scholar] [CrossRef]
- Van Der Velden, S.; Braat, M.N.G.J.A.; Labeur, T.A.; Scholten, M.V.; Van Delden, O.M.; Bennink, R.J.; De Jong, H.W.A.M.; Lam, M.G.E.H. A Pilot Study on Hepatobiliary Scintigraphy to Monitor Regional Liver Function in 90Y Radioembolization. J. Nucl. Med. 2019, 60, 1430–1436. [Google Scholar] [CrossRef] [Green Version]
- Willowson, K.P.; Schembri, G.P.; Bernard, E.J.; Chan, D.L.; Bailey, D.L. Quantifying the effects of absorbed dose from radioembolisation on healthy liver function with [(99m)Tc]TcMebrofenin. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 838–848. [Google Scholar] [CrossRef] [PubMed]
- Madoff, D.C.; Odisio, B.C.; Schadde, E.; Gaba, R.C.; Bennink, R.J.; Van Gulik, T.M.; Guiu, B. Improving the Safety of Major Resection for Hepatobiliary Malignancy: Portal Vein Embolization and Recent Innovations in Liver Regeneration Strategies. Curr. Oncol. Rep. 2020, 22, 59. [Google Scholar] [CrossRef] [PubMed]
- Palard, X.; Edeline, J.; Rolland, Y.; Le Sourd, S.; Pracht, M.; Laffont, S.; Lenoir, L.; Boudjema, K.; Ugen, T.; Brun, V.; et al. Dosimetric parameters predicting contralateral liver hypertrophy after unilobar radioembolization of hepatocellular carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 392–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vouche, M.; Lewandowski, R.J.; Atassi, R.; Memon, K.; Gates, V.L.; Ryu, R.K.; Gaba, R.C.; Mulcahy, M.F.; Baker, T.; Sato, K.; et al. Radiation lobectomy: Time-dependent analysis of future liver remnant volume in unresectable liver cancer as a bridge to resection. J. Hepatol. 2013, 59, 1029–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafrouni, M.; Allimant, C.; Fourcade, M.; Vauclin, S.; Guiu, B.; Mariano-Goulart, D.; Ben Bouallègue, F. Analysis of differences between (99m)Tc-MAA SPECT- and (90)Y-microsphere PET-based dosimetry for hepatocellular carcinoma selective internal radiation therapy. EJNMMI Res. 2019, 9, 62. [Google Scholar] [CrossRef] [Green Version]
- Allimant, C.; Kafrouni, M.; Delicque, J.; Ilonca, D.; Cassinotto, C.; Assenat, E.; Ursic-Bedoya, J.; Pageaux, G.-P.; Mariano-Goulart, D.; Aho, S.; et al. Tumor Targeting and Three-Dimensional Voxel-Based Dosimetry to Predict Tumor Response, Toxicity, and Survival after Yttrium-90 Resin Microsphere Radioembolization in Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2018, 29, 1662–1670.e4. [Google Scholar] [CrossRef]
- Guiu, B.; Quenet, F.; Panaro, F.; Piron, L.; Cassinotto, C.; Herrerro, A.; Souche, F.R.; Hermida, M.; Pierredon-Foulongne, M.A.; Belgour, A.; et al. Liver venous deprivation versus portal vein embolization before major hepatectomy: Future liver remnant volumetric and functional changes. Hepatobiliary Surg. Nutr. 2020, 9, 564–576. [Google Scholar] [CrossRef]
- Piron, L.; Deshayes, E.; Cassinotto, C.; Quenet, F.; Panaro, F.; Hermida, M.; Allimant, C.; Assenat, E.; Pageaux, G.P.; Molinari, N.; et al. Deportalization, Venous Congestion, Venous Deprivation: Serial Measurements of Volumes and Functions on Morphofunctional 99mTc-Mebrofenin SPECT-CT. Diagnostics 2020, 11, 12. [Google Scholar] [CrossRef]
- Sangro, B.; Martínez-Urbistondo, D.; Bester, L.; Bilbao, J.I.; Coldwell, D.M.; Flamen, P.; Kennedy, A.; Ricke, J.; Sharma, R.A. Prevention and treatment of complications of selective internal radiation therapy: Expert guidance and systematic review. Hepatology 2017, 66, 969–982. [Google Scholar] [CrossRef]
- Phillips, R.; Karnofsky, D.A.; Hamilton, L.D.; Nickson, J.J. Roentgen therapy of hepatic metastases. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1954, 71, 826–834. [Google Scholar]
- Wharton, J.T.; Delclos, L.; Gallager, S.; Smith, J.P. Radiation hepatitis induced by abdominal irradiation with the cobalt 60 moving strip technique. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1973, 117, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Clement, B.; Grimaud, J.A.; Campion, J.P.; Deugnier, Y.; Guillouzo, A. Cell types involved in collagen and fibronectin production in normal and fibrotic human liver. Hepatology 1986, 6, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ros, N.; Iñarrairaegui, M.; Paramo, J.A.; Berasain, C.; Avila, M.A.; Chopitea, A.; Varo, N.; Sarobe, P.; Bilbao, J.I.; Dominguez, I.; et al. Radioembolization of hepatocellular carcinoma activates liver regeneration, induces inflammation and endothelial stress and activates coagulation. Liver Int. 2015, 35, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, R.J.; Donahue, L.; Chokechanachaisakul, A.; Kulik, L.; Mouli, S.; Caicedo, J.; Abecassis, M.; Fryer, J.; Salem, R.; Baker, T. (90) Y radiation lobectomy: Outcomes following surgical resection in patients with hepatic tumors and small future liver remnant volumes. J. Surg. Oncol. 2016, 114, 99–105. [Google Scholar] [CrossRef] [PubMed]
- De Graaf, W.; Van Lienden, K.P.; Van Den Esschert, J.W.; Bennink, R.J.; Van Gulik, T.M. Increase in future remnant liver function after preoperative portal vein embolization. Br. J. Surg. 2011, 98, 825–834. [Google Scholar] [CrossRef]
- Olthof, P.B.; Tomassini, F.; Huespe, P.E.; Truant, S.; Pruvot, F.R.; Troisi, R.I.; Castro, C.; Schadde, E.; Axelsson, R.; Sparrelid, E.; et al. Hepatobiliary scintigraphy to evaluate liver function in associating liver partition and portal vein ligation for staged hepatectomy: Liver volume overestimates liver function. Surgery 2017, 162, 775–783. [Google Scholar] [CrossRef]
- Guiu, B. Portal Vein Embolization versus 90Y Radioembolization. J. Vasc. Interv. Radiol. 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Number (%) or Median (Range) |
|---|---|
| Age (years) | 60 (46–83) |
| Gender | |
| Male | 14 (88%) |
| Female | 2 (12%) |
| Underlying liver disease | |
| Alcohol | 3 (19%) |
| Hepatitis C | 10 (63%) |
| Nonalcoholic steatohepatitis | 2 (12%) |
| Noncirrhotic | 1 (6%) |
| Child-Pugh score | |
| A5 | 15 (94%) |
| A6 | 1 (6%) |
| Performance status | |
| 0 | 11 (69%) |
| 1 | 5 (31%) |
| BCLC classification | |
| B | 2 (12%) |
| C | 14 (88%) |
| Tumor distribution | |
| Multifocal | 11 (69%) |
| Unilateral | 16 (100%) |
| Tumor size | |
| Unidimensional (mm) | 71 (37–155) |
| Volume (cm3) | 340 (32–1173) |
| Prior therapy | |
| Chemoembolization | 6 (38%) |
| Resection/Ablation | 2 (12%) |
| Sorafenib | 2 (12%) |
| Combined treatments | 2 (12%) |
| None | 7 (44%) |
| Alpha-foetoprotein | |
| Normal, <20 ng/mL | 5 (31%) |
| 20–200 ng/mL | 8 (50%) |
| ≥200 ng/mL | 3 (19%) |
| Portal vein invasion | |
| Yes | 11 (69%) |
| Main | 2 (18%) |
| Left/right branch | 6 (54%) |
| Segmental | 3 (27%) |
| Treatment | |
| Lobar right | 12 (75%) |
| Lobar left | 2 (12%) |
| Right sector (ant or post) | 2 (12%) |
| Dose (Gy) | |
| Tumor | 262 (205–461) |
| Irradiated non-tumoral liver | 112 (55–182) |
| Whole non-tumoral liver | 53 (20–85) |
| Day #15 (n = 11/16) | Month #1 (n = 13/16) | Month #2 (n = 10/16) | Month #3 (n = 11/16) | Month #6 (n = 3/16) | |
|---|---|---|---|---|---|
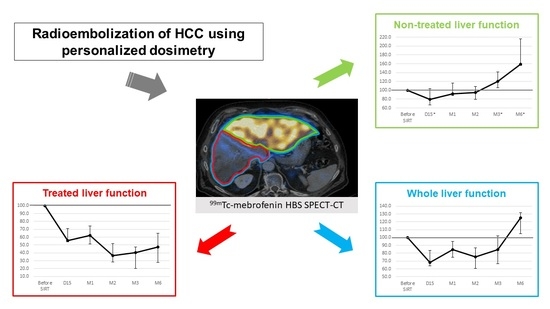
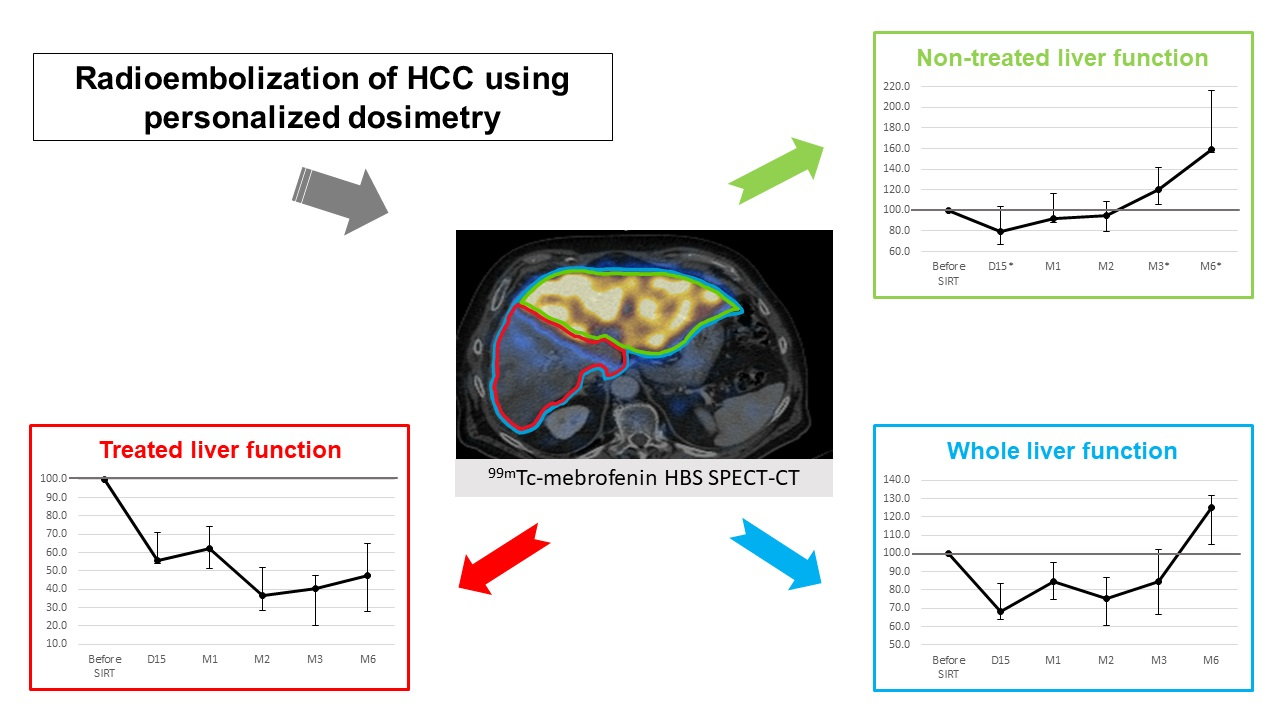
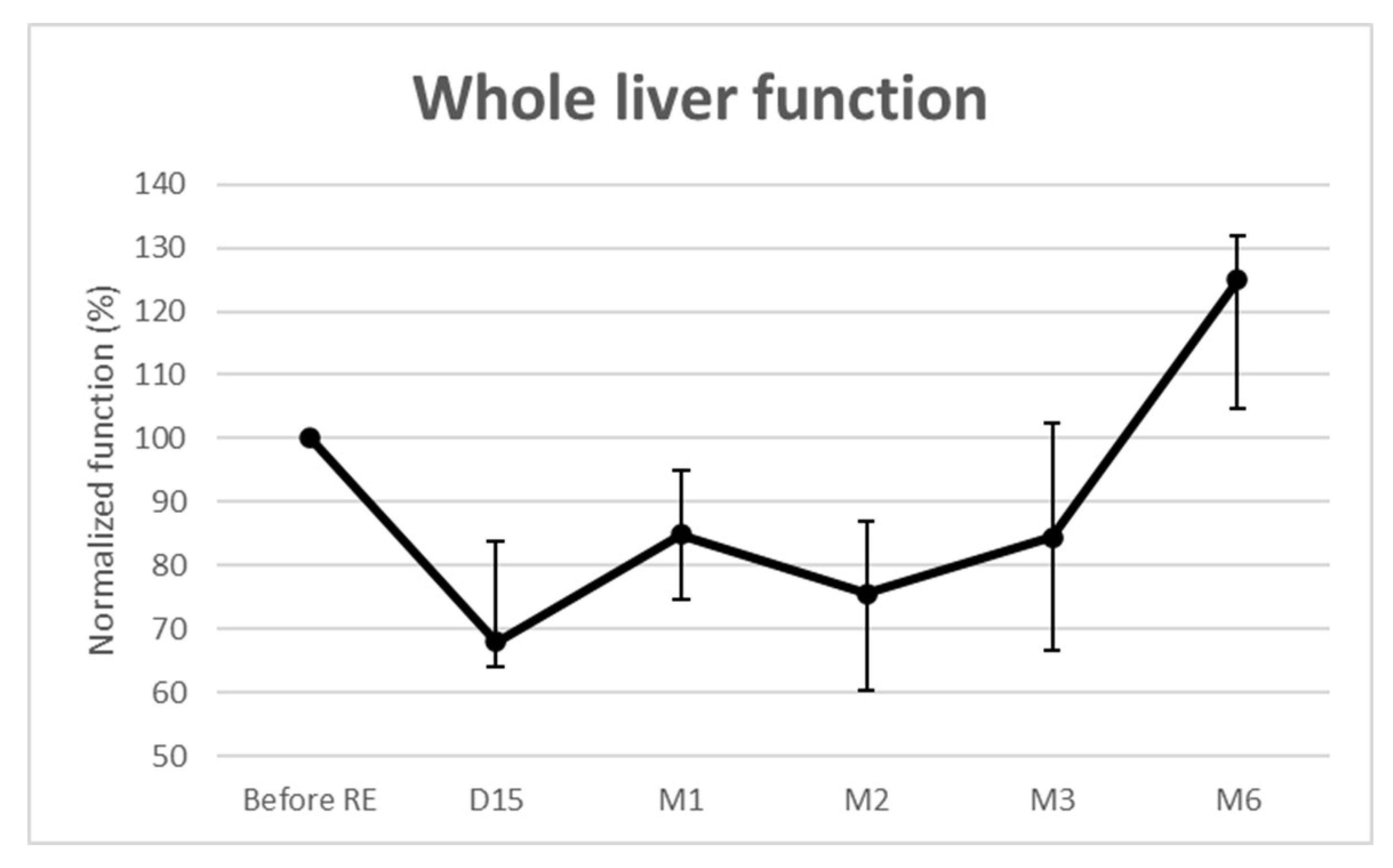
| Whole liver function (%) | 68.0 (64.0–83.8) | 84.9 (74.7–94.9) | 75.5 (60.3–86.9) | 84.4 (66.7–102.3) | 125.0 (104.8–131.9) |
| Treated liver function (%) | 55.6 (53.9–71.1) | 62.0 (51.1–74.4) | 36.3 (28.4–52.0) | 40.1 (20.2–47.5) | 47.2 (27.6–64.9) |
| Nontreated liver function (%) | 79.2 (67.1–104.0) | 91.9 (88.1–116.3) | 94.5 (79.6–108.8) | 119.7 (105.9–141.3) | 159.0 (155.9–216.8) |
| Treated liver volume (%) | 95 (85–103) | 88 (84–99) | 76 (71–87) | 60 (53–69) | 35 (33–63) |
| Nontreated liver volume (%) | 106 (102–115) | 118 (115–121) | 129 (111–133) | 129 (107–152) | 152 (129–222) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allimant, C.; Deshayes, E.; Kafrouni, M.; Santoro, L.; de Verbizier, D.; Fourcade, M.; Cassinotto, C.; Hermida, M.; Guillot, C.; Mariano-Goulart, D.; et al. Hepatobiliary Scintigraphy and Glass 90Y Radioembolization with Personalized Dosimetry: Dynamic Changes in Treated and Nontreated Liver. Diagnostics 2021, 11, 931. https://doi.org/10.3390/diagnostics11060931
Allimant C, Deshayes E, Kafrouni M, Santoro L, de Verbizier D, Fourcade M, Cassinotto C, Hermida M, Guillot C, Mariano-Goulart D, et al. Hepatobiliary Scintigraphy and Glass 90Y Radioembolization with Personalized Dosimetry: Dynamic Changes in Treated and Nontreated Liver. Diagnostics. 2021; 11(6):931. https://doi.org/10.3390/diagnostics11060931
Chicago/Turabian StyleAllimant, Carole, Emmanuel Deshayes, Marilyne Kafrouni, Lore Santoro, Delphine de Verbizier, Marjolaine Fourcade, Christophe Cassinotto, Margaux Hermida, Chloé Guillot, Denis Mariano-Goulart, and et al. 2021. "Hepatobiliary Scintigraphy and Glass 90Y Radioembolization with Personalized Dosimetry: Dynamic Changes in Treated and Nontreated Liver" Diagnostics 11, no. 6: 931. https://doi.org/10.3390/diagnostics11060931