
Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
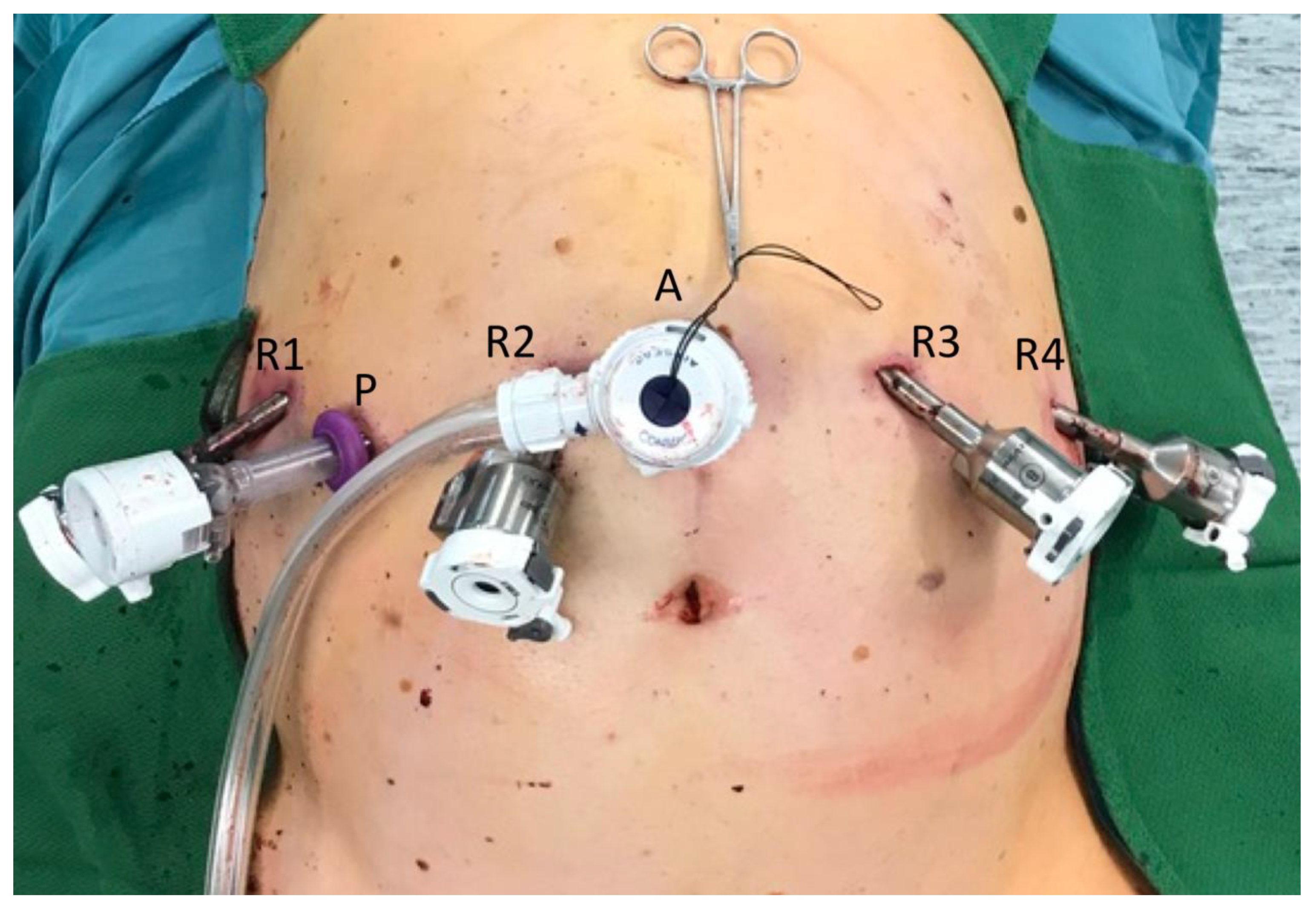
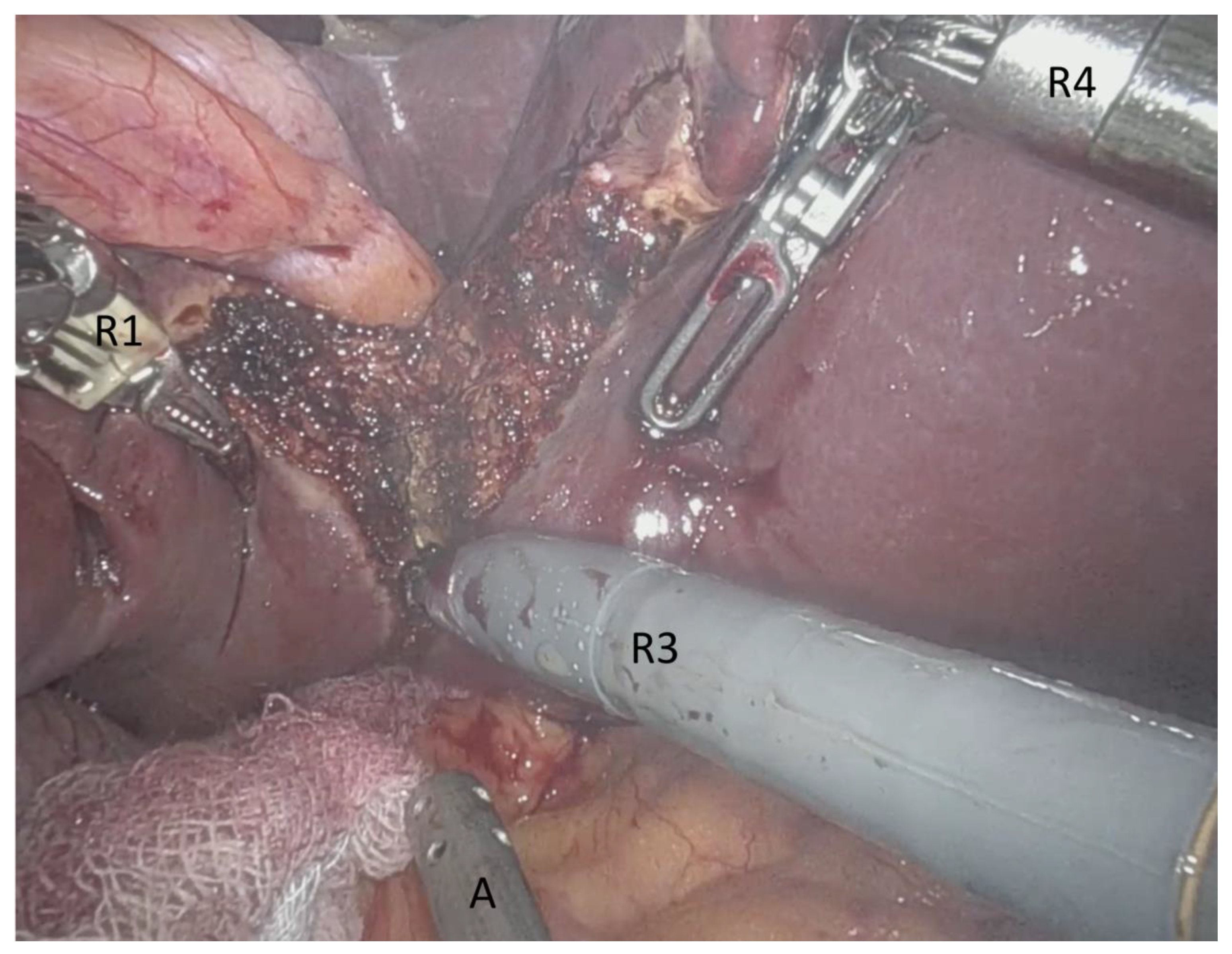
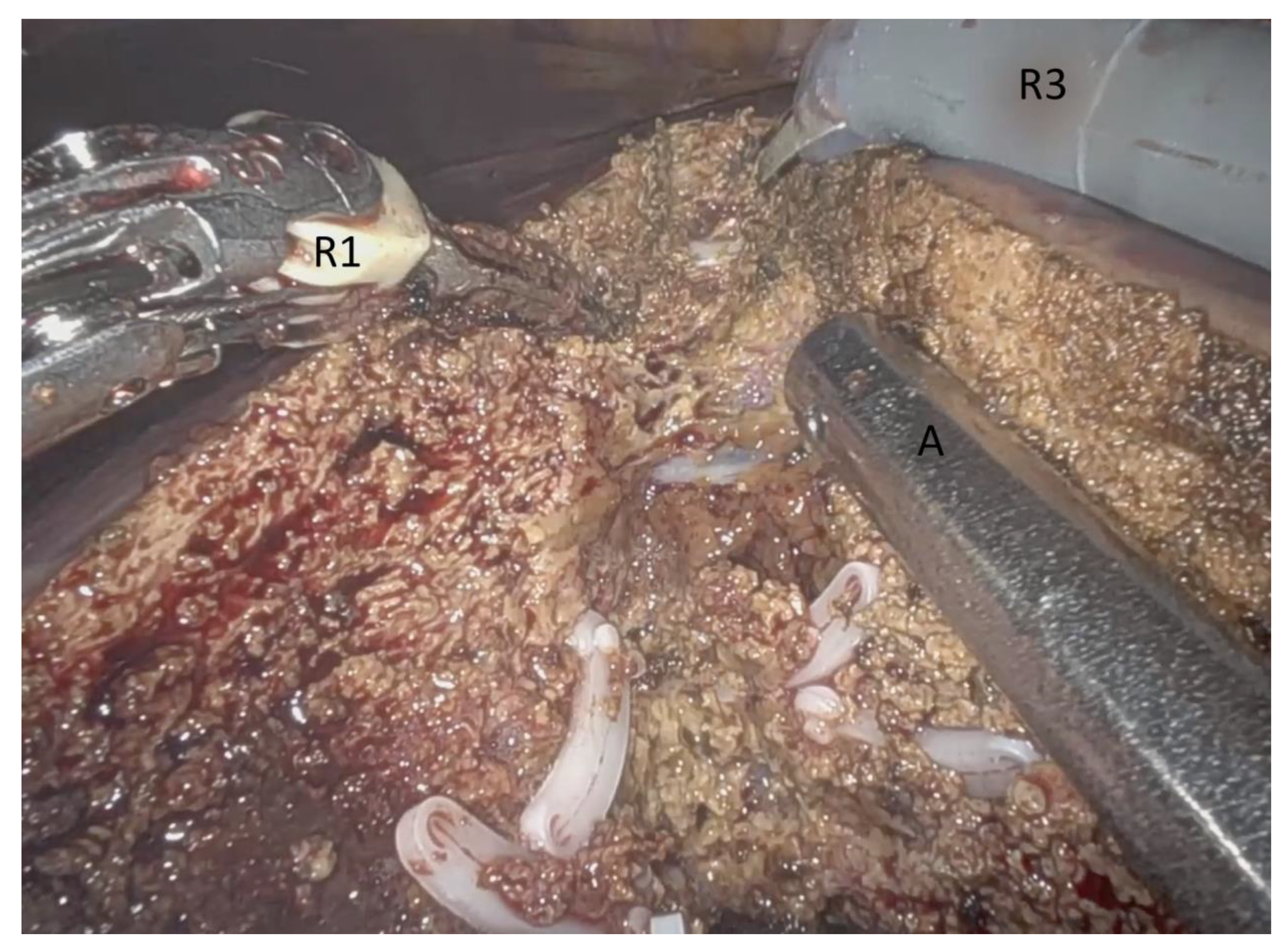
2.2. Robotic-Assisted Liver Resection Using the Three Device (3D) Technique
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Perioperative Outcomes
3.2. Histopathology and Resection Margins
3.3. Comparison of Major and Minor Robotic Liver Resections
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buell, J.F.; Cherqui, D.; Geller, D.A.; O’Rourke, N.; Iannitti, D.; Dagher, I.; Koffron, A.J.; Thomas, M.; Gayet, B.; Han, H.S.; et al. The international position on laparoscopic liver surgery: The Louisville Statement, 2008. Ann. Surg. 2009, 250, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Gigot, J.-F.; Glineur, D.; Azagra, J.S.; Goergen, M.; Ceuterick, M.; Morino, M.; Etienne, J.; Marescaux, J.; Mutter, D.; van Krunckelsven, L.; et al. Laparoscopic liver resection for malignant liver tumors: Preliminary results of a multicenter European study. Ann. Surg. 2002, 236, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belli, G.; Gayet, B.; Han, H.S.; Wakabayashi, G.; Kim, K.H.; Cannon, R.; Kaneko, H.; Gamblin, T.; Koffron, A.; Dagher, I.; et al. Laparoscopic left hemihepatectomy a consideration for acceptance as standard of care. Surg. Endosc. 2013, 27, 2721–2726. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, G.; Cherqui, D.; Geller, D.A.; Buell, J.F.; Kaneko, H.; Han, H.S.; Asbun, H.; O’Rourke, N.; Tanabe, M.; Koffron, A.J.; et al. Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in Morioka. Ann. Surg. 2015, 261, 619–629. [Google Scholar]
- Choi, G.H.; Chong, J.U.; Han, D.H.; Choi, J.S.; Lee, W.J. Robotic hepatectomy: The Korean experience and perspective. Hepatobiliary Surg. Nutr. 2017, 6, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Gayet, B.; Cavaliere, D.; Vibert, E.; Perniceni, T.; Levard, H.; Denet, C.; Christidis, C.; Blain, A.; Mal, F. Totally laparoscopic right hepatectomy. Am. J. Surg. 2007, 194, 685–689. [Google Scholar] [CrossRef]
- Ishizawa, T.; Gumbs, A.A.; Kokudo, N.; Gayet, B. Laparoscopic segmentectomy of the liver: From segment I to VIII. Ann. Surg. 2012, 256, 959–964. [Google Scholar] [CrossRef]
- Gumbs, A.A.; Gayet, B. Totally laparoscopic left hepatectomy. Surg. Endosc. 2007, 21, 1221. [Google Scholar] [CrossRef] [PubMed]
- Gumbs, A.A.; Gayet, B. Totally laparoscopic central hepatectomy. J. Gastrointest. Surg. 2008, 12, 1153. [Google Scholar] [CrossRef]
- Croner, R.S.; Perrakis, A.; Brunner, M.; Matzel, K.E.; Hohenberger, W. Pioneering robotic liver surgery in Germany: First experiences with liver malignancies. Front. Surg. 2015, 2, 18. [Google Scholar] [CrossRef] [Green Version]
- Croner, R.S.; Perrakis, A.; Hohenberger, W.; Brunner, M. Robotic liver surgery for minor hepatic resections: A comparison with laparoscopic and open standard procedures. Langenbeck Arch. Surg. 2016, 401, 707–714. [Google Scholar] [CrossRef]
- Chen, P.D.; Wu, C.-Y.; Hu, R.-H.; Chen, C.-N.; Yuan, R.-H.; Liang, J.-T.; Lai, H.-S.; Wu, Y.-M. Robotic major hepatectomy: Is there a learning curve? Surgery 2017, 161, 642–649. [Google Scholar] [CrossRef]
- Liu, R.; Wakabayashi, G.; Kim, H.; Choi, G.; Yiengpruksawan, A.; Fong, Y.; He, J.; Boggi, U.; Troisi, R.I.; Efanov, M.; et al. International consensus statement on robotic hepatectomy surgery in 2018. World J. Gastroenterol. 2019, 25, 1432–1444. [Google Scholar] [CrossRef]
- Wu, C.Y.; Chen, P.D.; Lee, C.Y.; Liang, J.T.; Wu, Y.M. Robotic-assisted right posterior segmentectomies for liver lesions: Single-center experience of an evolutional method in left semi-lateral position. J. Robot. Surg. 2019, 13, 231–237. [Google Scholar] [CrossRef]
- Wong, D.J.; Wong, M.J.; Choi, G.H.; Wu, Y.M.; Lai, P.B.; Goh, B.K.P. Systematic review and meta-analysis of robotic versus open hepatectomy. ANZ J. Surg. 2019, 89, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Goh, B.K.P.; Lee, L.S.; Lee, S.Y.; Chow, P.K.H.; Chan, C.Y.; Chiow, A.K.H. Initial experience with robotic hepatectomy in Singapore: Analysis of 48 resections in 43 consecutive patients. ANZ J. Surg. 2019, 89, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.D.; Wu, C.Y.; Hu, R.H.; Chou, W.H.; Lai, H.S.; Liang, J.T.; Lee, P.H.; Wu, Y.M. Robotic Versus Open Hepatectomy for Hepatocellular Carcinoma: A Matched Comparison. Ann. Surg. Oncol. 2017, 24, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Daskalaki, D.; Gonzalez-Heredia, R.; Brown, M.; Bianco, F.M.; Tzvetanov, I.; Davis, M.; Kim, J.; Benedetti, E.; Giulianotti, P.C. Financial Impact of the Robotic Approach in Liver Surgery: A Comparative Study of Clinical Outcomes and Costs Between the Robotic and Open Technique in a Single Institution. J. Laparoendosc. Adv. Surg. Tech. A 2017, 27, 375–382. [Google Scholar] [CrossRef]
- Kingham, T.P.; Leung, U.; Kuk, D.; Gönen, M.; D’Angelica, M.I.; Allen, P.J.; DeMatteo, R.P.; Laudone, V.P.; Jarnagin, W.R.; Fong, Y. Robotic Liver Resection: A Case-Matched Comparison. World J. Surg. 2016, 40, 1422–1428. [Google Scholar] [CrossRef] [Green Version]
- Montalti, R.; Scuderi, V.; Patriti, A.; Vivarelli, M.; Troisi, R.I. Robotic versus laparoscopic resections of posterosuperior segments of the liver: A propensity score-matched comparison. Surg. Endosc. 2016, 30, 1004–1013. [Google Scholar] [CrossRef]
- Lai, E.C.; Tang, C.N. Long-term Survival Analysis of Robotic Versus Conventional Laparoscopic Hepatectomy for Hepatocellular Carcinoma: A Comparative Study. Surg. Laparosc. Endosc. Percutan Tech. 2016, 26, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Jackson, N.R.; Hauch, A.; Hu, T.; Buell, J.F.; Slakey, D.P.; Kandil, E. The safety and efficacy of approaches to liver resection: A meta-analysis. JSLS 2015, 19, e2014.00186. [Google Scholar] [CrossRef] [Green Version]
- Di Benedetto, F.; Magistri, P.; Halazun, K.J. Use of robotics in liver donor right hepatectomy. Hepatobiliary Surg. Nutr. 2018, 7, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Giulianotti, P.C.; Sbrana, F.; Coratti, A.; Bianco, F.M.; Addeo, P.; Buchs, N.C.; Ayloo, S.M.; Benedetti, E. Totally robotic right hepatectomy: Surgical technique and outcomes. Arch. Surg. 2011, 146, 844–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.K., IV; Gao, F.; Strasberg, S.M. Perceived complexity of various liver resections: Results of a survey of experts with development of a complexity score and classification. J. Am. Coll Surg. 2015, 220, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Lai, E.C.; Tang, C.N.; Li, M.K. Robot-assisted laparoscopic hemi-hepatectomy: Technique and surgical outcomes. Int. J. Surg. 2012, 10, 11–15. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients; n (SD or Percent) | ||
|---|---|---|
| Total | 28 (100.0) | |
| Sex | male | 14 (50.0) |
| female | 14 (50.0) | |
| Age; years | 65.3 (11.1) | |
| Operation time; min | 307.6 (98.4) | |
| LOS; days | 13.3 (11.1) | |
| IBL; mL | 358.9 (369.0) | |
| Liver surgery-related morbidity | 3 (10.7) | |
| Previous abdominal surgery | 16 (57.1) | |
| Dignity of the lesion | malignant | 21 (75.0) |
| benign | 7 (25.0) | |
| R0-resection | 21 (100.0) | |
| Major liver resections | 12 (42.9) | |
| Minor liver resections | 16 (57.1) |
| n (%) | ||
|---|---|---|
| Type of liver resection | ||
| Right hemihepatectomy | 6 (21.4) | |
| Left hemihepatectomy | 4 (14.3) | |
| Left lateral liver resection | 6 (21.4) | |
| Bisegmentectomy | 4 (14.3) | |
| Anatomical one segment resection | 4 (14.3) | |
| Resection of three segments | 2 (7.1) | |
| Atypical two segment resection | 1 (3.6) | |
| Atypical one segment resection | 1 (3.6) | |
| Total | 28 (100.0) |
| Type of Liver Lesion | n (%) | |
|---|---|---|
| Malignant lesions | ||
| Colorectal liver metastases | 9 (32.1) | |
| HCC | 7 (25.0) | |
| CCA | 4 (14.3) | |
| HCC + CCA | 1 (3.6) | |
| Benign lesions | ||
| Liver hemangioma | 3 (10.7) | |
| Hepatic adenoma | 2 (7.1) | |
| Inflammatory tumor | 1 (3.6) | |
| Bile duct anomaly | 1 (3.6) | |
| Total | 28 (100.0) |
| Major Resections n (% or SD) | Minor Resections n (% or SD) | p-Value | |
|---|---|---|---|
| Total | 12 (42.9) | 16 (57.1) | |
| Operation time; min | 381.7 (80.6) | 252.0 (70.4) | <0.01 |
| LOS; days | 15.8 (11.6) | 11.3 (10.7) | 0.159 |
| IBL; mL | 495.8 (508.8) | 256.3 (170.2) | 0.090 |
| Liver surgery related morbidity | 3 (25.0) | 0 (0.0) | 0.067 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrakis, A.; Rahimli, M.; Gumbs, A.A.; Negrini, V.; Andric, M.; Stockheim, J.; Wex, C.; Lorenz, E.; Arend, J.; Franz, M.; et al. Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery. J. Clin. Med. 2021, 10, 5265. https://doi.org/10.3390/jcm10225265
Perrakis A, Rahimli M, Gumbs AA, Negrini V, Andric M, Stockheim J, Wex C, Lorenz E, Arend J, Franz M, et al. Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery. Journal of Clinical Medicine. 2021; 10(22):5265. https://doi.org/10.3390/jcm10225265
Chicago/Turabian StylePerrakis, Aristotelis, Mirhasan Rahimli, Andrew A. Gumbs, Victor Negrini, Mihailo Andric, Jessica Stockheim, Cora Wex, Eric Lorenz, Joerg Arend, Mareike Franz, and et al. 2021. "Three-Device (3D) Technique for Liver Parenchyma Dissection in Robotic Liver Surgery" Journal of Clinical Medicine 10, no. 22: 5265. https://doi.org/10.3390/jcm10225265