Maternal Coronavirus Infections and Neonates Born to Mothers with SARS-CoV-2: A Systematic Review


 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
3. Results
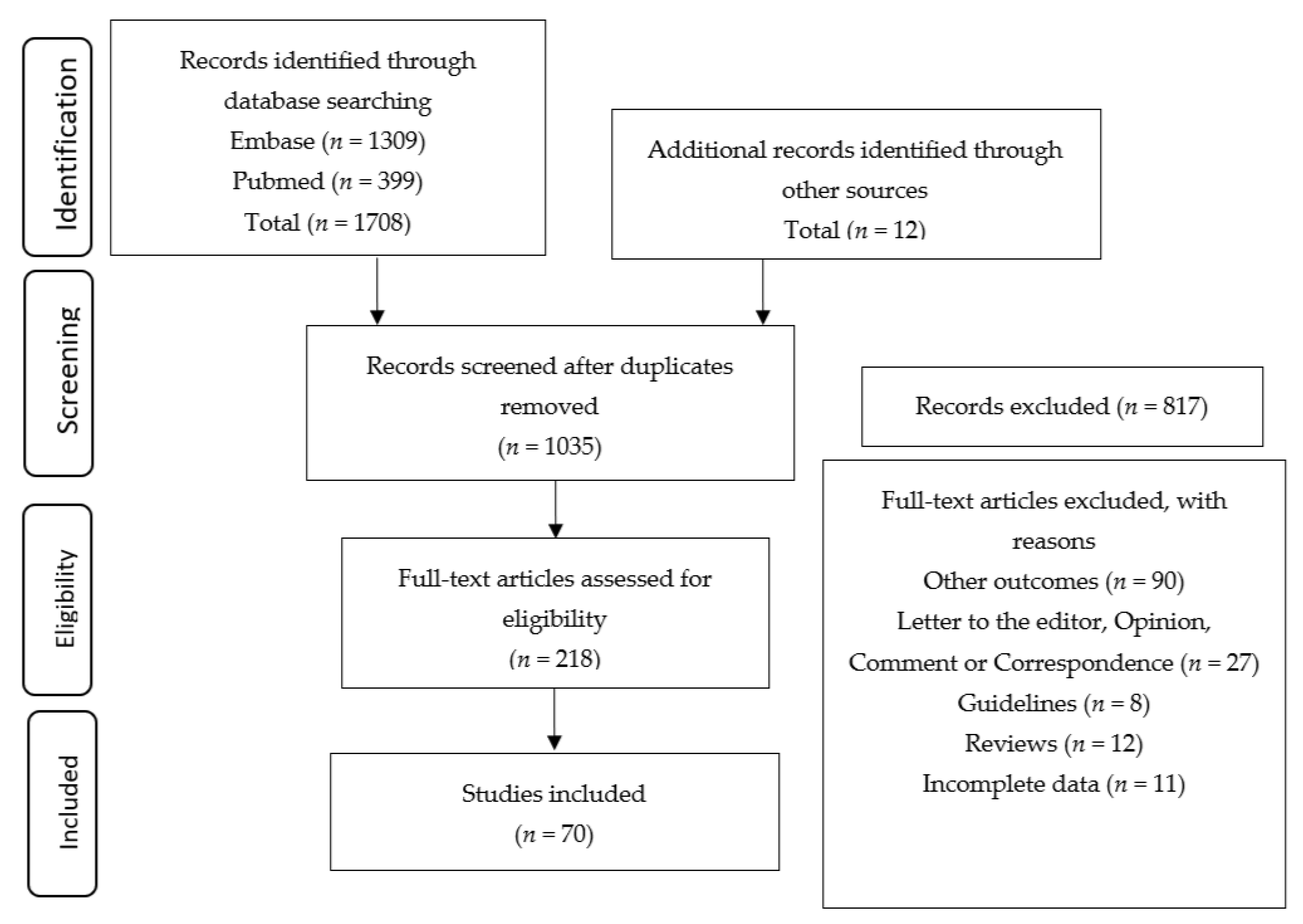
3.1. Study Selection
3.2. Synthesis of Results
3.3. Signs and Symptoms
3.4. Gestational Age
3.5. Type of Delivery
3.6. Comorbidity and Pregnancy Complications
3.7. Maternal Outcomes
3.8. Neonatal and Fetal Outcomes
3.9. Newborns and Placental and Breast Milk Samples Tested Positive for SARS-COV-2
3.10. Newborns Tested Negative for SARS-COV-2 and Vertical Transmission
4. Discussion
4.1. Strengths and Limitations
4.2. Future Recommendations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- The Lancet Infectious Diseases. COVID-19, a pandemic or not? Lancet Infect. Dis. 2020, 20, 383. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Giwa, A.L.; Desai, A.; Duca, A. Novel 2019 coronavirus SARS-CoV-2 (COVID-19): An updated overview for emergency clinicians. Emerg. Med. Pract. 2020, 22, 1–28. [Google Scholar]
- Khan, S.; Peng, L.; Siddique, R.; Nabi, G.; Nawsherwan; Xue, M.; Liu, J.; Han, G. Impact of COVID-19 infection on pregnancy outcomes and the risk of maternal-to-neonatal intrapartum transmission of COVID-19 during natural birth. Infect. Control. Hosp. Epidemiol. 2020, 41, 748–750. [Google Scholar] [CrossRef] [Green Version]
- Qiao, J. What are the risks of COVID-19 infection in pregnant women? Lancet 2020, 395, 760–762. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Lee, J.; Kim, E.; Woo, K.; Park, H.Y.; An, J. Emergency cesarean section on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) confirmed patient. Korean J. Anesthesiol. 2020, 73, 347–351. [Google Scholar] [CrossRef]
- Favre, G.; Pomar, L.; Qi, X.; Nielsen-Saines, K.; Musso, D.; Baud, D. Guidelines for pregnant women with suspected SARS-CoV-2 infection. Lancet Infect. Dis. 2020, 20, 652–653. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Liu, F.; Li, J.; Zhang, T.; Wang, D.; Lan, W. Clinical and CT imaging features of the COVID-19 pneumonia: Focus on pregnant women and children. J. Infect. 2020, 80, e7–e13. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.F.; O’Donoghue, K.; Grace, N.; Dorling, J.; Comeau, J.L.; Li, W.; Thornton, J.G. Maternal transmission of SARS-COV-2 to the neonate, and possible routes for such transmission: A systematic review and critical analysis. BJOG 2020, 127, 1324–1336. [Google Scholar] [CrossRef] [PubMed]
- Lopes de Sousa, Á.F.; Carvalho, H.E.F.d.; Oliveira, L.B.d.; Schneider, G.; Camargo, E.L.S.; Watanabe, E.; de Andrade, D.; Fernandes, A.F.C.; Mendes, I.A.C.; Fronteira, I. Effects of COVID-19 Infection during Pregnancy and Neonatal Prognosis: What Is the Evidence? Int. J. Environ. Res. Public Health 2020, 17, 4176. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.; Seo, D.; Warty, R.; Payne, O.; Salih, M.; Chin, K.L.; Ofori-Asenso, R.; Krishnan, S.; da Silva Costa, F.; Vollenhoven, B.; et al. Maternal and neonatal outcomes associated with COVID-19 infection: A systematic review. PLoS ONE 2020, 15, e0234187. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wang, M.; Zhu, Z.; Liu, Y. Coronavirus disease 2019 (COVID-19) and pregnancy: A systematic review. J. Matern. Fetal Neonatal Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Soares, C.B.; Hoga, L.A.; Peduzzi, M.; Sangaleti, C.; Yonekura, T.; Silva, D.R. Integrative review: Concepts and methods used in nursing. Rev. Esc. Enferm. USP 2014, 48, 335–345. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Alzamora, M.C.; Paredes, T.; Caceres, D.; Webb, C.M.; Valdez, L.M.; La Rosa, M. Severe COVID-19 during pregnancy and possible vertical transmission. Am. J. Perinatol. 2020, 37, 861. [Google Scholar]
- Baud, D.; Giannoni, E.; Pomar, L.; Qi, X.; Nielsen-Saines, K.; Musso, D.; Favre, G. COVID-19 in pregnant women–Authors’ reply. Lancet Infect. Dis. 2020, 20, 654. [Google Scholar] [CrossRef] [Green Version]
- Baud, D.; Greub, G.; Favre, G.; Gengler, C.; Jaton, K.; Dubruc, E.; Pomar, L. Second-trimester miscarriage in a pregnant woman with SARS-CoV-2 infection. JAMA 2020, 323, 2198–2200. [Google Scholar] [CrossRef]
- Blitz, M.J.; Rochelson, B.; Minkoff, H.; Meirowitz, N.; Prasannan, L.; London, V.; Rafael, T.J.; Chakravarthy, S.; Bracero, L.A.; Wasden, S.W.; et al. Maternal Mortality Among Women with COVID-19 Admitted to the Intensive Care Unit. Am. J. Obstet. Gynecol. 2020, 223, 595–599.e5. [Google Scholar] [CrossRef] [PubMed]
- Breslin, N.; Baptiste, C.; Gyamfi-Bannerman, C.; Miller, R.; Martinez, R.; Bernstein, K.; Ring, L.; Landau, R.; Purisch, S.; Friedman, A.M.; et al. COVID-19 infection among asymptomatic and symptomatic pregnant women: Two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am. J. Obstet Gynecol MFM 2020, 2, 100118. [Google Scholar] [CrossRef] [PubMed]
- Breslin, N.; Baptiste, C.; Miller, R.; Fuchs, K.; Goffman, D.; Gyamfi-Bannerman, C.; D’Alton, M. COVID-19 in pregnancy: Early lessons. Am. J. Obstet. Gynecol. MFM 2020, 2, 100111. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Costa, S.; Sanguinetti, M.; Cattani, P.; Posteraro, B.; Marchetti, S.; Carducci, B.; Lanzone, A.; Tamburrini, E.; Vento, G. Neonatal late onset infection with severe acute respiratory syndrome Coronavirus 2. Am. J. Perinatol. 2020, 37, 869–872. [Google Scholar]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Zhang, Y.; Huang, L.; Cheng, B.H.; Xia, Z.Y.; Meng, Q.T. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing Cesarean delivery: A case series of 17 patients. Can. J. Anaesth. J. Can. d’anesthesie 2020, 67, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Huang, B.; Luo, D.J.; Li, X.; Yang, F.; Zhao, Y.; Nie, X.; Huang, B.X. Pregnant women with new coronavirus infection: A clinical characteristics and placental pathological analysis of three cases. Zhonghua Bing Li Xue Za Zhi Chin. J. Pathol. 2020, 49, E005. [Google Scholar]
- Chen, S.; Liao, E.; Cao, D.; Gao, Y.; Sun, G.; Shao, Y. Clinical analysis of pregnant women with 2019 novel coronavirus pneumonia. J. Med. Virol. 2020, 92, 1556–1561. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Li, Y.; Wang, J.; Cai, H.; Cao, H.; Sheng, J. Pregnant women complicated with COVID-19: A clinical analysis of 3 cases. Zhejiang Da Xue Xue Bao. Yi Xue Ban J. of Zhejiang Univ. Med. Sci. 2020, 49, 240–244. [Google Scholar]
- Chen, Y.; Peng, H.; Wang, L.; Zhao, Y.; Zeng, L.; Gao, H.; Liu, Y. Infants Born to Mothers with a New Coronavirus (COVID-19). Front. Pediatr. 2020, 8, 104. [Google Scholar] [CrossRef]
- Dong, L.; Tian, J.; He, S.; Zhu, C.; Wang, J.; Liu, C.; Yang, J. Possible Vertical Transmission of SARS-CoV-2 From an Infected Mother to Her Newborn. JAMA 2020, 323, 1846–1848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, C.; Lei, D.; Fang, C.; Li, C.; Wang, M.; Liu, Y.; Bao, Y.; Sun, Y.; Huang, J.; Guo, Y.; et al. Perinatal Transmission of COVID-19 Associated SARS-CoV-2: Should We Worry? Clin. Infect. Dis 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrazzi, E.; Frigerio, L.; Savasi, V.; Vergani, P.; Prefumo, F.; Barresi, S.; Bianchi, S.; Ciriello, E.; Facchinetti, F.; Gervasi, M.T.; et al. Vaginal delivery in SARS-CoV-2-infected pregnant women in Northern Italy: A retrospective analysis. BJOG 2020, 127, 1116–1121. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, F.; Hannes, S.; Keating, N.; Martyn, F.; Browne, I.; Briet, J.; McAuliffe, F.M.; Baalman, J.H. COVID-19 infection during the third trimester of pregnancy: Current clinical dilemmas. Eur J. Obstet. Gynecol. Reprod. Biol. 2020, 251, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Gidlöf, S.; Savchenko, J.; Brune, T.; Josefsson, H. COVID-19 in pregnancy with comorbidities: More liberal testing strategy is needed. Acta Obstet. Et Gynecol. Scand. 2020, 99, 948–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hantoushzadeh, S.; Shamshirsaz, A.A.; Aleyasin, A.; Seferovic, M.D.; Aski, S.K.; Arian, S.E.; Pooransari, P.; Ghotbizadeh, F.; Aalipour, S.; Soleimani, Z.; et al. Maternal death due to COVID-19. Am. J. Obstet. Gynecol. MFM 2020, 223, 109.e1–109.e16. [Google Scholar] [CrossRef]
- Iqbal, S.N.; Overcash, R.; Mokhtari, N.; Saeed, H.; Gold, S.; Auguste, T.; Mirza, M.U.; Ruiz, M.E.; Chahine, J.J.; Waga, M.; et al. An Uncomplicated Delivery in a Patient with Covid-19 in the United States. N. Engl. J. Med. 2020, 382, e34. [Google Scholar] [CrossRef]
- Kalafat, E.; Yaprak, E.; Cinar, G.; Varli, B.; Ozisik, S.; Uzun, C.; Azap, A.; Koc, A. Lung ultrasound and computed tomographic findings in pregnant woman with COVID-19. Ultrasound Obstet. Gynecol. 2020, 55, 835–837. [Google Scholar] [CrossRef] [Green Version]
- Karami, P.; Naghavi, M.; Feyzi, A.; Aghamohammadi, M.; Novin, M.S.; Mobaien, A.; Qorbanisani, M.; Karami, A.; Norooznezhad, A.H. WITHDRAWN: Mortality of a pregnant patient diagnosed with COVID-19: A case report with clinical, radiological, and histopathological findings. Travel Med. Infect. Dis. 2020, 101665. [Google Scholar] [CrossRef]
- Kirtsman, M.; Diambomba, Y.; Poutanen, S.M.; Malinowski, A.K.; Vlachodimitropoulou, E.; Parks, W.T.; Erdman, L.; Morris, S.K.; Shah, P.S. Probable congenital SARS-CoV-2 infection in a neonate born to a woman with active SARS-CoV-2 infection. Can. Med. Assoc. J. 2020, 192, E647–E650. [Google Scholar] [CrossRef]
- Knight, M.; Bunch, K.; Vousden, N.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: National population-based cohort study. BMJ (Clin. Res. Ed.) 2020, 369, m2107. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Y.; Zeng, Y.; Song, T.; Pan, X.; Jia, M.; He, F.; Hou, L.; Li, B.; He, S.; et al. Critically ill pregnant patient with COVID-19 and neonatal death within two hours of birth. Int. J. Gynecol. Obstet. 2020, 150, 126–128. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Han, L.; Peng, M.; Lv, Y.; Ouyang, Y.; Liu, K.; Yue, L.; Li, Q.; Sun, G.; Chen, L.; et al. Maternal and neonatal outcomes of pregnant women with COVID-19 pneumonia: A case-control study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhao, R.; Zheng, S.; Chen, X.; Wang, J.; Sheng, X.; Zhou, J.; Cai, H.; Fang, Q.; Yu, F.; et al. Lack of Vertical Transmission of Severe Acute Respiratory Syndrome Coronavirus 2, China. Emerg. Infect. Dis. 2020, 26, 1335–1336. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.; Yang, H.; Kong, J.; Yang, H. Chest CT Findings in a Pregnant Patient with 2019 Novel Coronavirus Disease. Balk. Med. J. 2020. [Google Scholar] [CrossRef]
- Liu, D.; Li, L.; Wu, X.; Zheng, D.; Wang, J.; Yang, L.; Zheng, C. Pregnancy and Perinatal Outcomes of Women with Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Analysis. AJR Am. J. Roentgenol. 2020, 215, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Wang, Q.; Zhang, Q.; Chen, L.; Chen, J.; Zhang, B.; Lu, Y.; Wang, S.; Xia, L.; Huang, L. Coronavirus disease 2019 (COVID-19) during pregnancy: A case series. Available online: https://www.preprints.org/manuscript/202002.0373/v1. (accessed on 18 November 2020).
- Lokken, E.M.; Walker, C.L.; Delaney, S.; Kachikis, A.; Kretzer, N.M.; Erickson, A.; Resnick, R.; Vanderhoeven, J.; Hwang, J.K.; Barnhart, N.; et al. Clinical Characteristics of 46 Pregnant Women with a SARS-CoV-2 Infection in Washington State. Am. J. Obstet. Gynecol. MFM 2020. [Google Scholar] [CrossRef]
- London, V.; McLaren, R., Jr.; Atallah, F.; Cepeda, C.; McCalla, S.; Fisher, N.; Stein, J.L.; Haberman, S.; Minkoff, H. The Relationship between Status at Presentation and Outcomes among Pregnant Women with COVID-19. Am. J. Perinatol. 2020, 37, 991–994. [Google Scholar] [CrossRef]
- Martínez-Perez, O.; Vouga, M.; Cruz Melguizo, S.; Forcen Acebal, L.; Panchaud, A.; Muñoz-Chápuli, M.; Baud, D. Association Between Mode of Delivery Among Pregnant Women With COVID-19 and Maternal and Neonatal Outcomes in Spain. JAMA 2020, 324, 296. [Google Scholar] [CrossRef]
- Patanè, L.; Morotti, D.; Giunta, M.R.; Sigismondi, C.; Piccoli, M.G.; Frigerio, L.; Mangili, G.; Arosio, M.; Cornolti, G. Vertical transmission of COVID-19: SARS-CoV-2 RNA on the fetal side of the placenta in pregnancies with COVID-19 positive mothers and neonates at birth. Am. J. Obstet. Gynecol. MFM 2020, 2, 100145. [Google Scholar] [CrossRef]
- Penfield, C.A.; Brubaker, S.G.; Limaye, M.A.; Lighter, J.; Ratner, A.J.; Thomas, K.M.; Meyer, J.; Roman, A.S. Detection of SARS-COV-2 in Placental and Fetal Membrane Samples. Am. J. Obstet. Gynecol. MFM 2020, 2, 100133. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Wang, J.; Mo, Y.; Duan, W.; Xiang, G.; Yi, M.; Bao, L.; Shi, Y. Unlikely SARS-CoV-2 vertical transmission from mother to child: A case report. J. Infect. Public Health 2020, 13, 818–820. [Google Scholar] [CrossRef]
- Qiancheng, X.; Jian, S.; Lingling, P.; Lei, H.; Xiaogan, J.; Weihua, L.; Gang, Y.; Shirong, L.; Zhen, W.; GuoPing, X.; et al. Coronavirus disease 2019 in pregnancy. Int. J. Infect. Dis. 2020, 95, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Savasi, V.M.; Parisi, F.; Patanè, L.; Ferrazzi, E.; Frigerio, L.; Pellegrino, A.; Spinillo, A.; Tateo, S.; Ottoboni, M.; Veronese, P.; et al. Clinical Findings and Disease Severity in Hospitalized Pregnant Women with Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2020, 136, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Sentilhes, L.; De Marcillac, F.; Jouffrieau, C.; Kuhn, P.; Thuet, V.; Hansmann, Y.; Ruch, Y.; Fafi-Kremer, S.; Deruelle, P. COVID-19 in pregnancy was associated with maternal morbidity and preterm birth. Am. J. Obstet. Gynecol. MFM 2020. [Google Scholar] [CrossRef]
- Siying, Z.; Juanjuan, G.; Yuming, C.; Huijun, C.; Dan, X.; Jiafu, L.; Yuanzhen, Z. A case of new coronavirus infection in perinatal period. Chin. J. Perinat. Med. 2020, 23, 85–90. [Google Scholar]
- Wang, S.; Guo, L.; Chen, L.; Liu, W.; Cao, Y.; Zhang, J.; Feng, L. A case report of neonatal COVID-19 infection in China. Clin. Infect. Dis. 2020, 71, 853–857. [Google Scholar] [CrossRef]
- Wang, X.; Zhou, Z.; Zhang, J.; Zhu, F.; Tang, Y.; Shen, X. A case of 2019 Novel Coronavirus in a pregnant woman with preterm delivery. Clin. Infect. Dis. 2020, 71, 844–846. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Sun, R.; Chen, J.; Xie, Y.; Zhang, S.; Wang, X. Radiological findings and clinical characteristics of pregnant women with COVID-19 pneumonia. Int. J. Gynaecol. Obstet. 2020. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, C.; Dong, L.; Zhang, C.; Chen, Y.; Liu, J.; Zhang, C.; Duan, C.; Zhang, H.; Mol, B.W.; et al. Coronavirus disease 2019 among pregnant Chinese women: Case series data on the safety of vaginal birth and breastfeeding. BJOG 2020, 127, 1109–1115. [Google Scholar] [CrossRef]
- Xiong, X.; Wei, H.; Zhang, Z.; Chang, J.; Ma, X.; Gao, X.; Chen, Q.; Pang, Q. Vaginal Delivery Report of a Healthy Neonate Born to a Convalescent Mother with COVID-19. J. Med. Virol. 2020, 92, 1657–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, J.; Guo, J.; Fan, C.; Juan, J.; Yu, X.; Li, J.; Feng, L.; Li, C.; Chen, H.; Qiao, Y.; et al. Coronavirus disease 2019 in pregnant women: A report based on 116 cases. Am. J. Obstet. Gynecol. MFM 2020. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Hu, B.; Zhan, S.; Yang, L.Y.; Xiong, G. Effects of SARS-CoV-2 infection on pregnant women and their infants: A retrospective study in Wuhan, China. Arch. Pathol. Lab. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Wang, X.; Liu, P.; Wei, C.; He, B.; Zheng, J.; Zhao, D. Clinical characteristics and risk assessment of newborns born to mothers with COVID-19. J. Clin. Virol. 2020, 127, 104356. [Google Scholar] [CrossRef] [PubMed]
- Yu, N.; Li, W.; Kang, Q.; Xiong, Z.; Wang, S.; Lin, X.; Liu, Y.; Xiao, J.; Liu, H.; Deng, D.; et al. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: A retrospective, single-centre, descriptive study. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Fan, C.; Bian, J.; Shen, Y. Severe COVID-19 in a pregnant patient admitted to hospital in Wuhan. Int. J. Gynecol. Obstet. 2020, 150, 262–263. [Google Scholar] [CrossRef]
- Zeng, L.; Xia, S.; Yuan, W.; Yan, K.; Xiao, F.; Shao, J.; Zhou, W. Neonatal Early-Onset Infection With SARS-CoV-2 in 33 Neonates Born to Mothers With COVID-19 in Wuhan, China. JAMA Pediatr. 2020, 174, 722. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Jiang, Y.; Wei, M.; Cheng, B.H.; Zhou, X.C.; Li, J.; Tian, J.H.; Dong, L.; Hu, R.H. Analysis of the pregnancy outcomes in pregnant women with COVID-19 in Hubei Province. Zhonghua Fu Chan Ke Za Zhi 2020, 55, E009. [Google Scholar]
- Zhu, H.; Wang, L.; Fang, C.; Peng, S.; Zhang, L.; Chang, G.; Xia, S.; Zhou, W. Clinical analysis of 10 neonates born to mothers with 2019-nCoV pneumonia. Transl. Pediatrics 2020, 9, 51–60. [Google Scholar] [CrossRef]
- Lowe, B.; Bopp, B. COVID-19 vaginal delivery—A case report. Aust. N. Z. J. Obstet. Gynaecol. 2020, 60, 465–466. [Google Scholar] [CrossRef] [Green Version]
- Hijona Elósegui, J.J.; Carballo García, A.L.; Fernández Risquez, A.C.; Bermúdez Quintana, M.; Expósito Montes, J.F. Does the maternal-fetal transmission of SARS-CoV-2 occur during pregnancy? Rev. Clin. Esp. 2020. [Google Scholar] [CrossRef] [PubMed]
- Yue, L.; Han, L.; Li, Q.; Zhong, M.; Wang, J.; Wan, Z.; Chu, C.; Zeng, Y.; Peng, M.; Yang, L.; et al. Anaesthesia and infection control in cesarean section of pregnant women with coronavirus disease 2019 (COVID-19). medRxiv 2020. [Google Scholar] [CrossRef]
- Vivanti, A.J.; Vauloup-Fellous, C.; Prevot, S.; Zupan, V.; Suffee, C.; Do Cao, J.; Benachi, A.; De Luca, D. Transplacental transmission of SARS-CoV-2 infection. Nat. Commun. 2020, 11, 3572. [Google Scholar] [CrossRef] [PubMed]
- Sisman, J.; Jaleel, M.A.; Moreno, W.; Rajaram, V.; Collins, R.R.J.; Savani, R.C.; Rakheja, D.; Evans, A.S. Intrauterine Transmission of SARS-COV-2 Infection in a Preterm Infant. Pediatric Infect. Dis. J. 2020, 39, e265–e267. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Mohagheghi, P.; Beigi, B.; Zafaranloo, N.; Moshfegh, F.; Yazdani, A. Spectrum of neonatal COVID-19 in Iran: 19 infants with SARS-CoV-2 perinatal infections with varying test results, clinical findings and outcomes. J. Matern.-Fetal Neonatal Med. 2020, 1–10. [Google Scholar] [CrossRef]
- Pereira, A.; Cruz-Melguizo, S.; Adrien, M.; Fuentes, L.; Marin, E.; Perez-Medina, T. Clinical course of coronavirus disease-2019 in pregnancy. Acta Obstet. Et Gynecol. Scand. 2020, 99, 839–847. [Google Scholar] [CrossRef]
- Lv, Y.; Gu, B.; Chen, Y.; Hu, S.; Ruan, T.; Xu, G.; Ding, J.; Xu, X.; Shen, X. No intrauterine vertical transmission in pregnancy with COVID-19: A case report. J. Infect. Chemother. 2020, 26, 1313–1315. [Google Scholar] [CrossRef]
- Hosier, H.; Farhadian, S.F.; Morotti, R.A.; Deshmukh, U.; Lu-Culligan, A.; Campbell, K.H.; Yasumoto, Y.; Vogels, C.B.; Casanovas-Massana, A.; Vijayakumar, P.; et al. SARS-CoV-2 infection of the placenta. J. Clin. Investig. 2020, 130, 4947–4953. [Google Scholar] [CrossRef]
- Marín Gabriel, M.; Malalana Martínez, A.M.; Marín Martínez, M.E.; Anel Pedroche, J. Negative Transmission of SARS-CoV-2 to Hand-Expressed Colostrum from SARS-CoV-2-Positive Mothers. Breastfeed. Med. 2020, 15, 492–494. [Google Scholar] [CrossRef]
- Ferraiolo, A.; Barra, F.; Kratochwila, C.; Paudice, M.; Vellone, V.G.; Godano, E.; Varesano, S.; Noberasco, G.; Ferrero, S.; Arioni, C. Report of Positive Placental Swabs for SARS-CoV-2 in an Asymptomatic Pregnant Woman with COVID-19. Medicina 2020, 56, 306. [Google Scholar] [CrossRef]
- Fenizia, C.; Biasin, M.; Cetin, I.; Vergani, P.; Mileto, D.; Spinillo, A.; Gismondo, M.R.; Perotti, F.; Callegari, C.; Mancon, A.; et al. Analysis of SARS-CoV-2 vertical transmission during pregnancy. Nat. Commun. 2020, 11, 5128. [Google Scholar] [CrossRef] [PubMed]
- Facchetti, F.; Bugatti, M.; Drera, E.; Tripodo, C.; Sartori, E.; Cancila, V.; Papaccio, M.; Castellani, R.; Casola, S.; Boniotti, M.B.; et al. SARS-CoV2 vertical transmission with adverse effects on the newborn revealed through integrated immunohistochemical, electron microscopy and molecular analyses of Placenta. EBioMedicine 2020, 59. [Google Scholar] [CrossRef]
- Costa, S.; Posteraro, B.; Marchetti, S.; Tamburrini, E.; Carducci, B.; Lanzone, A.; Valentini, P.; Buonsenso, D.; Sanguinetti, M.; Vento, G.; et al. Excretion of SARS-CoV-2 in human breast milk. Clin. Microbiol. Infect. 2020, 26, 1430–1432. [Google Scholar] [CrossRef] [PubMed]
- Algarroba, G.N.; Rekawek, P.; Vahanian, S.A.; Khullar, P.; Palaia, T.; Peltier, M.R.; Chavez, M.R.; Vintzileos, A.M. Visualization of severe acute respiratory syndrome coronavirus 2 invading the human placenta using electron microscopy. Am. J. Obstet. Gynecol. MFM 2020, 223, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Lin, L.; Yan, Q.; Wei, W.; Yang, B.X.; Huang, R.; He, F.; Chen, D. Update on clinical outcomes of women with COVID-19 during pregnancy. Int. J. Gynaecol. Obstet. 2020, 150, 264–266. [Google Scholar] [CrossRef]
- Wan, S.; Li, M.; Ye, Z.; Yang, C.; Cai, Q.; Duan, S.; Song, B. CT Manifestations and Clinical Characteristics of 1115 Patients with Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-analysis. Acad. Radiol. 2020, 27, 910–921. [Google Scholar] [CrossRef]
- Celik, O.; Saglam, A.; Baysal, B.; Derwig, I.E.; Celik, N.; Ak, M.; Aslan, S.N.; Ulas, M.; Ersahin, A.; Tayyar, A.T.; et al. Factors preventing materno-fetal transmission of SARS-CoV-2. Placenta 2020, 97, 1–5. [Google Scholar] [CrossRef]
- Mahyuddin, A.P.; Kanneganti, A.; Wong, J.; Dimri, P.S.; Su, L.L.; Biswas, A.; Illanes, S.E.; Mattar, C.; Huang, R.-J.; Choolani, M. Mechanisms and evidence of vertical transmission of infections in pregnancy including SARS-CoV-2. Prenat. Diagn 2020. [Google Scholar] [CrossRef]
- Dashraath, P.; Wong, J.L.J.; Lim, M.X.K.; Lim, L.M.; Li, S.; Biswas, A.; Choolani, M.; Mattar, C.; Su, L.L. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am. J. Obstet. Gynecol. MFM 2020, 222, 521–531. [Google Scholar] [CrossRef]
- Rasmussen, S.A.; Jamieson, D.J. Caring for Women Who Are Planning a Pregnancy, Pregnant, or Postpartum During the COVID-19 Pandemic. JAMA 2020, 324, 190. [Google Scholar] [CrossRef]


{kind=link}
| First Author, Year, and Country | Study Size and Age | Study Design | Signs and Symptoms | Gestational Age | Type of Delivery and Maternal or Fetal Complications | GRADE * | |
|---|---|---|---|---|---|---|---|
| Before Delivery | Postpartum | ||||||
| Algarroba, et al., 2020 [85] EUA | n = 1 Age: 40 years | Case report | Worsening shortness of breath, cough, and hypoxia | NR | Third trimester (28 weeks gestational age) | Cesarean delivery (n = 1) | ●○○○ |
| Alzamora et al., 2020 [18] Peru | n = 1 Age: 41 years | Case report | General malaise, fatigue, and low-grade fever | NR | Third trimester (33 weeks gestational age) | Emergency cesarean section (n = 1) | ●○○○ |
| Baud et al., 2020 [20] Switzerland | n = 1 Age: 28 years | Case report | Fever (39.2 °C), myalgia, fatigue, mild pain with swallowing, diarrhea, and dry cough for 2 days | NR | Second trimester (19 weeks gestational age) | Vaginal deliveries (after 10 h of labor) (n = 1) | ●○○○ |
| Blitz et al., 2020 [21] USA | n = 13 Mean maternal age 33.8 ± 5.2 | Case series | Fever, subjective or measured (n = 12) Cough (n = 13) Dyspnea (n = 10) Myalgia (n = 6) Fatigue or malaise (n = 3) | NR | Third trimester (mean weeks gestational age 33.3 ± 5.3) | Cesarean for acute respiratory decompensation (n = 5) Cesarean for obstetrical indication (n = 1) Vaginal delivery (n = 1) | ●●●○ |
| Breslin et al., 2020 [22] USA | n = 43 Mean maternal age 29.7 ± 6.0 | Case series, retrospective | Symptomatic gestates (n = 29) Asymptomatic pregnant women (n = 14) Fever ≥37.5 °C (100.0 °F) (n = 14) Cough (n = 19) Myalgia or fatigue (n = 11) Dyspnea (n = 7) Headache (n = 8) Chest pain (n = 5) | Worse fever or increased breathing work | Third trimester (≥37 weeks gestational age) | Cesarean delivery (n = 8) Vaginal deliveries (n = 18) | ●●●○ |
| Breslin et al., 2020 [23] USA | n = 7 Age: 27 to 39 years | Case series | Fever ≥37.0 °C (100.0 °F) (n = 2) Cough (n = 3) Myalgias (n = 3) Chest pain (n = 2) Headache (n = 2) | Fever Severe hypertension Cough Severe bronchospasm and disproportionate reactive lung disease | Third trimester (≥37 weeks gestational age) | Emergency cesarean section (n = 7) | ●●○○ |
| Buonsenso et al., 2020 [24] Italy | n = 7 Age: 27 to 39 years | Observational study | NR Asymptomatic (n = 1) | NR | Second trimester (≥20 weeks gestational age) | Cesarean section (n = 2)—third trimester | ●●○○ |
| Chen et al., 2020 [28] China | n = 5 Age: 25 to 31 years | Descriptive study | Cough Sputum Coryza Asymptomatic (n = 3) | Low fever (37.5–38.5 °C) (n = 5) | Third trimester (39–40 weeks) | Emergency cesarean section (n = 1) (preeclampsia—fetal tachycardia) Elective cesarean section (n = 1) (gestational diabetes) Vaginal delivery (n = 3) | ●●○○ |
| Chen et al., 2020 [25] China | n = 9 Age: 26 to 40 years | Descriptive, retrospective study | Low fever without chills (n = 7) Myalgia (n = 3) Malaise (n = 2) Cough (n = 4) Dyspnea (n = 1) Sore throat (n = 2) Diarrhea (n = 1) | Fever (variation of 37.8–39.33 °C) (n = 6) | Third trimester (≥36 weeks gestational age) | Cesarean (n = 9) | ●●○○ |
| Chen et al., 2020 [27] China | n = 3 Age: 23 to 32 years | Descriptive, retrospective study | Fever and chest tightness (n = 1) | Fever (n = 3) | Third trimester (≥35 weeks gestational age) | Emergency cesarean section (n = 3) | ●○○○ |
| Chen et al., 2020 [26] China | n = 17 Mean maternal age 29.7 years | Descriptive, retrospective study | Mild fever without chills (≤39 °C) (n = 4) Cough (n = 4) Fatigue (n = 1) Chest distress (n = 2) Dyspnea (n = 1) Diarrhea (n = 1) | NR | Third trimester (≥35 weeks gestational age) | Elective cesarean delivery (n = 14) Emergency cesarean delivery (n = 3) | ●●○○ |
| Chen et al., 2020 [30] China | n = 4 Age: 23 to 34 years | Case report | Fever (n = 3) Cough (n = 2) Fatigue (n = 2) Headache (n = 2) Dyspnea (n = 2) | Anemia and dyspnea | Third trimester (≥37 weeks gestational age) | Cesarean section (n = 3) Vaginal delivery (n = 1) | ●○○○ |
| Chen et al., 2020 [29] China | n = 3 Age: 23 to 34 years | Case report | Cough (n = 3) Fever (n = 3) Fatigue (n = 3) Diarrhea, nausea, and vomiting | NR | First trimester (6 weeks) Second trimester (25 weeks) Third trimester (35 weeks) | Cesarean section delivery (n = 1) | ●●○○ |
| Costa et al., 2020 [84] Italy | n = 2 Age: 38 years and 42 years | Case report | Fever, shortness of breath, and diarrhea (n = 1) Cough (n = 1) | NR | Third trimester (n = 2) (≥34 weeks gestational age) | Caesarean section (n = 2) | ●○○○ |
| Dong et al., 2020 [31] China | n = 1 Age: 29 years | Case report | Fever, nasal congestion Liver injury | NR | Third trimester (34 weeks) | Cesarean section delivery (n = 1) | ●○○○ |
| Elósegui et al., 2020 [72] Spain | n = 4 Age: 27 to 40 years | Case series | Mild clinical symptoms | NR | Second trimester | SARS-CoV-2 in vaginal discharge and amniotic fluid in Caucasian pregnant women affected by mild acute symptoms of COVID-19 | ●○○○ |
| Facchetti et al., 2020 [83] Italy | n = 1 Age: 29 | Case report | Fever and idiopathic thrombocytopenia | NR | Third trimester (37 weeks gestational age) | Vaginal delivery was induced (n = 1) | ●○○○ |
| Fan et al., 2020 [32] China | n = 2 Age: 34 years and 29 years | Case report | Nasal congestion (n = 2) Fever (37. 3–38.5 °C) (n = 2) Skin rash (n = 1) Chill (n = 1) Sore throat (n = 1) | NR | Third trimester (37 weeks gestational age) (36 weeks gestational age) | Cesarean section delivery (n = 2) | ●○○○ |
| Ferrazzi et al., 2020 [33] Italy | n = 42 Mean maternal age 32.9 | Retrospective multicenter study | Fever (n = 20), cough (n = 7), myalgia/malaise (n = 7), dyspnea (n = 8) | NR | Third trimester (±30 weeks gestational age) | Elective cesarean (n = 18) Vaginal delivery (n = 24) | ●●●○ |
| Fenizia et al., 2020 [82] Italy | n = 31 Median age: 30 | Case report | NR | Admission to ICU and invasive ventilation (n = 1) | Third trimester (weeks median: 39) | Vaginal delivery (n = 25) Caesarean section (n = 6) | ●●○○ |
| Ferraiolo et al., 2020 [81] Italy | n = 1 Age: 30 | Case report | Asymptomatic | Asymptomatic | Third trimester (38 weeks gestational age) | Urgent cesarean section | ●○○○ |
| Fontanella et al., 2020 [34] the Netherlands and Ireland | n = 2 Age: 39 years and 29 years | Case report | Fever ≥37.3 °C (n = 2) (1) Cough and increasing dyspnea, thoracic pain with deep breathing (2) Productive cough, sore throat, and diarrhea | NR | Third trimester (31 weeks gestational age) (40 weeks gestational age) | Cesarean (n = 2) | ●○○○ |
| Gabriel et al., 2020 [80] Spain | n = 7 Median age: 33–43 | Observational prospective | Asymptomatic (n = 6) Fever, malaise, myalgia, headache (n = 1) | NR | Third trimester (≥38 weeks gestational age) | Vaginal delivery (n = 6) Cesarean section (n = 1) | ●○○○ |
| Gidlöf et al., 2020 [35] Sweden | n = 1 Age: 34 years | Case report | Hoarseness Increasing malaise Severe headache and photophobia | Oxygen saturation dropped to 87% Pulmonary edema/embolism | Third trimester (36 weeks gestational age) | Emergency cesarean—dichorionic twin pregnancy (n = 2) | ●○○○ |
| Hantoushzadeh et al., 2020 [36] Iran | n = 9 Age: 25 to 49 years | Case series | Fever (n = 9) Cough (n = 9) Dyspnea (n = 6) Myalgia (n = 4) | NR | Second trimester (n = 2) Third trimester (n = 7) | Cesarean delivery (n = 6) Vaginal delivery (n = 1) | ●●○○ |
| Hosier et al., 2020 [79] USA | n = 1 Age: 35 | Case report | Fever, malaise, nonproductive cough, diffuse myalgias, anorexia, nausea, and diarrhea | NR | Second trimester (22 weeks gestational age) | Urgent cesarean section | ●○○○ |
| Iqbal et al., 2020 [37] USA | n = 1 Age: 34 years | Case report | Fever, chills, dry cough, and myalgia | Fever 38.5 °C | Third trimester (39 weeks of gestation) | Spontaneous vaginal delivery (n = 1) | ●○○○ |
| Kalafat et al., 2020 [38] Turkey | n = 1 Age: 32 years | Case report | Nausea Dyspnea Swollen left leg | NR | Third trimester (35 weeks gestational age) | Cesarean (n = 1) | ●○○○ |
| Karami et al., 2020 [39] Iran | n = 1 Age: 27 years | Case report | Fever, cough, and myalgia for 3 days | NR | Third trimester (30 and 3/7 weeks gestation) | Vaginal delivery (n = 1) | ●○○○ |
| Khan et al., 2020 [5] China | n = 3 Age: 27 to 33 years | Case report | Cough (n = 3) Fever (≥37.3 °C) (n = 2) Chest tightness (n = 1) | NR | Third trimester (≥34 weeks of gestation) | Vaginal delivery (n = 3) | ●●○○ |
| Kirtsman et al., 2020 [40] Canada | n = 1 Age: 40 years | Case report | Cough Pyrexia Tachycardic (110–121 beats/min) Fever (39 °C) | NR | Third trimester (35 + 3 weeks gestation) | Cesarean delivery (n = 1) | ●●○○ |
| Knight et al., 2020 [41] UK | n = 427 | Cohort study | Fever (n = 280) Cough (n = 240) Breathlessness (n = 160) Tiredness or lethargy (n = 70) Headache (n = 60) | NR | Second trimester (≤26 weeks) (n = 4) Third trimester (>27 weeks) (n = 96) | Caesarean, maternal indication due to SARS-CoV-2 (n = 42) Caesarean, other indication (n = 114) Operative vaginal (n = 28) Unassisted vaginal (n = 78) | ●●●● |
| Lee et al., 2020 [7] Korea | n = 1 Age: 35 years | Case report | Fever (>38 °C), mild sore throat and cough | NR | Third trimester (37 weeks gestational age) | Cesarean delivery (n = 1) | ●○○○ |
| Li et al., 2020 [43] China | n = 16 Age: 26 to 37 years | Case-control study | Fever (n = 4) Cough (n = 4) | Fever (n = 8) | Third trimester (Mean weeks gestational age = 38 ± 0.2) | Total: 17 babies Vaginal delivery (n = 2) Cesarean section (n = 14) Twin pregnancy | ●●○○ |
| Li et al., 2020 [44] China | n = 1 Age: 30 years | Case report | Fever (37.2 °C), chills, or shortness of breath | NR | Third trimester (35 weeks gestational age) | Emergency cesarean section (n = 1) | ●○○○ |
| Li et al., 2020 [42] China | n = 1 Age: 31 years | Case report | Fever and dyspnea to acute respiratory distress syndrome and septic shock | NR | Third trimester (35 + 2 weeks gestational age) | Cesarean delivery (n = 1) | ●○○○ |
| Liao et al., 2020 [45] China | n = 1 Age: 25 years | Clinical case reported in a letter to the editor | Fatigue and mild dry cough for 3 days Fever (38.3 °C) | NR | Third trimester (35 weeks gestational age) | Emergency cesarean section (n = 1) | ●○○○ |
| Liu et al., 2020 [9] China | n = 16 Age: 22–42 years | Retrospective study | Fever (n = 7) Cough (n = 6) Short of breath (n = 2) Fatigue (n = 3) | Fever (n = 5) | Third trimester (>22 weeks gestational age) | Cesarean section (n = 10) | ●●●○ |
| Liu et al., 2020 [46] China | n = 15 Age: 23 to 40 years | Case report | Fever (n = 13) Cough (n = 9) Sore throat (n = 1) Dyspnea (n = 1) Myalgia (n = 3) Fatigue (n = 4) Diarrhea (n = 1) Asymptomatic (n = 2) | Fever (n = 1) | First and third trimesters (≥27 weeks gestational age) (12 to 38 weeks) | Cesarean section (n = 10) Vaginal delivery (n = 1) | ●●○○ |
| Liu et al., 2020 [47] China | n = 3 Age: 30 to 34 years | Case series study | Fever (37.8 °C) (n = 2) Cough (n = 2) | NR | Third trimester (>38 weeks gestational age) | Cesarean section (n = 2) Natural childbirth (n = 1) | ●●○○ |
| Lv et al., 2020 [78] China | n = 1 Age: 28 | Case report | Fever and cough | NR | Third trimester (31 weeks gestational age) | Cesarean section | ●○○○ |
| Lokken et al., 2020 [48] USA | n = 46 Age: 26 to 34 years | Retrospective study | Symptomatic (n = 43) Cough (n = 30) Fever or chill (n = 22) Nasal congestion (n = 21) Shortness of breath/dyspnea (n = 19) (44.2%) Asymptomatic (n = 3) | NR | Second or third trimester | Vaginal (n = 5) Cesarean (n = 3) Preterm birth at 33 weeks (n = 1) | ●●●○ |
| London et al., 2020 [49] USA | n = 68 Age: ≥30 years | Retrospective cohort study | Fever (n = 46) Cough (n = 46) Shortness of breath (n = 46) Sore throat (n = 46) Nausea (n = 46) Vomiting (n = 46) Asymptomatic (n = 22) | NR | First trimester (17 weeks gestational age) (n = 1) Second trimester (25 and 26 weeks) (n = 2) Third trimester (n = 65) | Cesarean delivery (n = 22) | ●●●○ |
| Lowe et al., 2020 [71] Australia | n = 1 Age: 31 years | Case report | Initially remained asymptomatic Fever | NR | Third trimester (40 weeks gestational age) | Vaginal delivery | ●○○○ |
| Martínez-Perez et al., 2020 [50] Spain | n = 82 Age: 33 years | Cohort | Symptomatic gestates (n = 60) Asymptomatic pregnant women (n = 22) | NR | Third trimester (≥29 weeks gestational age) | Delivered vaginally (n = 49) Cesarean delivery (n = 33) | ●●●○ |
| Patanè et al., 2020 [51] Italy | n = 22 Age: 33 years | Retrospective cohort study | Fever 38 °C (n = 2) Dry cough (n = 2) | NR | Third trimester (≥37.6 weeks gestational age) | Vaginal delivery (n = 1) Cesarean delivery (n = 1) | ●●○○ |
| Penfield et al., 2020 [52] USA | n = 32 Age: 22 to 40 years | Retrospective cohort study | NR | NR | Second and Third trimester (≥26 weeks) | Cesarean delivery (n = 4) Normal spontaneous vaginal delivery (n = 7) | ●●●○ |
| Peng et al., 2020 [53] China | n = 1 Age: 22 to 40 years | Case report | Fever, fatigue, shortness of breath | NR | Third trimester (35.2 weeks gestational age) | Cesarean (n = 1) | ●○○○ |
| Pereira et al., 2020 [77] Spain | n = 60 Median age: 34 years | Descriptive | Fever and cough | Admission to ICU (n = 1) (with HELLP syndrome) | Third trimester (median: 32 weeks) | During the study period, 23 women delivered: Cesarean section (n = 5) Vaginal (n = 18) | ●○○○ |
| Qiancheng et al., 2020 [54] China | n = 28 Mean maternal age 30 26.75–32 | Single-center, retrospective study | Cough (n = 7) Fever (n = 5) Abdominal pain (n = 5) Dyspnea (n = 2) Malaise (n = 1) | NR | First trimester (n = 3) Second trimester (n = 1) Third trimester (n = 24) | Cesarean section (n = 17) Vaginal delivery (n = 5) | ●●○○ |
| Savasi et al., 2020 [55] Italy | n = 91 Age: 15 to 48 years | Retrospective cohort study | Fever (n = 54) Cough (n = 62) Dyspnea (n = 27) | Symptomatic (n = 10) | First trimester (n = 4) Second trimester (n = 13) Third trimester (n = 50) | Cesarean (n = 31) Vaginal (n = 36) | ●●●○ |
| Schwartz et al., 2020 [76] Iran | n = 9 Age: 28 | Retrospective cohort study | NR | NR | Third trimester (>28 weeks gestational age) | Cesarean section (n = 8) Spontaneous vaginal delivery (n = 1) | ●●○○ |
| Sentilhes et al., 2020 [56] France | n = 38 Age: 19 to 42 years | Retrospective single-center study | Fatigue (n = 38) Cough (n = 25) Anosmia or ageusia (n = 18) Fever (n = 10) | NR | Third trimester (mean weeks gestational age 29.3 ± 8.5) | Cesarean (n = 6) Vaginal (n = 10) | ●●○○ |
| Sisman et al., 2020 [75] USA | n = 1 Age: 37 | Case report | Fever | NR | Third trimester (34 weeks gestational age) | Vaginal delivery (n = 1) | ●○○○ |
| Siying et al., 2020 [57] China | n = 1 Age: 33 | Case report | Dry cough 1 day before admission, without sputum, sore throat, fatigue | Dry cough | Third trimester (37 weeks gestational age) | Emergency caesarean section (n = 1) | ●○○○ |
| Vivanti et al., 2020 [74] France | n = 1 Age: 23 | Case report | Fever (38.6 °C), severe cough, and abundant expectoration | NR | Third trimester (35 + 2 weeks of gestation) | Cesarean delivery (n = 1) | ●○○○ |
| Wang et al., 2020 [59] China | n = 1 Age: 28 | Case report | Fever | NR | Third trimester (30 weeks pregnant) | Emergency cesarean (n = 1) | ●○○○ |
| Wang et al., 2020 [58] China | n = 1 Age: 34 | Case report | Fever (37.8 ℃) | NR | Third quarter (40 weeks gestational age) | Emergency cesarean (n = 1) | ●○○○ |
| Wu et al., 2020 [60] China | n = 23 Age: 21–37 years | Case report | Cough (n = 6), Fever (n = 4) Nasal congestion (n = 1) Clinically asymptomatic (n = 15) | NR | First trimester (n = 3) (≤12 weeks) Third trimester (n = 20) (≥28 weeks gestational age) | Cesarean section (n = 18) Vaginal delivery (n = 2) | ●●○○ |
| Wu et al., 2020 [61] China | n = 13 Age: 26–40 years | Descriptive study, retrospective | Fever (n = 8) Cough (n = 5) Dyspnea (n = 1) Myalgia (n = 1) Diarrhea (n = 1) | NR | First trimester (n = 5) Second trimester (n = 3) Third trimester (n = 5) | Caesarean section (n = 4) Natural delivery (n = 1) | ●●○○ |
| Xiong et al., 2020 [62] China | n = 1 Age: 25 years | Case report | Fever (38 °C) Dry cough Shivering | NR | Third trimester (33 weeks gestational age) | Vaginal delivery six hours after (n = 1) | ●●○○ |
| Yan et al., 2020 [63] China | n = 116 Mean maternal age 30.8 ± 3.8 | Descriptive study, retrospective | Fever (n = 59) Cough (n = 33) Clinically asymptomatic (n = 27) | NR | Third trimester (≥ 38 weeks gestational age) | Cesarean delivery (n = 85) Vaginal delivery (n = 14) | ●●●○ |
| Yang et al., 2020 [64] China | n = 26 Age: 21 to 40 years | Retrospective study | Fever (13 cases), cough (10 cases), vomiting (1 case) | NR | Third trimester (≥30 weeks gestational age) | Cesarean section (n = 20); Vaginal (n = 6 cases) | ●●○○ |
| Yang P et al., 2020 [65] China | n = 7 Age: 21 to 40 years | Case report | Fever (n = 5) Cough (n = 1) Abdominal pain (n = 1) | Fever | Third trimester (≥36 weeks gestational age) | Cesarean delivery (n = 7) | ●●○○ |
| Yu et al., 2020 [66] China | n = 7 Age: 29 to 34 years | Descriptive study, retrospective | Fever (n = 6) Cough (n = 1) Shortness of breath (n = 1) Diarrhea (n = 1) | NR | Third trimester (≥37 weeks gestational age) | Cesarean delivery (n = 7) | ●●○○ |
| Yu et al., 2020 [67] China | n = 1 Age: 35 | Descriptive study, retrospective | Low fever and dry cough | Dyspnea and cyanosis | Third trimester (34 weeks gestational age) | Vaginal delivery (n = 1) | ●○○○ |
| Yue et al., 2020 [73] China | n = 14 Mean maternal age 30.1 ± 3.4 | Case series study | Fever (n = 4) | NR | Third trimester (mean weeks gestational age 38 ± 0.4) | Emergency cesarean (n = 13) | ●●○○ |
| Zeng et al., 2020 [68] China | n = 33 Age: 24 to 34 years | Case report | Cough (n = 10) Fever on admission (n = 8) | Fever (n = 5) | Third trimester (≥31 weeks gestational age) | Cesarean delivery because of meconium-stained amniotic fluid Cesarean delivery (n = 26) Natural childbirth (n = 7) | ●●●○ |
| Zhang et al., 2020 [69] China | n = 16 Age: 24 to 34 years | Retrospective study | Cough (n = 3) Chest tightness (n = 3) Shortness of breath (n = 3) Diarrhea (n = 3) | NR | Third trimester (≥38 weeks gestational age) | Cesarean section (n = 10) | ●●○○ |
| Zhu et al., 2020 [70] China | n = 9 Mother of the twins (n = 1) Age: 25 to 34 years | Retrospective study | Fever (n = 7) Cough (n = 4) Diarrhea (n = 1) | NR | Third trimester (≥31 weeks gestational age) | Cesarean section (n = 7) Vaginal delivery (n = 2) | ●●○○ |
| Gestational Age | Comorbidity | Complications |
|---|---|---|
| Second trimester | Psoriasis [79] Severe hypertension [79] Coagulopathy [79] | Preeclampsia [79] |
| Third trimester | Asthma [21,23,50,56] Chronic comorbidity [82] Chronic hypertension [22,23] Type 2 diabetes mellitus [18,21,22,23,26,75] Dysfunction of blood coagulation [64] Hepatitis B [9,43] History of frequent bacterial infections (sinusitis, skin infection, and bronchitis) during this pregnancy [40] Hypertension [26,35,41,43,63] Hypothyroidism [59,64,66] Polycystic ovary syndrome [66] Mild-intermittent asthma [22] Obesity [21,22,34,35,50,56,69,75] Obstructive sleep apnea [21] Polycystic ovary syndrome [43] | Abnormal placenta (placenta previa) [70] Complete prior placenta [27] Complications in pregnancy ([73] Gestational diabetes [9,21,28,33,34,35,40,50,56,63,64,69] Gestational hypertension [9,21,25,56,64] Pneumonia secondary to COVID-19 [85] Sepsis [85] Maternal COVID-19 pneumonia [68] Intrauterine fetal distress [73] Placental detachment [27] Preeclampsia [25,28,50,63,69] Previous placenta [30] Severe preeclampsia [64] |
| Second and third trimesters * | Asthma [41,48] Cardiac disease [41] Diabetes [41] Hypertension [41] Obese [41] Overweight or obese [48] Type 2 diabetes [48] | Gestational diabetes [41,48] Gestational hypertension [48] |
| First, second, and third trimesters * | Asthma [49] Autoimmune disease [55] Chronic hepatitis B virus infection [54] Chronic hypertension [49] Diabetes [49,54] Endocrine disease [55] Hypertension [54] Hypothyroidism [54] Metabolic diseases [55] Obesity [55] | Gestational diabetes [49] Preeclampsia [49] |
| First Author and Year | Diagnosis Test | Type of Delivery | Positive COVID-19 Test Results |
|---|---|---|---|
| NEWBORNS | |||
| Alzamora et al., 2020 [18] | Nasopharyngeal swab was obtained for SARS-CoV-2 RT-PCR | Emergency cesarean section (n = 1) | Nasopharyngeal swab, 16 h after delivery, was positive for SARS-CoV-2 RT-PCR, and immunoglobulin (Ig)-M and IgG for SARS-CoV-2: Negative |
| Buonsenso et al., 2020 [24] | RT-PCR | Cesarean section (n = 1) | SARS-CoV-2 positive at 15 days of life, although asymptomatic |
| Facchetti et al., 2020 [83] | SARS-CoV-2 RNA on nasopharyngeal swab | Vaginal delivery was induced (n = 1) | Resulted inconclusive (amplification of less than three genes), while it was positive 36 and 72 h after birth and at the age of 17 days |
| Fenizia et al., 2020 [82] | Nasopharyngeal newborn swab was obtained for SARS-CoV-2 RT-PCR after the baby was cleaned | Vaginal delivery (n = 25) Caesarean section (n = 6) | Viral RNA positive in newborns (n = 2) |
| Ferrazzi et al., 2020 [33] | RT-PCR | (1) Elective cesarean section (n = 2) (2) Vaginal delivery (n = 1) | (1) Newborns had a positive test for COVID-19 infection at days one and three, respectively (2) The first test for SARS-CoV-2 was equivocal a few hours after delivery, but positive three days later |
| Hantoushzadeh et al., 2020 [36] | SARS-CoV-2 NAT | Cesarean section (n = 1) | Negative on day 1 of life but converted to positive on day 7 of life with an accompanying lymphopenia (nadir white blood cell 8.9, with 26% lymphocytes) The neonate was intubated for prematurity, developed pneumonia at day of life 2 There was maternal death |
| Knight et al., 2020 [41] | Detection of viral RNA on polymerase chain reaction testing of blood or a nasopharyngeal swab or aspirate | Cesarean section (n = 4) Vaginal birth (n = 2) | Positive test <12 h of age (n = 6) Positive test ≥12 h of age 6 (n = 6) |
| Kirtsman et al., 2020 [40] | RT-PCR Placental swabs (both maternal and fetal sides) were obtained Placental tissue was sent for PCR and histopathologic examination Nasopharyngeal swabs were obtained from the neonate on the day of birth, day 2, and day 7, after thorough cleansing of the baby and before contact with the mother | Cesarean section (n = 1) | All 3 of the neonate’s nasopharyngeal swabs were positive for SARS-CoV-2 gene targets via RT-PCR testing; neonatal plasma tested positive on day 4, and stool was positive on day 7 |
| Martínez-Perez et al., 2020 [50] | SARS-CoV-2 RNA RT-PCR | Vaginal delivery (n = 2) Cesarean section (n = 1) | Three newborns tested within 6 h after birth had a positive SARS-CoV-2 RT-PCR result Repeat testing at 48 h was negative None developed COVID-19 symptoms within 10 days |
| Patanè et al., 2020 [51] | SARS-CoV-2 RNA RT-PCR | Vaginal delivery (n = 1) Cesarean section (n = 1) | (1) The newborn had positive NP swabs immediately at birth, after 24 h, and after 7 days; he remained asymptomatic (2) Neonatal NP swab was 60 negative at birth and turned positive on day 7, with no contact between mother and neonate during that period |
| Savasi et al., 2020 [55] | Pharyngeal swab sampled for SARS-CoV-2 | Vaginal delivery (n = 3) Cesarean section (n = 1) | Positive on the seventh day (n = 1) |
| Schwartz et al., 2020 [76] | Infant RT-PCR testing | Cesarean section (n = 8) Spontaneous vaginal delivery (n = 1) | Positive by RT-PCR for SARS-CoV-2 (n = 9): 1 h after delivery (n = 1) 2 h after delivery (n = 1) DOL 2 (n = 1) DOL 3 (n = 1) DOL 4 (n = 2) DOL 6 (n = 1) DOL 7 (n = 1) DOL 24 (n = 1) |
| Sisman et al., 2020 [75] | Nasopharyngeal swab by RT-PCR for SARS-CoV-2 at 24 and 48 h of life | Vaginal delivery (n = 1) | Positive by nasopharyngeal swab |
| Vivanti et al., 2020 [74] | Nasopharyngeal and rectal swabs were first collected after having cleaned the baby at 1 h of life, and they were tested with RT-PCR Blood and nonbronchoscopic bronchoalveolar lavage fluid were collected for RT-PCR | Cesarean delivery (n = 1) | Nasopharyngeal and rectal Blood and nonbronchoscopic bronchoalveolar lavage fluid Clear amniotic fluid was collected prior to rupture of membranes during cesarean section and tested positive for both the E and S genes of SARS-CoV-2 |
| Zeng et al., 2020 [68] | SARS-CoV-2 real-time reverse transcriptase–polymerase | Cesarean section (n = 3) | (1) Nasopharyngeal and anal swabs were positive for SARS-CoV-2 on days 2 and 4 of life (2) Nasopharyngeal and anal swabs were positive for SARS-CoV-2 on days 2 and 4 of life and negative on day 6 (3) Nasopharyngeal and anal swabs were positive for SARS-CoV-2 on days 2 and 4 of life and negative on day 7 |
| Wang et al., 2020 [65] | SARS-CoV-2 RNA RT-PCR Pharyngeal swab | Emergency cesarean section (n = 1) | The result of pharyngeal swab for SARS-CoV-2 was positive at 36 h after birth |
| Yu et al., 2020 [67] | RT-PCR for SARS-CoV-2 | Cesarean section (n = 1) | Nucleic acid test for the throat swab of one neonate (child of patient 1) was positive at 36 h after birth |
| IgG Antibody | |||
| Dong et al., 2020 [31] | CT and RT-PCR nasopharyngeal swabs; and IgM and IgG antibody, cytokine, and other biochemistry tests in blood Vaginal secretions | Cesarean section (n = 1) | A neonate born to a mother with COVID-19 had elevated antibody levels (IgM) and abnormal cytokine test results 2 h after birth Nasopharyngeal swabs taken from 2 h to 16 days of age were negative Mother’s breast milk had a negative RT-PCR test result |
| Fenizia et al., 2020 [82] | Umbilical cord plasma: SARS-CoV-2 RT-PCR and SARS-CoV-2 IgG and IgM chemiluminescence immunoassay | Vaginal delivery (n = 25) Caesarean section (n = 6) | Viral RNA positive + IgG positive in umbilical cord plasma (n = 1) IgG positive in umbilical cord plasma (n = 10) IgM positive + IgG positive in umbilical cord plasma (n = 1) |
| Umbilical Cord | |||
| Fenizia et al., 2020 [82] | Umbilical cord: SARS-CoV-2 RT-PCR | Vaginal delivery (n = 25) Caesarean section (n = 6) | Viral RNA positive in umbilical cord (n = 1) |
| Vaginal Swab | |||
| Fenizia et al., 2020 [82] | Vaginal swab: SARS-CoV-2 RT-PCR | Vaginal delivery (n = 25) Caesarean section (n = 6) | Viral RNA positive in vaginal swab (n = 1) |
| Yang et al., 2020 [64] | RT-PCR for SARS-CoV-2 SARS-CoV-2IgM/IgG antibodies rapid test kit | Cesarean section (n = 1) Premature rupture of fetal membranes | Elevated IgM level of SARS-CoV-2 2 h after her birth Testing on her nasopharyngeal swab was negative (tested twice) |
| Symptomatic Cases | |||
| Fan et al., 2020 [32] | RT-PCR nasopharyngeal swab, maternal serum, placental tissues, umbilical cord blood, amniotic fluid, vaginal swabs, and breast milk | Cesarean section (n = 2) | Symptoms, suspected case: Two babies showed symptoms but failed to detect SARS-CoV-2 in any of the samples, including the newborn’s nasopharyngeal swab, maternal serum, placental tissues, umbilical cord blood, amniotic fluid, vaginal swabs, and breast milk |
| Gidlöf et al., 2020 [35] | RT-PCR | Emergency cesarean section (n = 2) | Twins symptoms, suspected cases: At 22 min after delivery developed breathing problems On the second day, she had a cyanotic attack while feeding Both twins had negative nasopharyngeal COVID-19 tests taken at 34 h and 4½ days of age COVID-19 tests performed on breast milk and maternal vaginal secretion on the fifth day were also negative |
| Placenta | |||
| Algarroba et al., 2020 | Electron microscopy | Cesarean delivery | A single virion was visible invading a syncytiotrophoblast A single virion was also visualized in a microvillus |
| Baud et al., 2020 [20] | Maternal—RT-PCR Deep nasopharyngeal Deep nasopharyngeal control Vagina Blood Fetus—RT-PCR Umbilical cord blood Amniotic fluid negative sterile Fetal armpit Placental submembrane Placental cotyledon Fetal anus Fetal liver Fetal thymus Fetal lung | Vaginal delivery (n = 1) | Placental submembrane—positive sterile Placental cotyledon—positive |
| Facchetti et al., 2020 [83] | Histological, immunohistochemical, in situ SARS-CoV-2 RNA, RNA in situ hybridization and electron microscopy | Vaginal delivery was induced (n = 1)—third trimester | Placenta: Tested positive for SARS-CoV-2, after detecting the presence of S-protein-specific transcripts by RNA-in situ hybridization; immunostains for SARS-CoV-2 proteins showed positivity in the cytoplasm of the syncytiotrophoblast for both S-protein and n-protein |
| Fenizia et al., 2020 [82] | SARS-CoV-2 RT-PCR | Vaginal delivery (n = 25) Caesarean section (n = 6) Third trimester | Viral RNA positive in placenta (n = 2) |
| Ferraiolo et al., 2020 | SARS-CoV-2 RT-PCR | Urgent cesarean section (n = 1)—third trimester | The definitive histological analysis of the placenta did not describe substantial macroscopic alterations, except for mild subchorionic deposition of fibrin and for the presence of a single ischemic area in the thickness of the chorionic disc |
| Hosier et al., 2020 | SARS-CoV-2 RT-PCR Whole-genome sequenced Histological examination Electron microscopy | Urgent cesarean section (n = 1)—second trimester | Placenta and umbilical cord were positive for SARS On histological examination, SARS-CoV-2 localized predominantly to the syncytiotrophoblast cells of the placenta Analysis of the placental region adjacent to the umbilical cord identified virus particles within the cytosol of placental cells consistent with the size and appearance of SARS-CoV-2 |
| Penfield et al., 2020 [52] | SARS-CoV-2 RNA RT-PCR | Cesarean section (n = 3) | Infected placentas (n = 1) or membrane swabs (n = 2) |
| Patanè et al., 2020 [51] | SARS-CoV-2 RNA RT-PCR | Vaginal delivery (n = 1) Cesarean section (n = 1) | SARS-CoV-2 RNA in the placentas |
| Vivanti et al., 2020 [74] | SARS-CoV-2 RNA RT-PCR | Cesarean delivery (n = 1) Third trimester | Placental infection as positive for SARS-CoV-2 RNA |
| Breast Milk | |||
| Costa et al., 2020 [84] | SARS-CoV-2 RT-PCR in six breast milk samples | Cesarean delivery (n = 2)—third trimester | Three of six breast milk samples (50%) had a cycle threshold value <40 (the value interpreted as positive for SARS-CoV-2 RNA), indicating that patient 1 excreted virus in her breast milk, albeit intermittently (n = 1) |
| Fenizia et al., 2020 [82] | Five days after delivery (T2), transitional/mature breast milk samples were collected from all breastfeeding women Diagnosis test SARS-CoV-2 RT-PCR and SARS-CoV-2 IgG and IgM chemiluminescence immunoassay | Vaginal delivery (n = 25) Caesarean section (n = 6) Third trimester | Viral RNA positive and IgM positive in breast milk (n = 1) |
| Wu et al., 2020 [61] | SARS-CoV-2 RNA RT-PCR—1st day after delivery Breast milk samples from three women were collected on the 1st, 6th, and 27th days after delivery Vaginal swabs Neonatal throat and anal swabs were collected on the 1st and 3rd days after birth | Caesarean section (n = 4) Natural delivery (n = 1) | Detection of SARS-CoV-2 in breast milk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaral, W.N.d.; Moraes, C.L.d.; Rodrigues, A.P.d.S.; Noll, M.; Arruda, J.T.; Mendonça, C.R. Maternal Coronavirus Infections and Neonates Born to Mothers with SARS-CoV-2: A Systematic Review. Healthcare 2020, 8, 511. https://doi.org/10.3390/healthcare8040511
Amaral WNd, Moraes CLd, Rodrigues APdS, Noll M, Arruda JT, Mendonça CR. Maternal Coronavirus Infections and Neonates Born to Mothers with SARS-CoV-2: A Systematic Review. Healthcare. 2020; 8(4):511. https://doi.org/10.3390/healthcare8040511
Chicago/Turabian StyleAmaral, Waldemar Naves do, Carolina Leão de Moraes, Ana Paula dos Santos Rodrigues, Matias Noll, Jalsi Tacon Arruda, and Carolina Rodrigues Mendonça. 2020. "Maternal Coronavirus Infections and Neonates Born to Mothers with SARS-CoV-2: A Systematic Review" Healthcare 8, no. 4: 511. https://doi.org/10.3390/healthcare8040511