Dry Eye Management: Targeting the Ocular Surface Microenvironment


 ,
, 
Abstract
:
1. Introduction
1.1. Current Strategy on Dry Eye Management
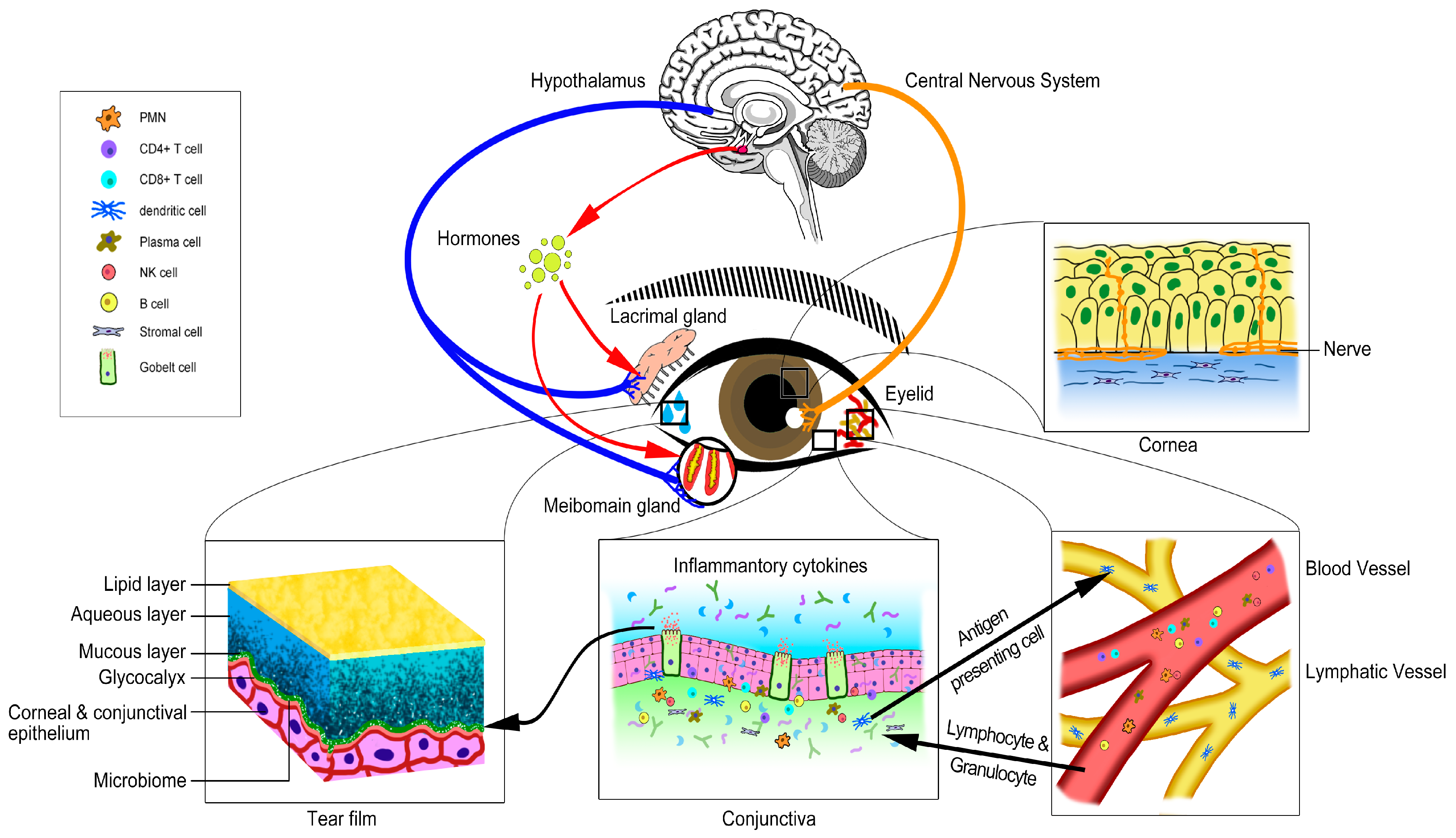
1.2. The Concept of Ocular Surface Microenvironment
2. The Components of Ocular Surface Microenvironment
2.1. Tissue Components of the Ocular Surface Microenvironment
2.1.1. Cornea
2.1.2. Conjunctiva
2.1.3. Lacrimal Glands
2.1.4. Meibomian Gland
2.1.5. Eyelids
2.2. Other Specific Components of the Ocular Surface Microenvironment
2.2.1. Tear Film
2.2.2. Immune Cells
2.2.3. Nerve Supply of the Ocular Surface
2.2.4. Systemic Hormones
2.2.5. Vascular and Lymphatic Systems
2.2.6. Ocular Surface Microbiome
2.3. Complexity and Integrity of the Ocular Surface Microenvironment
3. Ocular Surface Microenvironment Change in Dry Eye
3.1. The Change of Tissue Components of Ocular Surface Microenviroment in Dry Eye
3.1.1. Cornea
3.1.2. Conjunctiva
3.1.3. Lacrimal Gland
3.1.4. Meibomian Gland
3.1.5. Eyelids
3.2. The Changes of Other Specific Components of the Ocular Surface Microenvironment in Dry Eye
3.2.1. Tear Film
3.2.2. Immune Cells
3.3.3. Nerve Supply of Ocular Surface
3.3.4. Systemic Hormones
3.3.5. Vascular System
3.3.6. Ocular Surface Microbiome
4. Dry Eye Management: Ocular Surface Microenvironment Targeted Therapy
4.1. Therapy Targeting Cornea
4.2. Therapy Targeting Conjunctiva
4.3. Therapy Targeting Lacrimal Gland
4.4. Therapy Targeting Meibomian Gland
4.5. Therapy Targeting Eyelids
4.6. Therapy Targeting the Tear Film
4.6.1. Compensation of Tear
4.6.2. Stimulated Tear Production
4.6.3. Controlling Tear Evaporation
4.6.4. Regulating Excessive Nasolacrimal Drainage
4.7. Therapy Targeting Inflammation
4.8. Therapy Targeting Nerve Supply of the Ocular Surface
4.9. Therapy Targeting Systemic Hormones
4.10. Therapy Targeting Vascular and Lymphatic System
5. Conclusions and Prospective of Future Research
Acknowledgments
Conflicts of Interest
References
- Lemp, M.A.; Baudouin, C.; Baum, J.; Dogru, M.; Foulks, G.N.; Kinoshita, S.; Laibson, P.; McCulley, J.; Murube, J.; Pflugfelder, S.C.; et al. The definition and classification of dry eye disease: Report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 75–92. [Google Scholar]
- Stern, M.E.; Beuerman, R.W.; Fox, R.I.; Gao, J.; Mircheff, A.K.; Pflugfelder, S.C. The pathology of dry eye: The interaction between the ocular surface and lacrimal glands. Cornea 1998, 17, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Mantelli, F.; Massaro-Giordano, M.; Macchi, I.; Lambiase, A.; Bonini, S. The cellular mechanisms of dry eye: From pathogenesis to treatment. J. Cell. Physiol. 2013, 228, 2253–2256. [Google Scholar] [CrossRef] [PubMed]
- Kureshi, A.K.; Dziasko, M.; Funderburgh, J.L.; Daniels, J.T. Human corneal stromal stem cells support limbal epithelial cells cultured on RAFT tissue equivalents. Sci. Rep. 2015, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Watsky, M.A.; Jablonski, M.M.; Edelhauser, H.F. Comparison of conjunctival and corneal surface areas in rabbit and human. Curr. Eye Res. 1988, 7, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Inatomi, T.; SpurrMichaud, S.; Tisdale, A.S.; Zhan, Q.; Feldman, S.T.; Gipson, I.K. Expression of secretory mucin genes by human conjunctival epithelia. Investig. Ophthalmol. Vis. Sci. 1996, 37, 1684–1692. [Google Scholar]
- Paulsen, F.P.; Berry, M.S. Mucins and TFF peptides of the tear film and lacrimal apparatus. Prog. Histochem. Cytochem. 2006, 41, 1–53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Volpe, E.A.; Gandhi, N.B.; Schaumburg, C.S.; Siemasko, K.F.; Pangelinan, S.B.; Kelly, S.D.; Hayday, A.C.; Li, D.Q.; Stern, M.E.; et al. NK cells promote Th-17 mediated corneal barrier disruption in dry eye. PLoS ONE 2012, 7, e36822. [Google Scholar] [CrossRef] [PubMed]
- Hattori, T.; Saban, D.R.; Emami-Naeini, P.; Chauhan, S.K.; Funaki, T.; Ueno, H.; Dana, R. Donor-derived, tolerogenic dendritic cells suppress immune rejection in the indirect allosensitization-dominant setting of corneal transplantation. J. Leukoc. Biol. 2012, 91, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Khandelwal, P.; Blanco-Mezquita, T.; Emami, P.; Lee, H.S.; Reyes, N.J.; Mathew, R.; Huang, R.; Saban, D.R. Ocular mucosal CD11b+ and CD103+ mouse dendritic cells under normal conditions and in allergic immune responses. PLoS ONE 2013, 8, e64193. [Google Scholar] [CrossRef] [PubMed]
- Nadri, S.; Soleimani, M.; Kiani, J.; Atashi, A.; Izadpanah, R. Multipotent mesenchymal stem cells from adult human eye conjunctiva stromal cells. Differentiation 2008, 76, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Ko, A.Y.; Ko, J.H.; Lee, H.J.; Kim, M.K.; Wee, W.R.; Khwarg, S.I.; Oh, J.Y. Mesenchymal Stem/Stromal Cells Protect the Ocular Surface by Suppressing Inflammation in an Experimental Dry Eye. Mol. Ther. 2015, 23, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Conrady, C.D.; Joos, Z.P.; Patel, B.C. Review: The Lacrimal Gland and Its Role in Dry Eye. J. Ophthalmol. 2016, 2016, 7542929. [Google Scholar] [CrossRef] [PubMed]
- Obata, H. Anatomy and Histopathology of Human Meibomian Gland. Cornea 2002, 21, S70–S74. [Google Scholar] [CrossRef] [PubMed]
- Call, M.; Fischesser, K.; Lunn, M.O.; Kao, W.W. A unique lineage gives rise to the meibomian gland. Mol. Vis. 2016, 22, 168–172. [Google Scholar] [PubMed]
- Dutton, J.J.; Frueh, B.R. Eyelid Anatomy and Physiology with Reference to Blepharoptosis. In Evaluation and Management of Blepharoptosis; Cohen, A.J., Weinberg, D.A., Eds.; Springer: New York, NY, USA, 2011; pp. 13–26. [Google Scholar]
- Mishima, S.; Maurice, D.M. The oily layer of the tear film and evaporation from the corneal surface. Exp. Eye Res. 1961, 1, 39–45. [Google Scholar] [CrossRef]
- Pucker, A.D.; Nichols, J.J. Analysis of Meibum and Tear Lipids. Ocul. Surf. 2012, 10, 230–250. [Google Scholar] [CrossRef] [PubMed]
- Pucker, A.D.; Haworth, K.M. The Presence and Significance of Polar Meibum and Tear Lipids. Ocul. Surf. 2015, 13, 26–42. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.E.; Murphy, P.J. Changes in the tear film and ocular surface from dry eye syndrome. Prog. Retin. Eye Res. 2004, 23, 449–474. [Google Scholar] [CrossRef] [PubMed]
- Davidson, H.J.; Kuonen, V.J. The tear film and ocular mucins. Vet. Ophthalmol. 2004, 7, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Gipson, I.K.; Argueso, P. Role of mucins in the function of the corneal and conjunctival epithelia. Int. Rev. Cytol. 2003, 231, 1–49. [Google Scholar] [PubMed]
- Hodges, R.R.; Dartt, D.A. Tear film mucins: Front line defenders of the ocular surface; comparison with airway and gastrointestinal tract mucins. Exp. Eye Res. 2013, 117, 62–78. [Google Scholar] [CrossRef] [PubMed]
- Rolando, M.; Zierhut, M. The ocular surface and tear film and their dysfunction in dry eye disease. Surv. Ophthalmol. 2001, 45, S203–S210. [Google Scholar] [CrossRef]
- Klenkler, B.; Sheardown, H.; Jones, L. Growth Factors in the Tear Film: Role in Tissue Maintenance, Wound Healing, and Ocular Pathology. Ocul. Surf. 2007, 5, 228–239. [Google Scholar] [CrossRef]
- Knop, E.; Knop, N. Anatomy and Immunology of the Ocular Surface. Chem. Immunol. Allergy 2007, 92, 36–49. [Google Scholar] [PubMed]
- Vantrappen, L.; Geboes, K.; Missotten, L.; Maudgal, P.C.; Desmet, V. Lymphocytes and Langerhans cells in the normal human cornea. Investig. Ophthalmol. Vis. Sci. 1985, 26, 220–225. [Google Scholar]
- Stern, M.E.; Schaumburg, C.S.; Pflugfelder, S.C. Dry eye as a mucosal autoimmune disease. Int. Rev. Immunol. 2013, 32, 19–41. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.E.; Schaumburg, C.S.; Dana, R.; Calonge, M.; Niederkorn, J.Y.; Pflugfelder, S.C. Autoimmunity at the ocular surface: Pathogenesis and regulation. Mucosal Immunol. 2010, 3, 425–442. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Schaumburg, C.S.; Coursey, T.G.; Siemasko, K.F.; Volpe, E.A.; Gandhi, N.B.; Li, D.Q.; Niederkorn, J.Y.; Stern, M.E.; Pflugfelder, S.C.; et al. CD8(+) Cells Regulate the T-helper-17 Response in an Experimental Murine Model of Sjögren Syndrome. Mucosal Immunol. 2014, 7, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Dastjerdi, M.H.; Dana, R. Corneal Nerve Alterations in Dry Eye-associated Ocular Surface Disease. Int. Ophthalmol. Clin. 2009, 49, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Dartt, D.A. Neural Regulation of Lacrimal Gland Secretory Processes: Relevance in Dry Eye Diseases. Prog. Retin. Eye Res. 2009, 28, 155–177. [Google Scholar] [CrossRef] [PubMed]
- Knop, E.; Knop, N.; Millar, T.; Obata, H.; Sullivan, D.A. The international workshop on meibomian gland dysfunction: Report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1938–1978. [Google Scholar] [CrossRef] [PubMed]
- Diebold, Y.; Ríos, J.D.; Hodges, R.R.; Rawe, I.; Dartt, D.A. Presence of nerves and their receptors in mouse and human conjunctival goblet cells. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2270–2282. [Google Scholar]
- Sullivan, D.A.; Jensen, R.V.; Suzuki, T.; Richards, S.M. Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands? Mol. Vis. 2009, 15, 1553–1572. [Google Scholar] [PubMed]
- Versura, P.; Giannaccare, G.; Campos, E.C. Sex-steroid imbalance in females and dry eye. Curr. Eye Res. 2015, 40, 162–175. [Google Scholar] [CrossRef] [PubMed]
- Schirra, F.; Suzuki, T.; Richards, S.M.; Jensen, R.V.; Liu, M.; Lombardi, M.J.; Rowley, P.; Treister, N.S.; Sullivan, D.A. Androgen control of gene expression in the mouse meibomian gland. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3666–3675. [Google Scholar] [CrossRef] [PubMed]
- Truong, S.; Cole, N.; Stapleton, F.; Golebiowski, B. Sex hormones and the dry eye. Clin. Exp. Optom. 2014, 97, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Kinoshita, Y.; Tachibana, M.; Matsushima, Y.; Kobayashi, Y.; Adachi, W.; Sotozono, C.; Kinoshita, S. Expression of sex steroid hormone receptors in human cornea. Curr. Eye Res. 2001, 22, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Beauregard, C.; Brandt, P. Down regulation of interleukin-1β-induced nitric oxide production in lacrimal gland acinar cells by sex steroids. Curr. Eye Res. 2004, 29, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Knop, E.; Knop, N.; Sullivan, D.A.; List, E.O.; Kopchick, J.J.; Kam, W.R.; Ding, J. Growth Hormone Influence on the Morphology and Size of the Mouse Meibomian Gland. J. Ophthalmol. 2016, 2016, 5728071. [Google Scholar] [CrossRef] [PubMed]
- Wirostko, B.; Rafii, M.; Sullivan, D.A.; Morelli, J.; Ding, J. Novel therapy to treat corneal epithelial defects: A hypothesis with growth hormone. Ocul. Surf. 2015, 13, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Wirostko, B.; Sullivan, D.A. Human growth hormone promotes corneal epithelial cell migration in vitro. Cornea 2015, 34, 686. [Google Scholar] [CrossRef] [PubMed]
- Ebling, F.; Ebling, E.; Randall, V.; Skinner, J. The effects of hypophysectomy and of bovine growth hormone on the responses to testosterone of prostate, preputial, Harderian and lachrymal glands and of brown adipose tissue in the rat. J. Endocrinol. 1975, 66, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Mantelli, F.; Moretti, C.; Macchi, I.; Massaro-Giordano, G.; Cozzupoli, G.M.; Lambiase, A.; Bonini, S. Effects of Sex Hormones on Ocular Surface Epithelia: Lessons Learned From Polycystic Ovary Syndrome. J. Cell. Physiol. 2016, 231, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Pleyer, U.; Sherif, Z. Corticosteroids in ophthalmology. In Recent Advances in Glucocorticoid Receptor Action; Springer: Berlin/Heidelberg, Germany, 2002; pp. 65–81. [Google Scholar]
- Chauhan, S.K.; Dohlman, T.H.; Dana, R. Corneal lymphatics: Role in ocular inflammation as inducer and responder of adaptive immunity. J. Clin. Cell. Immunol. 2014, 5, 1000256. [Google Scholar] [CrossRef] [PubMed]
- Ecoiffier, T.; Sadovnikova, A.; Yuen, D.; Chen, L. Conjunctival Lymphatic Response to Corneal Inflammation in Mice. J. Ophthalmol. 2012, 2012, 953187. [Google Scholar] [CrossRef] [PubMed]
- Hos, D.; Bachmann, B.; Bock, F.; Onderka, J.; Cursiefen, C. Age-related changes in murine limbal lymphatic vessels and corneal lymphangiogenesis. Exp. Eye Res. 2008, 87, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Lohela, M.; Bry, M.; Tammela, T.; Alitalo, K. VEGFs and receptors involved in angiogenesis versus lymphangiogenesis. Curr. Opin. Cell Biol. 2009, 21, 154–165. [Google Scholar] [CrossRef] [PubMed]
- Dong, Q.; Brulc, J.M.; Iovieno, A.; Bates, B.; Garoutte, A.; Miller, D.; Revanna, K.V.; Gao, X.; Antonopoulos, D.A.; Slepak, V.Z.; et al. Diversity of Bacteria at Healthy Human Conjunctiva. Immunol. Microbiol. 2011, 52, 5408–5413. [Google Scholar] [CrossRef] [PubMed]
- Doan, T.; Akileswaran, L.; Andersen, D.; Johnson, B.; Ko, N.; Shrestha, A.; Shestopalov, V.; Lee, C.S.; Lee, A.Y.; VanGelder, R.N. Paucibacterial Microbiome and Resident DNA Virome of the Healthy Conjunctiva. Investig. Ophthalmol. Vis. Sci. 2016, 57, 5116–5126. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, H.E.; Azcuy, A.M.; Varnell, E.D.; Sloop, G.D.; Thompson, H.W.; Hill, J.M. HSV-1 DNA in tears and saliva of normal adults. Investig. Ophthalmol. Vis. Sci. 2005, 46, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Reading, N.C.; Sperandio, V. Quorum sensing: The many languages of bacteria. FEMS Microbiol. Lett. 2006, 254, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mshangila, B.; Paddy, M.; Kajumbula, H.; Ateenyi-Agaba, C.; Kahwa, B.; Seni, J. External ocular surface bacterial isolates and their antimicrobial susceptibility patterns among pre-operative cataract patients at Mulago National Hospital in Kampala, Uganda. BMC Ophthalmol. 2013, 13, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.E.; Graham, J.E.; Beirne, R.O.; Downes, S.C.; Moore, C.B.T. The effect of post-operative antibiotics on the ocular surface bacterial flora in cataract patients. Acta Ophthalmol. Scand. 2007, 85. [Google Scholar] [CrossRef]
- Miller, D.; Iovieno, A. The role of microbial flora on the ocular surface. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.; Harris, A.; Lumb, R.; Powell, K. Commensal ocular bacteria degrade mucin. Br. J. Ophthal. 2002, 86, 1412–1416. [Google Scholar] [CrossRef]
- Stern, M.E.; Gao, J.; Siemasko, K.F.; Beuerman, R.W.; Pflugfelder, S.C. The role of the lacrimal functional unit in the pathophysiology of dry eye. Exp. Eye Res. 2004, 78, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Muller, L.J.; Marfurt, C.F.; Kruse, F.; Tervo, T.M. Corneal nerves: Structure, contents and function. Exp. Eye Res. 2003, 76, 521–542. [Google Scholar] [CrossRef]
- Zoukhri, D.; Hodges, R.R.; Byon, D.; Kublin, C.L. Role of proinflammatory cytokines in the impaired lacrimation associated with autoimmune xerophthalmia. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1429–1436. [Google Scholar]
- Wang, Y.; Pei, G.; Cai, Y.C.; Zhao, Z.Q.; Wang, J.B.; Jiang, C.L.; Zheng, Z.C.; Liu, X.Y. Human interleukin-2 could bind to opioid receptor and induce corresponding signal transduction. Neuroreport 1996, 8, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Mircheff, A.K. Sjogrens syndrome as failed local immunohomeostasis: Prospects for cell-based therapy. Ocul. Surf. 2003, 1, 160–179. [Google Scholar] [CrossRef]
- Sanchis-Gimeno, J.A.; Lleo-Perez, A.; Alonso, L.; Rahhal, M.S.; Martinez-Soriano, F. Reduced corneal thickness values in postmenopausal women with dry eye. Cornea 2005, 24, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Pflugfelder, S.C. Corneal thickness is reduced in dry eye. Cornea 1999, 18, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.M.; Hamied, F.M.; Farhood, Q.K. Corneal thickness in dry eyes in an Iraqi population. Clin. Ophthalmol. 2017, 11, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Lin, F.; Huang, Z.; He, Q.; Han, W. Changes of Corneal Wavefront Aberrations in Dry Eye Patients after Treatment with Artificial Lubricant Drops. J. Ophthalmol. 2016, 2016, 1342056. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, C.; Barabino, S.; Rashid, S.; Dana, M.R. Corneal epithelial proliferation and thickness in a mouse model of dry eye. Exp. Eye Res. 2009, 89, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Meloni, M.; De Servi, B.; Marasco, D.; Del Prete, S. Molecular mechanism of ocular surface damage: Application to an in vitro dry eye model on human corneal epithelium. Mol. Vis. 2011, 17, 113–126. [Google Scholar] [PubMed]
- Kheirkhah, A.; Saboo, U.S.; Abud, T.B.; Dohlman, T.H.; Arnoldner, M.A.; Hamrah, P.; Dana, R. Reduced Corneal Endothelial Cell Density in Patients With Dry Eye Disease. Am. J. Ophthalmol. 2015, 159, 1022–1036. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Tseng, S.C.; Yoshino, K.; Monroy, D.; Felix, C.; Reis, B.L. Correlation of goblet cell density and mucosal epithelial membrane mucin expression with rose bengal staining in patients with ocular irritation. Ophthalmology 1997, 104, 223–235. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Corrales, R.M.; de Paiva, C.S. T helper cytokines in dry eye disease. Exp. Eye Res. 2013, 117, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Chhadva, P.; Alexander, A.; McClellan, A.L.; McManus, K.T.; Seiden, B.; Galor, A. The Impact of Conjunctivochalasis on Dry Eye Symptoms and Signs. Investig. Ophthalmol. Vis. Sci. 2015, 56, 2867–2871. [Google Scholar] [CrossRef] [PubMed]
- Kampitak, K.; Leelawongtawun, W. Precorneal tear film in pterygium eye. J. Med. Assoc. Thail. 2014, 97, 536–539. [Google Scholar]
- Roka, N.; Shrestha, S.P.; Joshi, N.D. Assessment of tear secretion and tear film instability in cases with pterygium and normal subjects. Nepal. J. Ophthalmol. 2013, 5, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.A.; Krenzer, K.L.; Rocha, E.M.; Toda, I. Aqueous tear deficiency in Sjögren’s syndrome: Possible causes and potential treatment. Oculodermal Dis. 1997, 95–152. [Google Scholar]
- Xuan, J.; Shen, L.; Malyavantham, K.; Pankewycz, O.; Ambrus, J.L.; Suresh, L. Temporal histological changes in lacrimal and major salivary glands in mouse models of Sjogren’s syndrome. BMC Oral Health 2013, 13, 51. [Google Scholar] [CrossRef] [PubMed]
- Bacman, S.; Berra, A.; Sterin-Borda, L.; Borda, E. Muscarinic acetylcholine receptor antibodies as a new marker of dry eye Sjogren syndrome. Investig. Ophthalmol. Vis. Sci. 2001, 42, 321–327. [Google Scholar]
- Sullivan, D.A. Sex hormones and Sjogren’s syndrome. J. Rheumatol. Suppl. 1997, 50, 17–32. [Google Scholar] [PubMed]
- Hassan, A.S.; Clouthier, S.G.; Ferrara, J.L.M.; Stepan, A.; Mian, S.I.; Ahmad, A.Z.; Elner, V.M. Lacrimal Gland Involvement in Graft-Versus-Host Disease: A Murine Model. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2692–2697. [Google Scholar] [CrossRef] [PubMed]
- Borchman, D.; Foulks, G.N.; Yappert, M.C.; Milliner, S.E. Differences in human meibum lipid composition with meibomian gland dysfunction using NMR and principal component analysis. Investig. Ophthalmol. Vis. Sci. 2012, 53, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.; Benjamin, L.; Snibson, G. Meibomian gland disease. Classification and grading of lid changes. Eye 1991, 5 Pt 4, 395–411. [Google Scholar] [CrossRef] [PubMed]
- Driver, P.J.; Lemp, M.A. Meibomian gland dysfunction. Surv. Ophthalmol. 1996, 40, 343–367. [Google Scholar] [CrossRef]
- Yap, M. Tear break-up time is related to blink frequency. Acta Ophthalmol. 1991, 69, 92–94. [Google Scholar] [CrossRef]
- Chang, M.; Lee, H.; Park, M.S.; Baek, S. The clinical characteristics and new classification of sticky eyelid syndrome in East Asian patients. Acta Ophthalmol. 2014, 92, e667–e670. [Google Scholar] [CrossRef] [PubMed]
- Geerling, G.; Tauber, J.; Baudouin, C.; Goto, E.; Matsumoto, Y.; O’Brien, T.; Rolando, M.; Tsubota, K.; Nichols, K.K. The international workshop on meibomian gland dysfunction: Report of the subcommittee on management and treatment of meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2050–2064. [Google Scholar] [CrossRef] [PubMed]
- Rynerson, J.M.; Perry, H.D. DEBS—A unification theory for dry eye and blepharitis. Clin. Ophthalmol. 2016, 10, 2455–2467. [Google Scholar] [CrossRef] [PubMed]
- Lucca, J.A.; Nunez, J.N.; Farris, R.L. A comparison of diagnostic tests for keratoconjunctivitis sicca: Lactoplate, Schirmer, and tear osmolarity. CLAO J. 1990, 16, 109–112. [Google Scholar] [PubMed]
- Luo, L.; Li, D.Q.; Pflugfelder, S.C. Hyperosmolarity-Induced Apoptosis in Human Corneal Epithelial Cells Is Mediated by Cytochrome c and MAPK Pathways. Cornea 2007, 26, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Q.; Luo, L.; Chen, Z.; Kim, H.S.; Song, X.J.; Pflugfelder, S.C. JNK and ERK MAP kinases mediate induction of IL-1β, TNF-α and IL-8 following hyperosmolar stress in human limbal epithelial cells. Exp. Eye Res. 2006, 82, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Begley, C.; Chen, M.; Bradley, A.; Bonanno, J.; McNamara, N.A.; Nelson, J.D.; Simpson, T. A Link between Tear Instability and Hyperosmolarity in Dry Eye. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3671–3679. [Google Scholar] [CrossRef] [PubMed]
- Kamao, T.; Yamaguchi, M.; Kawasaki, S.; Mizoue, S.; Shiraishi, A.; Ohashi, Y. Screening for dry eye with newly developed ocular surface thermographer. Am. J. Ophthalmol. 2011, 151, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Tomlinson, A. Importance of the lipid layer in human tear film stability and evaporation. Optom. Vis. Sci. 1997, 74, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Tiffany, J.M. The contribution of meibomian disease to dry eye. Ocul. Surf. 2004, 2, 149–165. [Google Scholar] [CrossRef]
- Abusharha, A.A.; Pearce, E.I. The effect of low humidity on the human tear film. Cornea 2013, 32, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Guillon, M.; Maissa, C. Contact lens wear affects tear film evaporation. Eye Contact Lens 2008, 34, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Guillon, M.; Maissa, C. Tear film evaporation—Effect of age and gender. Contact Lens Anterior Eye 2010, 33, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.C.; Cerretani, C.; Braun, R.J.; Radke, C.J. Evaporation-driven instability of the precorneal tear film. Adv. Colloid Interface Sci. 2014, 206, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.W.; Chang, C.J. Delayed tear clearance in contact lens associated papillary conjunctivitis. Curr. Eye Res. 2001, 22, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Afonso, A.A.; Monroy, D.; Stern, M.E.; Feuer, W.J.; Tseng, S.C.; Pflugfelder, S.C. Correlation of tear fluorescein clearance and Schirmer test scores with ocular irritation symptoms. Ophthalmology 1999, 106, 803–810. [Google Scholar] [CrossRef]
- Dursun, D.; Wang, M.; Monroy, D.; Li, D.-Q.; Lokeshwar, B.L.; Stern, M.E.; Pflugfelder, S.C.A. Mouse Model of Keratoconjunctivitis Sicca. Investig. Ophthalmol. Vis. Sci. 2002, 43, 632–638. [Google Scholar]
- Shrestha, R.K.; Borchman, D.; Foulks, G.N.; Yappert, M.C.; Milliner, S.E. Analysis of the Composition of Lipid in Human Meibum from Normal Infants, Children, Adolescents, Adults, and Adults with Meibomian Gland Dysfunction Using (1)H-NMR Spectroscopy. Investig. Ophthalmol. Vis. Sci. 2011, 52, 7350–7358. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.M.; Tong, L.; Yong, S.S.; Li, B.; Chaurasia, S.S.; Shui, G.; Wenk, M.R. Meibum Lipid Composition in Asians with Dry Eye Disease. PLoS ONE 2011, 6, e24339. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.; Thangavelu, M.; Zhang, L.; Green, K.B.; Nichols, K.K. iTRAQ Quantitative Proteomics in the Analysis of Tears in dry eye patients. Investig. Ophthalmol. Vis. Sci 2012, 53, 5052–5059. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.; Durán, J.A.; Etxebarria, J.; Merayo, J.; González, N.; Reigada, R.; García, I.; Acera, A.; Suárez, T. Tear proteome and protein network analyses reveal a novel pentamarker panel for tear film characterization in dry eye and meibomian gland dysfunction. J. Proteom. 2012, 78, 94–112. [Google Scholar] [CrossRef] [PubMed]
- Perumal, N.; Funke, S.; Pfe, N.; Grus, F.H. Proteomics analysis of human tears from aqueous-deficient and evaporative dry eye patients. Sci. Rep. 2016. [Google Scholar] [CrossRef] [PubMed]
- Argüeso, P.; Balaram, M.; Spurr-Michaud, S.; Keutmann, H.T.; Dana, M.R.; Gipson, I.K. Decreased Levels of the Goblet Cell Mucin MUC5AC in Tears of Patients with Sjögren Syndrome. Investig. Ophthalmol. Vis. Sci. 2002, 43, 1004–1011. [Google Scholar]
- Corrales, R.M.; Narayanan, S.; Fernández, I.; Mayo, A.; Galarreta, D.J.; Fuentes-Páez, G.; Chaves, F.J.; Herreras, J.M.; Calonge, M. Ocular Mucin Gene Expression Levels as Biomarkers for the Diagnosis of Dry Eye Syndrome. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8363–8369. [Google Scholar] [CrossRef] [PubMed]
- Caffery, B.; Heynen, M.L.; Joyce, E.; Jones, L.; Ritter, R.; Senchyna, M. MUC1 expression in Sjogren’s syndrome, KCS, and control subjects. Mol. Vis. 2010, 16, 1720–1727. [Google Scholar] [PubMed]
- Zhang, X.; Chen, W.; De Paiva, C.S.; Volpe, E.A.; Gandhi, N.B.; Farley, W.J.; Li, D.Q.; Niederkorn, J.Y.; Stern, M.E.; Pflugfelder, S.C.; et al. Desiccating Stress Induces CD4 T-Cell—Mediated Sjögren’s Syndrome—Like Corneal Epithelial Apoptosis via Activation of the Extrinsic Apoptotic Pathway by Interferon-γ. Am. J. Pathol. 2011, 179, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Niederkorn, J.Y.; Stern, M.E.; Pflugfelder, S.C.; De Paiva, C.S.; Corrales, R.M.; Gao, J.; Siemasko, K. Desiccating stress induces T cell-mediated Sjogren’s Syndrome-like lacrimal keratoconjunctivitis. J. Immunol. 2006, 176, 3950–3957. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Chen, W.; De Paiva, C.S.; Corrales, R.M.; Volpe, E.A.; McClellan, A.J.; Farley, W.J.; Li, D.Q.; Pflugfelder, S.C. Interferon-γ Exacerbates Dry Eye-Induced Apoptosis in Conjunctiva through Dual Apoptotic Pathways. Investig. Ophthalmol. Vis. Sci. 2011, 52, 6279–6285. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.S.; Chotikavanich, S.; Pangelinan, S.B.; Pitcher, J.D., 3rd; Fang, B.; Zheng, X.; Farley, W.J.; Li, D.Q.; Pflugfelder, S.C. IL-17 disrupts corneal barrier following desiccating stress. Mucosal Immunol. 2009, 2, 243–253. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.S.; Raince, J.K.; McClellan, A.J.; Shanmugam, K.P.; Pangelinan, S.B.; Volpe, E.A.; Corrales, R.M.; Farley, W.J.; Corry, D.B.; Li, D.Q.; Pflugfelder, S.C. Homeostatic control of conjunctival mucosal goblet cells by NKT-derived IL-13. Mucosal Immunol. 2011, 4, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Nepp, J.; Wirth, M. Fluctuations of Corneal Sensitivity in Dry Eye Syndromes—A Longitudinal Pilot Study. Cornea 2015, 34, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Cruzat, A.; Witkin, D.; Baniasadi, N.; Zheng, L.; Ciolino, J.B.; Jurkunas, U.V.; Chodosh, J.; Pavan-Langston, D.; Dana, R.; Hamrah, P. Inflammation and the nervous system: The connection in the cornea in patients with infectious keratitis. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5136–5143. [Google Scholar] [CrossRef] [PubMed]
- Waterman, S.A.; Gordon, T.P.; Rischmueller, M. Inhibitory effects of muscarinic receptor autoantibodies on parasympathetic neurotransmission in Sjögren’s syndrome. Arthritis Rheum. 2000, 43, 1647–1654. [Google Scholar] [CrossRef]
- Wickham, L.A.; Rocha, E.M.; Gao, J.; Krenzer, K.L.; da Silveira, L.A.; Toda, I.; Sullivan, D.A. Identification and hormonal control of sex steroid receptors in the eye. Adv. Exp. Med. Biol. 1998, 438, 95–100. [Google Scholar] [PubMed]
- Nakata, M.; Okada, Y.; Kobata, H.; Shigematsu, T.; Reinach, P.S.; Tomoyose, K.; Saika, S. Diabetes mellitus suppresses hemodialysis-induced increases in tear fluid secretion. BMC Res. Notes 2014, 7, 78. [Google Scholar] [CrossRef] [PubMed]
- Hyndiuk, R.A.; Kazarian, E.L.; Schultz, R.; Seideman, S. Neurotrophic corneal ulcers in diabetes mellitus. Arch. Ophthalmol. 1977, 95, 2193–2196. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Zalisnak, D.; Nash, D.; Yeu, E. Ocular surface diseases and corneal refractive surgery. Curr. Opin. Ophthalmol. 2014, 25, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Sutu, C.; Fukuoka, H.; Afshari, N.A. Mechanisms and management of dry eye in cataract surgery patients. Curr. Opin. Ophthalmol. 2016, 27, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Ang, R.T.; Dartt, D.A.; Tsubota, K. Dry eye after refractive surgery. Curr. Opin. Ophthalmol. 2001, 12, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Krenzer, K.L.; Reza Dana, M.; Ullman, M.D.; Cermak, J.M.; Tolls, D.B.; Evans, J.E.; Sullivan, D.A. Effect of Androgen Deficiency on the Human Meibomian Gland and Ocular Surface 1. J. Clin. Endocrinol. Metab. 2000, 85, 4874–4882. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.A.; Sullivan, B.D.; Evans, J.E.; Schirra, F.; Yamagami, H.; Liu, M.; Richards, S.M.; Suzuki, T.; Schaumberg, D.A.; Sullivan, R.M.; et al. Androgen deficiency, meibomian gland dysfunction, and evaporative dry eye. Ann. N. Y. Acad. Sci. 2002, 966, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Arakaki, R.; Ishimaru, N.; Hayashi, Y. Immunotherapeutic targets in estrogen deficiency-dependent Sjögren’s syndrome-related manifestations. Immunotherapy 2010, 2, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Sadeghi, P.B.; Akpek, E.K. Occult thyroid eye disease in patients presenting with dry eye symptoms. Am. J. Ophthalmol. 2009, 147, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Chauhan, S.K.; El Annan, J.; Nallasamy, N.; Zhang, Q.; Dana, R. Evidence of Corneal Lymphangiogenesis in Dry Eye Disease: A Potential Link to Adaptive Immunity? Arch. Ophthalmol. 2010, 128, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Min, J.H.; Lee, C.H.; Ji, Y.W.; Yeo, A.; Noh, H.; Song, I.; Kim, E.K.; Lee, H.K. Activation of Dll4/Notch Signaling and Hypoxia-Inducible Factor-1 α Facilitates Lymphangiogenesis in Lacrimal Glands in Dry Eye. PLoS ONE 2016, 11, e0147846. [Google Scholar] [CrossRef] [PubMed]
- Watters, G.A.; Turnbull, P.R.; Swift, S.; Petty, A.; Craig, J.P. Ocular surface microbiome in meibomian gland dysfunction. Clin. Exp. Ophthalmol. 2017, 45, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, R.; Satpathy, G.; Sangwan, S.; Kapil, A.; Aron, N.; Agarwal, T.; Pushker, N.; Sharma, N. Conjunctival Microbial Flora in Ocular Stevens–Johnson Syndrome Sequelae Patients at a Tertiary Eye Care Center. Cornea 2016, 35, 1117–1121. [Google Scholar] [CrossRef] [PubMed]
- Kugadas, A.; Gadjeva, M. Impact of Microbiome on Ocular Health. Ocul. Surf. 2016, 14, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Pflugfelder, S.C.; Geerling, G.; Kinoshita, S.; Lemp, M.A.; McCulley, J.; Nelson, D.; Novack, G.N.; Shimazaki, J.; Wilson, C. Management and therapy of dry eye disease: Report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 163–178. [Google Scholar]
- Sullivan, B.D.; Crews, L.A.; Messmer, E.M.; Foulks, G.N.; Nichols, K.K.; Baenninger, P.; Geerling, G.; Figueiredo, F.; Lemp, M.A. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: Clinical implications. Acta Ophthalmol. 2014, 92, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Viso, E.; Rodríguez-Ares, M.T.; Abelenda, D.; Oubiña, B.; Gude, F. Prevalence of asymptomatic and symptomatic meibomian gland dysfunction in the general population of Spain. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2601–2606. [Google Scholar] [CrossRef] [PubMed]
- Kojima, T.; Ishida, R.; Dogru, M.; Goto, E.; Matsumoto, Y.; Kaido, M.; Tsubota, K. The effect of autologous serum eyedrops in the treatment of severe dry eye disease: A prospective randomized case-control study. Am. J. Ophthalmol. 2005, 139, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Semeraro, F.; Forbice, E.; Nascimbeni, G.; Taglietti, M.; Romano, V.; Guerra, G.; Costagliola, C. Effect of Autologous Serum Eye Drops in Patients with Sjögren Syndrome-related Dry Eye: Clinical and In Vivo Confocal Microscopy Evaluation of the Ocular Surface. In Vivo 2016, 30, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; He, H.; Lin, Z.; Luo, P.; He, H.; Zhou, T.; Zhou, T. Therapeutic effects of epidermal growth factor on benzalkonium chloride-induced dry eye in a mouse model. Investig. Ophthalmol. Vis. Sci. 2012, 53, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Luo, P.; Zhao, H.; Chen, J.; He, H.; Xu, Y.; Lin, Z.; Zhou, Y.; Xu, J.; Liu, Z. Amniotic membrane extract ameliorates benzalkonium chloride-induced dry eye in a murine model. Exp. Eye Res. 2013, 115, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Gris, O.; del Campo, Z.; Wolley-Dod, C.; Guell, J.L.; Bruix, A.; Calatayud, M.; Adán, A. Amniotic membrane implantation as a therapeutic contact lens for the treatment of epithelial disorders. Cornea 2002, 21, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Bacon, A.S.; Astin, C.; Dart, J.K. Silicone rubber contact lenses for the compromised cornea. Cornea 1994, 13, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Pullum, K.W.; Whiting, M.A.; Buckley, R.J. Scleral contact lenses: The expanding role. Cornea 2005, 24, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Maulvi, F.A.; Shaikh, A.A.; Lakdawala, D.H.; Desai, A.R.; Pandya, M.M.; Singhania, S.S.; Vaidya, R.J.; Ranch, K.M.; Vyas, B.A.; Shah, D.O. Design and optimization of a novel implantation technology in contact lenses for the treatment of dry eye syndrome: In vitro and in vivo evaluation. Acta Biomater. 2017, 53, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Luo, L.; Pflugfelder, S.C.; Li, D.-Q. Doxycycline Inhibits TGF-β1–Induced MMP-9 via Smad and MAPK Pathways in Human Corneal Epithelial Cells. Investig. Ophthalmol. Vis. Sci. 2005, 46, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Kymionis, G.D.; Bouzoukis, D.I.; Diakonis, V.F.; Siganos, C. Treatment of chronic dry eye: Focus on cyclosporine. Clin. Ophthalmol. 2008, 2, 829–836. [Google Scholar] [CrossRef] [PubMed]
- De Paiva, C.; Pflugfelder, S. Rationale for anti-inflammatory therapy in dry eye syndrome. Arquivos Brasileiros de Oftalmologia 2008, 71, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Deng, R.; Su, Z.; Hua, X.; Zhang, Z.; Li, D.Q.; Pflugfelder, S.C. Osmoprotectants suppress the production and activity of matrix metalloproteinases induced by hyperosmolarity in primary human corneal epithelial cells. Mol. Vis. 2014, 20, 1243–1252. [Google Scholar] [PubMed]
- Sommer, A. Effects of Vitamin A Deficiency on the Ocular Surface. Ophthalmology 1983, 90, 592–600. [Google Scholar] [CrossRef]
- Kim, E.C.; Choi, J.-S.; Joo, C.K. A Comparison of Vitamin A and Cyclosporine A 0.05% Eye Drops for Treatment of Dry Eye Syndrome. Am. J. Ophthalmol. 2009, 147, 206–213.e3. [Google Scholar] [CrossRef] [PubMed]
- Guzman-Aranguez, A.; Gasull, X.; Diebold, Y.; Pintor, J. Purinergic Receptors in Ocular Inflammation. Mediat. Inflamm. 2014, 2014, 320906. [Google Scholar] [CrossRef] [PubMed]
- Keating, G.M. Diquafosol Ophthalmic Solution 3%: A Review of Its Use in Dry Eye. Drugs 2015, 75, 911–922. [Google Scholar] [CrossRef] [PubMed]
- Jehangir, N.; Bever, G.; Mahmood, S.M.J.; Moshirfar, M. Comprehensive Review of the Literature on Existing Punctal Plugs for the Management of Dry Eye Disease. J. Ophthalmol. 2016, 2016, 9312340. [Google Scholar] [CrossRef] [PubMed]
- Gottenberg, J.; Ravaud, P.; Puéchal, X.; Larroche, C.; Dubost, J.J.; Rist, S.; Saraux, A. Effects of hydroxychloroquine on symptomatic improvement in primary sjögren syndrome: The joquer randomized clinical trial. JAMA 2014, 312, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Faustman, D.L.; Vivino, F.B.; Carsons, S.E. TReatment of primary sjögren syndrome with rituximab. Ann. Intern. Med. 2014, 161, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Mariette, X.; Seror, R.; Quartuccio, L.; Baron, G.; Salvin, S.; Fabris, M.; Desmoulins, F.; Nocturne, G.; Ravaud, P.; de Vita, S. Efficacy and safety of belimumab in primary Sjögren’s syndrome: Results of the BELISS open-label phase II study. Ann. Rheum. Dis. 2015, 74, 526. [Google Scholar] [CrossRef] [PubMed]
- Holdgate, N.; St Clair, E.W. Recent advances in primary Sjogren’s syndrome. F1000Research 2016, 5, F1000. [Google Scholar] [CrossRef] [PubMed]
- Kossler, A.L.; Wang, J.; Feuer, W.; Tse, D.T. Neurostimulation of the lacrimal nerve for enhanced tear production. Ophthalmic Plast. Reconstr. Surg. 2015, 31, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, M.; Ogawa, M.; Oshima, M.; Sekine, Y.; Ishida, K.; Yamashita, K.; Desmoulins, F.; Nocturne, G.; Ravaud, P.; de Vita, S. Functional lacrimal gland regeneration by transplantation of a bioengineered organ germ. Nat. Commun. 2013, 4, 2497. [Google Scholar] [CrossRef] [PubMed]
- Greiner, J.V. A Single LipiFlow® Thermal Pulsation System Treatment Improves Meibomian Gland Function and Reduces Dry Eye Symptoms for 9 Months. Curr. Eye Res. 2012, 37, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Chen, Y.-H.; Turnbull, P.R.K. Prospective Trial of Intense Pulsed Light for the Treatment of Meibomian Gland DysfunctionProspective Trial of IPL for Treatment of MGD. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1965–1970. [Google Scholar] [CrossRef] [PubMed]
- Oleñik, A.; Mahillo-Fernández, I.; Alejandre-Alba, N.; Fernández-Sanz, G.; Pérez, M.A.; Luxan, S.; Quintana, S.; Martínez de Carneros Llorente, A.; García-Sandoval, B.; Jiménez-Alfaro, I. Benefits of ω-3 fatty acid dietary supplementation on health-related quality of life in patients with meibomian gland dysfunction. Clin. Ophthalmol. 2014, 8, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Korb, D.R.; Blackie, C.A.; Finnemore, V.M.; Douglass, T. Effect of using a combination of lid wipes, eye drops, and ω-3 supplements on meibomian gland functionality in patients with lipid deficient/evaporative dry eye. Cornea 2015, 34, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Fadlallah, A.; Rami, H.E.; Fahd, D.; Dunia, I.; Bejjani, R.; Chlela, E.; Waked, N.; Jabbour, E.; Fahed, S. Azithromycin 1.5% ophthalmic solution: Efficacy and treatment modalities in chronic blepharitis. Arquivos Brasileiros de Oftalmologia 2012, 75, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Kashkouli, M.B.; Fazel, A.J.; Kiavash, V.; Nojomi, M.; Ghiasian, L. Oral azithromycin versus doxycycline in meibomian gland dysfunction: A randomised double-masked open-label clinical trial. Br. J. Ophthalmol. 2015, 99, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.; Currie, Z.; Collin, J.R.O. Ophthalmic management of facial nerve palsy. Eye 2004, 18, 1225–1234. [Google Scholar] [CrossRef] [PubMed]
- Ichijima, H.; Petroll, W.M.; Jester, J.V.; Cavanagh, H.D. Confocal microscopic studies of living rabbit cornea treated with benzalkonium chloride. Cornea 1992, 11, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Gilbard, J.P.; Rossi, S.R. An electrolyte-based solution that increasescorneal glycogen and conjunctival goblet-cell density in a rabbit model for keratoconjunctivitis sicca. Ophthalmology 1992, 99, 600. [Google Scholar] [CrossRef]
- Velpandian, T.; Moksha, L. Mucoadhesive Polymers and Ocular Lubricants. In Pharmacology of Ocular Therapeutics; Velpandian, T., Ed.; Springer: Cham, Switzerland, 2016; pp. 269–283. [Google Scholar]
- Zheng, X.; Goto, T.; Ohashi, Y. Comparison of In Vivo Efficacy of Different Ocular Lubricants in Dry Eye Animal ModelsEfficacy of Ocular Lubricants in Animal Model. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3454–3460. [Google Scholar] [CrossRef] [PubMed]
- Simmons, P.A.; Carlisle-Wilcox, C.; Vehige, J.G. Comparison of novel lipid-based eye drops with aqueous eye drops for dry eye: A multicenter, randomized controlled trial. Clin. Ophthalmol. 2015, 9, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Purslow, C.; Murphy, P.J.; Wolffsohn, J.S. Effect of a liposomal spray on the pre-ocular tear film. Contact Lens Anterior Eye 2010, 33, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.Y.; Lee, Y.K.; Tsai, S.H.; Lin, Y.C.; Chen, Y.M. Autologous Serum Eye Drops Combined with Silicone Hydrogen Lenses for the Treatment of Postinfectious Corneal Persistent Epithelial Defects. Eye Contact Lens 2017, 43, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Petrone, D.; Condemi, J.J.; Fife, R.; Gluck, O.; Cohen, S.; Dalgin, P. A double-blind, randomized, placebocontrolled study of cevimeline in Sjogren’s syndrome patients with xerostomia and keratoconjunctivitis sicca. Arthritis Rheum. 2002, 46, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Koh, S. Clinical utility of 3% diquafosol ophthalmic solution in the treatment of dry eyes. Clin. Ophthalmol. 2015, 9, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Nakamachi, T.; Ohtaki, H.; Seki, T.; Yofu, S.; Kagami, N.; Hashimoto, H.; Shintani, N.; Baba, A.; Mark, L.; Lanekoff, I. PACAP suppresses dry eye signs by stimulating tear secretion. Nat. Commun. 2016, 7, 12034. [Google Scholar] [CrossRef] [PubMed]
- Friedman, N.J.; Butron, K.; Robledo, N.; Loudin, J.; Baba, S.N.; Chayet, A. A nonrandomized, open-label study to evaluate the effect of nasal stimulation on tear production in subjects with dry eye disease. Clin. Ophthalmol. 2016, 10, 795–804. [Google Scholar] [PubMed]
- Hart, D.E.; Simko, M.; Harris, E. How to produce moisture chamber eyeglasses for the dry eye patient. J. Am. Optom. Assoc. 1994, 65, 517–522. [Google Scholar] [PubMed]
- Romero-Rangel, T.; Stavrou, P.; Cotter, J.; Rosenthal, P.; Baltatzis, S.; Foster, C.S. Gas-permeable scleral contact lens therapy in ocular surface disease. Am. J. Ophthalmol. 2000, 130, 25–32. [Google Scholar] [CrossRef]
- Dimit, R.; Gire, A.; Pflugfelder, S.C.; Bergmanson, J.P. Patient ocular conditions and clinical outcomes using a PROSE scleral device. Contact Lens Anterior Eye 2013, 36, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Theophanous, C.; Irvine, J.A.; Parker, P.; Chiu, G.B. Use of Prosthetic Replacement of the Ocular Surface Ecosystem Scleral Lenses in Patients with Ocular Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2015, 21, 2180–2184. [Google Scholar] [CrossRef] [PubMed]
- Goto, E.; Shimazaki, J.; Monden, Y.; Takano, Y.; Yagi, Y.; Shimmura, S.; Tsubota, K. Low-concentration homogenized castor oil eye drops for noninflamed obstructive meibomian gland dysfunction. Ophthalmology 2002, 109, 2030–2035. [Google Scholar] [CrossRef]
- Tai, M.C.; Cosar, C.B.; Cohen, E.J.; Rapuano, C.J.; Laibson, P.R. The clinical efficacy of silicone punctal plug therapy. Cornea 2002, 21, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Gilbard, J.P.; Rossi, S.R.; Azar, D.T.; Heyda, K.G. Effect of punctal occlusion by Freeman silicone plug insertion on tear osmolarity in dry eye disorders. CLAO J. 1989, 15, 216–218. [Google Scholar] [PubMed]
- Shi, S.; Chen, W.; Zhang, X.; Ma, H.X.; Sun, L. Effects of silicone punctal plugs for tear deficiency dry eye patients. Chin. J. Ophthalmol. 2013, 49, 151–154. [Google Scholar]
- Tong, L.; Beuerman, R.; Simonyi, S.; Hollander, D.A.; Stern, M.E. Effects of Punctal Occlusion on Clinical Signs and Symptoms and on Tear Cytokine Levels in Patients with Dry Eye. Ocul. Surf. 2016, 14, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. How corticosteroids control inflammation: Quintiles Prize Lecture 2005. Br. J. Pharmacol. 2006, 148, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Colligris, B.; Crooke, A.; Huete-Toral, F.; Pintor, J. An update on dry eye disease molecular treatment: Advances in drug pipelines. Expert Opin. Pharmacother. 2014, 15, 1371–1390. [Google Scholar] [CrossRef] [PubMed]
- Nye, M.; Rudner, S.; Bielory, L. Emerging therapies in allergic conjunctivitis and dry eye syndrome. Expert Opin. Pharmacother. 2013, 14, 1449–1465. [Google Scholar] [CrossRef] [PubMed]
- Pinto-Fraga, J.; Lopez-Miguel, A.; Gonzalez-Garcia, M.J.; Fernandez, I.; Lopez-de-la-Rosa, A.; Enriquez-de-Salamanca, A.; Stern, M.E.; Calonge, M. Topical Fluorometholone Protects the Ocular Surface of Dry Eye Patients from Desiccating Stress: A Randomized Controlled Clinical Trial. Ophthalmology 2016, 123, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Patane, M.A.; Cohen, A.; From, S.; Torkildsen, G.; Welch, D.; Ousler, G.W., 3rd. Ocular iontophoresis of EGP-437 (dexamethasone phosphate) in dry eye patients: Results of a randomized clinical trial. Clin. Ophthalmol. 2011, 5, 633–643. [Google Scholar] [PubMed]
- Chen, J.; Dong, F.; Chen, W.; Sun, X.; Deng, Y.; Hong, J.; Zhang, M.; Yang, W.; Liu, Z.; Xie, L. Clinical efficacy of 0.1% pranoprofen in treatment of dry eye patients: A multicenter, randomized, controlled clinical trial. Chin. Med. J. 2014, 127, 2407–2412. [Google Scholar] [PubMed]
- Fujishima, H.; Fuseya, M.; Ogata, M.; Murat, D. Efficacy of bromfenac sodium ophthalmic solution for treatment of dry eye disease. Asia-Pac. J. Ophthalmol. 2015, 4, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Sosne, G.; Ousler, G.W. Thymosin β 4 ophthalmic solution for dry eye: A randomized, placebo-controlled, Phase II clinical trial conducted using the controlled adverse environment (CAE) model. Clin. Ophthalmol. 2015, 9, 877–884. [Google Scholar] [PubMed]
- Zhang, L.; Su, Z.; Zhang, Z.; Lin, J.; Li, D.; Pflugfelder, S.C. Effects of azithromycin on gene expression profiles of proinflammatory and anti-inflammatory mediators in the eyelid margin and conjunctiva of patients with meibomian gland disease. JAMA Ophthalmol. 2015, 133, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Brignole, F.; Pisella, P.J.; Goldschild, M.; De Saint Jean, M.; Goguel, A.; Baudouin, C. Flow Cytometric Analysis of Inflammatory Markers in Conjunctival Epithelial Cells of Patients with Dry Eyes. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1356–1363. [Google Scholar]
- Gürdal, C.; Genç, İ.; Saraç, Ö.; Gönül, İ.; Takmaz, T.; Can, İ. Topical Cyclosporine in Thyroid Orbitopathy-Related Dry Eye: Clinical Findings, Conjunctival Epithelial Apoptosis, and MMP-9 Expression. Curr. Eye Res. 2010, 35, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Siekierka, J.J.; Hung, S.H.Y.; Poe, M.; Lin, C.S.; Sigal, N.H. A cytosolic binding protein for the immunosuppressant FK506 has peptidyl-prolyl isomerase activity but is distinct from cyclophilin. Nature 1989, 341, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Moscovici, B.K.; Holzchuh, R.; Sakassegawa-Naves, F.E.; Hoshino-Ruiz, D.R.; Albers, M.B.; Santo, R.M.; Hida, R.Y. Treatment of Sjogren’s syndrome dry eye using 0.03% tacrolimus eye drop: Prospective double-blind randomized study. Contact Lens Anterior Eye 2015, 38, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Tauber, J.; Karpecki, P.; Latkany, R.; Luchs, J.; Martel, J.; Sall, K.; Raychaudhuri, A.; Smith, V.; Semba, C.P. Lifitegrast Ophthalmic Solution 5.0% versus Placebo for Treatment of Dry Eye Disease: Results of the Randomized Phase III OPUS-2 Study. Ophthalmology 2015, 122, 2423–2431. [Google Scholar] [CrossRef] [PubMed]
- Donnenfeld, E.D.; Karpecki, P.M.; Majmudar, P.A.; Nichols, K.K.; Raychaudhuri, A.; Roy, M.; Semba, C.P. Safety of Lifitegrast Ophthalmic Solution 5.0% in Patients With Dry Eye Disease: A 1-Year, Multicenter, Randomized, Placebo-Controlled Study. Cornea 2016, 35, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, J.D.; Torkildsen, G.L.; Lonsdale, J.D.; D’Ambrosio, F.A.; McLaurin, E.B.; Eiferman, R.A.; Kennedy, K.S.; Semba, C.P. Lifitegrast ophthalmic solution 5.0% for treatment of dry eye disease: Results of the OPUS-1 phase 3 study. Ophthalmology 2014, 121, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.F.; Yafawi, R.; Zhang, M.; McDowell, M.; Rittenhouse, K.D.; Sace, F.; Liew, S.H.; Cooper, S.R.; Pickering, E.H. Immunomodulatory Effect of the Topical Ophthalmic Janus Kinase Inhibitor Tofacitinib (CP-690,550) in Patients with Dry Eye Disease. Ophthalmology 2012, 119, e43–e50. [Google Scholar] [CrossRef] [PubMed]
- Liew, S.H.; Nichols, K.K.; Klamerus, K.J.; Li, J.Z.; Zhang, M.; Foulks, G.N. Tofacitinib (CP-690,550), a Janus Kinase Inhibitor for Dry Eye Disease: Results from a Phase 1/2 Trial. Ophthalmology 2012, 119, 1328–1335. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, K.; Fujimoto, Y.; Takeuchi, T.; Azuma, Y.T. Aggressive Crosstalk Between Fatty Acids and Inflammation in Macrophages and Their Influence on Metabolic Homeostasis. Neurochem. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Barabino, S.; Rolando, M.; Camicione, P.; Ravera, G.; Zanardi, S.; Giuffrida, S.; Calabria, G. Systemic linoleic and gamma-linolenic acid therapy in dry eye syndrome with an inflammatory component. Cornea 2003, 22, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Lambiase, A.; Aloe, L.; Mantelli, F.; Sacchetti, M.; Perrella, E.; Bianchi, P.; Rocco, M.L.; Bonini, S. Capsaicin-Induced Corneal Sensory Denervation and Healing Impairment Are Reversed by NGF TreatmentNGF in Experimental Corneal Denervation. Investig. Ophthalmol. Vis. Sci. 2012, 53, 8280–8287. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Lee, K.S.; Kim, H.C.; Lee, S.H.; Kim, E.K. Nerve growth factor concentration and implications in photorefractive keratectomy vs laser in situ keratomileusis. Am. J. Ophthalmol. 2005, 139, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.J.; Im, Y.S.; Kay, E.P.; Kim, J.Y.; Lee, J.E.; Lee, H.K. The role of nerve growth factor in hyperosmolar stress induced apoptosis. J. Cell. Physiol. 2008, 216, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Worda, C.; Nepp, J.; Huber, J.C.; Sator, M.O. Treatment of keratoconjunctivitis sicca with topical androgen. Maturitas 2001, 37, 209–212. [Google Scholar] [CrossRef]
- Rocha, E.; Wickham, L.; da Silveira, L.A.; Krenzer, K.; Yu, F.; Toda, I.; Sullivan, B.D.; Sullivan, D.A. Identification of androgen receptor protein and 5α-reductase mRNA in human ocular tissues. Br. J. Ophthalmol. 2000, 84, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Chauhan, S.K.; Dana, R. Blockade of Prolymphangiogenic VEGF-C suppresses Dry Eye Disease. Arch. Ophthalmol. 2012, 130, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Su, W.; Huang, J.; Zhou, J.; Qiu, S.; Liang, D. Doxycycline Inhibits Inflammation-Induced Lymphangiogenesis in Mouse Cornea by Multiple Mechanisms. PLoS ONE 2014, 9, e108931. [Google Scholar] [CrossRef] [PubMed]
- Fraunfelder, F.W. Liquid nitrogen cryotherapy for conjunctival lymphangiectasia: A case series. Trans. Am. Ophthalmol. Soc. 2009, 107, 229–232. [Google Scholar] [PubMed]
- Tan, J.C.; Mann, S.; Coroneo, M.T. Successful Treatment of Conjunctival Lymphangiectasia with Subconjunctival Injection of Bevacizumab. Cornea 2016, 35, 1375–1377. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Layers of the Tear Film | Compromised Components Related to Tear Film Instability and Ocular Surface Homeostasis | |
|---|---|---|
| Lipid layer [81,102,103] | ↓ Cholesteryl esters, ↓ Free fatty acids | Involved in evaporation retardation and possess surface-active properties |
| ↓ Wax esters | Bridge the polar and non-polar lipid phase, exert a condensing effect, due to the presence of the saturated fatty acid component | |
| ↓ Ttriacyl glycerides | Act as a buffer system for the phospholipids to resist the surface pressure changes in the air water interface | |
| ↓ Pphospholipids, ↓ Sphingomyelin, ↓ Cerebrosides | Maintains the integrity and arrangement of the non-polar lipids | |
| Aqueous layer [104,105,106] | ↓ Lipocalin | Involved in preventing corneal desiccation by scavenging lipids, removes fatty acid and phospholipid from the ocular surface |
| ↓ Lyzozymes | Act as an antibacterial agent by hydrolysing the β-(1-4) glycosidic linkages between bacterial cell wall carbohydrates | |
| ↓ Secretory Ig A | Prevents pathogen adhesion to the ocular surface epithelia, enhances phagocytosis | |
| ↓ Proline rich 4 protein | Act as an acute phase surfactant to maintain an antimicrobial environment in the ocular surface | |
| ↓ Lactoferrin | Act as an antibacterial, antiangiogenic, antiviral component | |
| ↓ Prolactin-inducible protein | Act as an antibacterial and influences the cell mediated immunity | |
| ↓ Zinc-α-2-glycoprotein | Involved in lipid metabolism | |
| ↓ Proteoglycan 4 (PRG 4/lubricin) | Act as a lubricant and surfactant preventing evaporation | |
| Mucin layer [107,108,109] | ↓ MUC5AC, ↓ MUC1, ↓ MUC4, ↓ MUC16 | Act as a barrier for pathogens and prevent microbial colonization, maintains the viscosity and surface tension of tear film |
| Components of OSM | Normal Function | Changes in Dry Eye | Targeting Therapy |
|---|---|---|---|
| Cornea | Normal barrier function Growth factors & cytokines Quiescent keratocytes | Scarring & ulcer Opacification Neovascularization Pannus formation Squamous metaplasia Extracellular matrix degradation ↓ Endothelial cell number | Lubricants Autologous serum Growth factors Amniotic membrane extract Amniotic membrane Contact lens MMP-9 inhibitors |
| Conjunctiva | Immune defense Secrets mucin | Squamous metaplasia ↓ Goblet cell density Chronic inflammation Conjunctivochalasis | Autologous serum Amniotic membrane Vitamin A MMP-9 inhibitor Growth factors Rebamipide Gefarnate Diquafosol tetrasodium Hydroxyeicosatetraenoic acid |
| Lacrimal Gland | Secretes: Fluid Mucopolysaccharides Electrolyte Microbicidal and other proteins Mucin | ↓ Aqueous tear ↓ Acinar and ductal cells Fibrosis Apoptosis Inflammation | Lubricants Immunomodulators Secretagogue Neurostimulation Cyclosporin A |
| Meibomian Gland | Accomplishes lipogenisis Secretes meibum Maintains tear film stability Prevents tear film evaporation | ↓ Meibum ↑ Tear evaporation ↑ Keratinization Apoptosis Inflammation | Warm compress Lid hygiene Lipiflow System™ Intense-Pulsed-Light ω-3 fatty acid Liposomal sprays |
| Eyelid | Physical defense Meibum distribution Prevents tear film evaporation | ↓ Eyelid laxity ↑ Tear evaporation Corneal ulcer Epithelial defect Inflammation Infrequent and ineffective blinking | Warm compress Lid hygiene Antibiotics Surgery |
| Tear Film | Ocular surface homeostasis Moistens & lubricates Transports nutrient & oxygen | Tear hyperosmolarity Tear film instability Excessive tear film evaporation Delayed tear clearance | Compensation of tear Artificial tears/serum Tear stimulation Pilocarpine, Pituitary adenylate cyclase-activating polypeptide, Diquafosol tetrasodium, Oculeve intranasal neurostimulation device Controlling tear evaporation Moisture-retaining eyeglasses, Swimming goggles, Prosthetic Replacement of the Ocular Surface Ecosystems, Castor oil eye drops Regulating excessive nasolacrimal drainage Punctal plugs |
| Inflammation | Immune homeostasis | Chronic inflammation ↑ Pro-inflammatory cytokine, ↑ Chemokine ↓ Glandular secretion ↑ Reactive oxygen species ↑ Apoptosis CD4+ T cells-mediated pathogenesis | Corticosteroids Nonsteroidal anti-inflammatory drugs Doxycycline Azithromycin Cyclosporin A FK506 Lifitegrast Tofacitinib Fatty acids |
| Nerve | Secretes neurotransmitters & nerve growth factors Controls tear reflex & landular secretions | ↓ Neuronal stimuli ↓ Corneal sensitivity Altered nerve morphology | Neurostimulation Nerve growth factor |
| Systemic hormones | Ocular surface homeostasis Regulates meibomain gland & lacrimal gland | Androgen deficiency Estrogen deficiency Thyroid hormones state disorder | Hormonal supplementation Androgen & estrogen receptor inhibitors |
| Vascular and Lymphatic systems | Transports growth factors Immune response Oxygen supply Lipogenesis | Lymphangiogenesis Hemangiogenesis | Anti lymphangiogenic agents |
| Ocular surface microbiome | Immune tolerance Eliminates pathogens Mucin turnover | Colonization of normal flora Opportunistic pathogen Drug resistance Infectious keratitis Conjunctivitis | Topical antibiotics Corticosteroids |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; M, V.J.; Qu, Y.; He, X.; Ou, S.; Bu, J.; Jia, C.; Wang, J.; Wu, H.; Liu, Z.; et al. Dry Eye Management: Targeting the Ocular Surface Microenvironment. Int. J. Mol. Sci. 2017, 18, 1398. https://doi.org/10.3390/ijms18071398
Zhang X, M VJ, Qu Y, He X, Ou S, Bu J, Jia C, Wang J, Wu H, Liu Z, et al. Dry Eye Management: Targeting the Ocular Surface Microenvironment. International Journal of Molecular Sciences. 2017; 18(7):1398. https://doi.org/10.3390/ijms18071398
Chicago/Turabian StyleZhang, Xiaobo, Vimalin Jeyalatha M, Yangluowa Qu, Xin He, Shangkun Ou, Jinghua Bu, Changkai Jia, Junqi Wang, Han Wu, Zuguo Liu, and et al. 2017. "Dry Eye Management: Targeting the Ocular Surface Microenvironment" International Journal of Molecular Sciences 18, no. 7: 1398. https://doi.org/10.3390/ijms18071398