Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Designs and Participants
2.2. Measurements
2.2.1. Physical Activity
2.2.2. Sleep Quality
2.2.3. Negative Emotions
2.2.4. Aggressiveness
2.2.5. COVID-19 Data
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Survey Participants
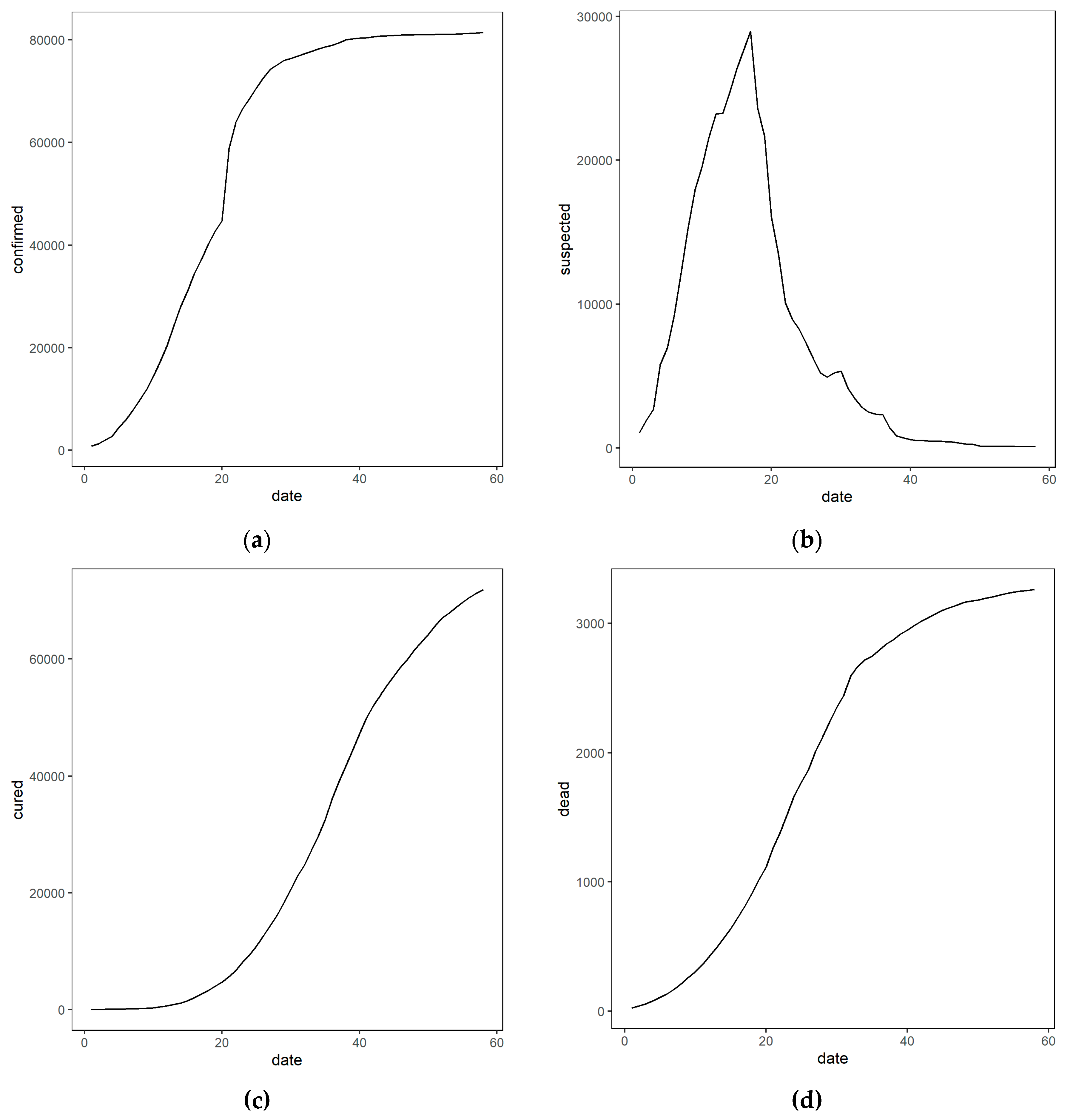
3.2. Epidemic Trends of the COVID-19 in China from January 23 to March 20, 2020
3.3. Relationships between Variables
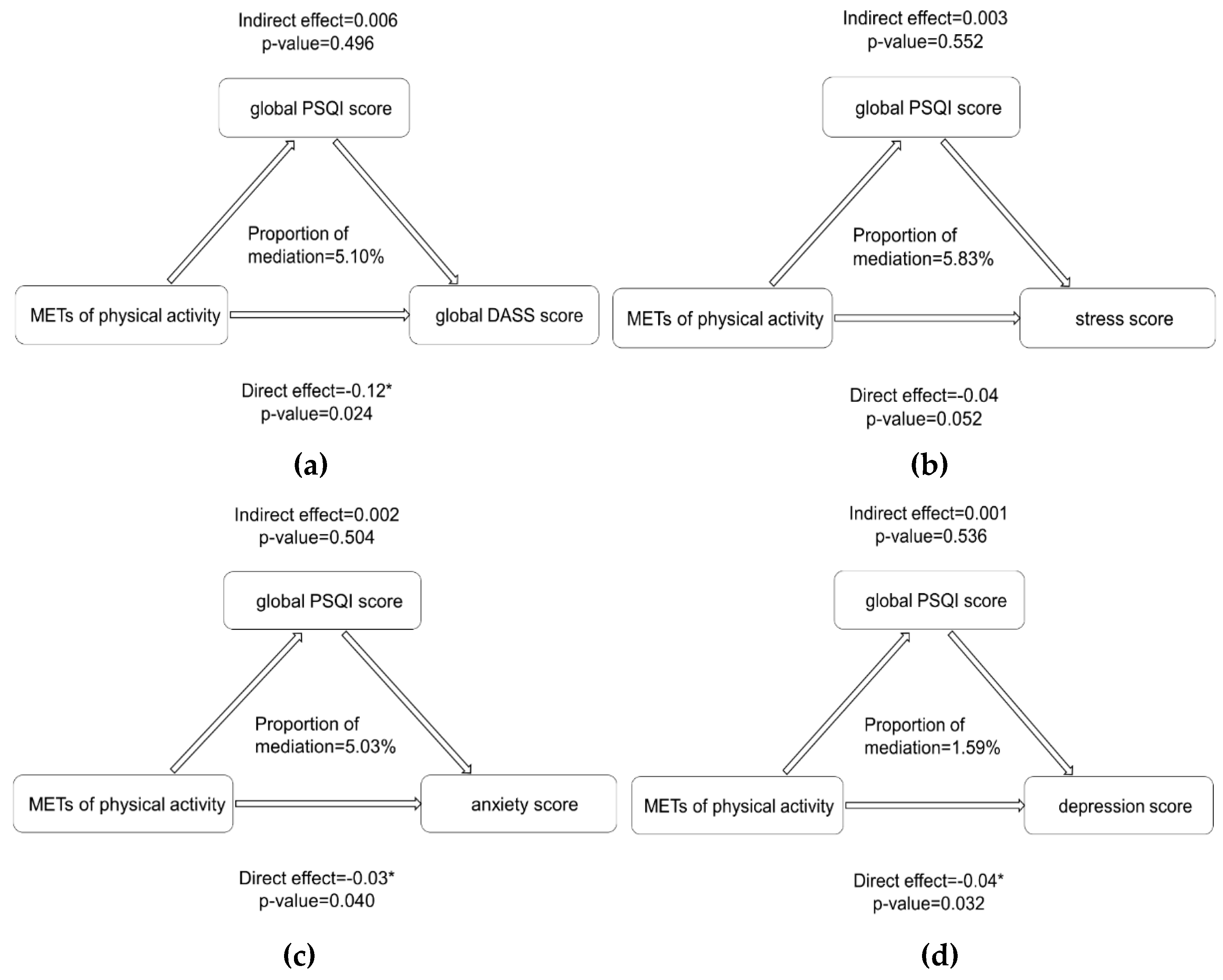
3.4. Underlying Influencing Mechanism
3.5. Dose-Response Relationships between Variables
4. Discussion
4.1. Prevalence of Negative Emotions during the Peak Time of the COVID-19 Outbreak
4.2. Adverse Impacts of COVID-19 and Underlying Mechanisms of Its Influence on Mental Health
4.3. The Fundamental Role of Exercise and Its Dose-Response Associations with Mental Health
4.4. Limitations
4.5. Strengths
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Approval Information
Participants’ Consent for Publication
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Shah, K.; Kamrai, D.; Mekala, H.; Mann, B.; Desai, K.; Patel, R.S. Focus on mental health during the coronavirus (COVID-19) pandemic: Applying learnings from the past outbreaks. Cureus 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Ahern, J.; Resnick, H.; Kilpatrick, D.; Bucuvalas, M.; Gold, J.; Vlahov, D. Psychological sequelae of the September 11 terrorist attacks in New York City. N. Engl. J. Med. 2002, 346, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, L.; Armour, C.; Cao, C.; Qing, Y.; Zhang, J.; Liu, P.; Zhang, B.; Wu, Q.; Zhao, Z.; et al. Assessing the underlying dimensionality of DSM-5 PTSD symptoms in Chinese adolescents surviving the 2008 Wenchuan earthquake. J. Anxiety Disord. 2015, 31, 90–97. [Google Scholar] [CrossRef]
- Tracy, M.; Norris, F.H.; Galea, S. Differences in the determinants of posttraumatic stress disorder and depression after a mass traumatic event. Depress. Anxiety 2011, 28, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.M.; Kang, W.S.; Cho, A.-R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Batawi, S.; Tarazan, N.; Al-Raddadi, R.; Al Qasim, E.; Sindi, A.; AL Johni, S.; Al-Hameed, F.M.; Arabi, Y.M.; Uyeki, T.M.; Alraddadi, B.M. Quality of life reported by survivors after hospitalization for Middle East respiratory syndrome (MERS). Health Qual. Life Outcomes 2019, 17, 101. [Google Scholar] [CrossRef] [Green Version]
- Cheung, Y.T.; Chau, P.H.; Yip, P.S.F. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int. J. Geriatr. Psychiatry 2008, 23, 1231–1238. [Google Scholar] [CrossRef]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 112934. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.-B.; Wang, X.-H.; Wang, H.-N. Challenges facing coronavirus disease 2019: Psychiatric services for patients with mental disorders: Psychiatric services facing COVID-19. Psychiatry Clin. Neurosci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Garfield, V.; Llewellyn, C.H.; Kumari, M. The relationship between physical activity, sleep duration and depressive symptoms in older adults: The English Longitudinal Study of Ageing (ELSA). Prev. Med. Rep. 2016, 4, 512–516. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Zhang, Q.; Du, Y.; Ye, Y.; He, Q. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese college freshmen. PLoS ONE 2014, 9, e100914. [Google Scholar] [CrossRef] [Green Version]
- Ji, X.W.; Chan, C.H.Y.; Lau, B.H.P.; Chan, J.S.M.; Chan, C.L.W.; Chung, K.-F. The interrelationship between sleep and depression: A secondary analysis of a randomized controlled trial on mind-body-spirit intervention. Sleep Med. 2017, 29, 41–46. [Google Scholar] [CrossRef]
- Karlsen, T.; Nes, B.M.; Tjønna, A.E.; Engstrøm, M.; Støylen, A.; Steinshamn, S. High-intensity interval training improves obstructive sleep apnoea. BMJ Open Sport Exerc. Med. 2017, 2, 8. [Google Scholar] [CrossRef]
- Lee, M.-S.; Kim, S.-R.; Min, G.-H.; Cho, B.-J. Effects of sittercise on elderly subjects’ depression and sleep quality. J. Phys. Ther. Sci. 2016, 28, 1120–1123. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, D.J.; Lee, C.C.Y.; Ho, E.Y.K.; Chan, K.L.; Chan, D.T.S. Reliability and validity of the Chinese version of IPAQ (short, last 7 days). J. Sci. Med. Sport 2007, 10, 45–51. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of Physical Activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Tsai, P.-S.; Wang, S.-Y.; Wang, M.-Y.; Su, C.-T.; Yang, T.-T.; Huang, C.-J.; Fang, S.-C. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep quality in the general population: Psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Zanon, C.; Brenner, R.E.; Baptista, M.N.; Vogel, D.L.; Rubin, M.; Al-Darmaki, F.R.; Gonçalves, M.; Heath, P.J.; Liao, H.-Y.; Mackenzie, C.S.; et al. Examining the dimensionality, reliability, and invariance of the Depression, Anxiety, and Stress Scale–21 (DASS-21) across eight countries. Assessment 2020, 107, 1–14. [Google Scholar] [CrossRef]
- Quek, T.; Ho, C.; Choo, C.; Nguyen, L.; Tran, B.; Ho, R. Misophonia in Singaporean psychiatric patients: A cross-sectional study. Int. J. Environ. Res. Public. Health 2018, 15, 1410. [Google Scholar] [CrossRef] [Green Version]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.; Sham, P.C.; Chua, S.E.; Wong, J.G. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Le, T.A.; Le, M.Q.T.; Dang, A.D.; Dang, A.K.; Nguyen, C.T.; Pham, H.Q.; Vu, G.T.; Hoang, C.L.; Tran, T.T.; Vuong, Q.-H.; et al. Multi-level predictors of psychological problems among methadone maintenance treatment patients in difference types of settings in Vietnam. Subst. Abuse Treat. Prev. Policy 2019, 14, 39. [Google Scholar] [CrossRef] [PubMed]
- Buss, A.H.; Perry, M. The Aggression Questionnaire. J. Pers. Soci. Psychol. 1992, 63, 452–459. [Google Scholar] [CrossRef]
- Sukhodolsky, D.G.; Golub, A.; Cromwell, E.N. Development and validation of the Anger Rumination Scale. Personal. Individ. Differ. 2001, 31, 689–700. [Google Scholar] [CrossRef]
- Maxwell, J.P. Development and preliminary validation of a Chinese version of the Buss–Perry Aggression Questionnaire in a population of Hong Kong Chinese. J. Pers. Assess. 2007, 88, 284–294. [Google Scholar] [CrossRef]
- Maxwell, J.P. Psychometric properties of a Chinese version of the Buss–Warren Aggression Questionnaire. Personal. Individ. Differ. 2008, 44, 943–953. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 112921. [Google Scholar] [CrossRef]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef]
- Kmietowicz, Z. Rules on isolation rooms for suspected COVID-19 cases in GP surgeries to be relaxed. BMJ 2020, m707. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Stamatakis, E.; Steptoe, A. Dose-response relationship between physical activity and mental health: The Scottish Health Survey. Br. J. Sports Med. 2009, 43, 1111–1114. [Google Scholar] [CrossRef]
- Loprinzi, P.D. Objectively measured light and moderate-to-vigorous physical activity is associated with lower depression levels among older US adults. Aging Ment. Health 2013, 17, 801–805. [Google Scholar] [CrossRef]
- Campbell, J.P.; Turner, J.E. Debunking the myth of exercise-induced immune suppression: Redefining the impact of exercise on immunological health across the lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef]
- Andrade, A.; Dominski, F.H.; Pereira, M.L.; de Liz, C.M.; Buonanno, G. Infection risk in gyms during physical exercise. Environ. Sci. Pollut. Res. 2018, 25, 19675–19686. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K.; American College of Sports Medicine American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Male | Female | p-Value | |
|---|---|---|---|---|
| N | 66 | 25 | 41 | |
| Age (Year), Mean (SD) | 20.70 (2.11) | 21.08 (1.94) | 20.46 (2.19) | 0.251 |
| Ethnicity, n (%) | ||||
| Han | 61 (92.42%) | 24 (96.00%) | 37 (90.24%) | 0.367 |
| Minority | 5 (7.58%) | 1 (4.00%) | 4 (9.76%) | |
| Body Mass Index, Mean (SD) | ||||
| BMI (kg/m2) | 21.11 (2.92) | 22.54 (2.56) | 20.24 (2.80) | 0.001 |
| Residence, n (%) | ||||
| City | 51 (77.27%) | 18 (72.00%) | 33 (80.49%) | 0.307 |
| Countryside | 15 (22.73%) | 7 (28.00%) | 8 (19.51%) | |
| METs of Weekly PA, Mean (SD) | ||||
| Vigorous PA | 354.55 (613.41) | 715.20 (785.62) | 134.63 (367.78) | <0.001 |
| Moderate PA | 250.30 (374.19) | 252.00 (301.66) | 249.27 (415.84) | 0.977 |
| Light PA | 327.50 (312.91) | 462.00 (370.67) | 245.49 (241.80) | 0.005 |
| Total PA | 932.35 (881.69) | 1429.200 (835.56) | 629.390 (772.00) | <0.001 |
| Sedentary Behavior, Mean (SD) | ||||
| Total minutes of weekly sedentariness | 2881.06 (1086.27) | 2830.40 (1351.02) | 2911.95 (905.38) | 0.770 |
| Physical Activity Level, n (%) | ||||
| Sedentary | 10 (15.15%) | 2 (8.00%) | 8 (19.51%) | 0.002 |
| Low | 19 (28.79%) | 2 (8.00%) | 17 (41.46%) | |
| Moderate | 29 (43.94%) | 15 (60.00%) | 14 (34.15%) | |
| High | 8 (12.12%) | 6 (24.00%) | 2 (4.88%) | |
| PSQI Level, n (%) | ||||
| Healthy (global PSQI ≤ 5) | 38 (57.58%) | 14 (56.00%) | 24 (58.54%) | 0.520 |
| Unhealthy (global PSQI > 5) | 28 (42.42%) | 11 (44.00%) | 17 (41.46%) | |
| Attitudes Towards COVID-19, n (%) | ||||
| Worried or very concerned | 56 (84.85%) | 21 (84.00%) | 35 (85.40%) | 0.572 |
| Not very worried or no care | 10 (15.15%) | 4 (16.00%) | 6 (14.60) | |
| Stress Level, n (%) | ||||
| normal | 47 (71.21%) | 20 (80.00%) | 27 (65.85%) | 0.171 |
| abnormal | 19 (28.79%) | 5 (20.00%) | 14 (34.15%) | |
| Anxiety Level, n (%) | ||||
| normal | 36 (54.55%) | 17 (68.00%) | 19 (46.34%) | 0.072 |
| abnormal | 30 (45.45%) | 8 (32.00%) | 22 (53.66%) | |
| Depression Level, n (%) | ||||
| normal | 51 (77.27%) | 21 (84.00%) | 30 (73.17%) | 0.240 |
| abnormal | 15 (22.73%) | 4 (16.00%) | 11 (26.83%) |
| Every 1000 Increase in COVID-19 Death Cases | Every 100-MET Increase in Physical Activity | |||
|---|---|---|---|---|
| Point Estimate | 95% CI | Point Estimate | 95% CI | |
| Sleep quality score | 0.15 | (−0.11, 0.41) | 0.0015 | (−0.0074, 0.010) |
| Sleep onset latency score | −0.07 | (−0.24, 0.09) | 0.0011 | (−0.0058, 0.0081) |
| Sleep duration score | 0.07 | (−0.13, 0.26) | 0.0026 | (−0.0046, 0.0098) |
| Sleep efficiency score | 0.29 * | (0.15, 0.44) | 0.0001 | (−0.0064, 0.0066) |
| Sleep disturbance score | 0.16 | (−0.08, 0.40) | 0.0026 | (−0.0075, 0.013) |
| Sleep medicine use score | −0.0002 | (−0.02, 0.02) | −0.0001 | (−0.0010, 0.00080) |
| Daytime dysfunction | 0.12 | (−0.04, 0.29) | 0.0054 | (−0.0015, 0.012) |
| Global PSQI score | 1.37 * | (0.55, 2.19) | 0.0110 | (−0.022, 0.044) |
| Stress score | −0.66 | (−2.09, 0.77) | −0.0389 | (−0.085, 0.0068) |
| Anxiety score | 0.18 | (−0.95, 1.31) | −0.03 | (−0.067, 0.0026) |
| Depression score | −0.03 | (−1.33, 1.26) | −0.04 * | (−0.080, −0.0022) |
| Global DASS score | −0.01 | (−3.54, 3.52) | −0.12 * | (−0.22, −0.010) |
| Aggressiveness score | −6.57 * | (−12.78, −0.36) | −0.03 | (−0.17, 0.12) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. https://doi.org/10.3390/ijerph17103722
Zhang Y, Zhang H, Ma X, Di Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. International Journal of Environmental Research and Public Health. 2020; 17(10):3722. https://doi.org/10.3390/ijerph17103722
Chicago/Turabian StyleZhang, Yao, Haoyu Zhang, Xindong Ma, and Qian Di. 2020. "Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China" International Journal of Environmental Research and Public Health 17, no. 10: 3722. https://doi.org/10.3390/ijerph17103722