A Comparison of Mental Health Care Systems in Northern and Southern Europe: A Service Mapping Study

 , , , and
, , , and
Abstract
:1. Introduction
- The typology and pattern of service availability, according to the main types of care and placement capacity,
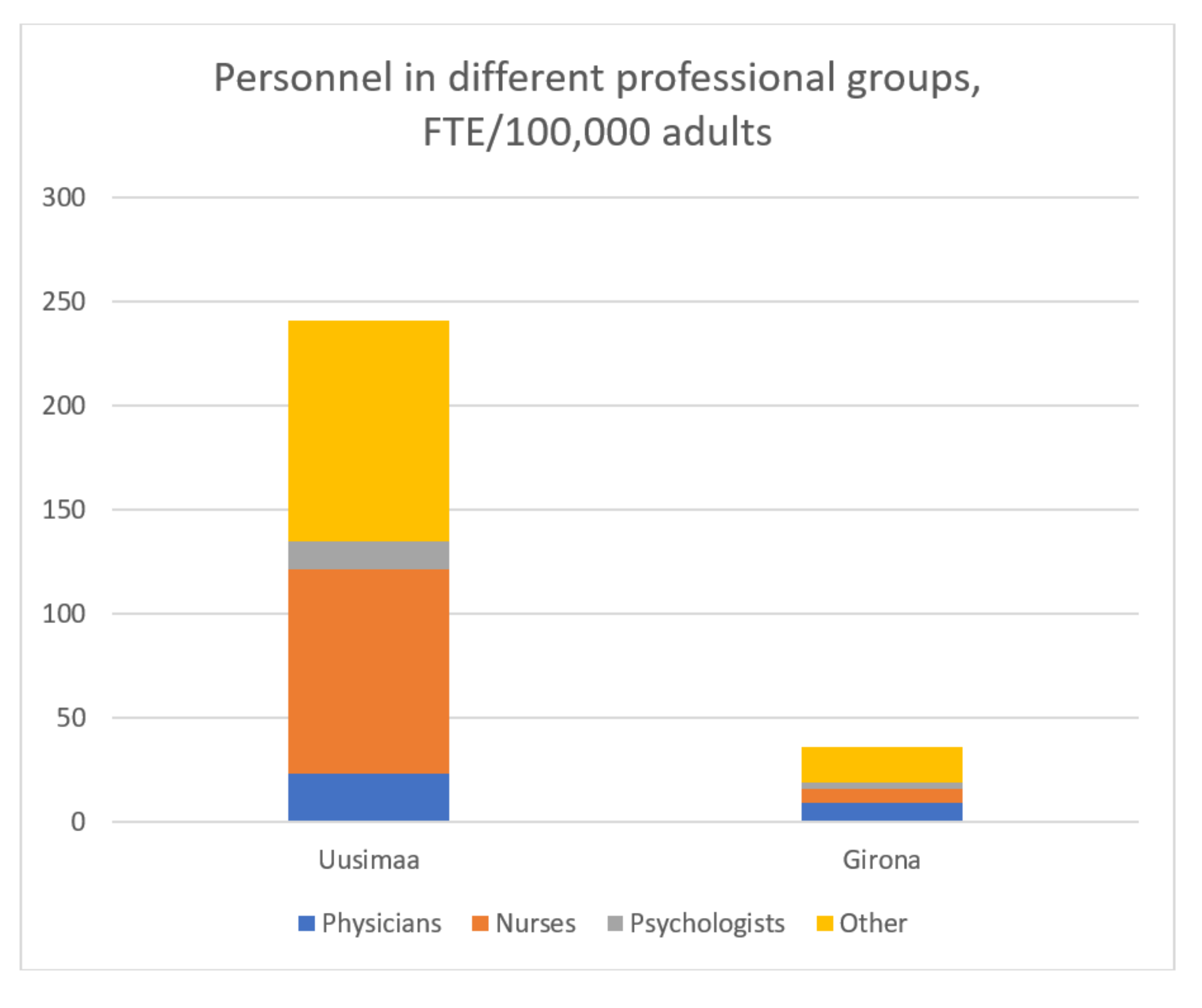
- the personnel resource allocation in different mental health professional groups, and
- the productivity of specialized services provided per personnel resource.
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England) 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Gutierrez-Colosia, M.R.; Salvador-Carulla, L.; Salinas-Perez, J.A.; Garcia-Alonso, C.R.; Cid, J.; Salazzari, D.; Montagni, I.; Tedeschi, F.; Cetrano, G.; Chevreul, K.; et al. Standard comparison of local mental health care systems in eight European countries. Epidemiol. Psychiatr. Sci. 2017, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Raine, R.; Fitzpatrick, R.; de Pury, J. Challenges, solutions and future directions in evaluative research. J. Health Serv. Res. Policy 2016, 21, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Rosenmöller, M.; McKee, M.; Baeten, R.; Glinos, I.A. Patient mobility: The context and issues. In Patient Mobility in the European Union Learning from Experience; Rosenmöller, M., McKee, M., Baeten, R., Eds.; WHO Regional Office, World Health Organization: Geneva, Switzerland, 2006; pp. 1–9. [Google Scholar]
- Unger, F.; Allinger, H.; Beckel, L.; Björnberg, A.; Brunnhuber, S.; Groth, H.; Haschke, F.; Heide, A.; Ittel, T.; Kashan, A.; et al. Health in the Regions: Cross Border Health Care: Harmonization in European Regions. European Institute of Health of the European Academy of Sciences and Arts. 2012. Available online: https://cor.europa.eu/en/documentation/studies/Documents/health-in-the-regions/health-in-the-regions.pdf (accessed on 20 May 2018).
- World Health Organization. World Health Organization Mental Health Action Plan 2013–2020; WHO Library Cataloguing-in-Publication Data, Ed.; World Health Organization: Geneva, Switzerland, 2013; ISBN 978-92-4-150602-1. [Google Scholar]
- Thornicroft, G.; Tansella, M. Components of a modern mental health service: A pragmatic balance of community and hospital care: Overview of systematic evidence. Br. J. Psychiatry 2004, 185, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Thornicroft, G.; Tansella, M. Balancing community-based and hospital-based mental health care. World Psychiatry 2002, 1, 84–90. [Google Scholar] [PubMed]
- Ministry of Social Affairs and Health. Plan for Mental Health and Substance Abuse Work; Final Evaluation of the Plan and Recommendations of the Steering Committee; Ministry of Social Affairs and Health: Helsinki, Finland, 2016.
- Ala-Nikkola, T.; Sadeniemi, M.; Kaila, M.; Saarni, S.; Kontio, R.; Pirkola, S.; Joffe, G.; Oranta, O.; Wahlbeck, K. How size matters: Exploring the association between quality of mental health services and catchment area size. BMC Psychiatry 2016, 16, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vuorenkoski, L.; Mladovsky, P.; Mossialos, E. Finland: Health system review. Health Syst. Transit. 2008, 10, 1–168. [Google Scholar]
- Sadeniemi, M.; Pirkola, S.; Pankakoski, M.; Joffe, G.; Kontio, R.; Malin, M.; Ala-Nikkola, T.; Wahlbeck, K. Does primary care mental health resourcing affect the use and costs of secondary psychiatric services? Int. J. Environ. Res. Public Health 2014, 11, 8743–8754. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, N.; Wahlbeck, K. From Reform intentions to Practice: Developments in Finnish Mental Health Care Since 1990; The National Institute for Health and Welfare: Helsinki, Finland, 2010; Available online: https://www.julkari.fi/bitstream/handle/10024/79925/d0d504f0-d878-4a19-97b3-e3b060f9b09a.pdf?sequence=1 (accessed on 31 May 2018).
- Wahlbeck, K.; Sailas, E.; Haaramo, P.; Vastamäki, M.; Joffe, G. Muutokset aikuisten ympärivuorokautisissa mielenterveyspalveluissa HUS-alueella 2012–2014. Lääkärilehti 2017, 72, 1429–1434. Available online: https://thl.fi/documents/974282/1449788/Muutokset_aikuisten_ymparivuorokautisissa_artikkeli.pdf/a13a6b43-6c0b-4d86-964d-5a2c6f9e00a8 (accessed on 31 May 2018).
- Salvador-Carulla, L.; Costa-Font, J.; Cabases, J.; McDaid, D.; Alonso, J. Evaluating mental health care and policy in Spain. J. Ment. Health Policy Econ. 2010, 13, 73–86. [Google Scholar] [PubMed]
- Vázquez-Barquero, J.L.; García, J. Deinstitutionalization and psychiatric reform in Spain. Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Política Social e Igualdad Centro de Publicaciones. Ministerio de Sanidad Política e Igualdad Estrategia en Salud Mental del Sistema Nacional de Salud 2009–2013; Ministerio de Sanidad, Política Social e Igualdad Centro de Publicaciones: Madrid, Spain, 2011.
- Ministerio de Sanidad, Política Social e Igualdad Centro de Publicaciones. Ministerio de Sanidad y Consumo Estrategia en Salud Mental del Sistema Nacional de Salud; Ministerio de Sanidad, Política Social e Igualdad Centro de Publicaciones: Madrid, Spain, 2007.
- Dezetter, A.; Briffault, X.; Bruffaerts, R.; De Graaf, R.; Alonso, J.; König, H.H.; Haro, J.M.; De Girolamo, G.; Vilagut, G.; Kovess-Masféty, V. Use of general practitioners versus mental health professionals in six European countries: The decisive role of the organization of mental health-care systems. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Blanco, A.; Palao, D.J.; Luciano, J.V.; Pinto-Meza, A.; Lujan, L.; Fernandez, A.; Roura, P.; Bertsch, J.; Mercader, M.; Haro, J.M. Prevalence of mental disorders in primary care: Results from the diagnosis and treatment of mental disorders in primary care study (DASMAP). Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Wahlbeck, K. European comparisons between mental health services. Epidemiol. Psychiatr. Sci. 2011, 20, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Contel, J.C.; Ledesma, A.; Blay, C.; Mestre, A.G.; Cabezas, C.; Puigdollers, M.; Zara, C.; Amil, P.; Sarquella, E.; Constante, C. Chronic and integrated care in Catalonia. Int. J. Integr. Care 2015, 15, 1–13. [Google Scholar] [CrossRef]
- Generalitat de Catalunya. Departament de Salut Pla Director de Salut Mental i Adiccions de Catalunya; Direcció General de Planificació i Avaluació; Generalitat de Catalunya: Barcelona, Spain, 2006; ISBN 8439372647. [Google Scholar]
- Beecham, J.; Johnson, S. The European Socio-Demographic Schedule (ESDS): Rationale, principles and development. Acta Psychiatr. Scand. Suppl. 2000, 405, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Eurostat GDP per Capita in PPS. Available online: http://ec.europa.eu/eurostat/tgm/table.do?tab=table&init=1&language=en&pcode=tec00114&plugin=1 (accessed on 11 April 2018).
- World Health Organization European Health Information Gateway. Health for All Explorer. Available online: https://gateway.euro.who.int/en/hfa-explorer/ (accessed on 12 April 2018).
- Organisation for Economic Co-Operation and Development (OECD). Health Expenditure and Financing. Available online: http://stats.oecd.org/Index.aspx?DataSetCode=SHA# (accessed on 10 April 2018).
- The Finnish Statistics and Indicator Bank. Available online: https://www.sotkanet.fi/sotkanet/en/index (accessed on 16 December 2017).
- Idescat Official Statistic Website of Catalonia. Available online: https://www.idescat.cat/pub/?geo=at%3AAT02&id=regdis&n=443#Plegable=geo (accessed on 11 April 2018).
- Salvador-Carulla, L.; Alvarez-Galvez, J.; Romero, C.; Gutierrez-Colosia, M.R.; Weber, G.; McDaid, D.; Dimitrov, H.; Sprah, L.; Kalseth, B.; Tibaldi, G.; et al. Evaluation of an integrated system for classification, assessment and comparison of services for long-term care in Europe: The eDESDE-LTC study. BMC Health Serv. Res. 2013, 13, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.; Kuhlmann, R.; EPCAT Group. European Psychiatric Assessment Team. The European Service Mapping Schedule (ESMS): Development of an Instrument for the Description and Classification of Mental Health Services. Acta Psychiatr. Scand. Suppl. 2000, 405, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Romero, C.; Weber, G.; Dimitrov, H.; Sprah, L.; Venner, B.; McDaid, D. Classification, Assessment and Comparison of European LTC Services. Ageing Long-Term Care 2011, 17, 27. [Google Scholar]
- Tibaldi, G.; Munizza, C.; Pasian, S.; Johnson, S.; Salvador-Carulla, L.; Zucchi, S.; Cesano, S.; Testa, C.; Scala, E.; Pinciaroli, L. Indicators Predicting use of Mental Health Services in Piedmont, Italy. J. Ment. Health Policy Econ. 2005, 8, 95–106. [Google Scholar] [PubMed]
- Fernandez, A.; Salinas-Perez, J.A.; Gutierrez-Colosia, M.R.; Prat-Pubill, B.; Serrano-Blanco, A.; Molina, C.; Jorda, E.; Garcia-Alonso, C.R.; Salvador-Carulla, L. Use of an Integrated Atlas of Mental Health Care for Evidence Informed Policy in Catalonia (Spain). Epidemiol. Psychiatr. Sci. 2015, 24, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Tibaldi, G.; Johnson, S.; Scala, E.; Romero, C.; Munizza, C. Patterns of mental health service utilisation in Italy and Spain. An investigation using the European Service Mapping Schedule. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Rezvyy, G.; Øiesvold, T.; Parniakov, A.; Ponomarev, O.; Lazurko, O.; Olstad, R. The Barents Project in Psychiatry: A Systematic Comparative Mental Health Services Study between Northern Norway and Archangelsk County. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Saldivia, S.; Martinez-Leal, R.; Vicente, B.; Garcia-Alonso, C.; Grandon, P.; Haro, J.M. Meso-level comparison of mental health service availability and use in Chile and Spain. Psychiatr. Serv. 2008, 59, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Dahl, H.M.; Rezvyy, G.; Bogdanov, A.; Øiesvold, T. Outpatient Clinics Treating Substance use Disorders in Northwest Russia and Northern Norway: A Descriptive Comparative Study. Int. J. Circumpolar Health 2017, 76, 1411733. [Google Scholar] [CrossRef] [PubMed]
- Idescat Suicides. By Sex and Provinces. Available online: https://www.idescat.cat/pub/?id=aec&n=616&lang=en&t=2011 (accessed on 11 April 2018).
- Eurostat: Your Key to European Statistics. Available online: http://ec.europa.eu/eurostat/data/database (accessed on 12 April 2018).
- Raine, R.; Fitzpatrick, R.; Barratt, H.; Bevan, G.; Black, N.; Boaden, R.; Bower, P.; Campbell, M.; Denis, J.-L.; Devers, K.; et al. Challenges, Solutions and Future Directions in the Evaluation of Service Innovations in Health Care and Public Heath; University of Cambridge: Cambridge, UK, 2016; Volume 4. [Google Scholar]
- Chung, Y.; Salvador-Carulla, L.; Salinas-Pérez, J.A.; Uriarte-Uriarte, J.J.; Iruin-Sanz, A.; García-Alonso, C.R. Use of the Self-Organising Map Network (SOMNet) as a Decision Support System for Regional Mental Health Planning. Health Res. Policy Syst. 2018, 16, 35. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jonsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.-U.; Jacobi, F. Size and burden of mental disorders in Europe—A critical review and appraisal of 27 studies. Eur. Neuropsychopharmacol. 2005, 15, 357–376. [Google Scholar] [CrossRef] [PubMed]
- Fryers, T.; Melzer, D.; Jenkins, R. Social inequalities and the common mental disorders—A systematic review of the evidence. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Murali, V. Poverty, Social Inequality and mental health. Adv. Psychiatr. Treat. 2004, 10, 216–224. [Google Scholar] [CrossRef]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J.; Rodero-Cosano, M.L.; Motrico, E.; Salinas-Perez, J.A.; Garcia-Alonso, C.; Salvador-Carulla, L. The impact of socio-economic status on self-rated health: Study of 29 countries using European social surveys (2002–2008). Int. J. Environ. Res. Public Health 2013, 10, 747–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eikemo, T.A.; Bambra, C.; Joyce, K.; Dahl, E. Welfare state regimes and income-related health inequalities: A comparison of 23 European countries. Eur. J. Public Health 2008, 18, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J.; Rodero-Cosano, M.L.; García-Alonso, C.; Salvador-Carulla, L. Changes in socioeconomic determinants of health: Comparing the effect of social and economic indicators through European welfare state regimes. J. Public Health (Bangkok) 2014, 22, 305–311. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and Suicidal Behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Pirkola, S.P.; Isometsa, E.; Suvisaari, J.; Aro, H.; Joukamaa, M.; Poikolainen, K.; Koskinen, S.; Aromaa, A.; Lonnqvist, J.K. DSM-IV mood-, anxiety- and alcohol use disorders and their comorbidity in the Finnish general population--results from the Health 2000 Study. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Peen, J.; Dekker, J. Social deprivation and psychiatric service use for different diagnostic groups. Soc. Sci. Med. 2001, 53, 1–8. [Google Scholar] [CrossRef]
- Dekker, J.; Peen, J.; Goris, A.; Heijnen, H.; Kwakman, H. Social deprivation and psychiatric admission rates in Amsterdam. Soc. Psychiatry Psychiatr. Epidemiol. 1997, 32, 485–492. [Google Scholar] [PubMed]
- Thornicroft, G. Social deprivation and rates of treated mental disorder. Developing statistical models to predict psychiatric service utilization. Br. J. Psychiatry 1991, 158, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Ala-Nikkola, T.; Pirkola, S.; Kaila, M.; Saarni, S.I.; Joffe, G.; Kontio, R.; Oranta, O.; Sadeniemi, M.; Wahlbeck, K. Regional correlates of psychiatric inpatient treatment. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Billari, F. Becoming an Adult in Europe: A Macro(/Micro)-Demographic Perspective. Demogr. Res. 2004, S3, 15–44. [Google Scholar] [CrossRef]
- Buchmann, M.C.; Kriesi, I. Transition to Adulthood in Europe. Annu. Rev. Sociol. 2011, 37, 481–503. [Google Scholar] [CrossRef]
- Eurostat. Being Young in Europe Today; Publications Office of the European Union: Luxembourg, Luxembourg, 2015; ISBN 9789279432439. [Google Scholar]
- Giuliano, P. Living Arrangements in Western Europe: Does Cultural Origin Matter? J. Eur. Econ. Assoc. 2007, 5, 927–952. [Google Scholar] [CrossRef]
- Reher, D.S. Family Ties in Western Europe. Is Strong Family and Low Fertility: A Paradox? Dalla Zuana, G., Micheli, G., Eds.; Kluwer Academic Publishers: Norwell, MA, USA, 2004; pp. 45–76. [Google Scholar]
- Oliva-Moreno, J.; Pena-Longobardo, L.M.; Vilaplana-Prieto, C. An estimation of the value of informal care provided to dependent people in Spain. Appl. Health Econ. Health Policy 2015, 13, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Vilaplana, M.; Ochoa, S.; Martínez, A.; Villalta, V.; Martínez-Leal, R.; Puigdollers, E.; Salvador, L.; Martorell, A.; Muñoz, P.E.; Haro, J.M. Validación en población española de la entrevista de carga familiar objetiva y subjetiva (ECFOS-II) en familiares de pacientes con esquizofrenia. Actas Esp. Psiquiatr. 2007, 35, 372–381. [Google Scholar] [PubMed]
- Oliva-Moreno, J.; López-Bastida, J.; Montejo-González, A.L.; Osuna-Guerrero, R.; Duque-González, B. The socioeconomic costs of mental illness in Spain. Eur. J. Heal. Econ. 2009, 10, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Honkonen, T.; Saarinen, S.; Salokangas, R.K. Deinstitutionalization and schizophrenia in Finland II: Discharged patients and their psychosocial functioning. Schizophr. Bull. 1999, 25, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Salvador-Carulla, L.; Mcdaid, D.; Straßmayr, C.; Endel, F.; Näätänen, P.; Kalseth, J.; Kalseth, B.; Matosevic, T.; Donisi, V.; et al. The REFINEMENT Glossary of Terms: An International Terminology for Mental Health Systems Assessment. Adm. Policy Ment. Health Ment. Health Serv. Res. 2017, 1–10. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A. Development of the International Classification of Mental Health Care (ICMHC). Acta Psychiatr. Scand. 2000, 102, 8–13. [Google Scholar] [CrossRef]
- Castelpietra, G.; Salvador-Carulla, L.; Almborg, A.; Fernandez, A.; Madden, R. Working Draft: Classifications of Interventions in Mental Health Care. An Expert Review. Eur. J. Psychiatry 2017. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Socioeconomic Indicator | Helsinki and Uusimaa | Girona |
|---|---|---|
| GDP per capita in PPS Index (EU-28 = 100) 1 | 155 (Helsinki and Uusimaa) 117 (Finland) | 108 (Girona) 93 (Spain) |
| % GDP for health expenditure 2 | 9.0% (Finland) | 9.5% (Spain) |
| Public and private health expenditure per capita 2 | 3486 US$ PPP per capita (Finland) | 3019 US$ PPP per capita (Spain) |
| Mid-year population over 18 years of age 3 | 1,221,596 | 600,368 |
| Population mean age (years) 3 | 39.5 | 40.4 |
| Gender (% female) 3 | 51.6% | 49.6% |
| Population Density (inhabitants per km2) 3 | 177 | 124 |
| Unemployed (% of population 18–64 years) 3 | 7.0% | 22.18% |
| Dependency ratio 3 | 46 | 47 |
| Single households (% of all households) 3 | 41.4% | 17.9% |
| People on disability pension due to mental disorders (% of all disability pensioners) 3 | 49.2% | 30.9% |
| Single parent families (% of all families) 3 | 22.5% | 7.7% |
| Migrant population (% of all residents) 3 | 8.9% | 21.4% |
| Overall mortality (per 100,000 residents) 3 | 727 | 754 |
| Suicide mortality per 100,000 adults 4 | 16.3 | 10.0 |
| Population aged 25–64 with upper secondary or tertiary education completed 5 | 85.4% | 54.9% (macro-area) |
| Main Type of Care | DESDE- LTC Code | MTC Units/100,000 Adults (Absolute Numbers in Brackets) | Beds/Places/Users /100,000 Adults (Absolute Numbers in Brackets) | ||
|---|---|---|---|---|---|
| Helsinki and Uusimaa | Girona | Helsinki and Uusimaa | Girona | ||
| Residential care | |||||
| Hospital, acute care | R1–3 | 1.64 (20) | 0.17 (1) | 23.74 (290 beds) | 7.01 (42 beds) |
| Hospital, non-acute | R4, R6 | 3.27 (40) | 0.33 (2) | 51.82 (633 beds) | 15.35 (92 beds) |
| Non-hospital | R5, R7 | 0.33 (4) | 0 | 3.77 (46 beds) | 0 |
| Non-physician cover, 24 h support | R8, R11 | 3.36 (41) | 0.17 (1) | 100.28 (1225 ** beds) | 9.68 (58 beds) |
| Non-physician cover, non-24 h support | R9–10, R12–13, R14 | 2.29 (28) | 1.67 (10) | 46.74 (571 beds) | 12.01 (72 beds) |
| Total residential care | R | 10.89 (133) | 2.34 (14) | 226.34 (2765 beds) | 44.04 (264 beds) |
| Day care | |||||
| Acute day care | D1 | 0.65 (8) | 0.17 (1) | 9.50 (116 places) | 4.2 (25 places) |
| Work-related day care | D2–3, D6–7 | 1.56 (19) | 1.33 (8) | 13.02 (159 *) | 32.5 (195 ** places) |
| Health-related day care | D4.1, D8.1 | 1.15 (14) | 0.50 (3) | 19.40 (237 *) | 12.5 (75 places) |
| Structured and non-structured day care | D4.2–D4.4, D5 | 0.33 (4) | 0.83 (5) | 5.57 (68) | 27.5 (165 places) |
| Total day care | D | 3.44 (42) | 2.84 (17) | 47.48 (580 * places) | 76.73 (460 ** places) |
| Outpatient care | |||||
| Acute mobile care | O1–2 | 0.08 (1) | 0 | 11.73 (143 users a month) | 0 |
| Acute care | O3–4 | 1.06 (13) | 0.17 (1) | 75.67 (924 users a month) | 57.38 (344 users a month) |
| Non-acute, mobile care | O5–7 | 1.15 (14) | 0.17 (1) | 19.87 (243 users a month) | 2.50 (15 users a month) |
| Non-acute | O8–10 | 5.08 (62) | 1.17 (7) | 220.51 (2694 ** users a month) | 244.55 (1466 *** users a month) |
| Total outpatient care | O | 7.37 (90) | 1.50 (9) | 327.78 (4004 ** users a month) | 304.43 (1825 users a month) |
| MTCs total | 21.69 (265) | 6.67 (40) | 273.82 (3345 * beds + places) | 120.77 (724 ** beds + places) | |
| Helsinki and Uusimaa | Girona | |||
|---|---|---|---|---|
| FTE/100,000 Adults | FTE | FTE/100,000 Adults | FTE | |
| Profession | ||||
| Physicians | 23.4 | 286 | 9.4 | 56 |
| Nurses | 98.3 | 1201 | 6.5 | 39 |
| Psychologists | 13.0 | 159 | 2.9 | 17 |
| Other (social workers, occupational therapists, auxiliary nurses) | 106.0 | 1295 | 17.2 | 103 |
| Total | 240.8 | 2941 | 36.0 | 216 |
| Total FTEs per main type of care | ||||
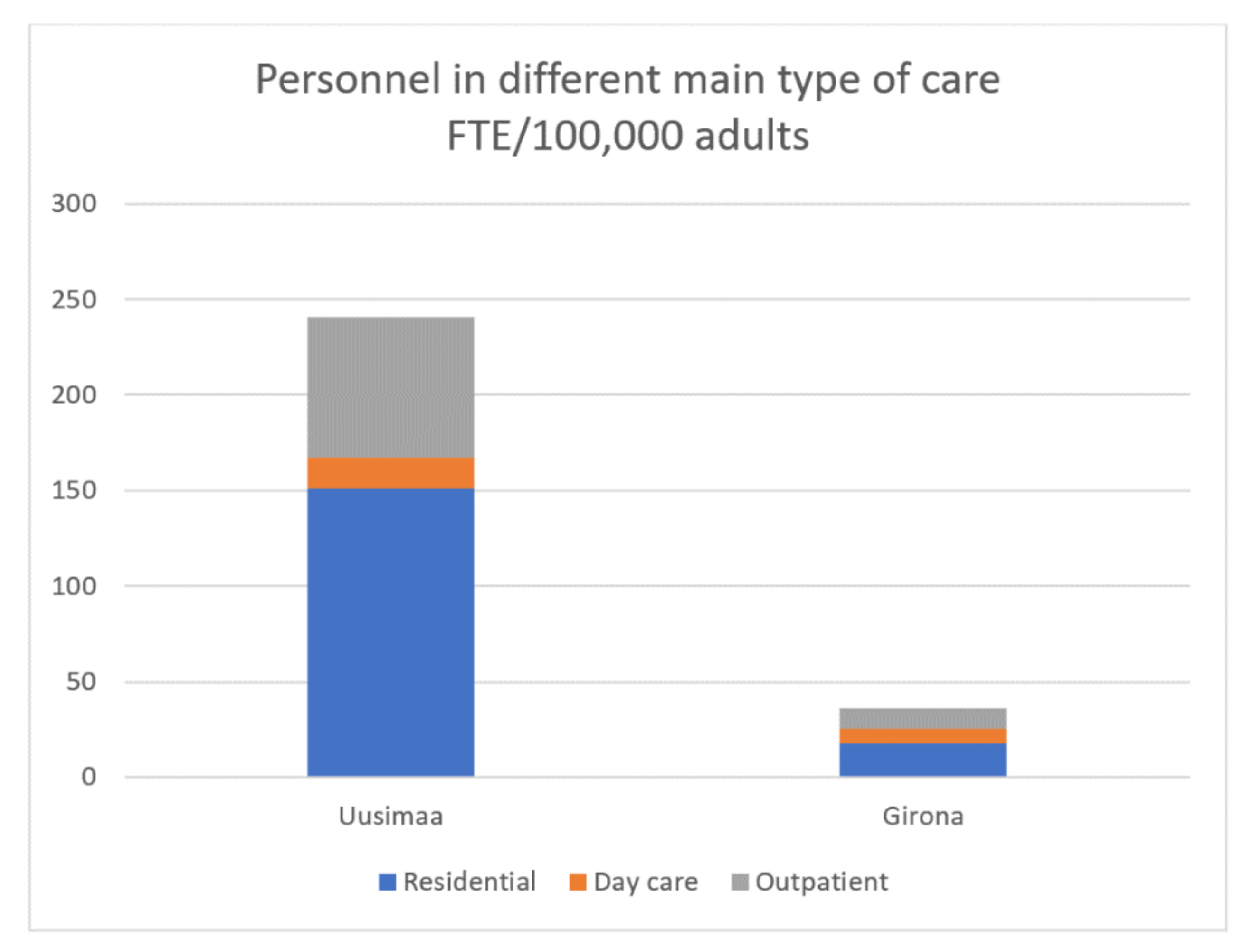
| Residential | 151.0 | 1845 | 17.7 | 106 |
| Day care | 15.9 | 194 | 7.8 | 47 |
| Outpatient | 73.8 | 902 | 10.5 | 63 |
| Total | 240.8 | 2941 | 36.0 | 216 |
| Productivity | Helsinki and Uusimaa | Girona |
|---|---|---|
| Outpatient visits in specialized psychiatric care per FTE (Absolute number in brackets) | 506.8 (409,573) | 1110.6 (69,967) |
| Psychiatric hospital inpatient days per FTE (Absolute number in brackets) | 231.3 (277,675) | 309.7 (28,490) |
| Number of FTE per occupied psychiatric hospital bed (Absolute number of occupied beds in brackets) | 1.58 (760.8) | 1.18 (78.1) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadeniemi, M.; Almeda, N.; Salinas-Pérez, J.A.; Gutiérrez-Colosía, M.R.; García-Alonso, C.; Ala-Nikkola, T.; Joffe, G.; Pirkola, S.; Wahlbeck, K.; Cid, J.; et al. A Comparison of Mental Health Care Systems in Northern and Southern Europe: A Service Mapping Study. Int. J. Environ. Res. Public Health 2018, 15, 1133. https://doi.org/10.3390/ijerph15061133
Sadeniemi M, Almeda N, Salinas-Pérez JA, Gutiérrez-Colosía MR, García-Alonso C, Ala-Nikkola T, Joffe G, Pirkola S, Wahlbeck K, Cid J, et al. A Comparison of Mental Health Care Systems in Northern and Southern Europe: A Service Mapping Study. International Journal of Environmental Research and Public Health. 2018; 15(6):1133. https://doi.org/10.3390/ijerph15061133
Chicago/Turabian StyleSadeniemi, Minna, Nerea Almeda, Jose A. Salinas-Pérez, Mencía R. Gutiérrez-Colosía, Carlos García-Alonso, Taina Ala-Nikkola, Grigori Joffe, Sami Pirkola, Kristian Wahlbeck, Jordi Cid, and et al. 2018. "A Comparison of Mental Health Care Systems in Northern and Southern Europe: A Service Mapping Study" International Journal of Environmental Research and Public Health 15, no. 6: 1133. https://doi.org/10.3390/ijerph15061133