
Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
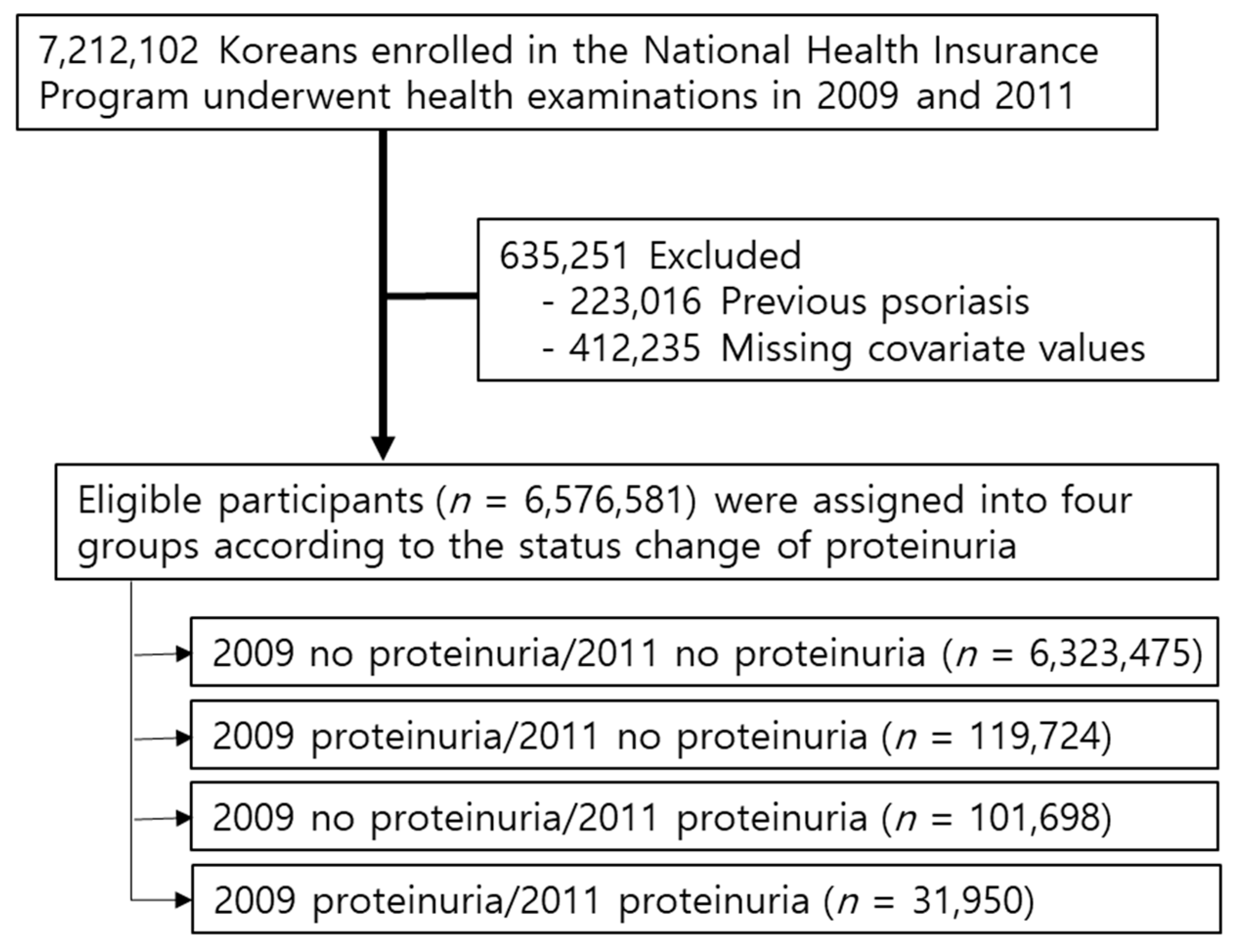
2.1. Study Design and Database
2.2. Measurements and Definitions
2.3. Study Outcomes and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Effects of Changes in Proteinuria on Psoriasis Development
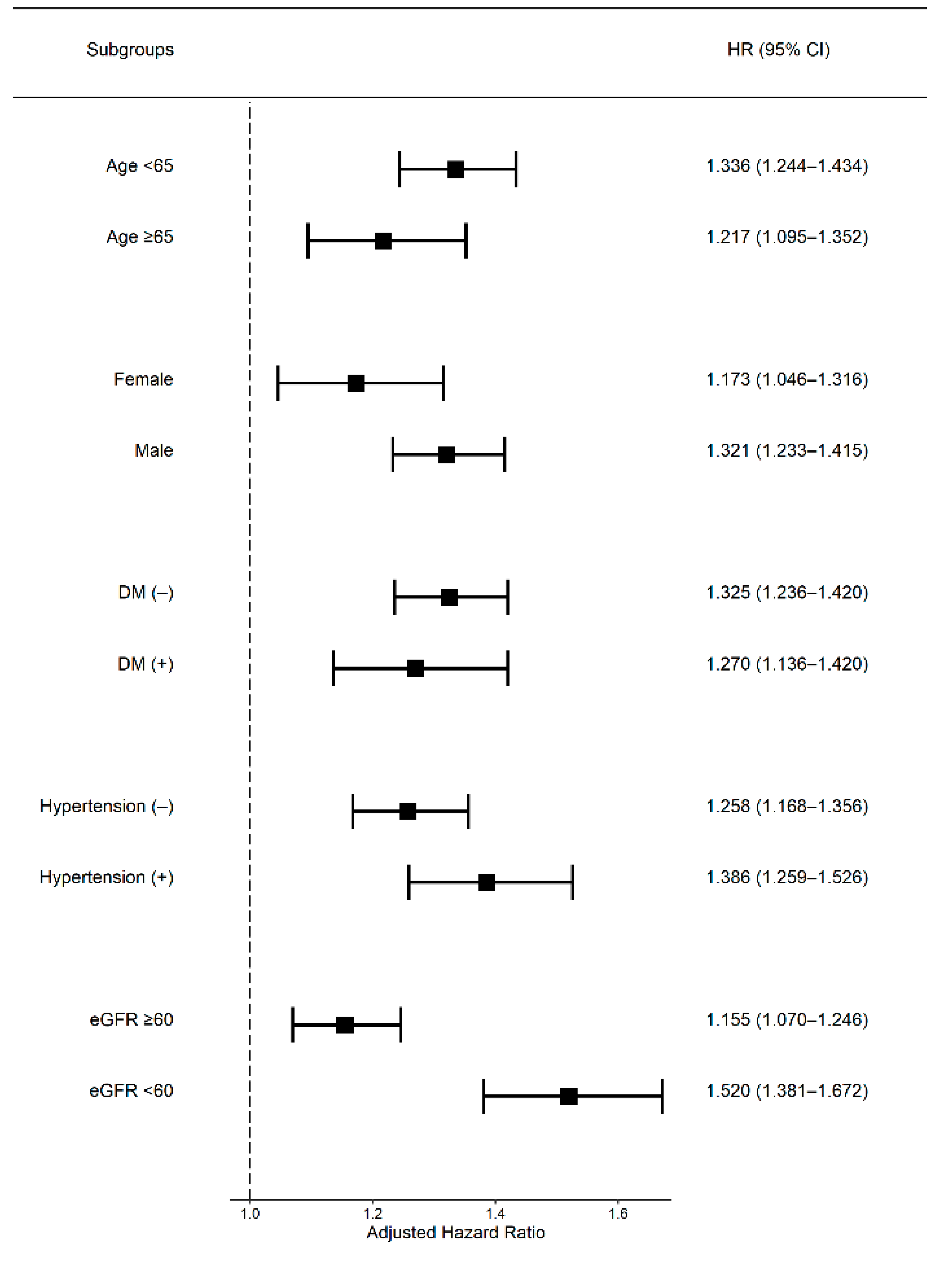
3.3. Subgroup Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Egeberg, A.; Mallbris, L.; Hilmar Gislason, G.; Skov, L.; Riis Hansen, P. Increased risk of migraine in patients with psoriasis: A Danish nationwide cohort study. J. Am. Acad. Dermatol. 2015, 73, 829–835. [Google Scholar] [CrossRef]
- Han, J.H.; Lee, J.H.; Han, K.D.; Seo, H.M.; Bang, C.H.; Park, Y.M.; Lee, J.Y.; Park, Y.G. Epidemiology and Medication Trends in Patients with Psoriasis: A Nationwide Population-based Cohort Study from Korea. Acta Derm. Venereol. 2018, 98, 396–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visconti, L.; Leonardi, G.; Buemi, M.; Santoro, D.; Cernaro, V.; Ricciardi, C.A.; Lacquaniti, A.; Coppolino, G. Kidney disease and psoriasis: Novel evidences beyond old concepts. Clin. Rheumatol. 2016, 35, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Skov, L.; Gislason, G.H.; Thyssen, J.P.; Mallbris, L. Incidence and Prevalence of Psoriasis in Denmark. Acta Derm. Venereol. 2017, 97, 808–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, J.C.; Shi, L.H.; Huang, J.Y.; Wu, X.F.; Wu, R.; Chiou, J.Y. Epidemiology and Medication Pattern Change of Psoriatic Diseases in Taiwan from 2000 to 2013: A Nationwide, Population-based Cohort Study. J. Rheumatol. 2018, 45, 385–392. [Google Scholar] [CrossRef]
- Gisondi, P. High prevalence of alcohol use disorders in patients with inflammatory skin diseases applies to both psoriasis and eczema. Br. J. Dermatol. 2017, 177, 606–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, D.L.; Spelman, L.S.; Martin, N.G. Psoriasis in Australian twins. J. Am. Acad. Dermatol. 1993, 29, 428–434. [Google Scholar] [CrossRef] [Green Version]
- Correia, B.; Torres, T. Obesity: A key component of psoriasis. Acta Biomed. 2015, 86, 121–129. [Google Scholar] [PubMed]
- Naldi, L.; Mercuri, S.R. Smoking and psoriasis: From epidemiology to pathomechanisms. J. Investig. Dermatol. 2009, 129, 2741–2743. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, E.; Sato, Y.; Minagawa, A.; Okuyama, R. Pathogenesis of psoriasis and development of treatment. J. Dermatol. 2018, 45, 264–272. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.E.; Paust, H.J.; Steinmetz, O.M.; Panzer, U. The Th17 immune response in renal inflammation. Kidney Int. 2010, 77, 1070–1075. [Google Scholar] [CrossRef] [Green Version]
- Ren, F.; Zhang, M.; Hao, L.; Sang, H. Kidney involvement in psoriasis: A case-control study from China. Int. Urol. Nephrol. 2017, 49, 1999–2003. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Han, J.H.; Bang, C.H.; Yoo, S.A.; Han, K.D.; Kim, H.N.; Park, Y.M.; Lee, J.Y.; Lee, J.H. Risk of End-Stage Renal Disease in Psoriatic Patients: Real-World Data from a Nationwide Population-Based Cohort Study. Sci. Rep. 2019, 9, 16581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, C.C.; Wang, J.; Chen, Y.F.; Wang, S.H.; Chen, F.L.; Tung, T.H. Risk of incident chronic kidney disease and end-stage renal disease in patients with psoriasis: A nationwide population-based cohort study. J. Dermatol. Sci. 2015, 78, 232–238. [Google Scholar] [CrossRef]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.Y.; Kwon, H.S.; Cha, B.S.; Park, J.Y.; Lee, K.U.; Ko, K.S.; Lee, B.W. Background and data configuration process of a nationwide population-based study using the korean national health insurance system. Diabetes Metab. J. 2014, 38, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Yang, H.K.; Han, K.; Kwon, H.S.; Park, Y.M.; Cho, J.H.; Yoon, K.H.; Kang, M.I.; Cha, B.Y.; Lee, S.H. Obesity, metabolic health, and mortality in adults: A nationwide population-based study in Korea. Sci. Rep. 2016, 6, 30329. [Google Scholar] [CrossRef]
- Ko, S.H.; Kim, D.J.; Park, J.H.; Park, C.Y.; Jung, C.H.; Kwon, H.S.; Park, J.Y.; Song, K.H.; Han, K.; Lee, K.U.; et al. Trends of antidiabetic drug use in adult type 2 diabetes in Korea in 2002–2013: Nationwide population-based cohort study. Medicine (Baltimore) 2016, 95, e4018. [Google Scholar] [CrossRef]
- Lee, S.W.; Lee, H.Y.; Ihm, S.H.; Park, S.H.; Kim, T.H.; Kim, H.C. Status of hypertension screening in the Korea National General Health Screening Program: A questionnaire survey on 210 screening centers in two metropolitan areas. Clin. Hypertens 2017, 23, 23. [Google Scholar] [CrossRef]
- Cecchi, R.; Seghieri, G.; Gironi, A.; Tuci, F.; Giomi, A. Relation between urinary albumin excretion and skin involvement in patients with psoriasis. Dermatology 1992, 185, 93–95. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Szepietowski, T. Is renal function altered in patients with psoriasis vulgaris?—A short review. J. Dermatol. 2000, 27, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Madeddu, P.; Ena, P.; Glorioso, N.; Cerimele, D.; Rappelli, A. High prevalence of microproteinuria, an early index of renal impairment, in patients with diffuse psoriasis. Nephron 1988, 48, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Kaftan, O.; Kaftan, B.; Toppare, M.F.; Eksioglu, M. Renal involvement in psoriasis. Dermatology 1996, 192, 189–190. [Google Scholar] [CrossRef] [PubMed]
- De Caterina, R.; Basta, G.; Lazzerini, G.; Dell’Omo, G.; Petrucci, R.; Morale, M.; Carmassi, F.; Pedrinelli, R. Soluble vascular cell adhesion molecule-1 as a biohumoral correlate of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 2646–2654. [Google Scholar] [CrossRef] [PubMed]
- Groves, R.W.; Kapahi, P.; Barker, J.N.; Haskard, D.O.; MacDonald, D.M. Detection of circulating adhesion molecules in erythrodermic skin disease. J. Am. Acad. Dermatol. 1995, 32, 32–36. [Google Scholar] [CrossRef]
- Cai, J.P.; Harris, K.; Falanga, V.; Taylor, J.R.; Chin, Y.H. UVB therapy decreases the adhesive interaction between peripheral blood mononuclear cells and dermal microvascular endothelium, and regulates the differential expression of CD54, VCAM-1, and E-selectin in psoriatic plaques. Br. J. Dermatol. 1996, 134, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Pedrinelli, R. Microalbuminuria in essential hypertension. A marker of systemic vascular damage? Nephrol. Dial. Transpl. 1997, 12, 379–381. [Google Scholar] [CrossRef]
- Pontremoli, R. Microalbuminuria in essential hypertension—Its relation to cardiovascular risk factors. Nephrol. Dial. Transpl. 1996, 11, 2113–2115. [Google Scholar] [CrossRef]
- Erley, C.M.; Risler, T. Microalbuminuria in primary hypertension: Is it a marker of glomerular damage? Nephrol. Dial. Transpl. 1994, 9, 1713–1715. [Google Scholar]
- Ena, P.; Madeddu, P.; Glorioso, N.; Cerimele, D.; Rappelli, A. High prevalence of cardiovascular diseases and enhanced activity of the renin-angiotensin system in psoriatic patients. Acta Cardiol. 1985, 40, 199–205. [Google Scholar]
- McDonald, C.J.; Calabresi, P. Psoriasis and occlusive vascular disease. Br. J. Dermatol. 1978, 99, 469–475. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Total (n = 6,576,851) | Non-Psoriasis Group (n = 6,414,383) | Psoriasis Group (n = 162,468) | p Value |
|---|---|---|---|---|
| Age (years) | 48.89 ± 13.53 | 48.83 ± 13.52 | 51.53 ± 13.82 | <0.0001 |
| Sex, male (%) | 3,747,448 (56.98) | 3,650,244 (56.91) | 97,204 (59.83) | <0.0001 |
| Current smoking | ||||
| None | 3,848,988 (58.52) | 3,758,772 (58.6) | 90,216 (55.53) | <0.0001 |
| Ex | 1,121,581 (17.05) | 1,090,826 (17.01) | 30,755 (18.93) | |
| Current | 1,606,282 (24.42) | 1,564,785 (24.39) | 41,497 (25.54) | |
| Drinking | ||||
| None | 3,337,444 (50.75) | 3,252,694 (50.71) | 84,750 (52.16) | <0.0001 |
| Mild | 2,764,312 (42.03) | 2,698,978 (42.08) | 65,334 (40.21) | |
| Heavy 1 | 475,095 (7.22) | 462,711 (7.21) | 12,384 (7.62) | |
| Physical activity, regular | 1,340,250 (20.38) | 1,306,224 (20.36) | 34,026 (20.94) | <0.0001 |
| Income, low 2 | 1,114,375 (16.94) | 1,085,828 (16.93) | 28,547 (17.57) | <0.0001 |
| BMI (kg/m2) | 23.83 ± 3.18 | 23.82 ± 3.18 | 24 ± 3.15 | <0.0001 |
| Waist circumference (cm) | 80.62 ± 9.00 | 80.6 ± 9.00 | 81.62 ± 8.97 | <0.0001 |
| Diabetes mellitus | 401,418 (6.10) | 389,720 (6.08) | 11,698 (7.20) | <0.0001 |
| Hypertension | 921,687 (14.01) | 896,970 (13.98) | 24,717 (15.21) | <0.0001 |
| Dyslipidemia | 718,083 (10.92) | 699,779 (10.91) | 18,304 (11.27) | <0.0001 |
| Fasting blood glucose (mg/dL) | 96.74 ± 22.39 | 96.71 ± 22.36 | 97.84 ± 23.65 | <0.0001 |
| Systolic blood pressure (mmHg) | 122.35 ± 14.69 | 122.33 ± 14.69 | 122.92 ± 14.71 | <0.0001 |
| Diastolic blood pressure (mmHg) | 76.36 ± 9.88 | 76.35 ± 9.88 | 76.55 ± 9.82 | <0.0001 |
| Total cholesterol (mg/dL) | 195.43 ± 40.62 | 195.42 ± 40.62 | 195.96 ± 40.63 | <0.0001 |
| Estimated GFR (mL/min/1.73 m2) | 87.21 ± 45.40 | 87.23 ± 45.46 | 86.37 ± 43.09 | <0.0001 |
| F/U duration (years) | 7.23 ± 0.93 | 7.32 ± 0.67 | 3.75 ± 2.14 | <0.0001 |
| Characteristics | Never Proteinuria (Neg/Neg) (n = 6,323,475) | Past Proteinuria (Pos/Neg) (n = 119,728) | New Proteinuria (Neg/Pos) (n = 101,698) | Persistent Proteinuria (Pos/Pos) (n = 31,950) | p Value |
|---|---|---|---|---|---|
| Psoriasis event | 155,413 (2.46) | 3186 (2.66) | 2744 (2.7) | 1125 (3.52) | <0.0001 |
| Follow-up duration (years) | 7.24 ± 0.91 | 7.14 ± 1.12 | 7.08 ± 1.25 | 6.91 ± 1.48 | <0.0001 |
| Age (years) | 48.73 ± 13.49 | 52.43 ± 13.90 | 52.77 ± 14.31 | 55.87 ± 13.15 | <0.0001 |
| Sex, male (%) | 3,604,171 (57.00) | 64,272 (53.68) | 57,672 (56.71) | 21,333 (66.77) | <0.0001 |
| Income 1 | 1,068,434 (16.9) | 22,119 (18.47) | 18,210 (17.91) | 5612 (17.56) | <0.0001 |
| Exercise 2 | 1,287,705 (20.36) | 24,902 (20.80) | 20,912 (20.56) | 6731 (21.07) | <0.0001 |
| Smoking | <0.0001 | ||||
| None | 3,699,938 (58.51) | 72,828 (60.83) | 59,386 (58.39) | 16,836 (52.69) | |
| Ex- | 1,075,202 (17.00) | 20,709 (17.30) | 18,423 (18.12) | 7247 (22.68) | |
| Current | 1,548,335 (24.49) | 26,191 (21.88) | 23,889 (23.49) | 7867 (24.62) | |
| Drinking | <0.0001 | ||||
| None | 3,199,180 (50.59) | 66,013 (55.14) | 54,373 (53.47) | 17,878 (55.96) | |
| Mild | 2,669,906 (42.22) | 44,552 (37.21) | 38,523 (37.88) | 11,331 (35.46) | |
| Heavy | 454,389 (7.19) | 9163 (7.65) | 8802 (8.66) | 2741 (8.58) | |
| DM | 359,676 (5.69) | 15,426 (12.88) | 17,737 (17.44) | 8579 (26.85) | <0.0001 |
| HTN | 861,774 (13.63) | 24,016 (20.06) | 24,827 (24.41) | 11,070 (34.65) | <0.0001 |
| Dyslipidemia | 684,227 (10.82) | 14,033 (11.72) | 14,490 (14.25) | 5333 (16.69) | <0.0001 |
| BMI (kg/m2) | 23.8 ± 3.16 | 24.34 ± 3.47 | 24.39 ± 3.57 | 25.05 ± 3.65 | <0.0001 |
| WC (cm) | 80.54 ± 8.96 | 82.1 ± 9.59 | 82.55 ± 9.79 | 85.1 ± 9.70 | <0.0001 |
| Glucose (mg/dL) | 97.07 ± 21.44 | 104.1 ± 32.44 | 109.01 ± 37.87 | 118.63 ± 46.63 | <0.0001 |
| SBP (mmHg) | 122.36 ± 14.48 | 125.21 ± 15.75 | 126.91 ± 17.01 | 132.09 ± 17.29 | <0.0001 |
| DBP (mmHg) | 76.28 ± 9.75 | 77.49 ± 10.41 | 78.57 ± 11.01 | 80.71 ± 11.24 | <0.0001 |
| TC (mg/dL) | 195.04 ± 36.48 | 194.55 ± 38.66 | 197.67 ± 40.82 | 198.9 ± 45.20 | <0.0001 |
| HDL | 55.22 ± 21.92 | 54.2 ± 19.28 | 54.43 ± 34.85 | 51.61 ± 17.17 | <0.0001 |
| LDL | 114.58 ± 44.17 | 112.92 ± 44.37 | 115.89 ± 56.72 | 114.64 ± 77.38 | <0.0001 |
| GFR (mL/min/1.73 m2) | 89.6 ± 37.71 | 86.18 ± 39.33 | 83.98 ± 36.21 | 72.26 ± 42.26 | <0.0001 |
| TG | 111.63 (111.58–111.68) | 119.23 (118.84–119.62) | 121.87 (121.43–122.32) | 144.46 (143.54–145.38) | <0.0001 |
| Proteinuria | Total (n) | Psoriasis (n) | IR (per 1000) | HR (95% Confidence Interval) | ||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| Never (Neg/Neg) | 6,323,475 | 155,413 | 3.40 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| Past (Pos/Neg) | 101,698 | 2744 | 3.81 | 1.12 (1.08–1.17) | 1.06 (1.02–1.10) | 1.05 (1.01–1.09) |
| New (Neg/Pos) | 119,728 | 3186 | 3.73 | 1.10 (1.06–1.14) | 1.04 (1.01–1.08) | 1.03 (1.00–1.07) |
| Persistent (Pos/Pos) | 31,950 | 1125 | 5.10 | 1.51 (1.42–1.60) | 1.33 (1.26–1.41) | 1.32 (1.24–1.40) |
| p value | <0.0001 | <0.0001 | <0.0001 | |||
| Proteinuria Significance | Total (n) | Psoriasis (n) | IR (per 1000) | HR (95% Confidence Interval) | ||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | ||||
| 2011 | ||||||
| Negative | 6,313,688 | 155,308 | 3.40 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| trace | 129,515 | 3291 | 3.54 | 1.04 (1.01–1.08) | 1.01 (0.98–1.05) | 1.01 (0.98–1.05) |
| 1+ | 88,245 | 2426 | 3.88 | 1.14 (1.10–1.19) | 1.07 (1.03–1.11) | 1.06 (1.02–1.11) |
| 2+ | 34,340 | 1068 | 4.46 | 1.31 (1.24–1.40) | 1.20 (1.13–1.27) | 1.19 (1.12–1.26) |
| 3+ | 9353 | 307 | 4.81 | 1.42 (1.27–1.59) | 1.26 (1.13–1.41) | 1.25 (1.12–1.40) |
| 4+ | 1710 | 68 | 5.93 | 1.78 (1.40–2.25) | 1.60 (1.27–2.03) | 1.58 (1.25–2.00) |
| p trend | < 0.0001 | < 0.0001 | < 0.0001 | |||
| 2009 | ||||||
| Negative | 6,279,838 | 154,350 | 3.40 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| trace | 145,335 | 3807 | 3.64 | 1.07 (1.04–1.11) | 1.04 (1.01–1.08) | 1.04 (1.01–1.08) |
| 1+ | 103,394 | 2802 | 3.80 | 1.12 (1.08–1.16) | 1.06 (1.02–1.10) | 1.05 (1.01–1.09) |
| 2+ | 37,429 | 1115 | 4.23 | 1.25 (1.18–1.32) | 1.15 (1.08–1.22) | 1.14 (1.08–1.21) |
| 3+ | 9107 | 333 | 5.29 | 1.57 (1.41–1.75) | 1.42 (1.27–1.58) | 1.40 (1.26–1.56) |
| 4+ | 1748 | 61 | 5.08 | 1.50 (1.17–1.93) | 1.34 (1.04–1.72) | 1.33 (1.03–1.70) |
| p trend | < 0.0001 | < 0.0001 | < 0.0001 | |||
| Proteinuria | Total (n) | Psoriasis (n) | IR (per 1000) | HR (95% CI) Model 3 | Proteinuria | Total (n) | Psoriasis (n) | IR (per 1000) | HR (95% CI) Model 3 |
|---|---|---|---|---|---|---|---|---|---|
| eGFR < 60 mL/min/1.73 m2 | eGFR ≥ 60 mL/min/1.73 m2 | ||||||||
| Never | 312,727 | 8848 | 3.96 | 1 (ref.) | Never | 6,010,748 | 146,565 | 3.37 | 1 (ref.) |
| Past | 12,695 | 427 | 4.88 | 1.13 (1.02–1.24) | Past | 107,033 | 2759 | 3.59 | 1.02 (0.98–1.06) |
| New | 13,018 | 474 | 5.40 | 1.24 (1.13–1.36) | New | 88,680 | 2270 | 3.59 | 1.01 (0.97–1.05) |
| Persistent | 10,075 | 454 | 6.86 | 1.52 (1.38–1.67) | Persistent | 21,875 | 671 | 4.35 | 1.16 (1.07–1.25) |
| p value | < 0.0001 | p value | 0.0023 | ||||||
| eGFR < 60 mL/min/1.73 m2 | eGFR ≥ 60 mL/min/1.73 m2 | ||||||||
| Negative | 314,640 | 8906 | 3.96 | 1 (ref.) | Negative | 5,999,048 | 146,402 | 3.37 | 1 (ref.) |
| trace | 10,782 | 369 | 4.90 | 1.16 (1.05–1.29) | Trace | 118,733 | 2922 | 3.42 | 0.99 (0.95–1.03) |
| 1+ | 11,831 | 432 | 5.37 | 1.22 (1.11–1.35) | 1+ | 76,414 | 1994 | 3.66 | 1.02 (0.98–1.07) |
| 2+ | 7750 | 318 | 6.21 | 1.40 (1.25–1.57) | 2+ | 26,590 | 750 | 3.98 | 1.09 (1.01–1.17) |
| 3+ | 2923 | 148 | 7.95 | 1.76 (1.50–2.08) | 3+ | 6430 | 159 | 3.52 | 0.94 (0.81–1.10) |
| 4+ | 589 | 30 | 8.11 | 1.79 (1.25–2.56) | 4+ | 1121 | 38 | 4.89 | 1.34 (0.98–1.84) |
| p trend | <0.0001 | p trend | 0.0817 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, E.H.; Kim, B.; Song, S.H.; Oh, T.R.; Suh, S.H.; Choi, H.S.; Kim, C.S.; Ma, S.K.; Han, K.-D.; Kim, S.W. Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 2356. https://doi.org/10.3390/jcm10112356
Bae EH, Kim B, Song SH, Oh TR, Suh SH, Choi HS, Kim CS, Ma SK, Han K-D, Kim SW. Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study. Journal of Clinical Medicine. 2021; 10(11):2356. https://doi.org/10.3390/jcm10112356
Chicago/Turabian StyleBae, Eun Hui, Bongseong Kim, Su Hyun Song, Tae Ryom Oh, Sang Heon Suh, Hong Sang Choi, Chang Seong Kim, Seong Kwon Ma, Kyung-Do Han, and Soo Wan Kim. 2021. "Proteinuria and Psoriasis Risk: A Nationwide Population-Based Study" Journal of Clinical Medicine 10, no. 11: 2356. https://doi.org/10.3390/jcm10112356