
Factors associated with Early Initiation of Breastfeeding in Western Nepal



Abstract
:1. Introduction
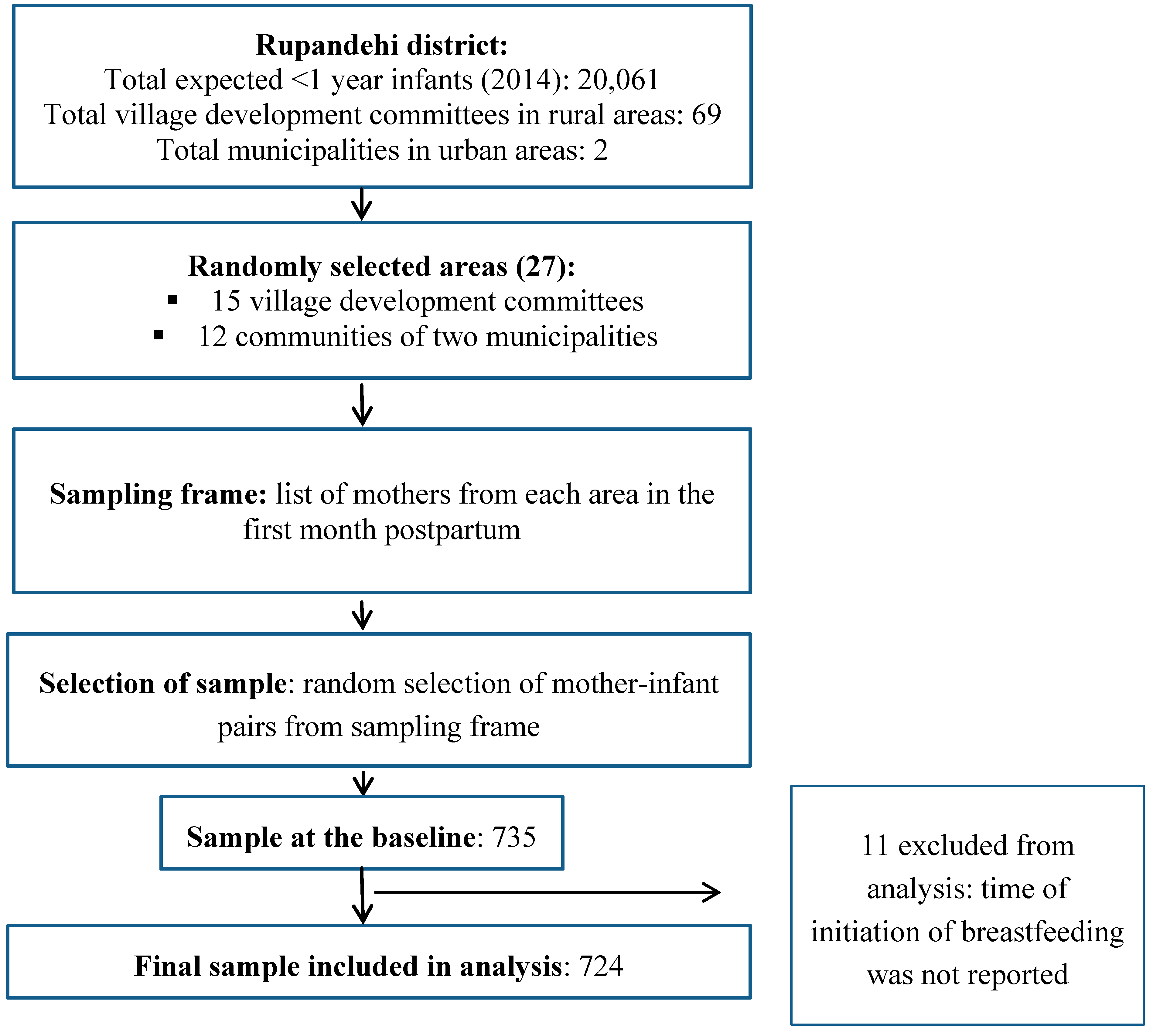
2. Experimental Section

2.1. Statistical Analyses
2.2. Ethical Considerations
3. Results
Factors Associated with Early Initiation of Breastfeeding

{kind=link}
| Factor | Frequency n (%) | Time to First Breastfeed | p Value * | |
|---|---|---|---|---|
| Delayed n (%) | Early n (%) | |||
| Maternal age (in years) # (n = 723) | 0.003 | |||
| 15–19 | 64 (8.9) | 30 (46.9) | 34 (53.1) | |
| 20–29 | 542 (75.0) | 301 (55.5) | 241 (44.5) | |
| 30–45 | 117 (16.2) | 82 (70.1) | 35 (29.9) | |
| Maternal education (n = 724) | 0.208 | |||
| No education | 190 (26.2) | 119 (62.6) | 71 (37.4) | |
| Primary/Lower secondary | 240 (33.1) | 129 (53.8) | 111 (46.2) | |
| Secondary | 128 (17.7) | 68 (53.1) | 60 (46.9) | |
| Higher | 166 (22.9) | 98 (59.0) | 68 (41.0) | |
| Maternal occupation (n = 724) | 0.001 | |||
| Employed | 30 (4.2) | 17 (56.7) | 13 (43.3) | |
| Semi-employed | 140 (19.3) | 99 (70.7) | 41 (29.3) | |
| Unemployed | 554 (76.5) | 298 (53.8) | 256 (46.2) | |
| Antenatal care visits # (n = 721) | 0.669 | |||
| No antenatal visit | 17 (2.4) | 11 (64.7) | 6 (35.3) | |
| 1–3 visits | 155 (21.5) | 92 (59.4) | 63 (40.6) | |
| 4 or more visits | 549 (76.1) | 310 (56.5) | 239 (43.5) | |
| Assistance during delivery (n = 724) | 0.069 | |||
| Unskilled/Traditional attendants | 86 (11.9) | 57 (66.3) | 29 (33.7) | |
| Skilled attendants | 638 (88.1) | 357 (56.0) | 281 (44.0) | |
| Mode of delivery (n = 724) | <0.001 | |||
| Vaginal | 623 (86.0) | 338 (54.3) | 285 (45.7) | |
| Caesarean | 101 (14.0) | 76 (75.2) | 25 (24.8) | |
| Ethnicity (n = 724) | 0.481 | |||
| Advantaged caste group | 270 (37.3) | 149 (55.2) | 121 (44.8) | |
| Middle caste groups | 366 (50.6) | 210 (57.4) | 156 (42.6) | |
| Dalit caste | 88 (12.2) | 55 (62.5) | 33 (37.5) | |
| Wealth quintile (n = 724) | <0.001 | |||
| 1 Lowest | 146 (20.2) | 61 (41.8) | 85 (58.2) | |
| 2 | 146 (20.2) | 84 (57.5) | 62 (42.5) | |
| 3 | 145 (20.0) | 85 (58.6) | 60 (41.4) | |
| 4 | 146 (20.2) | 98 (67.1) | 48 (32.9) | |
| 5 Highest | 141 (19.5) | 86 (61.0) | 55 (39.0) | |
| Delayed n (%) | Early n (%) | |||
| Sex of infant (n = 724) | 0.520 | |||
| Male | 379 (52.3) | 221 (58.3) | 158 (41.7) | |
| Female | 345 (47.7) | 193 (55.9) | 152 (44.1) | |
| Birth order # (n = 723) | 0.062 | |||
| First | 307 (42.5) | 170 (55.4) | 137 (44.6) | |
| Second or third | 329 (45.5) | 184 (55.9) | 145 (44.1) | |
| Fourth or more | 87 (12.0) | 60 (69.0) | 27 (31.0) | |
| Birth weight # (n = 668) | <0.001 | |||
| Low birth weight (<2500 g) | 93 (14.0) | 72 (77.4) | 21 (22.6) | |
| Average or greater (≥2500 g) | 573 (86.0) | 311 (54.3) | 262 (45.7) | |
| Place of residence (n = 724) | 0.577 | |||
| Rural | 373 (51.5) | 217 (58.2) | 156 (41.8) | |
| Urban | 351 (48.5) | 197 (56.1) | 154 (43.9) | |
| Prelacteal feeds (n = 724) | <0.001 | |||
| Not provided | 505 (69.8) | 252 (49.9) | 253 (50.1) | |
| Provided | 219 (30.2) | 162 (74.0) | 57 (26.0) | |
| Factors | Crude Odds Ratio (95% Confidence Interval) | p-Value | Adjusted Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|---|---|
| Maternal age (in years) | 0.004 | 0.040 | ||
| 15–19 | 1.00 | 1.00 | ||
| 20–29 | 0.71 (0.42, 1.19) | 0.83 (0.46, 1.50) | ||
| 30–45 | 0.38 (0.20, 0.71) | 0.45 (0.22, 0.93) | ||
| Assistance during delivery | 0.071 | 0.048 | ||
| Unskilled/Traditional attendant | 0.65 (0.40, 1.04) | 0.47 (0.22, 0.99) | ||
| Skilled attendant | 1.00 | 1.00 | ||
| Mode of delivery | p < 0.001 | p = 0.001 | ||
| Vaginal | 1.00 | 1.00 | ||
| Caesarean | 0.39 (0.24, 0.63) | 0.39 (0.23, 0.67) | ||
| Ethnicity | 0.483 | 0.038 | ||
| Advantaged caste group | 1.00 | 1.00 | ||
| Middle caste groups | 0.91 (0.67, 1.26) | 0.62 (0.40, 0.95) | ||
| Dalit caste | 0.75 (0.45, 1.21) | 0.52 (0.28, 0.94) | ||
| Wealth quintile | 0.001 | 0.001 | ||
| 1 Lowest | 2.18 (1.36, 3.49) | 2.43 (1.36, 4.37) | ||
| 2 | 1.15 (0.72, 1.85) | 1.36 (0.77, 2.40) | ||
| 3 | 1.10 (0.69, 1.77) | 1.22 (0.72, 2.06) | ||
| 4 | 0.77 (0.47, 1.24) | 0.69 (0.41, 1.15) | ||
| 5 Highest | 1.00 | 1.00 | ||
| Birth weight | <0.001 | <0.001 | ||
| Low birth weight (<2500 g) | 0.35 (0.21, 0.58) | 0.36 (0.21, 0.63) | ||
| Average or greater | 1.00 | 1.00 | ||
| Prelacteal feeds | <0.001 | <0.001 | ||
| Not provided | 2.85 (2.01, 4.04) | 2.00 (1.35, 2.98) | ||
| Provided | 1.00 | 1.00 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bhutta, Z.A.; Das, J.K.; Bahl, R.; Lawn, J.E.; Salam, R.A.; Paul, V.K.; Sankar, M.J.; Blencowe, H.; Rizvi, A.; Chou, V.B. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 2014, 384, 347–370. [Google Scholar] [CrossRef]
- Debes, A.K.; Kohli, A.; Walker, N.; Edmond, K.; Mullany, L.C. Time to initiation of breastfeeding and neonatal mortality and morbidity: A systematic review. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Edmond, K.M.; Zandoh, C.; Quigley, M.A.; Amenga-Etego, S.; Owusu-Agyei, S.; Kirkwood, B.R. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics 2006, 117, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Ellis, J. Neonatal hypothermia. J. Neonatal Nurs. 2005, 11, 76–82. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Benefits of Breastfeeding for Mom. Available online: http://www.healthychildren.org/English/ages-stages/baby/breastfeeding/Pages/Benefits-of-Breastfeeding-for-Mom.aspx (accessed on 19 March 2015).
- Nepal Demographic and Health Survey 2011; Ministry of Health and Population: Kathmandu, Nepal; New ERA: Kathmandu, Nepal; ICF International: Calverton, MD, USA, 2012.
- Chandrashekhar, T.; Joshi, H.; Binu, V.; Shankar, P.; Rana, M.; Ramachandran, U. Breast-feeding initiation and determinants of exclusive breast-feeding—A questionnaire survey in an urban population of western Nepal. Public Health Nutr. 2007, 10, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Banerjee, A.; Kaletwad, A. Factors associated with prelacteal feeding and timely initiation of breastfeeding in hospital-delivered infants in India. J. Hum. Lact. 2013, 29, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Senarath, U.; Siriwardena, I.; Godakandage, S.S.P.; Jayawickrama, H.; Fernando, D.N.; Dibley, M.J. Determinants of breastfeeding practices: An analysis of the Sri Lanka demographic and health survey 2006–2007. Matern. Child Nutr. 2012, 8, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Nepal Millennium Development Goals Progress Report 2013; National Planning Commission: Kathmandu, Nepal; United Nations Country Team Nepal: Kathmandu, Nepal, 2013.
- National Safe Motherhood and Newborn Health Long Term Plan (2006–2017); Family Health Division: Kathmandu, Nepal; Ministry of Health and Population: Kathmandu, Nepal, 2006.
- Darmstadt, G.L.; Kinney, M.V.; Chopra, M.; Cousens, S.; Kak, L.; Paul, V.K.; Martines, J.; Bhutta, Z.A.; Lawn, J.E. The Lancet Every Newborn Study Group. Who has been caring for the baby? Lancet 2014, 384, 174–188. [Google Scholar] [CrossRef]
- Adhikari, M.; Khanal, V.; Karkee, R.; Gavidia, T. Factors associated with early initiation of breastfeeding among Nepalese mothers: Further analysis of Nepal demographic and health survey, 2011. Int. Breastfeed. J. 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Bennett, L.; Dahal, D.; Govindasamy, P. Caste, Ethnic and Regional Identity in Nepal: Further Analysis of the 2006 Nepal Demographic and Health Survey; Macro International Inc.: Calverton, MD, USA, 2008. [Google Scholar]
- Karkee, R.; Lee, A.H.; Khanal, V.; Binns, C.W. Initiation of breastfeeding and factors associated with prelacteal feeds in central Nepal. J. Hum. Lact. 2014, 30, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Assessment of the Community Based Newborn Care Package; Child Health Division: Kathmandu, Nepal; Ministry of Health and Population: Kathmandu, Nepal, 2012.
- A Synthesis of Recent Studies on Maternal and Newborn Survival Interventions in Nepal; Child Health Division and Family Health Division: Kathmandu, Nepal; Ministry of Health and Population: Kathmandu, Nepal, 2014.
- Suvedi, B.K.; Pradhan, P.; Barnett, S.; Puri, M.; Rai Chitrakar, S.; Poudel, P.; Sharma, S.; Hulton, L. Nepal Maternal Mortality and Morbidity Study 2008/2009: Summary of Preliminary Findings; Family Health division, Department of Health Services, Ministry of Health, Government of Nepal: Kathmandu, Nepal, 2009.
- Scott, J.; Aitkin, I.; Binns, C.; Aroni, R. Factors associated with the duration of breastfeeding amongst women in Perth, Australia. Acta Paediatr. 1999, 88, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.A.; Binns, C.W.; Oddy, W.H.; Graham, K.I. Predictors of breastfeeding duration: Evidence from a cohort study. Pediatrics 2006, 117, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Duong, D.V.; Binns, C.W.; Lee, A.H. Introduction of complementary food to infants within the first six months postpartum in rural Vietnam. Acta Paediatr. 2005, 94, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Lee, A.H.; Binns, C.W. Factors associated with breastfeeding duration: A prospective cohort study in Sichuan province, China. World J. Pediatr. 2014, 11, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Qiao, L.; Xu, F.; Zhang, M.; Wang, Y.; Binns, C.W. Factors associated with breastfeeding duration a 30-month cohort study in northwest China. J. Hum. Lact. 2013, 29, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Abdulraheem, R.; Binns, C. The infant feeding practices of mothers in the Maldives. Public Health Nutr. 2007, 10, 502–507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices Part 1 Definitions; Department of Child and Adolescent Health and Development, World Health Organization: Washington, DC, USA, 2007. [Google Scholar]
- Ministry of Health and Population. Annual Report; Department of Health Services, Ministry of Health and Population: Kathmandu, Nepal, 2013.
- Khanal, V.; Adhikari, M.; Karkee, R.; Gavidia, T. Factors associated with the utilisation of postnatal care services among the mothers of Nepal: Analysis of Nepal demographic and health survey 2011. BMC Women Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Karkee, R.; Lee, A.; Khanal, V.; Binns, C. A community-based prospective cohort study of exclusive breastfeeding in central Nepal. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Nepal Demographic and Health Survey 2006; Ministry of Health and Population: Kathmandu, Nepal; New ERA: Kathmandu, Nepal; Macro International Inc.: Calverton, MD, USA, 2007.
- Haider, R.; Rasheed, S.; Sanghvi, T.G.; Hassan, N.; Pachon, H.; Islam, S.; Jalal, C. Breastfeeding in infancy: Identifying the program-relevant issues in Bangladesh. Int. Breastfeed. J. 2010, 5. [Google Scholar] [CrossRef] [PubMed]
- Mullany, L.; Katz, J.; Li, Y.; Khatry, S.; LeClerq, S.; Darmstadt, G.; Tielsch, J. Breast-feeding patterns, time to initiation, and mortality risk among newborns in southern Nepal. J. Nutr. 2008, 138, 599–603. [Google Scholar] [PubMed]
- Khanal, V.; Sauer, K. Determinants of the introduction of prelacteal feeds in rural Nepal: A cross-sectional community-based study. Breastfeed. Med. 2013, 8, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Maternal and Newborn Care: Learning Resource for Skilled Birth Attendants; National Health Training Center: Kathmandu, Nepal; Ministry of Health and Population: Kathmandu, Nepal, 2010.
- Godfrey, J.R.; Meyers, D. Toward optimal health: Maternal benefits of breastfeeding. J. Womens Health 2009, 18, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- Mullany, L.C.; Katz, J.; Khatry, S.K.; LeClerq, S.C.; Darmstadt, G.L.; Tielsch, J.M. Neonatal hypothermia and associated risk factors among newborns of southern Nepal. BMC Med. 2010, 8. [Google Scholar] [CrossRef] [PubMed]
- Dickson, K.E.; Simen-Kapeu, A.; Kinney, M.V.; Huicho, L.; Vesel, L.; Lackritz, E.; Rafique, N.; de Graft Johnson, J.; von Xylander, S.; Sylla, M. Every newborn: Health-systems bottlenecks and strategies to accelerate scale-up in countries. Lancet 2014, 384, 438–454. [Google Scholar] [CrossRef]
- Rowe-Murray, H.; Fisher, J. Baby friendly hospital practices: Cesarean section is a persistent barrier to early initiation of breastfeeding. Birth 2002, 29, 125–131. [Google Scholar] [CrossRef]
- Geiser, A. Social Exclusion and Conflict Transformation in Nepal: Women, Dalit and Ethnic Groups Fast Country Risk Profile Nepal. Available online: http://edoc.vifapol.de/opus/volltexte/2011/2436/ (accessed on 20 January 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khanal, V.; Scott, J.A.; Lee, A.H.; Karkee, R.; Binns, C.W. Factors associated with Early Initiation of Breastfeeding in Western Nepal. Int. J. Environ. Res. Public Health 2015, 12, 9562-9574. https://doi.org/10.3390/ijerph120809562
Khanal V, Scott JA, Lee AH, Karkee R, Binns CW. Factors associated with Early Initiation of Breastfeeding in Western Nepal. International Journal of Environmental Research and Public Health. 2015; 12(8):9562-9574. https://doi.org/10.3390/ijerph120809562
Chicago/Turabian StyleKhanal, Vishnu, Jane A. Scott, Andy H. Lee, Rajendra Karkee, and Colin W. Binns. 2015. "Factors associated with Early Initiation of Breastfeeding in Western Nepal" International Journal of Environmental Research and Public Health 12, no. 8: 9562-9574. https://doi.org/10.3390/ijerph120809562