
Prognostic Value of Preoperative Serum Levels of Periostin (PN) in Early Breast Cancer (BCa)


Abstract
:1. Introduction
2. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Patients (%) |
|---|---|
| Age at surgery, years | |
| Median (range) | 58 (31–84) |
| Menopausal status | |
| Pre-menopausal | 58 (31.9) |
| Post-menopausal | 124 (68.1) |
| Tumor size: cm in diameter | |
| ≤2 | 89 (48.9) |
| >2 | 93 (51.1) |
| Stage | |
| I | 69 (37.9) |
| II | 76 (41.8) |
| III | 37 (20.3) |
| ER status | |
| Poor (<10% of stained cells) | 40 (22.0) |
| Rich (≥10% of stained cells) | 142 (78.0) |
| PgR status | |
| Poor (<10% of stained cells) | 80 (44.0) |
| Rich (≥10% of stained cells) | 102 (56.0) |
| Ki-67 | |
| Low (<14% stained cells) | 85 (46.7) |
| High (≥14% stained cells) | 97 (53.3) |
| HER2 status | |
| Negative | 166 (91.2) |
| Positive | 16 (8.8) |
| Phenotype * | |
| Luminal A | 60 (33.1) |
| Luminal B (HER2-neg) | 73 (40.1) |
| Luminal B (HER2-pos) | 9 (4.9) |
| HER2 positive (non-luminal) | 7 (3.8) |
| Triple negative | 33 (18.1) |
| Adjuvant systemic therapy ** | |
| Delivered | 104 (57.1) |
| Undelivered | 78 (42.9) |
| PN epithelial (E) expression | |
| 0% immunostained cells | 111 (61.0) |
| ≥1% immunostained cells | 71 (39.0) |
| PN stromal (S) expression | |
| <90% immunostained cells | 94 (51.6) |
| ≥90% immunostained cells | 88 (48.4) |
| E/S PN expression | |
| E ≥ 1% S < 90% | 31 (17.0) |
| E = 0 S < 90% | 63 (34.6) |
| E = 0 S ≥ 90% | 48 (26.4) |
| E ≥ 1% S ≥ 90% | 40 (22.0) |
2.1. Correlation of Serum PN Level with Clinical Pathological Features and Tissue PN Expression
| Variables | ≤219 pg/mL (%) | >219 pg/mL (%) | p |
|---|---|---|---|
| Median age at surgery, years | |||
| ≤58 | 57 (62.6) | 38 (41.8) | |
| >58 | 34 (37.4) | 53 (58.2) | 0.005 |
| Menopausal status | |||
| Pre-menopausal | 32 (35.2) | 26 (28.6) | |
| Post-menopausal | 59 (64.8) | 65 (71.4) | 0.3 |
| Tumor size: cm in diameter | |||
| ≤2 | 45 (49.5) | 44 (48.4) | |
| >2 | 46 (50.5) | 47 (51.6) | 0.8 |
| Stage | |||
| I | 33 (36.3) | 36 (39.6) | |
| II | 40 (44.0) | 36 (39.6) | |
| III | 18 (19.7) | 19 (20.8) | 0.8 |
| Nodal status | |||
| Node-negative | 44 (48.4) | 49 (53.8) | |
| Node-positive | 47 (51.6) | 42 (46.2) | 0.4 |
| ER status | |||
| Poor (<10% of stained cells) | 24 (26.4) | 16 (17.6) | |
| Rich (≥10% of stained cells) | 67 (73.6) | 75 (82.4) | 0.1 |
| PgR status | |||
| Poor (<10% of stained cells) | 48 (52.7) | 32 (35.2) | |
| Rich (≥10% of stained cells) | 43 (47.3) | 59 (64.8) | 0.02 |
| Ki-67 | |||
| Low (<14% stained cells) | 42 (46.2) | 43 (47.3) | |
| High (≥14% stained cells) | 49 (53.8) | 48 (52.7) | 0.8 |
| HER2 status | |||
| Negative | 81 (89.0) | 85 (93.4) | |
| Positive | 10 (11.0) | 6 (6.6) | 0.3 |
| Phenotype * | |||
| Luminal A + Luminal B (HER2-neg) | 25 (27.5) | 35 (38.5) | |
| Others ** | 66 (72.5) | 56 (61.5) | 0.1 |
| Adjuvant systemic therapy *** | |||
| Undelivered | 32 (35.2) | 46 (50.5) | 0.04 |
| Delivered | 59 (64.8) | 45 (49.5) | |
| PN epithelial (E) expression | |||
| 0% immunostained cells | 57 (62.6) | 54 (59.3) | |
| ≥1% immunostained cells | 34 (37.4) | 37 (40.7) | 0.6 |
| PN stromal (S) expression | |||
| <90% immunostained cells | 46 (50.5) | 48 (52.7) | |
| ≥90% immunostained cells | 45 (49.5) | 43 (47.3) | 0.7 |
| E/S PN expression | |||
| E ≥ 1% S < 90% | 15 (16.5) | 16 (17.6) | |
| E = 0 S < 90% | 31 (34.1) | 32 (35.2) | |
| E = 0 S ≥ 90% | 26 (28.6) | 22 (24.1) | |
| E ≥ 1% S ≥ 90% | 19 (20.8) | 21 (23.1) | 0.9 |
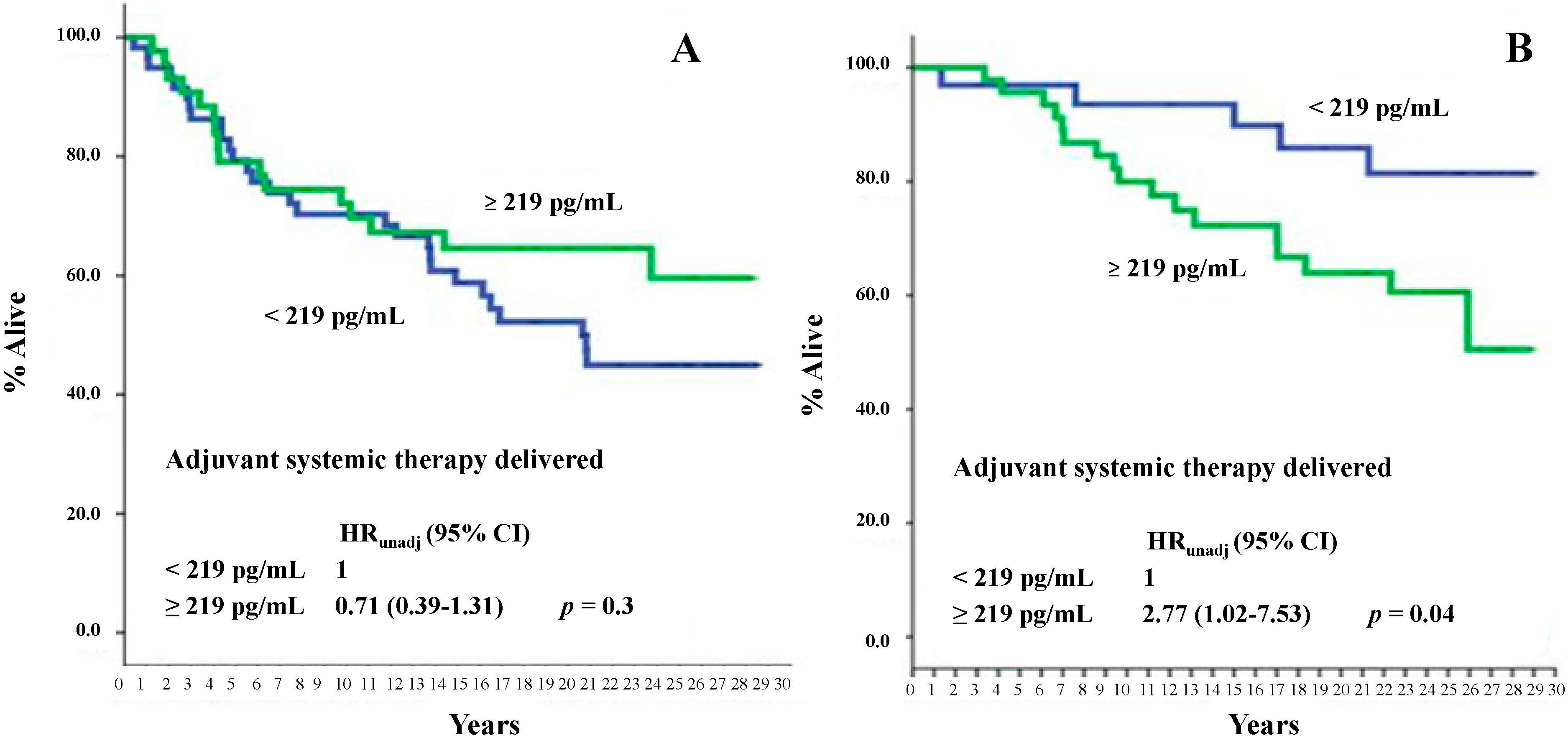
2.2. Correlation of Serum PN Levels with All-Cause Mortality and BCa-Specific Mortality




3. Discussion
3.1. General Remarks
3.2. Correlation of Serum PN Level with Clinical Pathological Features and Tissue PN Expression
3.3. Correlation of Serum PN Level with All-Cause Mortality and BCa-Specific Mortality
4. Experimental Section
4.1. Patient Selection and Sample Collection
4.2. Enzyme-Linked Immunosorbent Assay (ELISA) Evaluations
4.3. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Jin, J. JAMA patient page. Breast cancer screening: Benefits and harms. JAMA 2014, 312, 2585. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Panel members. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef] [PubMed]
- Jäger, W.; Krämer, S.; Palapelas, V.; Norbert, L. Breast cancer and clinical utility of CA 15-3 and CEA. Scand. J. Clin. Lab. Investig. Suppl. 1995, 221, 87–92. [Google Scholar] [CrossRef]
- Colomer, R.; Ruibal, A.; Genollá, J.; Rubio, D.; del Campo, J.M.; Bodi, R.; Salvador, L. Circulating CA 15-3 levels in the postsurgical follow-up of breast cancer patients and in non-malignant diseases. Breast Cancer Res. Treat. 1989, 13, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Donepudi, M.S.; Kondapalli, K.; Amos, S.J.; Venkanteshan, P. Breast cancer statistics and markers. J. Cancer Res. Ther. 2014, 10, 506–511. [Google Scholar] [PubMed]
- Witwer, K.W. Circulating microRNA biomarker studies: Pitfalls and potential solutions. Clin. Chem. 2015, 61, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Oskarsson, T. Extracellular matrix components in breast cancer progression and metastasis. Breast 2013, 22, S66–S72. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, K.; Amizuka, N.; Takeshita, S.; Takamatsu, H.; Katsuura, M.; Ozawa, H.; Toyama, Y.; Bonewald, L.F.; Kudo, A. Identification and characterization of a novel protein, Periostin, with restricted expression to periosteum and periodontal ligament and increased expression by transforming growth factor beta. J. Bone Miner. Res. 1999, 14, 1239–1249. [Google Scholar] [CrossRef] [PubMed]
- Ruan, K.; Bao, S.; Ouyang, G. The multifaceted role of periostin in tumorigenesis. Cell. Mol. Life Sci. 2009, 66, 2219–2230. [Google Scholar] [CrossRef] [PubMed]
- Morra, L.; Moch, H. Periostin expression and epithelial-mesenchymal transition in cancer: A review and an update. Virchows Arch. 2011, 459, 465–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, H.; Dai, M.; Auclair, D.; Kaji, M.; Fukai, I.; Kiriyama, M.; Yamakawa, Y.; Fujii, Y.; Chen, L.B. Serum level of the periostin, a homologue of an insect cell adhesion molecule, in thymoma patients. Cancer Lett. 2001, 172, 37–42. [Google Scholar] [CrossRef]
- Fujimoto, K.; Kawaguchi, T.; Nakashima, O.; Ono, J.; Ohta, S.; Kawaguchi, A.; Tonan, T.; Ohshima, K.; Yano, H.; Hayabuchi, N.; et al. Periostin, a matrix protein, has potential as a novel serodiagnostic marker for cholangiocarcinoma. Oncol. Rep. 2011, 25, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Ben, Q.W.; Zhao, Z.; Ge, S.F.; Zhou, J.; Yuan, F.; Yuan, Y.Z. Circulating levels of periostin may help identify patients with more aggressive colorectal cancer. Int. J. Oncol. 2009, 34, 821–828. [Google Scholar] [PubMed]
- Lv, Y.; Wang, W.; Jia, W.D.; Sun, Q.K.; Huang, M.; Zhou, H.C.; Xia, H.H.; Liu, W.B.; Chen, H.; Sun, S.N.; et al. High preoparative levels of serum periostin are associated with poor prognosis in patients with hepatocellular carcinoma after hepatectomy. Eur. J. Surg. Oncol. 2013, 39, 1129–1135. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.; Sun, H.; Lv, X.; Yang, D.; Zhang, J.; Shi, Y. Expression of periostin in the serum of NSCLC and its function on proliferation and migration of human lung adenocarcinoma cell line (A549) in vitro. Mol. Biol. Rep. 2010, 37, 2285–2293. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Yu, C.Y.; Dai, M.; Tam, C.; Loda, M.; Auclair, D.; Chen, L.B.; Elias, A. Elevated serum periostin levels in patients with bone metastases from breast but not lung cancer. Breast Cancer Res. Treat. 2003, 77, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, P.V.; Rubagotti, A.; Zinoli, L.; Salvi, S.; Boccardo, S.; Boccardo, F. Prognostic value of stromal and epithelial periostin (PN) expression in human breast cancer (BCa): Correlation with clinical pathological features and mortality outcome. Ann. Oncol. 2015, 26. Abstract 68P. [Google Scholar] [CrossRef]
- Malanchi, I.; Santamaria-Martínez, A.; Susanto, E.; Peng, H.; Lehr, H.A.; Delaloye, J.F.; Huelsken, J. Interactions between cancer stem cells and their niche govern metastatic colonization. Nature 2011, 481, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Non parametric estimation from incomplete observation. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuzzo, P.V.; Rubagotti, A.; Argellati, F.; Di Meglio, A.; Zanardi, E.; Zinoli, L.; Comite, P.; Mussap, M.; Boccardo, F. Prognostic Value of Preoperative Serum Levels of Periostin (PN) in Early Breast Cancer (BCa). Int. J. Mol. Sci. 2015, 16, 17181-17192. https://doi.org/10.3390/ijms160817181
Nuzzo PV, Rubagotti A, Argellati F, Di Meglio A, Zanardi E, Zinoli L, Comite P, Mussap M, Boccardo F. Prognostic Value of Preoperative Serum Levels of Periostin (PN) in Early Breast Cancer (BCa). International Journal of Molecular Sciences. 2015; 16(8):17181-17192. https://doi.org/10.3390/ijms160817181
Chicago/Turabian StyleNuzzo, Pier Vitale, Alessandra Rubagotti, Francesca Argellati, Antonio Di Meglio, Elisa Zanardi, Linda Zinoli, Paola Comite, Michele Mussap, and Francesco Boccardo. 2015. "Prognostic Value of Preoperative Serum Levels of Periostin (PN) in Early Breast Cancer (BCa)" International Journal of Molecular Sciences 16, no. 8: 17181-17192. https://doi.org/10.3390/ijms160817181