
Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the COVID-19 Pandemic in Spain

 , , , , ,
, , , , ,  , , , , , , and add
Show full author list
, , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohorts
2.2. Study Participants
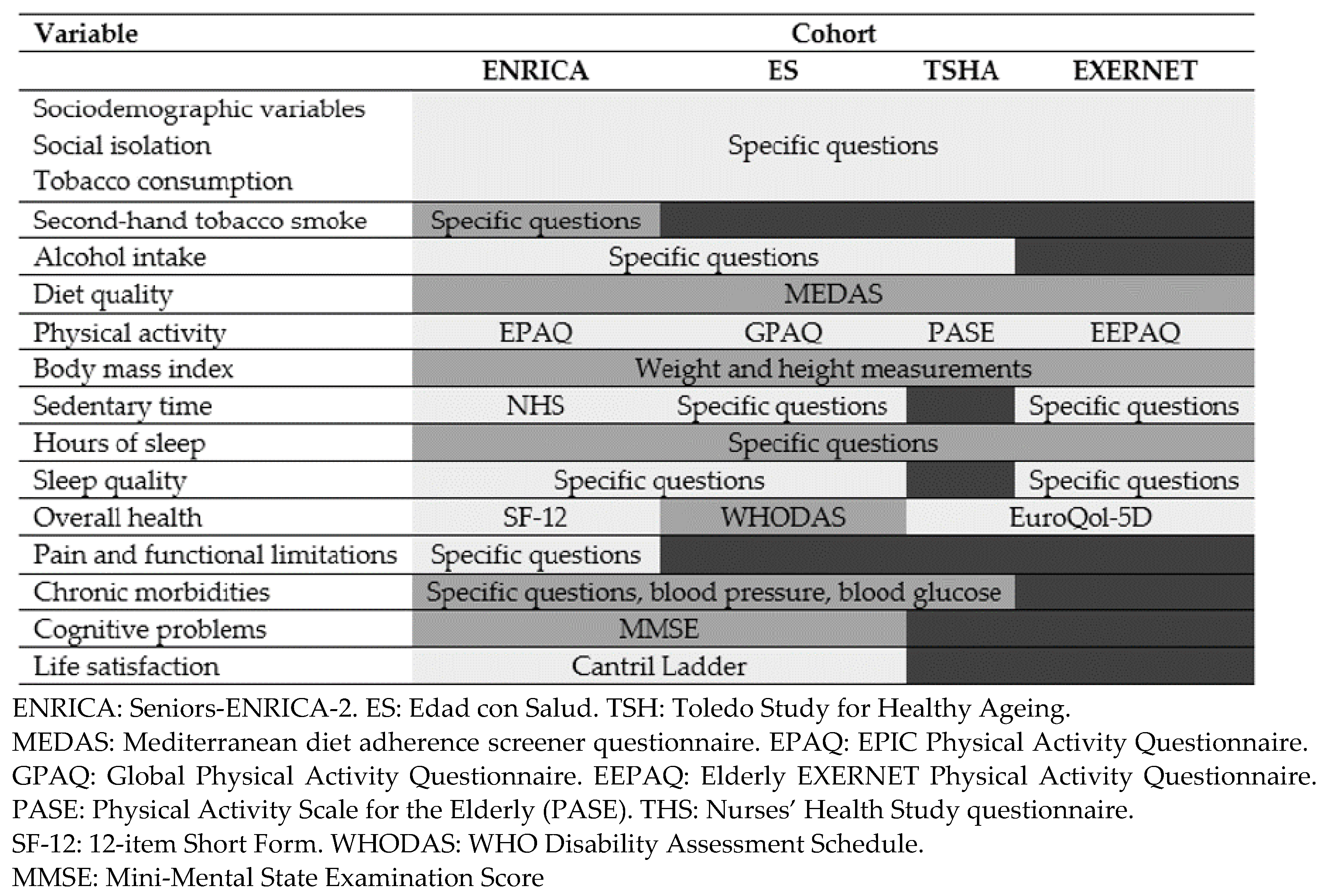
2.3. Study Variables
2.3.1. Baseline Information
2.3.2. Follow-Up Information
2.4. Statistical Analysis
- Changes in alcohol consumption. Participants in ENRICA, ES, and TSHA cohorts were classified into the following categories: (a) drinkers who increased their frequency of consumption (i.e., changed from not daily to daily drinkers); (b) drinkers who decreased their frequency of intake (i.e., changed from daily to not daily or to no consumption at all); (c) drinkers who did not change their frequency of consumption (reference); and (d) non-drinkers who maintained their non-drinking status during confinement.
- Changes in diet quality. A “worsening” (a) and an “improvement” (b) categories were created including individuals who had either decreased or increased, respectively, their MEDAS score ≥ 1 point over follow-up; while a “reference” (c) category classified those who experienced no changes or slight increases/decreases (below 1 point) on this score.
- Changes in weight. Individuals who gained or lost >1 kg were classified into an “increased weight” (a) or “decreased weight” (b) category, respectively, while those who experienced no or small (<1 kg) change in weight were classified into a “maintained weight” or “reference” (c) category.
- Changes in physical activity and sedentary time. Participants in ENRICA, TSHA, and EXERNET cohorts were classified as experiencing: (a) “Unhealthier changes”, if they decreased physical activity or increased sedentary time more than the observed 75th percentile in each cohort; (b) “Healthier (than average or reference) changes”, if they decreased activity or increased sedentary time less than the 25th percentile or if they had slightly increased activity or decreased sedentary time with confinement; and (c) “Average” or “reference” changes if they changed between the 25th and 75th percentile.
- Changes in night-time sleep. The following categories were defined: (a) “Worsening”, those who at baseline had normal sleep and developed short or long sleep with confinement; (b) “Improvement”, those who at baseline had short or long sleep and developed normal sleep during confinement; and (c) “Reference”, those who stayed in the same normal/non-normal sleep category.
- Changes in sleep quality. Finally, older adults in ENRICA, ES, and EXERNET cohorts were classified into: (a) “Worsening”, if they had suffered an increase in the “poor sleep quality” score during confinement; (b) “Improvement”, if they decreased in that score; and (c) “Reference”, if they had no changes.
3. Results
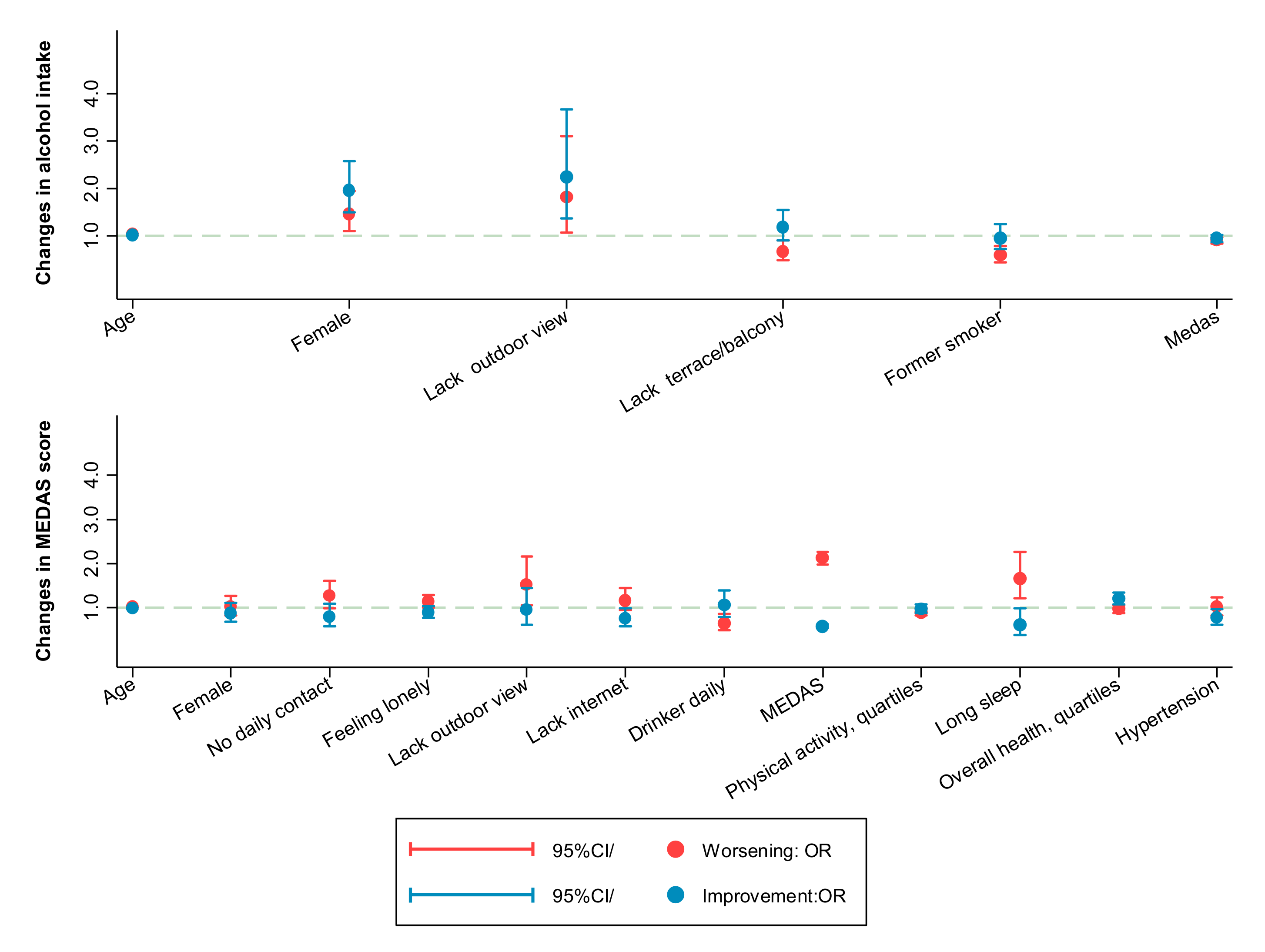
3.1. Changes in Tobacco Exposure, Alcohol Intake, Diet Quality, and Weight
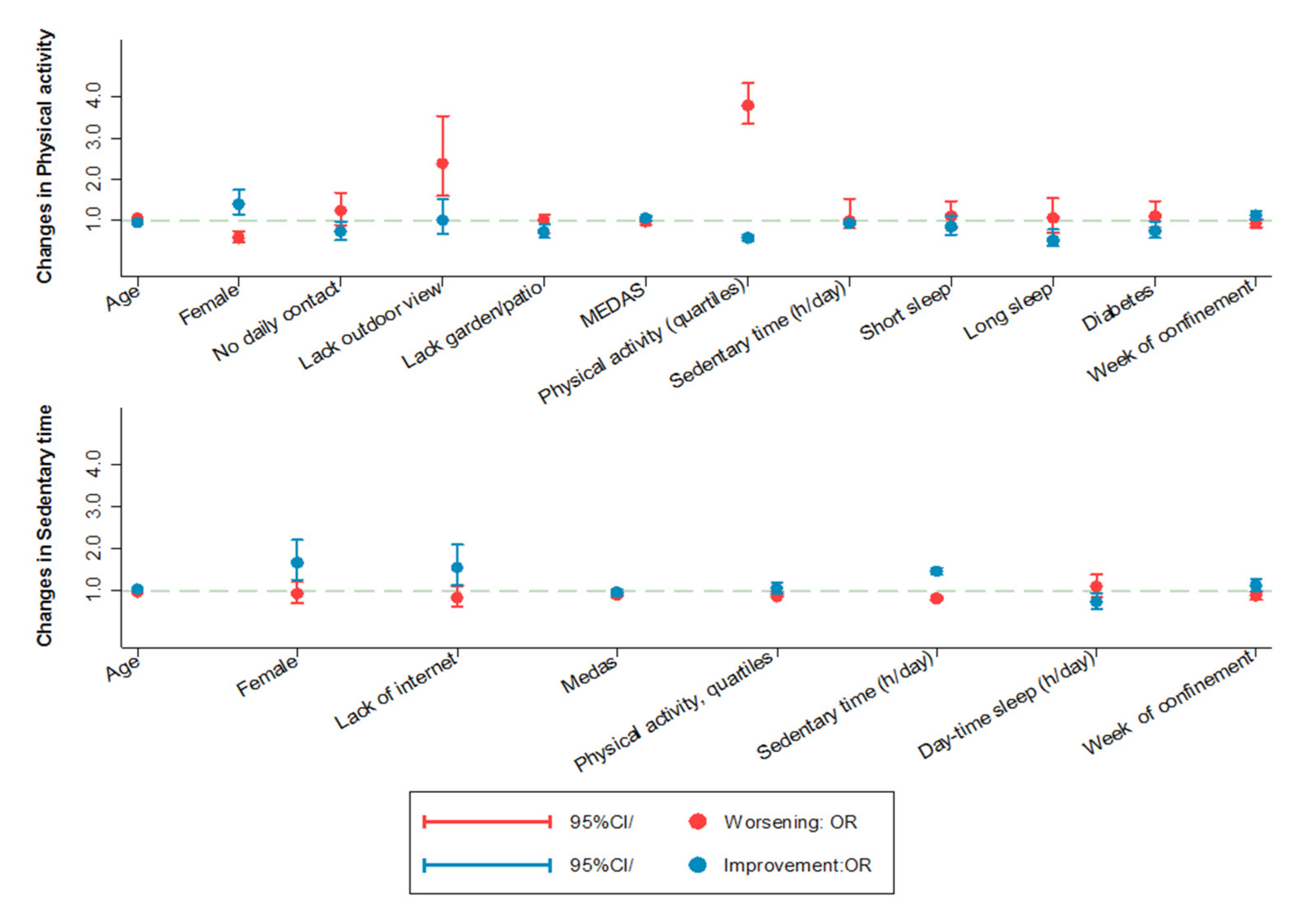
3.2. Changes in Physical Activity and Sedentary Time
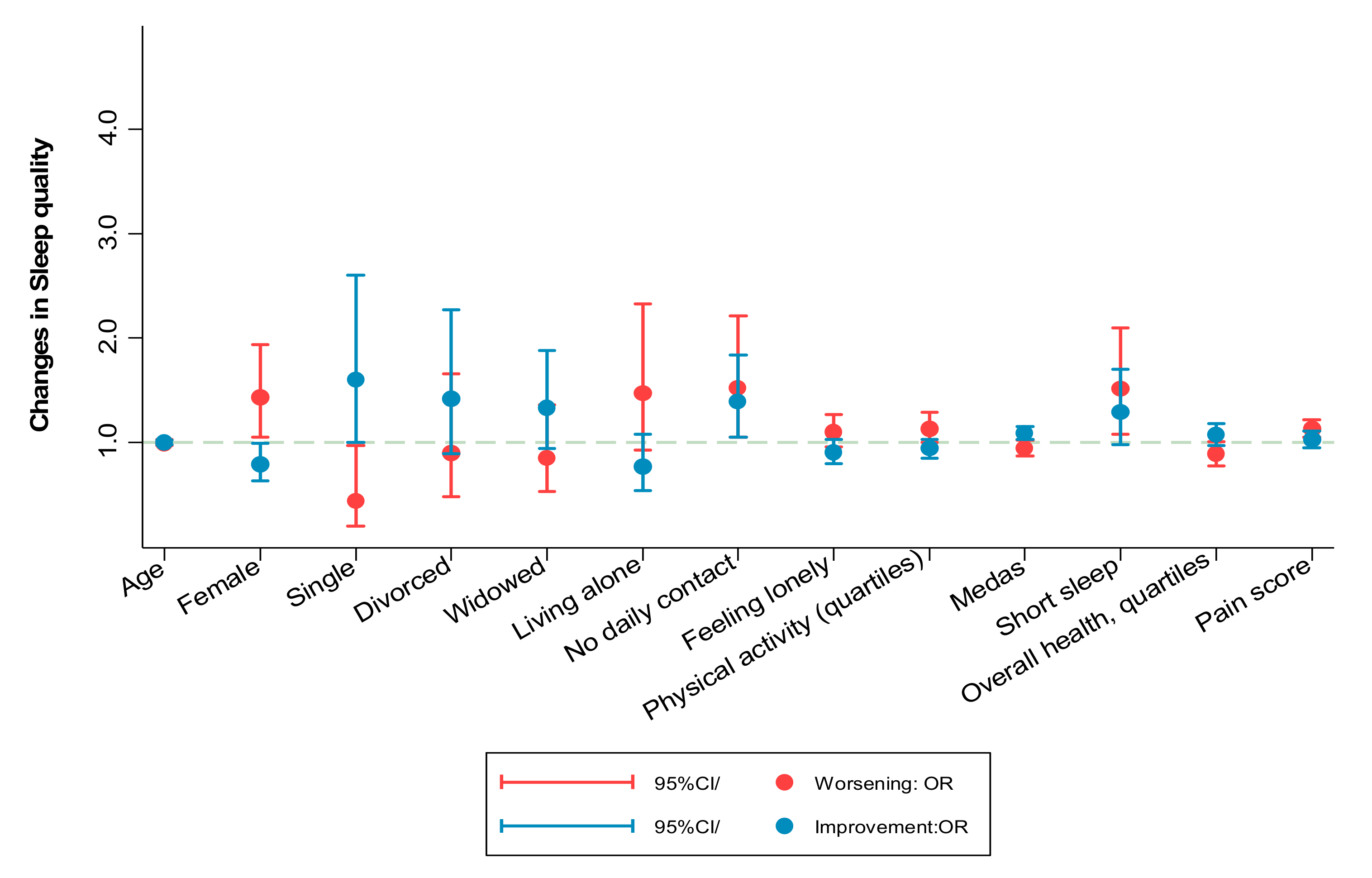
3.3. Changes in Sleep Duration and Sleep Quality
3.4. Changes in Physical and Mental Health and Pain
3.5. Sensitivity Analyses
4. Discussion
Study Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions with the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915. [Google Scholar] [CrossRef] [Green Version]
- International Monetary Fund. World Economic Outlook, October 2020: A Long and Difficult Ascent; International Monetary Fund: Washington, DC, USA, 2020. [Google Scholar]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2020, 75, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, A.; Sampogna, G.; Giallonardo, V.; Del Vecchio, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; et al. Effects of the lockdown on the mental health of the general population during the COVID-19 pandemic in Italy: Results from the COMET collaborative network. Eur. Psychiatry 2020, 63, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, F.; Léger, D.; Fressard, L.; Peretti-Watel, P.; Verger, P. The Coconel Group Covid-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J. Sleep Res. 2021, 30, e13119. [Google Scholar] [CrossRef]
- Real Decreto 463/2020, de 14 de Marzo, Por el Que se Declara el Estado de Alarma para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-3692 (accessed on 1 July 2021).
- Real Decreto 10/2020, de 29 de Marzo, Por el Que se Regula un Permiso Retribuido Recuperable para las Personas Trabaja-Doras por Cuenta Ajena Que No Presten Servicios Esenciales, Con el Fin de Reducir la Movilidad de la Población en el Con-Texto de la Lucha Contra El COVID-19. Available online: https://www.boe.es/buscar/doc.php?id=BOE-A-2020-4166 (accessed on 1 July 2021).
- Justo-Alonso, A.; García-Dantas, A.; González-Vázquez, A.I.; Sánchez-Martín, M.; Del Río-Casanova, L. How did Different Generations Cope with the COVID-19 Pandemic? Early Stages of the Pandemic in Spain. Psicothema 2020, 32, 490–500. [Google Scholar]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Pérez, S.; Masegoso, A.; Hernández-Espeso, N. Levels and variables associated with psychological distress during confinement due to the coronavirus pandemic in a community sample of Spanish adults. Clin. Psychol. Psychother. 2020. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Kapczinski, F.; Cardoso, T.D.A.; Atienza-Carbonell, B.; Rosa, A.R.; Mota, J.C.; De Boni, R.B. The assessment of lifestyle changes during the COVID-19 pandemic using a multidimensional scale. Rev. Psiquiatr. Salud Ment. 2021, 14, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Werneck, A.O.; Silva, D.R.; Malta, D.C.; Lima, M.G.; Souza-Júnior, P.R.; Azevedo, L.O.; Barros, M.B.; Szwarcwald, C.L. The mediation role of sleep quality in the association between the incidence of unhealthy movement behaviors during the COVID-19 quarantine and mental health. Sleep Med. 2020, 76, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Robillard, R.; Dion, K.; Pennestri, M.; Solomonova, E.; Lee, E.; Saad, M.; Murkar, A.; Godbout, R.; Edwards, J.D.; Quilty, L.; et al. Profiles of sleep changes during the COVID-19 pandemic: Demographic, behavioural and psychological factors. J. Sleep Res. 2021, 30, e13231. [Google Scholar] [CrossRef] [PubMed]
- López-Moreno, M.; López, M.T.I.; Miguel, M.; Garcés-Rimón, M. Physical and Psychological Effects Related to Food Habits and Lifestyle Changes Derived from Covid-19 Home Confinement in the Spanish Population. Nutrients 2020, 12, 3445. [Google Scholar] [CrossRef]
- López, J.M.M.; Loaiza, L.I.S.; Belda, B.V.; Cepeda, A.; Cobas, A.C. Food habits in the Galician population during confinement for COVID-19. Nutr. Hosp. 2020, 37, 1190–1196. [Google Scholar] [CrossRef]
- Fernandez-Rio, J.; Cecchini, J.A.; Mendez-Gimenez, A.; Carriedo, A. Weight changes during the COVID-19 home confinement. Effects on psychosocial variables. Obes. Res. Clin. Pract. 2020, 14, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef] [PubMed]
- Marty, L.; de Lauzon-Guillain, B.; Labesse, M.; Nicklaus, S. Food choice motives and the nutritional quality of diet during the COVID-19 lockdown in France. Appetite 2021, 157, 105005. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case. Int. J. Environ. Res. Public Health 2020, 17, 6961. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Real Decreto 900/2020, de 9 de Octubre, por el Que se Declara el Estado de Alarma para Responder Ante Situaciones de Es-Pecial Riesgo por Transmisión no Controlada de Infecciones Causadas por el SARS-CoV-2. Available online: https://www.boe.es/buscar/act.php?id=BOE-A-2020-12109 (accessed on 1 July 2021).
- National Health Interview Survey, Spain; Ministry of Health. 2017. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2017/encuestaResDetall2017.htm (accessed on 1 July 2021).
- García-Esquinas, E.; Carrasco-Rios, M.; Ortolá, R.; Prieto, M.S.; Pérez-Gómez, B.; Gutiérrez-González, E.; Banegas, J.; Queipo, R.; Olmedo, P.; Gil, F.; et al. Selenium and impaired physical function in US and Spanish older adults. Redox Biol. 2021, 38, 101819. [Google Scholar] [CrossRef]
- Olaya, B.; Moneta, M.V.; Lara, E.; Miret, M.; Martín-María, N.; Moreno-Agostino, D.; Ayuso-Mateos, J.L.; Abduljabbar, A.S.; Haro, J.M.; Essau, C.A.; et al. Fruit and Vegetable Consumption and Potential Moderators Associated with All-Cause Mortality in a Representative Sample of Spanish Older Adults. Nutrients 2019, 11, 1794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Garcia, F.J.; Avila, G.G.; Alfaro-Acha, A.; Andres, M.S.A.; Lanza, M.D.L.A.D.L.T.; Aparicio, M.V.E.; Aparicio, S.H.; Zugasti, J.L.L.; Reus, M.G.-S.; Rodriguez-Artalejo, F.; et al. The prevalence of frailty syndrome in an older population from Spain. The Toledo study for healthy aging. J. Nutr. Health Aging 2011, 15, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Bruton, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Vila-Maldonado, S.; Gesteiro, E.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; et al. The effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 4312. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Pols, M.A.; Peeters, P.H.; Ocké, M.C.; Slimani, N.; Bueno-De-Mesquita, H.B.; Collette, H.J. Estimation of reproducibility and relative validity of the questions included in the EPIC Physical Activity Questionnaire. Int. J. Epidemiol. 1997, 26, S181–S189. [Google Scholar] [CrossRef] [Green Version]
- López-Rodríguez, C.; Laguna, M.; Gómez-Cabello, A.; Gusi, N.; Espino, L.; Villa, G.; Pedrero-Chamizo, R.; Casajus, J.; Ara, I.; Aznar, S. Validation of the self-report EXERNET questionnaire for measuring physical activity and sedentary behavior in elderly. Arch. Gerontol. Geriatr. 2017, 69, 156–161. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Logan, S.L.; Gottlieb, B.H.; Maitland, S.B.; Meegan, D.; Spriet, L.L. The Physical Activity Scale for the Elderly (PASE) Questionnaire; Does It Predict Physical Health? Int. J. Environ. Res. Public Health 2013, 10, 3967–3986. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Turner-Bowker, D.M.; Gandek, B. How to Score Version 2 of the Sf-12 Health Survey (with a Supplement Documenting Version 1); Quality Metric Inc. Health Assessment Laboratory: Boston, MA, USA, 2002. [Google Scholar]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; Von Korff, M.; Pull, C. Developing the World Health Organization Disability Assessment Schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef]
- Hernandez, G.; Garin, O.; Pardo, Y.; Vilagut, G.; Pont, A.; Suárez, M.; Neira, M.; Rajmil, L.; Gorostiza, I.; Ramallo-Fariña, Y.; et al. Validity of the EQ–5D–5L and reference norms for the Spanish population. Qual. Life Res. 2018, 27, 2337–2348. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.E.; Waite, L.J.; Hawkley, L.C.; Cacioppo, J.T. A Short Scale for Measuring Loneliness in Large Surveys. Res. Aging 2004, 26, 655–672. [Google Scholar] [CrossRef]
- Rios, M.M.C.D.L.; Ortolá, R.; Rodríguez-Artalejo, F.; García-Esquinas, E. Exposure to secondhand tobacco smoke is associated with reduced muscle strength in US adults. Aging 2019, 11, 12674–12684. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; López-Fontana, C.; Varo, J.J.; Villegas, A.S.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef]
- Leon-Gonzalez, R.; Rodriguez-Artalejo, F.; Ortola, R.; Lopez-Garcia, E.; Garcia-Esquinas, E. Social Network and Risk of Poor Sleep Outcomes in Older Adults: Results from a Spanish Prospective Cohort Study. Nat. Sci. Sleep 2021, 13, 399–409. [Google Scholar] [CrossRef] [PubMed]
- García-Esquinas, E.; Rodríguez-Sánchez, I.; Ortolá, R.; Lopez-Garcia, E.; Caballero, F.F.; Rodríguez-Mañas, L.; Banegas, J.R.; Rodríguez-Artalejo, F. Gender Differences in Pain Risk in Old Age: Magnitude and Contributors. Mayo Clin. Proc. 2019, 94, 1707–1717. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Andrade, E.; Martínez-Gómez, D.; Caballero, F.F.; López-García, E.; Rodríguez-Artalejo, F. Television viewing time as a risk factor for frailty and functional limitations in older adults: Results from 2 European prospective cohorts. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- Lobo, A.; Saz, P.; Marcos, G.; Día, J.L.; de la Cámara, C.; Ventura, T.; Morales, A.F.; Fernando, P.L.; Montanes, J.A.; Aznar, S. Evalidation and standardization of the cognition mini-exam (first Spanish version of the Mini-Mental Status Examination) in the general geriatric population. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Glatzer, W.; Gulyas, J. Cantril Self-Anchoring Striving Scale. In Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Sun, Y.; Li, Y.; Bao, Y.; Meng, S.; Sun, Y.; Schumann, G.; Kosten, T.; Strang, J.; Lu, L.; Shi, J. Brief Report: Increased Addictive Internet and Substance Use Behavior During the COVID-19 Pandemic in China. Am. J. Addict. 2020, 29, 268–270. [Google Scholar] [CrossRef] [PubMed]
- Tabac, Alcool: Quel Impact du Confinement sur la Consommation Des Français? Available online: /presse/2020/tabac-alcool-quel-impact-du-confinement-sur-la-consommation-des-francais (accessed on 1 July 2021).
- Bommelé, J.; Hopman, P.; Walters, B.H.; Geboers, C.; Croes, E.; Fong, G.T.; Quah, A.C.K.; Willemsen, M. The double-edged relationship between COVID-19 stress and smoking: Implications for smoking cessation. Tob. Induc. Dis. 2020, 18, 63. [Google Scholar] [CrossRef]
- Chen, D. The psychosocial impact of the COVID-19 pandemic on changes in smoking behavior: Evidence from a nationwide survey in the UK. Tob. Prev. Cessat. 2020, 6, 1–5. [Google Scholar] [CrossRef]
- Xu, Y.; Li, Z.; Yu, W.; He, X.; Ma, Y.; Cai, F.; Liu, Z.; Zhao, R.; Wang, D.; Guo, Y.-F.; et al. The association between subjective impact and the willingness to adopt healthy dietary habits after experiencing the outbreak of the 2019 novel coronavirus disease (COVID-19): A cross-sectional study in China. Aging 2020, 12, 20968–20981. [Google Scholar] [CrossRef]
- Sánchez-López, M.D.P.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Reliability, external validity and factor structure in the Spanish population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Yesavage, J.A.; Brink, T.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Koopmann, A.; Georgiadou, E.; Kiefer, F.; Hillemacher, T. Did the General Population in Germany Drink More Alcohol during the COVID-19 Pandemic Lockdown? Alcohol Alcohol. 2020, 55, 698–699. [Google Scholar] [CrossRef]
- Tran, T.D.; Hammarberg, K.; Kirkman, M.; Nguyen, H.T.M.; Fisher, J. Alcohol use and mental health status during the first months of COVID-19 pandemic in Australia. J. Affect. Disord. 2020, 277, 810–813. [Google Scholar] [CrossRef]
- Neill, E.; Meyer, D.; Toh, W.L.; Van Rheenen, T.E.; Phillipou, A.; Tan, E.J.; Rossell, S.L. Alcohol use in Australia during the early days of the COVID-19 pandemic: Initial results from the COLLATE project. Psychiatry Clin. Neurosci. 2020, 74, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, C.; Cowell, A.J.; Dowd, W.N. Alcohol Consumption in Response to the COVID-19 Pandemic in the United States. J. Addict. Med. 2020. [Google Scholar] [CrossRef]
- Rossinot, H.; Fantin, R.; Venne, J. Behavioral Changes during COVID-19 Confinement in France: A Web-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 8444. [Google Scholar] [CrossRef]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Ismail, L.C.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Alles, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the COVID-19 lockdown period (March-May 2020): Results from the French NutriNet-Sante cohort study. MedRxiv 2021, 133, 924–938. [Google Scholar]
- Achón, M.; Serrano, M.; García-González, Á.; Alonso-Aperte, E.; Varela-Moreiras, G. Present Food Shopping Habits in the Spanish Adult Population: A Cross-Sectional Study. Nutrients 2017, 9, 508. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Cooper, J.A. COVID-19–Related Home Confinement in Adults: Weight Gain Risks and Opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Constant, A.; Conserve, D.F.; Gallopel-Morvan, K.; Raude, J. Socio-Cognitive Factors Associated With Lifestyle Changes in Response to the COVID-19 Epidemic in the General Population: Results from a Cross-Sectional Study in France. Front. Psychol. 2020, 11, 579460. [Google Scholar] [CrossRef]
- Martínez-De-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown: A longitudinal study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef]
- Vahia, I.V.; Jeste, D.V.; Reynolds, C.F. Older Adults and the Mental Health Effects of COVID-19. JAMA 2020, 324, 2253. [Google Scholar] [CrossRef]
- Delussi, M.; Gentile, E.; Coppola, G.; Prudenzano, A.M.P.; Rainero, I.; Sances, G.; Abagnale, C.; Caponnetto, V.; De Cesaris, F.; Frattale, I.; et al. Investigating the Effects of COVID-19 Quarantine in Migraine: An Observational Cross-Sectional Study from the Italian National Headache Registry (RICe). Front. Neurol. 2020, 11, 597881. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n/Total Participants for Each Variable and Study Cohort | Main Analyses | |||||
|---|---|---|---|---|---|---|
| ENRICA | ES | TSHA | Exernet | Model 1 | Model 2 | |
| Tobacco exposure; RRR (95%CI) † | ||||||
| Former smokers | 521/1323 | 139/464 | 193/829 | 71/425 | 1.33 (1.05; 1.66) | 1.26 (1.00; 1.60) |
| Active smokers | 118/1323 | 73/464 | 56/829 | 7/425 | 1.10 (0.88; 1.38) | 1.01 (0.80; 1.27) |
| Exposure to SHS; OR (95%CI) † | 70/1197 | 3.64 (1.70; 7.80) | 4.13 (1.95; 8.79) | |||
| Daily alcohol intake; RRR (95%CI) † | ||||||
| No | 371/1323 | 135/464 | 84/829 | 1.03 (0.77; 1.37) | 0.68 (0.54; 0.85) | |
| Yes or almost daily | 389/1323 | 78/464 | 229/829 | 1.00 (0.77; 1.31) | 1.17 (0.97; 1.41) | |
| Snack consumption; OR (95%CI) † | 603/1323 | 0.72 (0.60; 0.85) | 0.72 (0.60; 0.85) | |||
| Food to calm anxiety; OR (95%CI) † | 175/1323 | 0.54 (0.40; 0.73) | 0.56 (0.41; 0.76) | |||
| MEDAS index;x changes (95%CI) ‡ | 1323 | 464 | 829 | 425 | −0.53 (−0.61; −0.45) | −0.53 (−0.60; −0.45) |
| Adherence to MEDAS items; OR (95%CI) † | ||||||
| Olive oil preference | 1323 | 464 | 829 | 425 | 3.17 (1.67; 6.01) | 4.27 (1.76; 10.36) |
| ≥4 tbs of olive oil/day | 1323 | 464 | 829 | 425 | 0.47 (0.39; 0.57) | 0.51 (0.42; 0.63) |
| 2 srv vegetables/day | 1323 | 464 | 829 | 425 | 0.38 (0.28; 0.48) | 0.50 (0.39; 0.65) |
| ≥2 srv fruit/day | 1323 | 464 | 829 | 425 | 0.70 (0.59; 0.85) | 0.78 (0.63; 0.96) |
| <2 srv red meat/day | 1323 | 464 | 829 | 425 | 1.30 (1.07; 1.82) | 1.61 (1.21; 2.14) |
| <2 srv butter/day | 1323 | 464 | 829 | 425 | 0.98 (0.73; 1.31) | 1.10 (0.81; 1.49) |
| <1 soda drink/day | 1323 | 464 | 829 | 425 | 1.20 (0.89; 1.63) | 1.34 (0.97; 1.84) |
| ≥7 glasses wine/week | 1323 | 464 | 829 | 425 | 0.65 (0.51; 0.83) | 0.69 (0.53; 0.91) |
| ≥2 srv legumes/week | 1323 | 464 | 829 | 425 | 1.49 (1.23; 1.83) | 2.07 (1.63; 2.63) |
| ≥2 srv fish/week | 1323 | 464 | 829 | 425 | 0.72 (0.60; 0.86) | 0.86 (0.71; 0.99) |
| <2 srv sweets/week | 1323 | 464 | 829 | 425 | 1.24 (1.05; 1.47) | 1.48 (1.23; 1.76) |
| ≥2 srv nuts/week | 1323 | 464 | 829 | 425 | 0.97 (0.81; 1.16) | 1.19 (0.96; 1.47) |
| poultry > red meat | 1323 | 464 | 829 | 425 | 4.07 (3.26; 5.08) | 5.25 (4.05; 6.80) |
| ≥2 srv sofrito/week | 1323 | 464 | 829 | 425 | 0.35 (0.29; 0.42) | 0.33 (0.27; 0.40) |
| Weight;x changes (95%CI) ‡ | 792 | 241 | 313 | 221 | −0.09 (−0.32; 0.14) | −0.57 (−1.29; 0.15) |
| Physical activity;x changes (95%CI) ‡ | ||||||
| Overall (METs h/wk) | 1323 | 425 | −16.35 (−18.08; −14.6) | −17.48 (−18.61; −16.35) | ||
| Recreational (METs h/wk) | 1323 | 425 | −10.95 (−12.02; −9.87) | −11.32 (−12.24; −10.41) | ||
| Household (METs h/wk) | 1323 | 425 | −5.39 (−6.66; −4.12) | −6.04 (−7.11; −4.98) | ||
| PASE score | 832 | −6.42 (−11.14; −1.70) | −16.66 (−19.59; −13.73) | |||
| Sedentary time;x changes (95%CI) ‡ | ||||||
| Overall (min/day) | 1323 | 425 | 91.89 (81.61; 102.1) | 91.68 (81.21; 102.11) | ||
| TV time (min/day) | 1323 | 27.18 (19.56; 34.80) | 27.93 (20.23; 35.63) | |||
| Other screen time (min/day) | 1319 | 50.20 (45.57; 54.83) | 50.60 (45.83; 55.44) | |||
| Reading (min/day) | 1323 | 16.30 (12.34; 20.25) | 15.53 (11.37; 19.58) | |||
| Listening to music (min/day) | 1323 | 7.52 (4.61; 10.43) | 7.25 (4.26; 10.24) | |||
| Sleep characteristics;x changes (95%CI) ‡ | ||||||
| Hours/night-time sleep | 1323 | 464 | 829 | 425 | −0.02 (−0.08; 0.04) | −0.00 (−0.06; 0.05) |
| Minutes/day-time sleep | 1317 | 421 | −12.50 (−14.18; −10.8) | −12.08 (−13.73; −10.43) | ||
| Poor sleep quality score | 1289 | 430 | 395 | 0.13 (0.10; 0.16) | 0.12 (0.09; 0.15) | |
| Nº poor sleep indicators | 1285 | 0.06 (−0.02; 0.14) | 0.08 (0.00; 0.15) | |||
| Overall health §; x changes (95%CI) | ||||||
| SF-12, PCS ‡ | 1311 | 5.03 (4.45; 5.60) | 4.79 (4.72; 5.38) | |||
| SF-12, MCS ‡ | 1311 | −1.20 (−1.80; −0.58) | −1.19 (−1.81; −0.58) | |||
| WHODAS-12 | 464 | 2.57 (1.29; 3.84) | −0.18 (−1.85; 1.48) | |||
| Pain scale;x changes (95%CI) ‡ | 1296 | 0.17 (0.06; 0.30) | 0.18 (0.05; 0.30) | |||
| Changes in Physical Component Score | Changes in Mental Component Score | Changes in WHODAS-12 | Changes in Pain Scale † | |
|---|---|---|---|---|
| x (95%CI); n = 1243 | x (95%CI); n = 1243 | x (95%CI); n = 1460 | x (95%CI); n = 983 | |
| Sociodemographic factors | ||||
| Age, yr | −0.19 (−0.29; −0.08) | 0.12 (0.00; 0.23) | 0.14 (−0.05; 0.33) | 0.01 (−0.01; 0.04) |
| Female | −0.16 (−1.21; 0.89) | −2.46 (−3.65; −1.35) | −0.93 (−3.73; 1.88) | 0.28 (0.03; 0.51) |
| Education | ||||
| Primary or less | Ref. | Ref. | Ref. | Ref. |
| Secondary | −0.17 (−1.28; 0.93) | 0.18 (−1.02; 1.38) | −0.63 (−3.57; 2.32) | −0.05 (−0.31; 0.21) |
| University | 0.90 (−0.20; 1.99) | 0.11 (−1.08; 1.31) | −4.12 (−7.70; −0.53) | −0.13 (−0.30; 0.12) |
| Civil status | ||||
| Married | Ref. | Ref. | Ref. | Ref. |
| Single | −0.74 (−2.74; 1.25) | 2.16 (0.00; 4.33) | 2.68 (−3.82; 9.28) | 0.29 (−0.19; 0.76) |
| Divorced | −0.02 (−2.05; 2.01) | 0.94 (−1.26; 3.15) | 1.80 (−2.78; 6.39) | 0.20 (−0.31; 0.70) |
| Widowed | −0.75 (−2.20; 0.69) | 1.24 (−0.33; 2.81) | −1.79 (−6.04; 2.45) | 0.14 (−0.21; 0.49) |
| Living alone | 0.74 (−0.72; 2.20) | −1.40 (−3.00; 0.09) | −0.10 (−4.06; 3.87) | −0.12 (−0.48; 0.23) |
| No daily contact with family/friends other than cohabitants | 0.23 (−1.04; 1.50) | −0.24 (−1.62; 1.14) | 0.46 (−2.24; 3.17) | 0.06 (−0.05; 0.18) |
| Feeling lonely | 0.22 (−0.26; 0.70) | −1.02 (−1.54; −0.50) | 0.37 (−0.78; 1.52) | 0.06 (−0.05; 0.18) |
| Housing conditions | ||||
| Lack of outdoor views | 0.40 (−1.12; 1.92) | −0.94 (−2.60; 0.71) | 3.29 (−0.93; 7.51) | 0.14 (−0.22; 0.50) |
| Lack of terrace/balcony | 0.27 (−0.69; 1.21) | 0.23 (−0.80; 1.27) | −1.95 (−4.56; 0.66) | −0.05 (−0.28; 0.18) |
| Lack of garden/yard | −1.38 (−2.60; −0.16) | −0.44 (1.78; 0.89) | −1.09 (3.77; 1.60) | 0.02 (−0.28; 0.18) |
| No internet access | 0.45 (−0.66; 1.56) | −0.50 (−1.70; 0.70) | 1.61 (−1.62; 4.84) | −0.02 (−0.28; 0.24) |
| Too much noise | 1.62 (−1.18; 4.42) | −5.05 (−8.10; −2.00) | −0.00 (−5.80; 5.79) | 0.74 (0.10; 1.38) |
| Lifestyle behaviors | ||||
| Smoking | ||||
| Never smokers | Ref. | Ref. | Ref. | Ref. |
| Former smokers | 0.12 (−0.83; 1.08) | 0.22 (−0.81; 1.26) | −1.93 (−4.88; 1.03) | 0.05 (−0.17; 0.27) |
| Smoker | 0.10 (−1.42; 1.61) | −0.62 (−2.27; 1.03) | 0.95 (−2.73; 4.62) | −0.13 (−0.48; 0.22) |
| Alcohol intake | ||||
| Not drinker | Ref. | Ref. | Ref. | Ref. |
| Drinker, not daily | −0.05 (−1.08; 0.99) | −0.23 (−1.36; 0.90) | −0.02 (−2.92; 2.88) | 0.03 (−0.21; 0.28) |
| Drinker, daily/almost daily | −0.15 (−2.22; 0.92) | −0.33 (−1.49; 0.84) | −0.94 (−4.60; 2.72) | 0.08 (−0.17; 0.33) |
| MEDAS | −0.02 (−0.27; 0.23) | 0.11 (−0.16; 0.38) | −0.28 (−0.98; 0.42) | 0.06 (−0.00; 0.12) |
| PA (cohort-specific quartiles) | ||||
| 1st quartile (less) | Ref. | Ref. | Ref. | Ref. |
| 2nd quartile | 0.58 (−0.59; 1.75) | −0.74 (−2.01; 0.53) | −2.64 (−6.07; 0.79) | 0.06 (−0.22; 0.33) |
| 3rd quartile | 1.61 (0.40; 2.83) | −1.05 (−2.34; 0.28) | −5.48 (−8.92; −2.02) | −0.12 (−0.40; 0.16) |
| 4th quartile | 1.03 (−0.25; 2.31) | −1.35 (−2.75; 0.05) * | −4.20 (−7.90; −0.49) * | −0.02 (−0.32; 0.28) |
| BMI | ||||
| Normoweight | Ref. | Ref. | Ref. | Ref. |
| Overweight | −0.11 (−1.10; 0.89) | 0.05 (−1.03; 1.13) | −1.23 (−4.20; 1.75) | −0.14 (−0.37; 0.09) |
| Obese | −0.14 (−1.38; 1.10) | −0.29 (−1.64; 1.06) | −1.18 (−4.47; 2.10) | −0.05 (−0.34; 0.24) |
| ST (cohort-specific quartiles) | ||||
| 1st quartile (less time) | Ref. | Ref. | Ref. | Ref. |
| 2nd quartile | −0.31 (−1.48; 0.86) | −0.55 (−1.83; 0.71) | 0.32 (−3.05; 3.68) | 0.24 (−0.04; 0.51) |
| 3rd quartile | −0.26 (−0.89; 1.41) | −1.06 (−2.31; 0.19) | −0.39 (−3.62, 2.85) | −0.06 (−0.33; 0.21) |
| 4th quartile | −0.53 (−1.71; 0.64) | −0.16 (−1.43; 1.12) | 3.39 (−0.38; 7.15) | −0.03 (−0.31; 0.25) |
| Sleep characteristics | ||||
| Hours of night-time sleep | ||||
| Normal sleep | Ref. | Ref. | Ref. | Ref. |
| Short sleep (≤6 h) | −0.62 (−1.76; 0.51) | −0.04 (−1.27; 1.19) | 1.03 (−2.65; 4.70) | 0.46 (0.19; 0.73) |
| Long sleep (≥9 h) | 0.67 (−1.34; 2.68) | −1.32 (−3.51; 0.87) | −1.76 (−5.62; 2.11) | −0.29 (−0.76; 0.17) |
| Hours of day-time sleep ‡ | ||||
| None | Ref. | Ref. | − | Ref. |
| Short nap (≤30 min) | 0.04 (−0.93; 1.01) | −1.15 (−2.20; −0.10) | −0.11 (−0.34; 0.11) | |
| Long nap (30–60 min) | −0.81 (−2.08; 0.46) | 0.50 (−0.87; 1.87) | −0.04 (−0.34; 0.25) | |
| Very long nap (≥60min) | 1.26 (−1.74; 2.27) | −2.49 (−4.66; −0.33) | −0.19 (−0.66; 0.27) | |
| Overall sleep quality | ||||
| Very good | −0.47 (−1.81; 0.87) | 2.09 (0.64; 3.53) | −0.58 (−3.20; 2.05) | 0.04 (−0.27; 0.35) |
| Good | Ref. | Ref. | Ref. | Ref. |
| Fair | −0.65 (−1.73; 0.44) | −1.92 (−3.01; −0.75) | 3.15 (−1.38; 7.68) | 0.18 (−0.08; 0.43) |
| Poor/very poor | −4.04 (−7.07; −1.02) * | 0.49 (−2.78; 3.77) | −3.79 (−16.7; 9.10) | −0.04 (−0.83; 0.75) |
| Health-related variables | ||||
| Overall health | − | − | − | |
| 1st quartile | Ref. | |||
| 2nd quartile | −0.46 (−0.80; −0.13) | |||
| 3rd quartile | −0.56 (−0.92; −0.22) | |||
| 4th quartile (best) | −0.64 (−1.00; −0.27) † | |||
| Chronic morbidities | ||||
| Diabetes | 0.56 (−0.54; 1.67) | −0.22 (−1.42; 0.30) | 0.32 (−3.02; 3.67) | −0.05 (−0.32; 0.22) |
| Hypertension | −0.22 (−1.08; 0.64) | −0.55 (−1.49; 0.39) | −0.30 (−2.83; 2.23) | 0.05 (−0.15; 0.25) |
| CVD‡ | −2.53 (−4.72; −0.34) | 0.98 (−1.41; 3.36) | −0.59 (−4.52; 3.33) | 0.24 (−0.22; 0.49) |
| Cancer‡ | −1.98 (−3.76; −0.20) | −0.81 (−2.75; 1.13) | 0.84 (−3.21; 4.89) | 0.19 (−0.27; 0.66) |
| Osteo-muscular disease | −0.69 (−1.58; 0.21) | 0.33 (−0.65; 1.30) | 2.49 (−0.13; 5.10) | 0.57 (0.36; 0.79) |
| Depression | −1.87 (−3.39; −0.34) | −1.36 (−3.91; 0.30) | 0.88 (−4.50; 13.05) | 0.30 (0.00; 0.65) |
| Mobility limitations | −2.37 (−3.49; 1.25) | −1.67 (−2.90; −0.44) | 0.25 (0.01; 0.50) | |
| Negative aging experience scale | −0.16 (−0.58; 0.26) | −0.85 (−1.31; −0.40) | 0.02 (−0.08; 0.12) | |
| Cantril Ladder | 0.28 (0.03; 0.52) | 0.20 (−0.06; 0.47) | −0.11 (−0.16; −0.05) | |
| Low MMSE score (<23) | 1.59 (−1.16; 4.34) | −3.24 (−6.23; −0.26) | 0.18 (−0.52; 0.88) | |
| Years since baseline examination | −0.50 (−1.46; 0.47) | 0.48 (−0.57; 1.54) | 0.50 (−1.46; 0.47) | −0.23 (−0.46; −0.00) |
| Week of the State of Alarm | −0.64 (−1.07; −0.20) | 0.99 (0.52; 1.46) | 0.39 (−0.67; 1.45) | 0.10 (0.00; 0.20) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Esquinas, E.; Ortolá, R.; Gine-Vázquez, I.; Carnicero, J.A.; Mañas, A.; Lara, E.; Alvarez-Bustos, A.; Vicente-Rodriguez, G.; Sotos-Prieto, M.; Olaya, B.; et al. Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the COVID-19 Pandemic in Spain. Int. J. Environ. Res. Public Health 2021, 18, 7067. https://doi.org/10.3390/ijerph18137067
García-Esquinas E, Ortolá R, Gine-Vázquez I, Carnicero JA, Mañas A, Lara E, Alvarez-Bustos A, Vicente-Rodriguez G, Sotos-Prieto M, Olaya B, et al. Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the COVID-19 Pandemic in Spain. International Journal of Environmental Research and Public Health. 2021; 18(13):7067. https://doi.org/10.3390/ijerph18137067
Chicago/Turabian StyleGarcía-Esquinas, Esther, Rosario Ortolá, Iago Gine-Vázquez, José A. Carnicero, Asier Mañas, Elvira Lara, Alejandro Alvarez-Bustos, German Vicente-Rodriguez, Mercedes Sotos-Prieto, Beatriz Olaya, and et al. 2021. "Changes in Health Behaviors, Mental and Physical Health among Older Adults under Severe Lockdown Restrictions during the COVID-19 Pandemic in Spain" International Journal of Environmental Research and Public Health 18, no. 13: 7067. https://doi.org/10.3390/ijerph18137067