
A Systematic Review on Cross-Cultural Comparative Studies of Sleep in Young Populations: The Roles of Cultural Factors


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Study Screening and Data Extraction
2.4. Quality Assessment
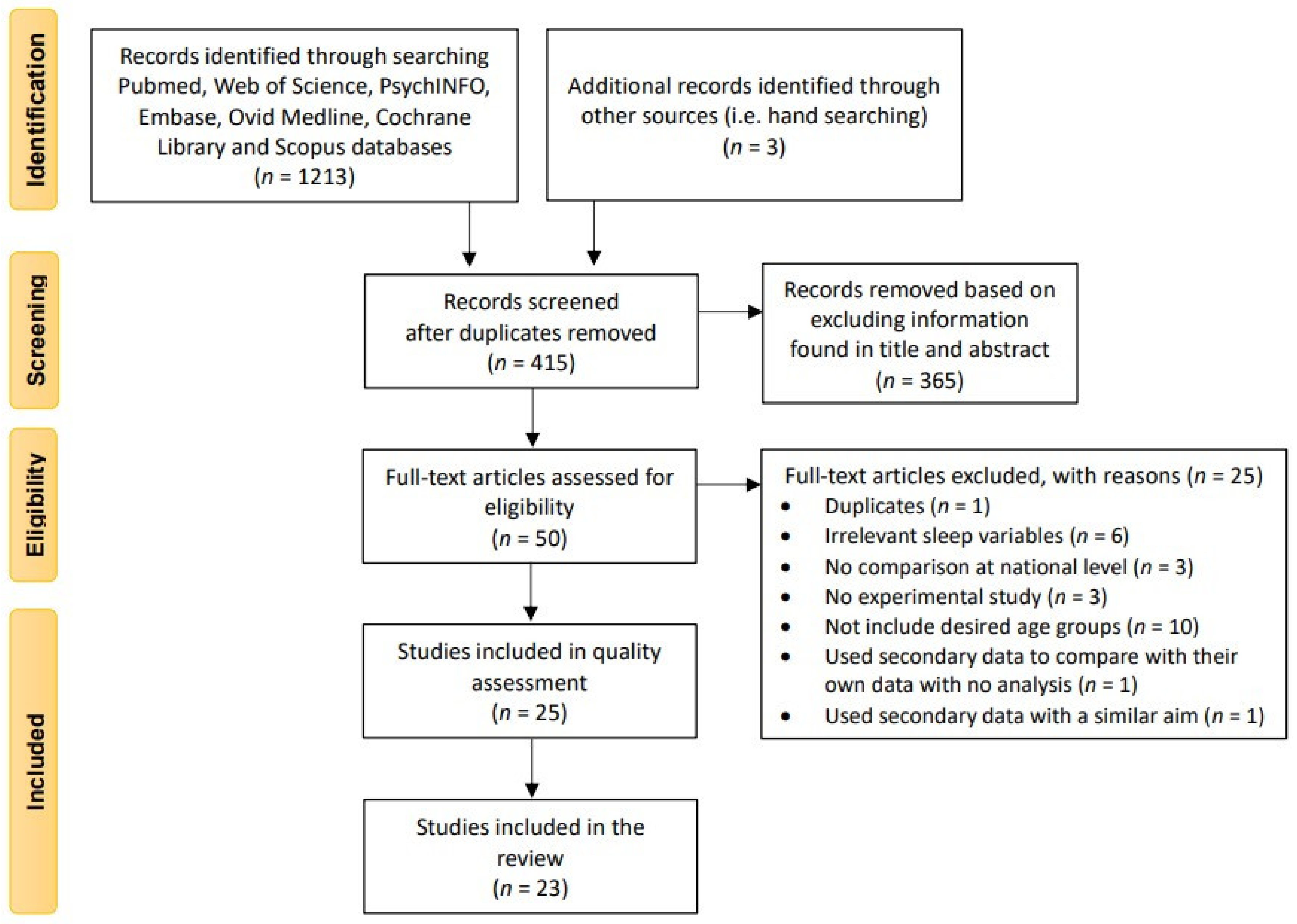
2.5. Search Results
3. Results and Discussion
3.1. Sleep Duration and Disturbances
3.1.1. Summary
- In general, children from Europe, North America and Australasia were more likely to have an earlier bedtime, earlier wake up time and longer nocturnal sleep duration than children in Asia and the Middle East region.
- Infants in Asia were more likely to have more frequent and longer habitual naps than other countries.
- Parents from countries in Asia reported more sleep disturbances in their infants and children than those from Europe, North America and Australasia, including nocturnal awakenings, bedtime resistance, sleep latency and general sleep problems.
- Cultural differences in sleep duration and disturbances were found between countries within the same region, however results were varied.
- Most studies used parent-reported questionnaires (Children’s Sleep Habits Questionnaire; CSHQ and the Brief Infant Sleep Questionnaire; BISQ).
- Discrepancies were identified between actigraphy and parent/self-report sleep data for nocturnal sleep duration and sleep quality.
- Most studies included typically developing children, one study included children with Autism Spectrum Disorder (ASD).
3.1.2. Sleep Duration: Bedtime, Wake Up Time, Nocturnal Sleep Duration, Habitual Naps and Total Sleep Time
3.1.3. Sleep Disturbances: Nocturnal Awakenings, Bedtime Resistance, Sleep Latency, Sleep Problems, Daytime Sleepiness, and Sleep Quality
3.2. Cultural Factors: Child, Parent and Environmental Factors Associated with Sleep
3.2.1. Summary
3.2.2. Methodological Variability of Studies and the Identification of Culturally Relevant Factors
3.2.3. Child Variables Associated with Sleep
- Universal factors included unhealthy diet, poor emotional and cognitive status, and a preference for eveningness, which were all negatively associated with child and adolescent sleep duration and disturbances consistently across multiple countries.
- Cultural factors included poor psychological health (e.g., pressure from home and being easily scared), physical activities and screen time, and these were all negatively associated with child and adolescent sleep duration and disturbances and differed between countries.
- Studies that controlled for other factors (e.g., country, time spent playing outdoors and extracurricular activities) when examining the relationship between child factors and sleep duration or disturbances, did not find significant relationships between nocturnal sleep duration, child weight, and extracurricular activities.
- Physical health-related factors: physiological status at bedtime, diet and obesity.
3.2.4. Parent Variables Associated with Sleep
- Universal factors included bedtime routine, parental warmth, and maternal sleep which were all positively associated with children and adolescents’ sleep duration and disturbances consistently across multiple countries.
- Cultural factors included parental education level which was associated with parent’s perception on children’s sleep disturbances and differed between countries.
- Parenting practices: bedtime routines, bedtime rituals and parental warmth.
3.2.5. Environmental Variables Associated with Sleep
- The number of family members was associated with children and adolescents’ sleep duration and disturbances across multiple countries.
- Cultural factors included presence of siblings, co-sleeping or falling asleep alone, and maternal employment status, which were all associated with children and adolescents’ sleep duration and disturbances and differed between countries.
- Studies that controlled for other factors (e.g., country, time spent playing outdoors and extracurricular activities) when examining the relationship between environmental factors and sleep duration, did not find significant relationships between nocturnal sleep duration, and school start/finish time, season and daylight duration. This may represent that the effect of other factors (e.g., country) are significant in these relationships.
- Family composition: the number of siblings and family members in one household.
4. Conclusions and Considerations for Future Research
4.1. Cultural Considerations for Measuring Sleep
4.2. Comparisons between Countries in Larger Regional Areas
4.3. The Consideration of Other Cultural Factors
4.4. Identifying “True” Cultural Factors
4.5. Scope for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Criterion | Latz et al. [23] | Iwawaki & Schuller [16] | LeBourgeois et al. [30] | Liu et al. [31] | Mindell et al. [17] | Mindell et al. [42] | Hense et al. [32] | Kohyama et al. [33] | Sadeh et al. [24] | Dewald et al. [25] | Mindell et al. [34] | Short et al. [35] | Varzsonyl et al. [26] | Chaput et al. [43] | Mindell et al. [44] | Mindell et al. [45] | Ahn et al. [36] | Biggs et al. [37] | Irwanto et al. [41] | Tynjälä et al. [27] | Mindell et al. [38] | Takahashi et al. [39] | Carneiro et al. [28] | Daban & Goh [40] | van Selms et al. [29] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clearly focused question | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Appropriate design | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Clearly defined recruitment | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sample size based on a power calculation a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a |
| Outcome measurements valid and reliable | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✕ |
| Exposure measurements valid and reliable | ✕ | ✓ | ✓ | n/a | p | p | p | p | p | n/a | p | ✕ | ✕ | p | p | ✓ | p | ✕ | n/a | ✕ | ✓ | ✕ | ✕ | ✓ | ✕ |
| Confounding factors accounted | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✕ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ |
| Appropriate statistical analysis | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Precise estimate of effect | ✕ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✕ | ✓ | ✓ | ✕ | ✓ | ✓ |
| Reliable results with acknowledged possible bias | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Ability to generalize results | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✓ | ✕ | ✕ | ✕ |
| Interpretation related to the existing evidence | ✓ | ✕ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Overall Methodological Quality | L | L | M | M | M | M | H | M | L | L | M | M | L | M | M | M | M | M | M | L | M | M | L | M | L |
Appendix B
| Authors (Year) | Included Countries | Ages (Mean)/ Gender (% of Male Participants) | Cultural Factor Domains | Detailed Results | ||
|---|---|---|---|---|---|---|
| Child | Parent | Environmental | ||||
| Latz et al. (1999) [23] | Japan (n = 56) | 6–47 months (M = 30.3)/ 72% | not measured | Parental education level, sleep initiating and resuming methods | Number in household, maternal employment, co-sleeping in body contact, adult company at bedtime | Parental Differences in parental factors between countries - Mother’s education (years): American (14.2) < Japanese (14.6) - Father’s education (years): American (14.6) < Japanese (16.0) *** - Sleep initiating and resuming methods: Bottle in bed: Japanese (9%) < American (20%) Body contact when children woke at night: Japanese (9%) < American (61%) ** Environmental Differences in environmental factors between countries - No. in household: American (4.1) < Japanese (4.2) - Mother employed outside home: Japanese (20%) < American (26%) - Co-sleeping (in body contact, ≥3 a week): American (15%) < Japanese (59%) *** - Adult company at bedtime: American (16%) < Japanese (68%) *** Associations between co-sleeping and sleep disturbances in each country US: Co-sleeping with body contact was associated with more bedtime protests,*** night awakenings** and overall stressful sleep problems.** Japan: Co-sleeping with body contact was only associated with increased night awakenings.* |
| US (n = 61) | 6–47 months (M = 25.0)/ 67% | |||||
| LeBourgeois et al. (2005) [30] | Italy (n = 776) | 12–17 years (M = 14.6y) /55.4% | Physiologically sleep-inhibiting, cognitive and emotional status at bedtime, circadian preference, puberty | Bedtime routine | SES, Bed/bedroom sharing | Child Differences in child factors between countries - Physiological status (Score): American (3.9) < Italian (4.7) *** - Cognitive status (score): American (3.3) < Italian (4.0) *** - Emotional status (score): American (4.2) < Italian (4.7) *** - Circadian preference (Morning/Eveningness scale score): American (26.0) < Italian (26.3) - Pubertal status (Pubertal Developmental Scale score): Italian (3.1) < American (3.2) Associations with sleep disturbances in each country - Physiologically sleep-inhibiting status was not significantly associated with the sleep quality of adolescents in the U.S. and Italy. - Better cognitive status had a significantly positive association with sleep quality of adolescents in the U.S. and Italy.*** - Better emotional status had a significantly positive association with sleep quality of adolescents in the U.S. and Italy.*** - Morningness was associated with significantly better overall sleep quality than eveningness in adolescents in the U.S. and Italy.*** - Pubertal status was not significantly associated with the sleep quality of adolescents in the U.S. and Italy Parental Differences in parental factors between countries Bedtime routine (score): American (3.9) < Italian (4.1) Associations between bedtime routine and sleep disturbances in each country Bedtime routine was not associated with the sleep quality of adolescents in the U.S. and Italy. Environmental Differences in environmental factors between countries - SES (head of household’s occupation on a scale of 1 (unskilled) to 9 (professional)): Italian (4.5) < American (5.1) *** - No bed/bedroom sharing (score): Italian (4.5) < American (5.1) *** Associations with sleep disturbances in each country - SES was not significantly associated with sleep quality in both adolescents in the U.S. and Italy. - Bed/Bedroom sharing US: Bed/bedroom sharing was significantly associated with less success in maintaining and reinitiating sleep.*** Italy: Significant association was not shown. |
| US (n = 572) | 12 to 17 years (M = 14.6y) /41.2% | |||||
| Mindell et al. (2010) [17] | 17 countries (n = 29,287) divided into | not measured | Maternal education level, bedtime routine | Sleeping location, maternal employment | Parental Differences in parental factors between countries - Maternal education level *** Elementary school (%): P-A (1.05) < P-C (1.43) High school (%): P-A (39.31) < P-C (42.45) College (%): P-C (38.15) < P-A (42.76) Postgraduate (%): P-A (16.88) < P-C (17.97) - Consistent bedtime routine (%): P-C (60.65) < P-A (71.13) **** Environmental Differences in environmental factors between countries - Sleeping Location Sleep in parent’s bed: P-C (11.8%) < P-A (64.65%) **** Sleep in parent’s room: P-C (21.95%) < P-A (86.47%) **** Sleep in own room: P-A (7.03%) < P-C (62.54%) **** - Mother’s employment status *** Full time (%): P-C (29.86) < P-A (60.41) Part time (%): P-A (4.86) < P-C (15.36) Home/student (%): P-A (34.73) < P-C (54.7) Controlling sleep location examining differences in sleep duration and disturbances between countries - Significant differences in sleep duration and disturbances between P-C and P-A countries were maintained, except for the longest period of consolidated sleep.*** | |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported)/52.5% | |||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/51.9% | |||||
| Mindell et al. (2010) [42] | 17 countries (n = 29,287) divided into P-C countries (n = 7960; AU, CA, NZ, US, UK) and P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/51.9% (for entire sample) | not measured | Sleep initiating and resuming method | Sleeping location | Parental Differences in parental factors between countries - Sleep initiation methods Bottle-feeding (%): P-C (16.01) < P-A (37.25) **** Nursing (%): P-C (19.74) < P-A (28.07) **** Rocking (%): P-C (20.69) < P-A (23.50) **** Holding (%): P-A (26.11) < P-C (26.63) Watching TV (%): P-C (4.41) < P-A (6.85) - Sleep resuming methods Holding or rocking to sleep (%): P-C (21.09) < P-A (28.77) **** Picking up—returning awake (%): P-A (5.18) < P-C (18.47) **** Rub or pat in crib/bed (%): P-C (28.51) < P-A (31.89) **** Giving a bottle (%): P-C (21.07) < P-A (33.61) **** Nurse back to sleep (%): P-C (25.00) < P-A (29.30) **** Verbal comfort in crib (%): P-A (13.06) < P-C (15.95) **** Bring child to parents’ bed (%): P-A (7.46) < P-C (19.37) **** Let cry to fall asleep (%): P-A (1.97) < P-C (15.65) **** Wait a few minutes (%): P-A (21.30) < P-C (45.53) **** Play until ready for sleep (%): P-C (1.22) < P-A (5.58) **** Watch TV or video (%): P-A (1.03) < P-C (1.39) Sing to child (%): P-C (8.74) < P-A (11.98) **** Environmental Differences in environmental factors between countries - Sleeping location In crib/bed alone in the room: P-A (3.58%) < P-C (56.98%) **** In parent’s bed alone: P-C (2.00%) < P-A (5.50%) **** In crib/bed with parent present: P-A (11.91%) < P-C (12.45%) In parents’ bed with parent: P-C (10.99%) < P-A (38.41%) **** In another room of the house: P-A (2.30%) < P-C (5.01%) **** Associations between falling asleep alone and, sleep duration and disturbances in each country P-C: falling asleep alone in own crib/bed was a predictor for longer nocturnal sleep, fewer night awakenings and longest continuous sleep episode. P-A: Sleep duration and disturbances were not predicted. |
| Hense et al. (2011) [32] | 8 European countries (n = 31,543) including | 2–9 years | Overweight, playing outdoors, time spent in front of TV or PC | Parental education level | Daylight, season | Child Associations with sleep duration after controlling for other cultural factors - Overweight: Overweight had a significantly positive association with sleep duration,*** but the association was disappeared after controlling for other factors (e.g., age, parental education level, country, season, daylight hours, screen time and time playing outside). - Playing outdoors: Playing outdoors had a significantly positive association with sleep duration,*** but the association was disappeared after controlling for other factors (e.g., age, parental education level, country, season, daylight hours, overweight and screen time). - Screen time (Time spent in front of TV or PC): Screen time had a significantly negative association with sleep duration,*** but the association was disappeared after controlling for other factors (e.g., age, parental education level, country, season, daylight hours, overweight and time playing outside). Parental Associations with sleep duration after controlling for other cultural factors - Parental education level: Children with medium or low parental education level were more likely to have shorter nocturnal sleep duration than those with high parental education level.*** However, the association was disappeared when other factors were controlled (e.g., age, country, season and daylight hours) Environmental Associations with sleep duration after controlling for other cultural factors - Daylight: Longer daylight hours was significantly associated with shorter duration of sleep.*** However, the association was disappeared when other factors were controlled (e.g., age, parental education level, country, seasons, overweight, screen time and time playing outdoors). - Season: Fall/winter was significantly associated with longer duration of sleep than spring/summer*** However, the association was disappeared when other factors were controlled (e.g., age, parental education level, country and daylight hours). |
| Estonia (n = 1331) | (M = 5.8 y)/48.9% | |||||
| Italy (n = 1643) | (M = 6.2 y)/52.0% | |||||
| Hungary (n = 902) | (M = 6.7 y)/49.2% | |||||
| Cyprus (n = 953) | (M = 6.3 y)/49.4% | |||||
| Spain (n = 504) | (M = 5.5 y)/42.4% | |||||
| Sweden (n = 1215) | (M = 5.7 y)/51.7% | |||||
| Germany (n = 1586) | (M = 6.1 y)/51.5% | |||||
| Belgium (n = 408) | (M = 5.5 y)/52.5% | |||||
| Kohyama et al. (2011) [33] | Japan (n = 872) | Birth–3 years (mean not reported)/48.6% | not measured | Bedtime routine | Sleeping location, parental presence at bedtime | Parental Differences in parental factors between countries - Consistent bedtime routine (%): Other Asian countries (60.13) < Japan (72.71).*** Environmental Differences in environmental factors between countries - Sleeping location Parent’s bed: Other Asian countries (64.43%) < Japan (69.72%) Parent’s room: Other Asian countries (86.40%) < Japan (88.07%) Own room: Japan (2.98%) < Other Asian countries (7.20%) *** Parental presence at bedtime: Japan (97.80%) < Other Asian countries (99.56%) *** |
| 11 Asian countries including CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH and VN (n = 20,455) | Birth–3 years (mean not reported)/48.1% | |||||
| Sadeh et al. (2011) [24] | 17 countries (n = 29,287) divided into P-C countries (n = 7960; AU, CA, NZ, US, UK) and P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/48.1% (for entire sample) | not measured | Maternal education level | Presence of siblings, maternal employment | Parental The impact of maternal education level on sleep disturbances in each country P-A: Maternal education level had a significant effect on the parental definition of “severe sleep problems”.**** Parents with lower education level were less likely to define their child’s sleep as a severe sleep problem. P-C: Significant effect of maternal education level was not shown. Environmental The impact of environmental factors on sleep disturbances in each country - Maternal employment P-A: Mother’s employment had a significant effect on the parental definition of “severe sleep problems”.**** Mothers with higher employment level were more likely to define their child’s sleep as a severe sleep problem. P-C: Significant effect of maternal employment was not shown. - Presence of siblings (only child vs. other children) P-A: Presence of siblings had a significant effect on the parental definition of “severe sleep problems”.**** This indicated that only child’s sleep was less likely to be defined as a severe sleep problem than those with siblings. P-C: Significant effect of the presence of siblings was not shown. |
| Mindell et al. (2013) [34] | 17 countries (n = 2590) divided into | Daily outdoor time, Screen time (i.e., television viewing, using a computer, playing other electronic games) | Bedtime routine, maternal education level | Maternal employment, sleeping location | Child Differences in child factors between countries - Daily outdoor time: P-C (2.30 h) < P-A (3.79 h) *** - Screen time (television viewing, using a computer, playing other electronic games): P-C (2.21 h) < P-A (2.47 h) *** Overall associations with sleep duration and disturbances - Daily outdoor time showed a significantly positive association with bedtime and daytime sleep, and negative association with night-time sleep *** - Screen time showed a significantly positive association with bedtime, wake up time, sleep onset latency, number of night awakenings and night-time sleep *** Parental Differences in parental factors between countries (Sleeping location) - Bedtime routine: P-A (62.2%) < P-C (87.3%) **** - Maternal education level: No significant differences Elementary school (%): P-C (0.4) < P-A (0.5) High school (%): P-A (36.2) < P-C (37.5) College (%): P-C (43.0) < P-A (46.2) Postgraduate (%): P-A (17.1) < P-C (19.1) Overall associations between bedtime routine and sleep duration and disturbances - The frequency of a consistent bedtime routine showed significantly positive associations with night-time sleep and total sleep time whereas negative associations with bedtime, sleep onset latency, number of night awakenings, wake up time and daytime sleep were found *** Environmental Differences in environmental factors between countries - Maternal employment status **** Full time (%): P-C (27.7) < P-A (45.4) Part time (%): P-A (8.6) < P-C (21.6) Home/student (%): P-A (46.0) < P-C (50.7) - Sleeping location Own room (%): P-A (10.1) < P-C (79.5) **** Own bed (%): P-A (28.1) < P-C (90.6) **** Controlling sleeping location examining differences in sleep duration and disturbances between countries - Significant differences in sleep patterns between P-C and P-A countries were maintained after controlling for sleeping location, except for sleep onset latency.*** | |
| P-C countries (n = 1139; AU, NZ, CA, US, UK) | 3–6 years (mean not reported) /49.8% | |||||
| P-A countries (n = 1447; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | 3–6 years (mean not reported) /50.2% | |||||
| Short et al. (2013) [35] | Australia (n = 385) | 13–18 years (M = 15.57 y) / 60% | School start time, Extracurricular load, Circadian preference | Parent-set bedtime | not measured | Child Differences in child factors between countries - School Start time: American (7:45 am) < Australian (8:32 am) *** - Extracurricular load (hours): Australian (8.12) < US (13.4) *** Extracurricular load includes part-time work, sport, other activities and homework. Part-time work (hours): Australian (1.51) < US (3.25) *** Sport (hours): US (2.17) < Australian (2.27) Other activities (hours): Australian (0.51) < US (1.54) *** Homework (hours): Australian (4.17) < US (6.52) *** - Circadian preference (Smith Morningness/Eveningness Questionnaire score): Australian (33.25) < American (33.94) Controlling countries examining the impact of child factors on sleep duration - School start time had the largest effect on sleep duration *** For every hour earlier school start time, adolescents had an average of 29 min less sleep per night. This significant effect was disappeared after controlling for countries. - Extracurricular load was significantly associated with sleep duration per night.** Adolescents had 4 min less sleep per night with every hour spent per day on extracurricular activities. The significant relationship between extracurricular load and sleep duration was disappeared after controlling for countries.** Parental Differences in parental factors between countries - Parent-set bedtime: American (6.8%) < Australian (17.5%) *** Controlling countries examining the impact of parental factors on sleep duration - Adolescents gained 24 min of sleep per night if they had a parent-set bedtime. The significant relationship between parent-set bedtime and sleep duration was maintained after controlling for the country.** |
| US (n = 302) | 13–19 years (M = 16.03 y) /35% | |||||
| Chaput et al. (2015) [43] | 12 countries (n = 5777) including | 9–11 years | Diet, physical activity, screen time (i.e., hours of watching TV, playing video games and using computer) | not measured | not measured | Child-related Overall associations with sleep duration and disturbances - Healthy/unhealthy diet: Unhealthy diet was associated with a later bedtime,*** a shorter sleep duration* and poorer sleep efficiency*** after controlling for covariates (e.g., age, gender, highest parental education and body mass index), but a healthy diet was only associated with an earlier bedtime.** The relationships were similar across sites, but not specified. - Physical activity: Moderate-to-vigorous physical activity was negatively associated with bedtime,**** sleep duration,**** and sleep efficiency **** after controlling for covariates **** Associations between sleep duration or disturbances (duration, efficiency and bedtime) and moderate-to-vigorous physical activity were different between study sites, but data are not shown. - Screen time: Screen time (i.e., hours of watching TV, playing video games and using a computer) was positively associated with bedtime after controlling for covariables (e.g., age, gender, highest parental education and body mass index) **** Screen time was also negatively associated with sleep quality, but the significant association was disappeared after controlling for covariables. No significant association was shown between screen time and nocturnal sleep duration. Associations between sleep duration or disturbances (duration, efficiency and bedtime) and screen time were different between study sites, but data were not shown. |
| Australia (n = 433) | (M = 10.7 y)/46.7% | |||||
| Canada (n = 496) | (M = 10.5 y)/40.9% | |||||
| China (n = 459) | (M = 9.9 y)/51.6% | |||||
| India (n = 433) | (M = 10.5 y)/45.1% | |||||
| UK (n = 374) | (M = 10.9 y)/42.8% | |||||
| US (n = 421) | (M = 9.9 y)/40.4% | |||||
| Brazil (n = 435) | (M = 10.5 y)/48.5% | |||||
| Colombia (n = 820) | (M = 10.5 y)/49.2% | |||||
| Finland (n = 526) | (M = 10.4 y)/45.3% | |||||
| Kenya (n = 452) | (M = 10.2 y)/45.4% | |||||
| Portugal (n = 563) | (M = 10.4 y)/41.6% | |||||
| South Africa (n = 452) | (M = 10.2 y)/38.6% | |||||
| Mindell et al. (2015) [44] | 13 countries including AU/NZ, CA, UK, US, CN, HK, IN, JP, KR, MY, PH, SG and TH (n = 10085) | Birth–5.11 years (mean not reported)/49.6% (for entire sample) | not measured | Bedtime routine | not measured | Parental Differences in parental factors between countries - Bedtime routine: P-A (64.4%) < P-C (82.6%) **** Overall associations between bedtime routine and sleep disturbances - Children with a consistent bedtime routine have earlier bedtimes, shorter sleep onset latency, more night-time sleep, fewer and shorter duration of night awakenings, and more total sleep per 24 h *** |
| Mindell et al. (2015) [45] | 13 countries (n = 10085) including | not measured | Maternal education level, Maternal sleep | Number of children, Maternal employment | Parental Differences in parental factors between countries - Maternal education level **** Elementary school (%): P-A (0.4) < P-C (0.5) High school (%): P-A (33.5) < P-C (34.3) College (%): P-C (43.9) < P-A (49.1) Postgraduate (%): P-A (17.2) < P-C (21.4) Overall association between maternal sleep and sleep duration and disturbances - Maternal sleep was positively associated with children’s bedtime, wake up time, number of night awakenings and nocturnal sleep duration and the stronger relationship was shown in younger children *** Environmental Differences in environmental factors between countries - The number of children: No significant differences 1–P-A (53.9%) < P-C (54.3%) 2–P-A (32.6%) < P-C (33.7%) 3+–P-C (12.1%) < P-A (13.4%) - Maternal employment status **** Full time (%): P-C (27.0) < P-A (48.3) Part time (%): P-A (5.7) < P-C (17.6) Home/student (%): P-A (46.0) < P-C (55.4) | |
| P-C countries (n = 4152; AU/NZ, CA, UK, US) and | Birth–6 years (mean not reported)/50.7% | |||||
| P-A countries (n = 5933; CN, HK, IN, JP, KR, MY, PH, SG and TH) | Birth–6 years (mean not reported)/50.2% | |||||
| Vazsonyi et al. (2015) [26] | Swiss (n = 5575) | 15–18 years (M = 17.17)/ 50.0% | not measured | Parental warmth | not measured | Parental Associations between parental warmth and sleep duration and disturbances in each country - Both Swiss and Georgia: Parental warmth had a significantly positive correlation with sleep quality and sleep quantity. |
| Georgia (n = 6692) | 15–18 years (M = 15.83)/ 40.0% | |||||
| Biggs et al. (2016) [37] | Australia (n = 87) | 5–12 years (M = 9.6 y) /58% | not measured | Maternal education level | Season, Daylight amount | Parental Differences in parental factors between countries - Maternal education level < 11 Years schooling (%): No significant differences Australia (16) = Canada (16) High school Graduate (%): Australia (22) < Canada (27) College/University (%): Australia (22) < Canada (24) University Graduate (%): Canada (32) < Australia (37) Unknown (%): Australia (3) < Canada (1) Environmental Differences in environmental factors between countries - Seasons of study: No significant differences Spring: Canada (15%) < Australia (20%) Summer: Australia (23%) < Canada (26%) Fall: Australia (18%) < Canada (32%) Winter: Canada (28%) < Australia (39%) - Daylight duration: Australia (11:50) < Canada (11:55) |
| Canada (n = 101) | 5–12 years (M = 9.0 y) /56% | |||||
| Mindell et al. (2017) [38] | ME countries (n = 669; Saudi Arabia, Egypt, Algeria, United Arab Emirates, Jordan, Morocco, Iraq, Kuwai, Oman, Palestinian territories, Libyan Arab Jamahiriya, Bahrain, Israel and 83 from other Arab countries) | Birth–3 years (mean not reported) /50.2% | not measured | Bedtime routine | not measured | Parental Differences in parental factors between countries - Bedtime routine (5+ times/week): ME (46.79%) < PA (61.65%) < PC (71.13%) *** Overall associations between bedtime routine and sleep duration and disturbances - The frequency of a consistent bedtime routine had a significantly negative correlation with bedtime, sleep onset latency, number of night awakenings and duration of night awakenings, while positive correlation with nocturnal sleep and total sleep duration *** |
| P-C and P-A countries from Mindell et al. (2010; n = 29,287) [15] | Birth–3 years (mean not reported) /51.94% | |||||
| Takahashi et al. (2018) [39] | Japan (n = 505) | 4–5 years (mean not reported) /47.3% | not measured | Parental education level | Family structure, Number of siblings | Parental Differences in parental factors between countries - Maternal education level *** Middle school or below (%): Japan (4.6) < China (13.9) High school (%): China (21.7) < Japan (74.4) Undergraduate or above (%): Japan (21.0) < China (64.4) - Paternal education level *** Middle school or below (%): Japan (5.9) < China (12.0) High school (%): China (20.8) < Japan (65.5) Undergraduate or above (%): Japan (28.6) < China (67.2) Environmental Differences in environmental factors between countries - Family structure: No significant differences Nuclear family: China (56.2%) < Japan (61.2%) Extended family: Japan (35.6%) < China (40.2%) Single parent or other: Japan (3.2%) < China (3.6%) - The number of siblings *** Only child: Japan (16.2%) < China (82.5%) Not the only child: China (17.5%) < Japan (83.8%) |
| China (n = 1909) | 4–5 years (mean not reported) /53.0% | |||||
| Carneiro et al. (2019) [28] | Cape Verde (n = 206) | 2–15 years (mean not reported) /46% | Bedtime television | Parental education level | Number of cohabitants, number of cohabitant children | Child Associations between bedtime screen time and sleep disturbances in each country - Bedtime screen time (Fell asleep while watching TV): Mozambique: Bedtime screen time had a significantly positive association with children’s CSHQ scores*** showing that MZ children who “sometimes” watching TV at bedtime had approximately 12% higher CSHQ scores than children who “rarely” watching TV at bedtime. On the other hand, children who “usually” watch TV at bedtime had approximately 7% higher CSHQ scores than children who “rarely” watching TV at bedtime. Cape Verde: Significant association was not shown. Parental Differences in parental factors between countries Mother education (<10 years, %): Mozambique (6%) < Cape Verde (74%) *** Mother education (≥10 years, %): Cape Verde (26%) < Mozambique (94%) *** Father education (<10 years, %): Mozambique (8%) < Cape Verde (68%) *** Father education (≥10 years, %): Cape Verde (32%) < Mozambique (92%) *** Associations between parental education level with sleep disturbances in each country - Maternal education level Cape Verde: Mothers’ educational level had a significant association with the CSHQ scores, showing that children whose mothers have more than 9 years of education had approximately 7% lower CSHQ scores. Mozambique: Significant association was not shown. - Paternal education level Mozambique: Fathers’ educational level had a significant association with the CSHQ scores,* showing that children whose fathers have more than 11 years of education had approximately 4% lower CSHQ scores* than children whose fathers have less than 10 years of education. Cape Verde: Significant association was not shown. Environmental Differences in family factors between countries - The number of cohabitant children *** (< 3): Cape Verde (58%) < Mozambique (80%) (≥ 3): Mozambique (20%) < Cape Verde (42%) *** - The number of cohabitants in family *** (< 5): Cape Verde (37%) < Mozambique (70%) (≥ 5): Mozambique (30%) < Cape Verde (63%) Associations between environmental factors with sleep disturbances in each country - The number of cohabitants children Both Cape Verde and Mozambique: Number of cohabitant children did not have a significant association with CSHQ scores (overall sleep problems) - The number of cohabitants in family Both Cape Verde and Mozambique: Number of cohabitants in the family did not have a significant association with CSHQ scores (overall sleep problems) |
| Mozambique (n = 438) | 4–13 years (mean not reported) /49% | |||||
| Daban & Goh (2019) [40] | 6 Southeast Asia countries (n = 5987) including | Birth–3 years | not measured | Bedtime routine | Sleeping location | Parental Differences in parental factors between countries Consistent bedtime routine: PH (52.03) < ML (52.75) < SG (59.74) < ID (65.66) < VT (71) < TH (71.46) **** Environmental Differences in environmental factors between countries - Sleeping location Own room (%): TH (1.01) < VT (2.1) < PH (6.58) < ML (8.53) < ID (9.72) < SG (19.28) **** Parent’s room (%): SG (73.73) < ID (81.9) < ML (84.05) < PH (86.56) < VT (94.3) < TH (94.54) **** Parent’s bed: SG (35.86) < ML (44.03) < PH (65.09) < ID (70.73) < TH (77.23) < VT (83.2) **** |
| Indonesia (n = 967) | (mean not reported) /50.2% | |||||
| Malaysia (n = 997) | (mean not reported) /50.4% | |||||
| Philippines (n = 1034) | (mean not reported) /49.8% | |||||
| Singapore (n = 1001) | (mean not reported) /51.6% | |||||
| Thailand (n = 988) | (mean not reported) /49.2% | |||||
| Vietnam (n = 1000) | (mean not reported) /49.4% | |||||
| van Selms et al. (2019) [29] | Netherland (n = 1131) | 7–12 years (M = 10.0) /44.6% | Pressure from home, Pressure from school, Easily scared, Worried | not measured | not measured | Child Differences in child factors between countries - Pressure from home (%): Indonesia (16.5) < The Netherlands (21.8) < Armenia (24.0) ** - Pressure from school (%): Indonesia (22.4) < The Netherland (23.9) < Armenia (31.4) ** - Easily scared (%): The Netherlands (27.0) < Indonesia (58.3) < Armenia (62.7) ** - Worried (%): The Netherland (46.7) < Armenia (49.3) < Indonesia (60.0) ** Associations between child factors with sleep disturbances in each country - Pressure from home Netherland and Indonesia: Children who experience pressure from the home situation, are more likely to have parental-reported SB. Armenia: Significant correlation was not shown - Pressure from school All countries: No association between pressure from school and parent-reported SB was shown. - Easily scared Netherland and Armenia: Children, who are easily scared, are more likely to have parent-reported SB. Indonesia: Significant correlation was not shown. - Worried All countries: No association between worried and parent-reported SB was shown. |
| Armenia (n = 886) | 7–12 years (M = 9.1) /49.0% | |||||
| Indonesia (n = 545) | 7–12 years (M = 9.5) /41.5% | |||||
| 7 | 17 | 13 | ||||
References
- Astill, R.G.; Van Der Heijden, K.B.; Van Ijzendoorn, M.H.; Van Someren, E.J.W. Sleep, cognition, and behavioral problems in school-age children: A century of research meta-analyzed. Psychol. Bull. 2012, 138, 1109–1138. [Google Scholar] [CrossRef]
- Maasalo, K.; Fontell, T.; Wessman, J.; Aronen, E.T. Sleep and behavioural problems associate with low mood in Finnish children aged 4-12 years: An epidemiological study. Child Adolesc. Psychiatry Ment. Health 2016, 10, 37. [Google Scholar] [CrossRef] [Green Version]
- Shanahan, L.; Copeland, W.E.; Angold, A.; Bondy, C.L.; Costello, E.J. Sleep Problems Predict and Are Predicted by Generalized Anxiety/Depression and Oppositional Defiant Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Snell, E.K.; Adam, E.K.; Duncan, G.J. Sleep and the Body Mass Index and Overweight Status of Children and Adolescents. Child Dev. 2007, 78, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Arguelles, L.; Jiang, F.; Chen, W.; Jin, X.; Yan, C.; Tian, Y.; Hong, X.; Qian, C.; Zhang, J.; et al. Sleep, School Performance, and a School-Based Intervention among School-Aged Children: A Sleep Series Study in China. PLOS ONE 2013, 8, e67928. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Feng, R.; Ji, X.; Cui, N.; Raine, A.; Mednick, S.C. Midday napping in children: Associations between nap frequency and duration across cognitive, positive psychological well-being, behavioral, and metabolic health outcomes. Sleep 2019, 42, 126. [Google Scholar] [CrossRef] [PubMed]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Hillard, P.J.A.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, S.S.; Takeuchi, D.T. Social determinants of inadequate sleep in US children and adolescents. Public Health 2016, 138, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Qin, Z.; Wang, N.; Ware, R.S.; Sha, Y.; Xu, F. Lifestyle-related behaviors and health-related quality of life among children and adolescents in China. Health Qual. Life Outcomes 2021, 19, 1–9. [Google Scholar] [CrossRef]
- Fricke-Oerkermann, L.; Plück, J.; Schredl, M.; Heinz, K.; Mitschke, A.; Wiater, A.; Lehmkuhl, G. Prevalence and Course of Sleep Problems in Childhood. Sleep 2007, 30, 1371–1377. [Google Scholar] [CrossRef] [Green Version]
- Gradisar, M.; Gardner, G.; Dohnt, H. Recent worldwide sleep patterns and problems during adolescence: A review and meta-analysis of age, region, and sleep. Sleep Med. 2011, 12, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Xu, G.; Liu, Z.; Lu, N.; Ma, R.; Zhang, E. Sleep patterns and sleep disturbances among Chinese school-aged children: Prevalence and associated factors. Sleep Med. 2013, 14, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Jenni, O.G.; O’Connor, B.B. Children’s Sleep: An Interplay Between Culture and Biology. Pediatrics 2005, 115, 204–216. [Google Scholar] [CrossRef]
- Owens, J.A. Introduction: Culture and sleep in children. Pediatrics 2005, 115, 201–203. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A. Socio-Cultural Considerations and Sleep Practices in the Pediatric Population. Sleep Med. Clin. 2008, 3, 97–107. [Google Scholar] [CrossRef]
- Iwawaki, S.; Schuller, I.S. Cross-cultural (Japan-Slovakia) comparison of some aspects of sleeping patterns and anxiety. Stud. Psychol. 2001, 43, 215–224. [Google Scholar]
- Mindell, J.A.; Sadeh, A.; Wiegand, B.; How, T.H.; Goh, D.Y. Cross-cultural differences in infant and toddler sleep. Sleep Med. 2010, 11, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.P.; Hardy, S.T.; Hale, L.E.; Gazmararian, J.A. Racial disparities and sleep among preschool aged children: A systematic review. Sleep Health 2019, 5, 49–57. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- EndNote; Version X7; Thomson Reuters: Toronto, ON, Canada, 2019.
- Critical Appraisal Skills Programme. CASP (Case Control Study) Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/03/CASP-Case-Control-Study-Checklist-2018_fillable_form.pdf (accessed on 15 December 2020).
- Smith, T.O.; Easton, V.; Bacon, H.; Jerman, E.; Armon, K.; Poland, F.; MacGregor, A.J. The relationship between benign joint hypermobility syndrome and psychological distress: A systematic review and meta-analysis. Rheumatology 2014, 53, 114–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latz, S.; Wolf, A.W.; Lozoff, B. Cosleeping in context: Sleep practices and problems in young children in Japan and the United States. Arch. Pediatr. Adolesc. Med. 1999, 153, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A.; Mindell, J.; Rivera, L. “My child has a sleep problem”: A cross-cultural comparison of parental definitions. Sleep Med. 2011, 12, 478–482. [Google Scholar] [CrossRef] [PubMed]
- Dewald, J.F.; Short, M.A.; Gradisar, M.; Oort, F.J.; Meijer, A.M. The Chronic Sleep Reduction Questionnaire (CSRQ): A cross-cultural comparison and validation in Dutch and Australian adolescents. J. Sleep Res. 2012, 21, 584–594. [Google Scholar] [CrossRef]
- Vazsonyi, A.T.; Harris, C.; Terveer, A.M.; Pagava, K.; Phagava, H.; Michaud, P.A. Parallel mediation effects by sleep on the parental warmth-problem behaviour links: Evidence from national probability samples of Georgian and Swiss adolescents. J. Youth Adolesc. 2015, 44, 331–345. [Google Scholar] [CrossRef]
- Tynjälä, J.; Kannas, L.; Välimaa, R. How young Europeans sleep. Health Educ. Res. 1993, 8, 69–80. [Google Scholar] [CrossRef]
- Carneiro, I.M.; Fonseca, P.; Ferreira, R. Children’s Sleep Habits Questionnaire in Two Subpopulations from Cape Verde and Mozambique: Exploratory and Regression Analysis. Acta Médica Portuguesa 2019, 32, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Van Selms, M.K.A.; Marpaung, C.; Pogosian, A.; Lobbezoo, F. Geographical variation of parental-reported sleep bruxism among children: Comparison between the Netherlands, Armenia and Indonesia. Int. Dent. J. 2019, 69, 237–243. [Google Scholar] [CrossRef]
- LeBourgeois, M.K.; Giannotti, F.; Cortesi, F.; Wolfson, A.R.; Harsh, J. The Relationship Between Reported Sleep Quality and Sleep Hygiene in Italian and American Adolescents. Pediatrics 2005, 115, 257–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Liu, L.; Owens, J.A.; Kaplan, D.L. Sleep Patterns and Sleep Problems Among Schoolchildren in the United States and China. Pediatrics 2005, 115, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Hense, S.; Barba, G.; Pohlabeln, H.; De Henauw, S.; Marild, S.; Molnar, D.; Moreno, L.A.; Hadjigeorgiou, C.; Veidebaum, T.; Ahrens, W. Factors that Influence Weekday Sleep Duration in European Children. Sleep 2011, 34, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, J.; Mindell, J.A.; Sadeh, A. Sleep characteristics of young children in Japan: Internet study and comparison with other Countries in Asia. Pediatr. Int. 2011, 53, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Mindell, J.A.; Sadeh, A.; Kwon, R.; Goh, D.Y. Cross-cultural differences in the sleep of preschool children. Sleep Med. 2013, 14, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Short, M.A.; Gradisar, M.; Lack, L.C.; Wright, H.R.; Dewald, J.F.; Wolfson, A.R.; Carskadon, M.A. A cross-cultural comparison of sleep duration between US And Australian adolescents: The effect of school start time, parent-set bedtimes, and extracurricular load. Health Educ. Behav. 2012, 40, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Ahn, Y.; Williamson, A.A.; Seo, H.-J.; Sadeh, A.; Mindell, J.A. Sleep Patterns among South Korean Infants and Toddlers: Global Comparison. J. Korean Med. Sci. 2016, 31, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Biggs, S.N.; Meltzer, L.J.; Tapia, I.E.; Traylor, J.; Nixon, G.M.; Horne, R.S.; Doyle, L.W.; Asztalos, E.; Mindell, J.A.; Marcus, C.L.; et al. Sleep/Wake Patterns and Parental Perceptions of Sleep in Children Born Preterm. J. Clin. Sleep Med. 2016, 12, 711–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mindell, J.A.; Lee, C.; Sadeh, A. Young child and maternal sleep in the Middle East. Sleep Med. 2017, 32, 75–82. [Google Scholar] [CrossRef]
- Takahashi, M.; Wang, G.; Adachi, M.; Jiang, F.; Jiang, Y.; Saito, M. Differences in sleep problems between Japanese and Chinese pre-school aged children: A cross-cultural com-parison within the Asian region. Sleep Med. 2018, 48, 42–48. [Google Scholar] [CrossRef]
- Daban, K.D.Y.; Goh, D.Y.T. Comparison of sleep characteristics, patterns, and problems in young children within the Southeast Asian region. Behav. Sleep Med. 2019, 17, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Irwanto, N.; Rehatta, M.; Hartini, S.; Takada, S. Sleep Problem of Children with Autistic Spectrum Disorder Assessed by Children Sleep Habits Questionnaire-Abbreviated in Indonesia and Japan. Kobe J. Med. Sci. 2016, 62, E22–E26. [Google Scholar]
- Mindell, J.A.; Sadeh, A.; Kohyama, J.; How, T.H. Parental behaviours and sleep outcomes in infants and toddlers: A cross-cultural comparison. Sleep Med. 2010, 11, 393–399. [Google Scholar] [CrossRef]
- Chaput, J.P.; Katzmarzyk, P.T.; LeBlanc, A.G.; Tremblay, M.S.; Barreira, T.V.; Broyles, S.T. Associations between sleep patterns and lifestyle behaviours in children: An international comparison. Int. J. Obes. Suppl. 2015, 5, S59–S65. [Google Scholar] [CrossRef] [Green Version]
- Mindell, J.A.; Li, A.M.; Sadeh, A.; Kwon, R.; Goh, D.Y. Bedtime Routines for Young Children: A Dose-Dependent Association with Sleep Outcomes. Sleep 2015, 38, 717–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mindell, J.A.; Sadeh, A.; Kwon, R.; Goh, D.Y.T. Relationship Between Child and Maternal Sleep: A Developmental and Cross-Cultural Comparison. J. Pediatr. Psychol. 2015, 40, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Owens, J.A. Sleep in children: Cross-cultural perspectives. Sleep Biol. Rhythm. 2004, 2, 165–173. [Google Scholar] [CrossRef]
- Khan, M.K.A.; Faught, E.L.; Chu, Y.L.; Ekwaru, J.P.; Storey, K.E.; Veugelers, P.J. Is it nutrients, food items, diet quality or eating behaviours that are responsible for the association of children’s diet with sleep? J. Sleep Res. 2017, 26, 468–476. [Google Scholar] [CrossRef]
- Hyun, M.K.; Baek, Y.; Lee, S. Association between digestive symptoms and sleep disturbance: A cross-sectional community-based study. BMC Gastroenterol. 2019, 19, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1–14. [Google Scholar] [CrossRef]
- Desjardins, S.; Tanguay-Labonté, M. The Effects of Physical Activity on Sleep among Adolescents and Adults: A Narrative Review. J. Sleep Sleep Disord. Res. 2018, 1, 42–59. [Google Scholar] [CrossRef]
- Williams, S.M.; Farmer, V.L.; Taylor, B.J.; Taylor, R.W. Do More Active Children Sleep More? A Repeated Cross-Sectional Analysis Using Accelerometry. PLoS ONE 2014, 9, e93117. [Google Scholar] [CrossRef] [Green Version]
- Pesonen, A.-K.; Sjöstén, N.M.; Matthews, K.A.; Heinonen, K.; Martikainen, S.; Kajantie, E.; Tammelin, T.; Eriksson, J.G.; Strandberg, T.; Räikkönen, K. Temporal Associations between Daytime Physical Activity and Sleep in Children. PLoS ONE 2011, 6, e22958. [Google Scholar] [CrossRef]
- Passos, G.S.; Poyares, D.; Santana, M.G.; Garbuio, S.A.; Tufik, S.; Mello, M.T. Effect of Acute Physical Exercise on Patients with Chronic Primary Insomnia. J. Clin. Sleep Med. 2010, 6, 270–275. [Google Scholar] [CrossRef] [Green Version]
- Garmy, P.; Nyberg, P.; Jakobsson, U. Sleep and Television and Computer Habits of Swedish School-Age Children. J. Sch. Nurs. 2012, 28, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieters, D.; De Valck, E.; Vandekerckhove, M.; Pirrera, S.; Wuyts, J.; Exadaktylos, V.; Haex, B.; Michiels, N.; Verbraecken, J.; Cluydts, R. Effects of Pre-Sleep Media Use on Sleep/Wake Patterns and Daytime Functioning Among Adolescents: The Moderating Role of Parental Control. Behav. Sleep Med. 2014, 12, 427–443. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Pramstaller, P.P.; Ricken, J.; Havel, M.; Guth, A.; Merrow, M. A marker for the end of adolescence. Curr. Biol. 2004, 14, R1038–R1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorleifsdottir, B.; Björnsson, J.; Benediktsdottir, B.; Gislason, T.; Kristbjarnarson, H. Sleep and sleep habits from childhood to young adulthood over a 10-year period. J. Psychosom. Res. 2002, 53, 529–537. [Google Scholar] [CrossRef]
- Dexter, D.; Bijwadia, J.; Schilling, D.; Applebaugh, G. Sleep, sleepiness and school start times: A preliminary study. WMJ: Off. Publ. State Med. Soc. Wis. 2003, 102, 44–46. [Google Scholar]
- Wolfson, A.R.; Spaulding, N.L.; Dandrow, C.; Baroni, E.M. Middle School Start Times: The Importance of a Good Night’s Sleep for Young Adolescents. Behav. Sleep Med. 2007, 5, 194–209. [Google Scholar] [CrossRef]
- Mindell, J.A.; Sadeh, A.; Kwon, R.; Goh, D.Y.T. Corrigendum to “Cross-cultural differences in the sleep of preschool children”. Sleep Med. 2014, 15, 1595–1596. [Google Scholar] [CrossRef]
- Hale, L.; Berger, L.M.; LeBourgeois, M.K.; Brooks-Gunn, J. Social and Demographic Predictors of Preschoolers’ Bedtime Routines. J. Dev. Behav. Pediatr. 2009, 30, 394–402. [Google Scholar] [CrossRef] [Green Version]
- Sadeh, A.; Mindell, J.A.; Luedtke, K.; Wiegand, B. Sleep and sleep ecology in the first 3 years: A web-based study. J. Sleep Res. 2009, 18, 60–73. [Google Scholar] [CrossRef]
- Caudill, W.; Plath, D.W. Who Sleeps by Whom? Parent-Child Involvement in Urban Japanese Families. Psychiatry 1966, 29, 344–366. [Google Scholar] [CrossRef] [PubMed]
- Morelli, G.; Rogoff, B.; Oppenhelm, D. Cultural variations in infants’ sleeping arrangements. Dev. Psychol. 1992, 28, 604–613. [Google Scholar] [CrossRef]
- Yang, C.-K.; Hahn, H.-M. Cosleeping in Young Korean Children. J. Dev. Behav. Pediatr. 2002, 23, 151–157. [Google Scholar] [CrossRef]
- Blair, P.S.; Sidebotham, P.; Evason-Coombe, C.; Edmonds, M.; Heckstall-Smith, E.M.A.; Fleming, P. Hazardous cosleeping environments and risk factors amenable to change: Case-control study of SIDS in south west England. BMJ 2009, 339, b3666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozoff, B.; Askew, G.L.; Wolf, A.W. Cosleeping and Early Childhood Sleep Problems: Effects of Ethnicity and Socioeconomic Status. J. Dev. Behav. Pediatr. 1996, 17, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Schachter, F.F.; Fuchs, M.L.; Bijur, P.E.; Stone, R.K. Cosleeping and sleep problems in Hispanic-American urban young children. Pediatrics 1989, 84, 522–530. [Google Scholar]
- Asaka, Y.; Takada, S. Comparing sleep measures of infants derived from parental reports in sleep diaries and acceleration sensors. Acta Paediatr. 2011, 100, 1158–1163. [Google Scholar] [CrossRef]
- National Sleep Foundation. Summary of Findings—2004 Sleep in America Poll. 2004. Available online: https://www.sleepfoundation.org/wp-content/uploads/2018/10/FINAL-SOF-2004.pdf?x25214 (accessed on 17 February 2021).
- Iglowstein, I.; Jenni, O.G.; Molinari, L.; Largo, R.H. Sleep Duration From Infancy to Adolescence: Reference Values and Generational Trends. Pediatrics 2003, 111, 302–307. [Google Scholar] [CrossRef]
- Seo, W.S.; Sung, H.-M.; Lee, J.H.; Koo, B.H.; Kim, M.J.; Kim, S.Y.; Choi, S.-J.; Shin, I.H. Sleep patterns and their age-related changes in elementary-school children. Sleep Med. 2010, 11, 569–575. [Google Scholar] [CrossRef]
- Holley, S.; Hill, C.M.; Stevenson, J. A Comparison of Actigraphy and Parental Report of Sleep Habits in Typically Developing Children Aged 6 to 11 Years. Behav. Sleep Med. 2010, 8, 16–27. [Google Scholar] [CrossRef]
- Rönnlund, H.; Elovainio, M.; Virtanen, I.; Matomäki, J.; Lapinleimu, H. Poor Parental Sleep and the Reported Sleep Quality of Their Children. Pediatrics 2016, 137, e20153425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.J.; Hu, W.; Wei, F.; Wu, G.; Korn, L.R.; Chapman, R.S. Children’s respiratory morbidity prevalence in relation to air pollution in four Chinese cities. Environ. Health Perspect. 2002, 110, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Ellison, C.G.; Bradshaw, M.; Storch, J.; Marcum, J.P.; Hill, T.D. Religious Doubts and Sleep Quality: Findings from a Nationwide Study of Presbyterians #090709revised. Rev. Relig. Res. 2011, 53, 119–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sheikh, M.; Buckhalt, J.A.; Mize, J.; Acebo, C. Marital Conflict and Disruption of Children’s Sleep. Child Dev. 2006, 77, 31–43. [Google Scholar] [CrossRef]
- Klein, T.P.; DeVoe, E.R.; Miranda-Julian, C.; Linas, K. Young children’s responses to September 11th: The New York City experience. Child Adolesc. Soc. Work. J. 2009, 30, 1–22. [Google Scholar] [CrossRef]
- Thabet, A.A.M.; Karim, K.; Vostanis, P. Trauma exposure in pre-school children in a war zone. Br. J. Psychiatry 2006, 188, 154–158. [Google Scholar] [CrossRef]
- Souders, M.C.; Mason, T.B.A.; Valladares Bucan, M.; Levy, S.E.; Mandell, D.S.; Weaver, T.E.; Pinto-Martin, J. Sleep Behaviors and Sleep Quality in Children with Autism Spectrum Disorders. Sleep 2009, 32, 1566–1578. [Google Scholar] [CrossRef]
- Polimeni, M.A.; Richdale, A.L.; Francis, A.J.P. A survey of sleep problems in autism, Asperger’s disorder and typically developing children. J. Intellect. Disabil. Res. 2005, 49, 260–268. [Google Scholar] [CrossRef]


| Authors (Year) | Included Countries | Ages (Mean)/Gender (% of Male Participants) | Sleep Measurement | Sleep Duration Variables Relevant to Review | Brief Summary of Findings |
|---|---|---|---|---|---|
| LeBourgeois et al. (2005) [30] | Italy (n = 776) | 12–17 years (M = 14.6y) /55.4% | Adolescent Sleep Hygiene Scale | (1) Duration of habitual naps | Adolescents in Italy had significantly higher scores in a daytime sleep hygiene question (e.g., not having more than 1-h naps during the day) (M = 5.1) than adolescents in the U.S (M = 3.9) (p < 0.001) |
| US (n = 572) | 12–17 years (M = 14.6y) /41.2% | ||||
| Liu et al. (2005) [31] | US (n = 494) | 4.83–11 years (M = 7.56 y) /51.2% | CSHQ |
| Children in China had a significantly later bedtime (M = 9.03), earlier wake up time (M = 6.46), and shorter nocturnal sleep duration (M = 9.25 h) than children in the U.S (Mbedtime = 8.46, Mwakeuptime = 6.91, Msleepduration = 10.15 h) (all ps < 0.001). |
| China (n = 517) | 7–13 years (M = 11.0 y) /47% | ||||
| Mindell et al. (2010) [17] | 17 countries (n = 29,287) divided into | BISQ |
| Significant differences in bedtime, wake up time, nocturnal sleep duration, number of habitual naps, duration of habitual naps and total sleep time were shown across 17 countries (All ps < 0.0001). Infants and toddlers in P-A countries had a significantly later bedtime (M = 21.44), later wake up time (M = 7.11), shorter nocturnal sleep duration (M = 9.19 h), more frequent habitual naps (M = 2.06), longer duration of habitual naps (M = 3.11 h) and shorter total sleep time (M = 12.31 h) than infants and toddlers in P-C countries (Mbedtime = 20.42, Mwakeuptime = 6.63, Msleepduration = 10.0 h, Mnumberofnaps = 2.04, Mdurationofnaps = 3.01 h, Mtotalsleeptime = 13.02 h) (all ps < 0.0001). | |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported) /52.5% | ||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported) /51.9% | ||||
| Hense et al. (2011) [32] | 8 European countries (n = 31,543) including | 2–9 years | A standardised 24-h recall | (1) Nocturnal sleep duration | Nocturnal sleep duration ranged from 9.5 h in Estonia to 11.2 h in Belgium. Children in Northern Europe (including Sweden, Germany and Belgium) had a significantly longer nocturnal sleep duration than children in Southern Europe (including Italy, Spain and Cyprus) and Eastern Europe (including Estonia and Hungary) (p < 0.001) |
| Estonia (n = 1331) | (M = 5.8 y)/48.9% | ||||
| Italy (n = 1643) | (M = 6.2 y)/52.0% | ||||
| Hungary (n = 902) | (M = 6.7 y)/49.2% | ||||
| Cyprus (n = 953) | (M = 6.3 y)/49.4% | ||||
| Spain (n = 504) | (M = 5.5 y)/42.4% | ||||
| Sweden (n = 1215) | (M = 5.7 y)/51.7% | ||||
| Germany (n = 1586) | (M = 6.1 y)/51.5% | ||||
| Belgium (n = 408) | (M = 5.5 y)/52.5% | ||||
| Kohyama et al. (2011) [33] | Japan (n = 872) | Birth–3 years (mean not reported) /48.6% | BISQ |
| Infants and toddlers in Japan had significantly less frequent habitual naps (M = 1.44), and shorter duration of habitual naps (M = 2.19h), than infants and toddlers in other 11 Asian countries (Mnumberofnaps = 2.09, Mdurationofnaps = 3.15 h) (p < 0.001). There were no significant differences in bedtime (Japan, M = 21.29; 11 Asian countries, M = 21.45), wake up time (Japan, M = 7.14; 11 Asian countries, M = 7.11), nocturnal sleep duration (Japan, M = 9.42 h; 11 Asian countries, M = 9.18 h) and total sleep time (Japan, M = 11.62 h; 11 Asian countries, M = 12.33 h) between infants and toddlers in Japan vs. 11 other Asian countries (p > 0.001). |
| 11 Asian countries including CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH and VN (n = 20,455) | Birth–3 years (mean not reported) /48.1% | ||||
| Dewald et al. (2012) [25] | Netherlands (n = 166) | 12.2–16.5 years (M = 15.2 y) /28% | Sleep diaries, actigraphy | (1) Nocturnal sleep duration | The results of the sleep diary demonstrated that adolescents in the Netherlands had a significantly shorter nocturnal sleep duration (M = 7:44) than adolescents in Australia (M = 8:27) (p < 0.001). However, actigraphy results did not show a significant difference in nocturnal sleep duration between adolescents in the Netherlands (M = 8:04) and Australia (M = 8:03) (p > 0.05). |
| Australia (n = 236) | 13.3–18.9 years (M = 15.5 y) /65% | ||||
| Mindell et al. (2013) [34] | 17 countries (n = 2590) divided into | BCSQ |
| Significant differences in bedtime, wake up time, number of habitual naps, duration of habitual naps and total sleep time were shown across 14 countries (All ps < 0.0001). Children in P-A countries had a significantly later bedtime (M = 9.85), later wake up time (M = 7.62), more frequent habitual naps (M = 1.93), longer duration of habitual naps (M = 1.58 h) and a shorter total sleep time (M = 9.44 h) than infants and toddlers in P-C countries (Mbedtime = 8.15, Mwakeuptime = 7.12, Mnumberofnaps = 1.32, Mdurationofnaps = 0.52 h, Mtotalsleeptime = 10.54 h) (All ps < 0.0001). | |
| P-C countries (n = 1139; AU, CA, NZ, US, UK) | 3–6 years (mean not reported) /49.8% | ||||
| P-A countries (n = 1447; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | 3–6 years (mean not reported) /50.2% | ||||
| Short et al. (2013) [35] | Australia (n = 385) | 13–18 years (M = 15.57 y) /60% | Sleep diary |
| Adolescents in the U.S. had a significantly earlier wake up time (M = 6:23) and shorter nocturnal sleep duration (M = 7 h 22 min) than adolescents in Australia (Mwakeuptime = 7:10, Msleepduration = 8 h 17 min), all ps < 0.001. However, no significant difference was found in bedtime between adolescents in the U.S. (M = 22:28) and Australia (M = 22:36). |
| US (n = 302) | 13–19 years (M = 16.03 y) /35% | ||||
| Ahn et al. (2016) [36] | South Korea (n = 1036) | Birth–3 years (mean not reported) /50.8% | BISQ |
| Significant differences in bedtime, nocturnal sleep duration, number of habitual naps, duration of habitual naps and total sleep time were shown across South Korea, P-A countries, and P-C countries (All ps < 0.001). Infants and toddlers in South Korea had the latest bedtime (M = 10:08 pm), the least frequent habitual naps (M = 1.64), the shortest duration of habitual naps (M = 2.47 h), and shortest total sleep time (M = 11.89 h) compared to infants and toddlers in P-A countries (Mbedtime = 9:25pm, Mnumberofnaps = 2.08, Mdurationofnaps = 3.15 h, Mtotalsleeptime = 12.33 h) and P-C countries (Mbedtime = 8:25pm, Mnumberofnaps = 2.04, Mdurationofnaps = 3.01 h, Mtotalsleeptime = 13.02 h). Nocturnal sleep duration of infants and toddlers in South Korea (M = 9.42 h) was significantly longer than nocturnal sleep duration of those in P-A countries (M = 9.12 h), but shorter than those in P-C countries (M = 10.01 h). |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported) /52.5% | ||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN) from Mindell et al. (2010) [17] | Birth–3 years (mean not reported) /51.9% | ||||
| Biggs et al. (2016) [37] | Australia (n = 87) | 5–12 years (M = 9.6 y) /58% | Actigraphy, National Sleep Foundation 2004 Sleep in America questionnaire |
| Actigraphy results demonstrated that children in Canada had a significantly later bedtime during weekdays (M = 21:13) and weekends (22:02), and an earlier wake up time at the weekend (M = 8:05), than children in Australia (Mbedtimeweekdays = 20:54, Mbedtimeweekends = 21:35, Mwakeuptimeweekends = 7:42) (all ps < 0.01). No significant differences were found for wake up time during weekdays or nocturnal sleep duration during the weekdays or weekends, between children in Canada (Mwakeuptimeweekdays = 8:41, Mnocturalsleepdurationweekdays = 493 min, Mnocturnalsleepdurationweekends = 485 min) and Australia (Mwakeuptimeweekdays = 8:31, Mnocturalsleepdurationweekdays = 491 min, Mnocturnalsleepdurationweekends = 480 min). Questionnaire-based nocturnal sleep results demonstrated significantly longer nocturnal sleep duration in children in Australia (M = 598 min) than children in Canada (M = 565 min) (p = 0.001). |
| Canada (n = 101) | 5–12 years (M = 9.0 y) /56% | ||||
| Mindell et al. (2017) [38] | ME countries (n = 669; Saudi Arabia, Egypt, Algeria, United Arab Emirates, Jordan, Morocco, Iraq, Kuwai, Oman, Palestinian territories, Libyan Arab Jamahiriya, Bahrain, Israel and 83 from other Arab countries) | Birth–3 years (mean not reported) /50.2% | BISQ |
| Infants and toddlers in the Middle East had a significantly later bedtime (M = 10:45), later wake up time (M = 8:38), shorter nocturnal sleep duration (M = 9.15 h), and shorter total sleep time (M = 11.72 h) than infants and toddlers in P-A countries (Mbedtime = 9:26, Mwakeuptime = 7:06, Mnocturnalsleepduration = 9.19h, Mtotalsleeptime = 12.31 h) and P-C countries (Mbedtime = 8:25, Mwakeuptime = 6:38, Mnocturnalsleepduration = 10.01 h, Mtotalsleeptime = 13.02 h) (all ps < 0.001). For habitual naps, infants and toddlers in P-A countries had more frequent habitual naps (M = 2.06), and a longer duration of habitual naps (M = 3.11 h), followed by infants and toddlers in P-C countries (Mnumberofhabitualnaps = 2.04, Mdurationofhabitualnaps = 3.01 h) and in Middle East countries (Mnumberofhabitualnaps = 1.90, Mdurationofhabitualnaps = 2.57 h) (all ps < 0.001). |
| P-C and P-A countries from Mindell et al. (2010; n = 29,287) [17] | Birth–3 years (mean not reported) /51.94% | ||||
| Takahashi et al. (2018) [39] | Japan (n = 505) | 4–5 years (mean not reported) /47.3% | CSHQ |
| Children in China had a significantly later bedtime (M = 21.70), later wake up time (M = 7.66), and longer total sleep time (M = 9.54 h) than children in Japan (Mbedtime = 21.36, Mwakeuptime = 6.69, Mtotalsleeptime = 9.03 h) (all ps < 0.001). |
| China (n = 1909) | 4–5 years (mean not reported) /53.0% | ||||
| Daban & Goh (2019) [40] | 6 Southeast Asia countries (n = 5987) including | Birth–3 years | BISQ |
| Significant differences in bedtime, wake up time, nocturnal sleep duration, frequency of habitual naps and duration of habitual naps were found across 6 Southeast Asia countries (all ps < 0.0001). |
| Indonesia (n = 967) | (mean not reported) /50.2% | ||||
| Malaysia (n = 997) | (mean not reported) /50.4% | ||||
| Philippines (n = 1034) | (mean not reported) /49.8% | ||||
| Singapore (n = 1001) | (mean not reported) /51.6% | ||||
| Thailand (n = 988) | (mean not reported) /49.2% | ||||
| Vietnam (n = 1000) | (mean not reported) /49.4% |
| Authors (Year) | Included Countries | Ages (Mean)/ Gender (% of Male Participants) | Sleep Measurement | Sleep Disturbance Variables Relevant to Review | Brief Summary of Findings |
|---|---|---|---|---|---|
| Latz et al. (1999) [23] | Japan (n = 56) | 6–48 months (Mean not reported) /50.0% | Interview questions on sleep problems |
| Infants and toddlers in the U.S. were more likely to have more than 3 night awakenings (30%), more bedtime resistance (26%) and more stress-related sleep problems (25%) per week than infants and toddlers in Japan (20%, 20% and 13%, respectively) All ps < 0.05. |
| US (n = 61) | 6–48 months (Mean not reported) /46.0% | ||||
| LeBourgeois et al. (2005) [30] | Italy (n = 776) | 12–17 years (M = 14.6 y) /55.4% | Adolescent Sleep–Wake Scale |
| Adolescents in Italy had significantly better sleep quality than adolescents in the U.S with higher scores in night waking, bedtime resistance and sleep latency (i.e., falling asleep) dimension (all ps < 0.001; specific data were not reported). |
| US (n = 572) | 12–17 years (M = 14.6 y) /41.2% | ||||
| Liu et al. (2005) [31] | US (n = 494) | 4.83–11 years (M = 7.56 y) /51.2% | CSHQ |
| Children in China had significantly greater problems in night awakenings (M = 3.85), bedtime resistance (M = 7.92), daytime sleepiness (M = 10.22) and overall sleep problems (M = 42.11) than children in the U.S (Mnightwaking = 3.49; Mbedtimeresistance = 7.01; Mdaytimesleepiness = 9.72; Msleepproblem = 38.71). All ps < 0.05. No significant difference was found in sleep latency between children in China (M = 1.28) and children in the U.S (M = 1.26). |
| China (n = 517) | 7–13 years (M = 11.0 y) /47% | ||||
| Mindell et al. (2010) [17] | 17 countries (n = 29,287) divided into | BISQ |
| Significant differences in the frequency and duration of night awakenings, bedtime resistance, sleep latency, sleep quality and overall sleep problems were shown across 17 countries (All ps < 0.0001). Infants and toddlers in P-A countries had significantly greater problems in the frequency of night awakenings (M = 1.69), duration of night awakenings (M = 0.52), sleep latency (19.29%), sleep quality (56.4%) and overall sleep problems (51.9%) than infants and toddlers in P-C countries (Mfrequencyofnightwakenings = 1.13; Mdurationofnightawakenings = 0.41; Msleeplatency = 9.57%; Msleepquality = 73.6%; Msleepproblem = 26.3%). However, no significant differences were found between infants and toddlers in P-A countries (M = 22.17%) and P-C countries (14.29%) in the percentage of children experiencing bedtime resistance. | |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported)/52.5% | ||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/51.9% | ||||
| Kohyama et al. (2011) [33] | Japan (n = 872) | Birth–3 years (mean not reported)/48.6% | BISQ |
| Infants and toddlers in Japan had significantly fewer night awakenings (M = 1.25) and shorter duration of night awakenings (M = 0.28 h) than infants and toddlers in 11 other Asian countries (Mfrequencyofnightawakenings = 1.71; Mdurationofnightawakenings = 0.53 h). Infants and toddlers in Japan were more likely to have bedtime resistance (M = 28.44%) and less likely to have sleep problems (M = 19.61%) than infants and toddlers in 11 other Asian countries (Mbedtimeresistance = 21.91%; Msleepproblem = 53.28%). All ps < 0.001. No significant differences were found in the percentage of children having sleep latency >30 min between infants and toddlers in Japan (M = 22.71%) vs. in 11 other Asian countries (M = 19.15%). |
| 11 Asian countries including CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH and VN (n = 20,455) | Birth–3 years (mean not reported)/48.1% | ||||
| Dewald et al. (2012) [25] | Netherlands (n = 166) | 12.2–16.5 years (M = 15.2 y) /28% | Sleep diaries, actigraphy |
| The actigraphy results showed no significant differences in sleep latency between adolescents in the Netherlands (M = 23 min) and in Australia (M = 23 min). The actigraphy results found significantly higher sleep quality in adolescents in the Netherlands (M = 80.04%) than peers in Australia (M = 77%) (p < 0.01), whereas sleep diary data found significantly higher sleep quality in adolescents in Australia (M = 96.66%) than peers in the Netherlands (M = 90.49%) (p < 0.001). |
| Australia (n = 236) | 13.3–18.9 years (M = 15.5 y) /65% | ||||
| Mindell et al. (2013) [34] | 17 countries (n = 2590) divided into | BCSQ |
| Significant differences in the frequency of night awakenings, duration of night awakenings, sleep latency, daytime sleepiness and sleep problems were shown across 14 countries (All ps < 0.0001). Children in P-A countries had a significantly longer sleep latency (M = 21.25 min) and a greater percentage of sleep problems (M = 24.2%) than children in P-C countries (Msleeplatency = 19.12mins; Msleepproblem = 18.4%) (all ps < 0.0001). No significant differences were found in the frequency of night awakenings (MP-C = 1.59; MP-A = 1.66), duration of night awakenings (MP-C = 7.19; MP-A = 9.90) and daytime sleepiness (MP-C = 12.6%; MP-A = 9.5%) between children in P-C countries and P-A countries. | |
| P-C countries (n = 1139; AU, CA, NZ, US, UK) | 3–6 years (mean not reported) /49.8% | ||||
| P-A countries (n = 1447; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | 3–6 years (mean not reported) /50.2% | ||||
| Ahn et al. (2016) [36] | South Korea (n = 1036) | Birth–3 years (mean not reported) /50.8% | BISQ | (1) Frequency and duration of night awakenings | Infants and toddlers in South Korea had the shortest duration of nocturnal awakenings (M = 0.34 min) compared to infants and toddlers in P-A countries (M = 0.53 min) and in P-C countries (M = 0.41 min) (p < 0.001). Infants and toddlers in South Korea had less frequent night awakenings (M = 1.49) than infants and toddlers in P-A countries (M = 1.70), and more frequent night awakenings than infants and toddlers in P-C countries (M = 1.13) (p < 0.001). |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported)/52.5% | ||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN) from Mindell et al. (2010) [17] | Birth–3 years (mean not reported)/51.9% | ||||
| Biggs et al. (2016) [37] | Australia (n = 87) | 5–12 years (M = 9.6 y) /58% | Actigraphy |
| Actigraphy results demonstrated no significant differences in the duration of night awakenings during weekdays (MAustralia = 77, MCanada = 73), weekends (MAustralia = 76, MCanada = 70), sleep latency during weekdays (MAustralia = 28 min, MCanada = 27mins) or weekends (MAustralia = 26 min, MCanada = 20 min), and sleep quality during weekdays (MAustralia = 79%, MCanada = 81%) or weekends (MAustralia = 79%, MCanada = 81%) between children in Australia vs. children in Canada (All ps > 0.05). |
| Canada (n = 101) | 5–12 years (M = 9.0 y) /56% | ||||
| Irwanto et al. (2016) [41] | Indonesia (n = 25) | 4–10 years of children with ASD (M = 4.8 y) /84% | CSHQ-A |
| Children with ASD in Indonesia had a significantly greater frequency of night awakenings (M = 2.76) and overall sleep problems (M = 41.12) than children with ASD in Japan (Mnightwaking = 2.36; Msleepproblem = 37.28) (all ps < 0.05). There was no significant difference in bedtime-related sleep problems between children with ASD in Indonesia (M = 18.88) and children with ASD in Japan (M = 17.88; p > 0.05). |
| Japan (n = 25) | 4–10 years of children with ASD (M = 7.7 y) /80% | ||||
| Mindell et al. (2017) [38] | ME countries (n = 669; Saudi Arabia, Egypt, Algeria, United Arab Emirates, Jordan, Morocco, Iraq, Kuwai, Oman, Palestinian territories, Libyan Arab Jamahiriya, Bahrain, Israel and 83 from other Arab countries) | Birth–3 years (mean not reported) /50.2% | BISQ |
| Infants and toddlers in the Middle East had a significantly higher frequency of night awakenings (M = 2,20), a longer duration of night awakenings (M = 41 min) and a greater percentage of bedtime resistance (38%), compared with infants and toddlers in P-A countries (Mfrequencyrofnightawakenings = 1.69; Mdurationofnightawakenings = 31mins; Mbedtimeresistance = 22.2%) and P-C countries (Mfrequencyrofnightawakenings = 1.13; Mdurationofnightawakenings = 25 min; Mbedtimeresistance = 14.3%). All ps < 0.001. Infants and toddlers in P-A countries had the greatest percentage of sleep problems (51.9%), compared with toddlers in Middle East countries (36.9%) and in P-C countries (26.3%) (p < 0.001). |
| P-C and P-A countries from Mindell et al. (2010; n = 29,287) [17] | Birth–3 years (mean not reported) /51.94% | ||||
| Takahashi et al. (2018) [39] | Japan (n = 505) | 4–5 years (mean not reported) /47.3% | CSHQ |
| Children in China had significantly greater sleep problems in the frequency of night awakenings (M = 4.09) and sleep latency (M = 1.61) than children in Japan (Mfrequencyofnightawakening = 3.47; Msleeplatency = 1.43), whereas children in China had significantly less problems in bedtime resistance (M = 11.05) than children in Japan (M = 12.49). All ps < 0.05. No significant differences between countries were found in daytime sleepiness (MJapan = 10.76; MChina = 11.12) and overall sleep problems (MJapan = 46.56; MChina = 47.35). |
| China (n = 1909) | 4–5 years (mean not reported) /53.0% | ||||
| Daban & Goh (2019) [40] | 6 Southeast Asia countries (n = 5987) including | Birth–3 years | BISQ |
| Significant differences were found in the frequency of night awakenings, the duration of night awakenings, sleep latency and sleep problems across 6 Southeast Asia countries (all ps > 0.0001). |
| Indonesia (n = 967) | (mean not reported) /50.2% | ||||
| Malaysia (n = 997) | (mean not reported) /50.4% | ||||
| Philippines (n = 1034) | (mean not reported) /49.8% | ||||
| Singapore (n = 1001) | (mean not reported) /51.6% | ||||
| Thailand (n = 988) | (mean not reported) /49.2% | ||||
| Vietnam (n = 1000) | (mean not reported) /49.4% | ||||
| van Selms et al. (2019) [29] | Netherland (n = 1131) | 7–12 years (M = 10.0) /44.6% | Simple author questions | (1) Sleep latency | A significantly greater percentage of children in Netherland had sleep latency (i.e., difficulty falling asleep; 60.4%), than children in Armenia (30.8%) and children in Indonesia (21.5%) (p < 0.01). |
| Armenia (n = 886) | 7–12 years (M = 9.1) /49.0% | ||||
| Indonesia (n = 545) | 7–12 years (M = 9.5) /41.5% |
| Authors (Year) | Included Countries | Ages (Mean)/ Gender (% of Male Participants) | Cultural Factor Domains | ||
|---|---|---|---|---|---|
| Child | Parental | Environmental | |||
| Latz et al. (1999) [23] | Japan (n = 56) | 6–47 months (M = 30.3) /72% | not measured | Parental education level, Sleep initiating and resuming methods | Number in household, Maternal employment, Co-sleeping in body contact, Adult company at bedtime |
| US (n = 61) | 6–47 months (M = 25.0) /67% | ||||
| LeBourgeois et al. (2005) [30] | Italy (n = 776) | 12–17 years (M = 14.6 y) /55.4% | Physiologically sleep-inhibiting, cognitive and emotional status at bedtime, Circadian preference, Puberty | Bedtime routine | SES, Bed/bedroom sharing |
| US (n = 572) | 12 to 17 years (M = 14.6 y) /41.2% | ||||
| Mindell et al. (2010) [17] | 17 countries (n = 29,287) divided into | not measured | Maternal education level, Bedtime routine | Sleeping location, Maternal employment | |
| P-C countries (n = 7960; AU, CA, NZ, US, UK) and | Birth–3 years (mean not reported)/52.5% | ||||
| P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/51.9% | ||||
| Mindell et al. (2010) [42] | 17 countries (n = 29,287) divided into P-C countries (n = 7960; AU, CA, NZ, US, UK) and P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/51.9% (for entire sample) | not measured | Sleep initiating and resuming method | Sleeping location |
| Hense et al. (2011) [32] | 8 European countries (n = 31,543) including | 2–9 years | Overweight, Playing outdoors, Time spent in front of TV or PC | Parental education level | Daylight, season |
| Estonia (n = 1331) | (M = 5.8 y)/48.9% | ||||
| Italy (n = 1643) | (M = 6.2 y)/52.0% | ||||
| Hungary (n = 902) | (M = 6.7 y)/49.2% | ||||
| Cyprus (n = 953) | (M = 6.3 y)/49.4% | ||||
| Spain (n = 504) | (M = 5.5 y)/42.4% | ||||
| Sweden (n = 1215) | (M = 5.7 y)/51.7% | ||||
| Germany (n = 1586) | (M = 6.1 y)/51.5% | ||||
| Belgium (n = 408) | (M = 5.5 y)/52.5% | ||||
| Kohyama et al. (2011) [33] | Japan (n = 872) | Birth–3 years (mean not reported)/48.6% | not measured | Bedtime routine | Sleeping location, Parental presence at bedtime |
| 11 Asian countries including CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH and VN (n = 20,455) | Birth–3 years (mean not reported)/48.1% | ||||
| Sadeh et al. (2011) [24] | 17 countries (n = 29,287) divided into P-C countries (n = 7960; AU, CA, NZ, US, UK) and P-A countries (n = 21327; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | Birth–3 years (mean not reported)/48.1% (for entire sample) | not measured | Maternal education level | Presence of siblings, Maternal employment |
| Mindell et al. (2013) [34] | 17 countries (n = 2590) divided into | Daily outdoor time, Screen time (i.e., television viewing, using a computer, playing other electronic games) | Bedtime routine, Maternal education level | Maternal employment, Sleeping location | |
| P-C countries (n = 1139; AU, CA, NZ, US, UK) | 3–6 years (mean not reported) /49.8% | ||||
| P-A countries (n = 1447; CN, HK, IN, ID, KR, JP, MY, PH, SG, TW, TH, VN). | 3–6 years (mean not reported) /50.2% | ||||
| Short et al. (2013) [35] | Australia (n = 385) | 13–18 years (M = 15.57 y) /60% | School start time, Extracurricular load, Circadian preference | Parent-set bedtime | not measured |
| US (n = 302) | 13–19 years (M = 16.03 y) /35% | ||||
| Chaput et al. (2015) [43] | 12 countries (n = 5777) including | 9–11 years | Diet, Physical activity, Screen time (i.e., hours of watching TV, playing video games and using computer) | not measured | not measured |
| Australia (n = 433) | (M = 10.7 y)/46.7% | ||||
| Canada (n = 496) | (M = 10.5 y)/40.9% | ||||
| China (n = 459) | (M = 9.9 y)/51.6% | ||||
| India (n = 433) | (M = 10.5 y)/45.1% | ||||
| UK (n = 374) | (M = 10.9 y)/42.8% | ||||
| US (n = 421) | (M = 9.9 y)/40.4% | ||||
| Brazil (n = 435) | (M = 10.5 y)/48.5% | ||||
| Colombia (n = 820) | (M = 10.5 y)/49.2% | ||||
| Finland (n = 526) | (M = 10.4 y)/45.3% | ||||
| Kenya (n = 452) | (M = 10.2 y)/45.4% | ||||
| Portugal (n = 563) | (M = 10.4 y)/41.6% | ||||
| South Africa (n = 452) | (M = 10.2 y)/38.6% | ||||
| Mindell et al. (2015) [44] | 13 countries including AU/NZ, CA, UK, US, CN, HK, IN, JP, KR, MY, PH, SG and TH (n = 10085) | Birth–5.11 years (mean not reported)/49.6% (for entire sample) | not measured | Bedtime routine | not measured |
| Mindell et al. (2015) [45] | 13 countries (n = 10085) including | not measured | Maternal education level, Maternal sleep | Number of children, Maternal employment | |
| P-C countries (n = 4152; AU/NZ, CA, UK, US) and | Birth–6 years (mean not reported)/ 50.7% | ||||
| P-A countries (n = 5933; CN, HK, IN, JP, KR, MY, PH, SG and TH) | Birth–6 years (mean not reported)/ 50.2% | ||||
| Vazsonyi et al. (2015) [26] | Swiss (n = 5575) | 15–18 years (M = 17.17)/ 50.0% | not measured | Parental warmth | not measured |
| Georgia (n = 6692) | 15–18 years (M = 15.83)/ 40.0% | ||||
| Biggs et al. (2016) [37] | Australia (n = 87) | 5–12 years (M = 9.6 y) /58% | not measured | Maternal education level | Season, Daylight amount |
| Canada (n = 101) | 5–12 years (M = 9.0 y) /56% | ||||
| Mindell et al. (2017) [38] | ME countries (n = 669; Saudi Arabia, Egypt, Algeria, United Arab Emirates, Jordan, Morocco, Iraq, Kuwai, Oman, Palestinian territories, Libyan Arab Jamahiriya, Bahrain, Israel and 83 from other Arab countries) | Birth–3 years (mean not reported) /50.2% | not measured | Bedtime routine | not measured |
| P-C and P-A countries from Mindell et al. (2010; n = 29,287) [17] | Birth–3 years (mean not reported) /51.94% | ||||
| Takahashi et al. (2018) [39] | Japan (n = 505) | 4–5 years (mean not reported) /47.3% | not measured | Parental education level | Family structure, Number of siblings |
| China (n = 1909) | 4–5 years (mean not reported) /53.0% | ||||
| Carneiro et al. (2019) [28] | Cape Verde (n = 206) | 2–15 years (mean not reported) /46% | Bedtime television | Parental education level | Number of cohabitants, Number of cohabitant children |
| Mozambique (n = 438) | 4–13 years (mean not reported) /49% | ||||
| Daban & Goh (2019) [40] | 6 Southeast Asia countries (n = 5987) including | Birth–3 years | not measured | Bedtime routine | Sleeping location |
| Indonesia (n = 967) | (mean not reported) /50.2% | ||||
| Malaysia (n = 997) | (mean not reported) /50.4% | ||||
| Philippines (n = 1034) | (mean not reported) /49.8% | ||||
| Singapore (n = 1001) | (mean not reported) /51.6% | ||||
| Thailand (n = 988) | (mean not reported) /49.2% | ||||
| Vietnam (n = 1000) | (mean not reported) /49.4% | ||||
| van Selms et al. (2019) [29] | Netherland (n = 1131) | 7–12 years (M = 10.0) /44.6% | Pressure from home, Pressure from school, Easily scared, Worried | not measured | not measured |
| Armenia (n = 886) | 7–12 years (M = 9.1) /49.0% | ||||
| Indonesia (n = 545) | 7–12 years (M = 9.5) /41.5% | ||||
| 7 | 17 | 13 | |||
| Universal Factors | Cultural Factors | |
|---|---|---|
| Child factors | ||
| Physical health-related factors | Physiological status at bedtime [30] Diet [43] | |
| Psychological health-related factors | Emotional status [30] Cognitive status [30] Pressure from school [29] Worried [29] | Pressure from home [29] Easily scared [29] |
| Physical activities | Vigorous physical activity [43] | |
| Screen time | Screen time [28,43] | |
| Academic related factors | NA | NA |
| Adolescent-related factors | Circadian preference [30] Puberty status [30] | |
| Parent factors | ||
| Parenting practices | Parental warmth [26] Bedtime routine [30] | |
| Parent-related factor | Maternal education level [24,28] Paternal education level [28] | |
| Environmental factors | ||
| Family composition | The number of families [28] The number of siblings [28] | Presence of siblings [24] |
| Lifestyles | SES [30] | Maternal employment status [24] |
| Sleeping arrangement | Bed/bedroom sharing [30] Falling asleep alone [42] Co-sleeping with body contact [23] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, M.; Dimitriou, D.; Halstead, E.J. A Systematic Review on Cross-Cultural Comparative Studies of Sleep in Young Populations: The Roles of Cultural Factors. Int. J. Environ. Res. Public Health 2021, 18, 2005. https://doi.org/10.3390/ijerph18042005
Jeon M, Dimitriou D, Halstead EJ. A Systematic Review on Cross-Cultural Comparative Studies of Sleep in Young Populations: The Roles of Cultural Factors. International Journal of Environmental Research and Public Health. 2021; 18(4):2005. https://doi.org/10.3390/ijerph18042005
Chicago/Turabian StyleJeon, Mina, Dagmara Dimitriou, and Elizabeth J. Halstead. 2021. "A Systematic Review on Cross-Cultural Comparative Studies of Sleep in Young Populations: The Roles of Cultural Factors" International Journal of Environmental Research and Public Health 18, no. 4: 2005. https://doi.org/10.3390/ijerph18042005