Subjective Oral Health-Related Quality of Life and Objective Oral Health in People with Ectodermal Dysplasia

 and
and
Abstract
:1. Introduction
2. Methods
2.1. Inclusion Criteria
2.2. Participants
2.3. Assessment of Physical Oral Health
2.4. Assessment of OHRQoL (OHIP)
2.5. Statistical Methods
3. Results
3.1. Participants
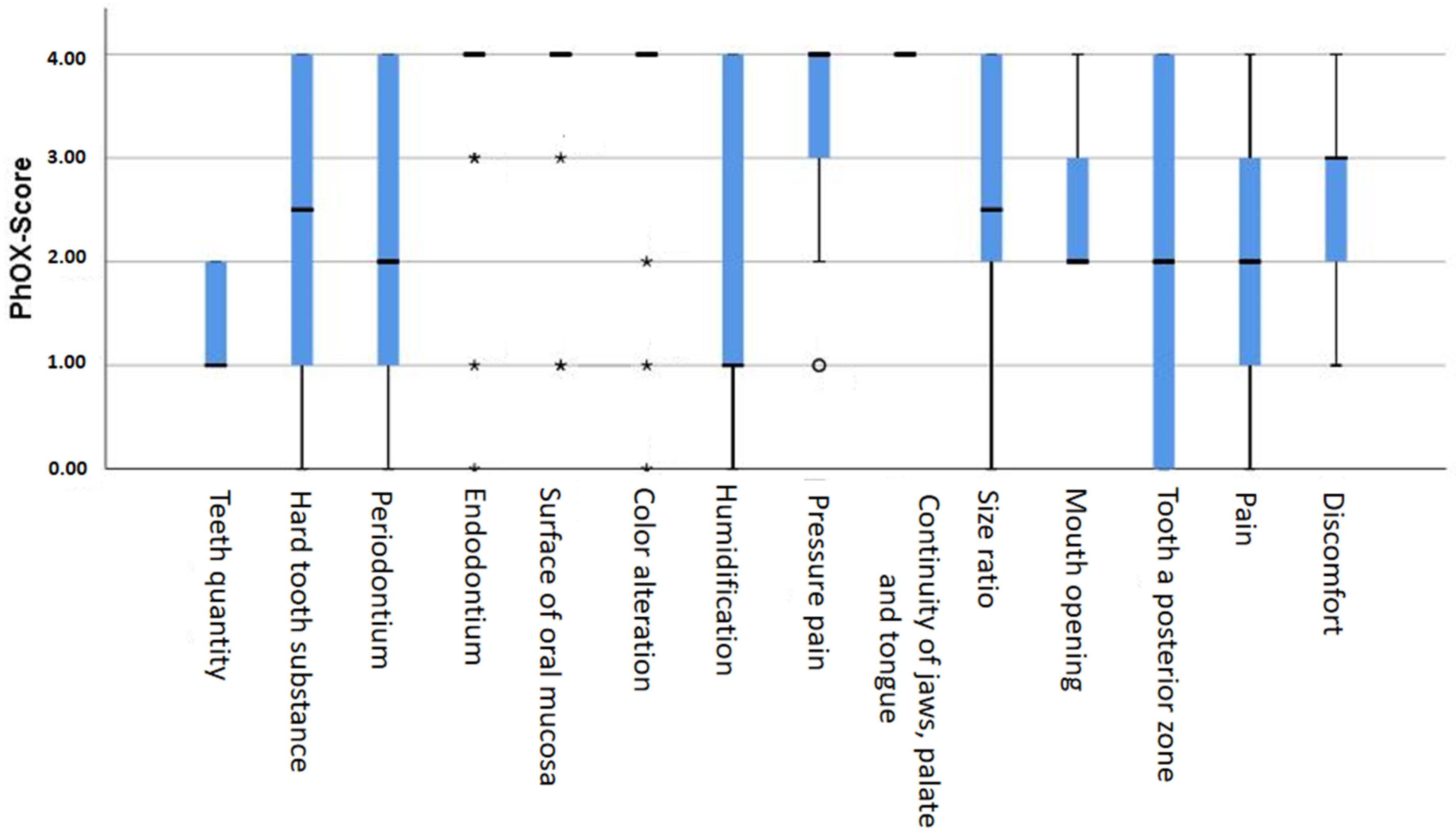
3.2. Physical Oral Health
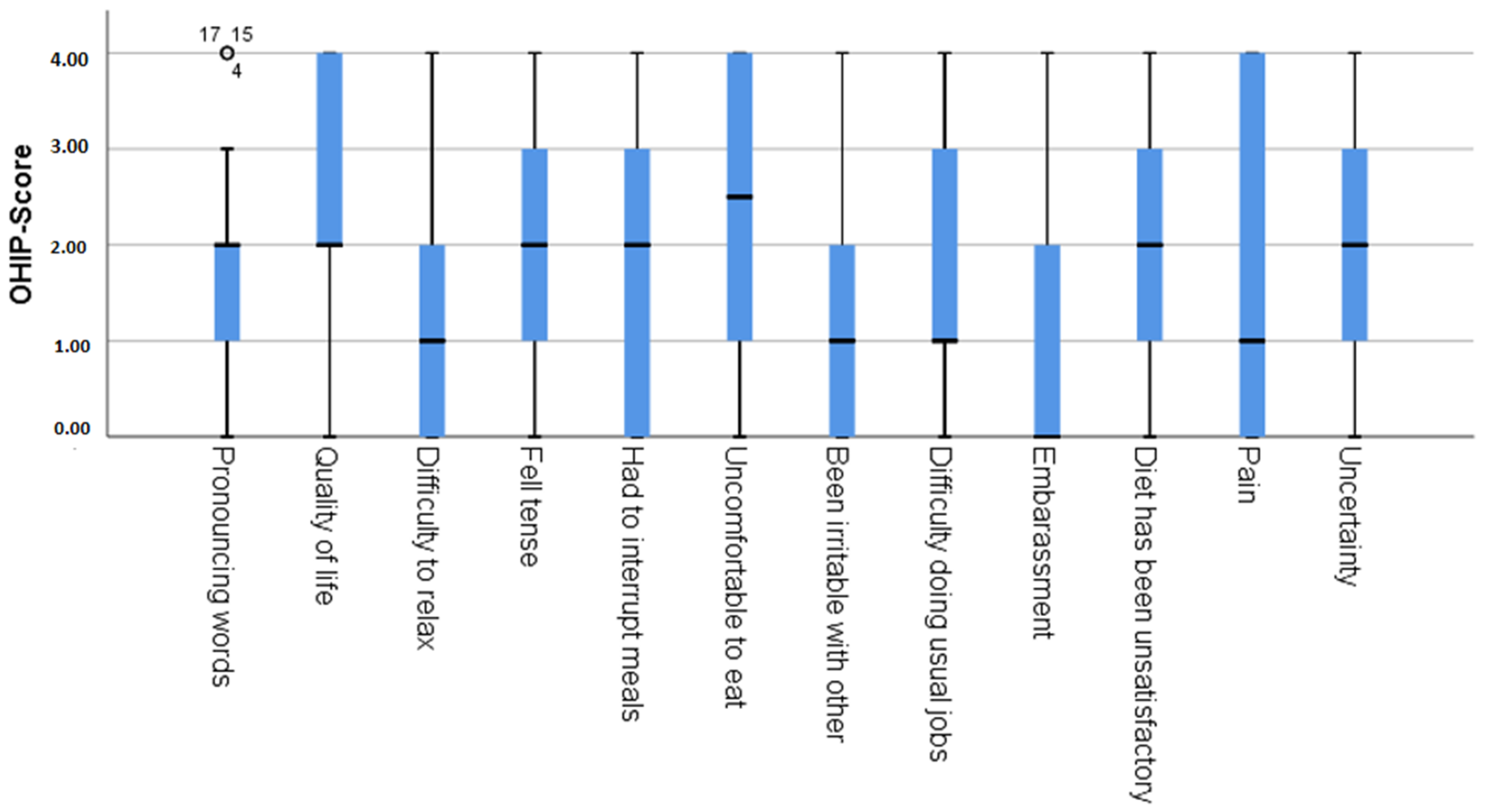
3.3. OHRQoL
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ED | ectodermal dysplasia |
| OHIP-14G | Oral Health Impact Profile-14 (German version) |
| OHRQoL | oral health-related quality of life |
| PhOX | Physical Oral Health Index |
References
- Wang, Y.; He, J.; Decker, A.M.; Hu, J.C.; Zou, D. Clinical outcomes of implant therapy in ectodermal dysplasia patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 1035–1043. [Google Scholar] [CrossRef]
- Wright, J.; Fete, M.; Schneider, H.; Zinser, M.; Koster, M.I.; Clarke, A.J.; Hadj-Rabia, S.; Tadini, G.; Pagnan, N.; Visinoni, A.F.; et al. Ectodermal dysplasias: Classification and organization by phenotype, genotype and molecular pathway. Am. J. Med. Genet. A 2019, 179, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, K.; Vinola, D.; John, J.B. Hypohidrotic ectodermal dysplasia-diagnostic aids and a report of 5 cases. J. Indian Soc. Pedod. Prev. Dent. 2010, 28, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.N.; Kumar, V. Ectodermal dysplasia-Maxillary and mandibular alveolar reconstruction with dental rehabilitation: A case report and review of the literature. Indian J. Plast. Surg. 2010, 43, 92–96. [Google Scholar] [CrossRef]
- Mikkola, M.L. Molecular aspects of hypohidrotic ectodermal dysplasia. Am. J. Med. Genet. A 2009, 149, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Nordgarden, H.; Jensen, J.L.; Storhaug, K. Oligodontia is associated with extra-oral ectodermal symptoms and low whole salivary flow rates. Oral Dis. 2001, 7, 226–232. [Google Scholar]
- Bergendal, B. Orodental manifestations in ectodermal dysplasia—A review. Am. J. Med. Genet. A 2014, 164A, 2465–2471. [Google Scholar] [CrossRef]
- Bergendal, B.; McAllister, A.; Stecksén-Blicks, C. Orofacial dysfunction in ectodermal dysplasias measured using the Nordic Orofacial Test-Screening protocol. Acta Odontol. Scand. 2009, 67, 377–381. [Google Scholar] [CrossRef]
- Saltnes, S.S.; Jensen, J.L.; Sæves, R.; Nordgarden, H.; Geirdal, A.Ø. Associations between ectodermal dysplasia, psychological distress and quality of life in a group of adults with oligodontia. Acta Odontol. Scand. 2017, 75, 564–572. [Google Scholar] [CrossRef]
- Visinoni, A.F.; Lisboa-Costa, T.; Pagnan, N.A.; Chautard-Freire-Maia, E.A. Ectodermal dysplasias: Clinical and molecular review. Am. J. Med. Genet. A 2009, 149, 1980–2002. [Google Scholar] [CrossRef]
- Hanisch, M.; Bohner, L.; Jung, S.; Kleinheinz, J. Seltene erkrankungen mit implantologischem therapiebedarf: Ektodermale dysplasien. Implantologie 2018, 26, 157–166. [Google Scholar]
- Hanisch, M.; Sielker, S.; Jung, S.; Kleinheinz, J.; Bohner, L. Self-assessment of oral health-related quality of life in people with ectodermal dysplasia in Germany. Int. J. Environ. Res. Public Health 2019, 16, 1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reissmann, D.R.; Aarabi, G.; von Wolff, A.; Kriston, L. The Physical Oral Health Index: Reliability and validity. J. Dent. Res. 2015, 94, 1465. [Google Scholar]
- Ramfjord, S.P. The Periodontal Disease Index (PDI). J. Periodontol. 1967, 38, 602–610. [Google Scholar] [CrossRef]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef] [PubMed]
- John, M.T.; Micheelis, W. Mundgesundheitsbezogene lebensqualität in der bevölkerung: Grundlagen und ergebnisse des OHIP aus einer repräsentativen stichprobe in Deutschland. IDZ Inf. 2003, 1, 1–28. [Google Scholar]
- Chrcanovic, B.R. Dental implants in patients with ectodermal dysplasia: A systematic review. J. Craniomaxillofac. Surg. 2018, 46, 1211–1217. [Google Scholar] [CrossRef]
- Guckes, A.D.; Scurria, M.S.; King, T.S.; McCarthy, G.R.; Brahim, J.S. Prospective clinical trial of dental implants in persons with ectodermal dysplasia. J. Prosthet. Dent. 2002, 88, 21–25. [Google Scholar] [CrossRef]
- Maiorana, C.; Poli, P.P.; Poggio, C.; Barbieri, P.; Beretta, M. Oral rehabilitation of a patient with ectodermal dysplasia treated with fresh-frozen bone allografts and computer-guided implant placement: A clinical case report. J. Oral Maxillofac. Surg. 2017, 75, 939–954. [Google Scholar] [CrossRef]
- Hanisch, M.; Hegemann, P.; Suwelack, D.; Kleinheinz, J. Rare diseases requiring dental implant therapy: Ectodermal dysplasia. Implantologie 2020, 28, 285–292. [Google Scholar]
- Oelerich, O.; Kleinheinz, J.; Reissmann, D.R.; Köppe, J.; Hanisch, M. Correlation between Oral Health-Related Quality of Life and Objectively Measured Oral Health in People with Ehlers–Danlos Syndromes. Int. J. Environ. Res. Public Health 2020, 17, 8243. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Syndrome Name(s) | Gene(s) | Distinguishing Features |
|---|---|---|
| Hypohidrotic ectodermal dysplasia (ED1; Christ–Siemens–Touraine syndrome) | Ectodysplasin A, EDA (300451) | Hypohidrosis, hypotrichosis, hypodontia, formanomalia of the teeth, smooth dry skin, craniofacial dysmorphology, periorbital pigmentation |
| Hypohidrotic ectodermal dysplasia 10A | Ectodysplasin A receptor, EDAR (604095) or EDARADD (606603) | Hypohidrosis, hypotrichosis, hypodontia, smooth dry skin, craniofacial dysmorphology, periorbital pigmentation |
| Hypohidrotic ectodermal dysplasia 10B | Ectodysplasin A receptor, EDAR (604095) or EDARADD (606603) | Hypohidrosis, hypotrichosis, hypodontia, smooth dry skin, craniofacial dysmorphology, periorbital pigmentation |
| Incontinentia pigmenti (IP) | IKBKG (300248) | Short stature, cataract, microphthalmia, hypodontia, formanomalia of the teeth, extra ribs, breast aplasia, staged skin involvement, nail dystrophy, atrophic hair |
| Ectodermal dysplasia and immunodeficiency 1 (EDAID1) | IKBKG (300248) | Hypohidrosis, hypotrichosis, morbidity/mortality secondary to immunodeficiency |
| Focal dermal hypoplasia (Goltz syndrome) | PORCN (300651) | Short stature, facial asymmetry, narrow auditory canals, hearing loss, oral papillomas, hypodontia, syndactyly, sparse hair, skin atrophy |
| Odontoonychodermal dysplasia (OODD) | WNT10A (606268) | Sparse eyebrows, severe hypodontia, formanomalia of the teeth, smooth tongue, hyperhidrosis, hyperkeratosis, dystrophic nails, sparse eyebrows, thin hair |
| Schopf–Schulz–Passarge syndrome | WNT10A (606268) | Hypodontia, eyelid cysts, keratoderma, hypoplastic nails, hypotrichiosis |
| Acro–dermato–ungual–lacrimal–tooth syndrome (ADULT syndrome) | TP63 (603273) | Lacrimal obstruction, hypodontia, dysplastic teeth, breast hypoplasia, ectrodactyly, thin skin, dysplastic nails |
| Ankyloblepharon-ectodermal defects-cleft lip and palate (AEC) syndrome (Hay–Wells syndrome) | TP63 (603273) | Scalp erosions, conductive hearing loss, maxillary hypoplasia, lacrimal duct atresia, hypotrichosis, ankyloblepharon, cleft lip, hypodontia |
| Rapp–Hodgkin syndrome | TP63 (603273) | Short stature, maxillary hypoplasia, hearing loss, cleft lip and palate, hypodontia, syndactyly, thin skin, hypohidrosis |
| Ectrodactyly, ectodermal dysplasia, and cleft lip and palate syndrome 3 (EEC3) | TP63 (603273) | Blepharophimosis, cleft lip and palate, microdontia, hypodontia, syndactyly, hypokeratosis, dystrophic nails, hypotrichiosis |
| Limb-mammary syndrome (LMS) | TP63 (603273) | Lacrimal duct atresia, hypodontia, cleft lip and palate, hypoplastic breasts, syndactyly, ectrodactyly, nail dystrophia |
| Ectodermal dysplasia, ectrodactyly, and macular dystrophy syndrome (EEMS) | CDH3 Cadherin 3 (114021) | Sparse scalp hair, eyebrows and eyelashes, hypodontia, small teeth, ectrodactyly, syndactyly, camptodactyly, normal sweating |
| Ectodermal dysplasia 4, hair/nail type (ECTD4) | KRT85 Keratin 85 (602767) | Nail dystrophy, onycholysis, absent eyebrows/eyelashes, alopecia, normal skin/teeth |
| Ectodermal dysplasia/skin fragility syndrome | PKP 1 Plakophilin 1 (601975) | Nail dystrophy and thickening, hypotrichosis, sweat glands, skin fragility |
| Monoilethrix (MNLIX) | Keratins 81, 86, 83; KRT81, KRT86, KRT83 (602153, 601928, 602765) | Follicular keratosis, nail dystrophy, hypotrichosis, brittle hair |
| Cleft lip/palate-ectodermal dysplasia (CLPED1) | Nectin 1 NECTIN1 (600644) | Malar hypoplasia, hypotrichosis, cleft lip/palate, hypodontia, syndactyly, onychodysplasia |
| Arthorgryposis and ectodermal dysplasia | Unknown | Short stature, microcephaly, cataract, cleft lip and palate, oligodontia, enamel defects, arthrogryposis, hypohidrosis, onychodysplasia |
| Dermoodontodysplasia | Unknown | Trichodysplasia, onychodysplasia, dental anomalies |
| Domain | # | Item | Weight | Range |
|---|---|---|---|---|
| Teeth and surrounding tissue | 1 | Number of teeth | 3 | 0–12 |
| 2 | Tooth structure | 3 | 0–12 | |
| 3 | Periodontium | 3 | 0–12 | |
| 4 | Endodontia | 2 | 0–8 | |
| Soft tissue intraoral | 5 | Surface | 1 | 0–4 |
| 6 | Color | 2 | 0–8 | |
| 7 | Moisturization | 1 | 0–4 | |
| Soft tissue and jaw | 8 | Pain on palpation | 1 | 0–4 |
| 9 | Continuity | 1 | 0–4 | |
| 10 | Proportion | 1 | 0–4 | |
| Function | 11 | Mouth opening | 1 | 0–4 |
| 12 | Supporting area | 3 | 0–12 | |
| Perception | 13 | Pain | 2 | 0–8 |
| 14 | Paresthesia | 1 | 0–4 |
| PhOX Values (%) | |||||
|---|---|---|---|---|---|
| Domain | 0 | 1 | 2 | 3 | 4 |
| Teeth quantity | 0 | 68.2 | 31.8 | 0 | 0 |
| Condition of teeth | 18.2 | 9.1 | 22.7 | 9.1 | 40.9 |
| Condition of periodontium | 4.5 | 22.7 | 45.5 | 0 | 27.3 |
| Condition of endodontium | 4.5 | 4.5 | 0 | 9.1 | 81.8 |
| Surface of oral mucosa | 0 | 9.1 | 0 | 4.5 | 86.4 |
| Color of oral mucosa | 4.5 | 4.5 | 4.5 | 0 | 86.4 |
| Moistening of oral mucosa | 9.1 | 59.1 | 0 | 0 | 31.8 |
| Pain on palpation of jaws and muscles | 0 | 9.1 | 4.5 | 13.6 | 63.6 |
| Continuity of jaws, palate and tongue | 0 | 0 | 0 | 0 | 100 |
| Size ratio of jaws | 4.5 | 18.2 | 27.3 | 13.6 | 36.4 |
| Mouth opening capacity | 0 | 0 | 72.7 | 9.1 | 18.2 |
| Number of supporting zones | 31.8 | 4.5 | 27.3 | 4.5 | 31.8 |
| Pain frequency | 9.1 | 22.7 | 2.3 | 27.3 | 9.1 |
| Paresthesia frequency | 0 | 13.6 | 22.7 | 36.4 | 22.7 |
| OHIP-14G Values (%) | |||||
|---|---|---|---|---|---|
| Domain | 0 | 1 | 2 | 3 | 4 |
| Difficulty pronouncing words | 18.2 | 27.3 | 31.8 | 9.1 | 13.6 |
| Taste | 59.1 | 27.3 | 0 | 0 | 13.6 |
| Quality of life | 9.1 | 9.1 | 36.4 | 13.6 | 31.8 |
| Difficulty relaxing | 27.3 | 27.3 | 22.7 | 0 | 22.7 |
| Felt tense | 13.6 | 27.3 | 22.7 | 18.2 | 18.2 |
| Had to interrupt meals | 31.8 | 13.6 | 22.7 | 9.1 | 22.7 |
| Uncomfortable to eat | 13.6 | 13.6 | 22.7 | 18.2 | 31.8 |
| Been irritable with others | 36.4 | 18.2 | 18.2 | 13.6 | 9.1 |
| Difficulty doing usual jobs | 22.7 | 36.4 | 9.1 | 13.6 | 18.2 |
| Unable to function | 59.1 | 13.6 | 9.1 | 4.5 | 13.6 |
| Embarrassment | 22.7 | 22.7 | 9.1 | 22.7 | 22.7 |
| Diet has been unsatisfactory | 31.8 | 22.7 | 9.1 | 9.1 | 27.3 |
| Pain | 18.2 | 18.2 | 31.8 | 13.6 | 18.2 |
| Uncertainty | 9.1 | 18.2 | 27.3 | 18.2 | 27.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niekamp, N.; Kleinheinz, J.; Reissmann, D.R.; Bohner, L.; Hanisch, M. Subjective Oral Health-Related Quality of Life and Objective Oral Health in People with Ectodermal Dysplasia. Int. J. Environ. Res. Public Health 2021, 18, 143. https://doi.org/10.3390/ijerph18010143
Niekamp N, Kleinheinz J, Reissmann DR, Bohner L, Hanisch M. Subjective Oral Health-Related Quality of Life and Objective Oral Health in People with Ectodermal Dysplasia. International Journal of Environmental Research and Public Health. 2021; 18(1):143. https://doi.org/10.3390/ijerph18010143
Chicago/Turabian StyleNiekamp, Nils, Johannes Kleinheinz, Daniel R. Reissmann, Lauren Bohner, and Marcel Hanisch. 2021. "Subjective Oral Health-Related Quality of Life and Objective Oral Health in People with Ectodermal Dysplasia" International Journal of Environmental Research and Public Health 18, no. 1: 143. https://doi.org/10.3390/ijerph18010143