
A Retrospective Comparison of Hemodynamic and Clinical Outcomes between Two Differently Designed Aortic Bioprostheses for Small Aortic Annuli

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Surgical Technique
2.3. Echocardiographic Assessment
2.4. Data Collection and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Operative Results
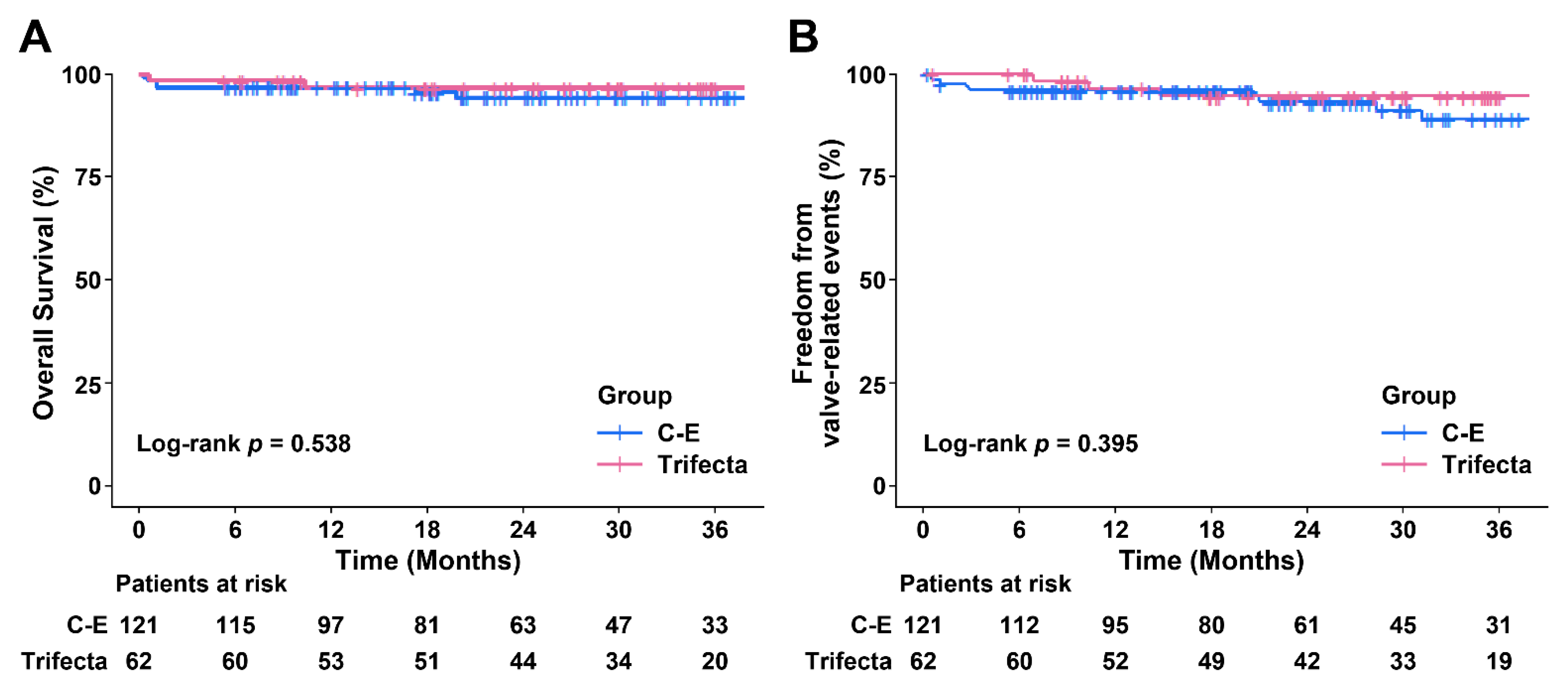
3.2. Early and Late Clinical Outcomes
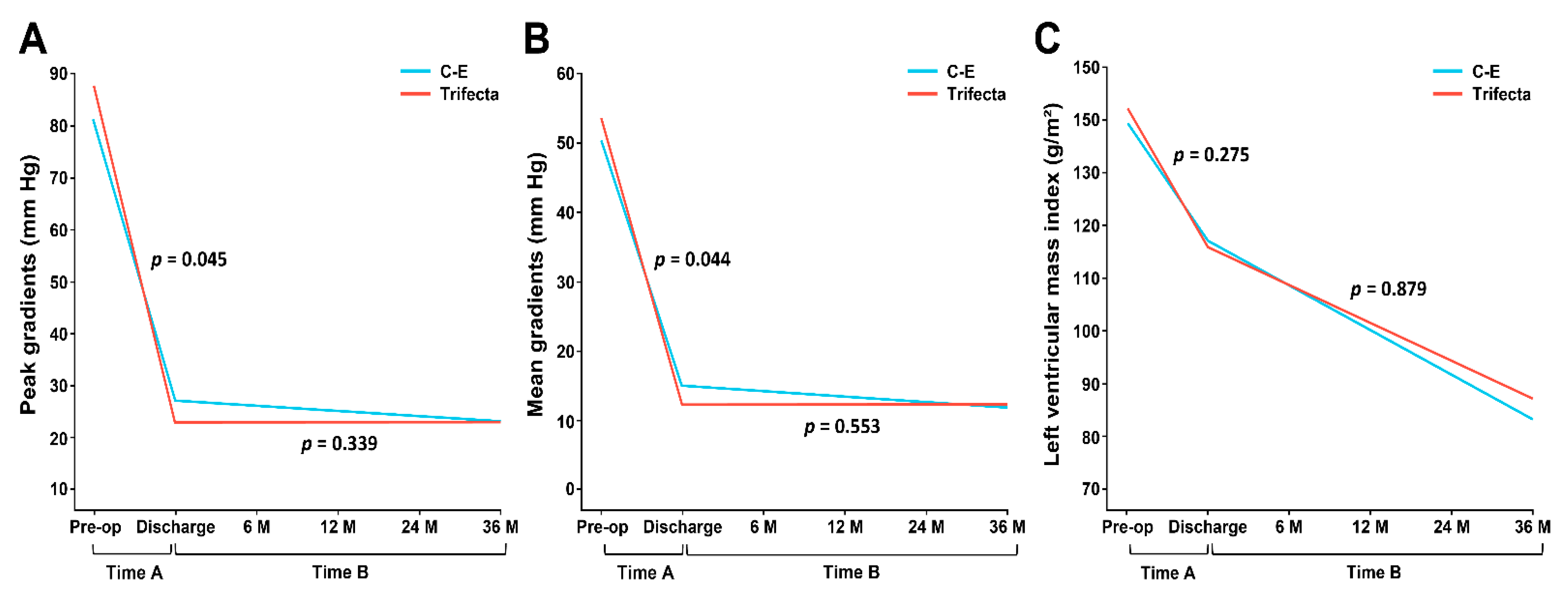
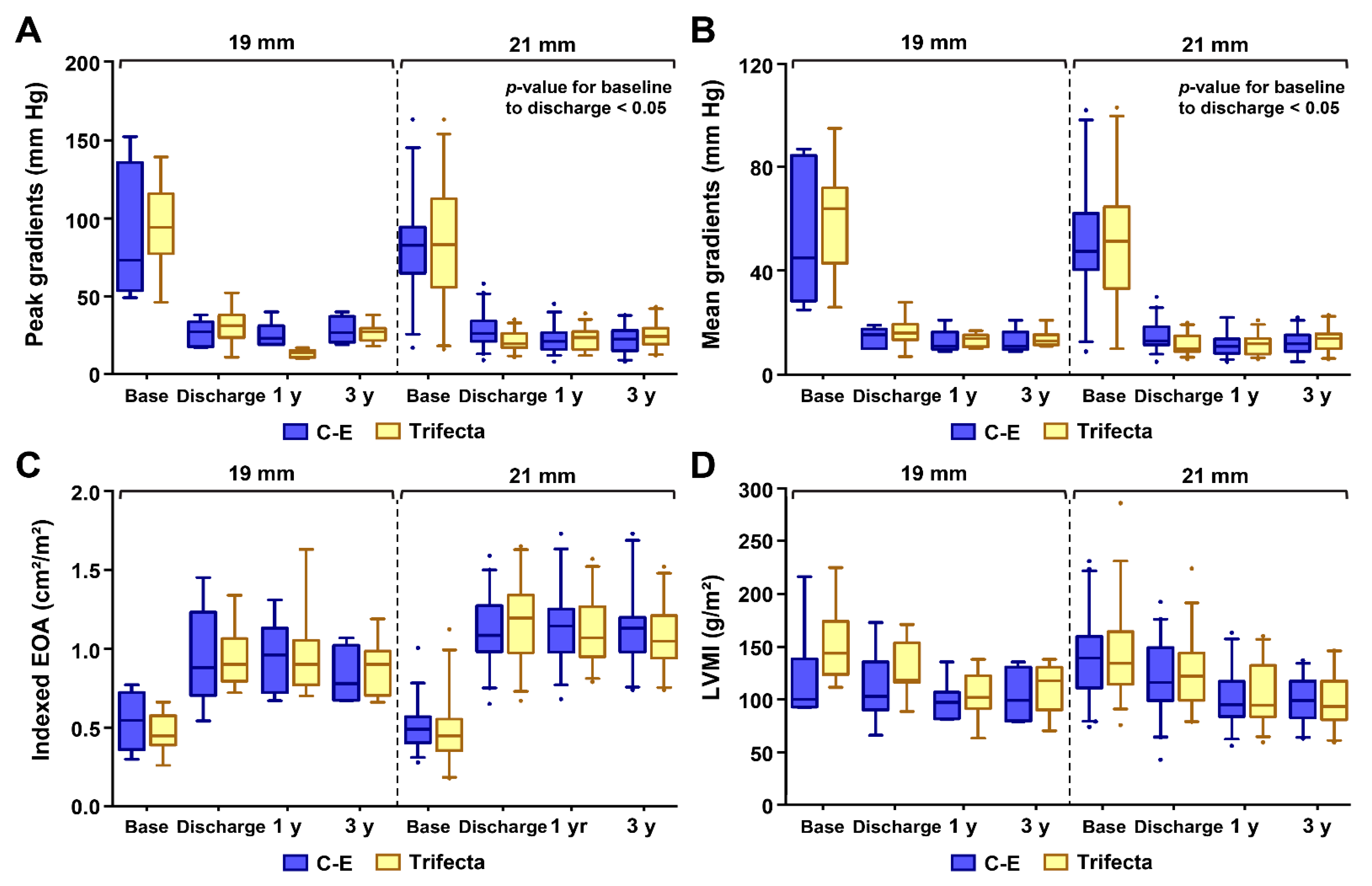
3.3. Hemodynamic Results for Matched Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahimtoola, S.H. Choice of prosthetic heart valve for adult patients. J. Am. Coll. Cardiol. 2003, 41, 893–904. [Google Scholar] [CrossRef] [Green Version]
- Domoto, S.; Niinami, H.; Uwabe, K.; Koike, H.; Tabata, M.; Morita, K.; Kambe, M.; Iguchi, A. Comparison of early haemodynamics of 19-mm aortic valve bioprostheses in patients with a small aortic annulus. Interact Cardiovasc. Thorac. Surg. 2016, 22, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Pibarot, P.; Weissman, N.J.; Stewart, W.J.; Hahn, R.T.; Lindman, B.R.; McAndrew, T.; Kodali, S.K.; Mack, M.J.; Thourani, V.H.; Miller, D.C.; et al. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: A PARTNER trial cohort—A analysis. J. Am. Coll. Cardiol. 2014, 64, 1323–1334. [Google Scholar] [CrossRef] [Green Version]
- Flameng, W.; Meuris, B.; Herijgers, P.; Herregods, M.C. Prosthesis-patient mismatch is not clinically relevant in aortic valve replacement using the Carpentier-Edwards Perimount valve. Ann. Thorac. Surg. 2006, 82, 530–536. [Google Scholar] [CrossRef]
- Bavaria, J.E.; Desai, N.D.; Cheung, A.; Petracek, M.R.; Groh, M.A.; Borger, M.A.; Schaff, H.V. The St Jude Medical Trifecta aortic pericardial valve: Results from a global, multicenter, prospective clinical study. J. Thorac. Cardiovasc. Surg. 2014, 147, 590–597. [Google Scholar] [CrossRef] [Green Version]
- Wendt, D.; Thielmann, M.; Plicht, B.; Assmann, J.; Price, V.; Neuhauser, M.; Jakob, H. The new St Jude Trifecta versus Carpentier-Edwards Perimount Magna and Magna Ease aortic bioprosthesis: Is there a hemodynamic superiority? J. Thorac. Cardiovasc. Surg. 2014, 147, 1553–1560. [Google Scholar] [CrossRef] [Green Version]
- Ugur, M.; Suri, R.M.; Daly, R.C.; Dearani, J.A.; Park, S.J.; Joyce, L.D.; Burkhart, H.M.; Greason, K.L.; Schaff, H.V. Comparison of early hemodynamic performance of 3 aortic valve bioprostheses. J. Thorac. Cardiovasc. Surg. 2014, 148, 1940–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Blais, C.; Dumesnil, J.G.; Baillot, R.; Simard, S.; Doyle, D.; Pibarot, P. Impact of valve prosthesis-patient mismatch on short-term mortality after aortic valve replacement. Circulation 2003, 108, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akins, C.W.; Miller, D.C.; Turina, M.I.; Kouchoukos, N.T.; Blackstone, E.H.; Grunkemeier, G.L.; Takkenberg, J.J.; David, T.E.; Butchart, E.G.; Adams, D.H.; et al. Guidelines for reporting mortality and morbidity after cardiac valve interventions. Ann. Thorac. Surg. 2008, 85, 1490–1495. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Gabella, T.; Voisine, P.; Puri, R.; Pibarot, P.; Rodes-Cabau, J. Aortic Bioprosthetic Valve Durability: Incidence, Mechanisms, Predictors, and Management of Surgical and Transcatheter Valve Degeneration. J. Am. Coll. Cardiol. 2017, 70, 1013–1028. [Google Scholar] [CrossRef]
- Colli, A.; Marchetto, G.; Salizzoni, S.; Rinaldi, M.; Di Marco, L.; Pacini, D.; Di Bartolomeo, R.; Nicolini, F.; Gherli, T.; Agrifoglio, M.; et al. The TRIBECA study: (TRI)fecta (B)ioprosthesis (E)valuation versus (C)arpentier Magna-Ease in (A)ortic position. Eur. J. Cardiothorac. Surg. 2016, 49, 478–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadokoro, N.; Fukushima, S.; Shimahara, Y.; Matsumoto, Y.; Yamashita, K.; Kawamoto, N.; Minami, K.; Kobayashi, J.; Fujita, T. Trifecta vs. Magna for Aortic Valve Replacement—Differences in Clinical Outcome and Valve Hemodynamics. Circ. J. 2018, 82, 2767–2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabata, M.; Shibayama, K.; Watanabe, H.; Sato, Y.; Fukui, T.; Takanashi, S. Simple interrupted suturing increases valve performance after aortic valve replacement with a small supra-annular bioprosthesis. J. Thorac. Cardiovasc. Surg. 2014, 147, 321–325. [Google Scholar] [CrossRef] [Green Version]
- Pibarot, P.; Dumesnil, J.G. Hemodynamic and clinical impact of prosthesis-patient mismatch in the aortic valve position and its prevention. J. Am. Coll. Cardiol. 2000, 36, 1131–1141. [Google Scholar] [CrossRef] [Green Version]
- Tasca, G.; Brunelli, F.; Cirillo, M.; Amaducci, A.; Mhagna, Z.; Troise, G.; Quaini, E. Mass regression in aortic stenosis after valve replacement with small size pericardial bioprosthesis. Ann. Thorac. Surg. 2003, 76, 1107–1113. [Google Scholar] [CrossRef]
- Beach, J.M.; Mihaljevic, T.; Rajeswaran, J.; Marwick, T.; Edwards, S.T.; Nowicki, E.R.; Thomas, J.; Svensson, L.G.; Griffin, B.; Gillinov, A.M.; et al. Ventricular hypertrophy and left atrial dilatation persist and are associated with reduced survival after valve replacement for aortic stenosis. J. Thorac. Cardiovasc. Surg. 2014, 147, 362–369.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Head, S.J.; Mokhles, M.M.; Osnabrugge, R.L.; Pibarot, P.; Mack, M.J.; Takkenberg, J.J.; Bogers, A.J.; Kappetein, A.P. The impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: A systematic review and meta-analysis of 34 observational studies comprising 27 186 patients with 133 141 patient-years. Eur. Heart J. 2012, 33, 1518–1529. [Google Scholar] [CrossRef] [Green Version]
- Rubens, F.D.; Gee, Y.Y.; Ngu, J.M.; Chen, L.; Burwash, I.G. Effect of aortic pericardial valve choice on outcomes and left ventricular mass regression in patients with left ventricular hypertrophy. J. Thorac. Cardiovasc. Surg. 2016, 152, 1291–1298.e2. [Google Scholar] [CrossRef] [Green Version]
- Une, D.; Mesana, L.; Chan, V.; Maklin, M.; Chan, R.; Masters, R.G.; Mesana, T.G.; Ruel, M. Clinical Impact of Changes in Left Ventricular Function After Aortic Valve Replacement: Analysis From 3112 Patients. Circulation 2015, 132, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Vollema, E.M.; Singh, G.K.; Prihadi, E.A.; Regeer, M.V.; Ewe, S.H.; Ng, A.C.T.; Mertens, B.J.A.; Klautz, R.J.M.; Ajmone Marsan, N.; Bax, J.J.; et al. Time course of left ventricular remodelling and mechanics after aortic valve surgery: Aortic stenosis vs. aortic regurgitation. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Ruel, M.; Al-Faleh, H.; Kulik, A.; Chan, K.L.; Mesana, T.G.; Burwash, I.G. Prosthesis-patient mismatch after aortic valve replacement predominantly affects patients with preexisting left ventricular dysfunction: Effect on survival, freedom from heart failure, and left ventricular mass regression. J. Thorac. Cardiovasc. Surg. 2006, 131, 1036–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiegl, K.; Deutsch, M.A.; Rondak, I.C.; Lange, R.; Guenzinger, R. Matched Comparison of Two Different Biological Prostheses for Complete Supra-annular Aortic Valve Replacement. Thorac. Cardiovasc. Surg. 2015, 63, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Johnston, D.R.; Soltesz, E.G.; Vakil, N.; Rajeswaran, J.; Roselli, E.E.; Sabik, J.F., 3rd; Smedira, N.G.; Svensson, L.G.; Lytle, B.W.; Blackstone, E.H. Long-term durability of bioprosthetic aortic valves: Implications from 12,569 implants. Ann. Thorac. Surg. 2015, 99, 1239–1247. [Google Scholar] [CrossRef] [Green Version]
- Flameng, W.; Herregods, M.C.; Vercalsteren, M.; Herijgers, P.; Bogaerts, K.; Meuris, B. Prosthesis-patient mismatch predicts structural valve degeneration in bioprosthetic heart valves. Circulation 2010, 121, 2123–2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, G.; Wu, Y.; Grunkemeier, G.L.; Furnary, A.P.; Starr, A. Durability of pericardial versus porcine aortic valves. J. Am. Coll. Cardiol. 2004, 44, 384–388. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, W.R.; Germann, E.; Aupart, M.R.; Neville, P.H.; Marchand, M.A.; Fradet, G.J. 15-year comparison of supra-annular porcine and PERIMOUNT aortic bioprostheses. Asian Cardiovasc. Thorac. Ann. 2006, 14, 200–205. [Google Scholar] [CrossRef]
- Forcillo, J.; Pellerin, M.; Perrault, L.P.; Cartier, R.; Bouchard, D.; Demers, P.; Carrier, M. Carpentier-Edwards pericardial valve in the aortic position: 25-years experience. Ann. Thorac. Surg. 2013, 96, 486–493. [Google Scholar] [CrossRef]
- Goldman, S.; Cheung, A.; Bavaria, J.E.; Petracek, M.R.; Groh, M.A.; Schaff, H.V. Midterm, multicenter clinical and hemodynamic results for the Trifecta aortic pericardial valve. J. Thorac. Cardiovasc. Surg. 2017, 153, 561–569.e2. [Google Scholar] [CrossRef] [Green Version]
- Kalra, A.; Rehman, H.; Ramchandani, M.; Barker, C.M.; Lawrie, G.M.; Reul, R.M.; Reardon, M.J.; Kleiman, N.S. Early Trifecta valve failure: Report of a cluster of cases from a tertiary care referral center. J. Thorac. Cardiovasc. Surg. 2017, 154, 1235–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneyuki, D.; Nakajima, H.; Asakura, T.; Yoshitake, A.; Tokunaga, C.; Tochii, M.; Hayashi, J.; Takazawa, A.; Izumida, H.; Iguchi, A. Early First-Generation Trifecta Valve Failure: A Case Series and a Review of the Literature. Ann. Thorac. Surg. 2020, 109, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubeda, H.; Aliter, H.; Gainer, R.A.; Theriault, C.; Doucette, S.; Hirsch, G.M. Six-year follow-up of aortic valve reoperation rates: Carpentier-Edwards Perimount versus St. Jude Medical Trifecta. J. Card. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables a | Unmatched | Matched | ||||
|---|---|---|---|---|---|---|
| C-E (n = 121) | Trifecta (n = 62) | SMD | C-E (n = 47) | Trifecta (n = 47) | SMD | |
| Patient Demographics | ||||||
| Age (years) | 73.3 ± 6.5 | 72.0 ± 7.9 | 0.180 | 73.5 ± 5.6 | 73.4 ± 4.3 | 0.021 |
| Female | 100 (82.6) | 47 (75.8) | 0.169 | 37 (78.7) | 38 (80.9) | 0.053 |
| Body surface area (m2) | 1.54 ± 0.14 | 1.56 ± 0.14 | 0.113 | 1.55 ± 0.12 | 1.55 ± 0.12 | 0.025 |
| Hypertension | 82 (67.8) | 38 (61.3) | 0.156 | 31 (66.0) | 33 (70.2) | 0.108 |
| Diabetes mellitus | 38 (31.4) | 15 (24.2) | 0.161 | 15 (31.9) | 13 (27.7) | 0.093 |
| Chronic renal failure | 19 (15.7) | 5 (8.1) | 0.238 | 2 (4.3) | 3 (6.4) | 0.095 |
| Cerebrovascular accidents | 25 (20.7) | 7 (11.3) | 0.258 | 5 (10.6) | 5 (10.6) | <0.001 |
| Chronic lung disease | 10 (8.3) | 5 (8.1) | 0.007 | 4 (8.5) | 3 (6.4) | 0.081 |
| Peripheral artery disease | 17 (14.0) | 4 (6.5) | 0.127 | 3 (6.4) | 3 (6.4) | <0.001 |
| Coronary artery disease | 34 (28.1) | 14 (22.6) | 0.393 | 10 (21.3) | 10 (21.3) | 0.121 |
| Previous PCI | 17 (14.0) | 2 (3.2) | 0.252 | 2 (4.3) | 1 (2.1) | <0.001 |
| Previous cardiac surgery | 14 (11.6) | 4 (6.5) | 0.179 | 1 (2.1) | 2 (4.3) | 0.121 |
| Atrial fibrillation/flutter | 40 (33.1) | 12 (19.4) | 0.315 | 10 (21.3) | 10 (21.3) | <0.001 |
| Logistic EuroSCORE (%) | 15.7 ± 16.5 | 12.8 ± 14.7 | 0.186 | 12.6 ± 12.2 | 12.4 ± 14.8 | 0.011 |
| EuroSCORE II (%) | 7.7 ± 12.1 | 4.9 ± 7.9 | 0.278 | 4.7 ± 5.3 | 4.8 ± 8.3 | 0.014 |
| NYHA III-IV | 63 (52.1) | 29 (46.8) | 0.106 | 21 (44.7) | 23 (48.9) | 0.094 |
| Valve pathology | ||||||
| Degenerative | 60 (49.6) | 33 (53.2) | 0.073 | 25 (53.2) | 27 (57.4) | 0.086 |
| Bicuspid | 13 (10.7) | 15 (24.2) | 0.360 | 11 (23.4) | 9 (19.1) | 0.104 |
| Rheumatic | 28 (23.1) | 7 (11.3) | 0.318 | 8 (17.0) | 6 (12.8) | 0.120 |
| Endocarditis | 10 (8.3) | 4 (6.5) | 0.069 | 2 (4.3) | 2 (4.3) | <0.001 |
| Prosthetic failure | 8 (6.6) | 2 (3.2) | 0.157 | 1 (2.1) | 2 (4.3) | 0.121 |
| Aortic stenosis | 78 (64.5) | 41 (66.1) | 0.035 | 32 (68.1) | 32 (68.1) | <0.001 |
| Aortic regurgitation | 16 (13.2) | 12 (19.4) | 0.167 | 7 (14.9) | 8 (17.0) | 0.058 |
| Mixed aortic lesion | 15 (12.4) | 7 (11.3) | 0.034 | 7 (14.9) | 5 (10.6) | 0.128 |
| Operative data | ||||||
| Valve size b | 0.292 | 0.529 | ||||
| 19 mm | 22 (18.2) | 17 (27.4) | 6 (12.8) | 13 (27.7) | ||
| 21 mm | 99 (81.8) | 45 (72.6) | 41 (87.2) | 34 (72.3) | ||
| Isolated AVR | 38 (31.4) | 32 (51.6) | 0.419 | 22 (46.8) | 25 (53.2) | 0.110 |
| Concomitant procedures | ||||||
| Coronary artery bypass | 13 (10.7) | 8 (12.9) | 0.067 | 7 (14.9) | 6 (12.8) | 0.062 |
| Mitral valve surgery | 54 (44.6) | 8 (12.9) | 0.748 | 9 (19.1) | 8 (17.0) | 0.055 |
| Tricuspid valve surgery | 37 (30.6) | 5 (8.1) | 0.595 | 6 (12.8) | 5 (10.6) | 0.066 |
| Aorta replacement | 8 (6.6) | 10 (16.1) | 0.303 | 7 (14.9) | 6 (12.8) | 0.062 |
| Surgical ablation | 16 (13.2) | 5 (8.1) | 0.168 | 4 (8.5) | 5 (10.6) | 0.072 |
| ACC time (min) b | 93.1 ± 40.4 | 79.0 ± 27.6 | 0.385 | 81.4 ± 37.3 | 80.5 ± 28.9 | 0.027 |
| CPB time (min) b | 120.2 ± 48.2 | 108.7 ± 36.8 | 0.257 | 103.8 ± 41.9 | 110.6 ± 38.0 | 0.170 |
| Variables a | Unmatched | Matched | ||||
|---|---|---|---|---|---|---|
| C-E (n = 121) | Trifecta (n = 62) | p-Value | C-E (n = 47) | Trifecta (n = 47) | p-Value | |
| Early results | ||||||
| Reoperation for bleeding | 8 (6.6) | 3 (4.8) | 0.752 | 1 (2.1) | 1 (2.1) | >0.999 |
| Renal failure | 5 (4.1) | 2 (3.2) | >0.999 | 1 (2.1) | 1 (2.1) | >0.999 |
| Prolonged ventilation | 9 (7.4) | 4 (6.5) | >0.999 | 2 (4.3) | 3 (6.4) | >0.999 |
| Cerebrovascular events | 4 (3.3) | 2 (3.2) | >0.999 | 1 (2.1) | 2 (4.3) | >0.999 |
| Atrial fibrillation | 20 (16.5) | 11 (17.7) | 0.836 | 9 (19.1) | 8 (17.0) | 0.789 |
| Operative mortality | 4 (3.3) | 1 (1.6) | 0.664 | 1 (2.1) | 1 (2.1) | >0.999 |
| Late results | ||||||
| Infective endocarditis | 0 (0) | 1 (1.6) | 0.339 | 0 (0) | 1 (2.1) | >0.999 |
| Pacemaker implantation | 3 (2.5) | 0 (0) | 0.552 | 1 (2.1) | 0 (0) | >0.999 |
| Paravalvular leakage | ||||||
| Mild | 3 (2.5) | 1 (1.6) | >0.999 | 1 (2.1) | 1 (2.1) | >0.999 |
| Moderate–severe | 0 (0) | 0 (0) | 0 (0) | 0 (0) | - | |
| Patient–prosthesis mismatch | ||||||
| Moderate | 22 (18.2) | 11 (17.7) | 0.942 | 6 (12.8) | 7 (14.9) | 0.765 |
| Severe | 5 (4.1) | 0 (0) | 0.169 | 0 (0) | 0 (0) | - |
| Variables a | Group | Baseline | Discharge | 1-Year | 3-Year | p-Value * | p-Value † |
|---|---|---|---|---|---|---|---|
| Peak gradient (mmHg) | C-E | 82.5 ± 32.8 | 27.9 ± 10.4 | 22.8 ± 8.3 | 22.8 ± 8.1 | 0.045 | 0.339 |
| Trifecta | 87.6 ± 34.2 | 24.0 ± 9.0 | 23.1 ± 6.7 | 25.5 ± 7.1 | |||
| Mean gradient (mmHg) | C-E | 50.9 ± 22.2 | 15.0 ± 5.3 | 11.9 ± 4.4 | 12.5 ± 4.5 | 0.044 | 0.553 |
| Trifecta | 53.9 ± 23.4 | 12.9 ± 4.8 | 12.2 ± 3.6 | 13.7 ± 3.9 | |||
| Aortic valve area (cm2) | C-E | 0.79 ± 0.24 | 1.71 ± 0.35 | 1.74 ± 0.35 | 1.66 ± 0.34 | 0.895 | 0.112 |
| Trifecta | 0.73 ± 0.26 | 1.70 ± 0.36 | 1.65 ± 0.30 | 1.56 ± 0.29 | |||
| Indexed EOA (cm2/m2) b | C-E | 0.51 ± 0.15 | 1.10 ± 0.24 | 1.12 ± 0.23 | 1.08 ± 0.24 | 0.995 | 0.097 |
| Trifecta | 0.47 ± 0.18 | 1.11 ± 0.25 | 1.07 ± 0.22 | 1.02 ± 0.21 | |||
| LVMI (g/m2) | C-E | 137.5 ± 40.1 | 119.0 ± 34.5 | 100.8 ± 24.5 | 98.9 ± 20.7 | 0.275 | 0.879 |
| Trifecta | 145.3 ± 39.0 | 126.5 ± 31.5 | 103.5 ± 26.5 | 101.6 ± 24.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.J.; Lee, S.; Joo, H.-C.; Youn, Y.-N.; Yoo, K.-J.; Lee, S.H. A Retrospective Comparison of Hemodynamic and Clinical Outcomes between Two Differently Designed Aortic Bioprostheses for Small Aortic Annuli. J. Clin. Med. 2021, 10, 1063. https://doi.org/10.3390/jcm10051063
Kim DJ, Lee S, Joo H-C, Youn Y-N, Yoo K-J, Lee SH. A Retrospective Comparison of Hemodynamic and Clinical Outcomes between Two Differently Designed Aortic Bioprostheses for Small Aortic Annuli. Journal of Clinical Medicine. 2021; 10(5):1063. https://doi.org/10.3390/jcm10051063
Chicago/Turabian StyleKim, Do Jung, Sak Lee, Hyun-Chel Joo, Young-Nam Youn, Kyung-Jong Yoo, and Seung Hyun Lee. 2021. "A Retrospective Comparison of Hemodynamic and Clinical Outcomes between Two Differently Designed Aortic Bioprostheses for Small Aortic Annuli" Journal of Clinical Medicine 10, no. 5: 1063. https://doi.org/10.3390/jcm10051063