
Is Mindfulness-Based Stress Reduction Effective for People with Hypertension? A Systematic Review and Meta-Analysis of 30 Years of Evidence

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Rationale and Objectives
3. Method
3.1. Eligibility Criteria
3.2. Systematic Literature Search
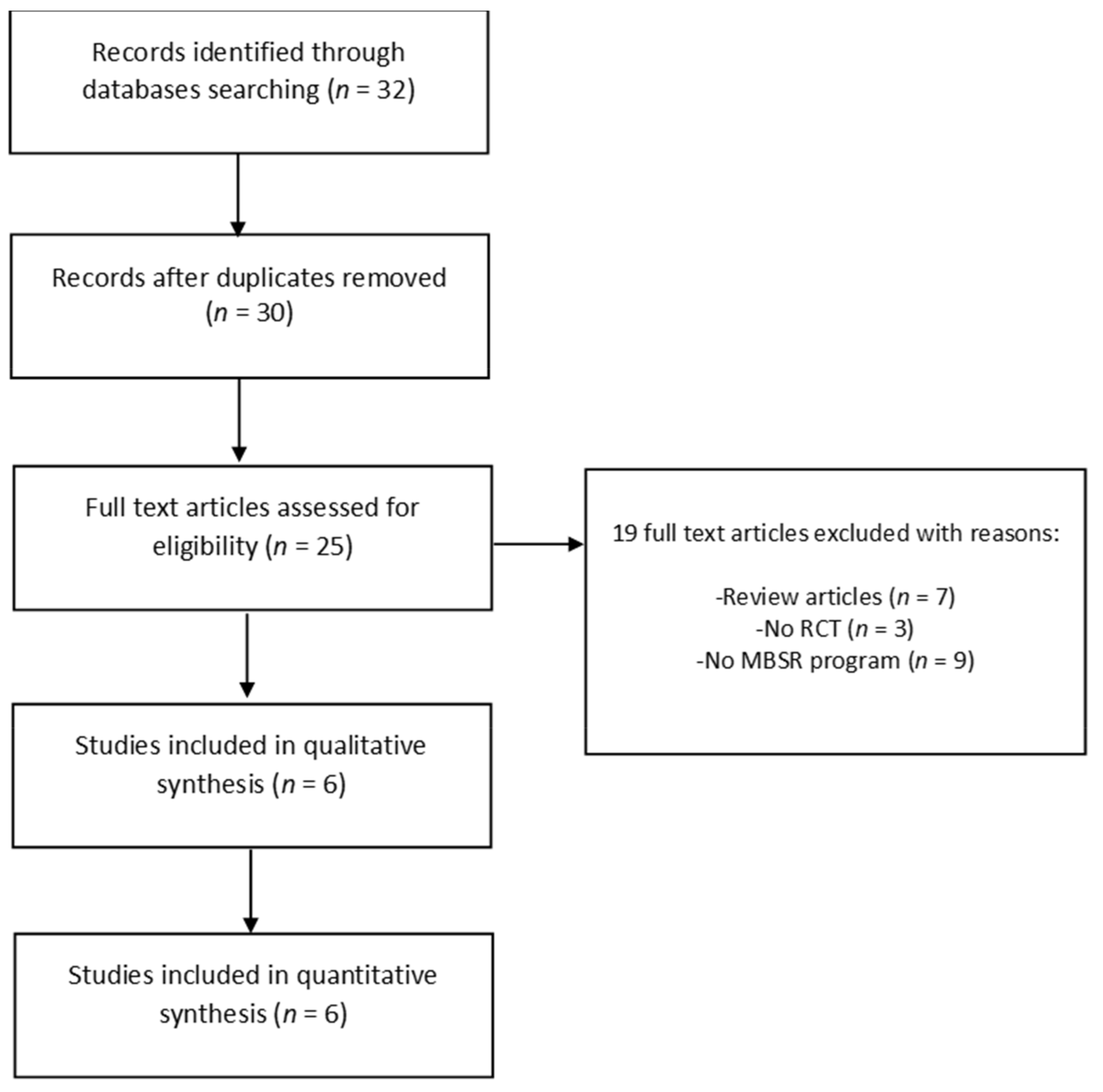
3.3. Study Selection
3.4. Data Extraction and Coding
3.5. Risk of Bias in Individual Studies
3.6. Meta-Analysis
4. Results
4.1. Study Selection
4.2. Study Characteristics
4.3. Participant and Setting Characteristics
4.4. Intervention Characteristics
4.5. Outcome Measures
BP Measures
4.6. Risk of Bias in Individual Studies
4.7. Meta-Analysis: Effects of MBSR versus Control Conditions on BP
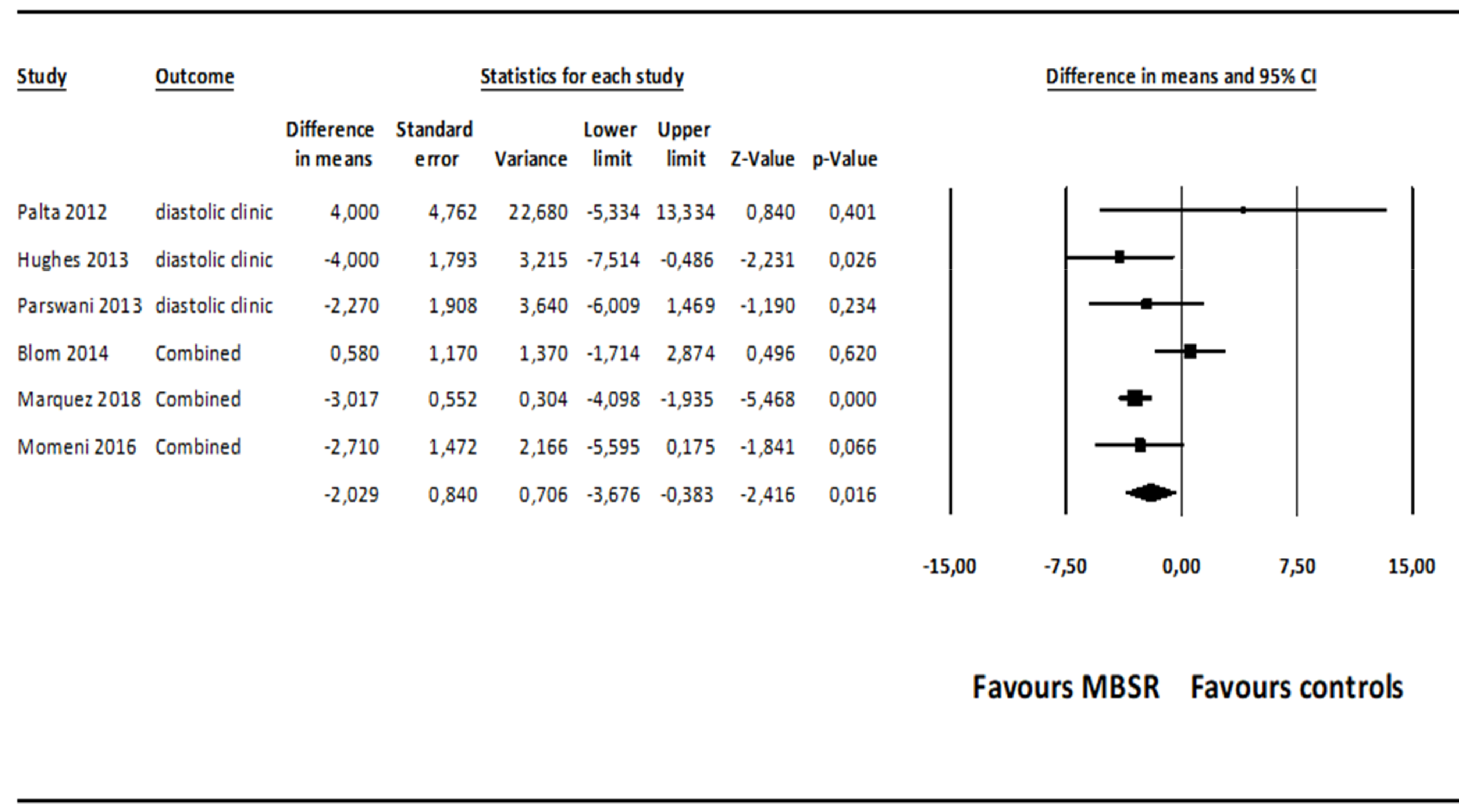
4.7.1. Diastolic BP
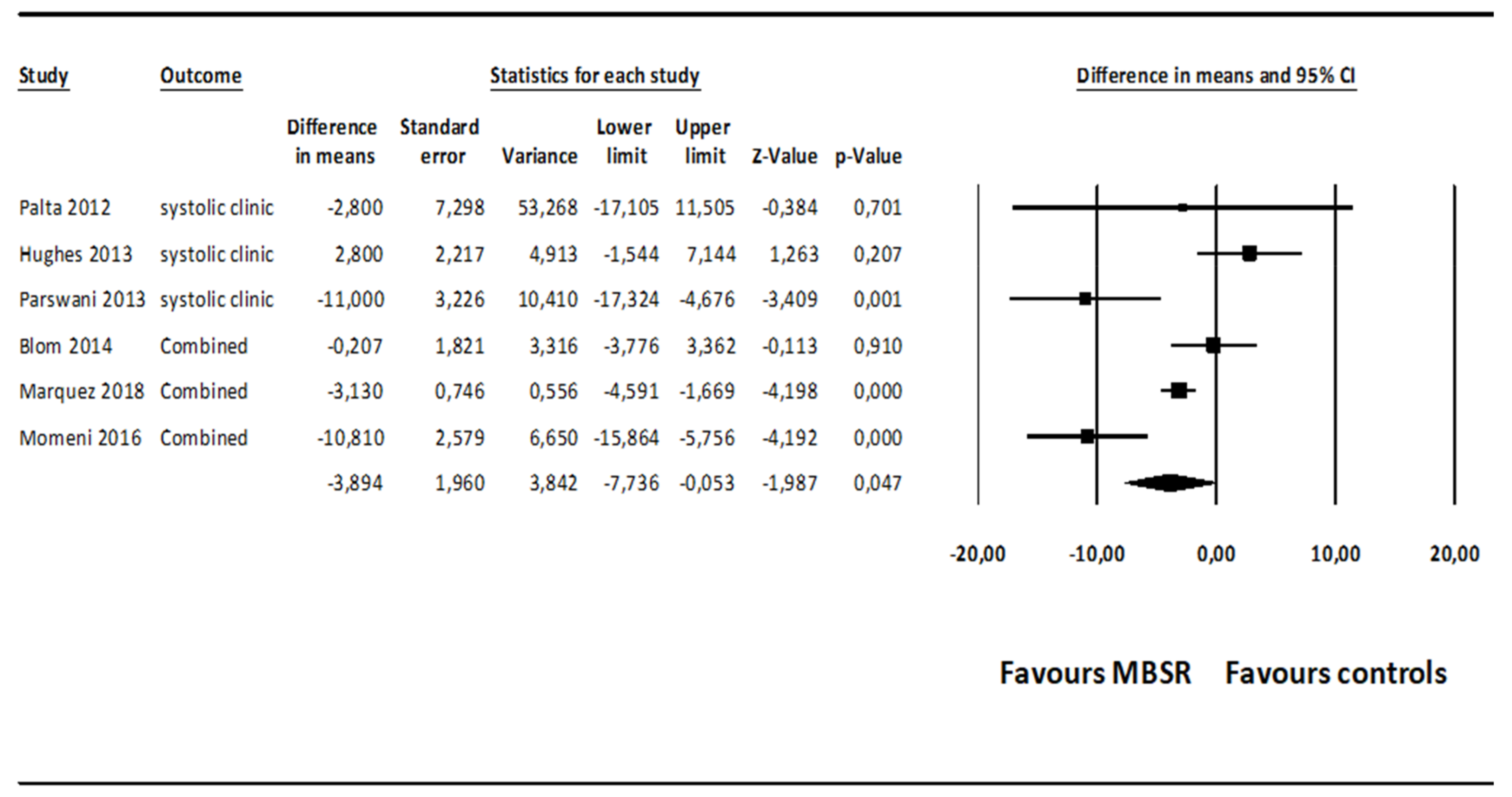
4.7.2. Systolic BP
4.8. Moderator Analyses
5. Discussion
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Health Estimates 2016: Disease Burden by Cause, Age, Sex, by Country and by Region, 2000–2016; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Zanchetti, A.; Christiaens, T.; Dominiczak, A.; Kjeldsen, S.E.; Nilsson, P.M.; Sirnes, P.A. Hipertensión. Hipertens. Riesgo Vasc. 2013, 30, 9–12. [Google Scholar]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.J.T.; et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 Report. JAMA 2003, 289, 2560–2571. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.; Evans, J.; Levy, D. Hypertension in Adults Across the Age Spectrum. Current Outcomes and Control in the Community. ACC Curr. J. Rev. 2005, 14, 22–23. [Google Scholar] [CrossRef]
- Song, J.-J.; Ma, Z.; Wang, J.; Chen, L.-X.; Zhong, J.-C. Gender Differences in Hypertension. J. Cardiovasc. Transl. Res. 2019, 13, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Moran, A.E. Trends in the Prevalence, Awareness, Treatment, and Control of Hypertension Among Young Adults in the United States, 1999 to 2014. Hypertension 2017, 70, 736–742. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.R.; McCormack, T.; Constanti, M.; McManus, R.J. Diagnosis and management of hypertension in adults: NICE guideline update 2019. Br. J. Gen. Pract. 2020, 70, 90–91. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Lunet, N.; Azevedo, A.; Barros, H. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. J. Hypertens. 2009, 27, 963–975. [Google Scholar] [CrossRef]
- Skinner, J.S.; Minhas, R. Commentary on NICE guidance for secondary prevention for patients following a myocardial in-farction. Heart 2007, 93, 864–866. [Google Scholar] [CrossRef] [Green Version]
- McEwen, B.S. Physiology and Neurobiology of Stress and Adaptation: Central Role of the Brain. Physiol. Rev. 2007, 87, 873–904. [Google Scholar] [CrossRef] [Green Version]
- Pozza, A.; Dèttore, D.; Coccia, M.E. Depression and anxiety in pathways of medically assisted reproduction: The role of infertility stress dimensions. Clin. Pract. Epidemiol. Ment. Health 2019, 15, 101–109. [Google Scholar] [CrossRef]
- Gasperin, D.; Netuveli, G.; Dias-da-Costa, J.S.; Pattussi, M.P. Effect of psychological stress on BP increase: A meta-analysis of cohort studies. Cad. Saude Publica 2009, 25, 715–726. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Molloy, G.J.; Stamatakis, E. Psychological distress as a risk factor for cardiovascular events: Pathophysiological and behavioral mechanisms. J. Am. Coll. Cardiol. 2008, 52, 2156–2162. [Google Scholar] [CrossRef] [Green Version]
- Chamik, T.; Viswanathan, B.; Gedeon, J.; Bovet, P. Associations between psychological stress and smoking, drinking, obesity, and high BP in an upper middle-income country in the African region. Stress Health 2018, 34, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iasevoli, M.; Giantin, V.; Voci, A.; Valentini, E.; Zurlo, A.; Maggi, S.; Siviero, P.; Orru, G.; Crepaldi, G.; Pegoraro, R.; et al. Discussing end-of-life care issues with terminally ill patients and their relatives: Comparisons among physicians, nurses and psychologists. Aging Clin. Exp. Res. 2012, 24, 35–42. [Google Scholar]
- Veltri, A.; Scarpellini, P.; Piccinni, A.; Conversano, C.; Giacomelli, C.; Bombardieri, S.; Bazzichi, L.; Dell’Osso, L. Methodological approach to depressive symptoms in fibromyalgia patients. Clin. Exp. Rheumatol. 2012, 30, 136–142. [Google Scholar]
- Dell’Osso, L.; Casu, G.; Carlini, M.; Conversano, C.; Gremigni, P.; Carmassi, C. Sexual obsessions and suicidal behaviors in patients with mood disorders, panic disorder and schizophrenia. Ann. Gen. Psychiatry 2012, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Di Giuseppe, M.; Miniati, M.; Miccoli, M.; Ciacchini, R.; Orrù, G.; Sterzo, R.L.; Di Silvestre, A.; Conversano, C. Defensive responses to stressful life events associated with cancer diagnosis. Mediterr. J. Clin. Psychol. 2012, 8. [Google Scholar] [CrossRef]
- Coin, A.; Najjar, M.; Catanzaro, S.; Orrù, G.; Sampietro, S.; Sergi, G.; Manzato, E.; Perissinotto, E.; Rinaldi, G.; Sarti, S.; et al. A retrospective pilot study on the development of cognitive, behavioral and functional disorders in a sample of patients with early dementia of alzheimer type. Arch. Gerontol. Geriatr. 2009, 49, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Sartori, G.; Zangrossi, A.; Orrù, G.; Monaro, M. Detection of Malingering in Psychic Damage Ascertainment; Ferrara, S., Ed.; Springer International Publishing: Berlin, Germany, 2017; pp. 330–341. [Google Scholar]
- Di Giuseppe, M.; Ciacchini, R.; Micheloni, T.; Bertolucci, I.; Marchi, L.; Conversano, C. Defense mechanisms in cancer patients: A systematic review. J. Psychosom. Res. 2018, 115, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Carmassi, C.; Stratta, P.; Massimetti, G.; Bertelloni, C.A.; Conversano, C.; Cremone, I.M.; Miccoli, M.; Baggiani, A.; Rossi, A.; Dell’Osso, L. New DSM-5 mala-daptive symptoms in PTSD: Gender differences and correlations with mood spectrum symptoms in a sample of high school students following survival of an earthquake. Ann. Gen. Psychiatry 2014, 13, 28. [Google Scholar] [CrossRef]
- Marazziti, D.; Tomaiuolo, F.; Dell’Osso, L.; Demi, V.; Campana, S.; Piccaluga, E.; Guagliumi, G.; Conversano, C.; Baroni, S.; Andreassi, M.G.; et al. Neuropsychological Testing in Interventional Cardiology Staff after Long-Term Exposure to Ionizing Radiation. J. Int. Neuropsychol. Soc. 2015, 21, 670–676. [Google Scholar] [CrossRef]
- Ferretti, F.; Pozza, A.; Bossini, L.; Del Matto, L.; DeSantis, S.; Olivola, M.; Gualtieri, G.; Coluccia, A.; Fagiolini, A. A comparison of physical comorbidities in patients with posttraumatic stress disorder developed after a terrorist attack or other traumatic event. J. Neurosci. Res. 2019, 97, 543–553. [Google Scholar] [CrossRef]
- Porcelli, B.; Pozza, A.; Bizzaro, N.; Fagiolini, A.; Costantini, M.C.; Terzuoli, L.; Ferretti, F. Association between stressful life events and autoimmune diseases: A systematic review and meta-analysis of retrospective case–control studies. Autoimmun. Rev. 2016, 15, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, F.; Pozza, A.; Bossini, L.; DeSantis, S.; Olivola, M.; Del Matto, L.; Gualtieri, G.; Gusinu, R.; Bezzini, D.; Fagiolini, A.; et al. Post-traumatic stress disorder in Italy: A comprehensive evaluation of all the ICD comorbidities and gender-related differences. BMC Res. Notes 2019, 12, 747. [Google Scholar] [CrossRef] [Green Version]
- Tenti, S.; Ferretti, F.; Gusinu, R.; Gallo, I.; Giannotti, S.; Pozza, A.; Fioravanti, A.; Coluccia, A. Impact of thumb osteoarthritis on pain, function, and quality of life: A comparative study between erosive and non-erosive hand osteoarthritis. Clin. Rheumatol. 2020, 39, 2195–2206. [Google Scholar] [CrossRef]
- Mezzacappa, E.S.; Kelsey, R.M.; Katkin, E.S.; Sloan, R.P. Vagal rebound and recovery from psychological stress. Psychosom. Med. 2001, 63, 650–657. [Google Scholar] [CrossRef]
- Brotman, D.J.; Golden, S.H.; Wittstein, I.S. The cardiovascular toll of stress. Lancet 2007, 370, 1089–1100. [Google Scholar] [CrossRef]
- Fugger, G.; Dold, M.; Bartova, L.; Kautzky, A.; Souery, D.; Mendlewicz, J.; Serretti, A.; Zohar, J.; Montgomery, S.; Frey, R.; et al. Comorbid hypertension in patients with major depressive disorder—Results from a European multicenter study. Eur. Neuropsychopharmacol. 2019, 29, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.Y.; Li, N.; Li, W.A.; Khan, H. Association between psychosocial stress and hypertension: A systematic review and me-ta-analysis. Neurol. Res. 2017, 39, 573–580. [Google Scholar] [CrossRef]
- Player, M.S.; Peterson, L.E. Anxiety Disorders, Hypertension, and Cardiovascular Risk: A Review. Int. J. Psychiatry Med. 2011, 41, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Sandström, Y.K.; Ljunggren, G.; Wändell, P.; Wahlström, L.; Carlsson, A.C. Psychiatric comorbidities in patients with hyper-tension–a study of registered diagnoses 2009–2013 in the total population in Stockholm County, Sweden. J. Hypertens. 2016, 34, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Brook, R.D.; Appel, L.J.; Rubenfire, M.; Ogedegbe, G.; Bisognano, J.D.; Elliott, W.J.; Fuchs, F.D.; Hughes, J.W.; Lackland, D.T.; Staffileno, B.A.; et al. Beyond medications and diet: Alternative approaches to lowering blood pressure: A scientific statement from the American Heart Association. Hypertension 2013, 61, 1360–1383. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain and Illness; De-lacourt: New York, NY, USA, 1990. [Google Scholar]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.V.; Abbey, S.; Speca, M.; Velting, D.; et al. Mindfulness: A Proposed Operational Definition. Clin. Psychol. Sci. Pract. 2006, 11, 230–241. [Google Scholar] [CrossRef]
- Reich, R.R.; Lengacher, C.A.; Klein, T.W.; Newton, C.; Shivers, S.; Ramesar, S.; Alinat, C.B.; Paterson, C.; Le, A.; Park, J.Y.; et al. A Randomized Controlled Trial of the Effects of Mindfulness-Based Stress Reduction (MBSR[BC]) on Levels of Inflammatory Biomarkers Among Recovering Breast Cancer Survivors. Biol. Res. Nurs. 2017, 19, 456–464. [Google Scholar] [CrossRef]
- Ellis, D.A.; Carcone, A.; Slatcher, R.; Naar-King, S.; Hains, A.; Graham, A.; Sibinga, E. Efficacy of Mindfulness-Based Stress Reduction in Emerging Adults with Poorly Controlled, Type 1 Diabetes: A Pilot Randomized Controlled Trial. Pediatr. Diabetes 2018, 20, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Khoo, E.-L.; Small, R.; Cheng, W.; Hatchard, T.; Glynn, B.; Rice, D.B.; Skidmore, B.; Kenny, S.; Hutton, B.; Poulin, P.A. Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: A systematic review and network meta-analysis. Évid. Based Ment. Health 2019, 22, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-Y.; Cui, Y.-X.; Zhou, Y.-Q.; Li, Y.-L. Effects of mindfulness-based stress reduction on prenatal stress, anxiety and depression. Psychol. Health Med. 2018, 24, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Hecht, F.M.; Moskowitz, J.T.; Moran, P.; Epel, E.S.; Bacchetti, P.; Acree, M.; Kemeny, M.E.; Mendes, W.B.; Duncan, L.G.; Weng, H.; et al. A randomized, controlled trial of mindfulness-based stress reduction in HIV infection. Brain Behav. Immun. 2018, 73, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Giuseppe, M.; Ciacchini, R.; Piarulli, A.; Nepa, G.; Conversano, C. Mindfulness dispositions and defense style as positive responses to psychological distress in oncology professionals. Eur. J. Oncol. Nurs. 2019, 40, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Di Giuseppe, M.; Miccoli, M.; Ciacchini, R.; Gemignani, A.; Orrù, G. Mindfulness, Age and Gender as Protective Factors Against Psychological Distress During COVID-19 Pandemic. Front. Psychol. 2020, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Conversano, C.; Ciacchini, R.; Orrù, G.; Di Giuseppe, M.; Gemignani, A.; Poli, A. Mindfulness, Compassion, and Self-Compassion Among Health Care Professionals: What’s New? A Systematic Review. Front. Psychol. 2020, 11, 1683. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Gemignani, A.; Conversano, C. Psychological resources against the traumatic experience of COVID-19. Clin. Neuropsychiatry 2020, 17, 85–87. [Google Scholar]
- Orrù, G.; Ciacchini, R.; Gemignani, A.; Conversano, C. Psychological intervention measures during the COVID-19 pandemic. Clin. Neuropsychiatry 2020, 17, 76–79. [Google Scholar]
- Carlson, L.E.; Speca, M.; Faris, P.; Patel, K.D. One year pre–post intervention follow-up of psychological, immune, endocrine and BP outcomes of mindfulness-based stress reduction (MBSR) in breast and prostate cancer outpatients. Brain Behav. Immun. 2007, 21, 1038–1049. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, X.; Wang, L.; Zhang, X. A randomized controlled trial of the effects of brief mindfulness meditation on anxiety symptoms and systolic BP in Chinese nursing students. Nurse Educ. Today 2013, 33, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Rainforth, M.V.; Schneider, R.H.; Nidich, S.I.; Gaylord-King, C.; Salerno, J.W.; Anderson, J.W. Stress reduction programs in patients with elevated BP: A systematic review and meta-analysis. Curr. Hypertens. Rep. 2007, 9, 520. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Han, K.S. BP response to meditation and yoga: A systematic review and meta-analysis. J. Altern. Complement. Med. 2017, 23, 685–695. [Google Scholar] [CrossRef]
- Solano Lopez, A.L. Effectiveness of the Mindfulness-Based Stress Reduction Program on BP: A Systematic Review of Literature. Worldviews Evid. Based Nurs. 2018, 15, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Linee guida per il reporting di revisioni sistematiche e meta-analisi: Il PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Re-lapse; Guildford Press: New York, NY, USA, 2000. [Google Scholar]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009; p. 452. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Egger, M. Regression methods to detect publication and other bias in meta-analysis. In Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; Rothstein, H.R., Sutton, A.J., Borenstein, M., Eds.; Wiley: Chichester, UK, 2005; pp. 99–100. [Google Scholar]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, J.W.; Fresco, D.M.; Myerscough, R.; van Dulmen, M.H.M.; Carlson, L.E.; Josephson, R. Randomized Controlled Trial of Mindfulness-Based Stress Reduction for Prehypertension. Psychosom. Med. 2013, 75, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blom, K.; Baker, B.; How, M.; Dai, M.; Irvine, J.; Abbey, S.; Abramson, B.L.; Myers, M.G.; Kiss, A.; Perkins, N.J.; et al. Hypertension Analysis of Stress Reduction Using Mindfulness Meditation and Yoga: Results From the Harmony Randomized Controlled Trial. Am. J. Hypertens. 2014, 27, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Momeni, J.; Omidi, A.; Raygan, F.; Akbari, H. The effects of mindfulness-based stress reduction on cardiac patients’ BP, per-ceived stress, and anger: A single-blind randomized controlled trial. J. Am. Soc. Hypertens. 2016, 10, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Palta, P.; Page, G.; Piferi, R.L.; Gill, J.M.; Hayat, M.J.; Connolly, A.B.; Szanton, S.L. Evaluation of a mindfulness-based intervention program to decrease BP in low-income African-American older adults. J. Urban Health 2012, 89, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Márquez, P.H.P.; Feliu-Soler, A.; Solé-Villa, M.J.; Matas-Pericas, L.; Filella-Agullo, D.; Ruiz-Herrerias, M.; Soler-Ribaudi, J.; Coll, A.R.-C.; Arroyo-Díaz, J.A. Benefits of mindfulness meditation in reducing blood pressure and stress in patients with arterial hypertension. J. Hum. Hypertens. 2018, 33, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Nyenhuis, D.L.; Yamamoto, C.; Luchetta, T.; Terrien, A.; Parmentier, A. Adult and geriatric normative data and validation of the profile of mood states. J. Clin. Psychol. 1999, 55, 79–86. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Parswani, M.J.; Sharma, M.P.; Iyengar, S.S. Mindfulness-based stress reduction program in coronary heart disease: A ran-domized control trial. Int. J. Yoga 2013, 6, 111. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Tang, Y.; Ge, J.; Liu, Y.; Jin, J.; He, M. Age and Diastolic Blood Pressure Play an Important Role in the Progression of White Matter Lesions: A Meta-Analysis. Eur. Neurol. 2020, 83, 351–359. [Google Scholar] [CrossRef]
- Flint, A.C.; Conell, C.; Ren, X.; Banki, N.M.; Chan, S.L.; Rao, V.A.; Melles, R.B.; Bhatt, D.L. Effect of Systolic and Diastolic Blood Pressure on Cardiovascular Outcomes. N. Engl. J. Med. 2019, 381, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Hilton, L.; Hempel, S.; Ewing, B.A.; Apaydin, E.; Xenakis, L.; Newberry, S.; Colaiaco, B.; Maher, A.R.; Shanman, R.M.; Sorbero, M.E.; et al. Mindfulness Meditation for Chronic Pain: Systematic Review and Meta-analysis. Ann. Behav. Med. 2017, 51, 199–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, H.; Cao, X.; Geng, J.; Chair, S.Y. Effects of mindfulness-based interventions on health-related outcomes for patients with heart failure: A systematic review. Eur. J. Cardiovasc. Nurs. 2020, 19, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Pozza, A.; Di Giuseppe, M.; Conversano, C. The psychosocial impact of COVID-19 pandemic in Italy: A lesson for mental health prevention in the first severely hit European country. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 531–533. [Google Scholar] [CrossRef]
- Biernacka, M.A.; Jakubowska-Winecka, A. Health locus of control as a psychological factor in improving treatment results in adolescents with primary hypertension and diabetes. Health Psychol. Rep. 2017, 1, 20–29. [Google Scholar] [CrossRef]
- Pozza, A.; Osborne, R.H.; Elsworth, G.R.; Ferretti, F.; Coluccia, A. Italian validation of the health education impact question-naire (heiQ) in people with chronic conditions. Health Qual. Life Outcomes 2020, 18, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferretti, F.; Pozza, A.; Pallassini, M.; Righi, L.; Marini, F.; Adami, S.; Coluccia, A. Gender invariance of dignity in non-terminal elderly patients with chronic diseases: A multicentric study. Qual. Quant. 2019, 53, 1645–1656. [Google Scholar] [CrossRef]
- Vaccaro, M.G.; Izzo, G.; Ilacqua, A.; Migliaccio, S.; Baldari, C.; Guidetti, L.; Lenzi, A.; Quattrone, A.; Aversa, A.; Emerenziani, G.P. Characterization of the Effects of a Six-Month Dancing as Approach for Successful Aging. Int. J. Endocrinol. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Barcaccia, B.; Baiocco, R.; Pozza, A.; Pallini, S.; Mancini, F.; Salvati, M. The more you judge the worse you feel. A judgemental attitude towards one’s inner experience predicts depression and anxiety. Personal. Individ. Differ. 2019, 138, 33–39. [Google Scholar] [CrossRef]
- Nigol, S.H.; Di Benedetto, M. The relationship between mindfulness facets, depression, pain severity and pain interference. Psychol. Health Med. 2019, 25, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.; Witkiewitz, K. Dismantling Mindfulness-Based Programs: A Systematic Review to Identify Active Components of Treatment. Mindfulness 2020, 11, 2470–2485. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Publication Date | Country | Inclusion (IC) and Exclusion (EC) Criteria | Study Design | Control Group | BP Assessment Time Points | Recruitment Strategy | Treatment | BP Outcomes | Anxiety, Depression, Stress Outcomes | Total Sample Size (Experimental Group; Control Group) | Diagnosis | PercentAge of Participants on Antihypertensive Agents | Mean Age (SD) | Percentage of Females | Percentage of Participants with Medical Comorbidities | Main Findings |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hughes [61] | 2013 | USA (OH) | IC: age between 30 and 60 years old. EC: being pre-hypertensive, taking antihypertensive medication, being experienced with meditation practices, being current smokers, having any disease (e.g., myocardial infarction, heart failure, chronic kidney disease, diabetes). | RCT | Active control condition including 8 group sessions of progressive muscle relaxation training | (1) PRE-TEST: Initial BP screening administered in a three-week period. (2) PRE-TEST: Clinic and ambulatory BP. (3) POST-TEST: Clinic and ambulatory BP. | Advertisement Participants were enrolled in 7 cohorts ranging in size from 3–11. | MBSR (8 weekly group sessions, each 2.5 h long) | Clinic SBP/DBP (seated BP reading automated oscillometric BP device). Ambulatory SBP and DBP: 24 h monitoring, ambulatory BP device. | Not reported | 56 (28; 28) | Elevated BP in the prehypertensive range (SBP 120–139 mm Hg or DBP 80–89 mm Hg) | 0 | 50.3 (6.5) | Total: 57% IG: 61% CL: 54% | Not specified | MBSR: statistically significant reductions in the primary outcomes of clinic SBP and DBP. MBSR is more effective in lowering elevated BP than an active control (PMR). |
| Blom [62] | 2013 | CANADA (ONT) | IC: aged 20 to 75 years with mean awake ambulatory systolic or diastolic BP ≥ 135/85 mm Hg or mean 24 h ambulatory BP ≥ 130/80 mm Hg (stage 1 hypertension). BP was required to be <160/100 mm Hg on both office and ambulatory measurements. Participants were naive to antihypertensive medication for at least 6 months before the baseline screening visit. | RCT | Wait list | (1) PRE-TEST (24 h ambulatory BP monitoring); (2) POST-TEST: 12 week after baseline (24 h ambulatory BP monitoring). (3) STUDY CLOSE: all participants returned 24 weeks after baseline for a third 24 h ambulatory BP recording. | Participants were recruited from referring physicians, advertisements in local newspapers, and posters at local hospitals. Study subjects were not given incentives for participation in the study but were reimbursed for parking. | MBSR (8 weekly group sessions, each 2.5 h long) | Clinic SBP/DBP (change in awake and 24 h ambulatory BP using an automated office BP measurement device, BpTRU). | Not reported | 101 (50; 51) | Stage 1 hypertension (mean S/DBP ≥ 135/85 mm Hg or mean 24 h ambulatory BP ≥ 130/80 mm Hg) | 0 | IG: 57 (12); CL: 55 (11) | IG: 64% CL: 63% | Not specified | MBSR did not significantly lower ambulatory BP when compared with BP change in a wait-list control group. |
| Momeni [63] | 2016 | IRAN (KASC) | IC: any cardiac diagnosis, suffering from hypertension, receiving antihypertensive agents, not having experienced new heart attacks or cardiac symptoms in the last six months before the study, age ranging from 35 to 60 years, able to participate in the study, high school diploma or higher degrees. EC: suffering from renal problems, diabetes mellitus, or active malignant conditions such as cancer, having a history of convulsion or epilepsy during the last six months prior to the study, being a pregnant or breastfeeding woman, having a history of drug abuse, having received psychological therapies during the month before the study, and having the history of using yoga, meditation, or Zen exercises. | Single-blinded RCT | Wait list | (1) PRE-TEST: DBP and SBP. (2) POST-TEST (same measures). | The study participants were recruited from all cardiac patients referring to a specialized private cardiac clinic located in Kashan, Iran, from April to June 2015. | MBSR (8 weekly group sessions, each 2.5 h long) | Clinic SBP and DBP: auscultatory method and AOBP method | PSS-14 [64] | 60 (30; 30) | Diagnosed cardiac problem | 100 | 47 (7); IG: 49.16 (6.31); CL: 46.16 (6.27) | 42% (IG: 43.3%, CL: 40%) | Coronary artery disease: 65%; Mitral valve replacement: 21%; Other CVD: 13% | Significant difference between the study groups regarding the post-test values of systolic BP, perceived stress. However, the study groups did not differ significantly in terms of diastolic BP |
| Palta [65] | 2012 | USA (MD) | IC: African Americans aged 62 years or older who were living in the building at the time of the baseline interview and had no plans to move. English language specking required. Consent form and baseline questionnaires filled. | RCT | Social support group Two research assistants guided the group by recording attendance and introducing the topic to be discussed by members of the group, but no mindfulness teaching or practices were offered during these meetings. To initiate communication among participants, the research assistants provided pre-planned conversation starters that mirrored the topics in the intervention group. Following the session, participants were offered a fruit and vegetable snack identical to the foods served to the intervention group. | (1) PRE-TEST: demographic information, PSS (Cohen, 1983) and blood pressure measurements with electronic blood pressure machine (2) POST-TEST: blood pressure measurements (same instrument) | Participants were recruited from a low-income senior housing facility in Baltimore City, through informational sessions, flyers, and tabling. This facility had not previously been exposed to any mindfulness programs. All participants were compensated for their time with a $25 gift card upon completion of each survey time point. | ELDERSHINE, mindfulness-based group (8 weekly group session, each 90 min long) | Clinic SBP and DBP | Not reported | 20 (12; 8) | not requested | 90 | IG: 72.3 (4.4) CL: 73.7 (5.8) | 95% | Not specified | Comparing the differences between post-intervention and baseline measurements, individuals in the intervention group exhibited a 16.70 mmHg lower diastolic blood pressure compared to the social support control group and this value was statistically significant (p = 0.003). |
| Màrquez [66] | 2018 | SPAIN | IC: hypertension, EC: medical history of symptomatic heart failure, or left ventricular ejection fraction symptomatic heart failure, cerebrovascular disease or any other condition that might result in death before study completion; patients concomitantly using BP-modifying drugs (cyclosporine, nonsteroidal anti-inflammatory drugs (NSAIDs), steroids, vasoconstrictors, etc.); pregnant women; patients participating in another clinical trial, and patients with previous experience of mindfulness, meditation, yoga, tai chi, chi kung, or similar techniques. | RCT | Active control condition Weekly health education over the same period. | (1) baseline (pre-intervention) visit (2) mid-point visit at week 4 (3) post-intervention visit, at week 8 (4) follow-up visit at week 20 | Recruited from among hospital employees and patients from hypertension unit with high-normal BP or grade 1 hypertension | 8-week MBCT | Clinic and ambulatory SBP, DBP | PSS-10 [64], POMS [67], DASS-21 [68] | 42 | High-normal BP or grade 1 hypertension | 69.9% | 56.5 (7.77) | 52.17% | Not specified | At week 8, the intervention group had statistically significant lower ABPM scores than the control group, health education groups, (124/77 mmHg vs 126/80 mmHg (p < 0.05) and 108/65 mmHg vs 114/69 mmHg (p < 0.05) for 24 h and night-time systolic BP (SBP), respectively) and also had lower clinically measured SBP values (130 mmHg vs 133 mmHg; p = 0.02). At week 20 (follow-up), means were lower in the intervention group (although not statistically significant). Significant post-intervention differences were observed between the two groups, specifically in terms of lower intervention group levels of anxiety (p = 0.02) and stress (p = 0.05), as measured by DASS-21, and of depression (p = 0.02), fatigue (p = 0.03) and confusion (p = 0.02), as measured by the POMS subscales. |
| Parswani [69] | 2013 | INDIA (KARN) | IC: age between 30 and 65 years old, hospitalized or had symptoms of heart disease within the last 1 year and echocardiography test showing ejection fraction >35% with ability to read, write and speak English language. EC: a clinical history suggestive of psychoses, obsessive compulsive disorder, mental retardation, mania, severe depression, neurological or serious medical conditions, and those with previous exposure or currently receiving any psychological intervention. | RCT | Control Group Patients were given health education about coronary heart disease and its management | (1) BASELINE (2) POST INTERVENTION (3) FOLLOW UP | Patients were recruited from the inpatient and outpatient services of St. Johns Medical College and Hospital, Bangalore | MBSR (8 to 10 weekly group sessions, each 1.5 h long) | Clinic SBP and DBP (sphygmomanometer) | HADS [70], PSS [64] | 30 | Coronary heart disease (CHD) | 100 | IG: 47.27 (12.15), CL: 50.60 (8.21) | 0% | Not specified | Systolic BP was significantly lower in the MBSR group than in the TAU group at post-assessment. No significant difference in DBP. The reduction in DBP was maintained at follow-up and patients showed further decrease. The scores of MBSR group on anxiety, depression and overall distress measured by the HADS were significantly lower than the TAU group. Perceived stress reduced significantly within patients of the MBSR group, and there was a significant difference between the two groups on this dimension at the end of the intervention. |
| Selection Bias Domains | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | ||
|---|---|---|---|---|---|---|
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Measures | Incomplete Outcome Bias | Selective Reporting |
| Hughes et al. [61] | ? | ? | ? | ? | + | + |
| Blom et al. [62] | + | − | + | − | + | + |
| Momeni et al. [63] | + | + | + | + | + | + |
| Palta et al. [65] | ? | − | − | ? | + | + |
| Màrquez et al. [66] | ? | ? | ? | ? | − | − |
| Parswani et al. [69] | + | ? | ? | ? | + | + |
| Type of Analysis | Outcome | k | MD | p-Value | 95% CI | I2 | Evidence of Publication Bias |
|---|---|---|---|---|---|---|---|
| Random-effect meta-analyses | |||||||
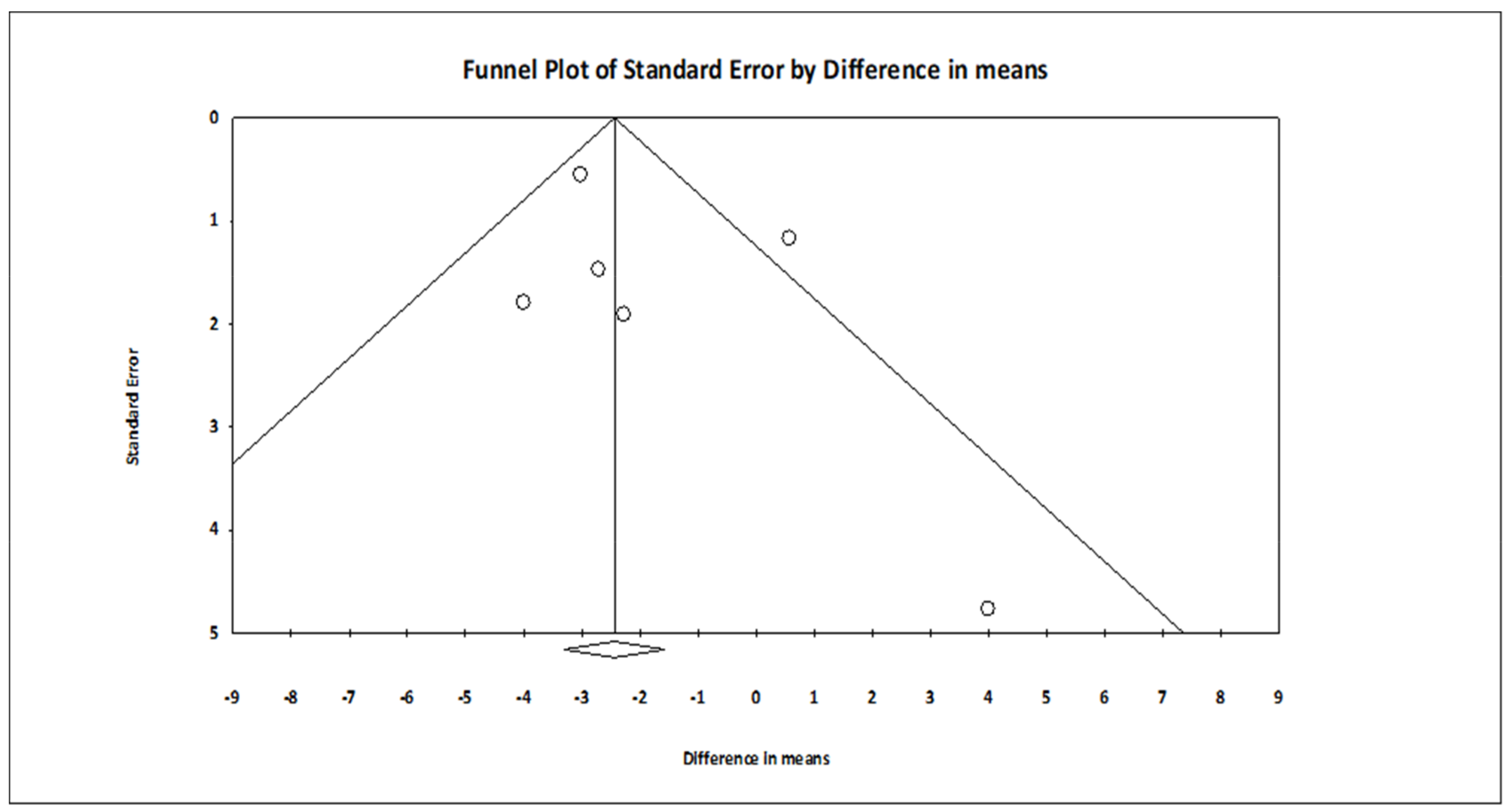
| Pooled effect sizes | Diastolic BP | 6 | −2.029 | 0.016 | −3.676 to 0.383 | 0.000 | No (intercept = 1.060, t(4) = 0.979, p = 0.191) |
| Pooled effect sizes | Systolic BP | 6 | −3.894 | 0.047 | −7.736 to 0.053 | 20.772 | No (intercept = −0.636, t(4) = 0.376, p = 0.362) |
| Sensitivity analyses | |||||||
| Excluding the studies with high risk of bias | Diastolic BP | 3 | −3.057 | 0.000 | −4.030 to −2.084 | 0.000 | No (intercept = −0.305, t(1) = 0.494, p = 0.353) |
| Excluding the studies with high risk of bias | Systolic BP | 3 | −3.544 | 0.232 | −9.359 to 2.271 | 38.879 | No (intercept = −0.448, t(1) = 0.100, p = 0.468) |
| Sensitivity analyses | |||||||
| MBSR versus wait list | Diastolic BP | 2 | −0.944 | 0.565 | −4.159–2.271 | 0.000 | N/A |
| MBSR versus wait list | Systolic BP | 2 | −5.351 | 0.313 | −15.738–5.035 | 0.000 | N/A |
| MBSR versus active control conditions | Diastolic BP | 4 | −2.963 | 0.108 | −3.954–1.973 | 0.000 | No (intercept = 0.748, t(2) = 0.991, p = 0.213) |
| MBSR versus active control conditions | Systolic BP | 4 | −3.218 | 0.197 | −8.304–1.818 | 20.111 | No (intercept = −0.123, t(2) = 0.062, p = 0.478) |
| Moderators (multivariate meta-regression) | Outcome | B | z (p-value) | ||||
| Mean age | Diastolic BP | 6 | 0.175 | 0.94 (0.174) | |||
| Percentage of females | −0.013 | −0.22 (0.411) | |||||
| Percentage of participants on anti-hypertensive medications | −0.015 | −0.74 (.230) | |||||
| Moderators (multivariate meta-regression) | Outcome | ||||||
| Mean age | Systolic BP | 6 | 0.253 | 0.97 (0.165) | |||
| Percentage of females | 0.043 | 0.50 (0.309) | |||||
| Percentage of participants on anti-hypertensive medications | −0.750 | −2.73 (0.003) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conversano, C.; Orrù, G.; Pozza, A.; Miccoli, M.; Ciacchini, R.; Marchi, L.; Gemignani, A. Is Mindfulness-Based Stress Reduction Effective for People with Hypertension? A Systematic Review and Meta-Analysis of 30 Years of Evidence. Int. J. Environ. Res. Public Health 2021, 18, 2882. https://doi.org/10.3390/ijerph18062882
Conversano C, Orrù G, Pozza A, Miccoli M, Ciacchini R, Marchi L, Gemignani A. Is Mindfulness-Based Stress Reduction Effective for People with Hypertension? A Systematic Review and Meta-Analysis of 30 Years of Evidence. International Journal of Environmental Research and Public Health. 2021; 18(6):2882. https://doi.org/10.3390/ijerph18062882
Chicago/Turabian StyleConversano, Ciro, Graziella Orrù, Andrea Pozza, Mario Miccoli, Rebecca Ciacchini, Laura Marchi, and Angelo Gemignani. 2021. "Is Mindfulness-Based Stress Reduction Effective for People with Hypertension? A Systematic Review and Meta-Analysis of 30 Years of Evidence" International Journal of Environmental Research and Public Health 18, no. 6: 2882. https://doi.org/10.3390/ijerph18062882