
Screening for Gestational Diabetes Mellitus in Early Pregnancy: What Is the Evidence?


1
Department of Clinical and Experimental Endocrinology, KU Leuven, Herestraat 49, 3000 Leuven, Belgium
2
Department of Endocrinology, University Hospital Gasthuisberg, KU Leuven, Herestraat 49, 3000 Leuven, Belgium
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2021, 10(6), 1257; https://doi.org/10.3390/jcm10061257
Submission received: 21 January 2021
/
Revised: 12 March 2021
/
Accepted: 16 March 2021
/
Published: 18 March 2021
(This article belongs to the Special Issue Recent Advances in Gestational Diabetes Mellitus)
Abstract
:The incidence of gestational diabetes mellitus (GDM) is increasing worldwide. This has a significant effect on the health of the mother and offspring. There is no doubt that screening for GDM between 24 and 28 weeks is important to reduce the risk of adverse pregnancy outcomes. However, there is no consensus about diagnosis and treatment of GDM in early pregnancy. In this narrative review on the current evidence on screening for GDM in early pregnancy, we included 37 cohort studies and eight randomized controlled trials (RCTs). Observational studies have shown that a high proportion (15–70%) of women with GDM can be detected early in pregnancy depending on the setting, criteria used and screening strategy. Data from observational studies on the potential benefit of screening and treatment of GDM in early pregnancy show conflicting results. In addition, there is substantial heterogeneity in age and BMI across the different study populations. Smaller RCTs could not show benefit but several large RCTs are ongoing. RCTs are also necessary to determine the appropriate cut-off for HbA1c in pregnancy as there is limited evidence showing that an HbA1c ≥6.5% has a low sensitivity to detect overt diabetes in early pregnancy.
1. Introduction
Worldwide, the incidence of gestational diabetes mellitus (GDM) is increasing. This has a significant effect on the health of the mother and offspring. GDM is defined as diabetes diagnosed in the second or third trimester of pregnancy provided that overt diabetes early in pregnancy has been excluded [1]. There is no doubt that screening for GDM between 24 and 28 weeks is important to reduce the risk for adverse pregnancy outcomes such as large-for-gestational age infants (LGA) and preeclampsia [2,3]. There is a large variation in recommendations concerning screening for GDM in early pregnancy. The “American Diabetes Association” (ADA) recommends screening for overt diabetes at first prenatal visit, especially in women with risk factors. However, the ADA does not provide any specific recommendations concerning screening for GDM in early pregnancy [4]. “The International Association of the Diabetes and Pregnancy Study Groups” (IADPSG) initially recommended classification of GDM in early pregnancy when a fasting plasma glucose (FPG) ≥ 5.1 mmol/L occurs. However, the IADPSG criteria have not been validated for use in early pregnancy. Other associations such as the “International Federation of Gynecology and Obstetrics” (FIGO) recommend to screen universally in early pregnancy for diabetes and GDM [5]. In contrast, the “National Institute for Health and Care Excellence” recommends screening for early GDM if there are risk factors present, such as obesity, previous history of GDM, family history of diabetes (first-degree relative), previous macrocosmic baby or an ethnicity with a high prevalence of diabetes [6]. Early testing for overt diabetes will lead to the identification of hyperglycemia under the threshold of overt diabetes. These women could be labeled as early GDM based on IADPSG criteria, but there is a lack of evidence from randomized controlled trials (RCTs) on the potential benefits and harms of diagnosing and treating GDM in early pregnancy compared to treatment later in pregnancy. The ongoing controversy reflects in a lack of international consensus on screening for GDM in early pregnancy. The aim of this narrative review was therefore to evaluate the current evidence on screening and treatment for GDM in early pregnancy. In addition, we also reviewed pragmatic approaches to screening for glucose intolerance in pregnancy in a pandemic setting.
2. Materials and Methods
2.1. Data Sources and Search Strategies
Between November 2020 and December 2020, a literature search was conducted on PubMed. Cross-sectional studies, case–control studies, cohort studies, and RCTs were considered for this review. This is a narrative review. We did not perform a systematic review due to heterogeneity of studies and could therefore not perform a meta-analysis.
We used the following inclusion criteria:
- The study population were pregnant women with early-onset GDM.
- The control group could either be mothers with early GDM who were not treated or mothers with GDM diagnosed at 24–28 weeks of pregnancy (late-onset GDM).
- The following comparisons were made: women with early GDM were compared to women with GDM diagnosed at 24–28 weeks or women with early GDM who received treatment before 24 weeks were compared to women with early GDM who did not receive treatment before 24 weeks.
- The pregnancy outcomes studied were the development of GDM at 24–28 weeks, gestational weight gain, cesarean section, shoulder dystocia, preeclampsia, need for insulin treatment, LGA, neonatal intensive care unit (NICU) admission, neonatal hypoglycemia, preterm delivery and gestation age at delivery.
We excluded animal studies, descriptive designs (case series and case reports), studies with a low quality (no method section, no p-values mentioned), and articles written in a language other than English, French or Dutch. We did not limit our search to a specific population or ethnicity, or to a specific age category.
We used the following search strategies:
(“diabetes, gestational”(MeSH Terms) OR “Gestational diabetes”(Title/Abstract) OR “diabetes mellitus”(MeSH Terms) OR “diabetes mellitus” (Title/Abstract)) AND (“Blood Glucose” (MeSH Terms) OR “Blood Glucose” (Title/Abstract) OR “Insulin Resistance” (MeSH Terms) OR “hyperglycemia/blood” (MeSH Terms) OR “hyperglycemia” (Title/Abstract) OR “Glucose Intolerance” (MeSH Terms) OR “Glucose Tolerance Test” (MeSH Terms) OR “Glucose Tolerance Test” (Title/Abstract) OR “early screening” (Title/Abstract)) AND (“pregnancy trimester, first” (MeSH Terms) OR “First trimester pregnancy”(Title/Abstract))
In addition, we searched the reference lists of the selected articles and relevant reviews by hand. We also did a manual search for articles on screening for GDM during the COVID-19 Pandemic. We focused on articles that proposed a pragmatic approach on screening for diabetes and GDM in early pregnancy during the COVID-19 pandemic and compared the rate of missed cases of GDM between different screening tests and strategies.
2.2. Data Synthesis and Analysis
The extracted data included the study design, country, number of study participants, the diagnostic criteria used for GDM, adjustments that were made and pregnancy outcomes. We reported our results in a descriptive manner. A p-value <0.05 was considered significant.
3. Results
3.1. Search Results
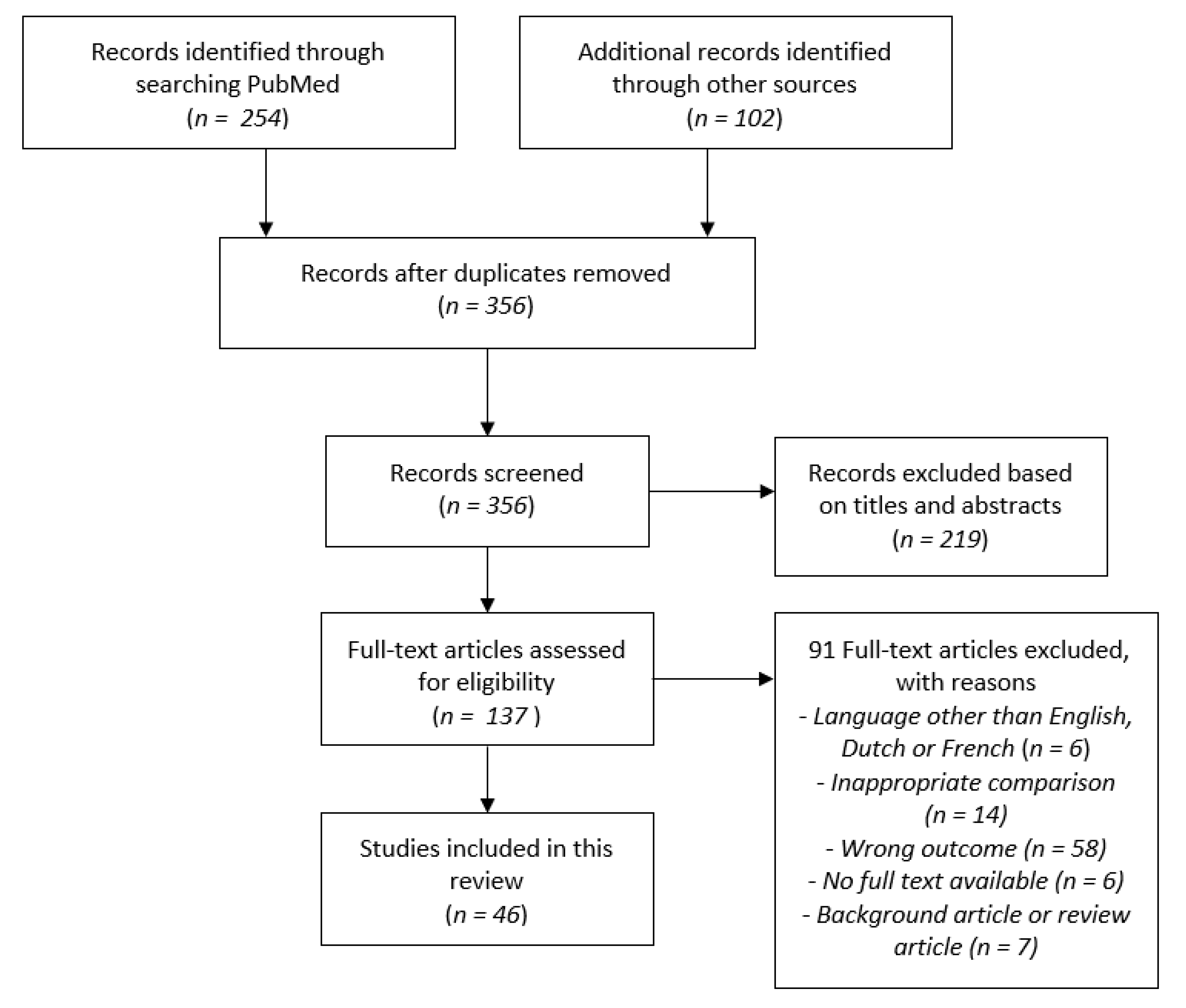
We identified 356 articles of which 137 articles were selected as possibly relevant. After examination of the full text, 46 studies were included in the current review (Figure 1).
3.2. Study Characteristics
The study characteristics are shown in Table 1, Table 2 and Table 3. In total, there were seven prospective cohort studies (15.6%), 29 retrospective cohort studies (63.0%), eight RCTs (17.8%), one post-hoc analysis (2.2%) and one population-based cohort study (2.2%). Six studies were performed in Asia (13.3%), 18 in Europe (39.1%), seven in America (15.6%), three in the Middle East (6.7%), four in Australia (8.9%), two in New Zealand (4.5%) and six multi-national studies (13.3%). All but one study was performed from 2000 onwards. Forty-one studies (89.9%) were performed from 2010 onwards. Twelve studies used the IADPSG criteria (26.7%). In total, 16 studies (34.9%) performed selective screening based on risk factors, while 30 studies (77.7%) used universal screening. Appendix A gives an overview of the diagnostic criteria used in the different studies.

{kind=link}
Table 1.
Observational studies.
| Author, Year/Country (Ref.) | Design | Subjects (N) | Study Population | Timeframe Testing (Weeks) | GDM Criteria | Comparison | Main Results |
|---|---|---|---|---|---|---|---|
| De Muylder, 1984/Belgium [7] | Prospective cohort study | 139 | Hi risk | <24 weeks | 3 h OGTT/O’Sullivan criteria | GDM diagnosis <24 weeks vs. GDM diagnosis 24–32 weeks vs. GDM diagnosis >32 weeks | Early GDM treated group had less complications such as preterm labor, preeclampsia and cesarean section |
| Bartha, 2000/Spain [8] | Prospective cohort study | 3986 | All pregnant women | First antenatal visit | 50 g GCT and 3 h 100 g OGTT | Early-onset (most during 1st trimester) vs. late-onset GDM | Early GDM diagnosis represented a high-risk subgroup |
| Barahona, 2005/Spain [9] | Retrospective study | 1708 offspring | Women with GDM | <24 weeks | 50 g GCT and 3 h OGTT/2nd and 3rd Workshop Conference Criteria on GDM | GDM diagnosis <24 weeks vs. 24–30 weeks vs. >31 weeks | Early GDM diagnosis was a predictor of adverse maternal and neonatal outcome |
| Hawkins, 2008/US [10] | Retrospective cohort study | 3334 | All pregnant women | <24 weeks (Hi risk) | 50 g GCT and 3 h 100 g OGTT/NDDG criteria | Diet-treated GDM <24 weeks (early diagnosis in hi risk population) vs. ≥24 weeks (routine diagnosis) | Twofold increased risk of preeclampsia in women with early diagnosis of diet treated GDM |
| Riskin, 2009/Israel [11] | Retrospective study | 6129 | Singleton pregnancies >24 weeks in mothers without ODIP or 1st FTFPG ≥5.8 mmol/L | <13 weeks | FTFPG/C&C criteria | FPG categories (<4.2 mmol/L, 4.2–4.4 mmol/L, 4.5–4.7 mmol/L, 4.8–5.0 mmol/L, 5.1–5.2 mmol/L, 5.3–5.5 mmol/L and 5.6–5.8 mmol/L) | Higher FTFPG in early pregnancy increased the risk of adverse pregnancy outcomes |
| Plasencia, 2011/Spain [12] | Retrospective study | 1716 | Singleton pregnancies | 6–14 weeks | 50 g GCT and 3 h 100 g OGTT/C&C criteria | GDM vs. non-GDM and GCT and OGTT results at 6–14 vs. 20–30 weeks | Effective diagnosis of GDM in the first trimester could be achieved by lowering the GCT and OGTT plasma glucose cut-offs |
| Corrado, 2012/Italy [13] | Retrospective study | 738 | Singleton pregnancies | <13 weeks | FTFPG/IADPSG criteria | FTFPG vs. 2 h 75 g OGTT early in the third trimester | FPG ≥5.1 mmol/L may be considered a highly predictive risk factor for GDM |
| Zhu W.W., 2013/China [14] | Retrospective cohort study | 14,039 | All pregnant women without ODIP | First antenatal visit (<24 weeks) | FPG/China GDM diagnosis criteria | 6 FPG groups (<4.1, 4.1–4.59, 4.60–5.09, 5.10–5.59, 5.6–6.09, 6.10–6.99 mmol/L) | Only 30.3% of women who had an FPG of ≥5.1 mmol/L still had an FPG of ≥5.1 mmol/L at 24–28 weeks |
| Alunni, 2015/US [15] | Retrospective cohort study | 2652 | Singleton pregnancies in women without ODIP | ≤24 weeks | HbA1c and FPG/HbA1c ≥5.7% or FPG ≥5.1 mmol/L at ≤24 weeks or C&C criteria | Early screening vs. standard two-step ACOG approach (1 h 50 g GCT followed by a 3 h 100 g OGTT/C&C Criteria) | Implementing early screening for GDM gave no significant difference in neonatal outcomes |
| Amylidi, 2015/ Switzerland [16] | Retrospective cohort study | 208 | Hi risk | <13 weeks | HbA1c/ADA and HAPO study guidelines | GDM vs. non-GDM (diagnosis based on one-step standardized 2 h 75 g OGTT between 24 and 28 weeks) and HbA1c ≥6% vs. <6% | Values HbA1c ≥6.0% in early pregnancy were predictive of GDM |
| Harreiter, 2016/ International [17] | Retrospective study | 1035 | Pregnant women with BMI ≥ 29.0 kg/m2 | Early pregnancy | 2 h 75 g OGTT/ WHO 2013 criteria | NGT vs. early GDM vs. DIP | Pre-pregnancy BMI was a significant predictor of early GDM and the only predictor among nulliparous women |
| Mañé, 2016/ Spain [18] | Prospective multi-ethnic cohort study | 1228 | Singleton pregnancies in women without ODIP | <13 weeks | HbA1c/≥5.9% | HbA1c ≥5.9% vs. HbA1c <5.9% | Early HbA1c ≥5.9% measurement identified women at high risk for poorer pregnancy outcomes |
| Osmundson, 2016/US [19] | Retrospective cohort study | 2812 | Singleton pregnancy >20 weeks | ≤136/7 weeks | HbA1c (prediabetes: 5.7–6.4%) | Prediabetic women (HbA1c of 5.7–6.4%) vs. women with a normal first trimester HbA1c (< 5.7%) | HbA1c early in pregnancy was a poor test to identify women who will develop GDM |
| Sweeting, 2016/Australia [20] | Retrospective cohort study | 4873 | Hi risk | <24 weeks | 2 h 75 g OGTT/ADIPS diagnostic criteria | T2DM vs. GDM <12 weeks vs. GDM 12–23 weeks vs. GDM ≥24 weeks | Early GDM in high-risk women remains associated with poorer pregnancy outcomes |
| Sweeting, 2017/Australia [21] | Retrospective cohort study | 3098 | Hi risk | <24 weeks | HbA1c measurement at time of GDM diagnosis | Early GDM (<24 weeks) vs. standard GDM (≥24 weeks) | HbA1c >5.9% early in pregnancy identified an increased risk of LGA, macrosomia, C-section, and hypertensive disorders in standard GDM |
| Hosseini, 2018/Iran [22] | Prospective population-based cohort study | 929 | Singleton pregnancies | 6–14 weeks | FPG/IADPSG | Normal pregnancy vs. early-onset GDM (6–14 weeks) vs. late-onset GDM (24–28 weeks) | Early-onset GDM was associated with poorer pregnancy outcomes |
| Ryan, 2018/UK [23] | Retrospective clinical audit of prospectively maintained database | 576 | Hi risk singleton pregnancies | 11–13 weeks | FPG/SIGN 2010 thresholds | Routine vs. early screening | Early screening improved the pregnancy outcomes, such as emergency cesarean section, neonatal hypoglycemia and macrosomia. |
| Salman, 2018/Israel [24] | Retrospective cohort study | 5030 | Singleton pregnancies of women without ODIP | <13 weeks | FTFPG cut-off 5.3 mmol/L | Women with FTFPG < 5.3 mmol/L and FTFPG ≥ 5.3 mmol/L | FTFPG ≥5.3 mmol/L was an independent risk factor for adverse perinatal outcome |
| Bianchi, 2019/Italy [25] | Retrospective study | 290 | Hi risk | 16–18 weeks | 2 h 75 g OGTT (and FPG)/IADPSG criteria | Early (16–18 weeks) vs. standard (24–28 weeks) screening | Similar short-term maternal-fetal outcomes in both groups |
| Del Val López, 2019/Spain [26] | Retrospective study | 1425 | All pregnant women without ODIP | <13 weeks | FTFPG/O’Sullivan criteria | FTFPG <5.1 and ≥5.1 mmol/L (FTFPG vs. classical 2-step OGTT) | FTFPG was not a good substitute for conventional diagnosis of GDM in the second trimester |
| Mañé, 2019/Spain [27] | Retrospective analysis of a prospective observational cohort study | 1228 | Women with singleton pregnancy without ODIP | <13 weeks | FPG and HbA1c/Criteria unknown | FPG vs. HbA1c cut-off values | FTFPG levels were not a better predictor of pregnancy complications than HbA1c |
| Benhalima, 2020/Belgium [28] | Multi-centric prospective cohort study | 2006 | All pregnant women | 6–14 weeks | FPG/IADPSG criteria | FPG ≥5.1–5.5 mmol/L in early pregnancy vs. FPG <5.1 mmol/L in early pregnancy | Group with increased FPG in early pregnancy had significantly more NICU admissions |
| Boriboonhirunsarn/Thailand, 2020 [29] | Retrospective cohort study | 1200 | All pregnant women | <24 weeks | 50 g GCT and 100 g OGTT/ADA and ACOG recommendation | No GDM vs. early-onset GDM vs. late-onset GDM | Significant lower gestational weight gain and higher rates of preeclampsia, LGA infants, and NICU admission despite treatment for early-onset GDM |
| Clarke, 2020/Australia [30] | Retrospective cohort study | 769 | Hi risk with singleton pregnancy and without ODIP | <24 weeks | 75 g 2 h OGTT/IADPSG criteria, as per the ADIPS guidelines | Early GDM (hi risk women diagnosed <24 weeks) vs. late GDM (women diagnosed ≥24 weeks) | Early pregnancy GDM was not associated with an adverse outcome |
| Cosson, 2020/France [31] | Retrospective study | 523 | Women with singleton pregnancy and without ODIP | <22 weeks | FPG/IADPSG criteria | Immediate care vs. no immediate care for early fasting hyperglycemia | Treating women with early fasting hyperglycemia, especially when FPG is ≥5.5 mmol/L, may improve pregnancy outcomes |
| Immanuel, 2020/International [32] | Post-hoc analysis of DALI study | 869 | Women with BMI ≥29 kg/m2 with singleton pregnancy and without ODIP | <20 weeks | HbA1c and 2 h 75 g OGTT/IADPSG criteria | HbA1c ≥5.7% vs. <5.7% group (prediabetes threshold) | Limited use of early pregnancy HbA1c for predicting GDM or adverse outcomes in overweight/obese European women |
| Jokelainen, 2020/Finland [33] | Population-based cohort study | 1401 | All singleton pregnancies without ODIP | 12–16 weeks | 2 h 75 g OGTT/FCCG | Early- vs. late-GDM vs. no GDM | Of the women who had early GDM based on the IADPSG/WHO criteria, 39.1% received the diagnosis of late GDM at the second OGTT |
| Liu, 2020/China [34] | Prospective cohort study | 522 | Singleton pregnancies | 18–20 weeks | 2 h 75 g OGTT/IADPSG-2015 guidelines | 4 groups: NGT (no GDM diagnosis), EGDM (GDM diagnosis in only early OGTT), LGDM (GDM diagnosis in only standard OGTT) and GDM (GDM diagnosis in both OGTTs) | Early GDM diagnosis at 18–20 weeks is associated with adverse outcomes |
| Nakanishi, 2020/Japan [35] | Multicenter prospective cohort study | 146 | Hi risk without ODIP | <20 weeks | 2 h 75 g OGTT/IADPSG criteria 2010 | False-positive early GDM (early+/late-) vs. true GDM (early+/late+) (late = standard) | Of the 146 women diagnosed with early-onset GDM, 69 (47%) had normal 75 g OGTT values at 24–28 weeks of gestation. |
| Sesmilo, 2020/Spain [36] | Retrospective cohort study | 6845 | Singleton pregnancies in women without ODIP and available data | <13 weeks | FPG/NDDG criteria | FPG: ≤4.3, 4.4–4.6, 4.7–4.8 and ≥4.9 mmol/L | FTFPG is an early marker of GDM and LGA. |
GDM: gestational diabetes mellitus; OGTT: oral glucose tolerance test; hi risk: high risk; GCT: glucose challenge test; NDDG: National Diabetes Data Group; ODIP: overt diabetes in pregnancy; FTFPG: first trimester fasting plasma glucose; HAPO: Hyperglycemia and Adverse Pregnancy Outcomes; C&C: Carpenter and Coustan; IADPSG: International Association of the Diabetes and Pregnancy Study Groups; FPG: fasting plasma glucose; HbA1c: hemoglobin A1C; ACOG: American Congress of Obstetricians and Gynecologists; ADA: American Diabetes Association; BMI: body mass index; WHO: World Health Organization; NGT: normal glucose tolerance; DIP: diabetes in pregnancy; ADIPS: Australian diabetes in pregnancy society; LGA: large-for-gestational age; C-section: cesarian section; SIGN: Scottish Intercollegiate Guidelines Network; NICU: neonatal intensive care unit; T2DM: type 2 diabetes mellitus; FCCG: Finnish Current Care Guideline; EGDM: early-onset gestational diabetes; LGDM: late-onset gestational diabetes; DALI: Diabetes and Pregnancy Vitamin D And Lifestyle Intervention for Gestational Diabetes Mellitus Prevention.
Table 2.
Randomized controlled trials.
| Author, Year/Country (Ref.) | Subjects (N) | Study Population | Timeframe Testing (Weeks) | GDM Criteria | Comparison | Main Results |
|---|---|---|---|---|---|---|
| Osmundson, 2016/US [37] | 83 | Women with singleton pregnancy and without ODIP | <14.0 weeks | HbA1c/between 5.7 and 6.4% | Usual care vs. early treatment for GDM with diet, BG monitoring, and insulin as needed | Early treatment did not significantly reduce the risk of GDM except in non-obese women |
| Hughes, 2018 (PINTO feasibility study)/New Zealand [38] | 47 | Women with singleton pregnancy and without ODIP | <14.0 weeks | HbA1c/between ≥5.9 and 6.4%/2 h 75 h OGTT New Zealand criteria | Standard care vs. early intervention in pregnancies complicated by prediabetes | First results expected in 2021 |
| Simmons, 2018 (ToBOGM pilot study)/Australia [39] | 79 | Hi risk women with singleton pregnancy | <20.0 weeks (4–19.6 weeks) | 2 h 75 g OGTT/IADPSG criteria | Women with booking GDM receiving immediate (clinical referral or ongoing treatment) vs. deferred (no) treatment vs. women without booking GDM (“decoys”) | More NICU admission in the early GDM group with a tendency for more SGA but less LGA |
| Simmons, 2018 (ToBOGM study protocol)/International [40] | 4000 | Hi risk women with singleton pregnancy | <20.0 weeks (4–19.6 weeks) | 2 h 75 g OGTT/2014 Australasian Diabetes-in-Pregnancy Society criteria for pregnant women with GA 24–28 weeks | Intervention (immediate treatment) vs. control (no treatment) vs. decoys (NGT but undergo all procedures) vs. non-active (NGT and records reviewed postnatally) | First results expected mid-2021 |
| Vinter, 2018 (LiP study)/Denmark [41] | 90 | Obese pregnant women (BMI 30–45 kg/m2) with singleton pregnancy | 12–15 weeks | 2 h 75 g OGTT/IADPSG Criteria | Lifestyle intervention vs. SoC | Lifestyle intervention was not effective in improving obstetric or metabolic outcomes |
| Roeder, 2019 (RCT)/US [42] | 157 | Women with hyperglycemia and singleton pregnancy without ODIP | ≤15.0 weeks | HbA1c and/or FPG, respectively, 5.7–6.4% and/or 5.1–6.9 mmol/L | Early pregnancy vs. 3rd trimester treatment of hyperglycemia | Treatment in early pregnancy did not improve maternal or neonatal outcomes significantly |
| Harper, 2020 (EGGO study)/US [43] | 922 | Obese women (BMI ≥30 kg/m2) without ODIP and history of bariatric surgery | 14–20 weeks | 2-step method: 1 h 50 g GCT followed by a 3 h 100 g OGTT/C&C criteria | Early GDM screening (14–20 weeks) vs. routine screening (24–28 weeks) | Early GDM screening in obese women did not reduce the composite perinatal outcomes, such as macrosomia, C-section and shoulder dystocia |
| Hung-Yuan Li (TESGO study)/Taiwan (NCT03523143) | 2068 | Singleton pregnancy without ODIP | 18–20 weeks | 75 g 2 h OGTT/IADPSG criteria | Early screening group (18–20 weeks) vs. standard screening group (24–28 weeks) | Results expected beginning of 2021 |
ODIP: overt diabetes in pregnancy; HbA1c: hemoglobin A1c; GDM: gestational diabetes mellitus; BG: blood glucose; PINTO: Pre diabetes in pregnancy, can early intervention improve outcomes; OGTT: oral glucose tolerance test; Hi risk: high risk; ToBOGM: Treatment of Booking Gestational diabetes Mellitus; IADPSG: International Association of the Diabetes and Pregnancy Study Groups; NICU: neonatal intensive care unit; SGA: small-for-gestational age; LGA: large-for-gestational age; GA: gestational age; NGT: normal glucose tolerance; LIP: Lifestyle in Pregnancy; BMI: body mass index; SoC: standard of care; FPG: fasting plasma glucose; GCT: glucose challenge test; C&C: Carpenter and Coustan; C-section: cesarean section; EGGO: Early Gestational Diabetes Screening in the Gravid Obese Woman; TESGO: The Effect of Early Screening and Intervention for Gestational Diabetes Mellitus on Pregnancy Outcomes.
3.3. Screening for Overt Diabetes in Early Pregnancy
The prevalence of type 2 diabetes (T2DM) in women of childbearing age is increasing. Since T2DM is often asymptomatic at the beginning and women with severe hyperglycemia early in pregnancy are at high risk for adverse pregnancy outcomes, timely detection and treatment of diabetes is needed. Most international associations such as the IADPSG, the ADA and the World Health Organization (WHO) recommend therefore to screen for overt diabetes at the first antenatal visit using an FPG, HbA1c or 75 g oral glucose tolerance test (OGTT) with the same cut-offs as for non-pregnant populations. The measurements of FPG and HbA1c should ideally be repeated twice to confirm the diagnosis of overt diabetes. HbA1c can be used to screen for diabetes but not to screen for GDM due to the very low sensitivity [44]. Measurement of fasting glycemia has a higher sensitivity than HbA1c to screen for diabetes. On the other hand, HbA1c has the advantage that it can be performed in the non-fasting state. An observational study from New Zealand [45] showed that an HbA1c ≥5.9% identified all women with diabetes who completed an OGTT before 20 weeks of pregnancy and this also identified a group at significantly increased risk for adverse pregnancy outcomes, such as preeclampsia and shoulder dystocia. In addition, the study demonstrated that an HbA1c ≥6.5% would have missed almost half of these women. These data suggest therefore that the currently recommended HbA1c is too high for screening purposes in pregnancy. However, large RCTs are required to confirm these results.
3.4. Screening for GDM in Early Pregnancy
As shown in Table 1, numerous observational studies were performed over the years. These studies show conflicting results. In general, most studies show that women with early GDM are at high risk for adverse pregnancy outcomes but treatment of GDM early in pregnancy compared to later in pregnancy does not always translate into improved outcomes. Seven studies reported an improved pregnancy outcome by treatment of early-onset GDM [7,9,10,29,30,31,34]. Barahona et al. [9] showed that diagnosing GDM early in pregnancy is a predictor of adverse maternal and neonatal outcomes, such as pregnancy-induced hypertension, insulin treatment during pregnancy, preterm birth, hyperbilirubinemia and perinatal mortality. More recently, Cosson et al. [31] reported that women who received initial care vs. those who did not, were more likely to be insulin-treated during pregnancy (58.0% vs. 20.9%, respectively; p < 0.00001), gained less gestational weight (8.6 ± 5.4 kg vs. 10.8 ± 6.1 kg, respectively; p < 0.00001), had a lower rate of preeclampsia (1.2% vs. 2.6%, respectively; adjusted odds ratio (aOR): 0.247 (0.082–0.759), p = 0.01), and similar rates of LGA infants and shoulder dystocia. A very recent study from Thailand showed that early GDM women had a high risk for adverse pregnancy outcomes with higher rates of preeclampsia, LGA infants, and NICU admission [29].
However, five studies described no beneficial effect of early diagnosing or treatment of GDM on maternal or neonatal outcomes [15,20,22,25,30]. Both Alluni et al. [15] and Bianchi et al. [25] showed that patients diagnosed and treated for early-onset GDM were more prone to be insulin-treated during pregnancy but showed no differences in neonatal outcomes such as small-for-gestational age (SGA) infants, cesarean sections, macrosomia, and LGA. An Australian study demonstrated also that early diagnosis and intervention had no effect on pregnancy outcomes [21]. This was confirmed by a recent Australian study showing no differences in pregnancy outcomes between early-onset GDM and late-onset GDM [30].
RCTs are needed to determine whether treating early-onset GDM improves pregnancy outcomes compared to standard treatment of GDM at 24–28 weeks of pregnancy. Table 2 gives an overview of the (ongoing) RCTs. The largest RCTs such as the “Prediabetes in pregnancy, can early intervention improve outcomes” PINTO study, the “Treatment of Booking Gestational diabetes Mellitus” (ToBOGM) study and the “Effect of Early Screening and Intervention for Gestational Diabetes Mellitus on Pregnancy Outcomes” (TESGO) study are still ongoing. Results are expected at the earliest in 2021. The ToBOGM study, the “Early Gestational Diabetes Screening in the Gravid Obese Woman” (EGGO) study and “Lifestyle in Pregnancy” (LiP) study focused on high-risk populations and obese women. In contrast, the TESGO and PINTO studies included also lower risk women.
A small RCT showed that early treatment of mild hyperglycemia (women with an HbA1c of 5.7–6.4%) did not reduce the risk of GDM, except for non-obese women [37]. The pilot study of ToBOGM [39] demonstrated that early treatment may have both benefits and harms for mother and offspring. NICU admission was highest in the treated early GDM group (36% vs. 0% p = 0.043), driven by a higher rate of SGA infants. Women who received no treatment for early-onset GDM had more LGA infants (0% vs. 33% p = 0.030). The LiP study [41] focused on the effect of lifestyle intervention vs. standard care for obese women with early GDM. They found that lifestyle intervention in early pregnancy did not improve obstetric or metabolic outcomes. In addition, the EGGO study [43] showed no effect on the composite perinatal outcomes in obese women who had early screening for GDM. Similarly, Roeder et al. [42] did not find any improvement in maternal and neonatal outcomes after treatment in early pregnancy.
3.5. Criteria to Define GDM in Early Pregnancy
Of all observational studies (Table 1), 15 studies discussed the diagnostic criteria for GDM early in pregnancy [11,12,13,14,16,18,21,24,26,27,28,31,32,35,36]. Riskin et al. showed that first trimester fasting glucose levels (FTFPG) in the non-diabetic range resulted in a higher risk for adverse pregnancy outcomes, such as more cesarian sections, LGA and macrosomia. These findings were confirmed by a recent Belgium study [28] demonstrating more NICU admissions in the high FTFPG group (FPG ≥ 5.1–5.5 mmol/L). A large Chinese study showed that an FTFPG of 6.1–7.0 mmol/L in early pregnancy is a strong predictor for GDM later in pregnancy [14]. In contrast, an FTFPG ≥ 5.1 mmol/L (GDM according to IADPSG criteria) was not a good predictor for GDM in their population. Several other studies (including studies in European populations) confirmed that ≥ 5.1 mmol/L is a poor predictor for GDM early in pregnancy [26,28]. A Belgium study [28] for instance demonstrated that only 37% of all women with an FTFPG ≥ 5.1–5.5 mmol/L, developed GDM based on the OGTT later in pregnancy. A French study proposed to use an FTFPG ≥ 5.5 mmol/L to start treatment for GDM in early pregnancy, as they demonstrated improved pregnancy outcomes in their population [31].
Few studies evaluated HbA1c in early pregnancy to diagnose GDM. These studies showed that an HbA1c ≥ 5.9% identifies women at high risk for adverse pregnancy outcomes independently of GDM diagnosis later in pregnancy [21,27].
A small RCT showed that early treatment of women with a first trimester HbA1c of 5.7–6.4% did not significantly reduce the risk of GDM, except in non-obese women [37]. Roeder et al. [42] used HbA1c ≥ 5.7% and/or an FTFPG ≥ 5.1 mmol/L to identify women with hyperglycemia early in pregnancy. Treatment in early pregnancy did not improve maternal or neonatal outcomes. Only 19% of this cohort developed GDM later in pregnancy [42]. In contrast, the ToBOGM pilot trial reported that 89% of untreated women (with an FPG ≥ 5.1 mmol/L early in pregnancy) had GDM at 24–28 weeks [39].
3.6. Screening for Diabetes and GDM in Early Pregnancy in COVID Times
Due to the COVID-19 pandemic, screening for GDM using OGTT’s might lead to an increased risk for exposure to the virus. Six large observational studies describe how screening for GDM could be organized in a pragmatic way using blood tests, and risk calculators applied to underlying risk factors (Table 3).
Table 3.
Screening for diabetes and GDM (early) in pregnancy in COVID times.
| Article | Pragmatic Approach | Main Results |
|---|---|---|
| Thangaratinam, 2020 [49] | Test strategy:
HbA1c ≥ 5.7% or FPG ≥ 5.6 mmol/L or RPG ≥ 9 mmol/L: treat as GDM. | Using FPG alone will only pick up about half of all women with GDM, based on NICE or IADPSG criteria. Combining FPG with HbA1c may improve the detection rate. Maintaining existing FPG thresholds may be preferable, and services may consider lower thresholds consistent with the IADPSG diagnostic criteria (FPG ≥ 5.1), if resources allow. |
| Torlone, 2020 [50] | Screening for overt diabetes:
Screening for GDM: risk factors assessment
| A fasting glucose value can be considered diagnostic for GDM only when it is obtained at the gestational age when the OGTT should have been carried out, i.e., between 16 and 18 weeks in high-risk pregnant women or between 24 and 28 weeks in medium-risk women. |
| McIntyre, 2020 (Diagnosis and management GDM during COVID-19) [47] | Early in pregnancy: all guidelines: HbA1c ≥ 5.9% Standard screening (24–28 weeks): UK: at risk; GDM if HbA1c ≥ 5.7% and/or FVPG ≥ 5.6 mmol/L and/or Random VPG (not preferred) ≥ 9.0 mmol/L CAN: GDM if HbA1c ≥ 5.7% and/or Random VPG ≥ 11.1 mmol/L AUS: fasting VPG: Fasting VPG < 4.7 mmol/L = normal Fasting VPG 4.7–5.0 mmol/L = OGTT, WHO 2013 criteria Fasting VPG ≥ 5.1 mmol/L = GDM | Detecting only those with marked hyperglycemia |
| McIntyre, 2020 (Testing for GDM during COVID-19) [46] | UK: Risk factor based; no OGTT; GDM if HbA1c ≥ 5.7% and/or FVPG ≥ 5.6 mmol/L and/or Random VPG (not preferred) ≥ 9.0 mmol/L CAN: universal testing; no OGTT; GDM if HbA1c ≥ 5.7% and/or Random VPG ≥ 11.1 mmol/L AUS: fasting VPG: Fasting VPG < 4.7 mmol/L = normal Fasting VPG 4.7–5.0 mmol/L = OGTT, WHO 2013 criteria Fasting VPG ≥ 5.1 mmol/L = GDM | All post COVID-19 modified pathways reduced GDM frequency. Missed GDM’s in Canadian women gave similar rates of pregnancy outcomes. Using UK modifications, missed GDM group was at slightly lower risk. Using the Australian modifications, missed GDM group was at substantially lower risk. |
| Meek, 2020 [48] | To evaluate the diagnostic and prognostic performance of alternative diagnostic strategies to 2 h 75 g OGTTs: HbA1c, RPG and FPG GDM diagnosis: criteria of the UK National Institute for Health and Care Excellence and IADPSG criteria | RPG at 12 weeks, and FPG or HbA1c at 28 weeks identify women with hyperglycemia at risk of suboptimal pregnancy outcomes. |
| Seshiah, 2020 [51] | The “single test procedure” for diagnosing GDM: 2 h PG ≥ 7.8 mmol/L with 75 g oral glucose administered to a pregnant woman in the fasting or non-fasting state, without regard to the time of the last meal (glucose load can also be taken at home and the pregnant woman can visit the hospital 2 h after the glucose ingestion to give a single sample for plasma glucose estimation) | The economical and evidence based “single test procedure” of DIPSI is most appropriate for screening during the COVID pandemic as performing OGTTs is resource intensive, the fasting state is impractical with very high dropout rate. |
GDM: gestational diabetes mellitus; HbA1c: hemoglobin A1c; RPG: random plasma glucose; OGTT: oral glucose tolerance test; FPG: fasting plasma glucose; NICE: National Institute for Health and Care Excellence; IADPSG: International Association of the Diabetes and Pregnancy Study Groups; VPG: venous plasma glucose; UK: United Kingdom; CAN: Canada; AUS: Australia; WHO: World Health Organization; PG: plasma glucose; DIPSI: Diabetes in Pregnancy Study Group India.
McIntyre et al. [46,47] described the diagnosis and management of GDM during COVID-19 in Australia, Canada and the United Kingdom (UK). For early screening, the guidelines were similar in the different countries, with an HbA1c ≥ 5.9% considered as hyperglycemia. For diagnosing GDM at 24–28 weeks, each country had a slightly different approach. The UK invited only women at high risk. GDM was diagnosed if HbA1c ≥ 5.7% and/or fasting venous plasma glucose (FVPG) ≥ 5.6 mmol/L and/or random venous plasma glucose (VPG) (not preferred) ≥ 9.0 mmol/L. Canada recommended universal screening. GDM was diagnosed if HbA1c ≥ 5.7% and/or random VPG ≥ 11.1 mmol/L. Australia used universal testing with an initial FVPG. If FVPG was between 4.7 and 5.0 mmol/L, an OGTT was performed. If FVPG ≥ 5.1 mmol/L, then GDM was diagnosed immediately.
Meek et al. [48] reported that random plasma glucose (RPG) at 12 weeks, and FPG or HbA1c at 28 weeks identifies women with hyperglycemia at risk of suboptimal pregnancy outcomes. When an OGTT is not possible, as an alternative RPG, FPG and HbA1c are recommended. Thangaratinam et al. [49] suggested additional tests at booking to detect overt diabetes and identify those at highest risk for GDM. HbA1c ≥ 6.5% or RPG ≥ 11.1 mmol/L is considered as pre-existing diabetes. As the recommended antenatal routine booking blood tests are often not performed in the fasting state, a pragmatic approach was suggested with the use of RPG. GDM can be diagnosed by HbA1c 5.9–6.4% or RPG 9–11 mmol/L to diagnose diabetes. The following thresholds for diagnosing GDM were suggested: HbA1c ≥ 5.7%, FPG ≥ 5.6 mmol/L or RPG ≥ 9 mmol/L.
To conclude, Italian recommendations [50] propose that if an OGTT cannot be safely performed, screening for GDM should be based on risk factors and the FPG value. Women with high risk factors should be tested at 16–18 weeks and an FPG ≥5.1 mmol/L is diagnosed as GDM. Women with high risk factors and an FPG ≤5.1 mmol/L or women with medium risk factors should be tested at 24–28 weeks. If FPG ≥5.1 mmol/L at 24–28 weeks, the woman will be diagnosed with GDM.
4. Discussion
4.1. Summary of Findings
In this narrative review, we demonstrate that there is need for clear guidelines and criteria concerning overt diabetes and early screening for GDM. The HbA1c threshold of diabetes as currently recommended is probably too high to detect all women with overt diabetes in early pregnancy. Furthermore, observational studies show conflicting results on the effects of screening and treatment of GDM in early pregnancy. It is also not clear which diagnostic criteria should be used to define GDM in early pregnancy. Evidence from large RCTs is needed to evaluate whether treatment has a beneficial effect on maternal and neonatal outcomes, without increased risk for harm (such as increased risk for SGA infants). Large RCTs such as the TOBOGM study will also help to inform which diagnostic criteria are appropriate to use for GDM in early pregnancy.
The COVID-19 pandemic has brought us additional challenges. OGTT’s could often not be performed as they involve high exposure risks and health service burden. Different guidelines have proposed pragmatic approached to screening with HbA1c, FPG or even RPG as an alternative during the pandemic.
4.2. Results in Relation to What We Already Know
Screening for overt diabetes in early pregnancy is necessary. At the moment, the threshold for diagnosing overt diabetes is an HbA1c ≥6.5%. However, there is limited data suggesting that in pregnancy the cut-off of HbA1c should be lowered to ≥5.9% to identify all women with diabetes as this identifies a population at high risk for adverse pregnancy outcomes. A threshold of ≥6.5% would have missed half of these women [45].
Screening and treatment of GDM between 24 and 28 weeks of pregnancy is widely accepted. This is beneficial to reduce adverse pregnancy outcomes. More women are identified with mild hyperglycemia in early pregnancy due to increased screening for overt diabetes. Observational studies show conflicting results as to whether screening and treatment of GDM in early pregnancy is beneficial compared to screening later in pregnancy. Some studies have shown that despite treatment, early-onset GDM women have more adverse pregnancy complications than late-onset GDM women, while other studies demonstrated similar short-term obstetrical outcomes in both groups and improved outcomes in the early screening group. At this moment, we can only speculate whether the fact that early treatment of GDM often only leads to similar pregnancy outcomes might represent success rather than failure. We cannot exclude that treatment of this group later in pregnancy might lead to more adverse pregnancy outcomes. In addition, studies had substantial heterogeneity in maternal age in pregnancy and BMI. In developed countries, increasing maternal age in pregnancy disposes to higher insulin resistance, whereas most pregnant women are younger in developing countries. Data are needed from well-designed RCTs. In the meantime, treatment of mild hyperglycemia in early pregnancy remains controversial due to lack of evidence from large RCTs supporting any benefit of treatment of GDM before 24 weeks of pregnancy. Moreover, a diagnosis of GDM could also be associated with increased medicalization of pregnancy (with more inductions and cesarean sections) and an increased risk for SGA infants due to overtreatment. Furthermore, it remains unclear which diagnostic criteria should be used to define GDM in early pregnancy, and whether universal or selective screening should be used to detect GDM before 24 weeks. Many studies evaluated high risk populations and there was also a high heterogeneity in the risk factors used across the different studies to screen for GDM in early pregnancy. Several studies have shown that FPG in early pregnancy is a poor predictor for GDM later in pregnancy. The IADPSG criteria might therefore not be appropriate to use in early pregnancy.
4.3. Practical Implications
As for maternal and neonatal outcomes, smaller RCTs did not show benefits of early screening and treatment of GDM. The EGGO and LIP studies were performed in obese populations and showed no improvement in pregnancy outcomes in the group who received treatment early in pregnancy compared to treatment later in pregnancy. These data suggest that future studies should focus on interventions starting pre-pregnancy in obese women. The pilot study of the TOBOGM study showed both benefits and harms of early treatment of GDM in a high-risk population. The treated group had a lower LGA rate but more NICU admissions, mainly due to a higher SGA rate. SGA can be a consequence of overtreatment [52], or insufficient gestational weight gain [53]. This highlights the need for data from large RCTs. The results of several large ongoing RCTs are expected for mid-2021 at the earliest. Many studies were conducted in a high-risk population. It is therefore also important to have evidence on the potential benefit or harm of screening for early GDM in low-risk populations and when using a universal screening strategy.
As we are waiting for stronger evidence from RCT’s, we do currently not recommend screening and treatment of GDM before 24–28 weeks of gestation in our center [54]. In line with the Flemish consensus of 2019 on screening for GDM [54], we recommend to universally screen for overt diabetes in early pregnancy. In addition, we propose a pragmatic approach for women who are diagnosed with mild hyperglycemia (FPG 5.5–6.9 mmol/L) in early pregnancy. We do not label these women as early GDM but advise follow-up with a dietician early in pregnancy (since these women are often overweight) and provide screening for GDM with an OGTT at 24 weeks of pregnancy [54].
The first results of the RCTs also show that treatment of women with HbA1c ≥ 5.7% and/or an FTFPG ≥ 5.1 mmol/L in early pregnancy, does not improve pregnancy outcomes [42]. HbA1c alone was not a good predictor for GDM early in pregnancy, because of the low sensitivity. It should always be used with other standard diagnostic tests for GDM, as was also demonstrated by the systematic review of Renz et al. [44]. FPG level generally further decreases by the end of the first trimester. Using FPG early in pregnancy, can lead to false positive results. Several studies have shown that an FPG level is a poor predictor for GDM with a sensitivity and specificity of 33–66% to predict GDM later in pregnancy. In contrast, the ToBOGM pilot study reported that 89% of the untreated women with early GDM in their study developed GDM at 24–28 weeks of gestation [39]. However, an OGTT was used in early pregnancy to screen for GDM (not only FTFPG) and this study evaluated a high-risk population.
Studies did not always report the pre-analytical method of collecting blood for FPG. Correct pre-analytic sampling of plasma glucose is important to prevent glycolysis and to prevent false negative results. A recent study of O’Malley showed that fluoride tubes must be stored on ice or must be centrifuged within 30 min to prevent glycolysis [55].
Since 2020, we have been faced with the impact of the COVID-19 pandemic on health care delivery. This might also impact screening for GDM and diabetes in pregnancy. There is a need to balance the sometimes-competing requirement of lowering the risk of direct viral transmission against the potential adverse impact of service changes. A pragmatic approach to screening for GDM is advised if an OGTT is not feasible. As an alternative, FPG, RPG and HbA1c, can be used. Women with a high-risk profile or with a history of GDM need to be closely monitored. It is important that usual guidelines and care will be re-evaluated as soon as possible [46,47,48,49,51].
4.4. Strengths and Limitations
A strength of this overview is that we performed an extensive narrative review including 45 studies evaluating the evidence on screening for GDM from both observational studies and RCTs. We provided an updated and detailed overview of the different observational and (ongoing) RCT’s, including data on timing of screening, the diagnostic criteria used for GDM, the screening strategy and comparator used. In addition, we highlighted the heterogeneity in risk factors used for selective screening in early pregnancy. However, our review also has several limitations. We did not perform a systematic review and could therefore not perform a meta-analysis. We could therefore also not assess the risk of bias of individual studies and did not contact the authors for obtaining missing and unpublished data. In addition, we did not assess the pre-analytical method of collecting blood for FPG determination.
5. Conclusions
Observational studies show conflicting results as to whether screening and treatment of GDM in early pregnancy is beneficial. However, most studies show that women with early GDM are at high risk of adverse pregnancy outcomes. A slight majority of relevant observational studies report an improved pregnancy outcome by treatment of early-onset GDM. However, so far, RCTs have not provided conclusive evidence of the beneficial effects of early treatment. Evidence from large RCTs is urgently needed, also evaluating lower risk populations to determine appropriate early-pregnancy OGTT thresholds for the diagnosis of GDM, and to assess the impact of early treatment on obstetrical outcomes and long-term offspring health. RCTs are also necessary to determine the appropriate cut-off of HbA1c in early pregnancy to identify women at risk for adverse pregnancy outcomes. Therefore, we currently recommend a pragmatic approach for women diagnosed with mild hyperglycemia in early pregnancy. A pragmatic approach to screen for GDM can be implemented during the COVID-19 pandemic, using FPG, RPG or HbA1c. However, routine guidelines and care must be re-evaluated as soon as possible.
Author Contributions
L.R., K.B. (Kaat Beunen) and K.B. (Katrien Benhalima) wrote the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
Katrien Benhalima is the recipient of a “Fundamenteel Klinisch Navorserschap FWO Vlaanderen”.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
This table gives an overview of the gestational diabetes mellitus diagnosis criteria used in this review.
Table A1.
This table gives an overview of the gestational diabetes mellitus diagnosis criteria used in this review.
| Criteria | OGTT | FPG | 1 h | 2 h | 3 h | Number of Abnormal Values |
|---|---|---|---|---|---|---|
| C&C | 100 g | ≥5.3 mmol/L | ≥10 mmol/L | ≥8.6 mmol/L | ≥7.8 mmol/L | ≥2 |
| NDDG | 100 g | ≥5.8 mmol/L | ≥10.5 mmol/L | ≥9 mmol/L | ≥8 mmol/L | ≥2 |
| IADPSG, WHO 2013 | 75 g | ≥5.1 mmol/L | ≥10 mmol/L | ≥8.5 mmol/L | ≥1 | |
| ADA | 100 g | ≥5.3 mmol/L | ≥10 mmol/L | ≥8.6 mmol/L | 7.8 mmol/L | ≥2 |
| WHO 1999 | 75 g | ≥6 mmol/L | ≥7.8 mmol/L | ≥1 | ||
| Finnish Diabetes Association | 75 g | >5.3 mmol/L | >10 mmol/L | >8.6 mmol/L | ≥1 | |
| New-Zealand criteria | 75 g | ≥5.5 mmol/L | ≥9 mmol/L | ≥1 | ||
| O’Sullivan criteria | 100 g | ≥5 mmol/L | ≥9 mmol/L | ≥7.8 mmol/L | ≥6.9 mmol/L | ≥2 |
| Chinese GDM criteria | 75 g | ≥5.1 mmol/L | ≥10 mmol/L | ≥8.5 mmol/L | ≥1 | |
| ADIPS | 75 g | ≥5.1 mmol/L | ≥10 mmol/L | ≥8.5 mmol/L | ≥1 | |
| Scottish Intercollegiate Guidelines Network | 75 g | ≥5.1 mmol/L | ≥10 mmol/L | ≥8.5 mmol/L | ≥1 | |
| DIPSI | 75 g | ≥7.8 mmol/L | ≥1 |
OGTT: oral glucose tolerance test; FPG: fasting plasma glucose; C&C: Carpenter and Coustan; NDDG: National Diabetes Data Group; IADPSG: International Association of the Diabetes and Pregnancy Study Groups; WHO: World Health Organization; ADA: American Diabetes Association; ADIPS: Australian Diabetes in Pregnancy society; DIPSI: Diabetes in Pregnancy Study Group India.
References
- Standards of medical care in diabetes–2013. Diabetes Care 2013, 36 (Suppl. 1), S11–S66. [CrossRef] [PubMed] [Green Version]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; McPhee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 14. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes–2020. Diabetes Care 2020, 43, S183–S192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hod, M.; Kapur, A.; Sacks, D.A.; Hadar, E.; Agarwal, M.; Di Renzo, G.C.; Roura, L.C.; McIntyre, H.D.; Morris, J.L.; Divakar, H. The International Federation of Gynecology and Obstetrics (FIGO) Initiative on gestational diabetes mellitus: A pragmatic guide for diagnosis, management, and care#. Int. J. Gynecol. Obstet. 2015, 131, S173–S211. [Google Scholar]
- Webber, J.; Charlton, M.; Johns, N. Diabetes in pregnancy: Management of diabetes and its complications from preconception to the postnatal period (NG3). Br. J. Diabetes 2015, 15, 107–111. [Google Scholar] [CrossRef] [Green Version]
- De Muylder, X. Perinatal complications of gestational diabetes: The influence of the timing of the diagnosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 1984, 18, 35–42. [Google Scholar] [CrossRef]
- Bartha, J.L.; Martinez-Del-Fresno, P.; Comino-Delgado, R. Gestational diabetes mellitus diagnosed during early pregnancy. Am. J. Obstet. Gynecol. 2000, 182, 346–350. [Google Scholar] [CrossRef]
- Barahona, M.J.; Sucunza, N.; García-Patterson, A.; Hernández, M.; Adelantado, J.M.; Ginovart, G.; De Leiva, A.; Corcoy, R. Period of gestational diabetes mellitus diagnosis and maternal and fetal morbidity. Acta Obstet. Gynecol. Scand. 2005, 84, 622–627. [Google Scholar] [CrossRef]
- Hawkins, J.S.; Lo, J.Y.; Casey, B.M.; McIntire, D.D.; Leveno, K.J. Diet-treated gestational diabetes mellitus: Comparison of early vs routine diagnosis. Am. J. Obstet. Gynecol. 2008, 198, 287.e1–287.e6. [Google Scholar] [CrossRef]
- Riskin-Mashiah, S.; Younes, G.; Damti, A.; Auslender, R. First-trimester fasting hyperglycemia and adverse pregnancy outcomes. Diabetes Care 2009, 32, 1639–1643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plasencia, W.; Garcia, R.; Pereira, S.; Akolekar, R.; Nicolaides, K.H. Criteria for screening and diagnosis of gestational diabetes mellitus in the first trimester of pregnancy. Fetal Diagn. Ther. 2011, 30, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Corrado, F.; D’Anna, R.; Cannata, M.L.; Interdonato, M.L.; Pintaudi, B.; Di Benedetto, A. Correspondence between first-trimester fasting glycaemia, and oral glucose tolerance test in gestational diabetes diagnosis. Diabetes Metab. 2012, 38, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.W.; Yang, H.X.; Wei, Y.M.; Yan, J.; Wang, Z.L.; Li, X.L.; Wu, H.R.; Li, N.; Zhang, M.H.; Liu, X.H.; et al. Evaluation of the value of fasting plasma glucose in the first prenatal visit to diagnose gestational diabetes mellitus in china. Diabetes Care 2013, 36, 586–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alunni, M.L.; Roeder, H.A.; Moore, T.R.; Ramos, G.A. First trimester gestational diabetes screening—Change in incidence and pharmacotherapy need. Diabetes Res. Clin. Pract. 2015, 109, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Amylidi, S.; Mosimann, B.; Stettler, C.; Fiedler, G.M.; Surbek, D.; Raio, L. First-trimester glycosylated hemoglobin in women at high risk for gestational diabetes. Acta Obstet. Gynecol. Scand. 2016, 95, 93–97. [Google Scholar] [CrossRef] [Green Version]
- Harreiter, J.; Simmons, D.; Desoye, G.; Corcoy, R.; Adelantado, J.M.; Devlieger, R.; van Assche, A.; Galjaard, S.; Damm, P.; Mathiesen, E.R.; et al. IADPSG and WHO 2013 Gestational Diabetes Mellitus Criteria Identify Obese Women With Marked Insulin Resistance in Early Pregnancy: Table 1. Diabetes Care 2016, 39, e90–e92. [Google Scholar] [CrossRef] [Green Version]
- Mañé, L.; Flores-Le Roux, J.A.; Benaiges, D.; Rodríguez, M.; Marcelo, I.; Chillarón, J.J.; Pedro-Botet, J.; Llauradó, G.; Gortazar, L.; Carreras, R.; et al. Role of first trimester HbA1c as a predictor of adverse obstetric outcomes in a multi-ethnic cohort. J. Clin. Endocrinol. Metab. 2016. [Google Scholar] [CrossRef] [PubMed]
- Osmundson, S.S.; Zhao, B.S.; Kunz, L.; Wang, E.; Popat, R.; Nimbal, V.C.; Palaniappan, L.P. First Trimester Hemoglobin A1c Prediction of Gestational Diabetes. Amer. J. Perinatol. 2016, 33, 977–982. [Google Scholar] [CrossRef]
- Sweeting, A.N.; Ross, G.P.; Hyett, J.; Molyneaux, L.; Constantino, M.; Harding, A.J.; Wong, J. Gestational Diabetes Mellitus in Early Pregnancy: Evidence for Poor Pregnancy Outcomes Despite Treatment. Diabetes Care 2016, 39, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Sweeting, A.N.; Ross, G.P.; Hyett, J.; Molyneaux, L.; Tan, K.; Constantino, M.; Harding, A.J.; Wong, J. Baseline HbA1c to identify high-risk gestational diabetes: Utility in early vs standard gestational diabetes. J. Clin. Endocrinol. Metab. 2017, 102, 150–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseini, E.; Janghorbani, M.; Shahshahan, Z. Comparison of risk factors and pregnancy outcomes of gestational diabetes mellitus diagnosed during early and late pregnancy. Midwifery 2018, 66, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.K.; Haddow, L.; Ramaesh, A.; Kelly, R.; Johns, E.C.; Denison, F.C.; Dover, A.R.; Reynolds, R.M. Early screening and treatment of gestational diabetes in high-risk women improves maternal and neonatal outcomes: A retrospective clinical audit. Diabetes Res. Clin. Pract. 2018, 144, 294–301. [Google Scholar] [CrossRef]
- Salman, L.; Arbib, N.; Borovich, A.; Shmueli, A.; Chen, R.; Wiznitzer, A.; Hadar, E. The impact of first trimester fasting glucose level on adverse perinatal outcome. J. Perinatol. 2018, 38, 451–455. [Google Scholar] [CrossRef]
- Bianchi, C.; de Gennaro, G.; Romano, M.; Battini, L.; Aragona, M.; Corfini, M.; Del Prato, S.; Bertolotto, A. Early vs. standard screening and treatment of gestational diabetes in high-risk women—An attempt to determine relative advantages and disadvantages. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 598–603. [Google Scholar] [CrossRef]
- Del Val, T.L.; Lázaro, V.A.; Lacalle, C.G.; Moreno, B.T.; Carbajal, G.C.; Fernandez, B.A. Fasting glucose in the first trimester: An initial approach to diagnosis of gestational diabetes. Endocrinol. Diabetes Nutr. 2019, 66, 11–18. [Google Scholar]
- Mañé, L.; Flores-Le Roux, J.A.; Pedro-Botet, J.; Gortazar, L.; Chillarón, J.J.; Llauradó, G.; Payà, A.; Benaiges, D. Is fasting plasma glucose in early pregnancy a better predictor of adverse obstetric outcomes than glycated haemoglobin? Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 79–84. [Google Scholar] [CrossRef]
- Benhalima, K.; Van Crombrugge, P.; Moyson, C.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Maes, T.; Dufraimont, E.; De Block, C.; et al. Women with mild fasting hyperglycemia in early pregnancy have more neonatal intensive care admissions. J. Clin. Endocrinol. Metab. 2020. [Google Scholar] [CrossRef] [PubMed]
- Boriboonhirunsarn, D.; Sunsaneevithayakul, P.; Pannin, C.; Wamuk, T. Prevalence of early-onset GDM and associated risk factors in a university hospital in Thailand. J. Obstet. Gynaecol. 2020, 1–5. [Google Scholar] [CrossRef]
- Clarke, E.; Cade, T.J.; Brennecke, S. Early Pregnancy Screening for Women at High-Risk of GDM Results in Reduced Neonatal Morbidity and Similar Maternal Outcomes to Routine Screening. J. Pregnancy 2020, 2020, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Cosson, E.; Vicaut, E.; Berkane, N.; Cianganu, T.L.; Baudry, C.; Portal, J.-J.; Boujenah, J.; Valensi, P.; Carbillon, L. Prognosis associated with initial care of increased fasting glucose in early pregnancy: A retrospective study. Diabetes Metab. 2020. [Google Scholar] [CrossRef]
- Immanuel, J.; Simmons, D.; Desoye, G.; Corcoy, R.; Adelantado, J.M.; Devlieger, R.; Lapolla, A.; Dalfra, M.G.; Bertolotto, A.; Harreiter, J.; et al. Performance of early pregnancy HbA1c for predicting gestational diabetes mellitus and adverse pregnancy outcomes in obese European women. Diabetes Res. Clin. Pract. 2020, 168, 108378. [Google Scholar] [CrossRef]
- Jokelainen, M.; Stach-Lempinen, B.; Rönö, K.; Nenonen, A.; Kautiainen, H.; Teramo, K.; Klemetti, M.M. Oral glucose tolerance test results in early pregnancy: A Finnish population-based cohort study. Diabetes Res. Clin. Pract. 2020, 162, 108077. [Google Scholar] [CrossRef]
- Liu, B.; Cai, J.; Xu, Y.; Long, Y.; Deng, L.; Lin, S.; Zhang, J.; Yang, J.; Zhong, L.; Luo, Y.; et al. Early Diagnosed Gestational Diabetes Mellitus Is Associated With Adverse Pregnancy Outcomes: A Prospective Cohort Study. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, S.; Aoki, S.; Kasai, J.; Shindo, R.; Obata, S.; Hasegawa, Y.; Mochimaru, A.; Miyagi, E. High probability of false-positive gestational diabetes mellitus diagnosis during early pregnancy. BMJ Open Diabetes Res. Care 2020, 8, e001234. [Google Scholar] [CrossRef]
- Sesmilo, G.; Prats, P.; Garcia, S.; Rodríguez, I.; Rodríguez-Melcón, A.; Berges, I.; Serra, B. First-trimester fasting glycemia as a predictor of gestational diabetes (GDM) and adverse pregnancy outcomes. Acta Diabetol. 2020, 57, 697–703. [Google Scholar] [CrossRef]
- Osmundson, S.S.; Norton, M.E.; El-Sayed, Y.Y.; Carter, S.; Faig, J.C.; Kitzmiller, J.L. Early Screening and Treatment of Women with Prediabetes: A Randomized Controlled Trial. Amer. J. Perinatol. 2016, 33, 172–179. [Google Scholar] [CrossRef]
- Hughes, R.C.E.; Rowan, J.; Williman, J. Prediabetes in pregnancy, can early intervention improve outcomes? A feasibility study for a parallel randomised clinical trial. BMJ Open 2018, 8, e018493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmons, D.; Nema, J.; Parton, C.; Vizza, L.; Robertson, A.; Rajagopal, R.; Ussher, J.; Perz, J. The treatment of booking gestational diabetes mellitus (TOBOGM) pilot randomised controlled trial. BMC Pregnancy Childbirth 2018, 18, 151. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Hague, W.M.; Teede, H.J.; Cheung, N.W.; Hibbert, E.J.; Nolan, C.J.; Peek, M.J.; Girosi, F.; Cowell, C.T.; Wong, V.W.M.; et al. Hyperglycaemia in early pregnancy: The Treatment of Booking Gestational diabetes Mellitus (TOBOGM) study. A randomised controlled trial. Med. J. Aust. 2018, 209, 405–406. [Google Scholar] [CrossRef] [PubMed]
- Vinter, C.A.; Tanvig, M.H.; Christensen, M.H.; Ovesen, P.G.; Jørgensen, J.S.; Andersen, M.S.; McIntyre, H.D.; Jensen, D.M. Lifestyle Intervention in Danish Obese Pregnant Women With Early Gestational Diabetes Mellitus According to WHO 2013 Criteria Does Not Change Pregnancy Outcomes: Results From the LiP (Lifestyle in Pregnancy) Study. Diabetes Care 2018, 41, 2079–2085. [Google Scholar] [CrossRef] [Green Version]
- Roeder, H.A.; Moore, T.R.; Wolfson, M.T.; Gamst, A.C.; Ramos, G.A. Treating hyperglycemia in early pregnancy: A randomized controlled trial. Am. J. Obstet. Gynecol. MFM 2019, 1, 33–41. [Google Scholar] [CrossRef]
- Harper, L.M.; Jauk, V.; Longo, S.; Biggio, J.R.; Szychowski, J.M.; Tita, A.T. Early gestational diabetes screening in obese women: A randomized controlled trial. Am. J. Obstet. Gynecol. 2020, 222, 495.e1–495.e8. [Google Scholar] [CrossRef]
- Renz, P.B.; Chume, F.C.; Timm, J.R.T.; Pimentel, A.L.; Camargo, J.L. Diagnostic accuracy of glycated hemoglobin for gestational diabetes mellitus: A systematic review and meta-analysis. Clin. Chem. Lab. Med. 2019, 57, 1435–1449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, R.C.E.; Moore, M.P.; Gullam, J.E.; Mohamed, K.; Rowan, J. An early pregnancy HbA1c ≥5.9% (41 mmol/mol) is optimal for detecting diabetes and identifies women at increased risk of adverse pregnancy outcomes. Diabetes Care 2014, 37, 2953–2959. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, H.D.; Gibbons, K.S.; Ma, R.C.W.; Tam, W.H.; Sacks, D.A.; Lowe, J.; Madsen, L.R.; Catalano, P.M. Testing for gestational diabetes during the COVID-19 pandemic. An evaluation of proposed protocols for the United Kingdom, Canada and Australia. Diabetes Res. Clin. Pract. 2020, 167, 108353. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, H.D.; Moses, R.G. The Diagnosis and Management of Gestational Diabetes Mellitus in the Context of the COVID-19 Pandemic. Diabetes Care 2020, 43, 1433–1434. [Google Scholar] [CrossRef] [PubMed]
- Meek, C.L.; Lindsay, R.S.; Scott, E.M.; Aiken, C.E.; Myers, J.; Reynolds, R.; Simmons, D.; Yamamoto, J.M.; McCance, D.R.; Murphy, H.R. Approaches to screening for hyperglycaemia in pregnant women during and after the COVID-19 pandemic. Diabet. Med. 2020, e14380. [Google Scholar] [CrossRef]
- Thangaratinam, S.; Cooray, S.D.; Sukumar, N.; Huda, M.S.B.; Devlieger, R.; Benhalima, K.; McAuliffe, F.; Saravanan, P.; Teede, H.J. ENDOCRINOLOGY IN THE TIME OF COVID-19: Diagnosis and management of gestational diabetes mellitus. Eur. J. Endocrinol. 2020, 183, G49–G56. [Google Scholar] [CrossRef]
- Torlone, E.; Festa, C.; Formoso, G.; Scavini, M.; Sculli, M.A.; Succurro, E.; Sciacca, L.; Di Bartolo, P.; Purrello, F.; Lapolla, A. Italian recommendations for the diagnosis of gestational diabetes during COVID-19 pandemic: Position statement of the Italian Association of Clinical Diabetologists (AMD) and the Italian Diabetes Society (SID), diabetes, and pregnancy study group. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1418–1422. [Google Scholar] [CrossRef]
- Seshiah, V.; Balaji, V.; Banerjee, S.; Sahay, R.; Divakar, H.; Jain, R.; Chawla, R.; Das, A.K.; Gupta, S.; Krishnan, D. Diagnosis and principles of management of gestational diabetes mellitus in the prevailing COVID-19 pandemic. Int. J. Diabetes Dev. Ctries. 2020, 40, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Langer, O.; Levy, J.; Brustman, L.; Anyaegbunam, A.; Merkatz, R.; Divon, M. Glycemic control in gestational diabetes mellitus--how tight is tight enough: Small for gestational age versus large for gestational age? Am. J. Obstet. Gynecol. 1989, 161, 646–653. [Google Scholar] [CrossRef]
- Catalano, P.M.; Mele, L.; Landon, M.B.; Ramin, S.M.; Reddy, U.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. Inadequate weight gain in overweight and obese pregnant women: What is the effect on fetal growth? Am. J. Obstet. Gynecol. 2014, 211, 137.e1–137.e7. [Google Scholar] [CrossRef] [Green Version]
- Benhalima, K.; Minschart, C.; Van Crombrugge, P.; Calewaert, P.; Verhaeghe, J.; Vandamme, S.; Theetaert, K.; Devlieger, R.; Pierssens, L.; Ryckeghem, H.; et al. The 2019 Flemish consensus on screening for overt diabetes in early pregnancy and screening for gestational diabetes mellitus. Acta Clin. Belg. 2020, 75, 340–347. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, E.G.; Reynolds, C.M.E.; O’Kelly, R.; Killalea, A.; Sheehan, S.R.; Turner, M.J. A Prospective Evaluation of Point-of-Care Measurements of Maternal Glucose for the Diagnosis of Gestational Diabetes Mellitus. Clin. Chem. 2020, 66, 316–323. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The literature search and selection process.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Raets, L.; Beunen, K.; Benhalima, K. Screening for Gestational Diabetes Mellitus in Early Pregnancy: What Is the Evidence? J. Clin. Med. 2021, 10, 1257. https://doi.org/10.3390/jcm10061257
AMA Style
Raets L, Beunen K, Benhalima K. Screening for Gestational Diabetes Mellitus in Early Pregnancy: What Is the Evidence? Journal of Clinical Medicine. 2021; 10(6):1257. https://doi.org/10.3390/jcm10061257
Chicago/Turabian StyleRaets, Lore, Kaat Beunen, and Katrien Benhalima. 2021. "Screening for Gestational Diabetes Mellitus in Early Pregnancy: What Is the Evidence?" Journal of Clinical Medicine 10, no. 6: 1257. https://doi.org/10.3390/jcm10061257
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.