
The Impact of Specific Viruses on Clinical Outcome in Children Presenting with Acute Heart Failure


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics and Baseline Echocardiographic Findings
2.2. Polymerase Chain Reaction (PCR) Analysis
2.3. Left Ventricular Volumes and Ejection Fraction
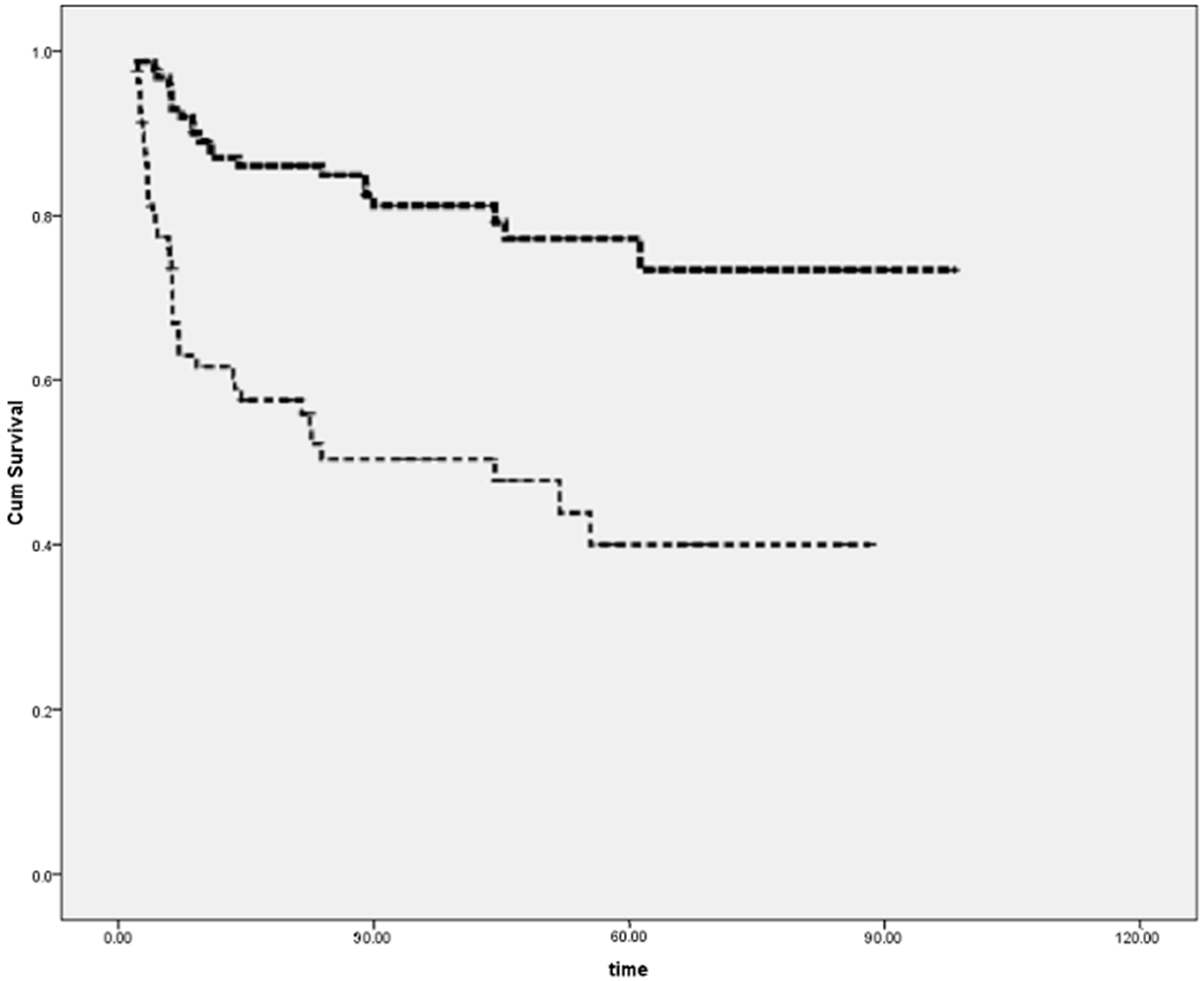
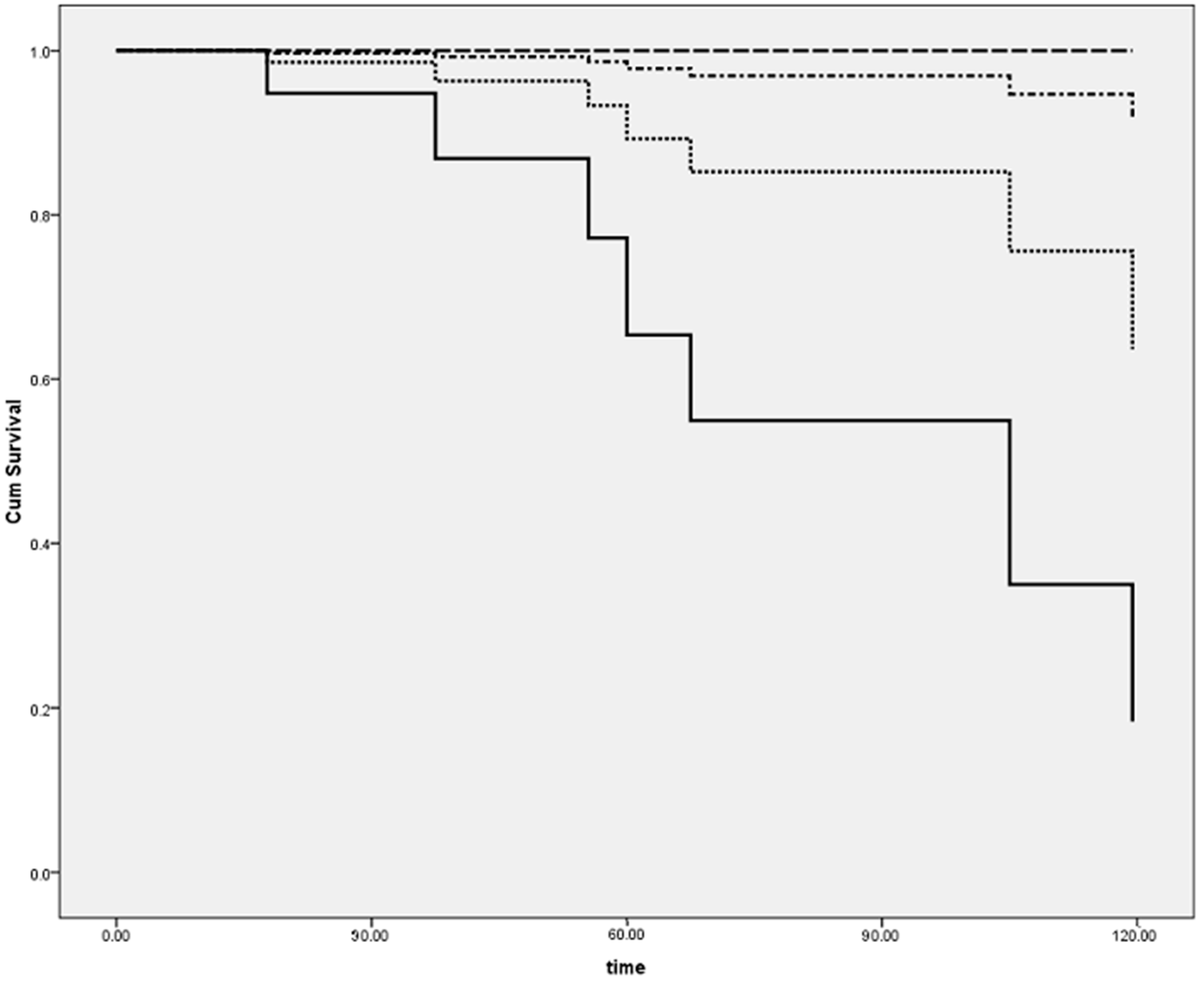
2.4. Follow-up and Prognosis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Follow-up
4.3. EMB Histology
4.4. Detection of Viral Genomes
4.5. Statistical Analysis
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| EMB | Endomyocardial biopsy |
| PCR | Polymerase chain reaction |
| PVB19 | Parvovirus B19 |
| DCM | Dilated cardiomyopathy |
| MRI | Magnetic resonance imaging |
| EF | Ejection fraction |
| EBV | Epstein–Barr virus |
| CMV | Cytomegalovirus |
| HSV | Herpes simplex virus |
| ENV | Enterovirus |
| ADV | Adenovirus |
| n | Number |
| EDV | End-diastolic volume |
| NS | Not significant |
| Myo | Myocarditis |
| LV | Left ventricular volume |
| DNA | Deoxyribonucleic acid |
| RNA | Ribonucleic acid |
References
- Kühl, U.; Schultheiss, H.P. Myocarditis in children. Heart Fail. Clin. 2010, 6, 483–496. [Google Scholar] [CrossRef] [PubMed]
- Rose, N.R. Myocarditis: Infection versus autoimmunity. J. Clin. Immunol. 2009, 29, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Baboonian, C.; Treasure, T. Meta-analysis of the association of enteroviruses with human heart disease. Heart 1997, 78, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.; Kontorovich, A.R.; Fuster, V.; Dec, G.W. Viral myocarditis-diagnosis, treatment, options, and current controversies. Nat. Rev. Cardiol. 2015, 12, 670–680. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, M.G.; Marcotte, F. Cardiac magnetic resonance assessment of myocarditis. Circ. Cardiovasc. Imaging 2013, 6, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.T.; Baughman, K.L.; Feldman, A.M.; Frustaci, A.; Jessup, M.; Kuhl, U.; Levine, G.N.; Narula, J.; Starling, R.C.; Towbin, J.; et al. The role of endomyocardial biopsy in the management of cardiovascular disease: a scientific statement from the American Heart Association, the American College of Cardiology, and the European Society of Cardiology. Endorsed by the Heart Failure Society of America and the Heart Failure Association of the European Society of Cardiology. J. Am. Coll. Cardiol. 2007, 50, 1914–1931. [Google Scholar] [PubMed]
- Magnani, J.W.; Danik, H.J.; Dec, G.W., Jr.; di Salvo, T.G. Survival in biopsy-proven myocarditis: A long-term retrospective analysis of the histopathologic, clinical, and hemodynamic predictors. Am. Heart J. 2006, 151, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Bowles, N.E.; Richardson, P.J.; Olsen, E.G.; Archard, L.C. Detection of Coxsackie-B-virus-specific RNA sequences in myocardial biopsy samples from patients with myocarditis and dilated cardiomyopathy. Lancet 1986, 1, 1120–1123. [Google Scholar] [CrossRef]
- Why, H.J.; Meany, B.T.; Richardson, P.J.; Olsen, E.G.; Bowles, N.E.; Cunningham, L.; Freeke, C.A.; Archard, L.C. Clinical and prognostic significance of detection of enteroviral RNA in the myocardium of patients with myocarditis or dilated cardiomyopathy. Circulation 1994, 89, 2582–2589. [Google Scholar] [CrossRef] [PubMed]
- Bowles, N.E.; Ni, J.; Kearney, D.L.; Pauschinger, M.; Schultheiss, H.P.; McCarthy, R.; Hare, J.; Bricker, J.T.; Bowles, K.R.; Towbin, J.A. Detection of viruses in myocardial tissues by polymerase chain reaction. Evidence of adenovirus as a common cause of myocarditis in children and adults. J. Am. Coll. Cardiol. 2003, 42, 4664–4672. [Google Scholar] [CrossRef]
- Salimans, M.M.; Holsappel, S.; van de Rijke, F.M.; Jiwa, N.M.; Raap, A.K.; Weiland, H.T. Rapid detection of human parvovirus B19 DNA by dot-hybridization and the polymerase chain reaction. J. Virol. Methods 1989, 23, 19–28. [Google Scholar] [CrossRef]
- Lotze, U.; Egerer, R.; Glück, B.; Zell, R.; Sigusch, H.; Erhardt, C.; Heim, A.; Kandolf, R.; Bock, T.; Wutzler, P.; et al. Low level myocardial parvovirus B19 persistence is a frequent finding in patients with heart disease but unrelated to ongoing myocardial injury. J. Med. Virol. 2010, 82, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Kandolf, R.; Ameis, D.; Kirschner, P.; Canu, A.; Hofschneider, P.H. In situ detection of enteroviral genomes in myocardial cells by nucleic acid hybridization: an approach to the diagnosis of viral heart disease. Proc. Natl. Acad. Sci. USA 1987, 84, 6272–6276. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.C.; Hilliard, A.A.; Cooper, L.T., Jr.; Rihal, C.S. Diagnosis and treatment of viral myocarditis. Mayo Clin. Proc. 2009, 84, 1001–1009. [Google Scholar] [CrossRef]
- Klein, R.M.; Jiang, H.; Niederacher, D.; Adams, O.; Du, M.; Horlitz, M.; Schley, P.; Marx, R.; Lankisch, M.R.; Brehm, M.U.; et al. Frequency and quantity of the parvovirus B19 genome in endomyocardial biopsies from patients with suspected myocarditis or idiopathic left ventricular dysfunction. Z. Kardiol. 2004, 93, 300–309. [Google Scholar] [PubMed]
- Tschöpe, C.; Bock, C.T.; Kasner, M.; Noutsias, M.; Westermann, D.; Schwimmbeck, P.L.; Pauschinger, M.; Poller, W.C.; Kühl, U.; Kandolf, R.; et al. High prevalence of cardiac parvovirus B19 infection in patients with isolated left ventricular diastolic dysfunction. Circulation 2005, 111, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Kühl, U.; Pauschinger, M.; Seeberg, B.; Lassner, D.; Noutsias, M.; Poller, W.; Schultheiss, H.P. Viral persistence in the myocardium is associated with progressive cardiac dysfunction. Circulation 2005, 112, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Bock, C.T.; Klingel, K.; Kandolf, R. Human parvovirus B19-associated myocarditis. N. Engl. J. Med. 2010, 362, 1248–1249. [Google Scholar] [CrossRef] [PubMed]
- Schowengerdt, K.O.; Ni, J.; Denfield, S.W.; Gajarski, R.J.; Bowles, N.E.; Rosenthal, G.; Kearney, D.L.; Price, J.K.; Rogers, B.B.; Schauer, G.M.; et al. Association of parvovirus B19 genome in children with myocarditis and cardiac allograft rejection: diagnosis using the polymerase chain reaction. Circulation 1997, 96, 3549–3554. [Google Scholar] [CrossRef] [PubMed]
- Francalanci, P.; Chance, J.L.; Vatta, M.; Jimenez, S.; Li, H.; Towbin, J.A.; Bowles, N.E. Cardiotropic viruses in the myocardium of children with end-stage heart disease. J. Heart Lung Transplant. 2004, 23, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Aretz, H.T.; Billingham, M.E.; Edwards, W.D.; Factor, S.M.; Fallon, J.T.; Fenoglio, J.J., Jr.; Olsen, E.G.; Schoen, F.J. Myocarditis: A histopathologic definition and classification. Am. J. Cardiovasc. Pathol. 1987, 1, 3–14. [Google Scholar] [PubMed]
- Gagliardi, M.G.; Bevilacqua, M.; Bassano, C.; Leonardi, B.; Boldrini, R.; Camassei, F.D.; Fierabracci, A.; Ugazio, A.G.; Bottazzo, G.F. Long term follow up of children with myocarditis treated by immunosuppression and of children with dilated cardiomyopathy. Heart 2004, 90, 1167–1171. [Google Scholar] [CrossRef] [PubMed]
- Enders, G.; Dötsch, J.; Bauer, J.; Nützenadel, W.; Hengel, H.; Haffner, D.; Schalasta, G.; Searle, K.; Brown, K.E. Life-threatening parvovirus B19-associated myocarditis and cardiac transplantation as possible therapy: Two case reports. Clin. Infect. Dis. 1998, 26, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Bowles, N.E.; Rose, M.L.; Taylor, P.; Banner, N.R.; Morgan-Capner, P.; Cunningham, L.; Archard, L.C.; Yacoub, M.H. End-stage dilated cardiomyopathy. Persistence of enterovirus RNA in myocardium at cardiac transplantation and lack of immune response. Circulation 1989, 80, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Amabile, N.; Fraisse, A.; Bouvenot, J.; Chetaille, P.; Ovaert, C. Outcome of acute fulminant myocarditis in children. Heart 2006, 92, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Dina, J.; Villedieu, F.; Labombarda, F.; Chetaille, P.; Ovaert, C. Childhood myocarditis and parvovirus B19 genotypes. J. Clin. Virol. 2011, 50, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Molina, K.M.; Garcia, X.; Denfield, S.W.; Fan, Y.; Morrow, W.R.; Towbin, J.A.; Frazier, E.A.; Nelson, D.P. Parvovirus B19 myocarditis causes significant morbidity and mortality in children. Pediatr. Cardiol. 2013, 34, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Cohen, B.J.; Buckley, M.M. The prevalence of antibody to human parvovirus B19 in England and Wales. J. Med. Microbiol. 1988, 25, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Young, N.S.; Brown, K.E. Parvovirus B19. N. Engl. J. Med. 2004, 350, 586–597. [Google Scholar] [CrossRef] [PubMed]
- Magro, C.M.; Crowson, A.N.; Dawood, M.; Nuovo, G.J. Parvoviral infection of endothelial cells and its possible role in vasculitis and autoimmune disease. J. Rheumatol. 2002, 29, 1227–1235. [Google Scholar] [PubMed]
- Kühl, U.; Pauschinger, M.; Bock, T.; Klingel, K.; Schwimmbeck, C.P.; Seeberg, B.; Krautwurm, L.; Poller, W.; Schultheiss, H.P.; Kandolf, R. Parvovirus B19 infection mimicking acute myocardial infarction. Circulation 2003, 108, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Bültmann, B.D.; Klingel, K.; Sotlar, K.; Bock, C.T.; Baba, H.A.; Sauter, M.; Kandolf, R. Fatal parvovirus B19-associated myocarditis clinically mimicking ischemic heart disease: An endothelial cell-mediated disease. Hum. Pathol. 2003, 34, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Moulik, M.; Breinholt, J.P.; Dreyer, W.J.; Kearney, D.L.; Price, J.F.; Clunie, S.K.; Moffett, B.S.; Kim, J.J.; Rossano, J.W.; Jefferies, J.L.; et al. Viralendomyocardial infection is an independent predictor and potentially treatable risk factor for graft loss and coronary vasculopathy in pediatric cardiac transplant recipients. J. Am. Coll. Cardiol. 2010, 56, 582–592. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Patients | 63 |
| Female | 34 (54%) |
| Median age at diagnosis (range) | 2.8 (0.1–19.5) |
| Fever * | 13 |
| Symptoms at presentation | ≤7 days |
| EF at diagnosis | 30.8% ± 10.5% |
| Myocarditis | 22.5% |
| DCM | 63.5% |
| Mean follow-up ±SD | 4.2 ± 5 |
| Deaths | 14 (7.4%) |
| Heart transplantation | 39 (20.6%) |
| Diagnosis | EMBs | Viral Genome | |
|---|---|---|---|
| PCR Positive | PCR Amplifier | ||
| Myocarditis | 14 | 9 | PVB19 (n = 7) EBV (n = 2) PVB + EBV (n = 1) |
| Borderline myocarditis | 9 | 3 | PVB19 (n = 3) |
| DCM | 40 | 7 | PVB19 (n = 5) CMV (n = 1) PVB + HSV (n = 1) |
| Variable | Viral Genome (+) | Viral Genome (−) | p Value |
|---|---|---|---|
| LV-EDV (mL/m2) | 93 ± 29 | 103 ± 38 | <0.05 |
| Baseline LV-EF (%) | 36 ± 10 | 26 ± 10 | <0.01 |
| EF change at follow up (%) | +18 | +14 | <0.05 |
| Variable | Myocarditis | Borderline Myo | DCM | p Value for Trend |
|---|---|---|---|---|
| LV-EDV (mL/m2) | 98.7 ± 42 | 106.7 ± 23 | 134.9 ± 79 | <0.05 |
| LV-EF (%) | 30.9 ± 10 | 31.1 ± 14 | 30.7 ± 10 | NS |
| EF change at follow up (%) | +22 | +18 | +12 | <0.05 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gagliardi, M.G.; Fierabracci, A.; Pilati, M.; Chinali, M.; Bassano, C.; Saura, F.; Giovannoni, I.; Francalanci, P. The Impact of Specific Viruses on Clinical Outcome in Children Presenting with Acute Heart Failure. Int. J. Mol. Sci. 2016, 17, 486. https://doi.org/10.3390/ijms17040486
Gagliardi MG, Fierabracci A, Pilati M, Chinali M, Bassano C, Saura F, Giovannoni I, Francalanci P. The Impact of Specific Viruses on Clinical Outcome in Children Presenting with Acute Heart Failure. International Journal of Molecular Sciences. 2016; 17(4):486. https://doi.org/10.3390/ijms17040486
Chicago/Turabian StyleGagliardi, Maria Giulia, Alessandra Fierabracci, Mara Pilati, Marcello Chinali, Carlo Bassano, Francesca Saura, Isabella Giovannoni, and Paola Francalanci. 2016. "The Impact of Specific Viruses on Clinical Outcome in Children Presenting with Acute Heart Failure" International Journal of Molecular Sciences 17, no. 4: 486. https://doi.org/10.3390/ijms17040486