
High Central Venous Pressure after Cardiac Surgery Might Depict Hemodynamic Deterioration Associated with Increased Morbidity and Mortality

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
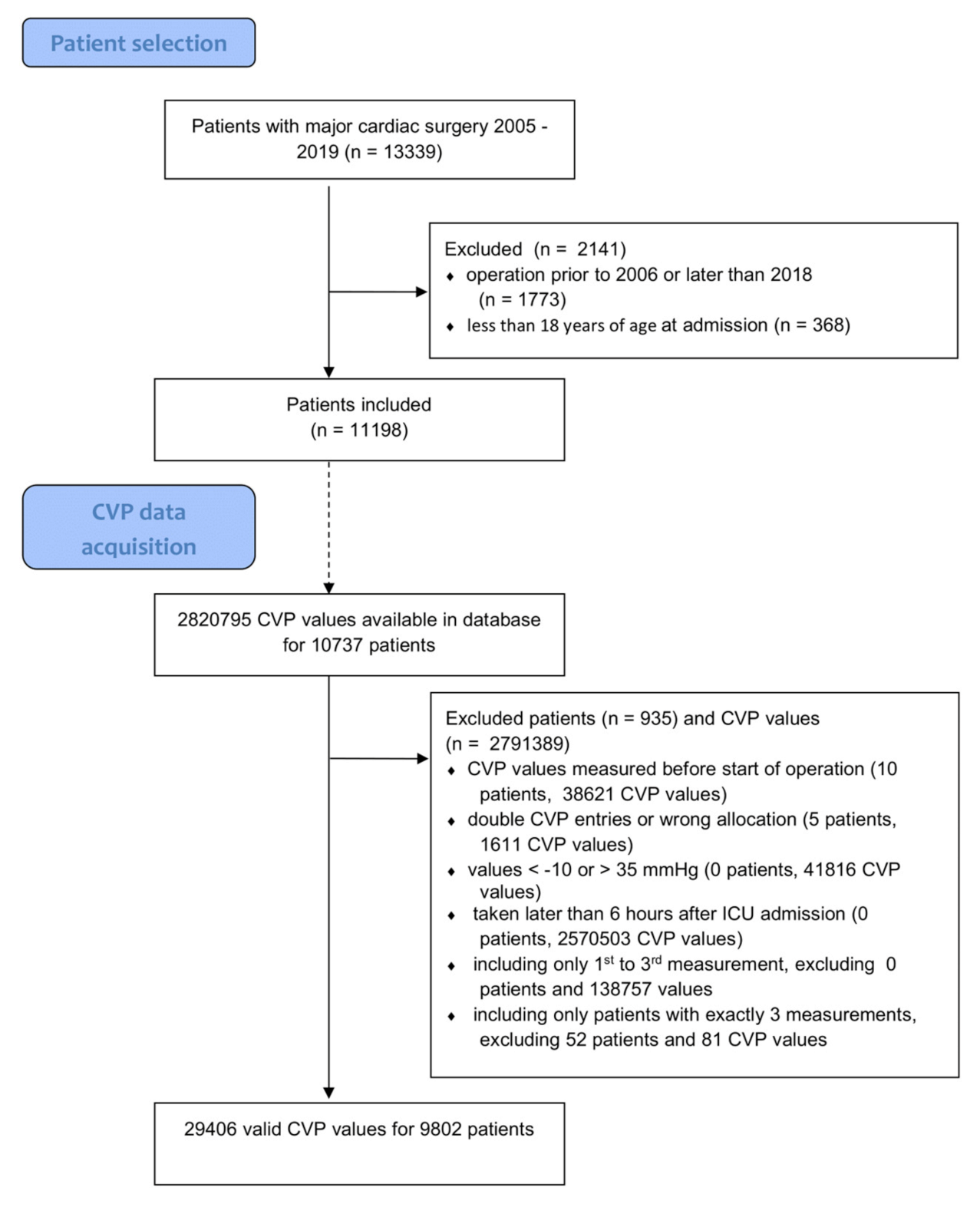
2.1. CVP Measurement and Determining Optimal Cut-Off Value
- CVP measurements <−10 mmHg and >35 mmHg were discarded;
- The first three available CVP values (usually spaced 30 min apart) per case following ICU admission were used to calculate the patient’s median initial CVP (miCVP);
- If fewer than three CVP values were available per case within six hours of ICU admission, this case was not included in analysis
2.2. Statistical Analysis
3. Results
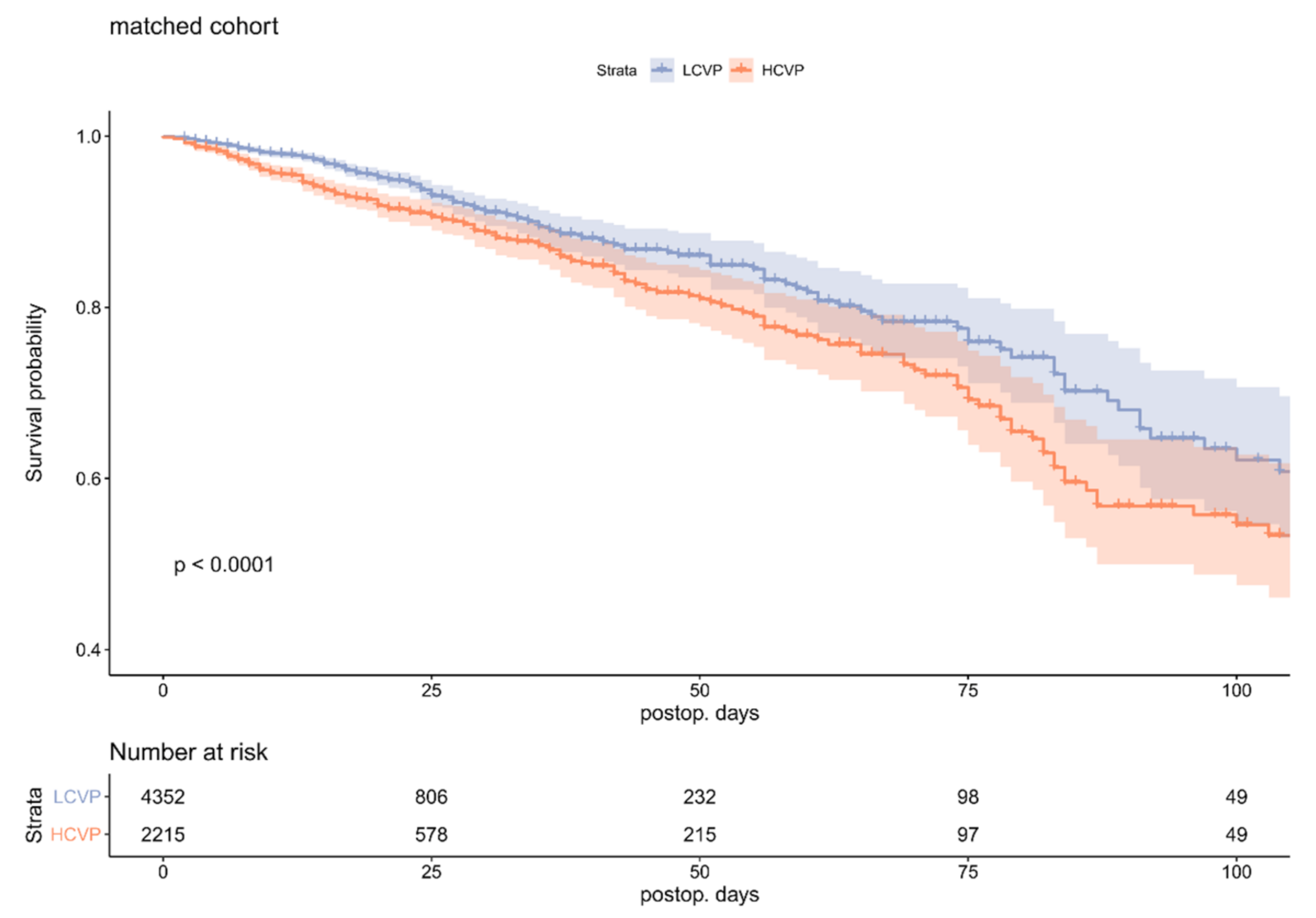
3.1. Survival
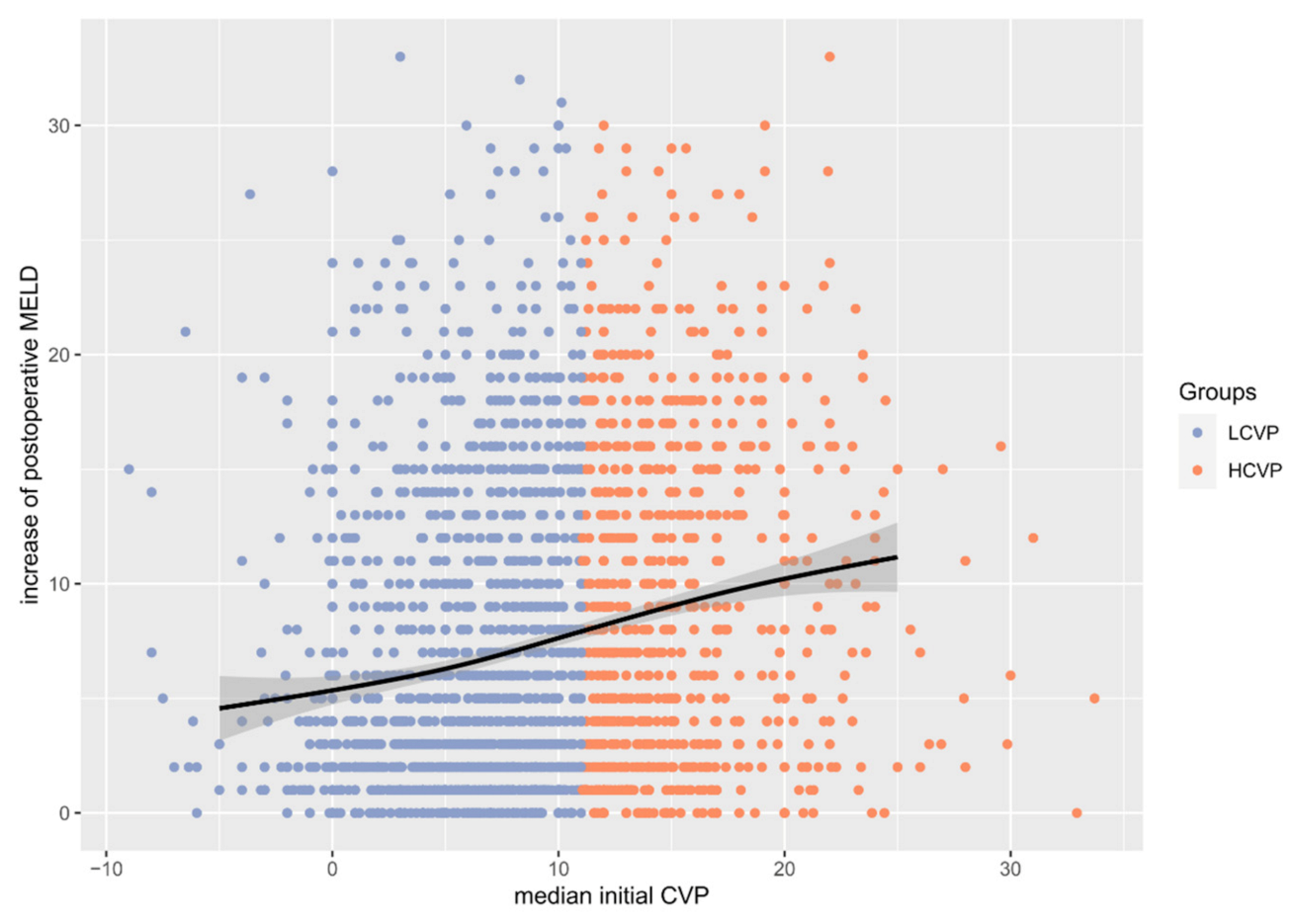
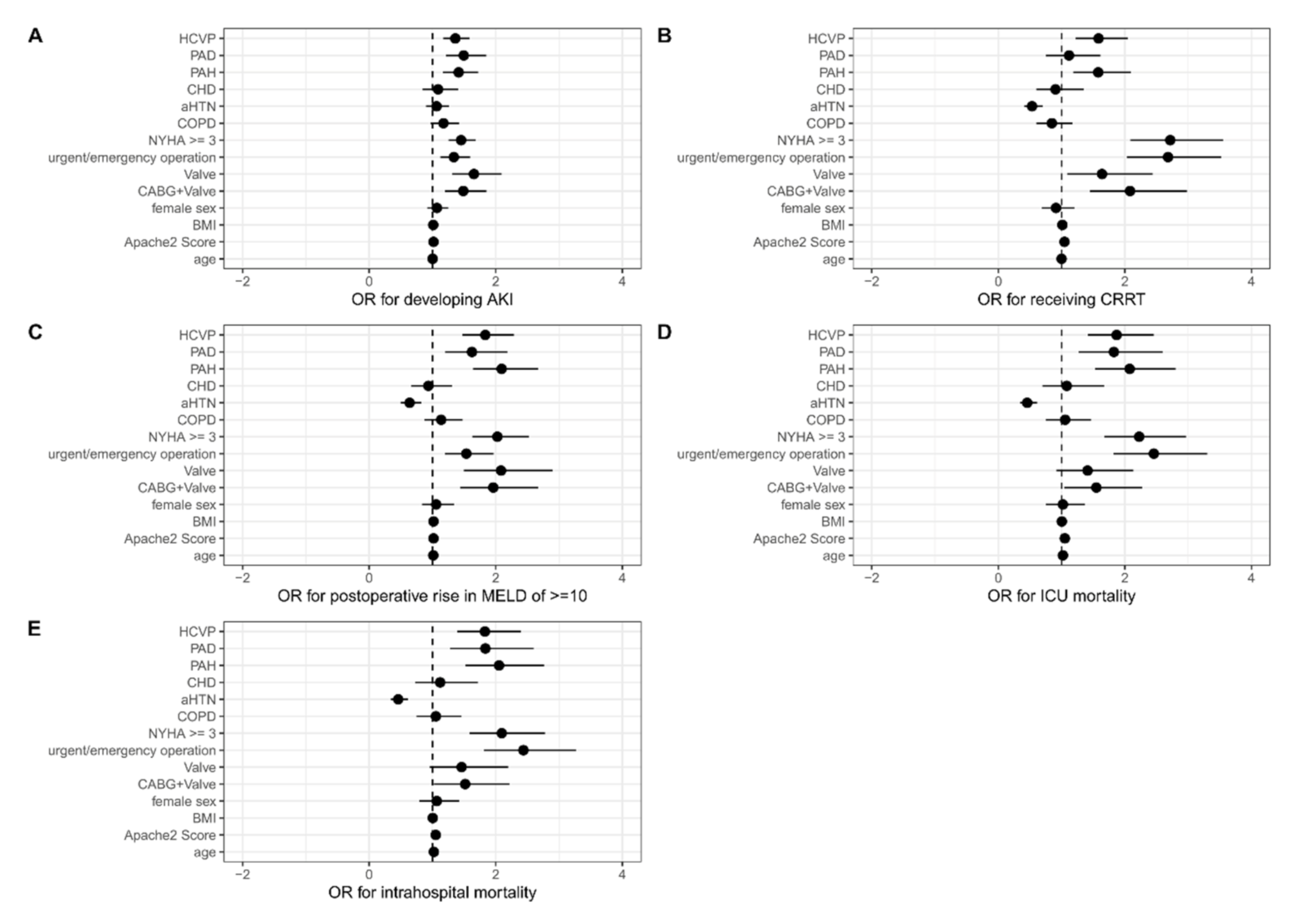
3.2. Outcome Parameters
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rhodes, A.; Moreno, R.P.; Metnitz, B.; Hochrieser, H.; Bauer, P.; Metnitz, P. Epidemiology and outcome following post-surgical admission to critical care. Intensive Care Med. 2011, 37, 1466–1472. [Google Scholar] [CrossRef]
- Ferguson, T.B.; Hammill, B.G.; Peterson, E.D.; DeLong, E.R.; Grover, F.L.; STS National Database Committee. A decade of change--risk profiles and outcomes for isolated coronary artery bypass grafting procedures, 1990–1999: A report from the STS National Database Committee and the Duke Clinical Research Institute. Society of Thoracic Surgeons. Ann. Thorac. Surg. 2002, 73, 480–489, discussion 489–490. [Google Scholar] [CrossRef]
- Landoni, G.; Pisano, A.; Lomivorotov, V.; Alvaro, G.; Hajjar, L.; Paternoster, G.; Neto, C.N.; Latronico, N.; Fominskiy, E.; Pasin, L.; et al. Randomized Evidence for Reduction of Perioperative Mortality: An Updated Consensus Process. J. Cardiothorac. Vasc. Anesth. 2017, 31, 719–730. [Google Scholar] [CrossRef] [Green Version]
- Aya, H.D.; Cecconi, M.; Hamilton, M.; Rhodes, A. Goal-directed therapy in cardiac surgery: A systematic review and meta-analysis. Br. J. Anaesth. 2013, 110, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Aya, H.D.; Rhodes, A.; Ster, I.C.; Fletcher, N.; Grounds, R.M.; Cecconi, M. Hemodynamic Effect of Different Doses of Fluids for a Fluid Challenge: A Quasi-Randomized Controlled Study. Crit. Care Med. 2017, 45, e161–e168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kastrup, M.; Carl, M.; Spies, C.; Sander, M.; Markewitz, A.; Schirmer, U. Clinical impact of the publication of S3 guidelines for intensive care in cardiac surgery patients in Germany: Results from a postal survey. Acta Anaesthesiol. Scand. 2013, 57, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Carl, M.; Alms, A.; Braun, J.; Dongas, A.; Erb, J.; Goetz, A.; Goepfert, M.; Gogarten, W.; Grosse, J.; Heller, A.R.; et al. S3 guidelines for intensive care in cardiac surgery patients: Hemodynamic monitoring and cardiocirculary system. Ger. Med. Sci. 2010, 8, 12. [Google Scholar] [CrossRef]
- Engelman, D.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA Surg. 2019, 154, 755. [Google Scholar] [CrossRef]
- Funcke, S.; Sander, M.; Goepfert, M.S.; Groesdonk, H.; Heringlake, M.; Hirsch, J.; Kluge, S.; Krenn, C.; Maggiorini, M.; Meybohm, P.; et al. Practice of hemodynamic monitoring and management in German, Austrian, Swiss intensive care units: The multicenter cross-sectional ICU-CardioMan Study. Ann. Intensive Care 2016, 6, 49. [Google Scholar] [CrossRef] [Green Version]
- Eskesen, T.G.; Wetterslev, M.; Perner, A. Systematic review including re-analyses of 1148 individual data sets of central venous pressure as a predictor of fluid responsiveness. Intensive Care Med. 2016, 42, 324–332. [Google Scholar] [CrossRef]
- Haddad, F.; Couture, P.; Tousignant, C.; Denault, A.Y. Denault. The right ventricle in cardiac surgery, a perioperative perspective: II. Pathophysiology, clinical importance, management. Anesth. Analg. 2009, 108, 422–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damman, K.; Van Deursen, V.M.; Navis, G.; Voors, A.A.; Van Veldhuisen, D.J.; Hillege, H.L. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J. Am. Coll. Cardiol. 2009, 53, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Damman, K.; Navis, G.; Smilde, T.D.J.; Voors, A.A.; Van Der Bij, W.; Van Veldhuisen, D.J.; Hillege, H.L. Decreased cardiac output, venous congestion and the association with renal impairment in patients with cardiac dysfunction. Eur. J. Heart Fail. 2007, 9, 872–878. [Google Scholar] [CrossRef]
- Habicher, M.; Zajonz, T.; Heringlake, M.; Böning, A.; Treskatsch, S.; Schirmer, U.; Markewitz, A.; Sander, M. S3 guidelines on intensive medical care of cardiac surgery patients: Hemodynamic monitoring and cardiovascular system-an update. Anaesthesist 2018, 67, 375–379. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Vincent, J.-L. Vincent. Should we measure the central venous pressure to guide fluid management? Ten answers to 10 questions. Crit. Care Lond. Engl. 2018, 22, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegler, B.; Bernhard, M.; Brenner, T.; Gerlach, H.; Henrich, M.; Hofer, S.; Kilger, E.; Kruger, W.; Lichtenstern, C.; Mayer, K.; et al. CVP—Farewell? Please don’t!: Comments on the S3 guidelines on “intravascular volume therapy in adults”. Anaesthesist 2015, 64, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balzer, F.; Sander, M.; Simon, M.; Spies, C.; Habicher, M.; Treskatsch, S.; Mezger, V.; Schirmer, U.; Heringlake, M.; Wernecke, K.-D.; et al. High central venous saturation after cardiac surgery is associated with increased organ failure and long-term mortality: An observational cross-sectional study. Crit. Care Lond. Engl. 2015, 19, 168. [Google Scholar] [CrossRef] [Green Version]
- Balzer, F.; Menk, M.; Ziegler, J.; Pille, C.; Wernecke, K.-D.; Spies, C.; Schmidt, M.; Weber-Carstens, S.; Deja, M. Predictors of survival in critically ill patients with acute respiratory distress syndrome (ARDS): An observational study. BMC Anesthesiol. 2016, 16, 108. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet Lond. Engl. 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Endre, Z.H. Acute kidney injury: Definitions and new paradigms. Adv. Chronic Kidney Dis. 2008, 15, 213–221. [Google Scholar] [CrossRef]
- Fluss, R.; Faraggi, D.; Reiser, B. Estimation of the Youden Index and its Associated Cutoff Point. Biom. J. 2005, 47, 458–472. [Google Scholar] [CrossRef] [Green Version]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Ming, K.; Rosenbaum, P.R. Substantial Gains in Bias Reduction from Matching with a Variable Number of Controls. Biometrics 2000, 56, 118–124. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 1 August 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Kassambar, A.; Kosinski, M.; Biecek, P. Survminer: Drawing Survival Curves Using ‘ggplot2’; 2020. Available online: https://CRAN.R-project.org/package=survminer (accessed on 1 August 2021).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: Berlin, Germany, 2000. [Google Scholar] [CrossRef]
- Thiele, C. Cutpointr: Determine and Evaluate Optimal Cutpoints in Binary Classification Tasks; 2020. Available online: https://CRAN.R-project.org/package=cutpointr (accessed on 1 August 2021).
- Ho, D.E.; Imai, K.; King, G.; Stuart, E. Stuart. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Subirana, I.; Sanz, H.; Vila, J. Building Bivariate Tables: The compareGroups Package for R. J. Stat. Softw. 2014, 57, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Shojaee, M.; Sabzghabaei, A.; Alimohammadi, H.; Derakhshanfar, H.; Amini, A.; Esmailzadeh, B. Effect of Positive End-Expiratory Pressure on Central Venous Pressure in Patients under Mechanical Ventilation. Emerg. Tehran Iran 2017, 5, e1. [Google Scholar]
- Hylkema, B.S.; Barkmeijer-Degenhart, P.; van der Mark, T.W.; Peset, R.; Sluiter, H.J. Central venous versus esophageal pressure changes for calculation of lung compliance during mechanical ventilation. Crit. Care Med. 1983, 11, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Walling, P.T.; Savege, M.T. A comparison of oesophageal and central venous pressures in the measurement of transpulmonary pressure change. Br. J. Anaesth. 1976, 48, 475–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Zhu, Z.; Zhao, C.; Guo, Y.; Chen, D.; Wei, Y.; Jin, J. Central venous pressure measurement is associated with improved outcomes in septic patients: An analysis of the MIMIC-III database. Crit. Care 2020, 24, 433. [Google Scholar] [CrossRef]
- Williams, J.B.; Peterson, E.D.; Wojdyla, D.; Harskamp, R.; Southerland, K.W.; Ferguson, T.B.; Smith, P.K.; Milano, C.A.; Lopes, R.D. Central venous pressure after coronary artery bypass surgery: Does it predict postoperative mortality or renal failure? J. Crit. Care 2014, 29, 1006–1010. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Delgado, J.C.; Esteve, F.; Javierre, C.; Perez, X.; Torrado, H.; Carrio, M.L.; Rodríguez-Castro, D.; Farrero, E.; Ventura, J.L. Short-term independent mortality risk factors in patients with cirrhosis undergoing cardiac surgery. Interact. Cardiovasc. Thorac. Surg. 2013, 16, 332–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.-K.; Wang, X.-T.; Liu, D.-W. Association between elevated central venous pressure and outcomes in critically ill patients. Ann. Intensive Care 2017, 7, 83. [Google Scholar] [CrossRef] [Green Version]
- Guyton, A.C. Determination of cardiac output by equating venous return curves with cardiac response curves. Physiol. Rev. 1955, 35, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Funk, D.J.; Jacobsohn, E.; Kumar, A. The role of venous return in critical illness and shock-part I: Physiology. Crit. Care Med. 2013, 41, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Marik, P.E. Iatrogenic salt water drowning and the hazards of a high central venous pressure. Ann. Intensive Care 2014, 4, 21. [Google Scholar] [CrossRef] [Green Version]
- Komuro, K.; Seo, Y.; Yamamoto, M.; Sai, S.; Ishizu, T.; Shimazu, K.; Takahashi, Y.; Imagawa, S.; Anzai, T.; Yonezawa, K.; et al. Assessment of renal perfusion impairment in a rat model of acute renal congestion using contrast-enhanced ultrasonography. Heart Vessels 2018, 33, 434–440. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, I.; Gaudino, M.; Ronco, C.; Lau, C.; Ivascu, N.; Girardi, L.N. Congestive kidney failure in cardiac surgery: The relationship between central venous pressure and acute kidney injury. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 800–805. [Google Scholar] [CrossRef] [Green Version]
- Burban, M.; Hamel, J.-F.; Tabka, M.; De La Bourdonnaye, M.; Duveau, A.; Mercat, A.; Calès, P.; Asfar, P.; Lerolle, N. Renal macro- and microcirculation autoregulatory capacity during early sepsis and norepinephrine infusion in rats. Crit. Care Lond. Engl. 2013, 17, R139. [Google Scholar] [CrossRef] [Green Version]
- Vellinga, N.A.; Ince, C.; Boerma, E.C. Elevated central venous pressure is associated with impairment of microcirculatory blood flow in sepsis: A hypothesis generating post hoc analysis. BMC Anesthesiol. 2013, 13, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Marx, G.; Schindler, A.W.; Mosch, C.; Albers, J.; Bauer, M.; Gnass, I.; Hobohm, C.; Janssens, U.; Kluge, S.; Kranke, P.; et al. Intravascular volume therapy in adults: Guidelines from the Association of the Scientific Medical Societies in Germany. Eur. J. Anaesthesiol. 2016, 33, 488–521. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (ALL) | LCVP | HCVP | p.Overall | N | |
|---|---|---|---|---|---|
| n = 6567 | n = 4352 | n = 2215 | |||
| Age * | 70.0 (62.0, 76.0) | 70.0 (62.0, 76.0) | 69.0 (62.0, 76.0) | 0.907 | 6567 |
| Sex *: | 0.309 | 6567 | |||
| M | 4620 (70.4%) | 3080 (70.8%) | 1540 (69.5%) | ||
| W | 1947 (29.6%) | 1272 (29.2%) | 675 (30.5%) | ||
| BMI | 27.2 (24.2, 30.8) | 26.8 (24.0, 30.2) | 28.0 (24.9, 31.9) | <0.001 | 3970 |
| Operation *: | 0.536 | 6567 | |||
| CABG | 3439 (52.4%) | 2297 (52.8%) | 1142 (51.6%) | ||
| CABG + Valve | 881 (13.4%) | 586 (13.5%) | 295 (13.3%) | ||
| Valve | 2247 (34.2%) | 1469 (33.8%) | 778 (35.1%) | ||
| Urgency *: | 0.342 | 6567 | |||
| elective | 5163 (78.6%) | 3437 (79.0%) | 1726 (77.9%) | ||
|
urgent/ emergency | 1404 (21.4%) | 915 (21.0%) | 489 (22.1%) | ||
| ASA: | 0.203 | 5577 | |||
| 1–2 | 184 (3.30%) | 132 (3.53%) | 52 (2.84%) | ||
| 3–5 | 5393 (96.7%) | 3612 (96.5%) | 1781 (97.2%) | ||
| Apache2 * | 19.0 (14.0;25.0) | 19.0 (14.0;25.0) | 19.0 (14.0;25.0) | 0.483 | 6567 |
| CCI * | 5.00 (3.00;7.00) | 5.00 (3.00;7.00) | 5.00 (3.00;7.00) | 0.269 | 6567 |
| CAD * | 5071 (77.2%) | 3368 (77.4%) | 1703 (76.9%) | 0.667 | 6567 |
| PAD * | 894 (13.6%) | 589 (13.5%) | 305 (13.8%) | 0.822 | 6567 |
| aHTN * | 5278 (80.4%) | 3497 (80.4%) | 1781 (80.4%) | 0.986 | 6567 |
| NYHA >= 3 * | 2286 (34.8%) | 1498 (34.4%) | 788 (35.6%) | 0.367 | 6567 |
| PAH * | 1098 (16.7%) | 715 (16.4%) | 383 (17.3%) | 0.395 | 6567 |
| COPD * | 1108 (16.9%) | 724 (16.6%) | 384 (17.3%) | 0.495 | 6567 |
| Diabetes * | 3365 (51.2%) | 2221 (51.0%) | 1144 (51.6%) | 0.657 | 6567 |
| CRI * | 1922 (29.3%) | 1259 (28.9%) | 663 (29.9%) | 0.415 | 6567 |
| (ALL) | LCVP | HCVP | p.Overall | N | |
|---|---|---|---|---|---|
| N = 6567 | n = 4352 | n = 2215 | |||
| ΔMELD >= 10 | 848 (31.0%) | 467 (26.1%) | 381 (40.3%) | <0.001 | 2733 |
| AKI | 4335 (66.0%) | 2793 (64.2%) | 1542 (69.6%) | <0.001 | 6567 |
| CRRT | 467 (7.11%) | 246 (5.65%) | 221 (9.98%) | <0.001 | 6567 |
| LOS (d) | 13.0 (9.00;22.0) | 13.0 (9.00;21.0) | 14.0 (9.00;25.0) | <0.001 | 6567 |
| LOS2 (d) | 13.0 (9.00;21.0) | 13.0 (9.00;20.0) | 14.0 (9.00;24.0) | <0.001 | 6114 |
| In-hospital mortality | 453 (6.90%) | 228 (5.24%) | 225 (10.2%) | <0.001 | 6567 |
| ICU mortality | 438 (6.67%) | 217 (4.99%) | 221 (9.98%) | <0.001 | 6567 |
| ICU LOS (d) | 7.00 (4.00;13.0) | 7.00 (4.00;12.0) | 7.00 (4.00;15.0) | 0.001 | 6567 |
| ICU LOS2 (d) | 7.00 (4.00;12.0) | 7.00 (4.00;12.0) | 7.00 (4.00;14.0) | 0.008 | 6114 |
| Ventilation (h) | 17.0 (10.0;39.0) | 16.0 (10.0;33.0( | 20.0 (10.0;56.5) | <0.001 | 6567 |
| Ventilation2 (h) | 16.0 (10.0;32.0) | 16.0 (10.0;29.0) | 18.0 (10.0;40.0) | <0.001 | 6114 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schiefenhövel, F.; Trauzeddel, R.F.; Sander, M.; Heringlake, M.; Groesdonk, H.V.; Grubitzsch, H.; Kruppa, J.; Berger, C.; Treskatsch, S.; Balzer, F. High Central Venous Pressure after Cardiac Surgery Might Depict Hemodynamic Deterioration Associated with Increased Morbidity and Mortality. J. Clin. Med. 2021, 10, 3945. https://doi.org/10.3390/jcm10173945
Schiefenhövel F, Trauzeddel RF, Sander M, Heringlake M, Groesdonk HV, Grubitzsch H, Kruppa J, Berger C, Treskatsch S, Balzer F. High Central Venous Pressure after Cardiac Surgery Might Depict Hemodynamic Deterioration Associated with Increased Morbidity and Mortality. Journal of Clinical Medicine. 2021; 10(17):3945. https://doi.org/10.3390/jcm10173945
Chicago/Turabian StyleSchiefenhövel, Fridtjof, Ralf F. Trauzeddel, Michael Sander, Matthias Heringlake, Heinrich V. Groesdonk, Herko Grubitzsch, Jochen Kruppa, Christian Berger, Sascha Treskatsch, and Felix Balzer. 2021. "High Central Venous Pressure after Cardiac Surgery Might Depict Hemodynamic Deterioration Associated with Increased Morbidity and Mortality" Journal of Clinical Medicine 10, no. 17: 3945. https://doi.org/10.3390/jcm10173945