
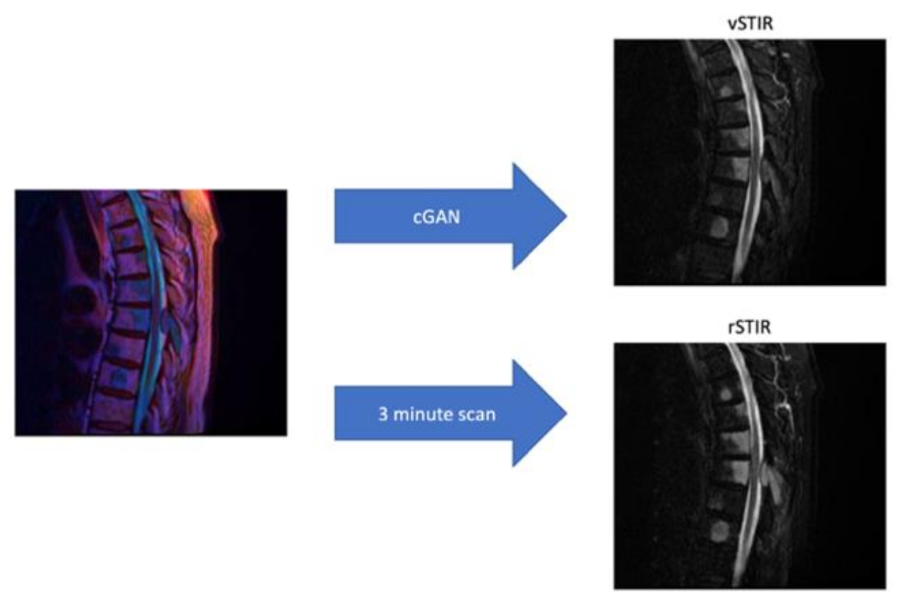
Generating Virtual Short Tau Inversion Recovery (STIR) Images from T1- and T2-Weighted Images Using a Conditional Generative Adversarial Network in Spine Imaging

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Network Architecture and Preprocessing
2.2. MRI
2.3. Dataset
2.4. Validation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| cGAN | conditional Generative Adversarial Network |
| GAN | Generative Adversarial Network |
| MRI | Magnetic Resonance Imaging |
| rSTIR | real Short Tau Inversion Recovery |
| STIR | Short Tau Inversion Recovery |
| vSTIR | virtual Short Tau Inversion Recovery |
References
- Yu, L.; Wang, X.; Lin, X.; Wang, Y. The Use of Lumbar Spine Magnetic Resonance Imaging in Eastern China: Appropriateness and Related Factors. PLoS ONE 2016, 11, e0146369. [Google Scholar] [CrossRef]
- Saadat, S.; Ghodsi, S.M.; Firouznia, K.; Etminan, M.; Goudarzi, K.; Naieni, K.H. Overuse or Underuse of MRI Scanners in Private Radiology Centers in Tehran. Int. J. Technol. Assess. Health Care 2008, 24, 277–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahnken, A.H.; Wildberger, J.E.; Adam, G.; Stanzel, S.; Schmitz-Rode, T.; Günther, R.W.; Buecker, A. Is There a Need for Contrast-Enhanced T1-Weighted MRI of the Spine after Inconspicuous Short Tau Inversion Recovery Imaging? Eur. Radiol. 2005, 15, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Y.; Hayashi, D. Role of Magnetic Resonance Imaging in Acute Spinal Trauma: A Pictorial Review. BMC Musculoskelet. Disord. 2016, 17, 310. [Google Scholar] [CrossRef] [Green Version]
- Low, R.N.; Austin, M.J.; Ma, J. Fast Spin-Echo Triple Echo Dixon: Initial Clinical Experience with a Novel Pulse Sequence for Simultaneous Fat-Suppressed and Nonfat-Suppressed T2-Weighted Spine Magnetic Resonance Imaging. J. Magn. Reson. Imaging JMRI 2011, 33, 390–400. [Google Scholar] [CrossRef]
- Yang, Q.; Yan, P.; Zhang, Y.; Yu, H.; Shi, Y.; Mou, X.; Kalra, M.K.; Zhang, Y.; Sun, L.; Wang, G. Low-Dose CT Image Denoising Using a Generative Adversarial Network With Wasserstein Distance and Perceptual Loss. IEEE Trans. Med. Imaging 2018, 37, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Kleesiek, J.; Morshuis, J.N.; Isensee, F.; Deike-Hofmann, K.; Paech, D.; Kickingereder, P.; Köthe, U.; Rother, C.; Forsting, M.; Wick, W.; et al. Can Virtual Contrast Enhancement in Brain MRI Replace Gadolinium?: A Feasibility Study. Investig. Radiol. 2019, 54, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Pizer, S.M.; Amburn, E.P.; Austin, J.D.; Cromartie, R.; Geselowitz, A.; Greer, T.; ter Haar Romeny, B.; Zimmerman, J.B.; Zuiderveld, K. Adaptive Histogram Equalization and Its Variations. Comput. Vis. Graph. Image Process. 1987, 39, 355–368. [Google Scholar] [CrossRef]
- Isola, P.; Zhu, J.-Y.; Zhou, T.; Efros, A.A. Image-to-Image Translation with Conditional Adversarial Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- Liu, J.; Hsueh, H.; Hsieh, E.; Chen, J.J. Tests for Equivalence or Non-Inferiority for Paired Binary Data. Stat. Med. 2002, 21, 231–245. [Google Scholar] [CrossRef]
- Cohen, J.P.; Luck, M.; Honari, S. How to Cure Cancer (in Images) with Unpaired Image Translation. 2018. Available online: https://openreview.net/forum?id=SJIA3pijM (accessed on 5 June 2018).
- Lui, K.-J.; Cumberland, W.G. A Test Procedure of Equivalence in Ordinal Data with Matched-Pairs. Biom. J. 2001, 43, 977–983. [Google Scholar] [CrossRef]
- Yang, Y.; Yan, L.-F.; Zhang, X.; Han, Y.; Nan, H.-Y.; Hu, Y.-C.; Hu, B.; Yan, S.-L.; Zhang, J.; Cheng, D.-L.; et al. Glioma Grading on Conventional MR Images: A Deep Learning Study With Transfer Learning. Front. Neurosci. 2018, 12, 804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.; Lu, X.; Yang, L.; Zhang, B.; Yu, D.; Zhao, Y.; Gao, L.; Wu, L.; Zhou, T. Automatic Lung Nodule Detection Using a 3D Deep Convolutional Neural Network Combined with a Multi-Scale Prediction Strategy in Chest CTs. Comput. Biol. Med. 2018, 103, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Du, Q.; Qiang, Y.; Yang, W.; Wang, Y.; Ma, Y.; Zia, M.B. DRGAN: A Deep Residual Generative Adversarial Network for PET Image Reconstruction. IET Image Process. 2020. [CrossRef]
- Smith-Bindman, R.; Kwan, M.L.; Marlow, E.C.; Theis, M.K.; Bolch, W.; Cheng, S.Y.; Bowles, E.J.A.; Duncan, J.R.; Greenlee, R.T.; Kushi, L.H.; et al. Trends in Use of Medical Imaging in US Health Care Systems and in Ontario, Canada, 2000–2016. JAMA 2019, 322, 843–856. [Google Scholar] [CrossRef]
- Tripathy, S.; Kannala, J.; Rahtu, E. Learning Image-to-Image Translation Using Paired and Unpaired Training Samples. In Proceedings of the Computer Vision—ACCV 2018, Perth, Australia, 2–6 December 2018; Jawahar, C.V., Li, H., Mori, G., Schindler, K., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 51–66. [Google Scholar]
- Odena, A.; Dumoulin, V.; Olah, C. Deconvolution and Checkerboard Artifacts. Distill 2016, 1, e3. [Google Scholar] [CrossRef]
- Mirsky, Y.; Mahler, T.; Shelef, I.; Elovici, Y. CT-GAN: Malicious Tampering of 3D Medical Imagery Using Deep Learning; 28th {USENIX} Security Symposium ({USENIX} Security 19); {USENIX} Association: Santa Clara, CA, USA, 2019; pp. 461–478. [Google Scholar]
- Jin, D.; Xu, Z.; Tang, Y.; Harrison, A.P.; Mollura, D.J. CT-Realistic Lung Nodule Simulation from 3D Conditional Generative Adversarial Networks for Robust Lung Segmentation. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2018, Granada, Spain, 16–20 September 2018; Frangi, A.F., Schnabel, J.A., Davatzikos, C., Alberola-López, C., Fichtinger, G., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2018; pp. 732–740. [Google Scholar]
- Quan, T.M.; Nguyen-Duc, T.; Jeong, W.-K. Compressed Sensing MRI Reconstruction Using a Generative Adversarial Network with a Cyclic Loss. IEEE Trans. Med. Imaging 2018, 37, 1488–1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galbusera, F.; Bassani, T.; Casaroli, G.; Gitto, S.; Zanchetta, E.; Costa, F.; Sconfienza, L.M. Generative Models: An Upcoming Innovation in Musculoskeletal Radiology? A Preliminary Test in Spine Imaging. Eur. Radiol. Exp. 2018, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lecler, A.; Duron, L.; Balvay, D.; Savatovsky, J.; Bergès, O.; Zmuda, M.; Farah, E.; Galatoire, O.; Bouchouicha, A.; Fournier, L.S. Combining Multiple Magnetic Resonance Imaging Sequences Provides Independent Reproducible Radiomics Features. Sci. Rep. 2019, 9, 2068. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Jang, H.; Jang, J.; Lee, Y.H.; Hwang, D. Deep-Learned Short Tau Inversion Recovery Imaging Using Multi-Contrast MR Images. Magn. Reson. Med. 2020, 84, 2994–3008; [Google Scholar] [CrossRef]
- Peerlings, J.; Woodruff, H.C.; Winfield, J.M.; Ibrahim, A.; Beers, B.E.V.; Heerschap, A.; Jackson, A.; Wildberger, J.E.; Mottaghy, F.M.; DeSouza, N.M.; et al. Stability of Radiomics Features in Apparent Diffusion Coefficient Maps from a Multi-Centre Test-Retest Trial. Sci. Rep. 2019, 9, 4800. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Yamada, K.; Watanabe, Y.; Matsui, M.; Ida, M.; Fujiwara, S.; Shibata, E. Variability in Absolute Apparent Diffusion Coefficient Values across Different Platforms May Be Substantial: A Multivendor, Multi-Institutional Comparison Study. Radiology 2008, 249, 624–630. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner | Aera | Avanto | Sonata | Symphony | Skyra |
|---|---|---|---|---|---|
| n | 521 | 188 | 7 | 16 | 21 |
| Field strength | 1.5T | 1.5T | 1.5T | 1.5T | 3T |
| Set | Studies | Patients | Sex (Male/Female) | Mean Age |
|---|---|---|---|---|
| Train | 612 | 514 | 284/328 | 60.3 |
| Test | 141 | 133 | 78/63 | 60.1 |
| Pathology | Bone Metastases | Myelopathy | Acute Vertebral Fracture | Spondylodiscitis | Epidural Abscess | Intraspinal Mass | Muscular Lesion |
|---|---|---|---|---|---|---|---|
| n | 41 | 24 | 39 | 42 | 24 | 33 | 26 |
| Rater | Mean Error (in %) | p-Value (Fisher Test) |
|---|---|---|
| 1 | 41 % | 0.008 |
| 2 | 44 % | 0.06 |
| 3 | 58 % | 0.992 |
| 4 | 48 % | 0.336 |
| 5 | 39 % | 0.001 |
| 6 | 45 % | 0.101 |
| Mean STIR | Mean vSTIR | Interrater Agreement STIR | Interrater Agreement vSTIR | Significance (p-Value) for Difference between Interrater Agreements | Significance (p-Value) for Equivalence (δ = 0.10) | Statistical Equivalent (δ = 0.10)? | |
|---|---|---|---|---|---|---|---|
| Hyperintense Vertebral Body | 32% (none) 39% (low) 29% (high) | 37% (none) 39% (low) 24% (high) | 0.61 (p < 0.01) | 0.59 (p < 0.01) | 0.37 | 0.08 | No |
| Vertebral Bone Fractures | 69% (none) 27% (low) 4% (high) | 66% (none) 30% (low) 4% (high) | 0.54 (p < 0.01) | 0.60 (p < 0.01) | 0.32 | 0.01 | Yes |
| Hyperintense Discs | 67% (none) 24% (low) 9% (high) | 71% (none) 20% (low) 9% (high) | 0.39 (p < 0.01) | 0.35 (p < 0.01) | 0.23 | 0.01 | Yes |
| Real STIR | 57% | 51% | 0.02 (p = 0.70) | <0.01 (p = 0.96) | 0.66 | 0.42 | No |
| Intraspinal Mass | 17% | 12% | 0.34 (p < 0.01) | 0.24 (p < 0.01) | 0.03 | 0.038 | Yes |
| Myelopathy | 19% | 17% | 0.63 (p < 0.01) | 0.66 (p < 0.01) | 0.57 | 0.001 | Yes |
| Muscular Edema | 26% | 26% | 0.52 (p < 0.01) | 0.43 (p < 0.01) | 0.07 | 0.001 | Yes |
| Spondylodiscitis | 21% | 22% | 0.66 (p < 0.01) | 0.59 (p < 0.01) | 0.13 | 0.003 | Yes |
| Epidural Abscess | 12% | 9% | 0.54 (p < 0.01) | 0.41 (p < 0.01) | <0.01 | 0.003 | Yes |
| Muscular Abscess | 8% | 7% | 0.31 (p < 0.01) | 0.39 (p < 0.01) | 0.13 | 0.004 | Yes |
| Bone Metastases | 22% | 17% | 0.64 (p < 0.01) | 0.56 (p < 0.01) | 0.07 | 0.055 | No |
| Intraspinal Neoplasia | 9% | 6% | 0.45 (p < 0.01) | 0.45 (p < 0.01) | 0.93 | <0.001 | Yes |
| Acute Traumatic Fracture | 13% | 13% | 0.79 (p < 0.01) | 0.58 (p < 0.01) | <0.01 | <0.001 | Yes |
| Pathological Fracture | 8% | 7% | 0.46 (p < 0.01) | 0.19 (p < 0.01) | <0.01 | <0.001 | Yes |
| Benign Bone Neoplasia | 2% | 2% | 0.12 (p < 0.01) | 0.43 (p < 0.01) | <0.01 | <0.001 | Yes |
| Normal | 16% | 17% | 0.70 (p < 0.01) | 0.60 (p < 0.01) | 0.03 | 0.004 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haubold, J.; Demircioglu, A.; Theysohn, J.M.; Wetter, A.; Radbruch, A.; Dörner, N.; Schlosser, T.W.; Deuschl, C.; Li, Y.; Nassenstein, K.; et al. Generating Virtual Short Tau Inversion Recovery (STIR) Images from T1- and T2-Weighted Images Using a Conditional Generative Adversarial Network in Spine Imaging. Diagnostics 2021, 11, 1542. https://doi.org/10.3390/diagnostics11091542
Haubold J, Demircioglu A, Theysohn JM, Wetter A, Radbruch A, Dörner N, Schlosser TW, Deuschl C, Li Y, Nassenstein K, et al. Generating Virtual Short Tau Inversion Recovery (STIR) Images from T1- and T2-Weighted Images Using a Conditional Generative Adversarial Network in Spine Imaging. Diagnostics. 2021; 11(9):1542. https://doi.org/10.3390/diagnostics11091542
Chicago/Turabian StyleHaubold, Johannes, Aydin Demircioglu, Jens Matthias Theysohn, Axel Wetter, Alexander Radbruch, Nils Dörner, Thomas Wilfried Schlosser, Cornelius Deuschl, Yan Li, Kai Nassenstein, and et al. 2021. "Generating Virtual Short Tau Inversion Recovery (STIR) Images from T1- and T2-Weighted Images Using a Conditional Generative Adversarial Network in Spine Imaging" Diagnostics 11, no. 9: 1542. https://doi.org/10.3390/diagnostics11091542