
Comparison of Anthropometric and Atherogenic Indices as Screening Tools of Metabolic Syndrome in the Kazakh Adult Population in Xinjiang


Abstract
:1. Introduction
2. Methods
2.1. Ethics Statement
2.2. Setting and Study Population
2.3. Questionnaire Survey
2.4. Serial Test and Parallel Test
2.5. Anthropometric Measurements and Laboratory Tests
2.6. Definition of MetS
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
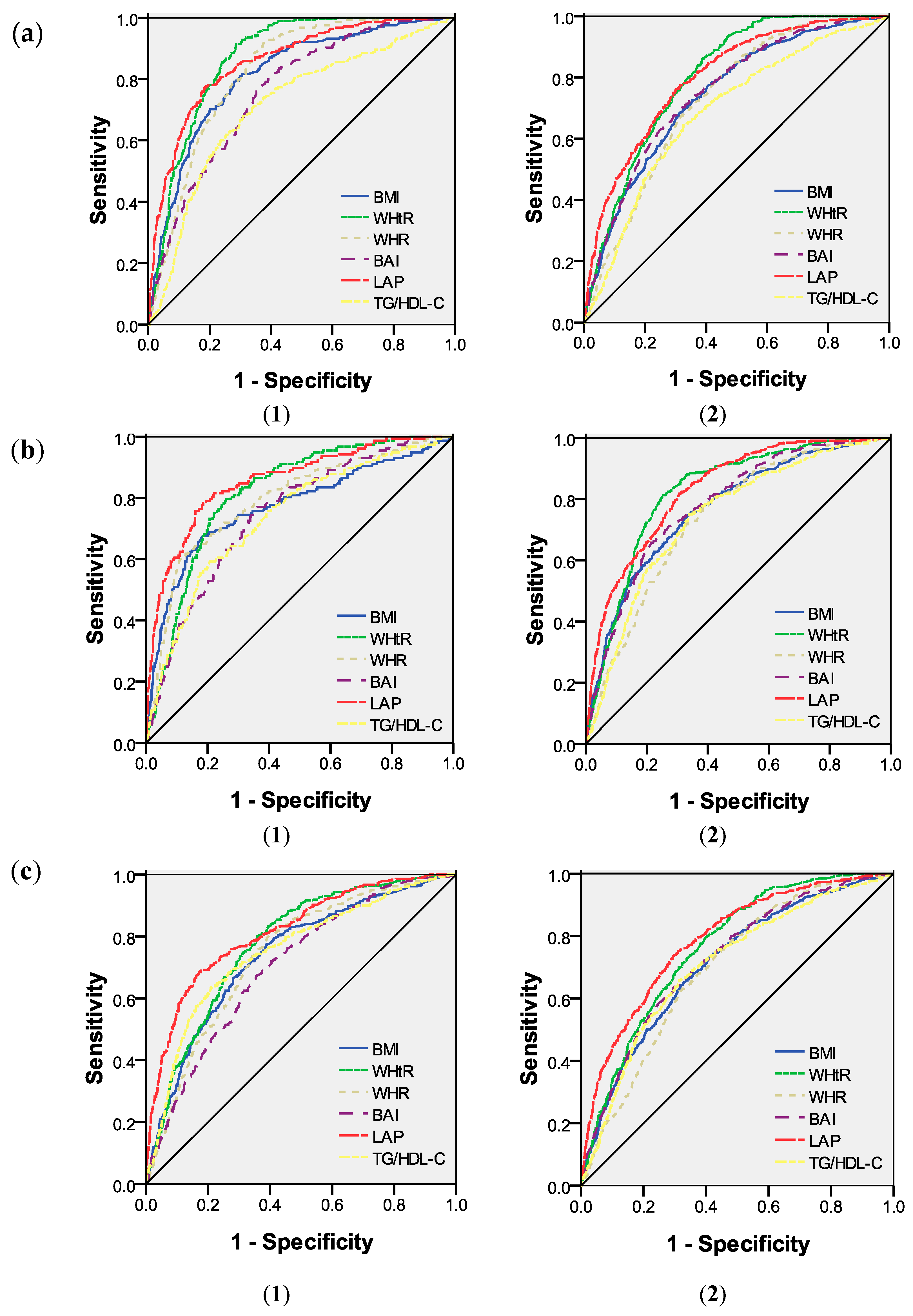
3.2. AUC of Each Variable for the Screening of MetS Using ROC Analyses
3.3. Cut-of, Sensitivity, Specificity and Youden’s Index of Each Variable According to the Different Criteria
3.4. Combined Screening Evaluation
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Magliano, D.J.; Shaw, J.E.; Zimmet, P.Z. How to best define the metabolic syndrome. Ann. Med. 2006, 38, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsén, B.; Lahti, K.; Nissén, M.; Taskinen, M.-R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Mozumdar, A.; Liguori, G. Persistent increase of prevalence of metabolic syndrome among US adults: NHANES III to NHANES 1999–2006. Diabetes Care 2011, 34, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Almoosawi, S.; Prynne, C.; Hardy, R.; Stephen, A. Time-of-day and nutrient composition of eating occasions: Prospective association with the metabolic syndrome in the 1946 British birth cohort. Int. J. Obes. 2013, 37, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.-F.; Reynolds, K.; Yang, W.-J. The prevalence of metabolic syndrome in the general adult population aged 35–74 years in China. Chin. J. Diabetes 2005, 13, 181–186. [Google Scholar]
- Sinha, S.; Misra, P.; Kant, S.; Krishnan, A.; Nongkynrih, B.; Vikram, N.K. Prevalence of metabolic syndrome and its selected determinants among urban adult women in South Delhi, India. Postgrad. Med. J. 2013, 89, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.Q.; Deng, J.; He, L.P.; Ling, W.H.; Su, Y.X.; Chen, Y.M. Comparison of various anthropometric and body fat indices in identifying cardiometabolic disturbances in Chinese men and women. PLoS ONE 2013, 8, e70893. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.D.; Yang, Y.N.; Ma, Y.T.; Pan, S.; He, C.H.; Liu, F.; Ma, X.; Fu, Z.Y.; Li, X.M.; Xie, X.; et al. Waist-to-Height Ratio and Triglycerides/High-Density Lipoprotein Cholesterol Were the Optimal Predictors of Metabolic Syndrome in Uighur Men and Women in Xinjiang, China. Metab. Syndr. Relat. Disord 2015, 13, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.D.; He, C.H.; Ma, Y.T.; Yang, Y.N.; Liu, F.; Pan, S.; Ma, X.; Li, X.M.; Fu, Z.Y.; Xie, X.; et al. Best anthropometric and atherogenic predictors of metabolic syndrome in the Chinese Han population in Xinjiang: The cardiovascular risk survey. Ann. Nutr. Metab. 2014, 65, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.-K.; Koo, M. Lipid accumulation product: A simple and accurate index for predicting metabolic syndrome in Taiwanese people aged 50 and over. BMC Cardiovasc. Disord. 2012, 12, 78. [Google Scholar] [CrossRef] [PubMed]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Liu, A.; Zhang, Y.; Wang, P. Waist-to-height ratio and cardiovascular risk factors among Chinese adults in Beijing. PLoS ONE 2013, 8, e69298. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Reynolds, K.; Wu, X.; Chen, J.; Duan, X.; Reynolds, R.F.; Whelton, P.K.; He, J.; Group, I.C. Prevalence of the metabolic syndrome and overweight among adults in China. Lancet 2005, 365, 1398–1405. [Google Scholar] [CrossRef]
- Motala, A.A.; Esterhuizen, T.; Pirie, F.J.; Omar, M.A. The prevalence of metabolic syndrome and determination of the optimal waist circumference cutoff points in a rural South African community. Diabetes Care 2011, 34, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Khanam, M.A.; Qiu, C.; Lindeboom, W.; Streatfield, P.K.; Kabir, Z.N.; Wahlin, A. The metabolic syndrome: Prevalence, associated factors, and impact on survival among older persons in rural Bangladesh. PLoS ONE 2011, 6, e20259. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.-F.; Hayashi, T.; Zhang, X.-J.; Funami, J.; Ge, L.; Li, J.; Huang, X.-L.; Cao, L.; Zhang, J.; Akihisa, I. Risks of CHD identified by different criteria of metabolic syndrome and related changes of adipocytokines in elderly postmenopausal women. J. Diabetes Complic. 2007, 21, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.M.; Park, J.; Ryu, S.Y.; Kim, J. The effect of menopause on the metabolic syndrome among Korean women the Korean National Health and Nutrition Examination Survey, 2001. Diabetes Care 2007, 30, 701–706. [Google Scholar] [CrossRef]
- Cho, G.J.; Lee, J.H.; Park, H.T.; Shin, J.H.; Hong, S.C.; Kim, T.; Hur, J.Y.; Lee, K.W.; Park, Y.K.; Kim, S.H. Postmenopausal status according to years since menopause as an independent risk factor for the metabolic syndrome. Menopause 2008, 15, 524–529. [Google Scholar] [PubMed]
- Müller, M.; Lagerpusch, M.; Enderle, J.; Schautz, B.; Heller, M.; Bosy-Westphal, A. Beyond the body mass index: Tracking body composition in the pathogenesis of obesity and the metabolic syndrome. Obes. Rev. 2012, 13 (Suppl. 2), 6–13. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Kahn, H.S. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: A population-based comparison. BMC Cardiovasc. Disord. 2005, 5, 26. [Google Scholar] [CrossRef] [PubMed]
- Gasevic, D.; Frohlich, J.; Mancini, G.; Lear, S.A. Clinical usefulness of lipid ratios to identify men and women with metabolic syndrome: A cross-sectional study. Lipids Health Dis. 2014, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Guo, S.; Zhang, J.; Ma, R.; Rui, D.; Xu, S.; Sun, F.; Hu, A.; Yang, Z. Study on the prevalence of metabolic syndrome among the Kazakh population in Xinjiang. Zhonghua Liu Xing Bing Xue Za Zhi 2010, 31, 747–750. [Google Scholar] [PubMed]
- Guo, H.; Ru-Lin, M.A.; Zhang, J.Y.; Rui, D.S.; Shang-Zhi, X.U.; Sun, F. Comparative analysis of epidemic characteristic of metabolic syndrome of Kazakh and Hans in Xinjiang. Chin. J. Hypertens. 2011, 19, 538–543. [Google Scholar]
- He, J.; Guo, S.; Liu, J.; Zhang, M.; Ding, Y.; Zhang, J.; Li, S.; Xu, S.; Niu, Q.; Guo, H. Ethnic Differences in Prevalence of General Obesity and Abdominal Obesity among Low-Income Rural Kazakh and Uyghur Adults in Far Western China and Implications in Preventive Public Health. PLoS ONE 2014, 9, e106723. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.-S.; Guo, S.-X.; Ma, R.-L.; Li, S.-G.; Guo, H.; Zhang, J.-Y.; Zhang, M.; Liu, J.-M.; He, J.; Yan, Y.-Z. Association of Metabolic Syndrome with the Adiponectin to Homeostasis Model Assessment of Insulin Resistance Ratio. Mediat. Inflamm. 2015. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.; Zimmet, P.; Shaw, J.; Group, I.E.T.F.C. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C. Diagnosis and management of the metabolic syndrome an American Heart Association/National Heart, Lung, and Blood Institute scientific statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef]
- Alberti, K.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- EpiData Software. Available online: http:/www.epidata.dk/ (accessed on 1 March 2016).
- Hosmer, D.W.; Lemeshow, S.; Cook, E. Applied Logistic Regression, 2nd ed.; John Wiley & Sons: New York, NY, USA, 2000. [Google Scholar]
- Zuo, H.; Shi, Z.; Hu, X.; Wu, M.; Guo, Z.; Hussain, A. Prevalence of metabolic syndrome and factors associated with its components in Chinese adults. Metabolism 2009, 58, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Hong, X.; Li, Z.; Zhang, W.; Jin, D.; Liu, X.; Zhang, Y.; Hu, F.B.; Wei, L.J.; Zang, T. Prevalence of metabolic syndrome and its relation to body composition in a Chinese rural population. Obesity 2006, 14, 2089–2098. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Huang, J.; Xu, G.; Yang, Z.; Liu, M.; Mi, Y.; Liu, W.; Wang, H.; Qian, D. Prevalence and determinants of metabolic syndrome among women in Chinese rural areas. PLoS ONE 2012, 7, e36936. [Google Scholar] [CrossRef] [PubMed]
- Fakhrzadeh, H.; Ebrahimpour, P.; Pourebrahim, R.; Heshmat, R.; Larijani, B. Metabolic Syndrome and its Associated Risk Factors in Healthy Adults: A Population-Based Study in Iran. Metab. Syndr. Relat. Disord. 2006, 4, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Paajanen, T.A.; Oksala, N.K.; Kuukasjärvi, P.; Karhunen, P.J. Short stature is associated with coronary heart disease: A systematic review of the literature and a meta-analysis. Eur. Heart J. 2010, 31, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, K.M.; Lindblad, U.; Ågren, B.; Nilsson-Ehle, P.; Råstam, L. Associations between body height, body composition and cholesterol levels in middle-aged men: The coronary risk factor study in southern Sweden (CRISS). Eur. J. Epidemiol. 2001, 17, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Taverna, M.J.; Martínez-Larrad, M.T.; Frechtel, G.D.; Serrano-Ríos, M. Lipid accumulation product: A powerful marker of metabolic syndrome in healthy population. Eur. J. Endocrinol. 2011. [Google Scholar] [CrossRef]
- Hamdy, O.; Porramatikul, S.; Al-Ozairi, E. Metabolic obesity: The paradox between visceral and subcutaneous fat. Curr. Diabetes Rev. 2006, 2, 367–373. [Google Scholar] [PubMed]
- Nguyen-Duy, T.B.; Nichaman, M.Z.; Church, T.S.; Blair, S.N.; Ross, R. Visceral fat and liver fat are independent predictors of metabolic risk factors in men. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E1065–E1071. [Google Scholar] [CrossRef] [PubMed]
- Sam, S.; Haffner, S.; Davidson, M.H.; D’Agostino, R.B.; Feinstein, S.; Kondos, G.; Perez, A.; Mazzone, T. Hypertriglyceridemic waist phenotype predicts increased visceral fat in subjects with type 2 diabetes. Diabetes Care 2009, 32, 1916–1920. [Google Scholar] [CrossRef] [PubMed]
- Zainuddin, L.R.M.; Isa, N.; Muda, W.M.W.; Mohamed, H.J. The prevalence of metabolic syndrome according to various definitions and hypertriglyceridemic-waist in Malaysian adults. Int. J. Prev. Med. 2011, 2, 229–237. [Google Scholar] [PubMed]
- Shao, J.; Yu, L.; Shen, X.; Li, D.; Wang, K. Waist-to-height ratio, an optimal predictor for obesity and metabolic syndrome in Chinese adults. J. Nutr. Health Aging 2010, 14, 782–785. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Nanri, H.; Hara, M.; Higaki, Y.; Imaizumi, T.; Taguchi, N.; Sakamoto, T.; Horita, M.; Shinchi, K.; Tanaka, K. Optimal cutoff values of waist circumference and the discriminatory performance of other anthropometric indices to detect the clustering of cardiovascular risk factors for metabolic syndrome in Japanese men and women. Environ. Health Prev. Med. 2011, 16, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.-P.; Oh, D.-K.; Min, H.; Kim, C.-S.; Park, J.-K.; Kim, Y.; Kim, S.S. Prospective Study of Optimal Obesity Index Cutoffs for Predicting Development of Multiple Metabolic Risk Factors: The Korean Genome and Epidemiology Study. J. Epidemiol. 2012, 22, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Motamed, N.; Razmjou, S.; Hemmasi, G.; Maadi, M.; Zamani, F. Lipid accumulation product and metabolic syndrome: A population-based study in northern Iran, Amol. J. Endocrinol. Investing. 2015, 39, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Kahn, H.; Cheng, Y. Longitudinal changes in BMI and in an index estimating excess lipids among white and black adults in the United States. Int. J. Obes. 2008, 32, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, S.; Prud’homme, D.; Bouchard, C.; Tremblay, A.; Després, J.-P. Sex differences in the relation of visceral adipose tissue accumulation to total body fatness. Am. J. Clin. Nutr. 1993, 58, 463–467. [Google Scholar] [PubMed]


{kind=link}
| Parameters | Male (n = 1494) | p | Female (n = 2258) | p | ||
|---|---|---|---|---|---|---|
| With MetS (n = 278) | Without MetS (n = 1216) | With MetS (n = 525) | Without MetS (n = 1733) | |||
| Age (years) | 51.45 ± 11.09 | 43.51 ± 13.66 | <0.001 | 50.34 ± 11.76 | 41.23 ± 12.55 | <0.001 |
| Height (cm) | 171.43 ± 6.63 | 169.82 ± 7.04 | <0.001 | 159.20 ± 6.67 | 158.14 ± 6.36 | <0.001 |
| Weight (kg) | 80.83 ± 11.86 | 67.91 ± 10.77 | <0.001 | 66.65 ± 11.14 | 58.32 ± 10.11 | <0.001 |
| WC (cm) | 100.03 ± 7.78 | 84.91 ± 10.13 | <0.001 | 92.51 ± 9.38 | 80.51 ± 10.85 | <0.001 |
| Hip circumference (cm) | 105.39 ± 6.79 | 96.82 ± 7.55 | <0.001 | 103.49 ± 8.50 | 95.30 ± 8.69 | <0.001 |
| Systolic BP (mmHg) | 144.19 ± 21.54 | 128.52 ± 22.09 | <0.001 | 140.47 ± 26.60 | 121.77 ± 21.41 | <0.001 |
| Diastolic BP (mmHg) | 92.89 ± 14.15 | 82.31 ± 13.26 | <0.001 | 90.48 ± 14.84 | 78.72 ± 13.33 | <0.001 |
| TG (mmol/L) | 1.70 ± 0.78 | 1.16 ± 0.72 | <0.001 | 1.31 ± 0.66 | 0.98 ± 0.49 | <0.001 |
| HDL-C (mmol/L) | 1.21 ± 0.38 | 1.37 ± 0.56 | <0.001 | 1.29 ± 0.55 | 1.49 ± 0.66 | <0.001 |
| FBG (mmol/L) | 6.02 ± 1.08 | 4.89 ± 1.12 | <0.001 | 5.55 ± 1.24 | 4.77 ± 0.92 | <0.001 |
| BMI | 27.82 ± 3.73 | 23.53 ± 3.39 | 0.005 | 26.68 ± 4.27 | 23.13 ± 3.72 | 0.005 |
| WHtR | 0.59 ± 0.05 | 0.50 ± 0.05 | <0.001 | 0.59 ± 0.06 | 0.51 ± 0.07 | <0.001 |
| WHR | 0.95 ± 0.04 | 0.88 ± 0.06 | <0.001 | 0.89 ± 0.05 | 0.84 ± 0.07 | <0.001 |
| BAI | 29.48 ± 3.88 | 25.84 ± 3.85 | <0.001 | 34.20 ± 5.11 | 29.73 ± 4.68 | <0.001 |
| LAP | 59.43 ± 28.89 | 23.49 ± 19.28 | <0.001 | 44.09 ± 22.12 | 22.13 ± 16.25 | <0.001 |
| TG/HDL-C | 1.55 ± 0.88 | 1.02 ± 0.80 | <0.001 | 1.17 ± 0.88 | 0.80 ± 0.69 | <0.001 |
| MetS-IDF | 278 (18.61%) | - | 525 (23.25%) | 0.001 | ||
| MetS-ATP III | 157 (10.51%) | - | 336 (14.88%) | <0.001 | ||
| MetS-JIS | 371 (24.83%) | - | 572 (25.33%) | 0.730 | ||
| Parameters | IDF Criteria | ATP III Criteria | JIS Criteria | |||
|---|---|---|---|---|---|---|
| AUC (95% CI) in Male | AUC (95% CI) in Female | AUC (95% CI) in Male | AUC (95% CI) in Female | AUC (95% CI) in Male | AUC (95% CI) in Female | |
| BMI | 0.815 (0.788, 0.842) | 0.744 (0.721, 0.767) | 0.772 (0.727, 0.817) | 0.771 (0.744, 0.798) | 0.74 (0.712, 0.769) | 0.713 (0.689, 0.737) |
| WHtR | 0.872 (0.854, 0.891) | 0.804 (0.786, 0.822) | 0.818 (0.787, 0.848) | 0.825 (0.803, 0.847) | 0.777 (0.751, 0.802) | 0.764 (0.743, 0.784) |
| WHR | 0.827 (0.804, 0.849) | 0.731 (0.709, 0.753) | 0.795 (0.756, 0.834) | 0.74 (0.714, 0.766) | 0.741 (0.713, 0.768) | 0.698 (0.675, 0.721) |
| BAI | 0.761 (0.733, 0.790) | 0.754 (0.731, 0.776) | 0.747 (0.709, 0.786) | 0.783 (0.758, 0.808) | 0.705 (0.675, 0.734) | 0.726 (0.702, 0.749) |
| LAP | 0.858 (0.834, 0.882) | 0.801 (0.781, 0.822) | 0.856 (0.823, 0.889) | 0.832 (0.811, 0.854) | 0.816 (0.791, 0.842) | 0.788 (0.767, 0.809) |
| TG/HDL-C | 0.715 (0.681, 0.749) | 0.688 (0.663, 0.714) | 0.739 (0.697, 0.780) | 0.742 (0.715, 0.770) | 0.752 (0.723, 0.782) | 0.707 (0.683, 0.732) |
| Parameters | IDF Criteria | ATP III Criteria | JIS Criteria | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off | Sen (%) | Spe (%) | Youden’s Index | Cut-off | Sen (%) | Spe (%) | Youden’s Index | Cut-off | Sen (%) | Spe (%) | Youden’s Index | |
| Male | ||||||||||||
| BMI | 24.84 | 79.10 | 72.00 | 0.511 | 26.72 | 67.50 | 81.70 | 0.492 | 23.73 | 77.60 | 61.10 | 0.387 |
| WHtR | 0.53 | 88.49 | 72.04 | 0.605 | 0.58 | 79.60 | 74.00 | 0.536 | 0.52 | 80.50 | 64.10 | 0.446 |
| WHR | 0.89 | 90.40 | 62.20 | 0.526 | 0.94 | 61.10 | 88.40 | 0.495 | 0.89 | 80.30 | 60.20 | 0.405 |
| BAI | 26.82 | 77.70 | 64.10 | 0.418 | 27.14 | 77.10 | 63.80 | 0.409 | 26.82 | 67.70 | 64.30 | 0.32 |
| LAP | 34.76 | 77.70 | 81.10 | 0.588 | 41.21 | 78.30 | 81.40 | 0.597 | 34.76 | 68.50 | 82.90 | 0.514 |
| TG/HDL-C | 1.08 | 68.30 | 68.80 | 0.371 | 1.20 | 59.20 | 79.30 | 0.385 | 1.20 | 63.90 | 78.60 | 0.425 |
| Female | ||||||||||||
| BMI | 24.35 | 68.40 | 68.70 | 0.371 | 24.50 | 73.80 | 67.40 | 0.412 | 24.33 | 64.20 | 68.10 | 0.323 |
| WHtR | 0.52 | 84.00 | 62.44 | 0.464 | 0.55 | 81.80 | 69.50 | 0.513 | 0.52 | 79.40 | 60.40 | 0.398 |
| WHR | 0.85 | 78.90 | 57.20 | 0.361 | 0.86 | 77.40 | 61.70 | 0.391 | 0.85 | 74.30 | 56.70 | 0.31 |
| BAI | 31.45 | 69.10 | 68.00 | 0.371 | 33.16 | 66.40 | 77.80 | 0.442 | 31.45 | 65.00 | 68.70 | 0.337 |
| LAP | 26.49 | 76.20 | 69.80 | 0.460 | 28.15 | 81.30 | 74.60 | 0.559 | 26.49 | 74.00 | 70.30 | 0.443 |
| TG/HDL-C | 0.79 | 64.60 | 67.40 | 0.320 | 0.79 | 75.00 | 66.10 | 0.411 | 0.79 | 65.70 | 68.70 | 0.344 |
| Screening | Sen (%) | Spe (%) | False Negative Rate (%) | False Positive Rate (%) | Youden’s Index |
|---|---|---|---|---|---|
| Male | |||||
| WHtR, LAP parallel test | 95.32 | 65.46 | 4.68 | 34.54 | 0.608 |
| WHtR, LAP serial test | 70.86 | 88.16 | 29.14 | 11.84 | 0.590 |
| Female | |||||
| WHtR, LAP parallel test | 93.90 | 54.01 | 6.10 | 45.99 | 0.479 |
| WHtR LAP serial test | 66.29 | 78.19 | 33.71 | 21.81 | 0.445 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.-H.; Zhang, M.; He, J.; Yan, Y.-Z.; Ma, J.-L.; Wang, K.; Ma, R.-L.; Guo, H.; Mu, L.-T.; Ding, Y.-S.; et al. Comparison of Anthropometric and Atherogenic Indices as Screening Tools of Metabolic Syndrome in the Kazakh Adult Population in Xinjiang. Int. J. Environ. Res. Public Health 2016, 13, 428. https://doi.org/10.3390/ijerph13040428
Zhang X-H, Zhang M, He J, Yan Y-Z, Ma J-L, Wang K, Ma R-L, Guo H, Mu L-T, Ding Y-S, et al. Comparison of Anthropometric and Atherogenic Indices as Screening Tools of Metabolic Syndrome in the Kazakh Adult Population in Xinjiang. International Journal of Environmental Research and Public Health. 2016; 13(4):428. https://doi.org/10.3390/ijerph13040428
Chicago/Turabian StyleZhang, Xiang-Hui, Mei Zhang, Jia He, Yi-Zhong Yan, Jiao-Long Ma, Kui Wang, Ru-Lin Ma, Heng Guo, La-Ti Mu, Yu-Song Ding, and et al. 2016. "Comparison of Anthropometric and Atherogenic Indices as Screening Tools of Metabolic Syndrome in the Kazakh Adult Population in Xinjiang" International Journal of Environmental Research and Public Health 13, no. 4: 428. https://doi.org/10.3390/ijerph13040428