The Performance of Deep Learning Algorithms on Automatic Pulmonary Nodule Detection and Classification Tested on Different Datasets That Are Not Derived from LIDC-IDRI: A Systematic Review

 and
and
Abstract
:1. Introduction
2. Materials and Methods
Literature Search Strategy
3. Study Inclusion Criteria
- 1
- If the technology was based on deep learning or had primary components of deep learning algorithms used to either detect pulmonary nodules and/or classify these nodules into different categories,and
- 2
- if the deep learning algorithm was tested on CT scans that were not part of or derived from the LIDC-IDRI database,and
- 3
- if any performance measures were reported, preferably in the form of, but not limited to sensitivity, specificity, accuracy, and/or AUC.
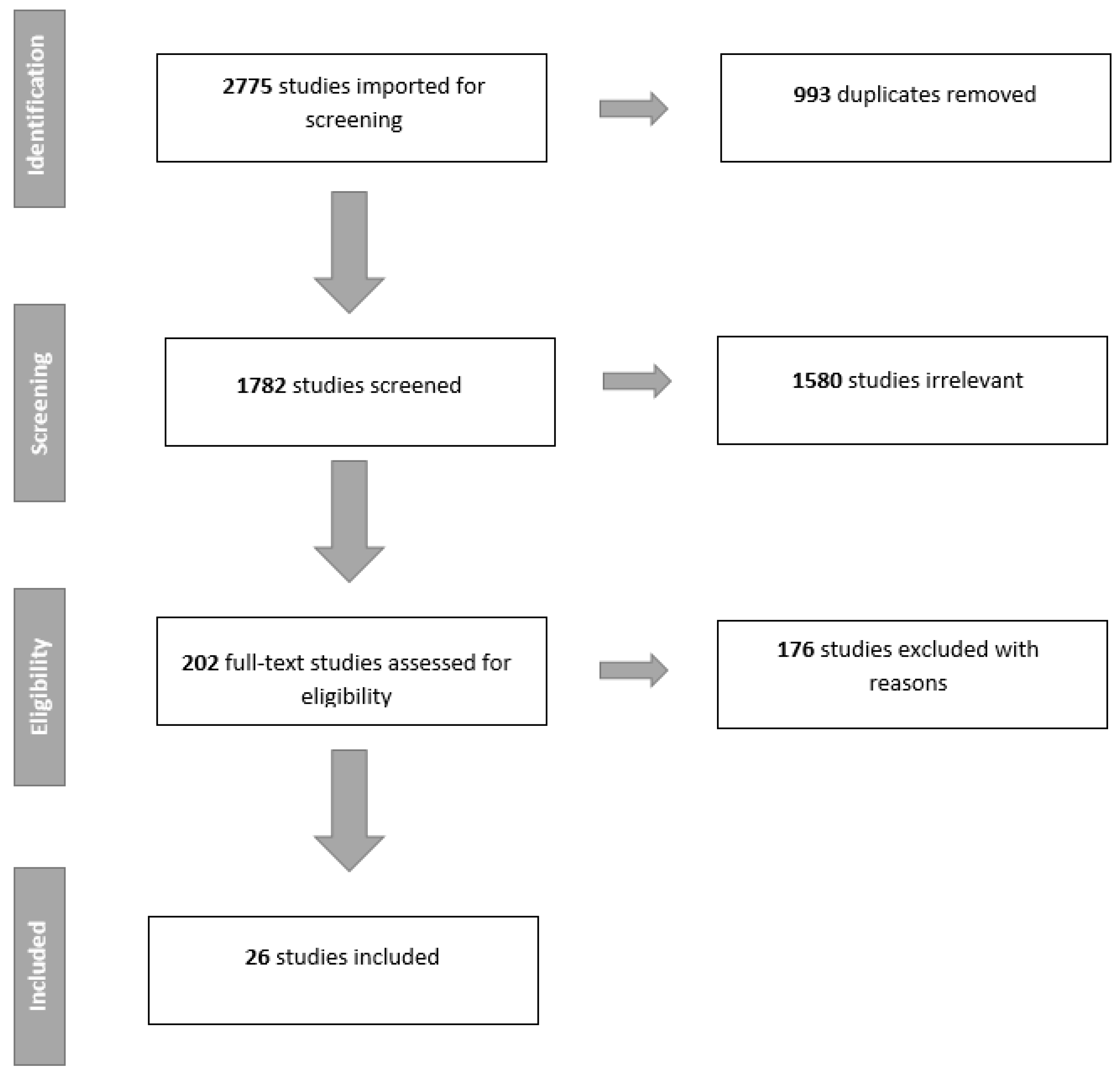
4. Literature Search Results
5. Detection Only (3 Studies)
6. Classification Only (16 Studies)
7. Both Detection and Classification (7 Studies)
8. Discussion
9. Conclusions
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Data Explorer ECIS. Available online: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-AE28E$2-All$4-1,2$3-All$6-0,14$5-2008,2008$7-8$CEstByCancer$X0_8-3$CEstRelativeCanc$X1_8-3$X1_9-AE28 (accessed on 5 August 2008).
- Fontana, R.S. The Mayo Lung Project: A perspective. Cancer 2000, 89, 2352–2355. [Google Scholar] [CrossRef]
- Oken, M.M.; Hocking, W.G.; Kvale, P.A.; Andriole, G.L.; Buys, S.S.; Church, T.R.; Crawford, E.D.; Fouad, M.N.; Isaacs, C.; Reding, D.J.; et al. Screening by chest radiograph and lung cancer mortality: The Prostate, Lung, Colorectal, and Ovarian (PLCO) randomized trial. JAMA 2011, 306, 1865–1873. [Google Scholar] [CrossRef]
- Gillaspie, E.A.; Allen, M.S. Computed tomographic screening for lung cancer: The Mayo Clinic experience. Thorac. Surg. Clin. 2015, 25, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Krupinski, E.A.; Berbaum, K.S.; Caldwell, R.T.; Schartz, K.M.; Madsen, M.T.; Kramer, D.J. Do Long Radiology Workdays Impact Nodule Detection in Dynamic CT Interpretation? J. Am. Coll. Radiol. 2012, 9, 191–198. [Google Scholar] [CrossRef]
- Sokolovskaya, E.; Shinde, T.; Ruchman, R.B.; Kwak, A.J.; Lu, S.; Shariff, Y.K.; Wiggins, E.F.; Talangbayan, L. The Effect of Faster Reporting Speed for Imaging Studies on the Number of Misses and Interpretation Errors: A Pilot Study. J. Am. Coll. Radiol. 2015, 12, 683–688. [Google Scholar] [CrossRef]
- Ozekes, S.; Osman, O. Computerized lung nodule detection using 3D feature extraction and learning based algorithms. J. Med. Syst. 2010, 34, 185–194. [Google Scholar] [CrossRef]
- Armato, S.G., 3rd; Li, F.; Giger, M.L.; MacMahon, H.; Sone, S.; Doi, K. Lung cancer: Performance of automated lung nodule detection applied to cancers missed in a CT screening program. Radiology 2002, 225, 685–692. [Google Scholar] [CrossRef]
- Huang, P.; Park, S.; Yan, R.; Lee, J.; Chu, L.C.; Lin, C.T.; Hussien, A.; Rathmell, J.; Thomas, B.; Chen, C.; et al. Added Value of Computer-aided CT Image Features for Early Lung Cancer Diagnosis with Small Pulmonary Nodules: A Matched Case-Control Study. Radiology 2018, 286, 286–295. [Google Scholar] [CrossRef]
- Revel, M.P.; Merlin, A.; Peyrard, S.; Triki, R.; Couchon, S.; Chatellier, G.; Frija, G. Software volumetric evaluation of doubling times for differentiating benign versus malignant pulmonary nodules. AJR Am. J. Roentgenol. 2006, 187, 135–142. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural Networks. In Proceedings of the Neural Information Processing Systems 25 (NIPS), Lake Tahoe, CA, USA, 3–6 December 2012. [Google Scholar]
- Chen, G.-L.; Zhang, J.-J.; Zhuo, D.-Y.; Pan, Y.-N.; Pang, C.-Y. Identification of pulmonary nodules via CT images with hierarchical fully convolutional networks. Med Biol. Eng. Comput. 2019, 57, 1567–1580. [Google Scholar] [CrossRef] [PubMed]
- Savaş, S.; Topaloğlu, N.; Kazcı, Ö.; Koşar, P.N. Classification of Carotid Artery Intima Media Thickness Ultrasound Images with Deep Learning. J. Med. Syst. 2019, 43, 273. [Google Scholar] [CrossRef] [PubMed]
- Azizpour, H.; Razavian, A.S.; Sullivan, J.; Maki, A.; Carlsson, S. From Generic to Specific Deep Representations for Visual Recognition, 2014. [CrossRef]
- Armato, S.G.; McLennan, G.; Bidaut, L.; McNitt-Gray, M.F.; Meyer, C.R.; Reeves, A.P.; Zhao, B.; Aberle, D.R.; Henschke, C.I.; Hoffman, E.A.; et al. The Lung Image Database Consortium (LIDC) and Image Database Resource Initiative (IDRI): A completed reference database of lung nodules on CT scans. Med. Phys. 2011, 38, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, Z.; Huang, H.; Lin, M.; Luo, D.-H. Evaluating the performance of a deep learning-based computer-aided diagnosis (DL-CAD) system for detecting and characterizing lung nodules: Comparison with the performance of double reading by radiologists. Thorac. Cancer 2019, 10, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Setio, A.A.A.; Ciompi, F.; Litjens, G.; Gerke, P.; Jacobs, C.; Van Riel, S.J.; Wille, M.M.W.; Naqibullah, M.; Sanchez, C.I.; Van Ginneken, B. Pulmonary Nodule Detection in CT Images: False Positive Reduction Using Multi-View Convolutional Networks. IEEE Trans. Med Imaging 2016, 35, 1160–1169. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K. A supervised ‘lesion-enhancement’ filter by use of a massive-training artificial neural network (MTANN) in computer-aided diagnosis (CAD). Phys. Med. Biol. 2009, 54. [Google Scholar] [CrossRef]
- Tajbakhsh, N.; Suzuki, K. Comparing two classes of end-to-end machine-learning models in lung nodule detection and classification: MTANNs vs. CNNs. Pattern Recognit. 2017, 63, 476–486. [Google Scholar] [CrossRef]
- Masood, A.; Sheng, B.; Li, P.; Hou, X.-H.; Wei, X.-E.; Qin, J.; Feng, D.-G. Computer-Assisted Decision Support System in Pulmonary Cancer detection and stage classification on CT images. J. Biomed. Inform. 2018, 79, 117–128. [Google Scholar] [CrossRef]
- Chen, S.-H.; Guo, J.-X.; Wang, C.-D.; Xu, X.-X.; Yi, Z.; Li, W.-M. DeepLNAnno: A Web-Based Lung Nodules Annotating System for CT Images. J. Med. Syst. 2019, 43. [Google Scholar] [CrossRef]
- Liao, F.-Z.; Liang, M.; Li, Z.; Hu, X.-L.; Song, S. Evaluate the Malignancy of Pulmonary Nodules Using the 3-D Deep Leaky Noisy-or Network. IEEE Trans. Neural Netw. Learn. Syst. 2019, 30, 3484–3494. [Google Scholar] [CrossRef]
- Liu, M.-Z.; Jiang, X.; Liu, Y.-H.; Zhao, F.-X.; Zhou, H.-L. A semi-supervised convolutional transfer neural network for 3D pulmonary nodules detection. Neurocomputing 2019, in press. [Google Scholar] [CrossRef]
- Wang, Y.; Yan, F.-R.; Lu, X.-F.; Zheng, G.-M.; Zhang, X.; Wang, C.; Zhou, K.-F.; Zhang, Y.-W.; Li, H.; Zhao, Q.; et al. IILS: Intelligent imaging layout system for automatic imaging report standardization and intra-interdisciplinary clinical workflow optimization. EBioMedicine 2019, 44, 162–181. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, J.-W.; Wen, Y.-F.; Lu, H.-B.; Niu, T.-Y.; Pan, J.-F.; Qian, D.-H. Pulmonary Nodule Detection in Volumetric Chest CT Scans Using CNNs-Based Nodule-Size-Adaptive Detection and Classification. IEEE Access 2019, 7, 46033–46044. [Google Scholar] [CrossRef]
- Alakwaa, W.; Nassef, M.; Badr, A. Lung Cancer Detection and Classification with 3D Convolutional Neural Network (3D-CNN). Int. J. Adv. Comput. Sci. Appl. 2017, 8. [Google Scholar] [CrossRef]
- Ciompi, F.; de Hoop, B.; van Riel, S.J.; Chung, K.; Scholten, E.T.; Oudkerk, M.; de Jong, P.A.; Prokop, M.; van Ginneken, B. Automatic classification of pulmonary peri-fissural nodules in computed tomography using an ensemble of 2D views and a convolutional neural network out-of-the-box. Med. Image Anal. 2015, 26, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Ciompi, F.; Chung, K.; Van Riel, S.J.; Setio, A.A.A.; Gerke, P.K.; Jacobs, C.; Th Scholten, E.; Schaefer-Prokop, C.; Wille, M.M.W.; Marchianò, A.; et al. Towards automatic pulmonary nodule management in lung cancer screening with deep learning. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef]
- Jakimovski, G.; Davcev, D. Using Double Convolution Neural Network for Lung Cancer Stage Detection. Appl. Sci. 2019, 9, 427. [Google Scholar] [CrossRef]
- Lakshmanaprabu, S.K.; Mohanty, S.N.; Shankar, K.; Arunkumar, N.; Ramirez, G. Optimal deep learning model for classification of lung cancer on CT images. Future Gener. Comput. Syst. 2019, 92, 374–382. [Google Scholar] [CrossRef]
- Liu, S.; Xie, Y.-T.; Jirapatnakul, A.; Reeves, A.P. Pulmonary nodule classification in lung cancer screening with three-dimensional convolutional neural networks. J. Med. Imaging 2017, 4, 1. [Google Scholar] [CrossRef]
- Liu, X.-L.; Hou, F.; Qin, H.; Hao, A. Multi-view multi-scale CNNs for lung nodule type classification from CT images. Pattern Recognit. 2018, 77, 262–275. [Google Scholar] [CrossRef]
- Nishio, M.; Sugiyama, O.; Yakami, M.; Ueno, S.; Kubo, T.; Kuroda, T.; Togashi, K. Computer-aided diagnosis of lung nodule classification between benign nodule, primary lung cancer, and metastatic lung cancer at different image size using deep convolutional neural network with transfer learning. PLoS ONE 2018, 13, e0200721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onishi, Y.; Teramoto, A.; Tsujimoto, M.; Tsukamoto, T.; Saito, K.; Toyama, H.; Imaizumi, K.; Fujita, H. Automated Pulmonary Nodule Classification in Computed Tomography Images Using a Deep Convolutional Neural Network Trained by Generative Adversarial Networks. BioMed Res. Int. 2019, 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polat, H.; Mehr, H.D. Classification of pulmonary CT images by using hybrid 3D-deep convolutional neural network architecture. Appl. Sci. (Switz.) 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Qiang, Y.; Ge, L.; Zhao, X.; Zhang, X.-L.; Tang, X.-X. Pulmonary nodule diagnosis using dual-modal supervised autoencoder based on extreme learning machine. Expert Syst. 2017, 34, e12224. [Google Scholar] [CrossRef]
- Rangaswamy, C.; Raju, G.T.; Seshikala, G. SVM, RBFNN and CNN classifiers for detection and classification of lung cancer from CT scans image. J. Int. Pharm. Res. 2019, 46, 230–236. [Google Scholar]
- Sori, W.J.; Feng, J.; Liu, S. Multi-path convolutional neural network for lung cancer detection. Multidimens. Syst. Signal Process. 2018, 30. [Google Scholar] [CrossRef]
- Wang, S.; Wang, R.; Zhang, S.; Li, R.; Fu, Y.; Sun, X.; Li, Y.; Sun, X.; Jiang, X.; Guo, X.; et al. 3D convolutional neural network for differentiating pre-invasive lesions from invasive adenocarcinomas appearing as ground-glass nodules with diameters ≤3 cm using HRCT. Quant. Imaging Med. Surg. 2018, 8, 491–499. [Google Scholar] [CrossRef]
- Yuan, J.-J.; Liu, X.-L.; Hou, F.; Qin, H.; Hao, A. Hybrid-feature-guided lung nodule type classification on CT images. Comput. Graph. (Pergamon) 2018, 70, 288–299. [Google Scholar] [CrossRef]
- Zhang, C.; Sun, X.; Dang, K.; Li, K.; Guo, X.-W.; Chang, J.; Yu, Z.-Q.; Huang, F.-Y.; Wu, Y.-S.; Liang, Z.; et al. Toward an Expert Level of Lung Cancer Detection and Classification Using a Deep Convolutional Neural Network. Oncologist 2019, 24. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, K. Overview of deep learning in medical imaging. Radiol. Phys. Technol. 2017, 10, 257–273. [Google Scholar] [CrossRef]
- Liu, G.-F.; Bao, H.-Q.; Han, B.-K. A Stacked Autoencoder-Based Deep Neural Network for Achieving Gearbox Fault Diagnosis. Math. Probl. Eng. 2018, 2018, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Kaggle Data Science Bowl 2017. Available online: https://www.kaggle.com/c/data-science-bowl-2017/data (accessed on 15 November 2019).
- ELCAP Public Lung Image Database. Available online: http://www.via.cornell.edu/databases/lungdb.html (accessed on 28 October 2019).
- Ru Zhao, Y.; Xie, X.; de Koning, H.J.; Mali, W.P.; Vliegenthart, R.; Oudkerk, M. NELSON lung cancer screening study. Cancer Imaging 2011, 11, S79–S84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Image and Data Archive of the University of South Carolina and Laboratory of Neuro Imaging. Available online: https://ida.loni.usc.edu/login.jsp (accessed on 28 October 2019).
- Multimedia database of Interstitial Lung Diseases. Available online: http://medgift.hevs.ch/wordpress/databases/ild-database/ (accessed on 15 November 2017).
- Pehrson, L.M.; Nielsen, M.B.; Ammitzbol Lauridsen, C. Automatic Pulmonary Nodule Detection Applying Deep Learning or Machine Learning Algorithms to the LIDC-IDRI Database: A Systematic Review. Diagnostics (Basel) 2019, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tajbakhsh, N.; Suzuki, K. A Comparative Study of Modern Machine Learning Approaches for Focal Lesion Detection and Classification in Medical Images: BoVW, CNN and MTANN. In Artificial Intelligence in Decision Support Systems for Diagnosis in Medical Imaging; Springer: Cham, Switzerland, 2018; pp. 31–58. [Google Scholar] [CrossRef]
- Suzuki, K.; Armato, S.G.; Li, F.; Sone, S.; Doi, K. Massive training artificial neural network (MTANN) for reduction of false positives in computerized detection of lung nodules in low-dose computed tomography. Med. Phys. 2003, 30, 1602–1617. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, K.; Shin, E.; Choy, G.; Do, S. How much data is needed to train a medical image deep learning system to achieve necessary high accuracy? arXiv 2015, arXiv:1511.06348. [Google Scholar]
- Yosinski, J.; Clune, J.; Bengio, Y.; Lipson, H. How transferable are features in deep neural networks? In Proceedings of the Neural Information Processing Systems 27 (NIPS 2014), Montreal, QC, Canada, 8–11 December 2014. [Google Scholar]
- Schlegl, T.; Ofner, J.; Langs, G. Unsupervised Pre-training Across Image Domains Improves Lung Tissue Classification; Springer: Cham, Switzerland, 2014; pp. 82–93. [Google Scholar] [CrossRef]
- Oquab, M.; Bottou, L.; Laptev, I.; Sivic, J. Learning and Transferring Mid-Level Image Representations using Convolutional Neural Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Columbus, OH, USA, 24–27 June 2014. [Google Scholar]
- Tajbakhsh, N.; Shin, J.Y.; Gurudu, S.R.; Hurst, R.T.; Kendall, C.B.; Gotway, M.B.; Liang, J. Convolutional Neural Networks for Medical Image Analysis: Full Training or Fine Tuning? IEEE Trans. Med. Imaging 2016, 35, 1299–1312. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going Deeper with Convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015. [Google Scholar]
- Taigman, Y.; Marc, M.Y.; Ranzato, A.; Wolf, L. DeepFace: Closing the Gap to Human-Level Performance in Face Verification. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Columbus, OH, USA, 24–27 June 2014. [Google Scholar]
- Nuance + NVIDIA Advance AI for Radiology Nuance. Available online: https://www.nuance.com/about-us/newsroom/press-releases/nuance-nvidia-advance-ai-radiology.html (accessed on 15 November 2019).


{kind=link}
| Detection | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author | Year | Deep Learning Architecture | Dataset for Training | Dataset for Testing | Sensitivity | Specificity | AUC | Accuracy |
| Suzuki, Kenji * [19] | 2009 | MTANN | Independent dataset A | Independent dataset B | 97 | N/A | N/A | N/A |
| Tajbakhsh, Nima et al. [20] | 2017 | CNN | Independent dataset | Independent dataset | 100 | N/A | N/A | N/A |
| MTANN | Independent dataset | Independent dataset | 100 | N/A | N/A | N/A | ||
| Masood, Anum et al. [21] | 2018 | FCNN | LIDC-IDRI, RIDER, LungCT-diagnosis, LUNA16, LISS, SPIE challenge dataset and independent dataset | RIDER | 74.6 | 86.5 | N/A | 80.6 |
| SPIE challenge dataset | 81.2 | 83 | N/A | 84.9 | ||||
| LungCT-diagnosis | 82.5 | 93.6 | N/A | 89.5 | ||||
| Independent dataset | 83.7 | 96.2 | N/A | 86.3 | ||||
| Chen, Sihang et al. [22] | 2019 | CNN | Independent dataset | Independent dataset | 97 | N/A | N/A | N/A |
| Liao, Fangzhou et al. [23] | 2019 | CNN | LUNA16 and DSB17 | DSB17 | 85.6 | N/A | N/A | N/A |
| Liu, Mingzhe et al. [24] | 2018 | CNN | LUNA16 and DSB17 | DSB17 | 85.6 | N/A | N/A | N/A |
| Li, Li et al. * [17] | 2018 | CNN | LIDC-IDRI and NLST | Independent dataset | 86.2 | N/A | N/A | N/A |
| Wang, Yang et al. [25] | 2019 | RCNN | Independent dataset | Independent dataset | N/A | N/A | N/A | N/A |
| Setio, A.A.A et al. * [18] | 2016 | CNN | LIDC-IDRI and ANODE09 | DLCST | 76.5 | N/A | N/A | 94 |
| ANODE09 | N/A | N/A | N/A | N/A | ||||
| Wang, Jun et al. [26] | 2019 | CNN | Tianchi AI challenge dataset and independent dataset | Independent dataset | 75.6 | N/A | N/A | N/A |
| Classification | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Deep Learning Architecture | Dataset for Training | Dataset for Testing | Categories for Testing | Sensitivity | Specificity | AUC | Accuracy |
| Alakwaa, Wafaa et al. [27] | 2017 | CNN | LUNA16 and DSB17 | DSB17 | Cancer vs. no cancer | N/A | N/A | N/A | 86.6 |
| Chen, Sihang et al. [22] | 2019 | CNN | Independent dataset | Independent dataset | Adenocarcinoma vs. benign | N/A | N/A | N/A | 87.5 |
| Ciompi, Francesco et al. [28] | 2015 | CNN | ImageNet and NELSON | NELSON | Peri-fissural nodules (PFN) vs. non-PFN | N/A | N/A | 84.7 | N/A |
| Ciompi, Francesco et al. *[29] | 2017 | CNN | MILD | DLCST | Multiple categories (overall) | N/A | N/A | N/A | 79.5 |
| Jakimovski, Goran et al. [30] | 2019 | CDNN | LONI database | LONI database | Cancer vs. no cancer | 99.9 | 98.7 | N/A | 99.6 |
| Lakshmanaprabu, S.K. et al. [31] | 2018 | ODNN | ELCAP | ELCAP | Abnormal vs. normal | 96.2 | 94.2 | N/A | 94.5 |
| Li, Li et al. * [17] | 2018 | CNN | LIDC-IDRI and NLST | Independent dataset | Multiple categories (overall) | N/A | N/A | N/A | N/A |
| Liao, Fangzhou et al. [23] | 2019 | CNN | LUNA16 and DSB17 | DSB17 | Cancer vs. no-cancer (scale) | N/A | N/A | 87 | 81.4 |
| Liu, Shuang et al. [32] | 2017 | CNN | NLST and ELCAP | NLST and ELCAP | Malign vs. benign | N/A | N/A | 78 | N/A |
| Liu, Xinglong et al. * [33] | 2017 | CNN | LIDC-IDRI | ELCAP | Multiple categories (overall) | N/A | N/A | N/A | 90.3 |
| Masood, Anum et al. [21] | 2018 | FCNN | LIDC-IDRI, RIDER, LungCT-Diagnosis, LUNA16, LISS, SPIE challenge dataset and Independent dataset | Independent dataset | Four stage categories (overall) | 83.7 | 96.2 | N/A | 96.3 |
| Nishio, Mizuho et al. [34] | 2018 | CNN | Independent dataset | Independent dataset | Benign, primary and metastic cancer (overall) | N/A | N/A | N/A | 68 |
| Onishi, Yuya et al. [35] | 2018 | DCNN | Independent dataset | Independent dataset | Malign vs. benign | N/A | N/A | 84.1 | 81.7 |
| Polat, Huseyin et al. [36] | 2019 | CNN | DSB17 | DSB17 | Cancer vs. no cancer | 88.5 | 94.2 | N/A | 91.8 |
| Qiang, Yan et al. [37] | 2017 | Deep SDAE-ELM | Independent dataset | Independent dataset | Malign vs. benign | 84.4 | 81.3 | N/A | 82.8 |
| Rangaswamy et al. [38] | 2019 | CNN | ILD | ILD | Malign vs. benign | 98 | 94 | N/A | 96 |
| Sori, Worku Jifara et al. [39] | 2018 | CNN | LUNA16 and DSB17 | DSB17 | Cancer vs. no cancer | 87.4 | 89.1 | N/A | 87.8 |
| Suzuki, Kenji * [19] | 2009 | MTANN | Independent dataset A | Independent dataset B | Malign vs. benign | 96 | N/A | N/A | N/A |
| Tajbakhsh, Nima et al. [20] | 2017 | CNN | Independent dataset | Independent dataset | Malign vs. benign | N/A | N/A | 77.6 | N/A |
| MTANN | Independent dataset | Independent dataset | Malign vs. benign | N/A | N/A | 88.1 | N/A | ||
| Wang, Shengping et al. [40] | 2018 | CNN | Independent dataset | Independent dataset | PIL vs. IAC | 88.5 | 80.1 | 89.2 | 84 |
| Wang, Yang et al. [25] | 2019 | RCNN | Independent dataset | Independent dataset | Malign vs. benign | 76.5 | 89.1 | 90.6 | 87.3 |
| Yuan, Jingjing et al. * [41] | 2017 | CNN | LIDC-IDRI | ELCAP | Multiple categories (overall) | N/A | N/A | N/A | 93.9 |
| Zhang, Chao et al. * [42] | 2019 | CNN | LUNA16, DSB17 and Independent dataset(A) | Independent dataset(B) | Malign vs. benign | 96 | 88 | N/A | 92 |
| Author | Year | Sensitivity | Specificity |
|---|---|---|---|
| Jakimovski, Goran et al. [30] | 2019 | 99.9 | 98.7 |
| Lakshmanaprabu, S.K. et al. [31] | 2018 | 96.2 | 94.2 |
| Masood, Anum et al. [21] | 2018 | 83.7 | 96.2 |
| Polat, Huseyin et al. [36] | 2019 | 88.5 | 94.2 |
| Qiang, Yan et al. [37] | 2017 | 84.4 | 81.3 |
| Rangaswamy et al. [38] | 2019 | 98 | 94 |
| Sori, Worku Jifara et al. [39] | 2018 | 87.4 | 89.1 |
| Suzuki, Kenji et al. [19] | 2009 | 96 * | N/A |
| Wang, Shengping et al. [40] | 2018 | 88.5 | 80.1 |
| Wang, Yang et al. [25] | 2019 | 76.5 | 89.1 |
| Zhang, Chao et al. [42] | 2019 | 96 * | 88 * |
| Author | Year | AUC |
|---|---|---|
| Ciompi, Francesco et al. [28] | 2015 | 84.7 |
| Liao, Fangzhou et al. [23] | 2019 | 87 |
| Liu, Shuang et al. [32] | 2017 | 78 |
| Onishi, Yuya et al. [35] | 2018 | 84.1 |
| Tajbakhsh, Nima et al.(CNN) [20] | 2017 | 77.6 |
| Tajbakhsh, Nima et al.(MTANN) [20] | 88.1 | |
| Wang, Shengping et al. [40] | 2018 | 89.2 |
| Wang, Yang et al. [25] | 2019 | 90.6 |
| Author | Year | Accuracy |
|---|---|---|
| Alakwaa, Wafaa et al. [27] | 2017 | 86.6 |
| Chen, Sihang et al. [22] | 2019 | 87.5 |
| Ciompi, Francesco et al. [29] | 2017 | 79.5 * |
| Jakimovski, Goran et al. [30] | 2019 | 99.6 |
| Lakshmanaprabu, S.K. et al. [31] | 2018 | 94.5 |
| Liao, Fangzhou et al. [23] | 2019 | 81.4 |
| Liu, Xinglong et al. [33] | 2017 | 90.3 * |
| Masood, Anum et al. [21] | 2018 | 96.3 |
| Nishio, Mizuho et al. [34] | 2018 | 68 |
| Onishi, Yuya et al. [35] | 2018 | 81.7 |
| Polat, Huseyin et al. [36] | 2019 | 91.8 |
| Qiang, Yan et al. [37] | 2017 | 82.8 |
| Rangaswamy et al. [38] | 2019 | 96 |
| Sori, Worku Jifara et al. [39] | 2018 | 87.8 |
| Wang, Shengping et al. [40] | 2018 | 84 |
| Wang, Yang et al. [25] | 2019 | 87.3 |
| Yuan, Jingjing et al. [41] | 2017 | 93.9 * |
| Zhang, Chao et al. [42] | 2019 | 92 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, D.; Mikela Vilmun, B.; Frederik Carlsen, J.; Albrecht-Beste, E.; Ammitzbøl Lauridsen, C.; Bachmann Nielsen, M.; Lindskov Hansen, K. The Performance of Deep Learning Algorithms on Automatic Pulmonary Nodule Detection and Classification Tested on Different Datasets That Are Not Derived from LIDC-IDRI: A Systematic Review. Diagnostics 2019, 9, 207. https://doi.org/10.3390/diagnostics9040207
Li D, Mikela Vilmun B, Frederik Carlsen J, Albrecht-Beste E, Ammitzbøl Lauridsen C, Bachmann Nielsen M, Lindskov Hansen K. The Performance of Deep Learning Algorithms on Automatic Pulmonary Nodule Detection and Classification Tested on Different Datasets That Are Not Derived from LIDC-IDRI: A Systematic Review. Diagnostics. 2019; 9(4):207. https://doi.org/10.3390/diagnostics9040207
Chicago/Turabian StyleLi, Dana, Bolette Mikela Vilmun, Jonathan Frederik Carlsen, Elisabeth Albrecht-Beste, Carsten Ammitzbøl Lauridsen, Michael Bachmann Nielsen, and Kristoffer Lindskov Hansen. 2019. "The Performance of Deep Learning Algorithms on Automatic Pulmonary Nodule Detection and Classification Tested on Different Datasets That Are Not Derived from LIDC-IDRI: A Systematic Review" Diagnostics 9, no. 4: 207. https://doi.org/10.3390/diagnostics9040207