Factors That Influence Linkages to HIV Continuum of Care Services: Implications for Multi-Level Interventions

 ,
,
Abstract
:1. Introduction
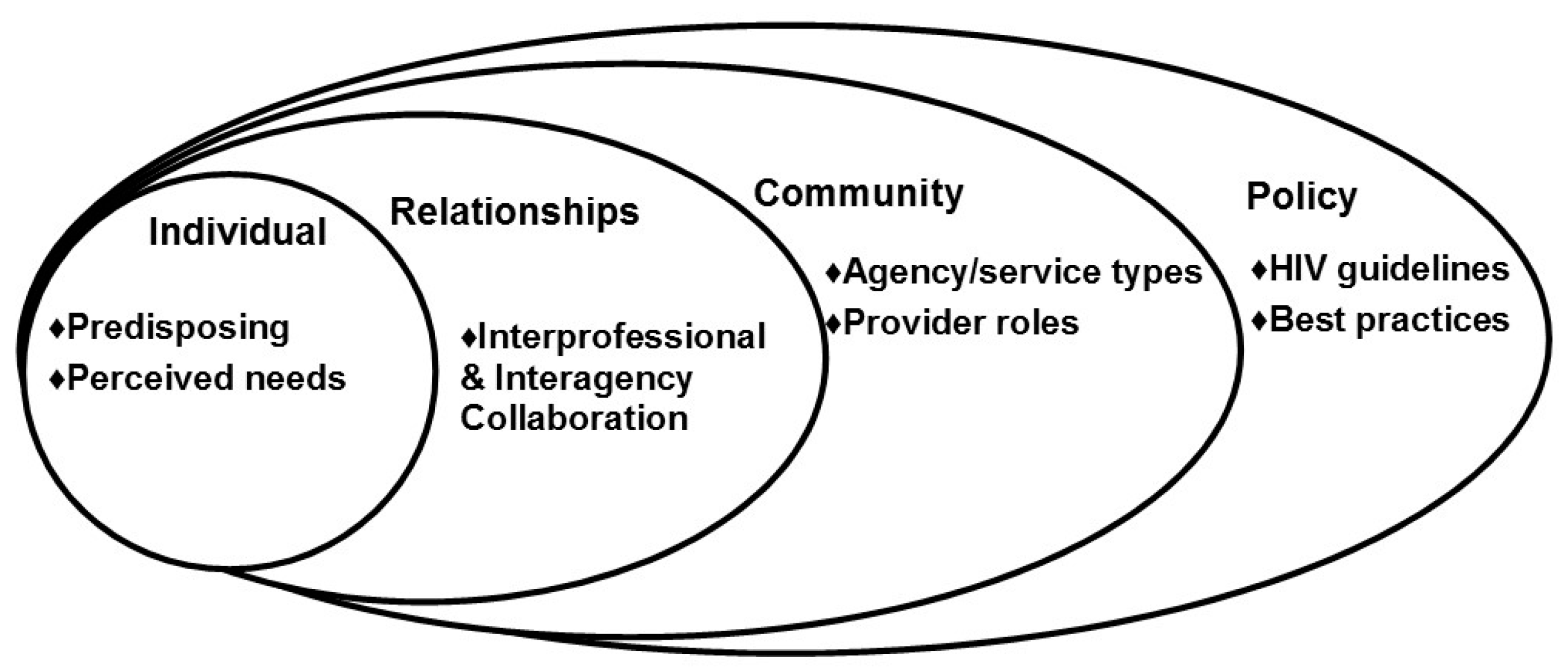
1.1. Conceptual Foundation
1.2. Factors that Influence Linkage-Making
2. Materials and Methods
2.1. Overview of Procedures for the Longitudinal Study
2.2. Criterion Sampling Strategy for In-Depth Interviews
2.3. Recruitment for In-Depth Interviews
2.4. Interview Protocol and Data Collection
2.5. Analytic Approach and Data Interpretation
3. Results
3.1. Sample Characteristics
3.2. Factors that Influence Linkage-Making
3.3. Individual Domain: Professional Knowledge Base
3.4. Relationship Domain: Interprofessional Collaboration
3.5. Community Domain: Providers’ Work-Related Changes
3.6. Policy Domain: Best Practices in a Competitive Environment
4. Discussion
4.1. Individual Domain: Professional Knowledge Base
4.2. Relationship Domain: Interprofessional Collaboration
4.3. Community Domain: Providers’ Work-Related Changes
4.4. Policy Domain: Best Practices in a Competitive Environment
4.5. Implications for Multi-Level Interventions and Future Research
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. HIV/AIDS. Global Health Observatory (GHO) Data 2016. Available online: http://www.who.int/gho/hiv/en/ (accessed on 29 December 2016).
- Centers for Disease Control and Prevention. Understanding the HIV Care Continuum; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017; pp. 1–4.
- World Health Organization. Clinical Guidelines Across the Continuum of Care: Linking People Diagnosed with HIV Infection to HIV Care and Treatment. In Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach June 13; World Health Organization: Geneva, Switzerland, 2013; p. 272. [Google Scholar]
- Cohen, M.S.; McCauley, M.; Gamble, T.R. HIV treatment as prevention and HPTN 052. Curr. Opin. HIV AIDS 2012, 7, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Dodd, P.J.; Garnett, G.P.; Hallett, T.B. Examining the promise of HIV elimination by ‘test and treat’ in hyperendemic settings. AIDS 2010, 24, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Porco, T.C.; Martin, J.N.; Page-Shafer, K.A.; Cheng, A.; Charlebois, E.; Grant, R.M.; Osmond, D.H. Decline in HIV infectivity following the introduction of highly active antiretroviral therapy. AIDS 2004, 18, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.A.; Mugavero, M.J.; Amico, K.R.; Cargill, V.A.; Chang, L.W.; Gross, R.; Orrell, C.; Altice, F.L.; Bangsberg, D.R.; Bartlett, J.G.; et al. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: Evidence-based recommendations from an international association of physicians in AIDS care panel. Ann. Intern. Med. 2012, 256, 817–833. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.M.; Spector, A.Y.; Rahman, R.; Gastolomendo, J.D. Research advisory board members’ contributions and expectations in the USA. Health Promot. Int. 2015, 30, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.M.; Spector, A.Y.; Valera, P.A. Exploring group dynamics for integrating scientific and experiential knowledge in community advisory boards for HIV research. AIDS Care 2011, 23, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Coates, T.J.; Richter, L.; Caceres, C. Behavioural strategies to reduce HIV transmission: How to make them work better. Lancet 2008, 372, 669–684. [Google Scholar] [CrossRef]
- Tross, S.; Campbell, A.N.C.; Cohen, L.R.; Calsyn, D.; Pavlicova, M.; Miele, G.; Hu, M.C.; Haynes, L.; Nugent, N.; Gan, W.; et al. Effectiveness of HIV/STD sexual risk reduction groups for women in substance abuse treatment programs: Results of NIDA clinical trials network trial. JAIDS J. Acquir. Immune Defic. Syndr. 2008, 48, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Integrated Prevention Services for HIV Infection, Viral Hepatitis, Sexually Transmitted Diseases, and Tuberculosis for Persons Who Use Drugs Illicitly: Summary Guidance from CDC and the U.S. Department of Health and Human Services; National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention: Atlanta, GA, USA, 2012; pp. 1–40.
- Choi, K.-H.; Hoff, C.; Gregorich, S.E.; Grinstead, O.; Gomez, C.; Hussey, W. The efficacy of female condom skills training in HIV risk reduction among women: A randomized controlled trial. Am. J. Public Health 2008, 98, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Mugavero, M.J.; Amico, K.R.; Horn, T.; Thompson, M.A. The state of engagement in HIV care in the United States: From cascade to continuum to control. Clin. Infect. Dis. 2013, 57, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Craw, J.; Gardner, L.; Rossman, A.; Gruber, D.; Noreen, O.; Jordan, D.; Rapp, R.; Simpson, C.; Phillips, K. Structural factors and best practices in implementing a linkage to HIV care program using the ARTAS model. BMC Health Serv. Res. 2010, 10, 246. [Google Scholar] [CrossRef] [PubMed]
- Rapp, R.C.; Ciomcia, R.; Zaller, N.; Draine, J.; Ferguson, A.; Cagey, R. The role of jails in engaging PLWHA in care: From jail to community. Aborig. Isl. Health Work J. 2013, 17 (Suppl. 2), S89–S99. [Google Scholar] [CrossRef] [PubMed]
- Gardner, L.; Metsch, L.; Anderson-Mahoney, P.; Loughlin, A.; Rio, C.; Strathdee, S.; Sansom, S.; Siegal, H.; Greenberg, A.; Holmberg, S.; et al. Efficacy of a brief case management intervention to link recently diagnosed HIV-infected persons to care. AIDS 2005, 19, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Pecoraro, A.; Royer-Malvestuto, C.; Rosenwasser, B.; Moore, K.; Howell, A.; Ma, M.; Woody, G.E. Factors contributing to dropping out from and returning to HIV treatment in an inner city primary care HIV clinic in the United States. AIDS Care 2013, 25, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Bradford, J.; Coleman, S.; Cunningham, W. HIV system navigation: An emerging model to improve HIV care access. AIDS Patient Care STDS 2007, 21 (Suppl. 1), S49–S58. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. High Impact Prevention: ARTAS; Effective Interventions. Available online: https://effectiveinterventions.cdc.gov/en/highimpactprevention/PublicHealthStrategies.aspx (accessed on 30 March 2015).
- Cheever, L. Engaging HIV-infected patients in care: Their lives depend on it. Clin. Infect. Dis. 2007, 44, 1500–1502. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Understanding the HIV Care Continuum; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2016; pp. 1–4.
- Cyrus, E.; Dawson, C.; Fennie, K.P.; Sheehan, D.M.; Mauck, D.E.; Sanchez, M.; Maddox, L.M.; Trepka, M.J. Disparity in retention in care and viral suppression for black caribbean-born immigrants living with HIV in Florida. Int. J. Environ. Res. Public Health 2017, 14, 285. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.M.; Mauck, D.E.; Fennie, K.P.; Cyrus, E.A.; Maddox, L.M.; Lieb, S.; Trepka, M.J. Black-white and country of birth disparities in retention in HIV care and viral suppression among Latinos with HIV in Florida, 2015. Int. J. Environ. Res. Public Health 2017, 14, 120. [Google Scholar] [CrossRef] [PubMed]
- Kurth, A.E.; Celum, C.; Baeten, J.M.; Vermund, S.H.; Wasserheit, J.N. Combination HIV prevention: Significance, challenges, and opportunities. Curr. HIV/AIDS Rep. 2010, 8, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Semaan, S.; Jarlais, D.C.D.; Sogolow, E.; Johnson, W.D.; Hedges, L.V.; Ramirez, G.; Flores, S.A.; Norman, L.; Sweat, M.D.; Needle, R. A meta-analysis of the effect of HIV prevention interventions on the sex behaviors of drug users in the United States. J. Acquir. Immune Defic. Syndr. 2002, 30 (Suppl. 1), S73–S93. [Google Scholar] [CrossRef] [PubMed]
- Gandelman, A.A.; DeSantis, L.M.; Rietmeijer, C.A. Assessing community needs and agency capacity—An integral part of implementing effective evidence based interventions. AIDS Educ. Prev. 2006, 18 (Suppl. A), 32–43. [Google Scholar] [CrossRef] [PubMed]
- Weiner, B.J. A theory of organizational readiness for change. Implement. Sci. 2009, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.R.; Reynolds, J.; Quan, M.A.; Call, S.; Crusto, C.A.; Kaufman, J.S. Measuring changes in interagency collaboration: An examination of the Bridgeport safe start initiative. Eval. Program Plann. 2007, 30, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Orchard, C.A.; Curran, V.; Kabene, S. Creating a culture for interdisciplinary collaborative professional PRACTICE. Med. Educ. Online 2005, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wittenberg-Lyles, E.; Oliver, D.P.; Demiris, G.; Regehr, K. Interdisciplinary collaboration in hospice team meetings. J. Interprof. Care 2010, 24, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Wright, A. Are fears of losing patients preventing appropriate referrals? Podiatry Today 2013, 26, 52–56. [Google Scholar]
- Kaaya, S.; Eustache, E.; Lapidos-Salaiz, I.; Musisi, S.; Psaros, C.; Wissow, L. Grand challenges: Improving HIV treatment outcomes by integrating interventions for co-morbid mental illness. PLoS Med. 2013, e1001447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, L.I.; Marks, G.; Metsch, L.R.; Loughlin, A.M.; O’Daniels, C.; Rio, C.D.; Anderson-Mahoney, P.; Wilkinson, J.D. Psychological and behavioral correlates of entering care for HIV infection: The Antiretroviral Treatment Access Study (ARTAS). AIDS Patient Care STDS 2007, 21, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Gruber, D.; Campos, P.; Dutcher, M.; Safford, L.; Phillips, K.; Craw, J.; Gardner, L. Linking recently diagnosed HIV-positive persons to medical care: Perspectives of referring providers. AIDS Care 2011, 23, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.M.; Spector, A.Y.; Yu, G.; Campbell, A.N.C. Transdisciplinary collaboration and endorsement of pharmacological and psychosocial evidence-based practices by medical and psychosocial substance abuse treatment providers in the United States. Drugs 2013, 20, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Rapp, C.A.; Etzel-Wise, D.; Marty, D.; Coffman, M.; Carlson, L.; Asher, D.; Callaghan, J. Evidence-based practice implementation strategies: Results of a qualitative study. Commun. Ment. Health J. 2007, 44, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Lavoie-Tremblay, M.; Sounan, C.; Lavigne, G.L.; Bonin, J.-P.; Lesage, A.D.; Denis, P.L.; Renaud, M.; Maisy, N.; Farand, L.; Racine, H. The psychosocial work environment and evidence utilization by health professionals. Can. J. Nurs. Res. 2008, 40, 112–128. [Google Scholar] [PubMed]
- Pinto, R.M.; Yu, G.; Spector, A.Y.; Gorroochurn, P.; McCarty, D. Substance abuse treatment providers’ involvement in research is associated with willingness to use findings in practice. J. Subst. Abuse Treat. 2010, 39, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research and Evaluation Methods, 3rd ed.; Sage Publications: London, UK, 2002. [Google Scholar]
- Ragin, C.C.; Becker, H.S. What is A Case? Exploring the Foundations of Social Inquiry; Cambridge University Press: Cambridge, UK, 1992. [Google Scholar]
- Bronstein, L.R. Index of interdisciplinary collaboration. Soc. Work Res. 2002, 26, 113–123. [Google Scholar] [CrossRef]
- Qantm Intellectual Property Ltd. NVivo Qualitative Data Analysis Software; QSR International: Doncaster, Australia, 2015. [Google Scholar]
- Lincoln, I.; Guba, E.G. Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985. [Google Scholar]
- Ajzen, I. The Theory of planned behavior. Org. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Perkins, M.B.; Jensen, P.S.; Jaccard, J.; Gollwitzer, P.; Oettingen, G.; Pappadopulos, E.; Hoagwood, K.E. Applying theory-driven approaches to understanding and modifying clinicians’ behavior: What do we know? Psychiatr. Serv. 2007, 58, 342. [Google Scholar] [CrossRef] [PubMed]
- Gardner, L.I.; Marks, G.; Craw, J.A.; Wilson, T.E.; Drainoni, M.-L.; Moore, R.D.; Mugavero, M.J.; Rodriguez, A.E.; Bradley-Springer, L.A.; Holman, S.; et al. A low-effort, clinic-wide intervention improves attendance for HIV primary care. Clin. Infect. Dis. 2012, 55, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Dombrowski, J.; Simoni, J.; Jane, M.; Katz, D.; Golden, M. Barriers to HIV care and treatment among participants in a public health HIV relinkage program. AIDS Patient Care STDs 2015, 29, 279. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Individual Domain: Professional Knowledge Base and Life Changes | I think by doing different trainings or webinars … bringing people together to talk about challenges, then brainstorming different resources, I think is helpful. Because you tend to only see things through your agency lens and have certain referrals or who you would go to. [Participant ID: A06P06] |
| I think that organizing interactive workshops where you’re sitting down with people from other agencies to try and figure out how to [link patients] is a good idea. [A01P14] | |
| I’m working on my master’s. I am starting to buy into the whole thing about collaboration. There were some classes I took that it was evident collaboration was important, where instead of it being one [provider], sometimes you need an outside [provider] along with you to observe while you’re doing it and vice versa. [A03P08] | |
| Relationship Domain: Interprofessional Collaboration | I said to everyone every time we have a case management meeting, “The [providers] in this room, we have a gold mine of resources. Every one of you have your own contact in every facility. Share that with your coworkers.” Because that’s the way to get in. We build—we know [providers] by name. They like that we know them by names. [A01P04] |
| I know these places exist, but without personal connections to those places, it feels like a shot in the dark [A01P14] | |
| You actually collaborate with your colleagues to know what agencies work, what don’t work. [A18P19] | |
| That’s been helpful to develop relationships so when somebody answers the phone I know who it is. “Is that really the earliest appointment?” “Don’t you have anything on Wednesday?” I feel our clients get better treatment. [A01P09] | |
| Community Domain: Providers’ Work-Related Changes | I feel like, before, I had less responsibility. I just had less responsibility, so I had more time to go more in-depth with different things. Whereas now, it’s more job responsibility and more out-of-work responsibility, has affected whether or not I’m focused on making referrals to people. [A01P14] |
| I would say when certain contracts end, [providers] get laid off or dismissed, you take on extra duties. When you take on extra duties that does affect how you collaborate because you have so much more to concentrate on instead of actually doing the actual collaboration. The client can suffer. [A03P08] | |
| In the last six months, one of the biggest changes is this managed care kit that’s coming out where everybody has to begin to really not only get to know the other agencies but begin collaboration for services that we don’t offer, so it’s been a lot of work. [A17P16] | |
| Policy Domain: Best Practices in a Competitive Environment | I just think it’s important to get outside of your own agency and promote how you can work collaboratively. Because I think people are worried that you are going to swoop in and steal their clients. And it is a legitimate fear. [A02P14] |
| It’s a very competitive world, and a lot of agencies feel that if they collaborate they will lose clients. If people would just get out of that mind frame and think that we’re all here together for one goal and we’re able to collaborate. [A12P12] | |
| That’s in the back of our minds, that we would not be sending somebody out to a non-evidence-based intervention… we definitely would be thinking about that. [A01P01] | |
| Yeah, that’s important to me also, because the evidence-based referral will show me that it worked. [A18P19] | |
| I think it’s about setting up a spirit of collaboration and delineating who does what and how we can help each other, and less of an environment of “you’re going to steal my clients”. [A02P14] |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, R.M.; Witte, S.S.; Filippone, P.L.; Baird, K.L.; Whitman, W.R. Factors That Influence Linkages to HIV Continuum of Care Services: Implications for Multi-Level Interventions. Int. J. Environ. Res. Public Health 2017, 14, 1355. https://doi.org/10.3390/ijerph14111355
Pinto RM, Witte SS, Filippone PL, Baird KL, Whitman WR. Factors That Influence Linkages to HIV Continuum of Care Services: Implications for Multi-Level Interventions. International Journal of Environmental Research and Public Health. 2017; 14(11):1355. https://doi.org/10.3390/ijerph14111355
Chicago/Turabian StylePinto, Rogério M., Susan S. Witte, Prema L. Filippone, Karen L. Baird, and Wendy R. Whitman. 2017. "Factors That Influence Linkages to HIV Continuum of Care Services: Implications for Multi-Level Interventions" International Journal of Environmental Research and Public Health 14, no. 11: 1355. https://doi.org/10.3390/ijerph14111355