
Pleomorphic Adenoma of the Parotid Gland and the Parapharyngeal Space: Two Diametrically Opposing Surgical Philosophies for the Same Histopathologic Entity? †
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dulguerov, P.; Todic, J.; Pusztaszeri, M.; Alotaibi, N.H. Why Do Parotid Pleomorphic Adenomas Recur? A Systematic Review of Pathological and Surgical Variables. Front. Surg. 2017, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, G.; Langrock, I.; Donath, K. A pathological classification of pleomorphic adenoma of the salivary glands (author’s transl). HNO 1976, 24, 415–426. [Google Scholar] [PubMed]
- Harney, M.S.; Murphy, C.; Hone, S.; Toner, M.; Timon, C.V. A histological comparison of deep and superficial lobe pleomorphic adenomas of the parotid gland. Head Neck 2003, 25, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Zbaren, P.; Stauffer, E. Pleomorphic adenoma of the parotid gland: Histopathologic analysis of the capsular characteristics of 218 tumors. Head Neck 2007, 29, 751–757. [Google Scholar] [CrossRef]
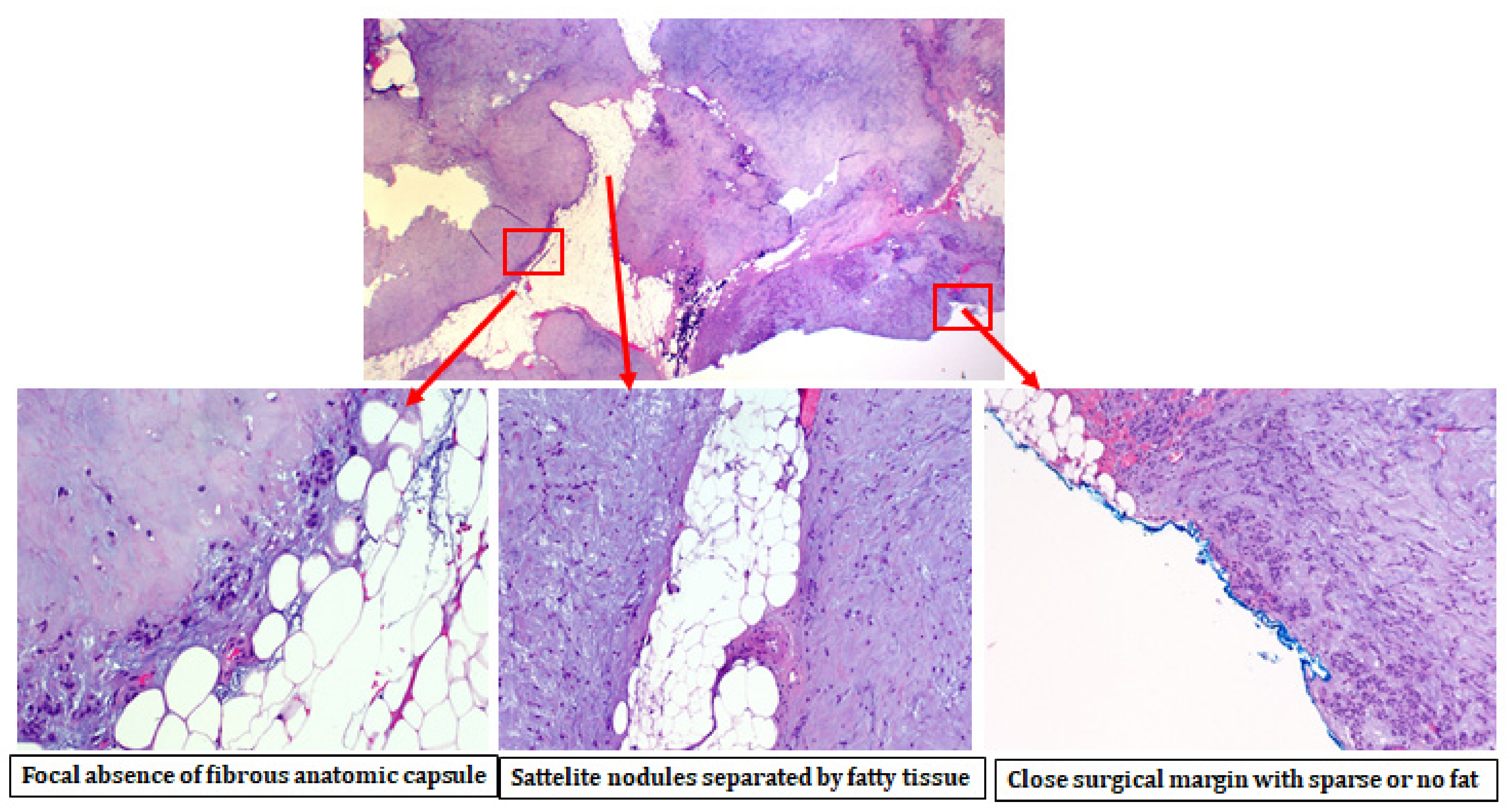
- Iro, A.K.; Agaimy, A.; Muller, S.K.; Sievert, M.; Iro, H.; Mantsopoulos, K. Satellite nodules in pleomorphic adenomas of the parotid gland: A nightmare for less invasive parotid surgery? Oral Oncol. 2021, 115, 105218. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Iro, A.K.; Sievert, M.; Muller, S.K.; Agaimy, A.; Schapher, M.; Koch, M.; Iro, H. Is extracapsular dissection for pleomorphic adenoma rather a euphemism for enucleation that jeopardises the intactness of the capsule? Br. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Sievert, M.; Iro, A.K.; Muller, S.K.; Koch, M.; Schapher, M.; Agaimy, A.; Iro, H. Histopathological comparison of pleomorphic adenomas of the parotid and submandibular gland. Oral Dis. 2021. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Iro, H. Tumour spillage of the pleomorphic adenoma of the parotid gland: A proposal for intraoperative measures. Oral Oncol. 2021, 112, 104986. [Google Scholar] [CrossRef]
- Buchta, P.; Thimsen, V.; Iro, A.K.; Agaimy, A.; Iro, H.; Mantsopoulos, K. The influence of the capsular defect as a risk factor for recurrence in pleomorphic adenoma. Laryngo Rhino Otol. 2021. [Google Scholar] [CrossRef]
- Valstar, M.H.; Andreasen, S.; Bhairosing, P.A.; McGurk, M. Natural history of recurrent pleomorphic adenoma: Implications on management. Head Neck 2020, 42, 2058–2066. [Google Scholar] [CrossRef]
- Carlson, R.E.; Ord, R.A. Salivary Gland Pathology, Diagnosis and Management; John Wiley & Sons: Hoboken, NJ, USA, 2021; pp. 238–241. [Google Scholar]
- Yang, T.L.; Hsiao, T.Y.; Wang, C.P.; Lou, P.J.; Ko, J.Y. Extracapsular dissection for minimal resection of benign parapharyngeal tumor. Eur. Arch. Otorhinolaryngol. 2012, 269, 2097–2102. [Google Scholar] [CrossRef]
- Horowitz, G.; Ben-Ari, O.; Wasserzug, O.; Weizman, N.; Yehuda, M.; Fliss, D.M. The transcervical approach for parapharyngeal space pleomorphic adenomas: Indications and technique. PLoS ONE 2014, 9, e90210. [Google Scholar] [CrossRef]
- Lopes, M.L.; Barroso, K.M.; Henriques, A.C.; Dos Santos, J.N.; Martins, M.D.; de Souza, L.B. Pleomorphic adenomas of the salivary glands: Retrospective multicentric study of 130 cases with emphasis on histopathological features. Eur. Arch. Otorhinolaryngol. 2017, 274, 543–551. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Muller, S.; Agaimy, A.; Goncalves, M.; Koch, M.; Wust, W.; Bohr, C.; Iro, H. Extracapsular dissection in the parapharyngeal space: Benefits and potential pitfalls. Br. J. Oral Maxillofac. Surg. 2017, 55, 709–713. [Google Scholar] [CrossRef]
- Mendelsohn, A.H.; Bhuta, S.; Calcaterra, T.C.; Shih, H.B.; Abemayor, E.; St John, M.A. Parapharyngeal space pleomorphic adenoma: A 30-year review. Laryngoscope 2009, 119, 2170–2174. [Google Scholar] [CrossRef]
- Guntinas-Lichius, O.; Klussmann, J.P.; Wittekindt, C.; Stennert, E. Parotidectomy for benign parotid disease at a university teaching hospital: Outcome of 963 operations. Laryngoscope 2006, 116, 534–540. [Google Scholar] [CrossRef]
- Piekarski, J.; Nejc, D.; Szymczak, W.; Wronski, K.; Jeziorski, A. Results of extracapsular dissection of pleomorphic adenoma of parotid gland. J. Oral Maxillofac. Surg. 2004, 62, 1198–1202. [Google Scholar] [CrossRef]
- Lombardi, D.; Ferrari, M.; Paderno, A.; Taboni, S.; Rampinelli, V.; Barbara, F.; Schreiber, A.; Mattavelli, D.; Tomasoni, M.; Farina, D.; et al. Selection of the surgical approach for lesions with parapharyngeal space involvement: A single-center experience on 153 cases. Oral Oncol. 2020, 109, 104872. [Google Scholar] [CrossRef]
- Paderno, A.; Piazza, C.; Nicolai, P. Recent advances in surgical management of parapharyngeal space tumors. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Fermi, M.; Serafini, E.; Ferri, G.; Alicandri-Ciufelli, M.; Presutti, L.; Mattioli, F. Management of parapharyngeal space tumors with transparotid-transcervical approach: Analysis of prognostic factors related with disease-control and functional outcomes. Eur. Arch. Otorhinolaryngol. 2021. [Google Scholar] [CrossRef]
- Riffat, F.; Dwivedi, R.C.; Palme, C.; Fish, B.; Jani, P. A systematic review of 1143 parapharyngeal space tumors reported over 20 years. Oral Oncol. 2014, 50, 421–430. [Google Scholar] [CrossRef]
- Zbaren, P.; Vander Poorten, V.; Witt, R.L.; Woolgar, J.A.; Shaha, A.R.; Triantafyllou, A.; Takes, R.P.; Rinaldo, A.; Ferlito, A. Pleomorphic adenoma of the parotid: Formal parotidectomy or limited surgery? Am. J. Surg. 2013, 205, 109–118. [Google Scholar] [CrossRef]
- Grant, J. An Atlas of Anatomy, 6th ed.; Williams & Wilkins: Baltimore, MD, USA, 1972. [Google Scholar]
- Patey, D.H.; Thackray, A.C. The pathological anatomy and treatment of parotid tumours with retropharyngeal extension (dumb-bell tumours); with a report of 4 personal cases. Br. J. Surg. 1957, 44, 352–358. [Google Scholar] [CrossRef]
- Stennert, E.; Guntinas-Lichius, O.; Klussmann, J.P.; Arnold, G. Histopathology of pleomorphic adenoma in the parotid gland: A prospective unselected series of 100 cases. Laryngoscope 2001, 111, 2195–2200. [Google Scholar] [CrossRef]
- Cotran, R.S.; Kumar, V.; Collins, T. Neoplasia. In Robbins’ Pathologic Basis of Disease, 6th ed.; Cotran, R.S., Kumar, V., Collins, T., Eds.; Saunders: Philadelphia, PA, USA, 1998. [Google Scholar]
- Evans, R.W.; Cruickshanks, A.H. Epithelial Tumours of the Salivary Glands; Saunders: Philadelphia, PA, USA, 1970. [Google Scholar]
- Eneroth, C.M. Mixed tumors of major salivary glands: Prognostic role of capsular structure. Ann. Otol. Rhinol. Laryngol. 1965, 74, 944–953. [Google Scholar] [CrossRef]
- Mantsopoulos, K.; Thimsen, V.; Gostian, A.O.; Muller, S.K.; Sievert, M.; Iro, A.K.; Agaimy, A.; Iro, H. Histopathology of Parotid Pleomorphic Adenomas: A “Pleomorphic Approach” to a Demanding Lesion. Laryngoscope 2022, 132, 73–77. [Google Scholar] [CrossRef]
- Kandasamy, J.; Smith, A.; Diaz, S.; Rose, B.; O’Brien, C. Heterogeneity of PLAG1 gene rearrangements in pleomorphic adenoma. Cancer Genet. Cytogenet 2007, 177, 1–5. [Google Scholar] [CrossRef]
- Agaimy, A.; Ihrler, S.; Baneckova, M.; Costes Martineau, V.; Mantsopoulos, K.; Hartmann, A.; Iro, H.; Stoehr, R.; Skalova, A. HMGA2-WIF1 Rearrangements Characterize a Distinctive Subset of Salivary Pleomorphic Adenomas With Prominent Trabecular (Canalicular Adenoma-like) Morphology. Am. J. Surg. Pathol. 2021. [Google Scholar] [CrossRef]
- Triantafyllou, A.; Thompson, L.D.; Devaney, K.O.; Bell, D.; Hunt, J.L.; Rinaldo, A.; Vander Poorten, V.; Ferlito, A. Functional Histology of Salivary Gland Pleomorphic Adenoma: An Appraisal. Head Neck Pathol. 2015, 9, 387–404. [Google Scholar] [CrossRef] [Green Version]
- Linxweiler, M.; Wang, J.; Morris, L.G.T. The role of immune surveillance in malignant transformation of benign salivary gland tumors. Oncotarget 2021, 12, 592–595. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parotid Gland | Parapharyngeal Space | Total | p Value | |
|---|---|---|---|---|
| Number of cases | 786 (93.1) | 58 (6.9) | 844 (100) | - |
| Age (years) | 48.7 (±15.4, range: 12–87) | 50.2 (±14.0, range: 25–84) | 48.9 (±15.4, range: 12–87) | 0.481 |
| Gender (male/female) | 273/513 | 18/40 | 291/553 | 0.567 |
| Size (mm) | 23.7 (± 10.6, range: 4–105) | 40.5 (± 13.8, range: 18–75) | 24.9 (±11.6, range: 4–105) | <0.001 |
| Recurrences (%) | 7/786 (0.8) | 1/58 (1.7) | 8/844 (0.9) | 0.527 |
| Average time from diagnosis to recurrence (months) | 72.8 (47–97) | 138 | 82.1 (47–138) | - |
| Histopathologic Features | Parotid Gland (%) | Parapharyngeal Space (%) | Total (%) | p | |
|---|---|---|---|---|---|
| Histologic subtype [2] | Hypercellular subtype (stroma content < 30%) | 189 (24) | 14 (24.1) | 203 | 0.972 |
| Mixed subtype (stroma content 30–50%) | 220 (28) | 17 (29.3) | 237 | ||
| Stroma-rich (myxoid) subtype (stroma content > 50%) | 377 (48) | 27 (46.6) | 404 | ||
| Total | 786 (100) | 58 (100) | |||
| Integrity of capsule | No capsule at all | 32 (4.1) | 4 (6.9) | 36 | 0.035 |
| Partial encapsulation | 105 (13.3) | 14 (24.1) | 119 | ||
| Intact capsule | 649 (8.3) | 40 (69) | 689 | ||
| Total | 786 (100) | 58 (100) | |||
| Pseudopodia | Presence of pseudopodia | 343 (43.6) | 22 (37.9) | 365 | 0.397 |
| No pseudopodia | 443 (56.4) | 36 (62.1) | 479 | ||
| Total | 786 (100) | 58 (100) | |||
| Satellite nodules | Presence of satellite nodules | 59 (8.1) | 12 (20.7) | 71 | <0.001 |
| Absence of satellite nodules | 727 (92.5) | 46 (79.3) | 773 | ||
| 786 (100) | 58 (100) | ||||
| Surgical invasion of the capsule | Surgical invasion of the capsule | 33 (4.2) | 5 (8.6) | 38 | 0.117 |
| No surgical invasion of capsule | 753 (95.8) | 53 (91.4) | 806 | ||
| Total | 786 (100) | 58 (100) | |||
| Parotid Gland | Parapharyngeal Space | p | |
|---|---|---|---|
| Number of satellite nodules/lesion (±SD) | 1.32 (±0.6) | 1 (±0.0) | 0.247 |
| Mean distance from the main lesion to the inner periphery of the most distant satellite nodule (mm) (±SD) | 1.2 (±1.2) | 0.7 (±0.5) | 0.412 |
| Mean size of the satellite nodules (mm) (±SD) | 1.9 (±2.1) | 1.7 (±1.1) | 0.817 |
| Mean distance from the main lesion to the outer periphery of the most distant satellite nodule (mm) | 3.1 (±2.3) | 2.4 (±1.4) | 0.516 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hornung, B.; Constantinidis, J.; Thimsen, V.; Agaimy, A.; Koch, M.; Gostian, A.-O.; Sievert, M.; Müller, S.K.; Iro, H.; Mantsopoulos, K. Pleomorphic Adenoma of the Parotid Gland and the Parapharyngeal Space: Two Diametrically Opposing Surgical Philosophies for the Same Histopathologic Entity? J. Clin. Med. 2022, 11, 142. https://doi.org/10.3390/jcm11010142
Hornung B, Constantinidis J, Thimsen V, Agaimy A, Koch M, Gostian A-O, Sievert M, Müller SK, Iro H, Mantsopoulos K. Pleomorphic Adenoma of the Parotid Gland and the Parapharyngeal Space: Two Diametrically Opposing Surgical Philosophies for the Same Histopathologic Entity? Journal of Clinical Medicine. 2022; 11(1):142. https://doi.org/10.3390/jcm11010142
Chicago/Turabian StyleHornung, Benita, Jannis Constantinidis, Vivian Thimsen, Abbas Agaimy, Michael Koch, Antoniu-Oreste Gostian, Matti Sievert, Sarina Katrin Müller, Heinrich Iro, and Konstantinos Mantsopoulos. 2022. "Pleomorphic Adenoma of the Parotid Gland and the Parapharyngeal Space: Two Diametrically Opposing Surgical Philosophies for the Same Histopathologic Entity?" Journal of Clinical Medicine 11, no. 1: 142. https://doi.org/10.3390/jcm11010142