Manipulation of Lateral Pharyngeal Wall Muscles in Sleep Surgery: A Review of the Literature

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
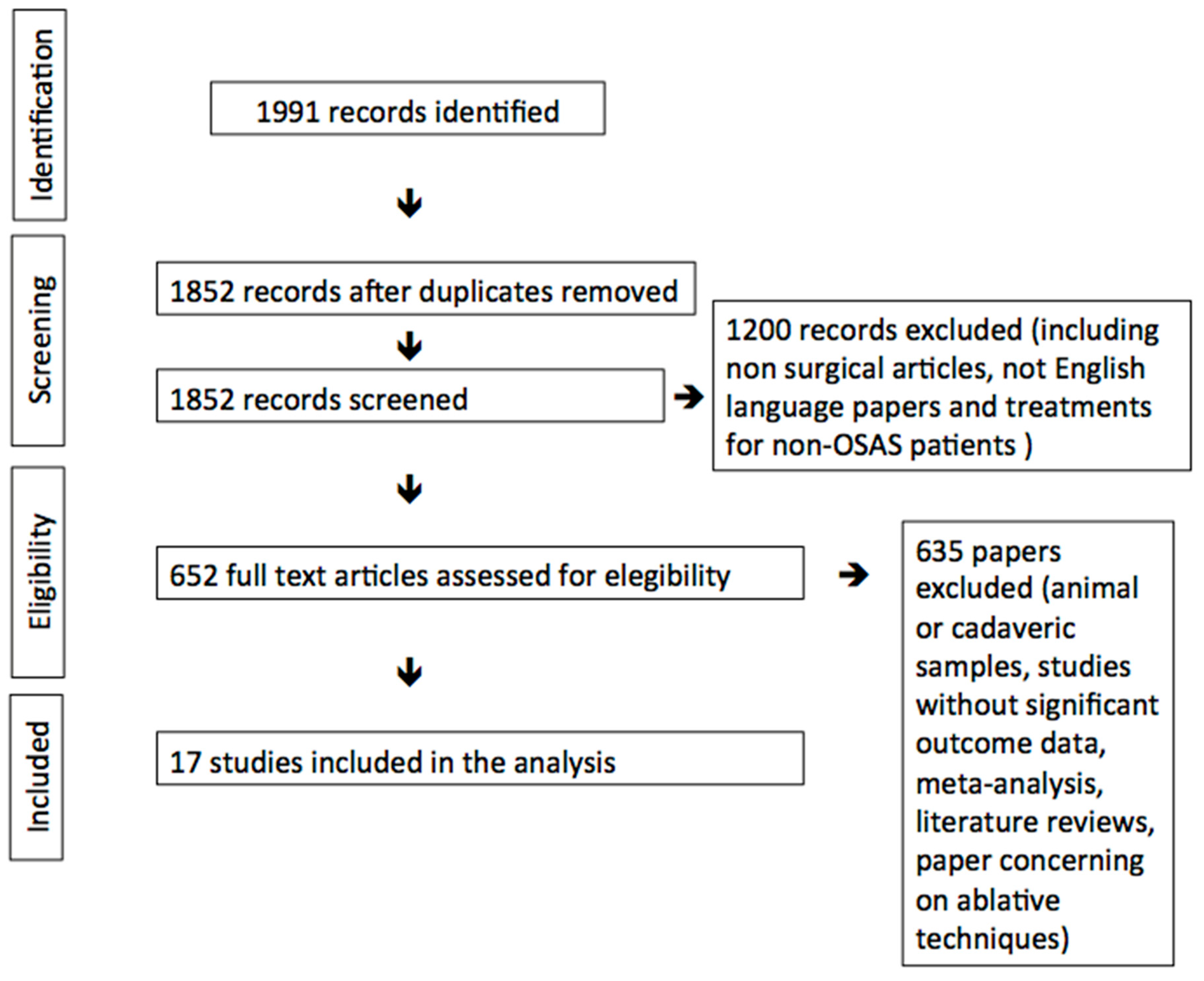
2. Materials and Methods
3. Results
4. Discussion
4.1. Superior Pharyngeal Constrictor
4.2. Palatopharyngeal Muscle
4.2.1. Total/Subtotal Section of Muscular Fibers
4.2.2. Partial Section of Muscular Fibers
4.2.3. Minimal Handling of Muscular Fibers
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Remmers, J.E.; DeGroot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.J.; Gefter, W.B.; A Hoffman, E.; Gupta, K.B.; Pack, A.I. Dynamic upper airway imaging during awake respiration in normal subjects and patients with sleep disordered breathing. Am. Rev. Respir. Dis. 1993, 148, 1385–1400. [Google Scholar] [CrossRef] [PubMed]
- Isono, S.; Remmers, J.E.; Tanaka, A.; Sho, Y.; Nishino, T. Static properties of the passive pharynx in sleep Apnea. Sleep 1996, 19, 175–177. [Google Scholar]
- Morrison, D.L.; Launois, S.H.; Isono, S.; Feroah, T.R.; Whitelaw, W.A.; Remmers, J.E. Pharyngeal narrowing and closing pressures in patients with obstructive sleep apnea. Am. Rev. Respir. Dis. 1993, 148, 606–611. [Google Scholar] [CrossRef]
- Flores-Orozco, E.I.; Tiznado-Orozco, G.E.; Díaz-Peña, R.; Orozco, E.I.F.; Galletti, C.; Gazia, F.; Galletti, F. Effect of a mandibular advancement device on the upper airway in a patient with obstructive sleep apnea. J. Craniofac. Surg. 2020, 31, e32–e35. [Google Scholar] [CrossRef]
- Fujita, S.; Cinway, W.; Zorik, F.; Roth, T. Surgical correction of ana-tomic abnormalities in obstructive sleep apnea syndrome: Uvulopalatopharyngoplasty. Otolaryngol. Head Neck Surg. 1981, 89, 923–934. [Google Scholar] [CrossRef]
- Cahali, M.B. Lateral pharyngoplasty: A new treatment for OSAHS. Laryngoscope 2003, 113, 1961. [Google Scholar] [CrossRef]
- Pang, K.P.; Plaza, G.; Baptista J, P.M.; Reina, C.O.; Chan, Y.H.; Pang, K.A.; Pang, E.B.; Wang, C.M.Z.; Rotenberg, B. Palate surgery for obstructive sleep apnea: A 17-year meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1697–1707. [Google Scholar] [CrossRef]
- Urrutia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemàticas y metaanálisis. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Pinto, J.A.; De Godoy, L.B.M.; Nunes, H.D.S.S.; Abdo, K.E.; Jahic, G.S.; Cavallini, A.F.; Freitas, G.S.; Ribeiro, D.K.; Duarte, C. Lateral-expansion pharyngoplasty: Combined technique for the treatment of obstructive sleep apnea syndrome. Int. Arch. Otorhinolaryngol. 2020, 24, e107–e111. [Google Scholar] [CrossRef] [Green Version]
- Li, H.-Y.; Lee, L.-A. Relocation pharyngoplasty for obstructive sleep apnea. Laryngoscope 2009, 119, 2472–2477. [Google Scholar] [CrossRef] [PubMed]
- Emara, T.A.; Hassan, M.H.; Mohamad, A.S.; Anany, A.M.; Ebrahem, A.E. Anterolateral advancement pharyngoplasty: A new technique for treatment of obstructive sleep apnea. Otolaryngol. Head Neck Surg. 2016, 155, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.P.; Woodson, B.T. Expansion Sphincter Pharyngoplasty: A new technique for the treatment of obstructive sleep apnea. Otolaryngol. Head Neck Surg. 2007, 137, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Sorrenti, G.; Piccin, O. Functional expansion pharyngoplasty in the treatment of obstructive sleep apnea. Laryngoscope 2013, 123, 2905–2908. [Google Scholar] [CrossRef]
- Elbassiouny, A.M.M.E. Soft palatal webbing flap palatopharyngoplasty for both soft palatal and oropharyngeal lateral wall collapse in the treatment of snoring and obstructive sleep apnea: A new innovative technique without tonsillectomy. Sleep Breath. 2014, 19, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Elbassiouny, A.M.M.E. Modified barbed soft palatal posterior pillar webbing flap palatopharyngoplasty. Sleep Breath. 2016, 20, 829–836. [Google Scholar] [CrossRef]
- Ulualp, S.O. Modified expansion sphincter pharyngoplasty for treatment of children with obstructive sleep apnea. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 817–822. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Kim, B.; Lee, D.; Choi, J.; Hwang, S.; Park, C.; Kim, S.; Cho, J.; Park, Y. A modified uvulopalatal flap with lateral pharyngoplasty for treatment in 92 adults with obstructive sleep apnoea syndrome. Clin. Otolaryngol. 2013, 38, 415–419. [Google Scholar] [CrossRef]
- Vicini, C.; Hendawy, E.; Campanini, A.; Eesa, M.; Bahgat, A.; Alghamdi, S.; Meccariello, G.; DeVito, A.; Montevecchi, F.; Mantovani, M. Barbed reposition pharyngoplasty (BRP) for OSAHS: A feasibility, safety, efficacy and teachability pilot study. “We are on the giant’s shoulders”. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 3065–3070. [Google Scholar] [CrossRef]
- Babademez, M.A.; Gul, F.; Kale, H.; Sancak, M. Technical update of barbed pharyngoplasty for retropalatal obstruction in obstructive sleep apnoea. J. Laryngol. Otol. 2019, 133, 622–626. [Google Scholar] [CrossRef]
- Mantovani, M.; Rinaldi, V.; Torretta, S.; Carioli, D.; Salamanca, F.; Pignataro, L. Barbed Roman blinds technique for the treatment of obstructive sleep apnea: How we do it? Eur. Arch. Oto-Rhino-Laryngol. 2015, 273, 517–523. [Google Scholar] [CrossRef] [PubMed]
- El-Ahl, M.A.S.; El-Anwar, M.W. Expansion pharyngoplasty by new simple suspension sutures without tonsillectomy. Otolaryngol. Head Neck Surg. 2016, 155, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-Y.; Lee, L.-A.; Kezirian, E.J.; Nakayama, M. Suspension palatoplasty for obstructive sleep apnea–a preliminary study. Sci. Rep. 2018, 8, 4224. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, M.; Missale, F.; Incandela, F.; Fragale, M.; Barbieri, A.; Roustan, V.; Canevari, F.R.; Peretti, G. Barbed suspension pharyngoplasty for treatment of lateral pharyngeal wall and palatal collapse in patients affected by OSAHS. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 1829–1835. [Google Scholar] [CrossRef]
- Sorrenti, G.; Pelligra, I.; Albertini, R.; Caccamo, G.; Piccin, O. Functional expansion pharyngoplasty: Technical update by unidirectional barbed sutures. Clin. Otolaryngol. 2018, 43, 1419–1421. [Google Scholar] [CrossRef]
- Montevecchi, F.; Meccariello, G.; Firinu, E.; Arigliani, M.; De Benedetto, M.; Palumbo, A.; Bahgat, Y.; Bahgat, A.; Saldana, R.L.; Marzetti, A.; et al. Prospective multicentre study on barbed reposition pharyngoplasty standing alone or as a part of multilevel surgery for sleep apnoea. Clin. Otolaryngol. 2018, 43, 483–488. [Google Scholar] [CrossRef]
- Vicini, C.; Meccariello, G.; Montevecchi, F.; De Vito, A.; Frassineti, S.; Gobbi, R.; Pelucchi, S.; Iannella, G.; Magliulo, G.; Cammaroto, G. Effectiveness of barbed repositioning pharyngoplasty for the treatment of obstructive sleep apnea (OSA): A prospective randomized trial. Sleep Breath. 2020, 24, 687–694. [Google Scholar] [CrossRef]
- Mantovani, M.; Minetti, A.; Torretta, S.; Pincherle, A.; Tassone, G.; Pignataro, L. The velo-uvulo-pharyngeal lift or “roman blinds” technique for treatment of snoring: A preliminary report. ACTA Otorhinolaryngol. Ital. 2012, 32, 48–53. [Google Scholar]
- Osman, A.M.; Tong, B.K.; Landry, S.A.; Edwards, B.A.; Joosten, S.A.; Hamilton, G.S.; Cori, J.M.; Jordan, A.S.; Stevens, D.; Grunstein, R.R.; et al. An assessment of a simple clinical technique to estimate pharyngeal collapsibility in people with obstructive sleep apnea. Sleep 2020. [Google Scholar] [CrossRef]
- De Vito, A.; Agnoletti, V.; Zani, G.; Corso, R.M.; D’Agostino, G.; Firinu, E.; Marchi, C.; Hsu, Y.-S.; Maitan, S.; Vicini, C. The importance of drug-induced sedation endoscopy (D.I.S.E.) techniques in surgical decision making: Conventional versus target controlled infusion techniques—A prospective randomized controlled study and a retrospective surgical outcomes analysis. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 2307–2317. [Google Scholar] [CrossRef]


{kind=link}
| Title | Structural Target and Modification of LPW | Number of Patients | Mean AHI Pre-Op | Mean AHI Post-Op | ∆ AHI. | Follow-Up Time (Months) | Complications Described and Relating Incidence |
|---|---|---|---|---|---|---|---|
| Lateral Pharyngoplasty: A New Treatment for Obstructive Sleep Hypopnea Syndrome [7] | SPC | 10 | 45.8 | 15.2 | 30.6 | 8.2 | Oronasal reflux (10%), taste loss (10%). |
| Lateral-Expansion Pharyngoplasty: Combined Technique for the Treatment of Obstructive Sleep Apnea Syndrome [10] | SPC | 38 | 22.4 | 13.6 | 8.8 | 7 | - |
| Relocation Pharyngoplasty for Obstructive Sleep Apnea [11] | SPC | 10 | 43.4 | 15.7 | 27.7 | 6 | - |
| Anterolateral Advancement Pharyngoplasty: A New Technique for Treatment of Obstructive Sleep Apnea [12] | SPC | 38 | 42.1 | 16.3 | 25.8 | 6 | - |
| Expansion Sphincter Pharyngoplasty: A New Technique for the Treatment of Obstructive Sleep Apnea [13] | PPM section | 45 | 44.2 | 12.0 | 32.2 | 6.5 | - |
| Functional Expansion Pharyngoplasty in the Treatment of Obstructive Sleep Apnea [14] | PPM section | 85 | 33.3 | 11.7 | 21.6 | 6 | Postsurgical bleeding (2.3%). |
| Soft Palatal Webbing Flap Palatopharyngoplasty for Both Soft Palatal and Obstructive Sleep Apnea: A New Innovative Technique without Tonsillectomy [15] | PPM section | 28 | 46.1 | 11 | 35.1 | 6 | Excessive postnasal discharge (10.7%) temporary velopharyngeal insufficiency (7.1%), sensation of oral dryness (25%). |
| Modified Barbed Soft Palatal Posterior Pillar Webbing Flap Palatopharyngoplasty [16] | PPM section | 21 | 47.7 | 12.3 | 35.4 | 6 | Temporary velopharyngeal insufficiency (5%), excessive postnasal discharge (19%). |
| Modified Expansion Sphincter pharyngoplasty for Treatment of Children with Obstructive Sleep Apnea [17] | PPM partial section | 25 | 60.5 | 2.0 | 58.5 | - | Postoperative bleeding (4%). |
| A Modified Uvulopalatal Flap with Lateral Pharyngoplasty for Treatment in 92 Adults with Obstructive Sleep Apnoea Syndrome [18] | PPM partial section | 92 | 39.1 | 7.9 | 21,2 | 6 | Nasal regurgitation, bleeding, dysphagia, Foreign body sensation. |
| Barbed Reposition Pharyngoplasty (BRP) for OSAHS: A Feasibility, Safety, Efficacy and Teachability Pilot Study. “We are on the giant’s shoulders” [19] | PPM partial section | 10 | 43.65 | 13.57 | 30.08 | 6 | Foreign body sensation, partial thread extrusion (20%). |
| Technical Update of Barbed Pharyngoplasty for Retropalatal Obstruction in Obstructive Sleep Apnoea [20] | PPM partial section | 17 | 29.9 | 5.4 | 24.5 | 6 | Foreign body sensation. |
| Barbed Roman Blinds Technique for Treatment of Obstructive Sleep Apnea: How We Do It? [21] | PPM minimal handling | 32 | 36.9 | 13.7 | 23.2 | 12 | - |
| Expansion Pharyngoplasty by New Simple Suspension Sutures without Tonsillectomy [22] | PPM minimal handling | 24 | 28.6 | 8.9 | 19.7 | 9 | - |
| Suspension Palatoplasty for Obstructive Sleep Apnea- Preliminary Study [23] | PPM minimal handling | 25 | 39.8 | 15.1 | 24.7 | 6 | Globus sensation of the throat. |
| Barbed Suspension Pharyngoplasty for Treatment of Lateral Pharyngeal Wall and Palatal Collapse in Patients Affected by OSAHS [24] | PPM minimal handling | 20 | 25 | 5 | 20 | 6 | Transient velopharyngeal insufficiency (10%), Partial thread extrusion (25%). |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cammaroto, G.; Stringa, L.M.; Iannella, G.; Meccariello, G.; Zhang, H.; Bahgat, A.Y.; Calvo-Henriquez, C.; Chiesa-Estomba, C.; Lechien, J.R.; Barillari, M.R.; et al. Manipulation of Lateral Pharyngeal Wall Muscles in Sleep Surgery: A Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 5315. https://doi.org/10.3390/ijerph17155315
Cammaroto G, Stringa LM, Iannella G, Meccariello G, Zhang H, Bahgat AY, Calvo-Henriquez C, Chiesa-Estomba C, Lechien JR, Barillari MR, et al. Manipulation of Lateral Pharyngeal Wall Muscles in Sleep Surgery: A Review of the Literature. International Journal of Environmental Research and Public Health. 2020; 17(15):5315. https://doi.org/10.3390/ijerph17155315
Chicago/Turabian StyleCammaroto, Giovanni, Luigi Marco Stringa, Giannicola Iannella, Giuseppe Meccariello, Henry Zhang, Ahmed Yassin Bahgat, Christian Calvo-Henriquez, Carlos Chiesa-Estomba, Jerome R. Lechien, Maria Rosaria Barillari, and et al. 2020. "Manipulation of Lateral Pharyngeal Wall Muscles in Sleep Surgery: A Review of the Literature" International Journal of Environmental Research and Public Health 17, no. 15: 5315. https://doi.org/10.3390/ijerph17155315