
Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.2.1. Demographics
2.2.2. Life Events
2.2.3. Mental Health Outcomes
2.2.4. Resilience Factors
2.3. Data Analysis
2.3.1. Exposure to Fires across Participant Subgroups
2.3.2. Prediction of Mental Health Outcomes
3. Results
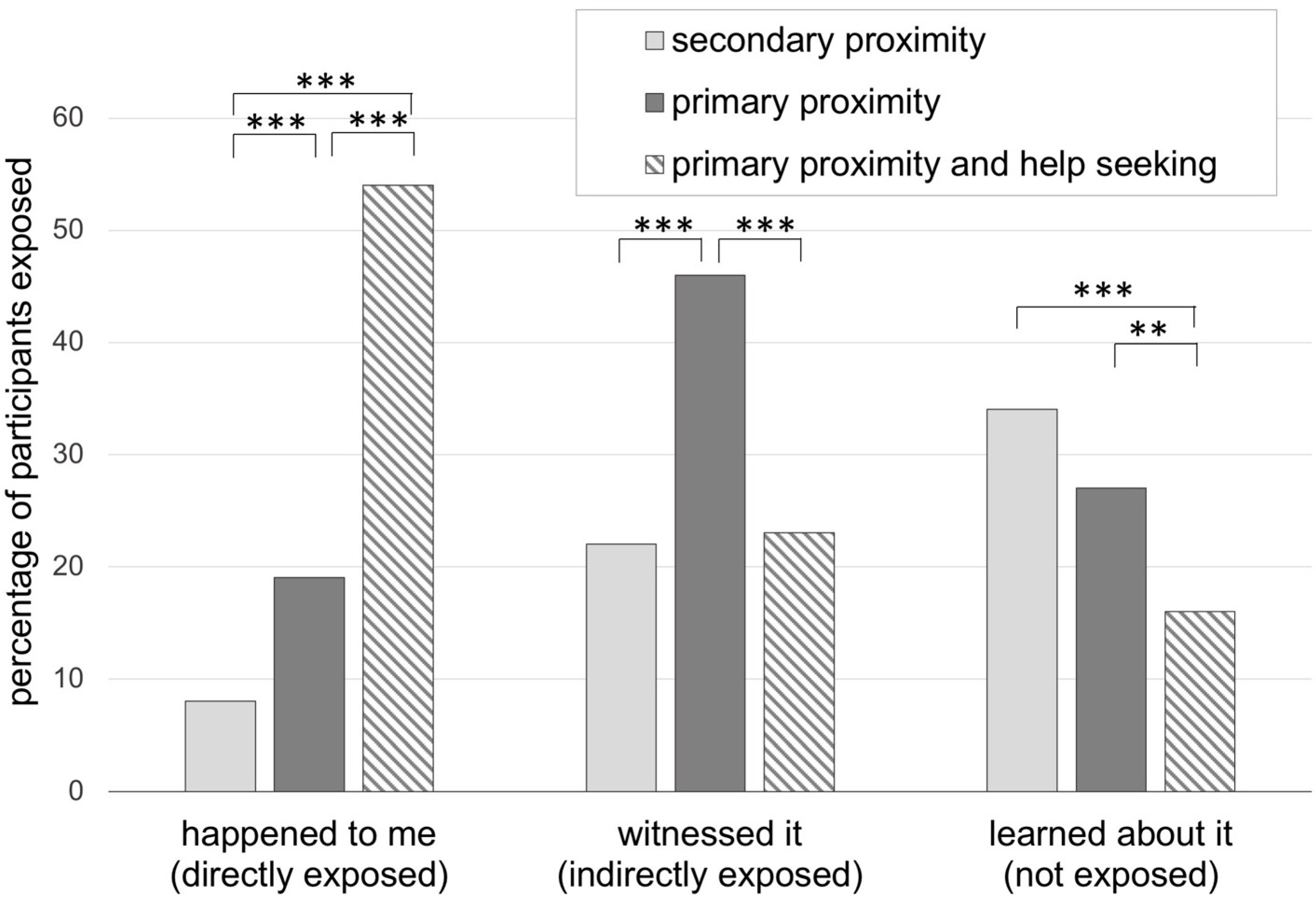
3.1. Exposure to Wildfires across Participant Subgroups
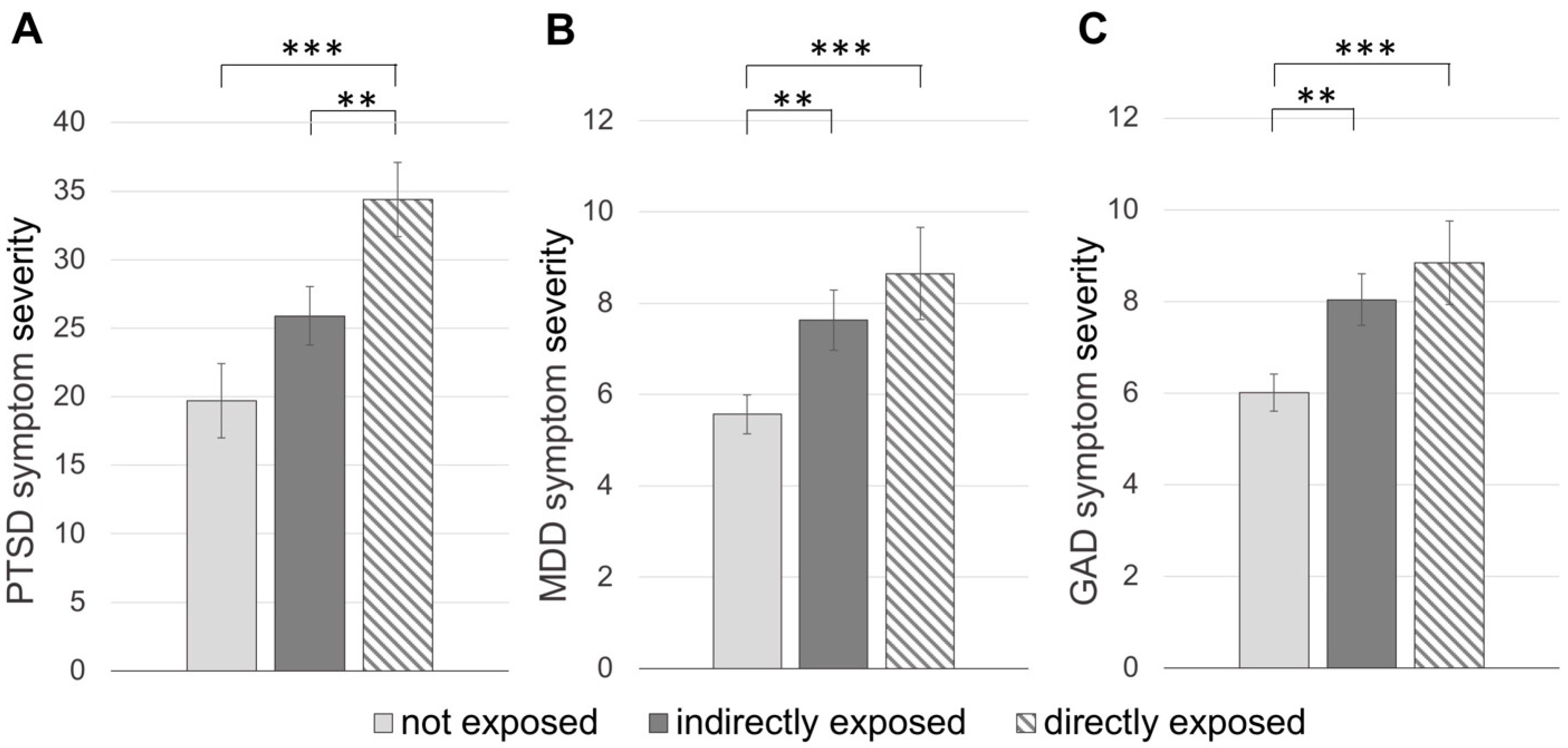
3.2. Mental Health Outcomes of Exposure to Wildfires
3.2.1. Post-Traumatic Stress Disorder
3.2.2. Major Depressive Disorder
3.2.3. General Anxiety Disorder
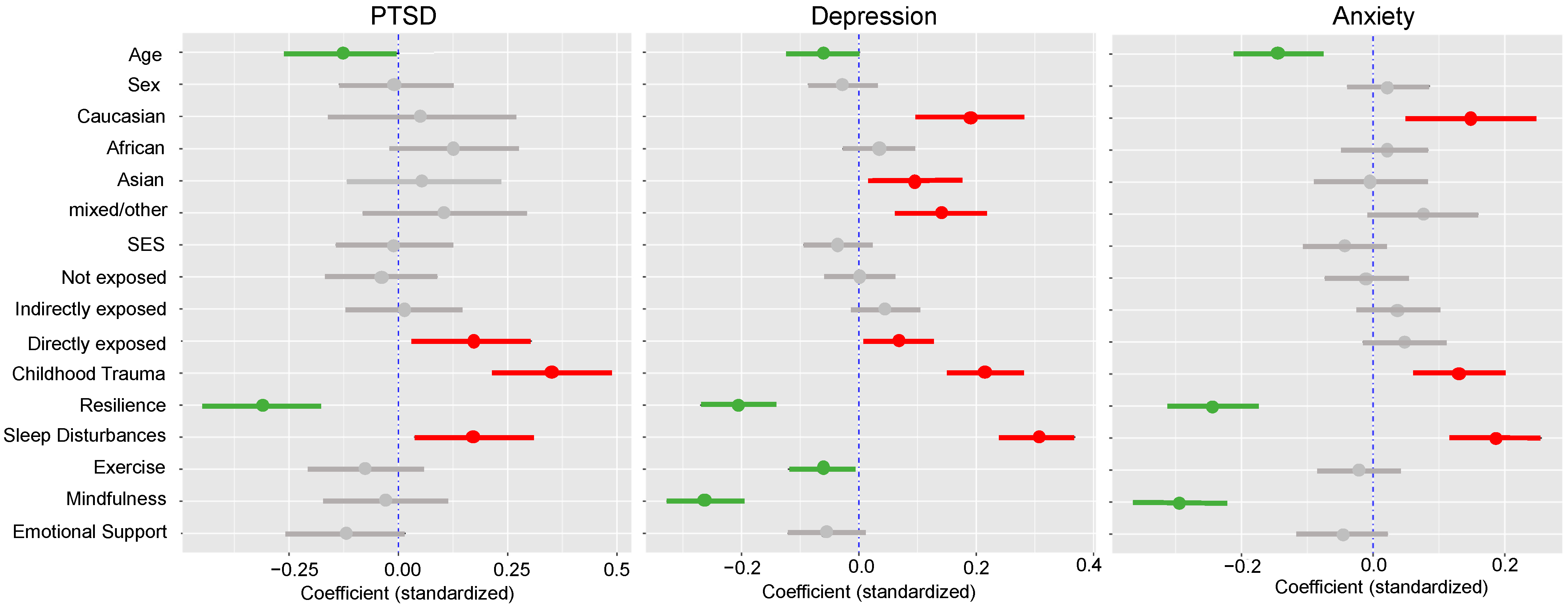
3.3. Influence of Vulnerability and Resilience Factors
3.3.1. Post-Traumatic Stress Disorder
3.3.2. Major Depressive Disorder
3.3.3. Generalized Anxiety Disorder
3.3.4. Interactions between Fire Exposure and Vulnerability or Resilience Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Masson-Delmotte, V.; Zhai, P.; Pörtner, H.O.; Roberts, D.; Skea, J.; Shukla, P.R.; Pirani, A.; Moufouma-Okia, W.; Péan, C.; Pidcock, R.; et al. (Eds.) Global Warming of 1.5 °C: An IPCC Special Report on the Impacts of Global Warming of 1.5 °C Above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change; IPCC: Geneva, Switzerland, 2018. [Google Scholar]
- International Federation of Red Cross and Red Crescent. Climate change—The early warning. In World Disasters Report 2009—Focus on Early Warning, Early Action; International Federation of Red Cross and Red Crescent: Geneva, Switzerland, 2009. [Google Scholar]
- Duffy, P.B.; Field, C.B.; Diffenbaugh, N.S.; Doney, S.C.; Dutton, Z.; Goodman, S.; Heinzerling, L.; Hsiang, S.; Lobell, D.B.; Mickley, L.J.; et al. Strengthened scientific support for the endangerment finding for atmospheric greenhouse gases. Science 2019, 363, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.; Leach, S.; Wachter, B.; Gardunio, B. The Extreme 2018 Northern California fire season. Bull. Am. Meteorol. Soc. 2020, 101, 2018–2021. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.P.; Abatzoglou, J.T.; Gershunov, A.; Guzman-Morales, J.; Bishop, D.A.; Balch, J.K.; Lettenmaier, D.P. Observed impacts of anthropogenic climate change on wildfire in california. Earth’s Future 2019, 7, 892–910. [Google Scholar] [CrossRef] [Green Version]
- Goss, M.; Swain, D.L.; Abatzoglou, J.T.; Sarhadi, A.; Kolden, C.A.; Williams, A.P.; Diffenbaugh, N.S. Climate change is increasing the likelihood of extreme autumn wildfire conditions across California. Environ. Res. Lett. 2020, 15, 094016. [Google Scholar] [CrossRef] [Green Version]
- Fire Statistics. CAL FIRE (2018). Available online: https://www.fire.ca.gov/incidents/2018/ (accessed on 25 December 2020).
- National Year-to-Date Report on Fires and Acres Burned. NIFC (2018). Available online: https://www.nifc.gov/fireInfo/fireInfo_statistics.html (accessed on 25 December 2020).
- The Human Cost of Weather-Related Disasters 1995–2015. Centre for Research on the Epidemiology Disasters (CRED), United Nations Office for Disaster Risk Reduct, 2015. Available online: https://www.undrr.org/publication/human-cost-weather-related-disasters-1995-2015 (accessed on 25 December 2020).
- Mora, C.; Spirandelli, D.; Franklin, E.C.; Lynham, J.; Kantar, M.B.; Miles, W.; Smith, C.Z.; Freel, K.; Moy, J.; Louis, L.V.; et al. Broad threat to humanity from cumulative climate hazards intensified by greenhouse gas emissions. Nat. Clim. Chang. 2018, 8, 1062–1071. [Google Scholar] [CrossRef]
- Sorondo, M.M.S.; Frumkin, H.; Ramanathan, V. Health, faith, and science on a warming planet. JAMA J. Am. Med. Assoc. 2018, 319, 1651–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batibeniz, F.; Ashfaq, M.; Diffenbaugh, N.S.; Key, K.; Evans, K.J.; Turuncoglu, U.U.; Önol, B. Doubling of U.S.: Population exposure to climate extremes by 2050. Earth’s Future 2020, 8, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Coyle, J.; Van Susteren, L. The Psychological Effects of Global Warming on the United States: February 2012 National Wildlife Federation Climate Education Program with Support from the Robert Wood Johnson Foundation Executive Summary. 2011. Available online: https://nwf.org/~/media/PDFs/Global-Warming/Reports/Psych_effects_Climate_Change_Ex_Sum_3_23.ashx (accessed on 25 December 2020).
- Lowe, S.R.; Bonumwezi, J.L.; Valdespino-Hayden, Z.; Galea, S. Posttraumatic stress and depression in the aftermath of environmental disasters: A review of quantitative studies published in 2018. Curr. Environ. Health Rep. 2019, 6, 344–360. [Google Scholar] [CrossRef]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef]
- Goldman, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Harville, E.W.; Shankar, A.; Dunkel Schetter, C.; Lichtveld, M. Cumulative effects of the Gulf oil spill and other disasters on mental health among reproductive-aged women: The gulf resilience on women’s health study. Psychol. Trauma Theory Res. Pract. Policy 2018, 10, 533. [Google Scholar] [CrossRef]
- Lee, J.; Blackmon, B.J.; Lee, J.Y.; Cochran, D.M., Jr.; Rehner, T.A. An exploration of posttraumatic growth, loneliness, depression, resilience, and social capital among survivors of hurricane Katrina and the deepwater horizon oil spill. J. Community Psychol. 2019, 47, 356–370. [Google Scholar] [CrossRef]
- Koopman, C.; Classen, C.; Spiegel, D. Dissociative responses in the immediate aftermath of the Oakland/Berkeley firestorm. J. Trauma. Stress 1996, 9, 521–540. [Google Scholar] [CrossRef]
- North, C.S.; Hong, B.A.; Suris, A.; Spitznagel, E.L. Distinguishing distress and psychopathology among survivors of the Oakland/Berkeley firestorm. Psychiatry 2008, 71, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Psarros, C.; Theleritis, C.G.; Martinaki, S.; Bergiannaki, I.D. Traumatic reactions in firefighters after wildfires in Greece. Lancet 2008, 371, 301. [Google Scholar] [CrossRef]
- Berry, L.H.; Bowen, K. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Berry, H. Pearl in the oyster: Climate change as a mental health opportunity. Australas. Psychiatry 2009, 17, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Thordardottir, E.B.; Gudmundsdottir, H.; Gudmundsdottir, B.; Hrólfsdóttir, A.M.; Aspelund, T.; Hauksdottir, A. Development and predictors of psychological outcomes following the 2008 earthquake in Iceland: A longitudinal cohort study. Scand. J. Public Health 2019, 47, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wang, Y.; Tang, W. Risk factors of post-traumatic stress and depressive disorders in longmenshan adolescents after the 2013 Lushan earthquake. Community Ment. Health J. 2019, 55, 497–506. [Google Scholar] [CrossRef] [PubMed]
- McFarlane, A.C.; Raphael, B. Ash wednesday: The effects of a fire. Aust. N. Z. J. Psychiatry 1984, 18, 341–351. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Conron, K.J.; Koenen, K.C.; Gilman, S.E. Childhood adversity, adult stressful life events, and risk of past-year psychiatric disorder: A test of the stress sensitization hypothesis in a population-based sample of adults. Psychol. Med. 2010, 40, 1647–1658. [Google Scholar] [CrossRef] [Green Version]
- Heleniak, C.; Jenness, J.L.; Vander Stoep, A.; McCauley, E.; McLaughlin, K.A. Childhood maltreatment exposure and disruptions in emotion regulation: A transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cognit. Ther. Res. 2016, 40, 394–415. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Llanes, J.M.; Vos, F.; Guha-Sapir, D. Measuring psychological resilience to disasters: Are evidence-based indicators an achievable goal? Environ. Health 2013, 12, 115. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; Delacorte Press: New York, NY, USA, 1990. [Google Scholar]
- Meltzer, L.J. Future directions in sleep and developmental psychopathology. J. Clin. Child Adolesc. Psychol. 2017, 46, 295–301. [Google Scholar] [CrossRef]
- Eidelman, P.; Gershon, A.; McGlinchey, E.; Harvey, A.G. Sleep and psychopathology. In The Oxford Handbook of Sleep and Sleep Disorders; Oxford Handbooks Online: Oxford, UK, 2012; pp. 172–189. [Google Scholar]
- Seelig, A.D.; Jacobson, I.G.; Donoho, C.J.; Trone, D.W.; Crum-Cianflone, N.F.; Balkin, T.J. Sleep and health resilience metrics in a large military cohort. Sleep 2008, 39, 1111–1120. [Google Scholar] [CrossRef] [Green Version]
- Tesler, N.; Gerstenberg, M.; Huber, R. Developmental changes in sleep and their relationships to psychiatric illness. Curr. Opin. Psychiatry 2013, 26, 572–579. [Google Scholar] [CrossRef]
- Haglund, M.E.; Nestadt, P.S.; Cooper, N.S.; Southwick, S.M.; Charney, D.S. Psychobiological mechanisms of resilience: Relevance to prevention and treatment of stress-related psychopathology. Dev. Psychopathol. 2007, 19, 889–920. [Google Scholar] [CrossRef] [PubMed]
- Student Well-Being & Basic Needs. CSU (2020). Available online: https://www2.calstate.edu/impact-of-the-csu/student-success/basic-needs-initiative/Pages/conference.aspx (accessed on 25 December 2020).
- Boudreau, B.; Poulin, C. An examination of the validity of the family affluence scale II (FAS II) in a general adolescent population of Canada. Soc. Indic. Res. 2009, 94, 29–42. [Google Scholar] [CrossRef]
- McFarlane, A.C. The long-term costs of traumatic stress: Intertwined physical and psychological consequences. World Psychiatry 2010, 9, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The Life Events Checklist for DSM-5 (LEC-5). National Center for PTSD, 2013. Available online: https://www.ptsd.va.gov/professional/assessment/te-measures/life_events_checklist.asp (accessed on 25 December 2020).
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and validation of a brief screening version of the childhood trauma questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Loewe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M. The patient-reported outcomes measurement information system (PROMIS). Med. Care 2007, 45, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Godin, G.; Shephard, R. Godin leisure-time exercise questionnaire. Med. Sci. Sports Exerc. 1997, 29, 36–38. [Google Scholar]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Pers. Soc. Psychol. 2003, 84, 822–848. [Google Scholar] [CrossRef] [Green Version]
- De Bruin, E.I.; Zijlstra, B.J.; van de Weijer-Bergsma, E.; Bögels, S.M. The mindful attention awareness scale for adolescents (MAAS-A): Psychometric properties in a Dutch sample. Mindfulness 2011, 2, 201–211. [Google Scholar] [CrossRef] [Green Version]
- Cyranowski, J.M.; Zill, N.; Bode, R.; Butt, Z.; Kelly, M.A.; Pilkonis, P.A.; Salsman, J.M.; Cella, D. Assessing social support, companionship, and distress: NIH toolbox adult social relationship scales. Health Psychol. 2013, 32, 293–301. [Google Scholar] [CrossRef] [Green Version]
- Shultz, J.M.; Besser, A.; Kelly, F.; Allen, A.; Schmitz, S.; Hausmann, V.; Herns Marcelin, L.; Neria, Y. Psychological consequences of indirect exposure to disaster due to the Haiti earthquake. Prehosp. Disaster Med. 2012, 27, 359–368. [Google Scholar] [CrossRef]
- Kar, N.; Krishnaraaj, R.; Rameshraj, K. Long-term mental health outcomes following the 2004 Asian tsunami disaster Long-term mental health outcomes following the 2004 Asian tsunami disaster A comparative study on direct and indirect exposure. Disaster Health 2014, 2, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Burke Harris, N. A Hidden Crisis—Findins on Adverse Childhood Experiences in California. 2020. Available online: https://www.socalgrantmakers.org/resources/hidden-crisis-findings-adverse-childhood-experiences-california (accessed on 25 December 2020).
- Wamsler, C.; Brossmann, J.; Hendersson, H.; Kristjansdottir, R.; McDonald, C.; Scarampi, P. Mindfulness in sustainability science, practice, and teaching. Sustain. Sci. 2018, 13, 143–162. [Google Scholar] [CrossRef] [Green Version]
- Wamsler, C.; Brink, E. Mindsets for sustainability: Exploring the link between mindfulness and sustainable climate adaptation. Ecol. Econ. 2018, 151, 55–61. [Google Scholar] [CrossRef]
- Hagen, C.; Lien, L.; Hauff, E.; Heir, T. Is mindfulness protective against PTSD? A neurocognitive study of 25 Tsunami disaster survivors. J. Negat. Results Biomed. 2016, 15, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Deng, Y.Q.; Li, S.; Tang, Y.Y. The relationship between wandering mind, depression and mindfulness. Mindfulness 2014, 5, 124–128. [Google Scholar] [CrossRef]
- Davidson, R.J. Mindfulness-based cognitive therapy and the prevention of depressive relapse: Measures, mechanisms, and mediators. JAMA Psychiatry 2016, 73, 547–548. [Google Scholar] [CrossRef]
- Mishra, J.; Sagar, R.; Parveen, S.; Kumaran, S.; Modi, K.; Maric, V.; Ziegler, D.; Gazzaley, A. Closed-loop digital meditation for neuro-cognitive & behavioral development in adolescents with childhood neglect. Nat. Transl. Psychiatry 2020, 10, 1–13. [Google Scholar]
- Van Susteren, L.; Al-Delaimy, W.K. Psychological impacts of climate change and recommendations. In Health of People, Health of Planet and Our Responsibility; Springer: Berlin/Heidelberg, Germany, 2020; pp. 177–192. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Primary ProximityHelp-Seeking | Primary Proximity | Secondary Proximity | χ2/H | df | n |
|---|---|---|---|---|---|---|---|
| M ± SD n (%) | M ± SD n (%) | M ± SD n (%) | |||||
| Age | 27.41 ± 9.72 | 21.72 ± 3.53 | 34.40 ± 19.41 | 93.79 *** | 2 | 725 | |
| Sex | Male | 28 (25.2) | 72 (19.9) | 102 (40.3) | 33.19 *** | 4 | 725 |
| Female | 82 (73.9) | 288 (79.8) | 151 (59.7) | ||||
| n/a | 1 (0.9) | 1 (0.3) | |||||
| Ethnicity | Caucasian | 77 (69.4) | 201 (55.7) | 130 (51.4) | 100.50 *** | 12 | 725 |
| African American | 3 (2.7) | 13 (3.6) | 3 (1.2) | ||||
| Asian | 7 (6.3) | 18 (5.0) | 72 (28.5) | ||||
| mixed/other | 13 (11.7) | 54 (14.9) | 30 (11.9) | ||||
| n/a | 11 (9.9) | 75 (21.0) | 18 (7.1) | ||||
| SES | 1.79 ± 0.63 | 2.11 ± 0.73 | 2.31 ± 0.66 | 40.63 *** | 2 | 713 | |
| n/a | 3 (2.7) | 5 (1.4) | 4 (1.6) |
| PTSD | MDD | GAD | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CI | CI | CI | ||||||||||
| β | f2 | LL | UL | β | f2 | LL | UL | β | f2 | LL | UL | |
| Age | 0.03 | 0.00 | −0.16 | 0.29 | −0.07 * | 0.03 | −0.10 | −0.04 | −0.10 * | 0.07 | −0.12 | −0.08 |
| Sex (male) | 2.96 | 0.00 | −3.09 | 8.09 | 0.32 | 0.00 | −0.72 | 1.30 | 0.99 * | 0.01 | 0.12 | 1.92 |
| Caucasian | 3.76 | 0.01 | −3.73 | 11.21 | 2.10 * | 0.01 | 0.76 | 3.33 | 1.54 * | 0.00 | 0.30 | 2.77 |
| African | 13.56 | 0.02 | −5.01 | 36.02 | 1.84 | 0.00 | −1.50 | 5.57 | 1.01 | 0.00 | −3.04 | 5.67 |
| Asian | 7.99 | 0.02 | −2.06 | 17.86 | 0.75 | 0.00 | −0.76 | 2.31 | −0.59 | 0.00 | −2.11 | 0.89 |
| mixed/other | 10.34 * | 0.03 | 0.86 | 20.19 | 3.44 * | 0.02 | 1.74 | 5.12 | 2.44 * | 0.01 | 0.85 | 4.17 |
| SES | −5.03 * | 0.04 | −8.72 | −1.31 | −1.20 * | 0.01 | −1.81 | −0.60 | −1.04 * | 0.01 | −1.62 | −0.42 |
| Not exposed | −3.88 | 0.01 | −9.60 | 2.06 | −0.26 | 0.00 | −1.19 | 0.63 | −0.40 | 0.00 | −1.24 | 0.44 |
| Indirectly exposed | 1.95 | 0.01 | −4.02 | 8.13 | 1.49 * | 0.01 | 0.48 | 2.44 | 1.24 * | 0.01 | 0.26 | 2.08 |
| Directly exposed | 9.54* | 0.06 | 3.91 | 15.53 | 1.99 * | 0.02 | 0.76 | 3.06 | 1.62 * | 0.01 | 0.53 | 2.65 |
| PTSD | MDD | GAD | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CI | CI | CI | ||||||||||
| β | f2 | LL | UL | β | f2 | LL | UL | β | f2 | LL | UL | |
| Age | −0.19* | 0.02 | −0.35 | −0.03 | −0.03 * | 0.01 | −0.04 | −0.01 | −0.06 * | 0.03 | −0.08 | −0.04 |
| Sex (male) | −0.31 | 0.00 | −5.38 | 5.15 | −0.37 | 0.00 | −1.07 | 0.36 | 0.29 | 0.00 | −0.40 | 1.00 |
| Caucasian | 2.12 | 0.00 | −4.53 | 8.88 | 2.25 * | 0.03 | 1.27 | 3.18 | 1.68 * | 0.02 | 0.74 | 2.71 |
| African | 12.26 | 0.02 | −1.55 | 27.65 | 1.36 | 0.00 | −3.02 | 5.11 | 0.77 | 0.00 | −4.16 | 5.12 |
| Asian | 3.58 | 0.00 | −5.77 | 13.57 | 1.56 * | 0.01 | 0.48 | 2.57 | −0.07 | 0.00 | −1.16 | 1.08 |
| mixed/other | 5.85 | 0.01 | −4.05 | 16.13 | 2.38 * | 0.02 | 1.04 | 3.73 | 1.25 | 0.01 | −0.23 | 2.69 |
| SES | −0.26 | 0.01 | −4.03 | 3.33 | −0.30 | 0.00 | −0.74 | 0.20 | −0.34 | 0.00 | −0.84 | 0.17 |
| Not exposed | −1.66 | 0.00 | −6.66 | 3.32 | 0.00 | 0.00 | −0.72 | 0.67 | −0.14 | 0.00 | −0.83 | 0.58 |
| Indirectly exposed | 0.48 | 0.00 | −4.20 | 5.40 | 0.54 | 0.00 | −0.18 | 1.28 | 0.44 | 0.00 | −0.30 | 1.18 |
| Directly exposed | 6.97 * | 0.04 | 1.53 | 12.50 | 0.94 * | 0.01 | 0.11 | 1.81 | 0.64 | 0.00 | −0.31 | 1.56 |
| Childhood Trauma | 9.04 * | 0.22 | 5.38 | 12.64 | 2.00 * | 0.13 | 1.28 | 2.76 | 1.17 * | 0.03 | 0.48 | 1.85 |
| Resilience | −1.22 * | 0.16 | −1.73 | −0.69 | −0.25 * | 0.14 | −0.32 | −0.17 | −0.28 * | 0.12 | −0.35 | −0.20 |
| Sleep Disturbances | 0.54 * | 0.05 | 0.07 | 1.01 | 0.27 * | 0.23 | 0.21 | 0.33 | 0.16 * | 0.05 | 0.10 | 0.22 |
| Exercise | −0.03 | 0.01 | −0.07 | 0.03 | −0.01 * | 0.02 | −0.01 | −0.00 | −0.00 | 0.01 | −0.01 | 0.00 |
| Mindfulness | −0.59 | 0.01 | −3.65 | 2.16 | −1.57 * | 0.16 | −1.96 | −1.21 | −1.67 * | 0.12 | −2.08 | −1.27 |
| Emotional Support | −0.29 | 0.00 | −0.64 | 0.06 | −0.05 | 0.04 | −0.09 | −.00 | −0.04 | 0.01 | −0.09 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, S.; Kornbluh, M.; Withers, M.C.; Grennan, G.; Ramanathan, V.; Mishra, J. Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire. Int. J. Environ. Res. Public Health 2021, 18, 1487. https://doi.org/10.3390/ijerph18041487
Silveira S, Kornbluh M, Withers MC, Grennan G, Ramanathan V, Mishra J. Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire. International Journal of Environmental Research and Public Health. 2021; 18(4):1487. https://doi.org/10.3390/ijerph18041487
Chicago/Turabian StyleSilveira, Sarita, Mariah Kornbluh, Mathew C. Withers, Gillian Grennan, Veerabhadran Ramanathan, and Jyoti Mishra. 2021. "Chronic Mental Health Sequelae of Climate Change Extremes: A Case Study of the Deadliest Californian Wildfire" International Journal of Environmental Research and Public Health 18, no. 4: 1487. https://doi.org/10.3390/ijerph18041487