
Dose Reduction in Coronary Artery Calcium Scoring Using Mono-Energetic Images from Reduced Tube Voltage Dual-Source Photon-Counting CT Data: A Dynamic Phantom Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Radiation Dose
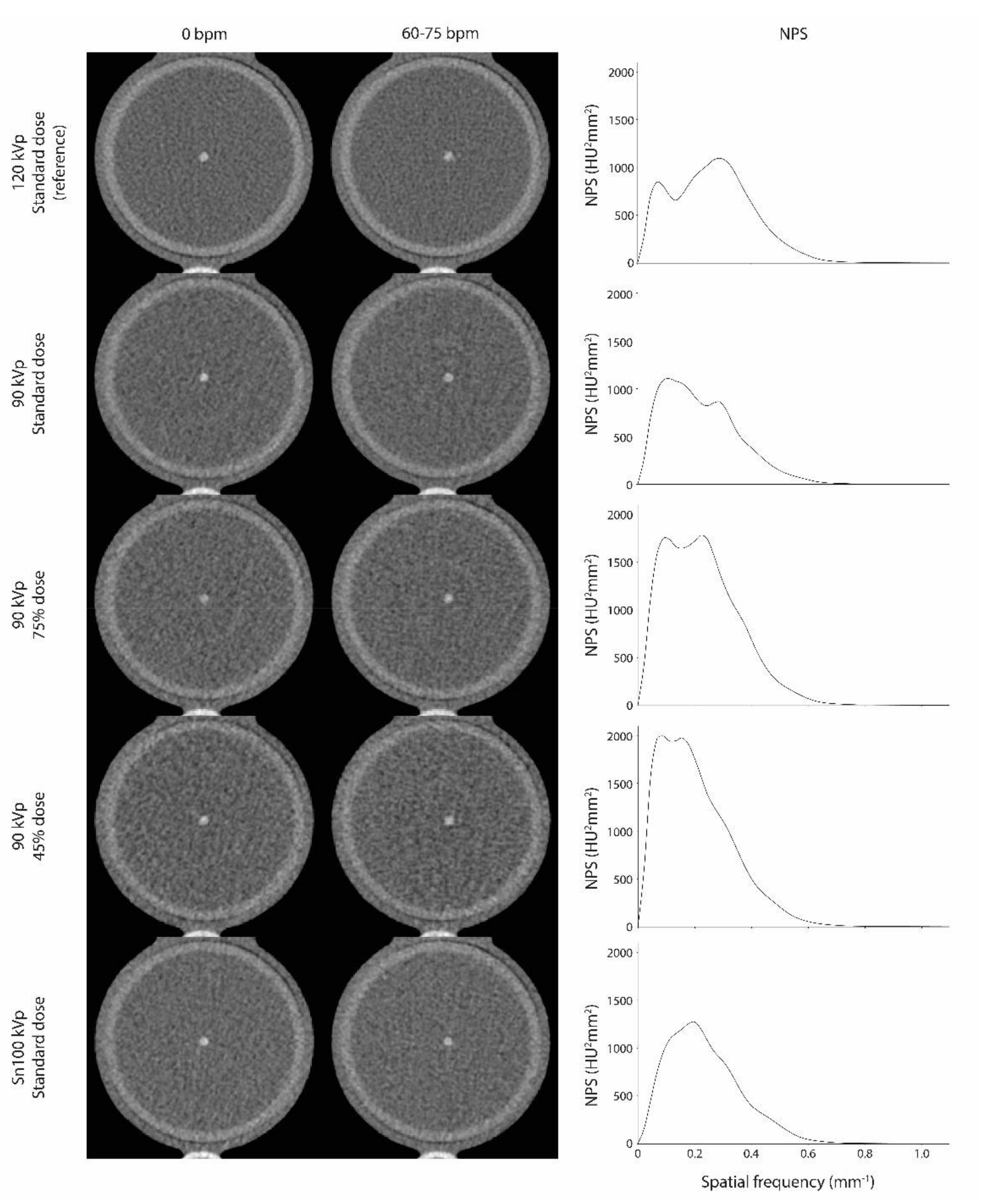
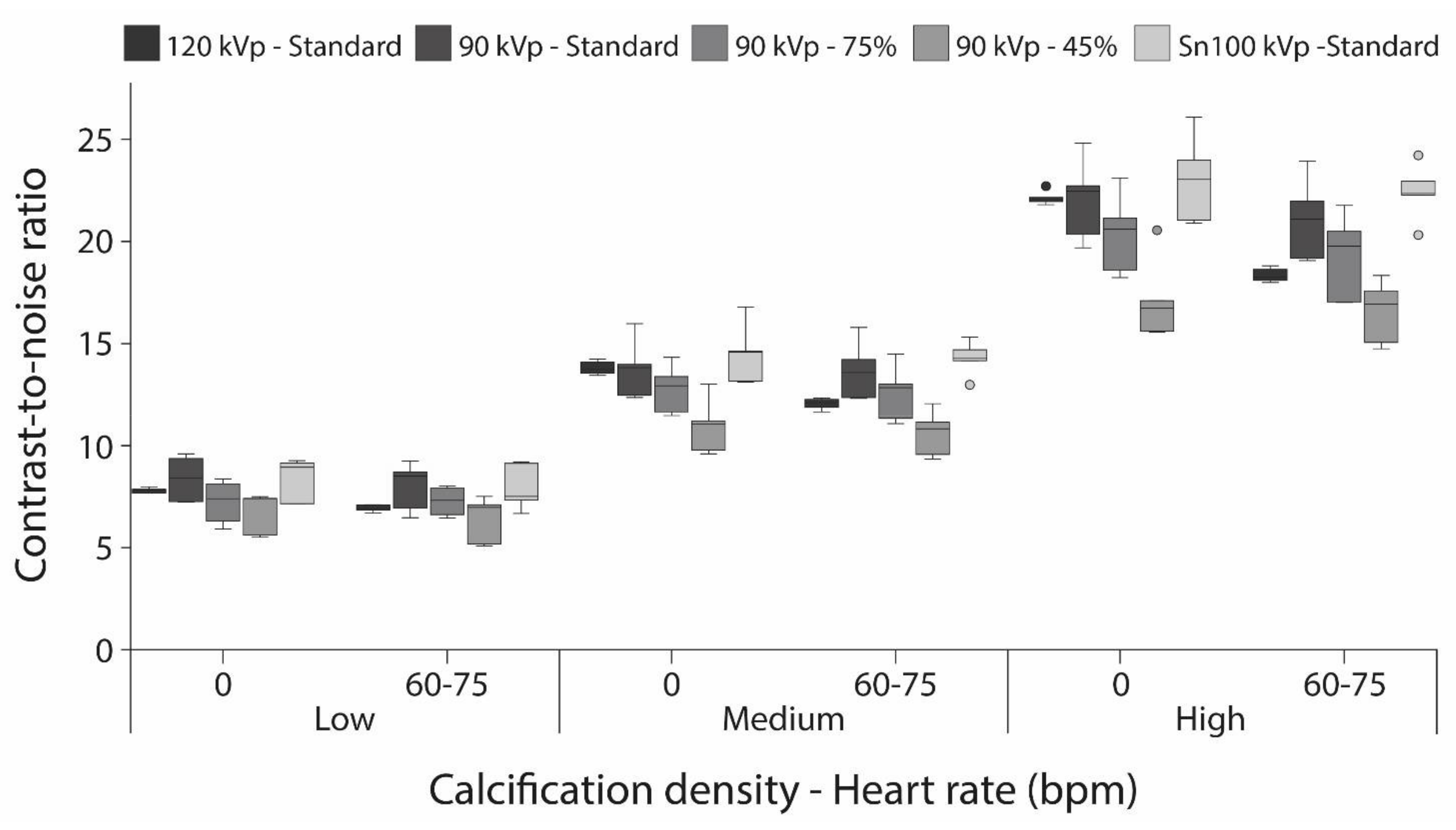
3.2. Image Quality
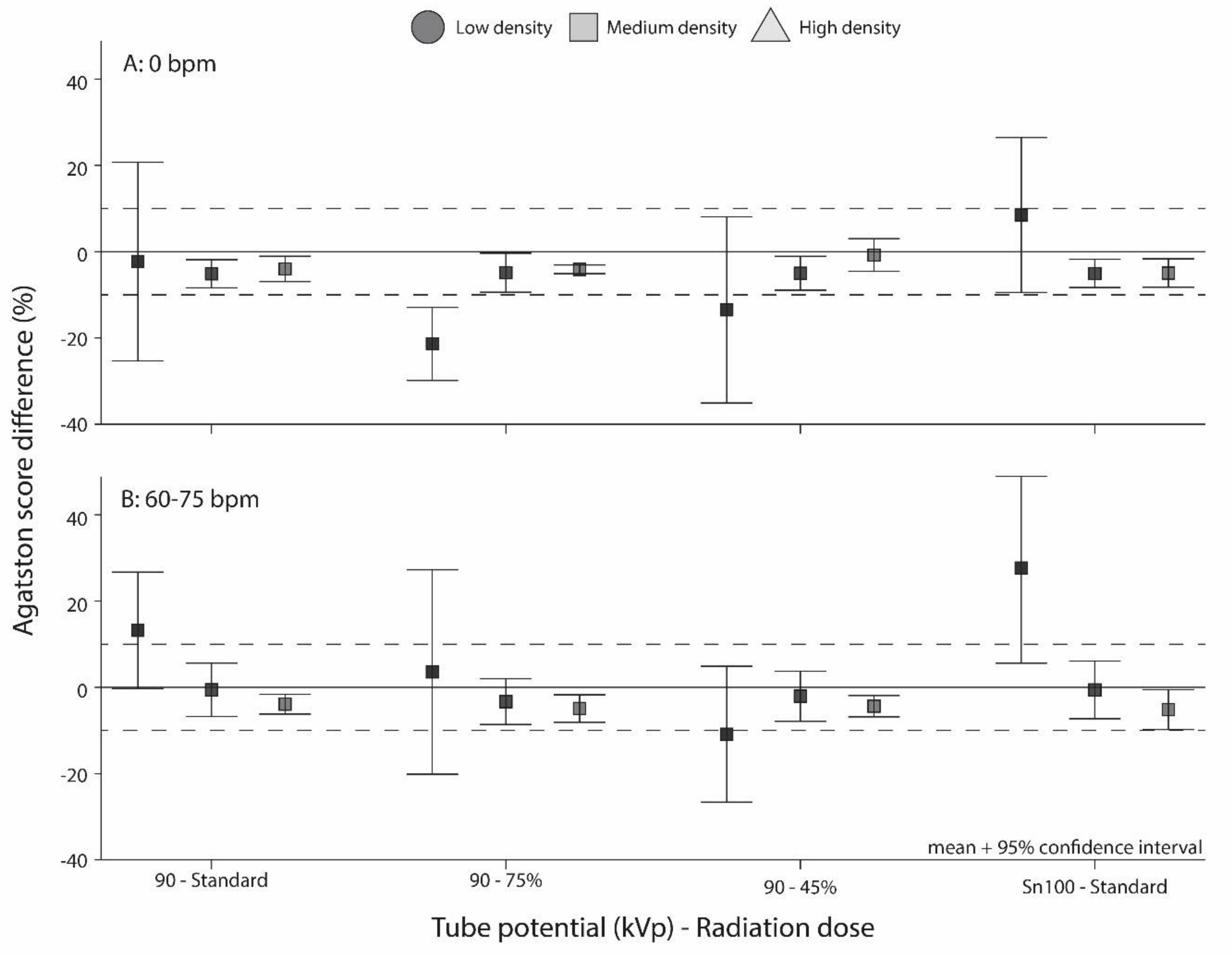
3.3. Influence on Agatston Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; Coggeshall, M.; et al. Global, Regional, and National Life Expectancy, All-Cause Mortality, and Cause-Specific Mortality for 249 Causes of Death, 1980–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality From Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M.; Detrano, R. Quantification of Coronary Artery Calcium Using Ultrafast Computed Tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Goff, D.C.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 49–76. [Google Scholar] [CrossRef] [Green Version]
- Greenland, P.; Alpert, J.S.; Beller, G.A.; Benjamin, E.J.; Budoff, M.J.; Fayad, Z.A.; Foster, E.; Hlatky, M.A.; Hodgson, J.M.B.; Kushner, F.G.; et al. 2010 ACCF/AHA Guideline for Assessment of Cardiovascular Risk in Asymptomatic Adults: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2010, 122, 2748–2764. [Google Scholar] [CrossRef] [PubMed]
- Hecht, H.; Blaha, M.J.; Berman, D.S.; Nasir, K.; Budoff, M.; Leipsic, J.; Blankstein, R.; Narula, J.; Rumberger, J.; Shaw, L.J. Clinical Indications for Coronary Artery Calcium Scoring in Asymptomatic Patients: Expert Consensus Statement from the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2017, 11, 157–168. [Google Scholar] [CrossRef]
- Budoff, M.J.; Achenbach, S.; Blumenthal, R.S.; Carr, J.J.; Goldin, J.G.; Greenland, P.; Guerci, A.D.; Lima, J.A.C.; Rader, D.J.; Rubin, G.D.; et al. Assessment of Coronary Artery Disease by Cardiac Computed Tomography: A Scientific Statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on C. Circulation 2006, 114, 1761–1791. [Google Scholar] [CrossRef] [Green Version]
- Blaha, M.J.; Mortensen, M.B.; Kianoush, S.; Tota-Maharaj, R.; Cainzos-Achirica, M. Coronary Artery Calcium Scoring: Is It Time for a Change in Methodology? JACC Cardiovasc. Imaging 2017, 10, 923–937. [Google Scholar] [CrossRef] [PubMed]
- Vonder, M.; van der Werf, N.R.; Leiner, T.; Greuter, M.J.W.; Fleischmann, D.; Vliegenthart, R.; Oudkerk, M.; Willemink, M.J. The Impact of Dose Reduction on the Quantification of Coronary Artery Calcifications and Risk Categorization: A Systematic Review. J. Cardiovasc. Comput. Tomogr. 2018, 12, 352–363. [Google Scholar] [CrossRef]
- Gräni, C.; Vontobel, J.; Benz, D.C.; Bacanovic, S.; Giannopoulos, A.A.; Messerli, M.; Grossmann, M.; Gebhard, C.; Pazhenkottil, A.P.; Gaemperli, O.; et al. Ultra-Low-Dose Coronary Artery Calcium Scoring Using Novel Scoring Thresholds for Low Tube Voltage Protocols—A Pilot Study. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1362–1371. [Google Scholar] [CrossRef] [PubMed]
- Vonder, M.; Pelgrim, G.J.; Huijsse, S.E.M.; Meyer, M.; Greuter, M.J.W.; Henzler, T.; Flohr, T.G.; Oudkerk, M.; Vliegenthart, R. Feasibility of Spectral Shaping for Detection and Quantification of Coronary Calcifications in Ultra-Low Dose CT. Eur. Radiol. 2017, 27, 2047–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwan, M.; Mettin, C.; Pflederer, T.; Seltmann, M.; Schuhbäck, A.; Muschiol, G.; Ropers, D.; Daniel, W.G.; Achenbach, S. Very Low-Dose Coronary Artery Calcium Scanning with High-Pitch Spiral Acquisition Mode: Comparison between 120-KV and 100-KV Tube Voltage Protocols. J. Cardiovasc. Comput. Tomogr. 2013, 7, 32–38. [Google Scholar] [CrossRef]
- Nakazato, R.; Dey, D.; Gutstein, A.; Le Meunier, L.; Cheng, V.Y.; Pimentel, R.; Paz, W.; Hayes, S.W.; Thomson, L.E.J.; Friedman, J.D.; et al. Coronary Artery Calcium Scoring Using a Reduced Tube Voltage and Radiation Dose Protocol with Dual-Source Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2009, 3, 394–400. [Google Scholar] [CrossRef]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-Counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Leng, S.; Bruesewitz, M.; Tao, S.; Rajendran, K.; Halaweish, A.F.; Campeau, N.G.; Fletcher, J.G.; McCollough, C.H. Photon-Counting Detector CT: System Design and Clinical Applications of an Emerging Technology. Radiographics 2019, 39, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Si-Mohamed, S.; Bar-Ness, D.; Sigovan, M.; Cormode, D.P.; Coulon, P.; Coche, E.; Vlassenbroek, A.; Normand, G.; Boussel, L.; Douek, P. Review of an Initial Experience with an Experimental Spectral Photon-Counting Computed Tomography System. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2017, 873, 27–35. [Google Scholar] [CrossRef]
- Si-Mohamed, S.; Bar-Ness, D.; Sigovan, M.; Tatard-Leitman, V.; Cormode, D.P.; Naha, P.C.; Coulon, P.; Rascle, L.; Roessl, E.; Rokni, M.; et al. Multicolour Imaging with Spectral Photon-Counting CT: A Phantom Study. Eur. Radiol. Exp. 2018, 2, 34. [Google Scholar] [CrossRef]
- Taguchi, K.; Iwanczyk, J.S. Vision 20/20: Single Photon Counting x-Ray Detectors in Medical Imaging. Med. Phys. 2013, 40, 100901. [Google Scholar] [CrossRef]
- Sandfort, V.; Persson, M.; Pourmorteza, A.; Noël, P.B.; Fleischmann, D.; Willemink, M.J. Spectral Photon-Counting CT in Cardiovascular Imaging. J. Cardiovasc. Comput. Tomogr. 2020, 15, 218–225. [Google Scholar] [CrossRef]
- Greffier, J.; Frandon, J. Spectral Photon-Counting CT System: Toward Improved Image Quality Performance in Conventional and Spectral CT Imaging. Diagn. Interv. Imaging 2021, 102, 271–272. [Google Scholar] [CrossRef] [PubMed]
- van der Werf, N.R.; Si-Mohamed, S.; Rodesch, P.A.; van Hamersvelt, R.W.; Greuter, M.J.W.; Boccalini, S.; Greffier, J.; Leiner, T.; Boussel, L.; Willemink, M.J.; et al. Coronary Calcium Scoring Potential of Large Field-of-View Spectral Photon-Counting CT: A Phantom Study. Eur. Radiol. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.H.; Ulzheimer, S.; Halliburton, S.S.; Shanneik, K.; White, R.D.; Kalender, W.A. Coronary Artery Calcium: A Multi-Institutional, Multimanufacturer International Standard for Quantification at Cardiac CT. Radiology 2007, 243, 527–538. [Google Scholar] [CrossRef]
- Husmann, L.; Leschka, S.; Desbiolles, L.; Schepis, T.; Gaemperli, O.; Seifert, B.; Cattin, P.; Frauenfelder, T.; Flohr, T.G.; Marincek, B.; et al. Coronary Artery Motion and Cardiac Phases: Dependency on Heart Rate—Implications for CT Image Reconstruction. Radiology 2007, 245, 567–576. [Google Scholar] [CrossRef] [Green Version]
- Van der Werf, N.R.; Willemink, M.J.; Willems, T.P.; Vliegenthart, R.; Greuter, M.J.W.; Leiner, T. Influence of Heart Rate on Coronary Calcium Scores: A Multi-Manufacturer Phantom Study. Int. J. Cardiovasc. Imaging 2017, 34, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Van Praagh, G.D.; van der Werf, N.R.; Wang, J.; van Ommen, F.; Poelhekken, K.; Slart, R.H.; Fleischmann, D.; Greuter, M.J.; Leiner, T.; Willemink, M.J. Fully Automated Quantification Method (FQM) of Coronary Calcium in an Anthropomorphic Phantom. Med. Phys. 2021. [Google Scholar] [CrossRef] [PubMed]
- Booij, R.; van der Werf, N.R.; Budde, R.P.J.; Bos, D.; van Straten, M. Dose Reduction for CT Coronary Calcium Scoring with a Calcium-Aware Image Reconstruction Technique: A Phantom Study. Eur. Radiol. 2020, 30, 3346–3355. [Google Scholar] [CrossRef] [Green Version]
- Funabashi, N.; Irie, R.; Namihira, Y.; Morimoto, R.; Aiba, M.; Ozawa, K.; Takaoka, H.; Ohta, J.; Masuda, Y.; Kobayashi, Y. Influence of Tube Voltage and Heart Rate on the Agatston Calcium Score Using an in Vitro, Novel ECG-Gated Dual Energy Reconstruction 320 Slice CT Technique. Int. J. Cardiol. 2015, 180, 218–220. [Google Scholar] [CrossRef]
- Funabashi, N.; Koide, K.; Mizuno, N.; Nagamura, K.; Ochi, S.; Yanagawa, N.; Okamoto, Y.; Uno, K.; Komuro, I. Influence of Heart Rate on the Detectability and Reproducibility of Multislice Computed Tomography for Measuring Coronary Calcium Score Using a Pulsating Calcified Mock-Vessel in Comparison with Electron Beam Tomography. Int. J. Cardiol. 2006, 113, 113–117. [Google Scholar] [CrossRef]
- Rutten, A.; Isgum, I.; Prokop, M. Coronary Calcification: Effect of Small Variation of Scan Starting Position on Agatston, Volume, and Mass Scores. Radiology 2008, 246, 90–98. [Google Scholar] [CrossRef]
- Groen, J.M.; Greuter, M.J.; Schmidt, B.; Suess, C.; Vliegenthart, R.; Oudkerk, M. The Influence of Heart Rate, Slice Thickness, and Calcification Density on Calcium Scores Using 64-Slice Multidetector Computed Tomography: A Systematic Phantom Study. Investig. Radiol. 2007, 42, 848–855. [Google Scholar] [CrossRef]
- Schlosser, T.; Hunold, P.; Voigtländer, T.; Schmermund, A.; Barkhausen, J. Coronary Artery Calcium Scoring: Influence of Reconstruction Interval and Reconstruction Increment Using 64-MDCT. Am. J. Roentgenol. 2007, 188, 1063–1068. [Google Scholar] [CrossRef]
- Willemink, M.J.; Abramiuc, B.; den Harder, A.M.; van der Werf, N.R.; de Jong, P.A.; Budde, R.P.J.; Wildberger, J.E.; Vliegenthart, R.; Willems, T.P.; Greuter, M.J.W.; et al. Coronary Calcium Scores Are Systematically Underestimated at a Large Chest Size: A Multivendor Phantom Study. J. Cardiovasc. Comput. Tomogr. 2015, 9, 415–421. [Google Scholar] [CrossRef]
- Detrano, R.C.; Anderson, M.; Nelson, J.; Wong, N.D.; Carr, J.J.; McNitt-Gray, M.; Bild, D.E. Coronary Calcium Measurements: Effect of CT Scanner Type and Calcium Measure on Rescan Reproducibility—MESA Study. Radiology 2005, 236, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Tigges, S.; Arepalli, C.D.; Tridandapani, S.; Oshinski, J.; Kurz, C.R.; Richer, E.J.; Chen, Z.; Stillman, A.E.; Raggi, P. A Phantom Study of the Effect of Heart Rate, Coronary Artery Displacement and Vessel Trajectory on Coronary Artery Calcium Score: Potential for Risk Misclassification. J. Cardiovasc. Comput. Tomogr. 2012, 6, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.K.; Mühlenbruch, G.; Wildberger, J.E.; Hohl, C.; Das, M.; Günther, R.W.; Mahnken, A.H. Coronary Artery Calcium Scoring with Multislice Computed Tomography: In Vitro Assessment of a Low Tube Voltage Protocol. Investig. Radiol. 2006, 41, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Eberhard, M.; Mergen, V.; Higashigaito, K.; Allmendinger, T.; Manka, R.; Flohr, T.; Schmidt, B.; Euler, A.; Alkadhi, H. Coronary Calcium Scoring with First Generation Dual-Source Photon-Counting CT-First Evidence from Phantom and In-Vivo Scans. Diagnostics 2021, 11, 1708. [Google Scholar] [CrossRef]
- Hong, C.; Pilgram, T.K.; Zhu, F.; Bae, K.T. Is Coronary Artery Calcium Mass Related to Agatston Score? Acad. Radiol. 2004, 11, 286–292. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Reference Scan | 90 kVp Standard Dose | 90 kVp 75% Dose | 90 kVp 45% Dose | Sn100 kVp Standard Dose |
|---|---|---|---|---|---|
| CT system | PCCT | PCCT | PCCT | PCCT | PCCT |
| Technique | Axial | Axial | Axial | Axial | Axial |
| Tube voltage (kVp) | 120 | 90 | 90 | 90 | 100 + Sn filter |
| Effective tube current time product (mAs) | 20 1 | 45 1 | 34 | 20 | 134 1 |
| Automatic exposure control | Off | Off | Off | Off | Off |
| Collimation (mm) | 144 × 0.4 | 144 × 0.4 | 144 × 0.4 | 144 × 0.4 | 144 × 0.4 |
| Field of view (mm) | 220 | 220 | 220 | 220 | 220 |
| Rotation time (s) | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 |
| Slice thickness/increment (mm) | 3.0/1.5 | 3.0/1.5 | 3.0/1.5 | 3.0/1.5 | 3.0/1.5 |
| Reconstruction kernel | Qr36 | Qr36 | Qr36 | Qr36 | Qr36 |
| Matrix size (pixels) | 512 × 512 | 512 × 512 | 512 × 512 | 512 × 512 | 512 × 512 |
| Reconstruction | FBP 2 | FBP 2 | FBP 2 | FBP 2 | FBP 2 |
| monoE level (keV) | 70 | 70 | 70 | 70 | 70 |
| Repetitions | 5 | 5 | 5 | 5 | 5 |
| Phantom speed | 0 & 20 mm/s | 0 & 20 mm/s | 0 & 20 mm/s | 0 & 20 mm/s | 0 & 20 mm/s |
| CTDIvol (mGy) | 4.06 | 2.97 | 2.26 | 1.33 | 2.21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Werf, N.R.; van Gent, M.; Booij, R.; Bos, D.; van der Lugt, A.; Budde, R.P.J.; Greuter, M.J.W.; van Straten, M. Dose Reduction in Coronary Artery Calcium Scoring Using Mono-Energetic Images from Reduced Tube Voltage Dual-Source Photon-Counting CT Data: A Dynamic Phantom Study. Diagnostics 2021, 11, 2192. https://doi.org/10.3390/diagnostics11122192
van der Werf NR, van Gent M, Booij R, Bos D, van der Lugt A, Budde RPJ, Greuter MJW, van Straten M. Dose Reduction in Coronary Artery Calcium Scoring Using Mono-Energetic Images from Reduced Tube Voltage Dual-Source Photon-Counting CT Data: A Dynamic Phantom Study. Diagnostics. 2021; 11(12):2192. https://doi.org/10.3390/diagnostics11122192
Chicago/Turabian Stylevan der Werf, Niels R., Margo van Gent, Ronald Booij, Daniel Bos, Aad van der Lugt, Ricardo P. J. Budde, Marcel J. W. Greuter, and Marcel van Straten. 2021. "Dose Reduction in Coronary Artery Calcium Scoring Using Mono-Energetic Images from Reduced Tube Voltage Dual-Source Photon-Counting CT Data: A Dynamic Phantom Study" Diagnostics 11, no. 12: 2192. https://doi.org/10.3390/diagnostics11122192