
Retinal Changes before and after Silicone Oil Removal in Eyes with Rhegmatogenous Retinal Detachment Using Swept-Source Optical Coherence Tomography


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Examination Procedures
2.3. Statistical Analyses
3. Results
3.1. Demographic Data
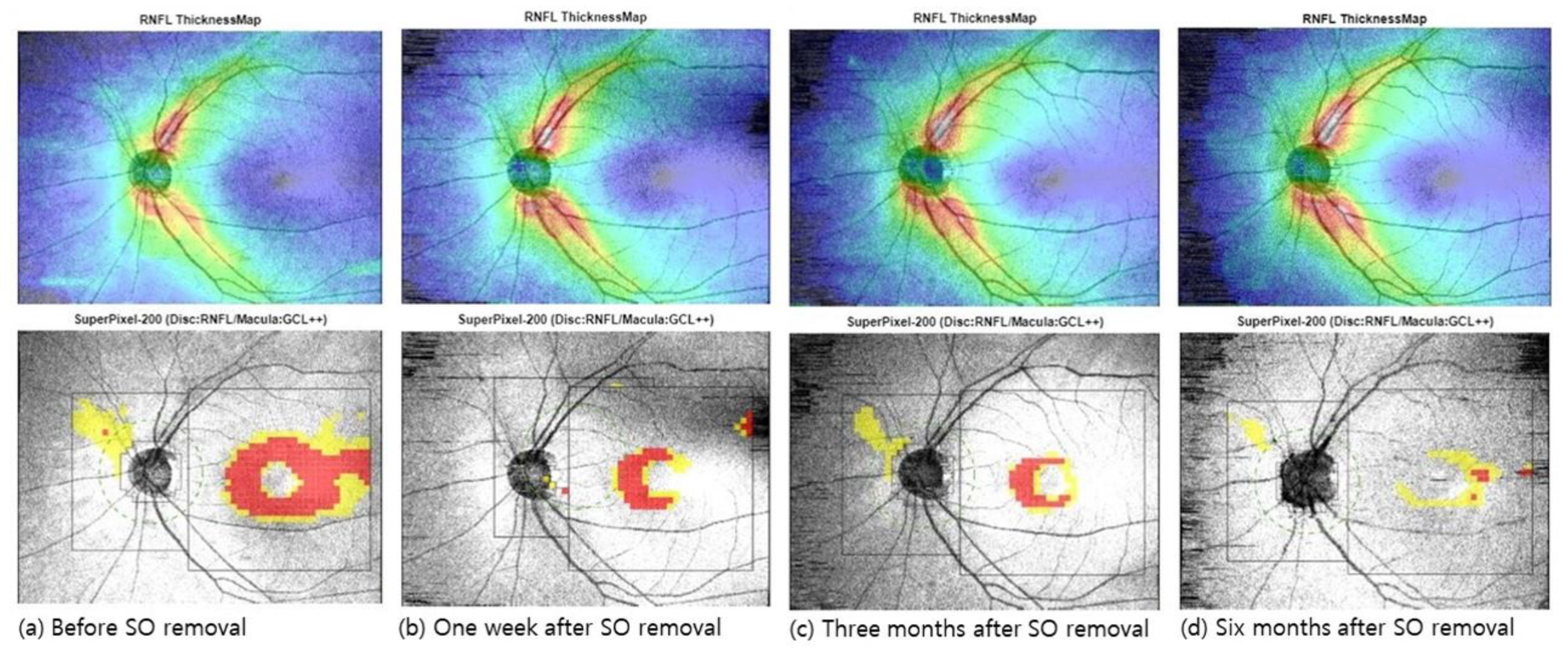
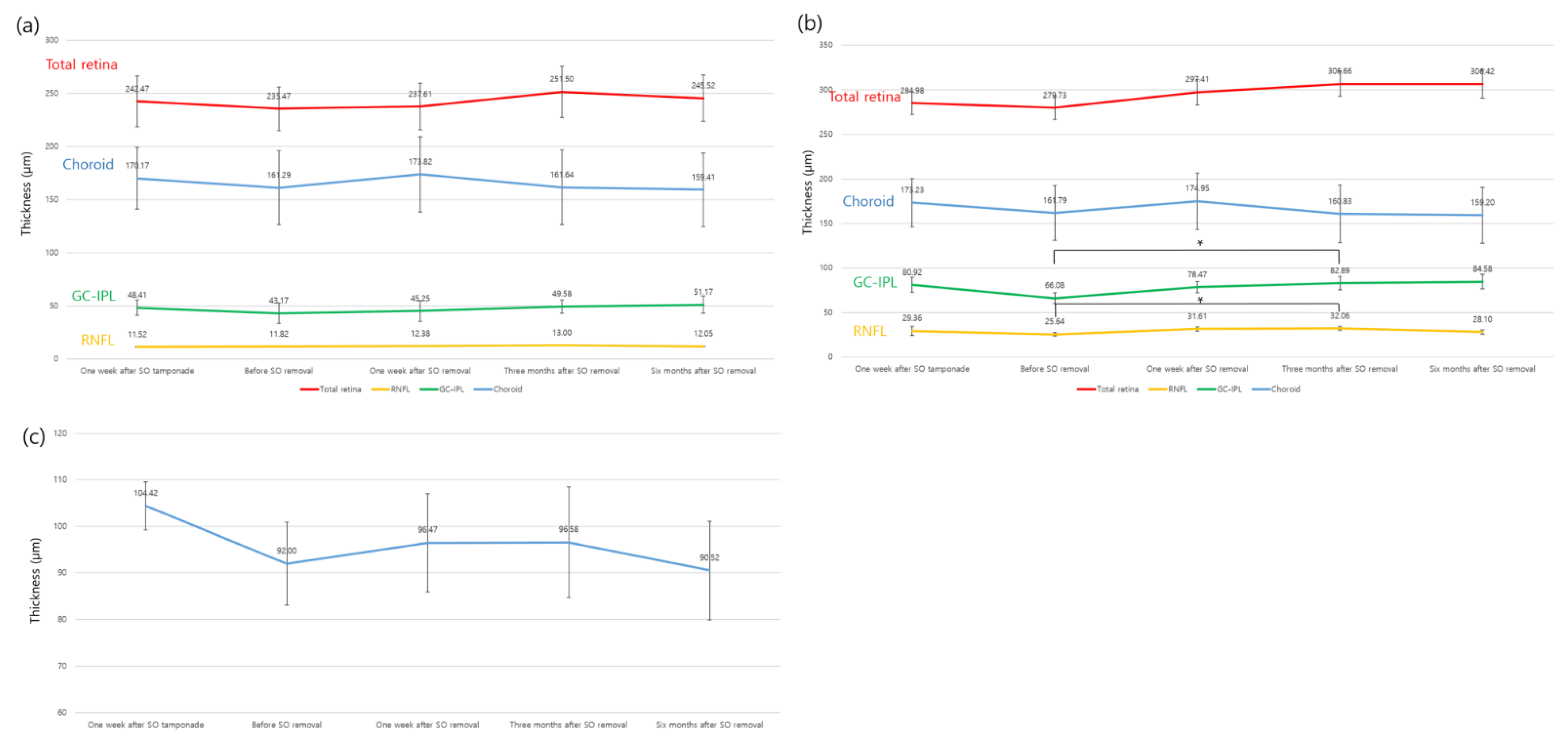
3.2. Changes in Retinal, Choroidal, and Peripapillary Thickness after SO Removal
3.3. Correlation between Visual Acuity and Thickness Changes
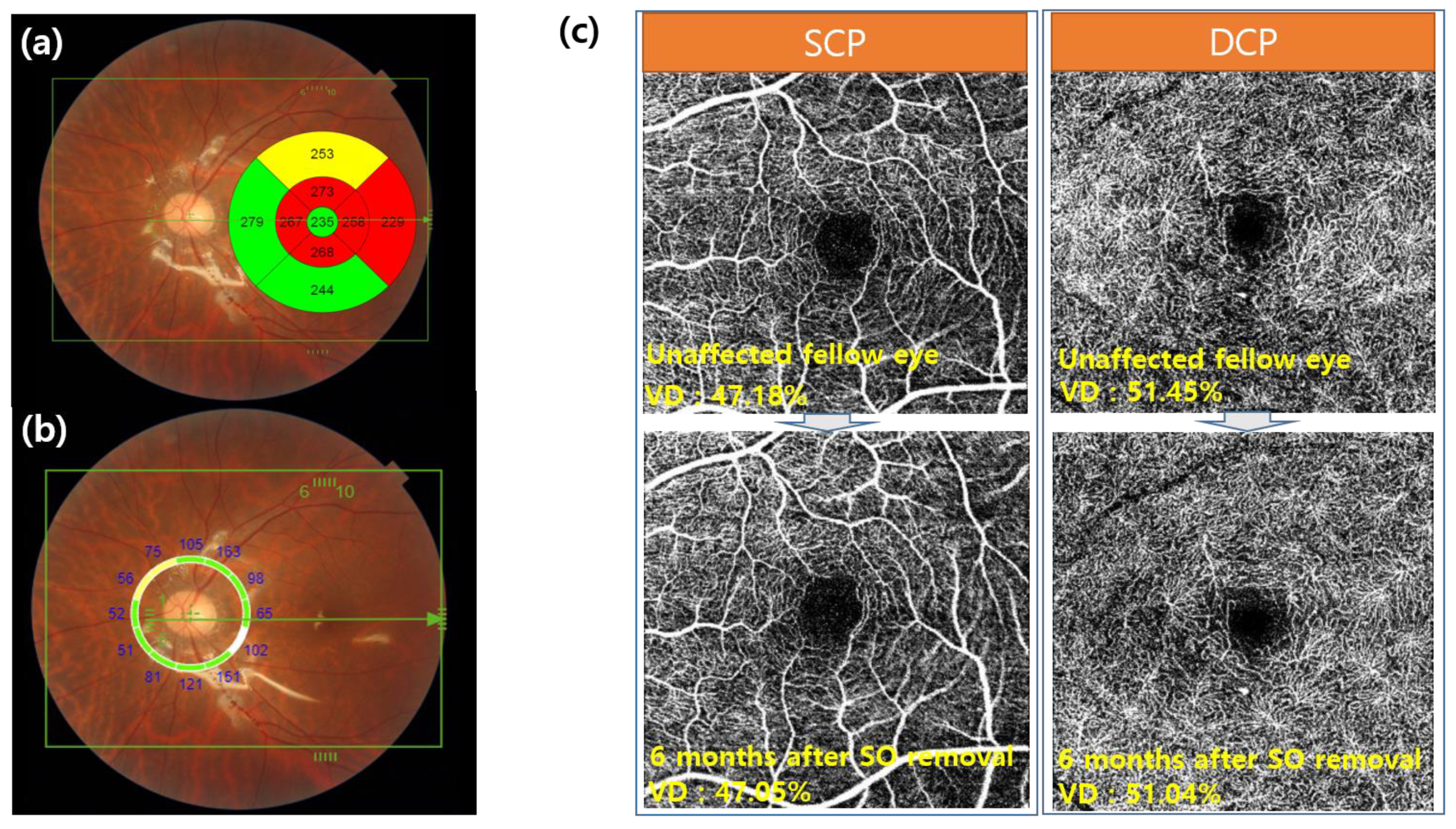
3.4. Changes of the VD on OCTA
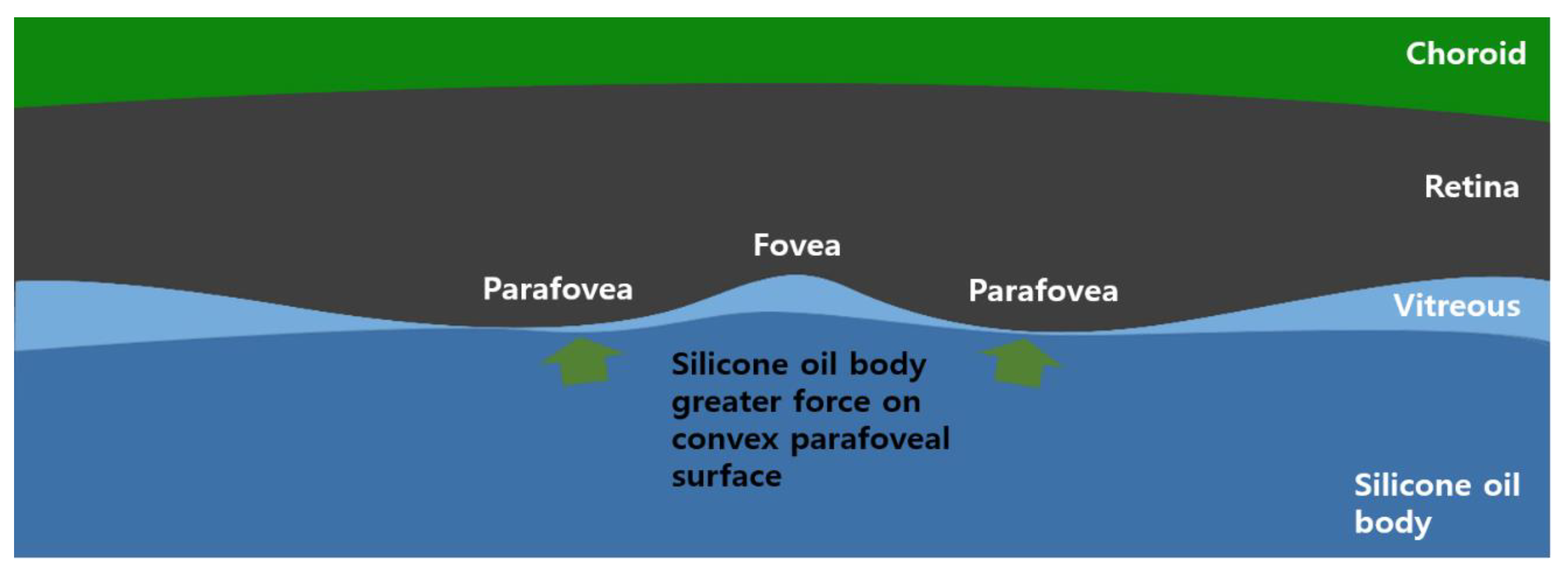
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zoric Geber, M.; Bencic, G.; Vatavuk, Z.; Ivekovic, R.; Friberg, T.R. Retinal nerve fibre layer thickness measurements after successful retinal detachment repair with silicone oil endotamponade. Br. J. Ophthalmol. 2015, 99, 853–858. [Google Scholar] [CrossRef]
- Christensen, U.C.; la Cour, M. Visual loss after use of intraocular silicone oil associated with thinning of inner retinal layers. Acta Ophthalmol. 2012, 90, 733–737. [Google Scholar] [CrossRef]
- Takkar, B.; Azad, R.; Kamble, N.; Azad, S. Retinal Nerve Fiber Layer Changes Following Primary Retinal Detachment Repair with Silicone Oil Tamponade and Subsequent Oil Removal. J. Ophthalmic Vis. Res. 2018, 13, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Purtskhvanidze, K.; Hillenkamp, J.; Tode, J.; Junge, O.; Hedderich, J.; Roider, J.; Treumer, F. Thinning of Inner Retinal Layers after Vitrectomy with Silicone Oil versus Gas Endotamponade in Eyes with Macula-Off Retinal Detachment. Ophthalmologica 2017, 238, 124–132. [Google Scholar] [CrossRef]
- Lee, S.H.; Han, J.W.; Byeon, S.H.; Kim, S.S.; Koh, H.J.; Lee, S.C.; Kim, M. Retinal Layer Segmentation after Silicone Oil or Gas Tamponade for Macula-on Retinal Detachment Using Optical Coherence Tomography. Retina 2018, 38, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Song, I.S.; Lee, J.H.; Shin, Y.U.; Lim, H.W.; Lee, W.J.; Lee, B.R. Macular Choroidal Thickness and Volume Measured by Swept-source Optical Coherence Tomography in Healthy Korean Children. Korean J. Ophthalmol. 2016, 30, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, R.; Di Antonio, L.; Di Staso, S.; Agnifili, L.; Di Gregorio, A.; Ciancaglini, M.; Mastropasqua, L. Optical Coherence Tomography Angiography in Retinal Vascular Diseases and Choroidal Neovascularization. J. Ophthalmol. 2015, 2015, 343515. [Google Scholar] [CrossRef]
- Sambhav, K.; Grover, S.; Chalam, K.V. The application of optical coherence tomography angiography in retinal diseases. Surv. Ophthalmol. 2017, 62, 838–866. [Google Scholar] [CrossRef]
- Hong, E.H.; Shin, Y.U.; Kang, M.H.; Cho, H.; Seong, M. Wide scan imaging with swept-source optical coherent tomography for glaucoma diagnosis. PLoS ONE 2018, 13, e0195040. [Google Scholar] [CrossRef] [Green Version]
- Shin, Y.U.; Lee, D.E.; Kang, M.H.; Seong, M.; Yi, J.H.; Han, S.W.; Cho, H. Optical coherence tomography angiography analysis of changes in the retina and the choroid after haemodialysis. Sci. Rep. 2018, 8, 17184. [Google Scholar] [CrossRef]
- Shoji, T.; Yoshikawa, Y.; Kanno, J.; Ishii, H.; Ibuki, H.; Ozaki, K.; Kimura, I.; Shinoda, K. Reproducibility of Macular Vessel Density Calculations Via Imaging With Two Different Swept-Source Optical Coherence Tomography Angiography Systems. Transl. Vis. Sci. Technol. 2018, 7, 31. [Google Scholar] [CrossRef] [Green Version]
- Nakayama, L.F.; Bergamo, V.C.; Conti, M.L.; Fares, N.T.; Costa, L.A.; Ambrogini, O., Jr.; de Moraes, N.S.B. The retinal foveal avascular zone as a systemic biomarker to evaluate inflammatory bowel disease control. Int. J. Retina Vitreous 2019, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, C.C.; Lai, M.Y.; Lean, J.S.; Linton, K.L.; Trese, M.; Abrams, G.; Ryan, S.J.; Azen, S.P. Postoperative intraocular pressure abnormalities in the Silicone Study. Silicone Study Report 4. Ophthalmology 1993, 100, 1629–1635. [Google Scholar] [CrossRef]
- Casswell, A.G.; Gregor, Z.J. Silicone oil removal. I. The effect on the complications of silicone oil. Br. J. Ophthalmol. 1987, 71, 893–897. [Google Scholar] [CrossRef] [Green Version]
- Casswell, A.G.; Gregor, Z.J. Silicone oil removal. II. Operative and postoperative complications. Br. J. Ophthalmol. 1987, 71, 898–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Park, D.Y.; Ha, H.S.; Kang, S.W. Topographic changes of retinal layers after resolution of acute retinal detachment. Invest. Ophthalmol. Vis. Sci. 2012, 53, 7316–7321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cebulla, C.M.; Ruggeri, M.; Murray, T.G.; Feuer, W.J.; Hernandez, E. Spectral domain optical coherence tomography in a murine retinal detachment model. Exp. Eye Res. 2010, 90, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Baran, R.T.; Baran, S.O.; Toraman, N.F.; Filiz, S.; Demirbilek, H. Evaluation of intraocular pressure and retinal nerve fiber layer, retinal ganglion cell, central macular thickness, and choroidal thickness using optical coherence tomography in obese children and healthy controls. Niger. J. Clin. Pract. 2019, 22, 539–545. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.X.; Jiang, R.; Ren, X.L.; Chen, J.D.; Shi, H.L.; Xu, L.; Wei, W.B.; Jonas, J.B. Intraocular pressure elevation and choroidal thinning. Br. J. Ophthalmol. 2016, 100, 1676–1681. [Google Scholar] [CrossRef]
- Caramoy, A.; Droege, K.M.; Kirchhof, B.; Fauser, S. Retinal layers measurements in healthy eyes and in eyes receiving silicone oil-based endotamponade. Acta Ophthalmol. 2014, 92, e292–e297. [Google Scholar] [CrossRef]
- Bae, S.H.; Hwang, J.S.; Yu, H.G. Comparative analysis of macular microstructure by spectral-domain optical coherence tomography before and after silicone oil removal. Retina 2012, 32, 1874–1883. [Google Scholar] [CrossRef]
- Rabina, G.; Azem, N.; Barequet, D.; Barak, A.; Loewenstein, A.; Schwartz, S. Silicone Oil Tamponade Effect on Macular Layer Thickness and Visual Acuity. Retina 2020, 40, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Lo, D.M.; Flaxel, C.J.; Fawzi, A.A. Macular Effects of Silicone Oil Tamponade: Optical Coherence Tomography Findings During and After Silicone Oil Removal. Curr. Eye Res. 2017, 42, 98–103. [Google Scholar] [CrossRef]
- Wolf, S.; Schon, V.; Meier, P.; Wiedemann, P. Silicone oil-RMN3 mixture ("heavy silicone oil") as internal tamponade for complicated retinal detachment. Retina 2003, 23, 335–342. [Google Scholar] [CrossRef]
- Fawcett, I.M.; Williams, R.L.; Wong, D. Contact angles of substances used for internal tamponade in retinal detachment surgery. Graefes Arch. Clin. Exp. Ophthalmol. 1994, 232, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J. The physical and surgical aspects of silicone oil in the vitreous cavity. Graefes Arch. Clin. Exp. Ophthalmol. 1987, 225, 452–456. [Google Scholar] [CrossRef]
- Saxena, S.; Gopal, L. Fluid vitreous substitutes in vitreo retinal surgery. Indian J. Ophthalmol. 1996, 44, 191–206. [Google Scholar]
- Peters, F.; Arabali, D. Interfacial tension between oil and water measured with a modified contour method. Colloids Surf. A: Physicochem. Eng. Asp. 2013, 426, 1–5. [Google Scholar] [CrossRef]
- Odrobina, D.; Golebiewska, J.; Maroszynska, I. Choroidal Thickness Changes after Vitrectomy with Silicone Oil Tamponade for Proliferative Vitreoretinopathy Retinal Detachment. Retina 2017, 37, 2124–2129. [Google Scholar] [CrossRef]
- Karimi, S.; Entezari, M.; Nikkhah, H.; Esfandiari, H.; Darvishpoor, T.; Tavakoli, M.; Safi, S. Effects of Intravitreal Silicone Oil on Subfoveal Choroidal Thickness. Ophthalmologica 2018, 239, 159–166. [Google Scholar] [CrossRef]
- Mirza, E.; Satirtav, G.; Oltulu, R.; Kerimoglu, H.; Gunduz, M.K. Subfoveal choroidal thickness change following pars plana vitrectomy with silicone oil endotamponade for rhegmatogenous retinal detachment. Int. Ophthalmol. 2019, 39, 1717–1722. [Google Scholar] [CrossRef]
- Jurisic, D.; Geber, M.Z.; Cavar, I.; Utrobicic, D.K. Retinal Layers Measurements following Silicone Oil Tamponade for Retinal Detachment Surgery. Semin. Ophthalmol. 2018, 33, 711–718. [Google Scholar] [CrossRef]
- Lu, B.; Zhang, P.; Liu, H.; Jia, H.; Yu, Y.; Wang, F.; Wang, H.; Sun, X. Peripapillary Vessel Density in Eyes with Rhegmatogenous Retinal Detachment after Pars Plana Vitrectomy. J. Ophthalmol. 2021, 2021, 6621820. [Google Scholar] [CrossRef]
- Karasu, B.; Eris, E.; Sonmez, O.; Bekmez, S. The effect of silicone oil presence time on macular and choroidal thickness with macula-off rhegmatogenous retinal detachment. J. Fr. Ophtalmol. 2020, 43, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Shalchi, Z.; Mahroo, O.A.; Shunmugam, M.; Mohamed, M.; Sullivan, P.M.; Williamson, T.H. Spectral domain optical coherence tomography findings in long-term silicone oil-related visual loss. Retina 2015, 35, 555–563. [Google Scholar] [CrossRef]
- Williamson, T.H.; Shunmugam, M.; Rodrigues, I.; Dogramaci, M.; Lee, E. Characteristics of rhegmatogenous retinal detachment and their relationship to visual outcome. Eye 2013, 27, 1063–1069. [Google Scholar] [CrossRef] [Green Version]
- Lavia, C.; Couturier, A.; Erginay, A.; Dupas, B.; Tadayoni, R.; Gaudric, A. Reduced vessel density in the superficial and deep plexuses in diabetic retinopathy is associated with structural changes in corresponding retinal layers. PLoS ONE 2019, 14, e0219164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.; Kim, J.; Lee, J. Macular Vessel Density and Ganglion Cell/Inner Plexiform Layer Thickness and Their Combinational Index Using Artificial Intelligence. J. Glaucoma 2018, 27, 750–760. [Google Scholar] [CrossRef]
- Bonfiglio, V.; Ortisi, E.; Scollo, D.; Reibaldi, M.; Russo, A.; Pizzo, A.; Faro, G.; Macchi, I.; Fallico, M.; Toro, M.D.; et al. Vascular changes after vitrectomy for rhegmatogenous retinal detachment: Optical coherence tomography angiography study. Acta Ophthalmol. 2020, 98, e563–e569. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Cheng, D.; Feng, X.; Zheng, L.; Dong, Y.; Hou, Q.; Chen, F. Effect of Body Position on Intraocular Pressure in Silicone Oil Tamponade Eyes. Retina 2018, 38, 939–944. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Parameter | p-Value | |
|---|---|---|
| Age (y) | 58.53 ± 9.28 | |
| Sex (male/female) | 17/13 | |
| Macular status (on/off) | 4/26 | |
| Phakic/Pseudophakic | 9/21 | |
| Mean duration of SO tamponade (months) | ||
| ≤3 months (n = 19) | ||
| >3 months (n = 11) | 3.14 ± 1.4 (2–7 months) | |
| BCVA (LogMAR) | 0.01 * | |
| preoperation/six months after SOR | 0.76 ± 0.85/0.16 ± 0.27 | |
| IOP (mmHg) | ||
| preoperation/six months after SOR | 14.21 ± 3.09/14.85 ± 2.47 | 0.45 |
| Spherical equivalent refractive error (diopter) | ||
| preoperation/six months after SOR | −2.45 ± 3.04/−2.39 ± 3.14 | 0.51 |
| Axial length (mm) | ||
| unaffected fellow eye | 24.54 ± 1.36 | |
| six months after SOR | 24.98 ± 1.90 | 0.072 |
| SCP vessel density (%) | ||
| unaffected fellow eye/six months after SOR | 47.18 ± 2.87/47.05 ± 2.91 | 0.862 |
| DCP vessel density (%) | ||
| unaffected fellow eye/six months after SOR | 51.45 ± 2.69/51.04 ± 3.14 | 0.747 |
| FAZ area (µm2) | ||
| unaffected fellow eye/six months after SOR | 352.81±191/323.18 ± 250 | 0.13 |
| Follow-Up Period | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unaffected Fellow Eye | 1 Week after SO Tamponade | Before SOR | 1 Week after SOR | 3 Months after SOR | 6 Months after SOR | Before SOR vs. 1 Week after SOR | Before SOR vs. 3 Months after SOR | Unaffected Fellow Eye vs. 6 Months after SOR | ||
| Fovea (µm) | Total retina | 251.82 ± 47.03 | 242.47 ± 39.97 | 235.47 ± 21.37 | 237.61 ± 21.50 | 251.50 ± 20.77 | 245.52 ± 20.98 | 0.75 | 0.078 | 0.48 |
| RNFL | 14.00 ± 11.31 | 11.52 ± 8.61 | 11.82 ± 10.28 | 12.38 ± 13.01 | 13.00 ± 11.21 | 12.05 ± 10.98 | 0.92 | 0.45 | 0.63 | |
| GC-IPL | 49.82 ± 19.64 | 48.41 ± 18.64 | 43.17 ± 18.27 | 45.25 ± 20.11 | 49.58 ± 17.49 | 51.17 ± 19.67 | 0.69 | 0.09 | 0.327 | |
| Choroid | 184.29 ± 50.21 | 170.17 ± 57.67 | 161.29 ± 45.48 | 173.82 ± 48.52 | 161.64 ± 51.59 | 159.41 ± 52.74 | 0.003 * | 0.938 | 0.053 | |
| Parafovea (µm) | Total retina | 311.13 ± 24.33 | 284.98 ± 25.69 | 279.73 ± 22.45 | 297.41 ± 25.71 | 306.66 ± 24.48 | 306.42 ± 22.65 | <0.001 * | <0.001 ** | 0.63 |
| RNFL | 30.00 ± 9.31 | 29.36 ± 3.86 | 25.64 ± 10.12 | 31.61 ± 9.81 | 32.06 ± 11.14 | 28.10 ± 10.44 | <0.001 * | <0.001 ** | 0.45 | |
| GC-IPL | 88.17 ± 14.15 | 80.92 ± 11.81 | 66.08 ± 15.35 | 78.47 ± 14.77 | 82.89 ± 17.96 | 84.58 ± 15.87 | <0.001 * | <0.001 ** | 0.49 | |
| Choroid | 180.47 ± 41.89 | 173.23 ± 59.16 | 161.79 ± 44.16 | 174.95 ± 43.25 | 160.83 ± 46.93 | 159.20 ± 47.55 | 0.001 * | 0.819 | 0.06 | |
| Optic disc (µm) | ppRNFL | 110.65 ± 16.21 | 104.42 ± 17.29 | 92.0 ± 19.68 | 96.47 ± 18.54 | 96.58 ± 17.46 | 90.52 ± 15.35 | 0.026 * | 0.290 | 0.003 *** |
| Linear Mixed Model | Post Hoc Analysis Derived Using Bonferroni (p-Value) | |||||||
|---|---|---|---|---|---|---|---|---|
| F | p-Value | Before SOR vs. 1 Week after SOR | One Week after SOR vs. 3 Months after SOR | 3 Months after SOR vs. 6 Months after SOR | Before SOR vs. 3 Months after SOR | One Week after SOR vs. 6 Months after SOR | Before SOR vs. 6 Months after SOR | |
| Fovea | ||||||||
| Total retina | 0.941 | 0.426 | - | - | - | - | - | - |
| RNFL | 0.043 | 0.988 | - | - | - | - | - | - |
| GC-IPL | 1.488 | 0.226 | - | - | - | - | - | - |
| Choroid | 0.164 | 0.920 | - | - | - | - | - | - |
| Parafovea | ||||||||
| Total retina | 2.731 | 0.049 * | 0.673 | 1.0 | 1.0 | 0.139 | 1.0 | 0.048 † |
| RNFL | 4.231 | 0.009 * | 0.054 | 1.0 | 0.516 | 0.009 † | 1.0 | 0.729 |
| GC-IPL | 5.137 | 0.003 * | 0.123 | 1.0 | 1.0 | 0.012 † | 1.0 | 0.004 † |
| Choroid | 0.244 | 0.865 | - | - | - | |||
| Optic disc ppRNFL | 0.335 | 0.80 | - | - | - | |||
| SO Tamponade Period | Area | Unaffected Fellow Eyes | 6 Months after SO Removal | p-Value | |
|---|---|---|---|---|---|
| ≤3 months (n = 19) | Parafovea | Total retina (µm) | 307.16 ± 18.14 | 295.65 ± 17.58 | 0.09 |
| RNFL (µm) | 27.75 ± 9.32 | 26.97 ± 13.87 | 0.64 | ||
| GC-IPL (µm) | 87.16 ± 16.75 | 84.25 ± 14.83 | 0.67 | ||
| Optic disc | ppRNFL | 107.12 ± 19.75 | 95.77 ± 18.16 | 0.07 | |
| >3 months (n = 11) | Parafovea | Total retina (µm) | 319.20 ± 20.55 | 303.59 ± 21.32 | 0.33 |
| RNFL (µm) | 35.40 ± 10.80 | 30.82 ± 12.24 | 0.59 | ||
| GC-IPL (µm) | 89.0 ± 17.10 | 85.4 ± 15.88 | 0.66 | ||
| Optic disc | ppRNFL (µm) | 105.4 ± 24.28 | 79.0 ± 17.23 | 0.019 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Cho, H.; Kang, M.; Hong, R.; Seong, M.; Shin, Y. Retinal Changes before and after Silicone Oil Removal in Eyes with Rhegmatogenous Retinal Detachment Using Swept-Source Optical Coherence Tomography. J. Clin. Med. 2021, 10, 5436. https://doi.org/10.3390/jcm10225436
Lee J, Cho H, Kang M, Hong R, Seong M, Shin Y. Retinal Changes before and after Silicone Oil Removal in Eyes with Rhegmatogenous Retinal Detachment Using Swept-Source Optical Coherence Tomography. Journal of Clinical Medicine. 2021; 10(22):5436. https://doi.org/10.3390/jcm10225436
Chicago/Turabian StyleLee, Jungwook, Heeyoon Cho, Minho Kang, Rimkyung Hong, Mincheol Seong, and Yongun Shin. 2021. "Retinal Changes before and after Silicone Oil Removal in Eyes with Rhegmatogenous Retinal Detachment Using Swept-Source Optical Coherence Tomography" Journal of Clinical Medicine 10, no. 22: 5436. https://doi.org/10.3390/jcm10225436