Short-Term Choriocapillaris Changes in Patients with Central Serous Chorioretinopathy after Half-Dose Photodynamic Therapy


Abstract
:
1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Visual Acuity
2.3. PDT
2.4. OCT
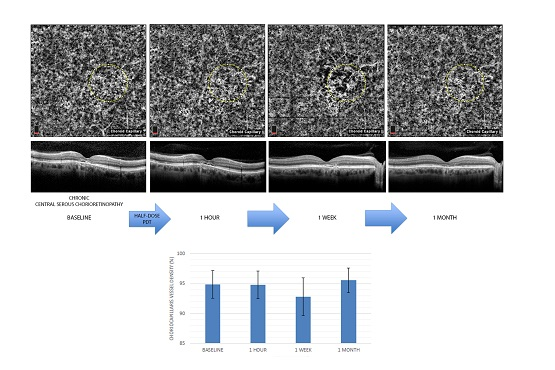
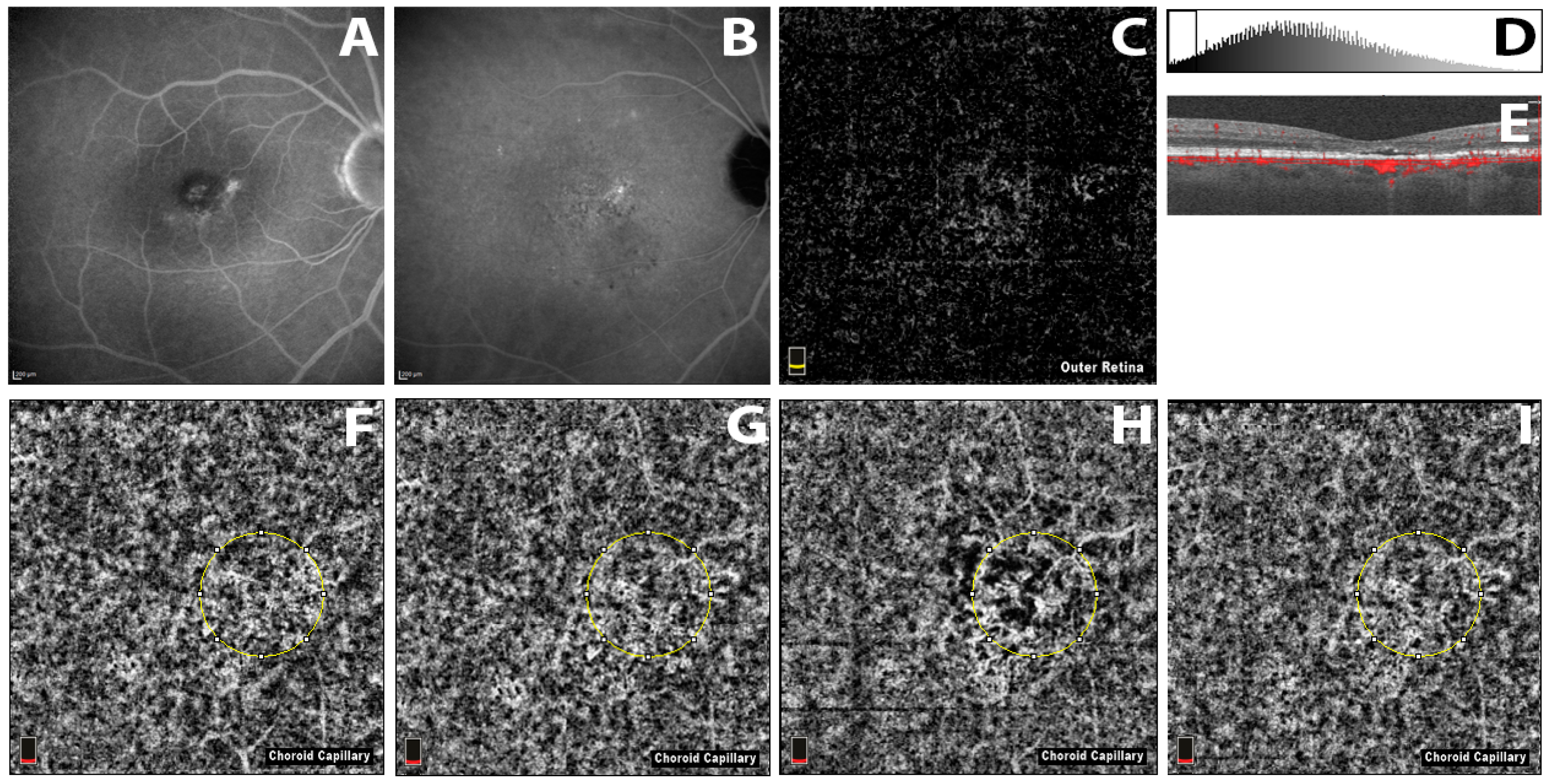
2.5. OCTA
2.5.1. Repeatability Assessment
2.5.2. Affected Eyes
2.5.3. Comparison with Fellow Eyes
3. Discussion
4. Materials and Methods
- Snellen BCVA of 20/200 or better
- Presence of active leakage on fluorescein angiography (FA) and choroidal vascular hyperpermeability on indocyanine green angiography (ICGA)
- Absence of CNV evidence on OCTA, FA and ICGA
- Absence of PED or posterior cystoid retinal degeneration
- Absence of any previous treatment
- Absence of any other chorioretinal disease
- Absence of media opacities
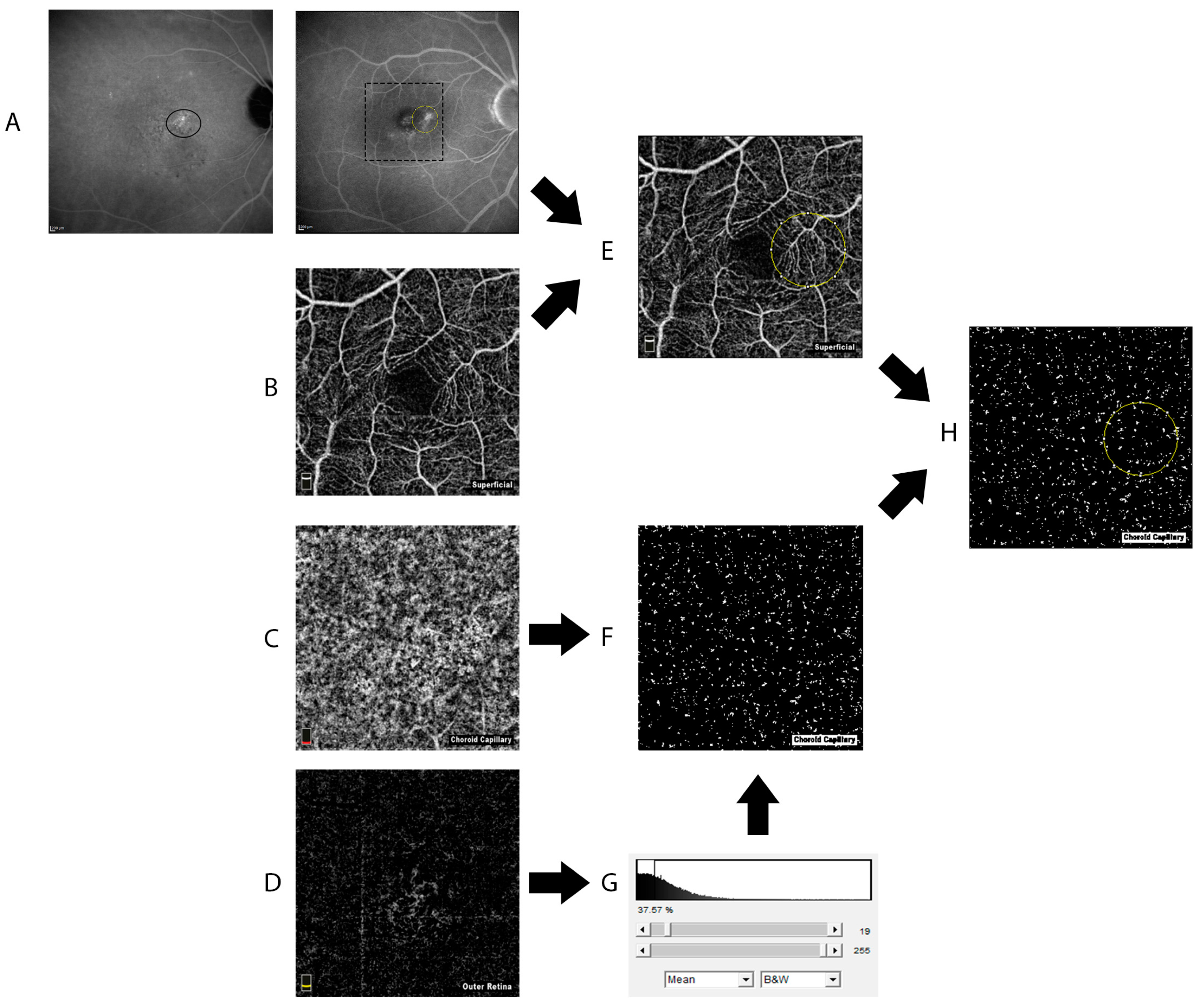
4.1. OCT-Angiography
4.2. Data Analysis and Statistic
- All data are presented as Mean ± Standard Deviation.
- The Shapiro-Wilk test was used to verify the normal distribution of data [17].
- Differences between data sets were evaluated with paired t-test.
- Repeatability between the two measurements from different operators was assessed evaluating the ICC.
- The Spearman coefficient was calculated to assess the correlation between CCVD and CFT.
- p value < 0.05 was considered significant.
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Gass, J.D.M. Pathogenesis of disciform detachment of the neuro-epithelium. II. Idiopathic central serous choroidopathy. Am. J. Ophthalmol. 1960, 63, 587–615. [Google Scholar]
- Kitzmann, A.S.; Pulido, J.S.; Diehl, N.N.; Hodge, D.O.; Burke, J.P. The incidence of central serous chorioretinopathy in Olmsted County, Minnesota, 1980–2002. Ophthalmology 2008, 115, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C.M.; Owens, S.L.; Smith, P.D.; Fine, S.L. Long-term follow-up of central serous chorioretinopathy. Br. J. Ophthalmol. 1984, 68, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Schachat, A.P.; Wilkinson, C.P. Ryan’s Retina, 6th ed.; Elsevier: New York, NY, USA, 2017; pp. 1464–1483. ISBN 9780323401975. [Google Scholar]
- Daruich, A.; Matet, A.; Dirani, A.; Bousquet, E.; Zhao, M.; Farman, N.; Jaisser, F.; Behar-Cohen, F. Central serous chorioretinopathy: Recent findings and new physiopathology hypothesis. Prog. Retin. Eye Res. 2015, 48, 82–118. [Google Scholar] [CrossRef] [PubMed]
- Teussink, M.M.; Breukink, M.B.; van Grinsven, M.J.; Hoyng, C.B.; Klevering, B.J.; Boon, C.J.; de Jong, E.K.; Theelen, T. OCT angiography compared to fluorescein and indocyanine green angiography in chronic central serous chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5229–5237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholson, B.; Noble, J.; Forooghian, F.; Meyerle, C. Central serous chorioretinopathy: Update on pathophysiology and treatment. Surv. Ophthalmol. 2013, 58, 103–126. [Google Scholar] [CrossRef] [PubMed]
- Salehi, M.; Wenick, A.S.; Law, H.A.; Evans, J.R.; Gehlbach, P. Interventions for central serous chorioretinopathy: A network meta-analysis. Cochrane Database Syst. Rev. 2015, CD011841. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Slakter, J.S.; Gross, N.E.; Spaide, R.F.; Costa, D.; Huang, S.J.; Klancnik, J.M., Jr.; Aizman, A. Indocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: A pilot study. Retina 2003, 23, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.I.; Glassman, A.R.; Aiello, L.P.; Chakravarthy, U.; Flaxel, C.J.; Spaide, R.F. Collaborative retrospective macula society study of photodynamic therapy forchronic central serous chorioretinopathy. Ophthalmology 2014, 121, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Nicoló, M.; Eandi, C.M.; Alovisi, C.; Grignolo, F.M.; Traverso, C.E.; Musetti, D.; Cardillo Piccolino, F. Half-fluence versus half-dose photodynamic therapy in chronic central serous chorioretinopathy. Am. J. Ophthalmol. 2014, 157, 1033–1037. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.M.; Lam, D.S.; Lai, T.Y.; Tam, B.S.; Liu, D.T.; Chan, C.K. Choroidal vascular remodelling in central serous chorioretinopathy after indocyanine green guided photodynamic therapy with verteporfin: A novel treatment at the primary disease level. Br. J. Ophthalmol. 2003, 87, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Schlötzer-Schrehardt, U.; Viestenz, A.; Naumann, G.O.; Laqua, A.; Michels, S.; Schmidt-Erfurth, U. Dose-related structural effects of photodynamic therapy on choroidal and retinal structures of human eyes. Graefes Arch. Clin. Exp. Ophthalmol. 2002, 240, 748–757. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Tan, O.; Tokayer, J.; Potsaid, B.; Wang, Y.; Liu, J.J.; Kraus, M.F.; Subhash, H.; Fujimoto, J.G.; Hornegger, J.; et al. Split-spectrum amplitude-decorrelation angiography with optical coherence tomography. Opt. Express 2012, 20, 4710–4725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quaranta-El Maftouhi, M.; El Maftouhi, A.; Eandi, C.M. Chronic central serous Chorioretinopathy imaged by optical coherence tomographic angiography. Am. J. Ophthalmol. 2015, 160, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.Y.; Wang, Q.; Wei, W.B.; Jonas, J.B. Optical coherence tomographic angiography in central serous chorioretinopathy. Retina 2016, 36, 2051–2058. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Piccolino, F.C.; de la Longrais, R.R.; Ravera, G.; Eandi, C.M.; Ventre, L.; Abdollah, A.; Manea, M. The foveal photoreceptor layer and visual acuity loss in central serous chorioretinopathy. Am. J. Ophthalmol. 2005, 139, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Cardillo Piccolino, F.; Eandi, C.M.; Ventre, L.; Rigault de la Longrais, R.C.; Grignolo, F.M. Photodynamic therapy for chronic central serous chorioretinopathy. Retina 2003, 23, 752–763. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.M.; Lai, T.Y.; Lai, R.Y.; Tang, E.W.; Liu, D.T.; Lam, D.S. Safety enhanced photodynamic therapy for chronic central serous chorioretinopathy: One-year results of a prospective study. Retina 2008, 28, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.M.; Lam, D.S.; Lai, T.Y.; Yuen, K.S.; Liu, D.T.; Chan, C.K.; Chen, W.Q. Treatment of choroidal neovascularization in central serous chorioretinopathy by photodynamic therapy with verteporfin. Am. J. Opthalmol. 2003, 136, 836–845. [Google Scholar] [CrossRef]
- Xu, Y.; Su, Y.; Li, L.; Qi, H.; Zheng, H.; Chen, C. Effect of photodynamic therapy on optical coherence tomography angiography in eyes with chronic central serous chorioretinopathy. Ophthalmologica 2017, 237, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Kawamura, A.; Yuzawa, M. Choriocapillaris changes imaged by OCT angiography after half-dose photodynamic therapy for chronic central serous chorioretinopathy. Ophthalmic Surg. Lasers Imaging Retina 2017, 48, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Alten, F.; Heiduschka, P.; Clemens, C.R.; Eter, N. Exploring choriocapillaris under reticular pseudodrusen using OCT-Angiography. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 2165–2173. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, E.; Cohen, S.Y.; Miere, A.; Querques, G.; Capuano, V.; Semoun, O.; El Ameen, A.; Oubraham, H.; Souied, E.H. Optical coherence tomography angiography in central serous chorioretinopathy. J. Ophthalmol. 2015, 2015, 134783. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Jonas, J.B.; Wei, W. Optical coherence tomography-assisted enhanced depth imaging of central serous chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2013, 54, 4659–4665. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Erfurth, U.; Hasan, T. Mechanisms of action of photodynamic therapy with verteporfin for the treatment of age-related macular degeneration. Surv. Ophthalmol. 2000, 45, 195–214. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Schlötzer-Schrehard, U.; Cursiefen, C.; Michels, S.; Beckendorf, A.; Naumann, G.O. Influence of photodynamic therapy on expression of vascular endothelial growth factor (VEGF), VEGF receptor 3, and pigment epithelium-derived factor. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4473–4480. [Google Scholar] [CrossRef]
- Husain, D.; Kramer, M.; Kenny, A.G.; Michaud, N.; Flotte, T.J.; Gragoudas, E.S.; Miller, J.W. Effects of photodynamic therapy using verteporfin on experimental choroidal neovascularization and normal retina and choroid up to 7 weeks after treatment. Investig. Ophthalmol. Vis. Sci. 1999, 40, 2322–2331. [Google Scholar]
- Al-Sheikh, M.; Phasukkijwatana, N.; Dolz-Marco, R.; Rahimi, M.; Iafe, N.A.; Freund, K.B.; Sadda, S.R.; Sarraf, D. Quantitative OCT angiography of the retinal microvasculature and the choriocapillaris in myopic eyes. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2063–2069. [Google Scholar] [CrossRef] [PubMed]
- Shinojima, A.; Kawamura, A.; Mori, R.; Fujita, K.; Yuzawa, M. Findings of optical coherence tomographic angiography at the choriocapillaris level in central serous chorioretinopathy. Ophthalmologica 2016, 236, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Alten, F.; Clemens, C.R.; Eter, N. OCT-Angiography strengthens the theory of a purely serous pigment epithelium detachment in age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1645–1647. [Google Scholar] [CrossRef] [PubMed]
- Iida, T.; Yannuzzi, L.A.; Spaide, R.F.; Borodoker, N.; Carvalho, C.A.; Negrao, S. Cystoid macular degeneration in chronic central serous chorioretinopathy. Retina 2003, 23, 137–138. [Google Scholar] [CrossRef]
- Imamura, Y.; Fujiwara, T.; Margolis, R.; Spaide, R.F. Enhanced depth imaging optical coherence tomography of the choroid in central serous chorioretinopathy. Retina 2009, 29, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Lai, T.Y.; Chan, W.M.; Li, H.; Lai, R.Y.; Liu, D.T.; Lam, D.S. Safety enhanced photodynamic therapy with half dose verteporfin for chronic central serous chorioretinopathy: A short term pilot study. Br. J. Ophthalmol. 2006, 90, 869–874. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value ± SD |
|---|---|
| Mean Age ± Standard Deviation (Years) | 51.8 ± 8.01 |
| Sex (Male/Female) | 18/1 |
| Mean duration of CSC ± Standard Deviation (Years) | 3.34 ± 1.40 |
| Patients with bilateral CSC (n) | 3 |
| Characteristic | Baseline | 1 h | p (Baseline vs. 1 h) | 1 w | p (Baseline vs. 1 w) | 1 m | p (Baseline vs. 1 m) |
|---|---|---|---|---|---|---|---|
| BCVA ± SD (LogMAR) | 0.34 ± 0.23 | N/A | N/A | 0.31 ± 0.20 | 0.287 | 0.26 ± 0.19 | 0.016 |
| CFT ± SD (μm) | 348.3 ± 144.42 | 332.7 ± 112.87 | 0.107 | 284.4 ± 67.08 | 0.01 | 249.75 ± 42.66 | 0.005 |
| CHT ± SD (μm) | 395.8 ± 89.61 | 397.1 ± 93.98 | 0.878 | 381.9 ± 93.88 | 0.134 | 364.55 ± 108.5 | 0.009 |
| CCVD ± SD (%) | 94.87 ± 2.32 | 94.8 ± 2.28 | 0.516 | 92.79 ± 3.16 | <0.001 | 95.55 ± 2.05 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassisi, M.; Lavia, C.; Alovisi, C.; Musso, L.; Eandi, C.M. Short-Term Choriocapillaris Changes in Patients with Central Serous Chorioretinopathy after Half-Dose Photodynamic Therapy. Int. J. Mol. Sci. 2017, 18, 2468. https://doi.org/10.3390/ijms18112468
Nassisi M, Lavia C, Alovisi C, Musso L, Eandi CM. Short-Term Choriocapillaris Changes in Patients with Central Serous Chorioretinopathy after Half-Dose Photodynamic Therapy. International Journal of Molecular Sciences. 2017; 18(11):2468. https://doi.org/10.3390/ijms18112468
Chicago/Turabian StyleNassisi, Marco, Carlo Lavia, Camilla Alovisi, Luca Musso, and Chiara M. Eandi. 2017. "Short-Term Choriocapillaris Changes in Patients with Central Serous Chorioretinopathy after Half-Dose Photodynamic Therapy" International Journal of Molecular Sciences 18, no. 11: 2468. https://doi.org/10.3390/ijms18112468