Spatial-Temporal Modelling of Disease Risk Accounting for PM2.5 Exposure in the Province of Pavia: An Area of the Po Valley


Abstract
:1. Introduction
2. Materials and Methods
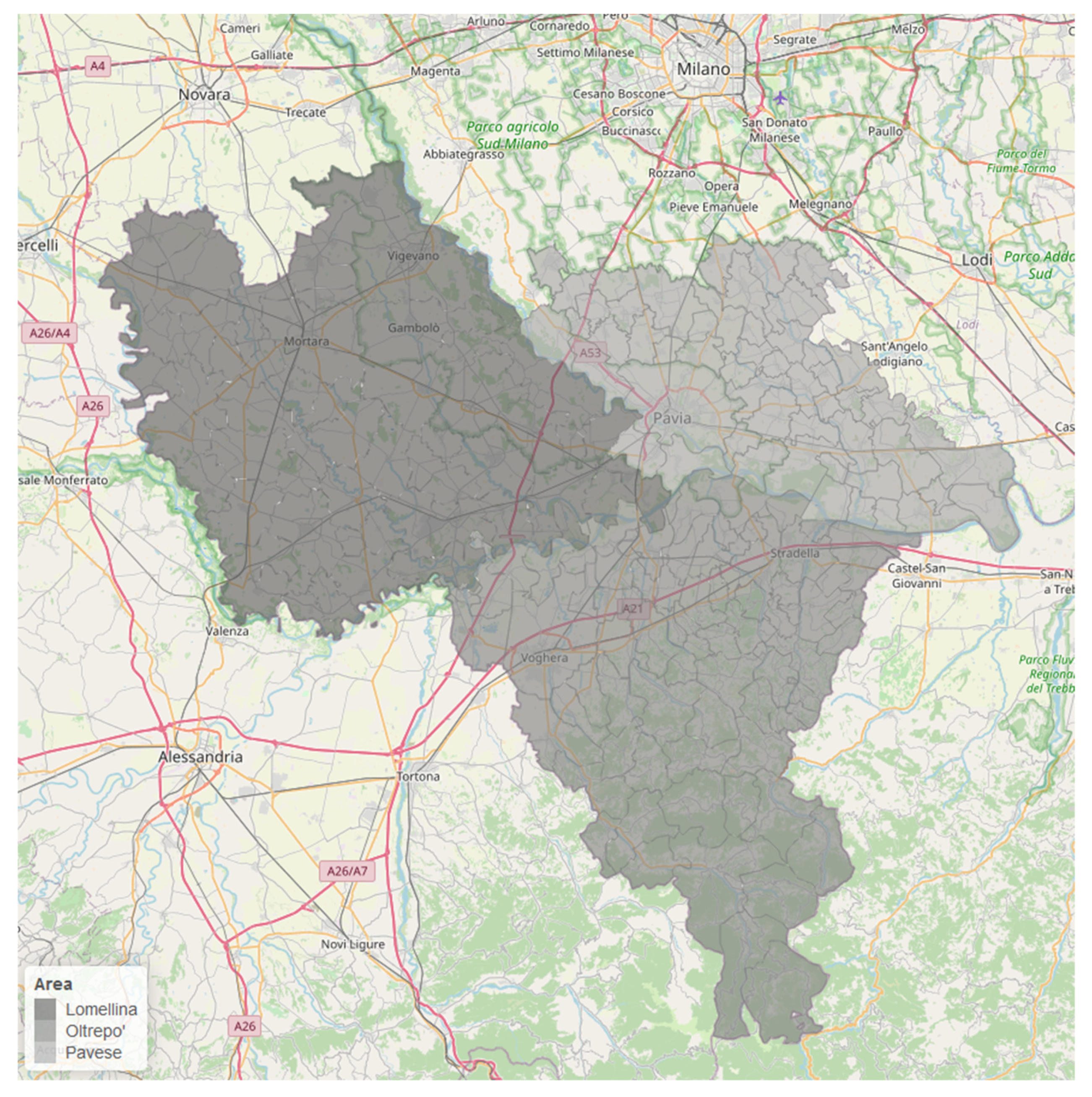
2.1. Study Area
2.2. The Study Design
2.3. The Outcome
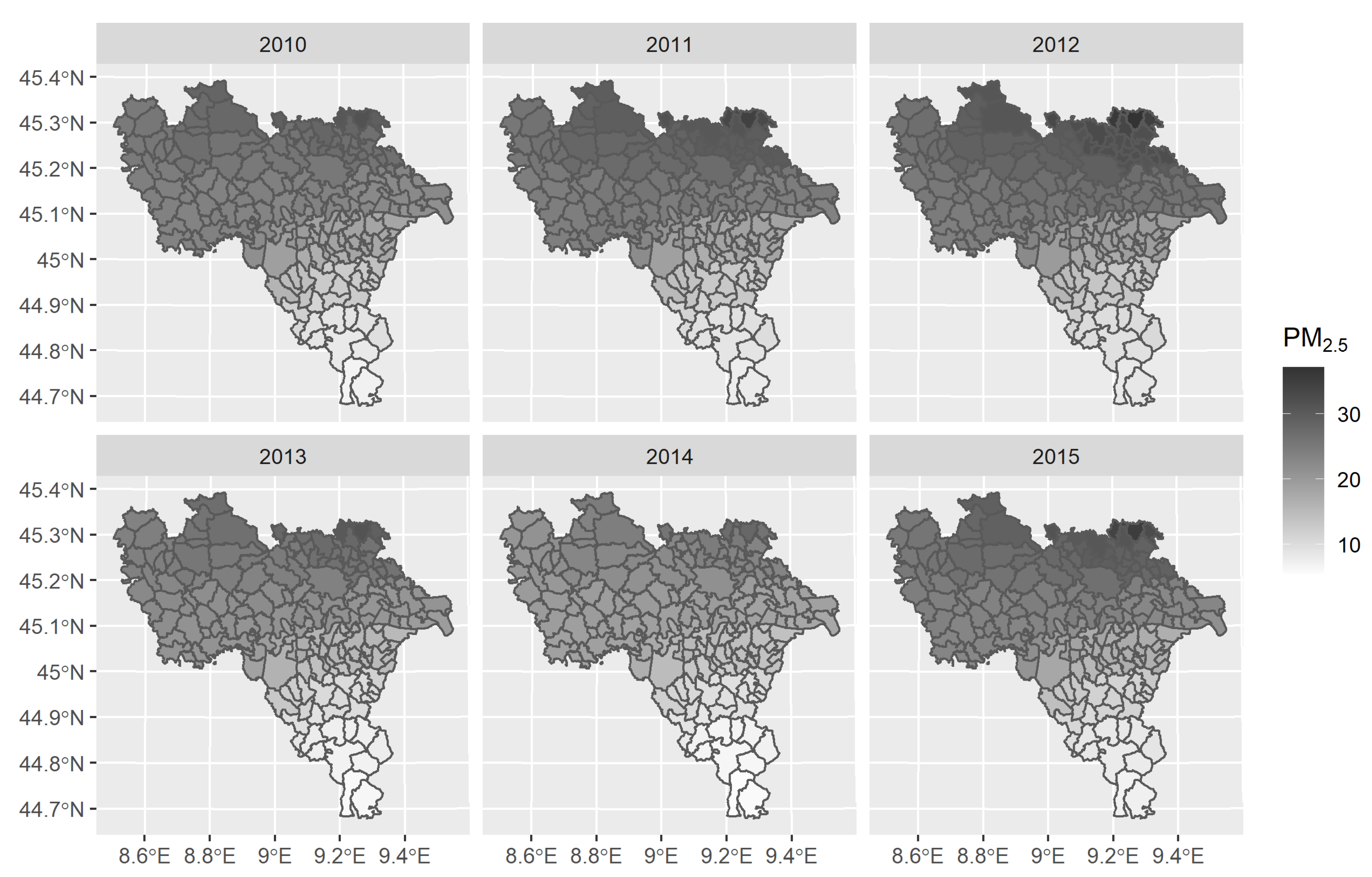
2.4. Environmental Exposure
2.5. The Population
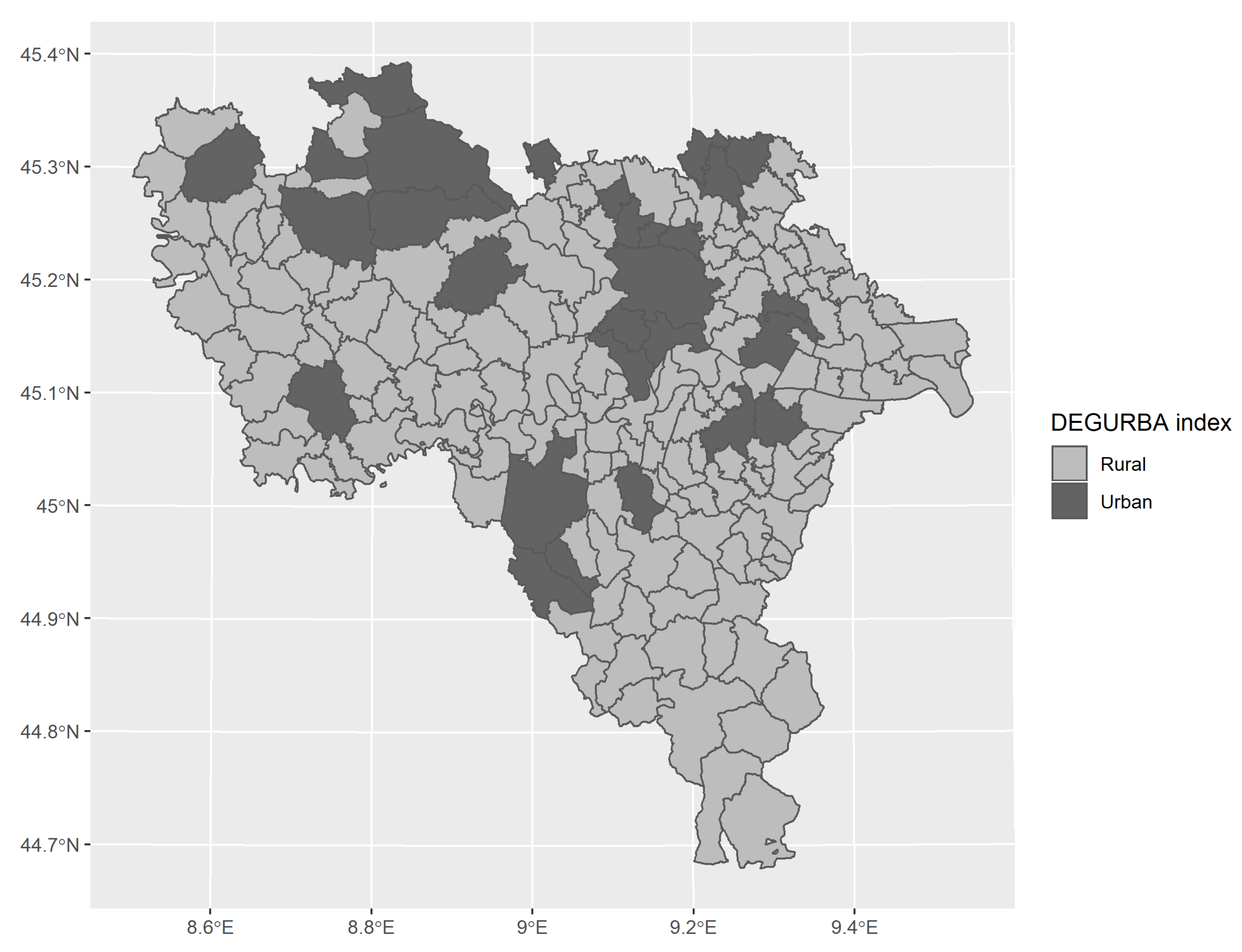
2.6. Degree of Urbanisation
2.7. Statistical Analyses
3. Results
3.1. Air Pollution and Degree of Urbanisation
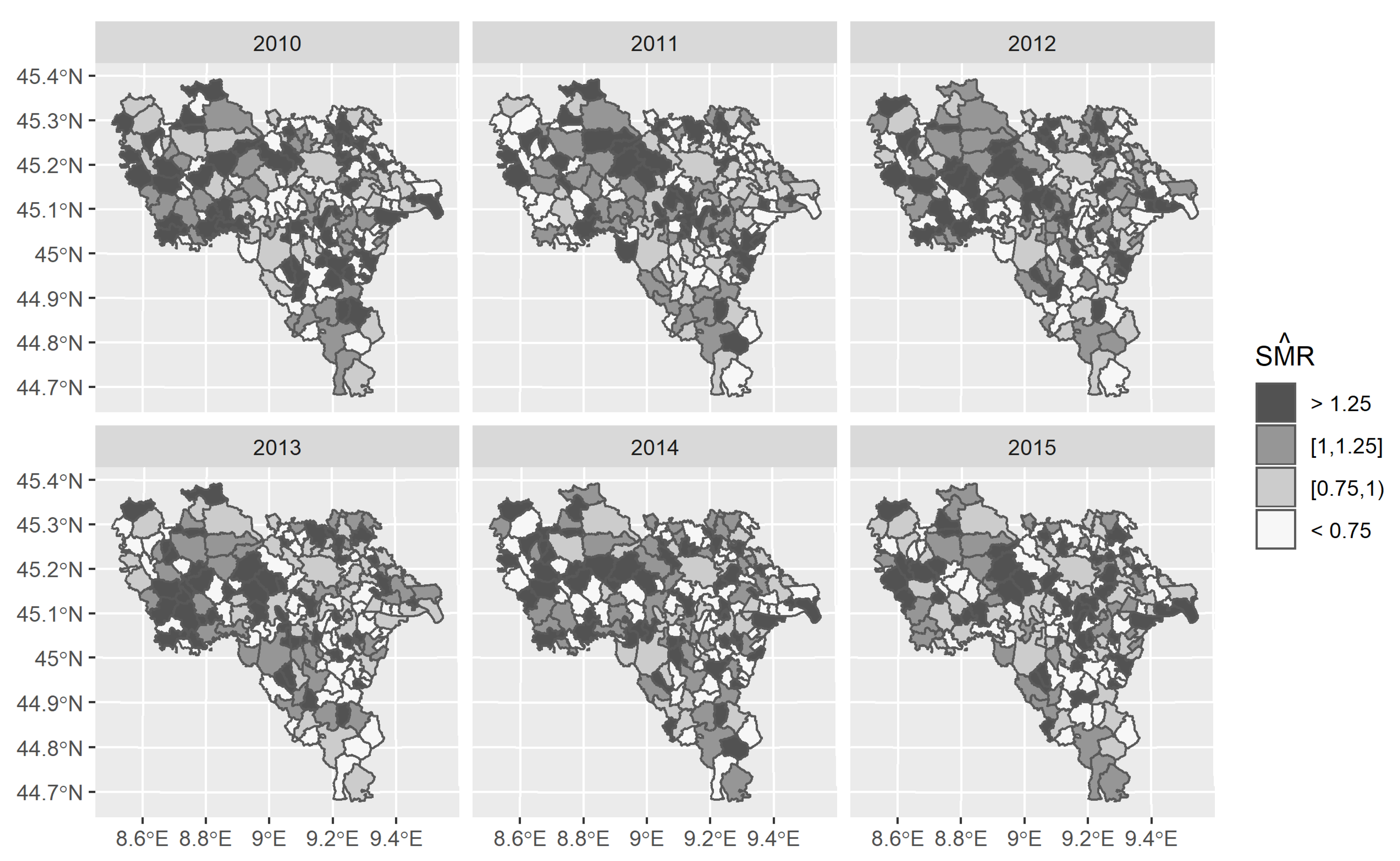
3.2. Cardiovascular Mortality
3.3. Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariates | 2.5th perc. | 25th perc. | Median | 75th perc. | 97.5th perc. | ||||
|---|---|---|---|---|---|---|---|---|---|
| (Intercept) | 0.977 | 0.009 | 0.958 | 0.970 | 0.977 | 0.984 | 0.997 | 0.013 | 0.986 |
| PM2.5 in μg/m3 | 1.075 | 0.020 | 1.034 | 1.061 | 1.075 | 1.089 | 1.116 | 0.999 | 0.000 |
| DEGURBA index rural vs urban | 1.022 | 0.014 | 0.993 | 1.012 | 1.021 | 1.031 | 1.050 | 0.937 | 0.062 |
| (a) Model 1 | |||||||||
| A | |||||||||
| Covariates | 2.5th perc. | 25th perc. | Median | 75th perc. | 97.5th perc. | ||||
| (Intercept) | −0.0207 | 0.0117 | −0.0437 | −0.0285 | −0.0208 | −0.0128 | 0.00221 | 0.0393 | 0.961 |
| PM2.5 in μg/m3 | 0.0731 | 0.0227 | 0.0291 | 0.0577 | 0.0728 | 0.0882 | 0.118 | 0.999 | 0.00065 |
| DEGURBA index rural vs urban | 0.0313 | 0.0180 | −0.00422 | 0.0194 | 0.0313 | 0.0436 | 0.0662 | 0.959 | 0.0413 |
| B | |||||||||
| (Intercept) | −0.0264 | 0.0175 | −0.0609 | −0.0383 | −0.0263 | −0.0145 | 0.00776 | 0.0644 | 0.936 |
| PM2.5 in μg/m3 | 0.0747 | 0.0233 | 0.0289 | 0.0593 | 0.0746 | 0.0902 | 0.121 | 1.00 | 0.000500 |
| DEGURBA index rural vs urban | 0.0316 | 0.0182 | −0.00454 | 0.0193 | 0.0318 | 0.0439 | 0.0670 | 0.959 | 0.0414 |
| Calendar year | 0.00210 | 0.00488 | −0.00754 | −0.00117 | 0.00209 | 0.00538 | 0.0117 | 0.671 | 0.329 |
| (b) Model 2 | |||||||||
| A | |||||||||
| Covariates | 2.5th perc. | 25th perc. | Median | 75th perc. | 97.5th perc. | ||||
| Intercept | −0.0228 | 0.0102 | −0.0426 | −0.0297 | −0.0228 | −0.0159 | −0.0026 | 0.0138 | 0.9860 |
| PM2.5 in μg/m3 | 0.0726 | 0.0193 | 0.0341 | 0.0596 | 0.0726 | 0.0855 | 0.1100 | 1.0000 | 0.00005 |
| DEGURBA index rural vs urban | 0.0217 | 0.0142 | −0.0063 | 0.0120 | 0.0217 | 0.0313 | 0.0494 | 0.9370 | 0.0628 |
| B | |||||||||
| (Intercept) | −0.0297 | 0.0140 | −0.0573 | −0.0391 | −0.0298 | −0.0203 | −0.0023 | 0.0168 | 0.9830 |
| PM2.5 in μg/m3 | 0.0749 | 0.0193 | 0.0368 | 0.0617 | 0.0749 | 0.0880 | 0.1130 | 1.0000 | 0.0001 |
| DEGURBA index rural vs urban | 0.0226 | 0.0151 | −0.0069 | 0.0123 | 0.0225 | 0.0329 | 0.0517 | 0.9310 | 0.0687 |
| Calendar year | 0.0018 | 0.0033 | −0.0046 | −0.0004 | 0.0018 | 0.0040 | 0.0083 | 0.7120 | 0.2880 |
| (c) Model 3 | |||||||||
| A | |||||||||
| Covariates | 2.5th perc. | 25th perc. | Median | 75th perc. | 97.5th perc. | ||||
| (Intercept) | −0.0236 | 0.0083 | −0.0399 | −0.0291 | −0.0236 | −0.0181 | −0.0073 | 0.0027 | 0.9970 |
| PM2.5 in μg/m3 | 0.0678 | 0.0201 | 0.0287 | 0.0544 | 0.0676 | 0.0814 | 0.1070 | 1.0000 | 0.0003 |
| DEGURBA index rural vs urban | 0.0284 | 0.0122 | 0.0046 | 0.0203 | 0.0285 | 0.0366 | 0.0522 | 0.9900 | 0.0102 |
| B | |||||||||
| (Intercept) | −0.0290 | 0.0122 | −0.0529 | −0.0373 | −0.0289 | −0.0207 | −0.0050 | 0.0089 | 0.9910 |
| PM2.5 in μg/m3 | 0.0693 | 0.0205 | 0.02910 | 0.0556 | 0.0693 | 0.0829 | 0.1090 | 1.0000 | 0.0004 |
| DEGURBA index rural vs urban | 0.0297 | 0.0127 | 0.0046 | 0.0211 | 0.0296 | 0.0382 | 0.0547 | 0.9890 | 0.0109 |
| Calendar year | 0.00144 | 0.00425 | −0.00700 | −0.00142 | 0.00145 | 0.00432 | 0.00974 | 0.634 | 0.366 |
| (d) Model 4 | |||||||||
| A | |||||||||
| Covariates | 2.5th perc. | 25th perc. | Median | 75th perc. | 97.5th perc. | ||||
| (Intercept) | −0.0235 | 0.0103 | −0.0436 | −0.0304 | −0.0235 | −0.0166 | −0.0031 | 0.0109 | 0.9890 |
| PM2.5 in μg/m3 | 0.0768 | 0.0207 | 0.0360 | 0.0628 | 0.0769 | 0.0906 | 0.1180 | 1.0000 | 0.0002 |
| DEGURBA index rural vs urban | 0.0209 | 0.0140 | −0.0067 | 0.0113 | 0.0207 | 0.0304 | 0.0483 | 0.9320 | 0.0680 |
| B | |||||||||
| (Intercept) | −0.0300 | 0.0141 | −0.0577 | −0.0395 | −0.0301 | −0.0206 | −0.0021 | 0.0182 | 0.9820 |
| PM2.5 in μg/m3 | 0.0792 | 0.0212 | 0.0380 | 0.0649 | 0.0793 | 0.09330 | 0.1200 | 1.0000 | 0.00005 |
| DEGURBA index rural vs urban | 0.0229 | 0.0150 | −0.0066 | 0.0127 | 0.0229 | 0.03280 | 0.0524 | 0.9370 | 0.0632 |
| Calendar year | 0.0001 | 0.0044 | −0.0078 | −0.0020 | 0.0010 | 0.0040 | 0.0098 | 0.5880 | 0.4120 |
References
- Rees, J.; Kanabar, D.; Pattani, S. ABC Asthma, 6th ed.; BMJ Publishing Group: Oxford, UK, 2010; ISBN 978-1-4051-8596-7. [Google Scholar]
- Yemaneberhan, H.; Bekele, Z.; Venn, A.; Lewis, S.; Parry, E.; Britton, J. Prevalence of wheeze and asthma and relation to atopy in urban and rural Ethiopia. Lancet 1997, 350, 85–90. [Google Scholar] [CrossRef]
- D’Amato, G. Outdoor air pollution in urban areas and allergic respiratory diseases. Monaldi Arch. Chest Dis. 1999, 54, 470–474. [Google Scholar] [PubMed]
- Koenig, J.Q. Air pollution and asthma. J. Allergy Clin. Immunol. 1999, 104, 717–722. [Google Scholar] [CrossRef]
- Künzli, N.; Medina, S.; Kaiser, R.; Quénel, P.; Horak, F., Jr.; Studnicka, M. Assessment of deaths attributable to air pollution: Should we use risk estimates bases on time series or on cohort studies? Am. J. Epidemiol. 2001, 153, 1050–1055. [Google Scholar]
- Baldacci, S.; Viegi, G. Respiratory effects of environmental pollution: Epidemiological data. Monaldi Arch. Chest Dis. 2002, 57, 156–160. [Google Scholar]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar]
- Boldo, E.; Linares, C.; Aragonés, N.; Lumbreras, J.; Borge, R.; de la Paz, D.; Pérez-Gómez, B.; Fernández-Navarro, P.; García-Pérez, J.; Pollán, M.; et al. Air quality modelling and mortality impact of fine particles reduction policies in Spain. Environ. Res. 2014, 128, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Khaniabadi, Y.O.; Goudarzi, G.; Daryanoosh, S.M.; Borgini, A.; Tittarelli, A.; De Marco, A. Exposure to PM10, NO2, and O3 and impacts on human health. Environ. Sci. Pollut. Res. Int. 2017, 24, 2781–2789. [Google Scholar] [CrossRef]
- Chen, Y.; Zang, L.; Du, W.; Xu, D.; Shen, G.; Zhang, Q.; Zou, Q.; Chen, J.; Zhao, M.; Yao, D. Ambient air pollution of particles and gas pollutants, and the predicted health risk from long-term exposure to PM2.5 in Zhejiang province, China. Environ. Sci Pollut. Res. Int. 2018, 25, 23833–23844. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.A.; Brook, R.; Pope, C.A., III. Air pollution and cardiovascular disease. Curr. Probl. Cardiol. 2015, 40, 207–238. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Court of Auditors. Special Report No 23/2018: Air Pollution: Our Health Still Insufficiently Protected. Available online: https://op.europa.eu/webpub/eca/special-reports/air-quality-23-2018/en/ (accessed on 16 September 2020).
- European Environment Agency. Outdoor Air Quality in Urban Areas. 2017. Available online: https://www.eea.europa.eu/publications/environmental-indicator-report-2017 (accessed on 16 September 2020).
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G.; Speizer, F.E. An Association between Air Pollution and Mortality in Six US Cities. N. Engl. J. Med. 1993, 329, 1753–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jerrett, M.; Burnett, R.T.; Ma, R.; Pope, C.A., III; Krewski, D.; Newbold, K.B.; Thurston, G.; Shi, Y.; Finkelstein, N.; Calle, E.E.; et al. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology 2005, 16, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Hoek, G.; van den Brandt, P.A.; Goldbohm, R.A.; Fischer, P.; Schouten, L.J.; Jerrett, M.; Hughes, E.; Armstrong, B.; Brunekreef, B. Long-term effects of traffic related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ. Health Perspect. 2008, 116, 196–202. [Google Scholar] [CrossRef]
- Baccini, M.; Biggeri, A.; Grillo, P.; Consonni, D.; Bertazzi, P.A. Health impact assessment of fine particle pollution at the regional level. Am. J. Epidemiol. 2011, 174, 1396–1405. [Google Scholar] [CrossRef] [Green Version]
- Alessandrini, E.R.; Faustini, A.; Chiusolo, M.; Stafoggia, M.; Gandini, M.; Demaria, M.; Antonelli, A.; Arena, P.; Biggeri, A.; Canova, C.; et al. Inquinamento atmosferico e mortalità in venticinque città italiane: Risultati del progetto EpiAir2. [Air pollution and mortality in twenty-five Italian cities: Results of the EpiAir2 Project]. Epidemiol. Prev. 2013, 37, 220–229. [Google Scholar]
- Carugno, M.; Consonni, D.; Randi, G.; Catelan, D.; Grisotto, L.; Bertazzi, P.A.; Biggeri, A.; Baccini, M. Air pollution exposure, cause-specific deaths and hospitalizations in a highly polluted Italian region. Environ. Res. 2016, 147, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Leogrande, S.; Alessandrini, E.R.; Stafoggia, M.; Morabito, A.; Nocioni, A.; Ancona, C.; Bisceglia, L.; Mataloni, F.; Giua, R.; Mincuzzi, A.; et al. Industrial air pollution and mortality in the Taranto area, Southern Italy: A difference-in-differences approach. Environ. Int. 2019, 132, 105030. [Google Scholar] [CrossRef]
- Lim, Y.R.; Bae, H.J.; Lim, Y.H.; Yu, S.; Kim, G.B.; Cho, Y.S. Spatial analysis of PM10 and cardiovascular mortality in the Seul metropolitan area. Environ. Health Toxicol. 2014, 29, e2014005. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Xu, L.; Zhou, Z.; Wu, Y.; Fang, Y. Application of SCM with Bayesian B-Spline to Spatio-Temporal Analysis of Hypertension in China. Int. J. Environ. Res. Public Health 2018, 15, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Monitoring and Evaluation Programme, EMEP Programme. Available online: www.emep.int (accessed on 16 September 2020).
- Simpson, D.; Benedictow, A.; Berge, H.; Bergström, R.; Emberson, L.D.; Fagerli, H.; Flechard, C.R.; Hayman, G.D.; Gauss, M.; Jonson, J.E.; et al. The EMEP MSC-W chemical transport model—technical description. Atmos. Chem. Phys. 2012, 7825–7865. [Google Scholar] [CrossRef] [Green Version]
- European Environment Agency. Directive 2008/50/EC of the European Parliament and of the Council on Ambient Air Quality and Cleaner Air for Europe. Available online: https://www.eea.europa.eu/policy-documents/directive-2008-50-ec-of (accessed on 16 September 2020).
- Agenzia Regionale per la Protezione dell’Ambiente. Temi Ambientali, Aria, Inquinanti, PM10 e PM2.5. Available online: https://www.arpalombardia.it/Pages/Aria/Inquinanti/PM10-PM2,5.aspx?firstlevel=Inquinanti (accessed on 16 September 2020).
- Demo-Geodemo. Maps, Population, Demography of ISTAT. Available online: http://demo.istat.it/ (accessed on 16 September 2020).
- European Environment Agency. Degree of Urbanisation (DEGURBA). Available online: https://www.eea.europa.eu/data-and-maps/data/external/degree-of-urbanisation-degurba (accessed on 16 September 2020).
- Waller, L.; Carlin, B. Bayesian Disease Mapping. Chapman Hall CRC Handb. Mod. Stat. Methods 2010, 2010, 217–243. [Google Scholar] [PubMed] [Green Version]
- Ripley, B.D. Spatial Statistics; Wiley Series in Probability and Statistics; Wiley: Hoboken, NJ, USA, 2005; p. 272. ISBN 978-0-471-72520-6. [Google Scholar]
- Besag, J.; York, J.; Mollié, A. Bayesian image restoration, with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991, 43, 1–20. [Google Scholar] [CrossRef]
- Morris, M.; Wheeler-Martin, K.; Simpson, D.; Mooney, S.J.; Gelman, A.; DiMaggio, C. Bayesian hierarchical spatial models: Implementing the Besag York Mollié model in Stan. Spat. Spatio-Temporal Epidemiol. 2019, 31, 100301. [Google Scholar] [CrossRef]
- Lawson, A.B. Bayesian Disease Mapping: Hierarchical Modeling in Spatial Epidemiology, 3rd ed.; Chapman and Hall/CRC: London, UK, 2018; ISBN 978-1-138-57542-4. [Google Scholar]
- Watanabe, S. Asymptotic equivalence of Bayes cross validation and widely applicable information criterion in singular learning theory. J. Mach. Learn Res. 2010, 11, 3571–3594. [Google Scholar]
- Gelman, A.; Hill, J. Data Analysis Using Regression and Multilevel/ Hierarchical Models; Cambridge University Press: New York, NY, USA, 2007; ISBN 978-0-521-68689-1. [Google Scholar]
- Gelman, A.; Hwang, J.; Vehtari, A. Understanding predictive information criteria for Bayesian models. Stat. Comput. 2014, 24, 997–1016. [Google Scholar] [CrossRef]
- Vehtari, A.; Gelman, A.; Gabry, J. Practical Bayesian model evaluation using leave-one-out cross-validation and WAIC. Stat. Comput. 2017, 27, 1413–1432. [Google Scholar] [CrossRef] [Green Version]
- Betancourt, M. A Conceptual Introduction to Hamiltonian Monte Carlo. arXiv 2017, arXiv:1701.02434. [Google Scholar]
- Stan Development Team. Stan Modeling Language Users Guide and Reference Manual, Version 2.18.0. 2018. Available online: http://mc-stan.org (accessed on 16 September 2020).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/ (accessed on 16 September 2020).
- Gelman, A.; Carlin, J.; Stern, H.; Dunson, D.; Vehtari, A.; Rubin, D. Bayesian Data Analysis, 3rd ed.; Taylor & Francis Ltd.: Oxfordshire, UK; Chapman & Hall Book: London, UK, 2013; ISBN 978-1-4398-9820-8. [Google Scholar]
- Stan Development Team. RStan: The R Interface to Stan. R Package Version 2.17.3. 2018. Available online: http://mc-stan.org (accessed on 16 September 2020).
- Vehtari, A.; Gelman, A.; Gabry, J. Pareto smoothed importance sampling. arXiv 2017, arXiv:1507.02646. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; D’Agostino-McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Kay, M. Tidybayes: Tidy Data and Geoms for Bayesian Models. R Package Version 2.1.1. 2020. Available online: http://mjskay.github.io/tidybayes/ (accessed on 16 September 2020).
- Pebesma, E. Simple Features for R: Standardized Support for Spatial Vector Data. R J. 2018, 10, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Bivand, R.S.; Edzer, P.E.; Gómez-Rubio, V. Applied Spatial Data Analysis with R, 2nd ed.; Springer: New York, NY, USA, 2013; ISBN 978-1-4614-7618-4. [Google Scholar]
- Bivand, R. Bindings for the ‘Geospatial’ Data Abstraction Library. 2020. Available online: https://rdrr.io/cran/rgdal/ (accessed on 16 September 2020).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- United States Environmental Protection Agency. Altitude as a factor in air pollution. In National Service Center for Environmental Publications (NSCEP): EPA/600/9-78/015 (NTIS PB285645); United States Environmental Protection Agency: Washington, DC, USA, 1978. Available online: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=2000TAGZ.TXT (accessed on 16 September 2020).
- Consonni, D.; DeMatteis, S.; Dallari, B.; Pesatori, A.C.; Riboldi, L.; Mensi, C. Impact of an asbestos cement factory on mesothelioma incidence in a community in Italy. Environ. Res. 2020, 183, 108968. [Google Scholar] [CrossRef] [PubMed]
- Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Goldberg, M.S.; Villeneuve, P.J.; Brion, O.; Khan, S.; Odwa Atari, D.; Jerrett, M.; Pope, C.A.; et al. Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ. Health Perspect. 2012, 120, 708–714. [Google Scholar] [CrossRef]
- Hayes, B.R.; Lim, C.; Zhang, Y.; Cromar, K.; Shao, Y.; Reynolds, R.H.; Silverman, T.D.; Jones, R.R.; Park, Y.; Jerrett, M.; et al. PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int. J. Epidemiol. 2020, 49, 25–35. [Google Scholar] [CrossRef]





| Mean | SD | Min | Max | Frequency of Municipalities Exceeding the Limit Value Defined for PM2.5 N (%) | |
|---|---|---|---|---|---|
| 2010 | 21.28 | 5.37 | 6.70 | 31.54 | 51 (27.12%) |
| 2011 | 22.48 | 6.11 | 7.50 | 34.45 | 75 (39.88%) |
| 2012 | 23.58 | 6.49 | 8.13 | 37.07 | 103 (57.78%), |
| 2013 | 19.40 | 5.77 | 5.88 | 31.39 | 31 (16.48%) |
| 2014 | 17.52 | 5.08 | 5.44 | 28.02 | 4 (2.12%) |
| 2015 | 21.38 | 6.33 | 6.92 | 35.31 | 55 (29.25%) |
| Observed Deaths | Mortality Risk Per 1000 | |||||
|---|---|---|---|---|---|---|
| Males | Females | Overall Population | Males | Females | Overall Population | |
| 2010 | 963 | 1424 | 2387 | 3.72 | 5.14 | 4.46 |
| 2011 | 947 | 1353 | 2300 | 3.66 | 4.88 | 4.29 |
| 2012 | 1000 | 1405 | 2405 | 3.87 | 5.07 | 4.49 |
| 2013 | 939 | 1362 | 2301 | 3.63 | 4.92 | 4.30 |
| 2014 | 944 | 1316 | 2260 | 3.65 | 4.75 | 4.22 |
| 2015 | 1054 | 1476 | 2530 | 4.06 | 5.33 | 4.72 |
| Models | Without Temporal Trend (A) | With Temporal Trend (B) | ||
|---|---|---|---|---|
| WAIC * | LOO-CV ** | WAIC | LOO-CV | |
| M1—Log-linear | 5350.4 ± 73.7 | 5350.4 ± 73.7 | 5353.2 ± 73.9 | 5353.3 ± 73.9 |
| M2—Log-linear with spatially unstructured random intercept | 5152.3 ± 58.7 | 5154.2 ± 58.8 | 5153.2 ± 58.8 | 5155.1 ± 58.8 |
| M3—Log-linear with spatially structured random intercept | 5306.4 ± 67.0 | 5314.5 ± 67.6 | 5306.9 ± 67.1 | 5314.6 ± 67.6 |
| M4—Log-linear with the BYM# convolution random component | 5163.8 ± 58.0 | 5171.3 ± 58.4 | 5163.7 ± 58.0 | 5171.2 ± 58.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trivelli, L.; Borrelli, P.; Cadum, E.; Pisoni, E.; Villani, S. Spatial-Temporal Modelling of Disease Risk Accounting for PM2.5 Exposure in the Province of Pavia: An Area of the Po Valley. Int. J. Environ. Res. Public Health 2021, 18, 658. https://doi.org/10.3390/ijerph18020658
Trivelli L, Borrelli P, Cadum E, Pisoni E, Villani S. Spatial-Temporal Modelling of Disease Risk Accounting for PM2.5 Exposure in the Province of Pavia: An Area of the Po Valley. International Journal of Environmental Research and Public Health. 2021; 18(2):658. https://doi.org/10.3390/ijerph18020658
Chicago/Turabian StyleTrivelli, Leonardo, Paola Borrelli, Ennio Cadum, Enrico Pisoni, and Simona Villani. 2021. "Spatial-Temporal Modelling of Disease Risk Accounting for PM2.5 Exposure in the Province of Pavia: An Area of the Po Valley" International Journal of Environmental Research and Public Health 18, no. 2: 658. https://doi.org/10.3390/ijerph18020658