Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Mental Health and Behavioral Outcomes
2.2. Hurricane Exposure
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Changes in Mental Health Symptoms between Baseline and Follow-Up
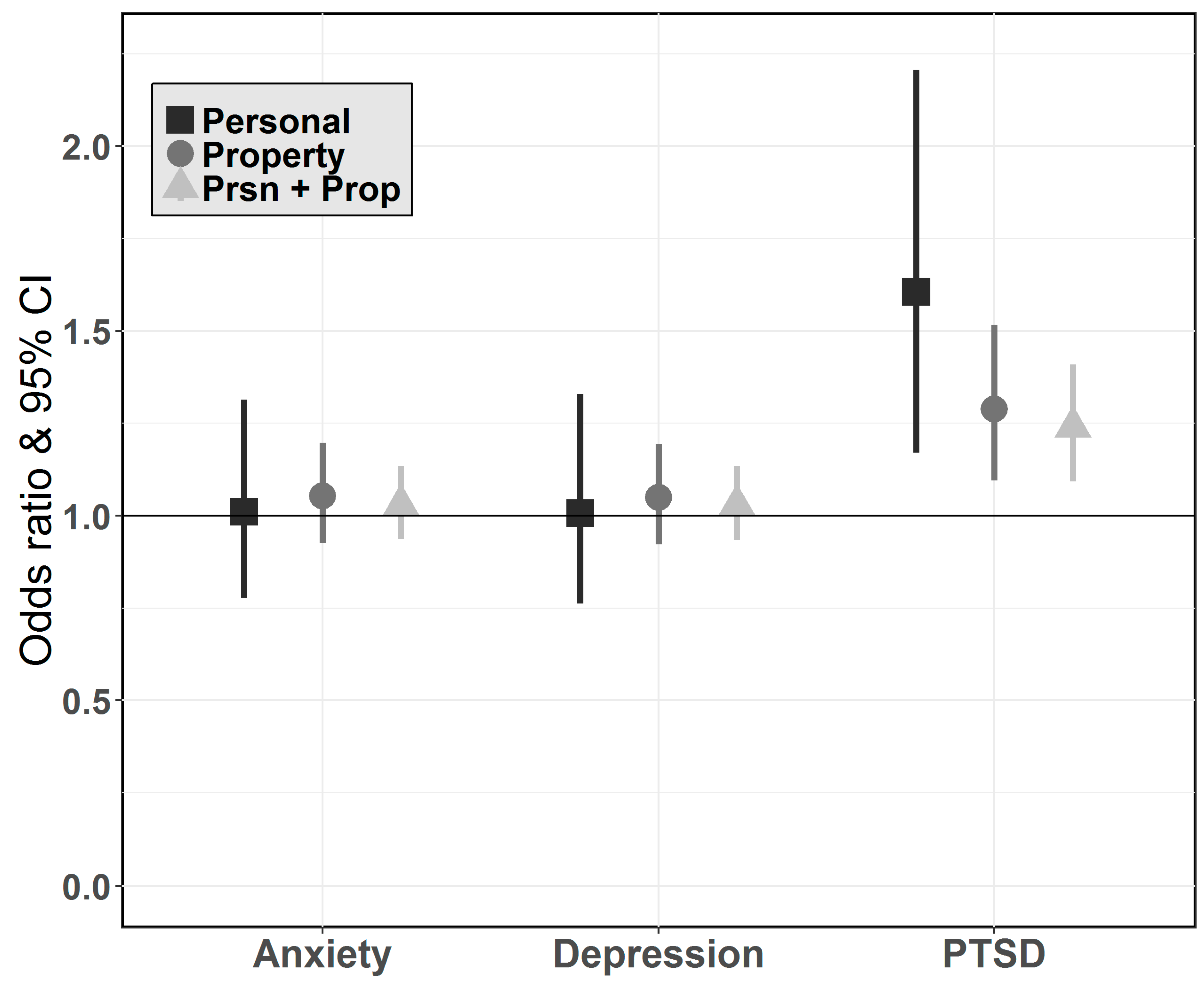
3.3. Factors Associated with Mental Health Symptoms at Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hurricane Research Division. The Thirty Costliest Mainland Us Tropical Cyclones 1900–2013. National Oceanic & Atmostpheric Administration, 2014. Available online: http://www.aoml.noaa.gov/hrd/tcfaq/costliesttable.html (accessed on 6 April 2016).
- Centers for Disease Control and Prevention. Deaths associated with hurricane sandy—October–november 2012. Morb. Mortal. Wkly. Rep. 2013, 62, 393–397. [Google Scholar]
- Staff, C.W. Superstorm Sandy: By the Numbers. Available online: http://www.cnn.com/2012/10/30/us/sandy-by-the-numbers/ (accessed on 3 April 2016).
- Abramson, D.; Alst, D.V.; Beedasy, J.; Findley, P.; Peek, L. Person report: The Sandy Child & Family Health Study. Columbia University National Center for Disaster Preparedness; New York University College of Global Public Health; Rutgers School of Social Work, 2015; Available online: https://www.researchgate.net/publication/280925388_Sandy_Child_and_Family_Health_Study_PERSON_Report (accessed on 6 April 2016).
- Boscarino, J.A. Community disasters, psychological trauma, and crisis intervention. Int. J. Emerg. Mental Health 2015, 17, 369–371. [Google Scholar]
- Caramanica, K.; Brackbill, R.M.; Stellman, S.D.; Farfel, M.R. Posttraumatic stress disorder after hurricane sandy among persons exposed to the 9/11 disaster. Int. J. Emerg. Mental Health 2015, 17, 356–362. [Google Scholar] [CrossRef]
- Galea, S.; Nandi, A.; Vlahov, D. The epidemiology of post-traumatic stress disorder after disasters. Epidemiol. Rev. 2005, 27, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Neria, Y.; Shultz, J.M. Mental health effects of hurricane sandy: Characteristics, potential aftermath, and response. JAMA 2012, 308, 2571–2572. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Chan, C.; Paxson, C.; Rouse, C.E.; Waters, M.; Fussell, E. The impact of hurricane katrina on the mental and physical health of low-income parents in new orleans. Am. J. Orthopsychiatry 2010, 80, 237. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Tracy, M.; Norris, F.; Coffey, S.F. Financial and social circumstances and the incidence and course of ptsd in mississippi during the first two years after hurricane katrina. J. Trauma. Stress 2008, 21, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Galea, S.; Gruber, M.J.; Sampson, N.A.; Ursano, R.J.; Wessely, S. Trends in mental illness and suicidality after hurricane katrina. Mol. Psychiatry 2008, 13, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Paxson, C.; Fussell, E.; Rhodes, J.; Waters, M. Five years later: Recovery from post traumatic stress and psychological distress among low-income mothers affected by hurricane katrina. Soc. Sci. Med. 2012, 74, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Heid, A.R.; Christman, Z.; Pruchno, R.; Cartwright, F.P.; Wilson-Genderson, M. Vulnerable, but why? Post-traumatic stress symptoms in older adults exposed to hurricane sandy. Disaster Med. Public Health Prep. 2016, 10, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Heid, A.R.; Pruchno, R.; Cartwright, F.P.; Wilson-Genderson, M. Exposure to hurricane sandy, neighborhood collective efficacy, and post-traumatic stress symptoms in older adults. Aging Ment. Health 2016, 21, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Hamama-Raz, Y.; Palgi, Y.; Shrira, A.; Goodwin, R.; Kaniasty, K.; Ben-Ezra, M. Gender differences in psychological reactions to hurricane sandy among new york metropolitan area residents. Psychiat. Quart. 2015, 86, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Palgi, Y.; Shrira, A.; Hamama-Raz, Y.; Palgi, S.; Goodwin, R.; Ben-Ezra, M. Not so close but still extremely loud: Recollection of the world trade center terror attack and previous hurricanes moderates the association between exposure to hurricane sandy and posttraumatic stress symptoms. Compr. Psychiatry 2014, 55, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Sampson, L.; Gruebner, O.; Galea, S. Mental health service need and use in the aftermath of hurricane sandy: Findings in a population-based sample of new york city residents. Community Ment. Health J. 2015, 52, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Manuel, J. The long road to recovery: Environmental health impacts of hurricane sandy. Environ. Health Perspect. 2013, 121, a152. [Google Scholar] [CrossRef] [PubMed]
- Gruebner, O.; Lowe, S.R.; Sampson, L.; Galea, S. The geography of post-disaster mental health: Spatial patterning of psychological vulnerability and resilience factors in new york city after hurricane sandy. Int. J. Health Geogr. 2015, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.M.; Rothenberg, P.; Kerath, S.M.; Liu, B.; Taioli, E. The lasting mental health effects of hurricane sandy on residents of the rockaways. J. Emerg. Manag. 2016, 14, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Schwartz, R.M.; Hirsch, J.; Silverman, R.; Liu, B.; Taioli, E. Effect of hurricane sandy on long island emergency departments visits. Disaster Med. Public Health Prep. 2016, 10, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.; Liu, B.; Sison, C.; Kerath, S.M.; Breil, T.; Murphy, L.; Taioli, E. Study design and results of a population-based study on perceived stress following hurricane sandy. Disaster Med. Public Health Prep. 2016, 10, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.M.; Sison, C.; Kerath, S.M.; Murphy, L.; Breil, T.; Sikavi, D.; Taioli, E. The impact of hurricane sandy on the mental health of new york area residents. Am. J. Disaster Med. 2014, 10, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Lieberman-Cribbin, W.; Liu, B.; Schneider, S.; Schwartz, R.; Taioli, E. Self-reported and fema flood exposure assessment after hurricane sandy: Association with mental health outcomes. PLoS ONE 2017, 12, e0170965. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Lowe, B. An ultra-brief screening scale for anxiety and depression: The phq-4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [PubMed]
- Ruggiero, K.J.; Del Ben, K.; Scotti, J.R.; Rabalais, A.E. Psychometric properties of the ptsd checklist-civilian version. J. Trauma. Stress 2003, 16, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Health, U.D.O.; Services, H. US Department of Agriculture. Dietary Guidelines for Americans 2015–2020; Skyhorse Publishing Inc.: New York, NY, USA, 2016. [Google Scholar]
- Galea, S.; Brewin, C.R.; Gruber, M.; Jones, R.T.; King, D.W.; King, L.A.; McNally, R.J.; Ursano, R.J.; Petukhova, M.; Kessler, R.C. Exposure to hurricane-related stressors and mental illness after hurricane katrina. Arch Gen. Psychiatry 2007, 64, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Sampson, L.; Gruebner, O.; Galea, S. Community unemployment and disaster-related stressors shape risk for posttraumatic stress in the longer-term aftermath of hurricane sandy. J Trauma. Stress 2016, 29, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.A. Secondary trauma or secondary disaster? Insights from hurricane katrina. Sociol. Spectrum 2007, 27, 613–632. [Google Scholar] [CrossRef]
- Chan, C.S.; Lowe, S.R.; Weber, E.; Rhodes, J.E. The contribution of pre-and postdisaster social support to short-and long-term mental health after hurricanes katrina: A longitudinal study of low-income survivors. Soc. Sci. Med. 2015, 138, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Rhodes, J.E. Trajectories of psychological distress among low-income, female survivors of hurricane katrina. Am. J Orthopsychiat. 2013, 83, 398–412. [Google Scholar] [CrossRef] [PubMed]
- Glass, K.; Flory, K.; Hankin, B.L.; Kloos, B.; Turecki, G. Are coping strategies, social support, and hope associated with psychological distress among hurricane katrina survivors? J. Soc. Clin. Psychol. 2009, 28, 779–795. [Google Scholar] [CrossRef]
- Pina, A.A.; Villalta, I.K.; Ortiz, C.D.; Gottschall, A.C.; Costa, N.M.; Weems, C.F. Social support, discrimination, and coping as predictors of posttraumatic stress reactions in youth survivors of hurricane katrina. J. Clin. Child Adolesc. Psychol. 2008, 37, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. Social and psychological resources and adaptation. Rev. Gen. Psychol. 2002, 6, 307. [Google Scholar] [CrossRef]
- Benight, C.C.; Ironson, G.; Klebe, K.; Carver, C.S.; Wynings, C.; Burnett, K.; Greenwood, D.; Baum, A.; Schneiderman, N. Conservation of resources and coping self-efficacy predicting distress following a natural disaster: A causal model analysis where the environment meets the mind. Anxiety Stress Coping 1999, 12, 107–126. [Google Scholar] [CrossRef]
- Bonanno, G.A.; Galea, S.; Bucciarelli, A.; Vlahov, D. What predicts psychological resilience after disaster? The role of demographics, resources, and life stress. J. Consult. Clin. Psychol. 2007, 75, 671. [Google Scholar] [CrossRef] [PubMed]
- Freedy, J.R.; Saladin, M.E.; Kilpatrick, D.G.; Resnick, H.S.; Saunders, B.E. Understanding acute psychological distress following natural disaster. J. Trauma. Stress 1994, 7, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Perilla, J.L.; Riad, J.K.; Kaniasty, K.; Lavizzo, E.A. Stability and change in stress, resources, and psychological distress following natural disaster: Findings from hurricane andrew. Anxiety Stress Coping 1999, 12, 363–396. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. Conservation of resources and disaster in cultural context: The caravans and passageways for resources. Psychiatry 2012, 75, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, M.E.; Santiago, C.D.; Einhorn, L. Coping with displacement from hurricane katrina: Predictors of one-year post-traumatic stress and depression symptom trajectories. Anxiety Stress Coping 2009, 22, 413–432. [Google Scholar] [CrossRef] [PubMed]
- Zwiebach, L.; Rhodes, J.; Roemer, L. Resource loss, resource gain, and mental health among survivors of hurricane katrina. J. Trauma. Stress 2010, 23, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, M.; Harville, E.; Xiong, X.; Buekens, P.; Pridjian, G.; Elkind-Hirsch, K. Loss of resources and hurricane experience as predictors of postpartum depression among women in Southern Louisiana. J. Womens Health 2010, 19, 877–884. [Google Scholar] [CrossRef] [PubMed]
- Sampson, L.; Lowe, S.R.; Gruebner, O.; Cohen, G.H.; Galea, S. Perceived service need after hurricane sandy in a representative sample of survivors: The roles of community-level damage and individual-level stressors. Disaster Med. Public Health Prep. 2016, 10, 428–435. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, G.; Vasterling, J.J.; Han, X.; Tharp, A.T.; Davis, T.; Deitch, E.A.; Constans, J.I. Preexisting mental illness and risk for developing a new disorder after hurricane katrina. J. Nerv. Mental Dis. 2013, 201, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Sampson, L.; Gruebner, O.; Galea, S. Psychological resilience after hurricane sandy: The influence of individual-and community-level factors on mental health after a large-scale natural disaster. PLoS ONE 2015, 10, e0125761. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.; Litz, B.; Herman, D.; Huska, J.A.; Keane, T.M. The PTSD checklist (PCL): Reliability, validity, and diagnostic utility. In Proceedings of the Annual Convention of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 25 October 1993. [Google Scholar]
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Löwe, B.; Wahl, I.; Rose, M.; Spitzer, C.; Glaesmer, H.; Wingenfeld, K.; Schneider, A.; Brähler, E. A 4-item measure of depression and anxiety: Validation and standardization of the patient health questionnaire-4 (PHQ-4) in the general population. J. Affect. Disorders 2010, 122, 86–95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | N | % | |
|---|---|---|---|
| Sex | Male | 29 | 22.31 |
| Female | 101 | 77.69 | |
| Race/Ethnicity (missing n = 2) | White | 73 | 57.03 |
| Black | 25 | 19.53 | |
| Hispanic Ethnicity | 18 | 14.06 | |
| Other/Mixed | 12 | 9.38 | |
| Education (missing n = 1) | <High School | 7 | 5.43 |
| ≥High School | 122 | 94.57 | |
| Medical Insurance (missing n = 1) | No | 11 | 8.53 |
| Yes | 118 | 91.47 | |
| Problem Alcohol Drinkers | No | 98 | 75.38 |
| Yes | 32 | 24.62 | |
| Current Smoker | No | 116 | 89.23 |
| Yes | 14 | 10.77 | |
| Mental health History | No | 94 | 72.31 |
| Yes | 36 | 27.69 | |
| Anxiety (PHQ4 score) | <2 | 65 | 50.00 |
| ≥2 | 65 | 50.00 | |
| Depression (PHQ4 score) | <2 | 84 | 64.62 |
| ≥2 | 46 | 35.38 | |
| Post-Traumatic Stress Disorder (PTSD) (PCL-S) (missing n = 1) | <30 | 92 | 71.32 |
| ≥30 | 37 | 28.68 | |
| Mental Health problems | Never | 94 | 72.31 |
| Before | 17 | 13.08 | |
| After | 8 | 6.15 | |
| Before and After | 11 | 8.46 | |
| Mean ± SD | Median | Range | |
| Age (years, missing n = 1) | 49.73 ± 20.82 | 52 | 18–92 |
| Elapsed time between Sandy and Baseline questionnaire (months, missing n = 0) | 14.47 ± 3.26 | 13.13 | 11.8–27.9 |
| Personal damage score (missing n = 0) | 1.25 ± 1.64 | 1 | 0–8 |
| Property damage score (missing n = 0) | 4.04 ± 3.41 | 3 | 0–14 |
| Personal and propertydamage score (missing n = 0) | 5.28 ± 4.59 | 3.5 | 0–21 |
| Variables | Baseline | Follow-Up | p-Value | |||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Anxiety | <2 | 65 | 50.00 | 76 | 58.5 | 0.11a |
| ≥2 | 65 | 50.00 | 54 | 41.5 | ||
| Mean ± SD | 129 | 1.82 ± 1.84 | 129 | 1.49 ± 1.73 | 0.01b | |
| Depression | <2 | 84 | 64.62 | 90 | 69.23 | 0.38 a |
| ≥2 | 46 | 35.38 | 40 | 30.77 | ||
| Mean ± SD | 130 | 1.22 ± 1.72 | 130 | 1.10 ± 1.61 | 0.39 b | |
| PTSD | <30 | 92 | 71.32 | 97 | 75.19 | 0.44 a |
| ≥30 | 37 | 58.68 | 32 | 24.81 | ||
| Mean ± SD | 129 | 26.95 ± 12.72 | 129 | 24.97 ± 11.57 | 0.001 b | |
| Anxiety | Depression | PTSD | ||||
|---|---|---|---|---|---|---|
| Estimate | p-Value | Estimate | p-Value | Estimate | p-Value | |
| Total Exposure Model | ||||||
| Intercept | −0.80722 | 0.6603 | 0.79931 | 0.638 | 13.67105 | 0.2423 |
| Mental Health Baseline | 1.08977 | 0.0005 | 0.88404 | 0.0021 | 4.37012 | 0.0257 |
| Gender | 0.62258 | 0.0903 | 0.06906 | 0.8377 | 0.13119 | 0.9551 |
| Age | −0.00334 | 0.6791 | −0.00234 | 0.7529 | 0.05646 | 0.2685 |
| Black | −0.48665 | 0.2135 | 0.21294 | 0.5538 | 4.84212 | 0.0513 |
| Hispanic | 0.03364 | 0.8798 | −0.0386 | 0.8512 | −0.35384 | 0.8027 |
| Other/Mixed | 0.11276 | 0.8265 | 1.24303 | 0.01 | 0.60231 | 0.8592 |
| Education | 0.11743 | 0.8531 | −0.67738 | 0.2495 | −6.26434 | 0.1211 |
| Mental Health History | 0.90104 | 0.0093 | 0.90403 | 0.0049 | 6.97867 | 0.0016 |
| Medical Insurance | 0.23852 | 0.6571 | 0.09397 | 0.85 | 0.06583 | 0.9852 |
| Elapsed Time | 0.01763 | 0.5895 | 0.02444 | 0.419 | 0.35813 | 0.0887 |
| Total Exposure | 0.00999 | 0.7626 | −0.01537 | 0.6152 | 0.69631 | 0.0012 |
| Personal Exposure Model | ||||||
| Intercept | −0.66597 | 0.7154 | 0.79232 | 0.6389 | 15.93477 | 0.1785 |
| Mental Health Baseline | 1.10431 | 0.0004 | 0.87524 | 0.0022 | 4.94715 | 0.0126 |
| Gender | 0.65571 | 0.0736 | 0.07207 | 0.8299 | 0.56356 | 0.8111 |
| Age | −0.00349 | 0.6658 | −0.00286 | 0.7002 | 0.07215 | 0.1661 |
| Black | −0.54218 | 0.1628 | 0.20651 | 0.5625 | 4.26012 | 0.0886 |
| Hispanic | 0.04301 | 0.8477 | −0.01686 | 0.9351 | −0.95971 | 0.5088 |
| Other/Mixed | 0.10969 | 0.8311 | 1.22454 | 0.0111 | 1.40813 | 0.683 |
| Education | 0.0987 | 0.8761 | −0.66869 | 0.2542 | −6.85456 | 0.095 |
| Mental Health History | 0.92534 | 0.0075 | 0.90824 | 0.0046 | 7.1842 | 0.0014 |
| Medical Insurance | 0.21566 | 0.6891 | 0.06753 | 0.8922 | 0.46097 | 0.8988 |
| Elapsed Time | 0.01663 | 0.611 | 0.02378 | 0.4316 | 0.37249 | 0.0819 |
| Personal Exposure | −0.03755 | 0.6804 | −0.05971 | 0.4779 | 1.54794 | 0.0094 |
| Property Exposure Model | ||||||
| Intercept | −0.88509 | 0.6296 | 0.76053 | 0.6547 | 13.87039 | 0.2381 |
| Mental Health Baseline | 1.07513 | 0.0006 | 0.8802 | 0.0023 | 4.28154 | 0.0301 |
| Gender | 0.60858 | 0.097 | 0.06018 | 0.8583 | 0.23397 | 0.9204 |
| Age | −0.00365 | 0.6513 | −0.00226 | 0.7618 | 0.04895 | 0.3407 |
| Black | −0.464 | 0.2334 | 0.22806 | 0.5252 | 4.64593 | 0.0619 |
| Hispanic | 0.0457 | 0.8378 | −0.04226 | 0.8382 | −0.04199 | 0.9766 |
| Other/Mixed | 0.09979 | 0.8461 | 1.24465 | 0.01 | 0.33993 | 0.9208 |
| Education | 0.13396 | 0.8326 | −0.67249 | 0.2536 | −6.1866 | 0.1279 |
| Mental Health History | 0.89183 | 0.0099 | 0.89709 | 0.0052 | 7.08582 | 0.0014 |
| Medical Insurance | 0.2298 | 0.6685 | 0.10165 | 0.838 | −0.33084 | 0.9261 |
| Elapsed Time | 0.01762 | 0.5891 | 0.02474 | 0.4135 | 0.347 | 0.1006 |
| Property Exposure | 0.02684 | 0.5448 | −0.01349 | 0.7423 | 0.88476 | 0.0023 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwartz, R.M.; Gillezeau, C.N.; Liu, B.; Lieberman-Cribbin, W.; Taioli, E. Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms. Int. J. Environ. Res. Public Health 2017, 14, 957. https://doi.org/10.3390/ijerph14090957
Schwartz RM, Gillezeau CN, Liu B, Lieberman-Cribbin W, Taioli E. Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms. International Journal of Environmental Research and Public Health. 2017; 14(9):957. https://doi.org/10.3390/ijerph14090957
Chicago/Turabian StyleSchwartz, Rebecca M., Christina N. Gillezeau, Bian Liu, Wil Lieberman-Cribbin, and Emanuela Taioli. 2017. "Longitudinal Impact of Hurricane Sandy Exposure on Mental Health Symptoms" International Journal of Environmental Research and Public Health 14, no. 9: 957. https://doi.org/10.3390/ijerph14090957