
Neurostimulation in People with Oropharyngeal Dysphagia: A Systematic Review and Meta-Analyses of Randomised Controlled Trials—Part I: Pharyngeal and Neuromuscular Electrical Stimulation

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Information Sources and Search Strategies
2.2. Inclusion and Exclusion Criteria
3. Systematic Review
3.1. Methodological Quality and Risk of Bias
3.2. Data Collection Process
3.3. Data, Items and Synthesis of Results
4. Meta-Analysis
5. Results
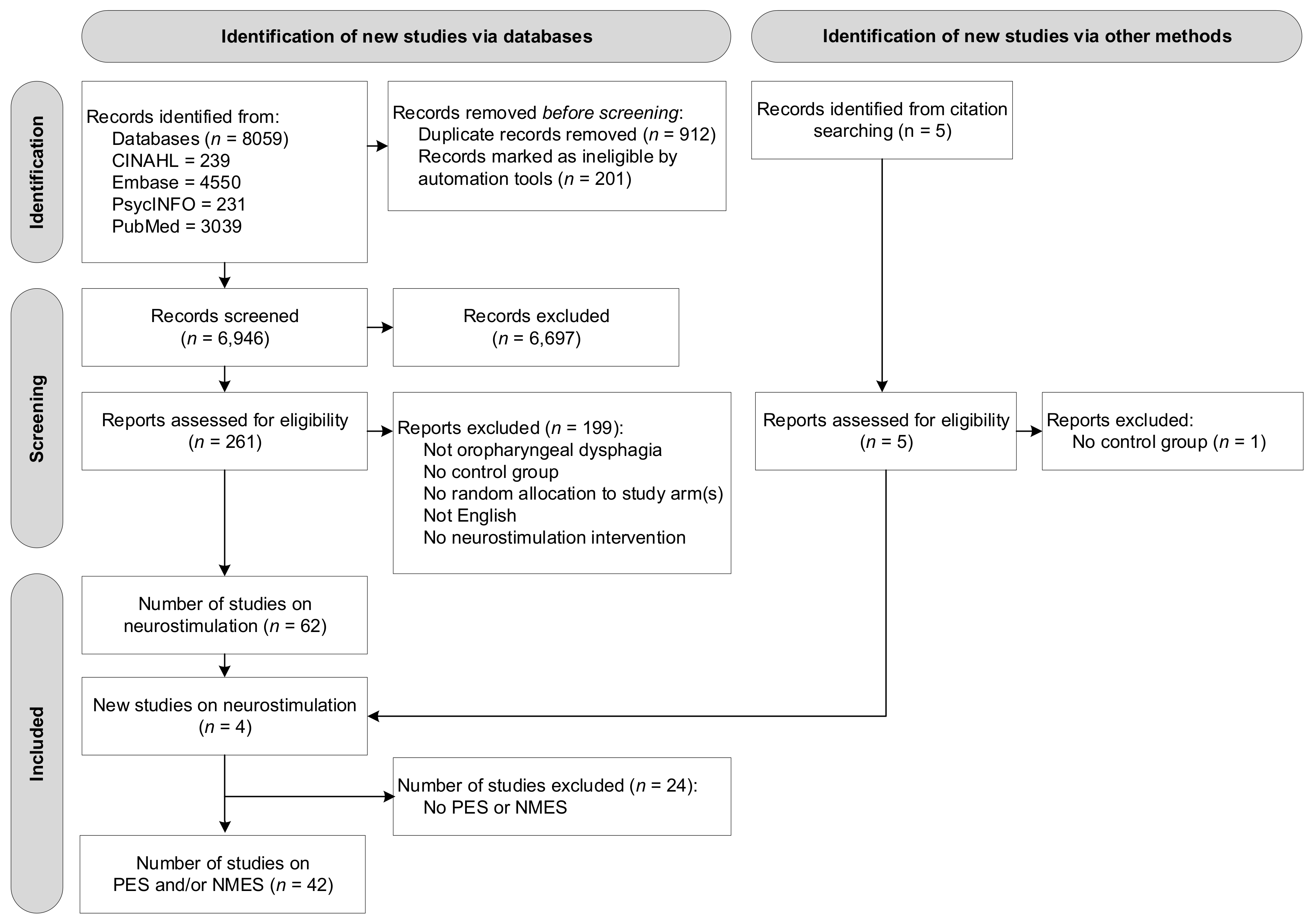
5.1. Study Selection
5.2. Description of Studies
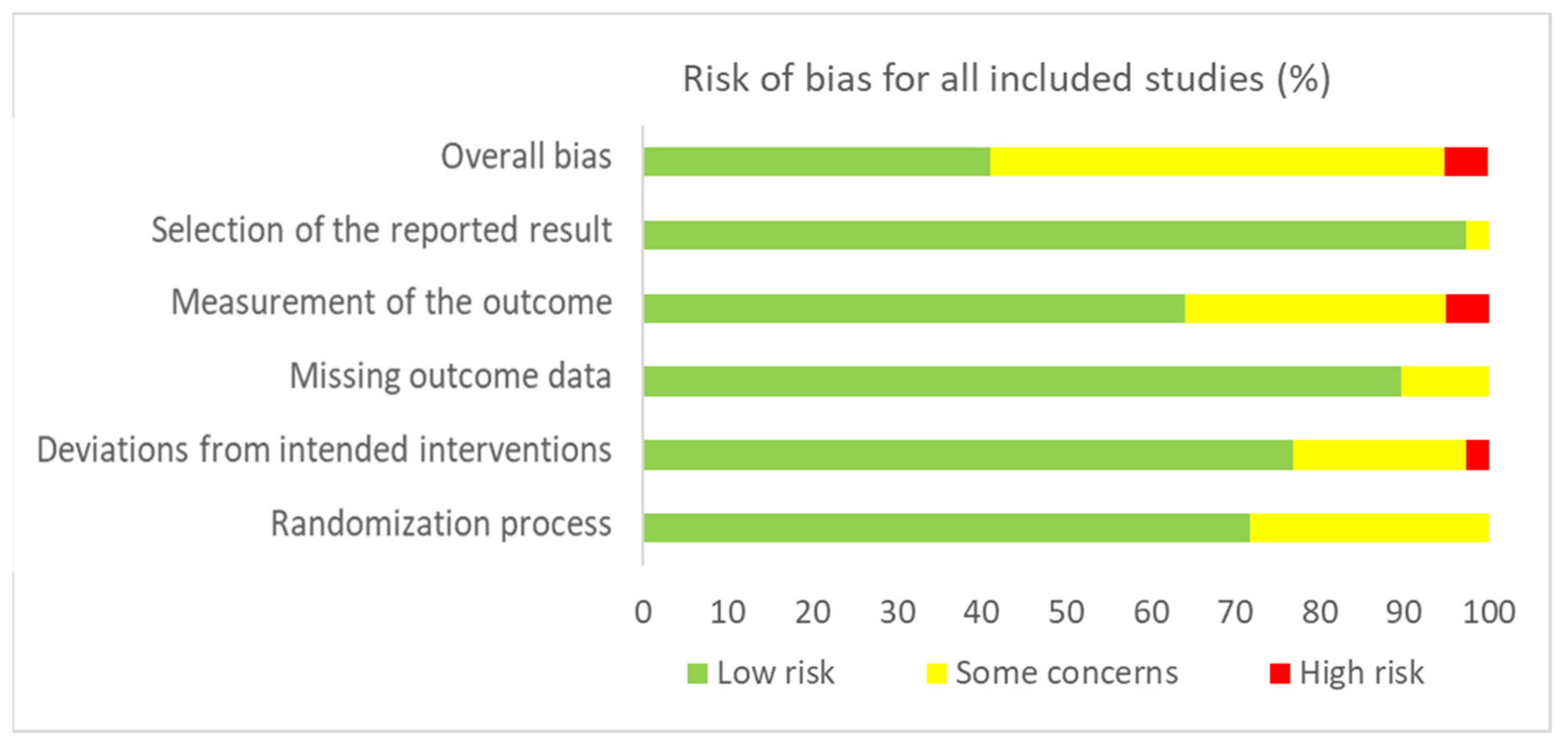
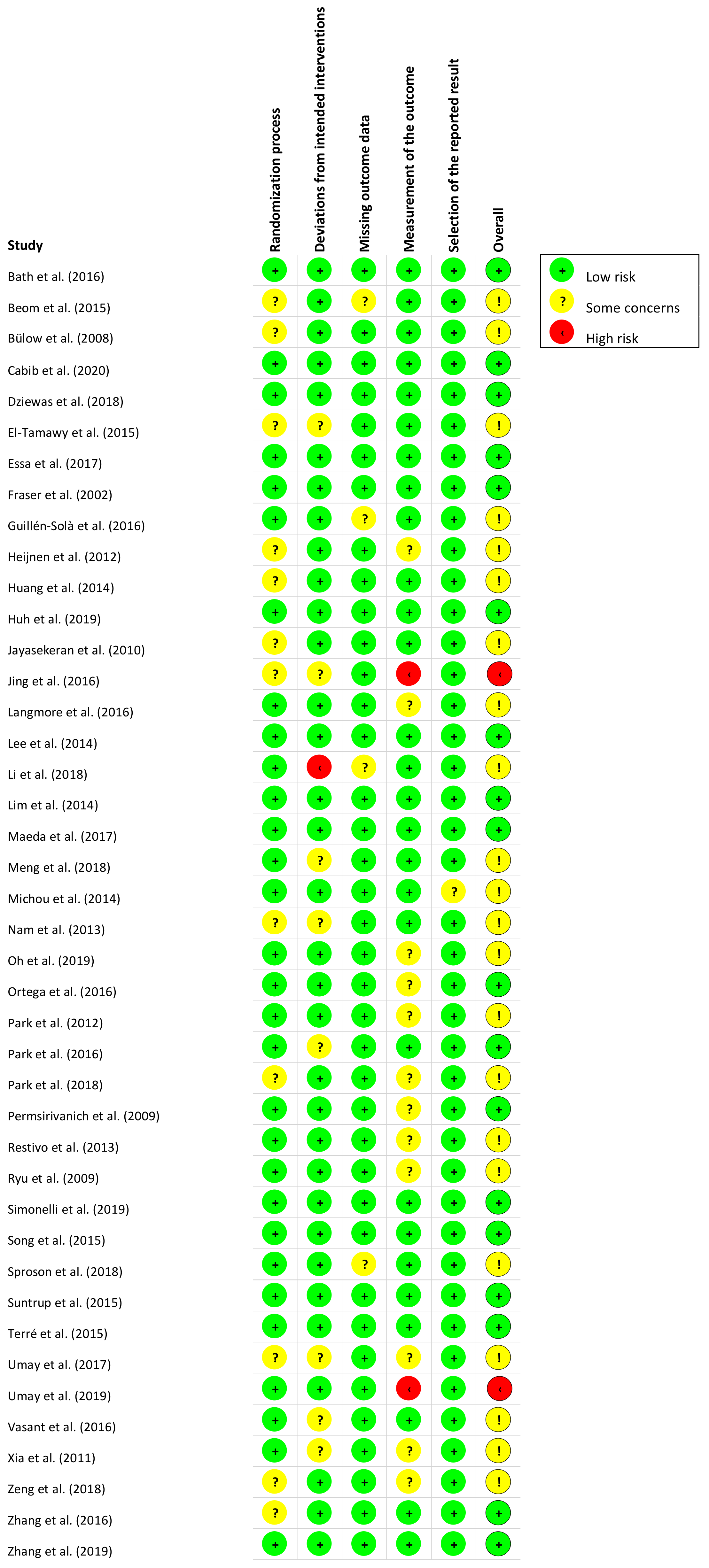
5.3. Risk of Bias Assessment and Methodological Quality
6. Meta-Analysis: Effects of Interventions
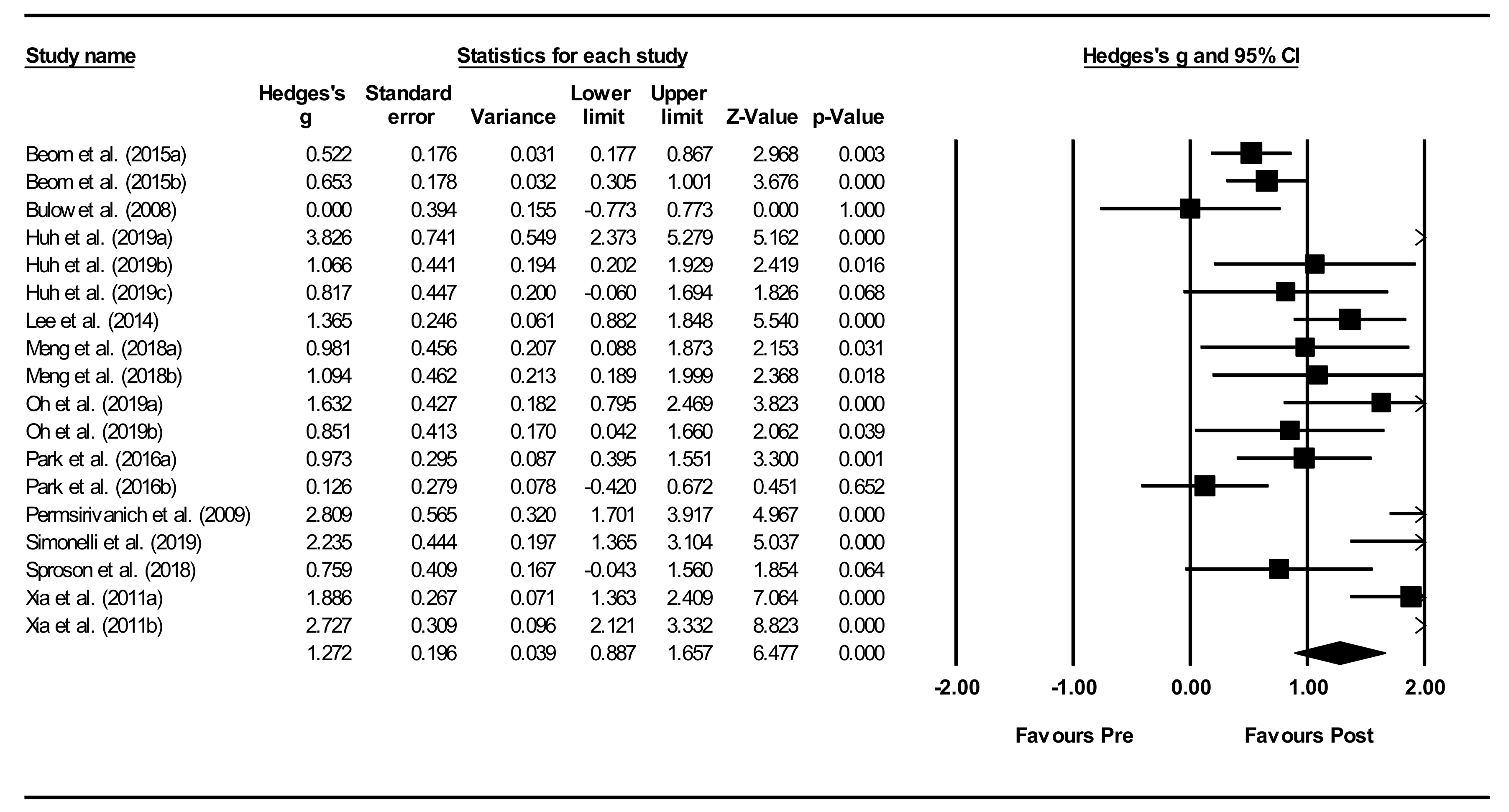
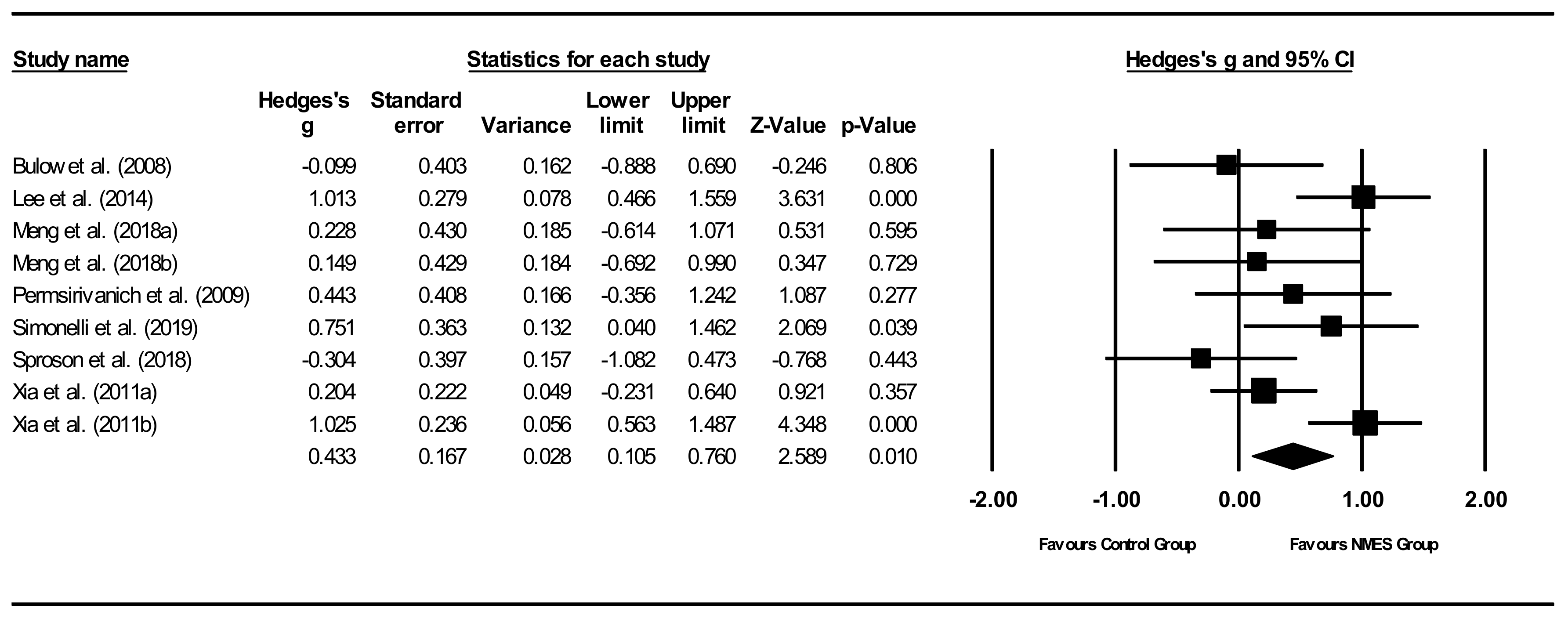
6.1. Neuromuscular Electrical Stimulation (NMES) Meta-Analysis
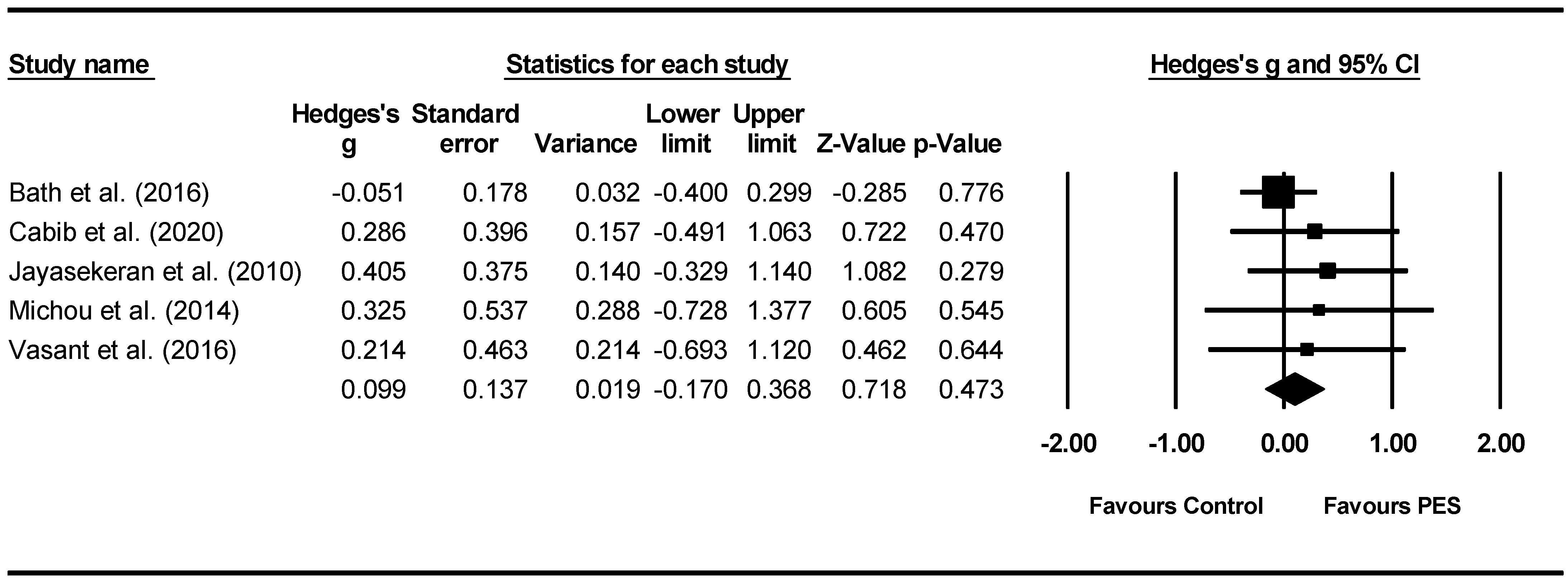
6.2. Pharyngeal Electrical Stimulation (PES) Meta-Analysis
7. Discussion
7.1. Systematic Review Findings
7.2. NMES
7.3. PES
7.4. Moderators
7.5. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Speyer, R. (Ed.) Behavioural Treatment of Oropharyngeal Dysphagia; Springer: Berlin, Germany, 2018. [Google Scholar]
- Speyer, R.; Cordier, R.; Kim, J.H.; Cocks, N.; Michou, E.; Wilkes-Gillan, S. Prevalence of drooling, feeding and swallowing problems in cerebral palsy across the lifespan: Systematic review and meta-analysis. Dev. Med. Child Neurol. 2019, 61, 1249–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R. A Systematic Review of the Prevalence of Oropharyngeal Dysphagia in Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, and Pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; Speyer, R.; Kertscher, B.; Denman, D.; Swan, K.; Cordier, R. Health-related quality of life in oropharyngeal dysphagia. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Wu, L.; Fang, Q.; Shen, M.; Zhang, L.; Liu, X. Effects of capsaicin on swallowing function in stroke patients with dysphagia: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Quiroz-González, S.; Torres-Castillo, S.; López-Gómez, R.E.; Estrada, I.J. Acupuncture points and their relationship with multireceptive fields of neurons. J. Acupunct. Meridian Stud. 2017, 10, 81–89. [Google Scholar] [CrossRef]
- Cheng, I.; Sasegbon, A.; Hamdy, S. Effects of neurostimulation on poststroke dysphagia: A synthesis of current evidence from randomised controlled trials. Neuromodulation Technol. Neural Interface 2021, 24, 1388–1401. [Google Scholar] [CrossRef]
- Michou, E.; Sasegbon, A.; Hamdy, S. Neurostimulation for the treatment of dysphagia after stroke: Behavioural treatment of oropharyngeal dysphagia. In Dysphagia: Diagnosis and Treatment, 2nd ed.; Ekberg, O., Ed.; Medical Radiology: Diagnostic Imaging; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Carnaby, G.D.; LaGorio, L.; Silliman, S.; Crary, M. Exercise-based swallowing intervention (McNeill Dysphagia Therapy) with adjunctive NMES to treat dysphagia post-stroke: A double-blind placebo-controlled trial. J. Oral Rehabil. 2020, 47, 501–510. [Google Scholar] [CrossRef]
- Alamer, A.; Melese, H.; Nigussie, F. Effectiveness of Neuromuscular Electrical Stimulation on Post-Stroke Dysphagia: A Systematic Review of Randomized Controlled Trials. Clin. Interv. Aging 2020, 15, 1521–1531. [Google Scholar] [CrossRef]
- Baijens, L.W.J.; Speyer, R.; Passos, V.L.; Pilz, W.; Van Der Kruis, J.; Haarmans, S.; Desjardins-Rombouts, C. Surface electrical stimulation in dysphagic parkinson patients: A randomized clinical trial. Laryngoscope 2013, 123, E38–E44. [Google Scholar] [CrossRef]
- Clark, H.; Lazarus, C.; Arvedson, J.; Schooling, T.; Frymark, T. Evidence-Based Systematic Review: Effects of Neuromuscular Electrical Stimulation on Swallowing and Neural Activation. Am. J. Speech Lang. Pathol. 2009, 18, 361–375. [Google Scholar] [CrossRef] [Green Version]
- Dionisio, A.; Duarte, I.C.; Patricio, M.; Castelo-Branco, M. Transcranial magnetic stimulation as an intervention tool to recover from language, swallowing and attentional deficits after stroke: A systematic review. Cerebrovasc. Dis. 2018, 18, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.; Xing, G.; Guoqiang, X.; Jin, Y.; Tang, Q.; He, B.; McClure, M.A.; Liu, H.; Chen, H.; Mu, Q. Repetitive transcranial magnetic stimulation as an alternative therapy for dysphagia after stroke: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 289–298. [Google Scholar] [CrossRef]
- Marchina, S.; Pisegna, J.M.; Massaro, J.M.; Langmore, S.E.; McVey, C.; Wang, J.; Kumar, S. Transcranial direct current stimulation for post-stroke dysphagia: A systematic review and meta-analysis of randomized controlled trials. J. Neurol. 2021, 268, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Momosaki, R.; Kinoshita, S.; Kakuda, W.; Yamada, N.; Abo, M. Noninvasive brain stimulation for dysphagia after acquired brain injury: A systematic review. J. Med. Investig. 2016, 63, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisegna, J.M.; Kaneoka, A.; Pearson, W.G.; Kumar, S.; Langmore, S.E. Effects of non-invasive brain stimulation on post-stroke dysphagia: A systematic review and meta-analysis of randomized controlled trials. Clin. Neurophysiol. 2016, 127, 956–968. [Google Scholar] [CrossRef] [Green Version]
- Bath, P.M.; Lee, H.S.; Everton, L.F. Swallowing therapy for dysphagia in acute and subacute stroke (Review). Cochrane Database Syst. Rev. 2018, 10, CD000323. [Google Scholar]
- Chiang, C.-F.; Lin, M.-T.; Hsiao, M.-Y.; Yeh, Y.-C.; Liang, Y.-C.; Wang, T.-G. Comparative Efficacy of Noninvasive Neurostimulation Therapies for Acute and Subacute Poststroke Dysphagia: A Systematic Review and Network Meta-analysis. Arch. Phys. Med. Rehabil. 2019, 100, 739–750.e4. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; McKenzie, J.E. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis; Biostat: Englewood, NJ, USA, 2014; Volume 3. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R. The file drawer problem and tolerance for null results. Psychol. Bull. 1979, 86, 638–664. [Google Scholar] [CrossRef]
- Beom, J.; Oh, B.-M.; Choi, K.H.; Kim, W.; Song, Y.J.; You, D.S.; Kim, S.J.; Han, T.R. Effect of Electrical Stimulation of the Suprahyoid Muscles in Brain-Injured Patients with Dysphagia. Dysphagia 2015, 30, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Bülow, M.; Speyer, R.; Baijens, L.; Woisard, V.; Ekberg, O. Neuromuscular Electrical Stimulation (NMES) in Stroke Patients with Oral and Pharyngeal Dysfunction. Dysphagia 2008, 23, 302–309. [Google Scholar] [CrossRef] [PubMed]
- El-Tamawy, M.S.; Darwish, M.H.; El-Azizi, H.S.; Abdelalim, A.M.; Taha, S.I. The influence of physical therapy on oropharyngeal dysphagia in acute stroke patients. Egypt. J. Neurol. Psychiatry Neurosurg. 2015, 52, 201–205. [Google Scholar]
- Guillén-Solà, A.; Sartor, M.M.; Soler, N.B.; Duarte, E.; Barrera, M.C.; Marco, E. Respiratory muscle strength training and neuromuscular electrical stimulation in subacute dysphagic stroke patients: A randomized controlled trial. Clin. Rehabilitation 2017, 31, 761–771. [Google Scholar] [CrossRef]
- Heijnen, B.J.; Speyer, R.; Baijens, L.W.J.; Bogaardt, H.C.A. Neuromuscular electrical stimulation versus traditionaltherapy in patients with Parkinson’s Disease and propharyngeal dysphagia: Effects on quality of life. Dysphagia 2012, 27, 336–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, K.-L.; Liu, T.-Y.; Huang, Y.-C.; Leong, C.-P.; Lin, W.-C.; Pong, Y.-P. Functional Outcome in Acute Stroke Patients with Oropharyngeal Dysphagia after Swallowing Therapy. J. Stroke Cerebrovasc. Dis. 2014, 23, 2547–2553. [Google Scholar] [CrossRef] [Green Version]
- Huh, J.; Park, E.; Min, Y.; Kim, A.; Yang, W.; Oh, H.; Nam, T.; Jung, T. Optimal placement of electrodes for treatment of post-stroke dysphagia by neuromuscular electrical stimulation combined with effortful swallowing. Singap. Med. J. 2020, 61, 487–491. [Google Scholar] [CrossRef]
- Jing, Q.; Yang, X.; Reng, Q. Effect of Neuromuscular Electrical Stimulation in Patients with Post-Stroke Dysphagia. Med. Sci. Technol. 2016, 57, 1–5. [Google Scholar] [CrossRef]
- Langmore, S.E.; McCulloch, T.M.; Krisciunas, G.P.; Lazarus, C.L.; Van Daele, D.J.; Pauloski, B.R.; Rybin, D.; Doros, G. Efficacy of electrical stimulation and exercise for dysphagia in patients with head and neck cancer: A randomized clinical trial. Head Neck 2015, 38, E1221–E1231. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Kim, S.B.; Lee, J.H.; Lee, S.J.; Ri, J.W.; Park, J.G. The Effect of Early Neuromuscular Electrical Stimulation Therapy in Acute/Subacute Ischemic Stroke Patients with Dysphagia. Ann. Rehabil. Med. 2014, 38, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Li, Y.; Huang, R.; Yin, J.; Shen, Y.; Shi, J. The value of adding transcutaneous neuromuscular electrical stimulation (VitalStim) to traditional therapy for post-stroke dysphagia: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2014, 51, 200–206. [Google Scholar]
- Maeda, K.; Koga, T.; Akagi, J. Interferential current sensory stimulation, through the neck skin, improves airway defense and oral nutrition intake in patients with dysphagia: A double-blind randomized controlled trial. Clin. Interv. Aging 2017, 12, 1879–1886. [Google Scholar] [CrossRef] [Green Version]
- Meng, P.; Zhang, S.; Wang, Q.; Wang, P.; Han, C.; Gao, J.; Yue, S. The effect of surface neuromuscular electrical stimulation on patients with post-stroke dysphagia. J. Back Musculoskelet. Rehabil. 2018, 31, 363–370. [Google Scholar] [CrossRef]
- Nam, H.S.; Beom, J.; Oh, B.-M.; Han, T.R. Kinematic Effects of Hyolaryngeal Electrical Stimulation Therapy on Hyoid Excursion and Laryngeal Elevation. Dysphagia 2013, 28, 548–556. [Google Scholar] [CrossRef]
- Oh, D.-H.; Park, J.-S.; Kim, H.-J.; Chang, M.-Y.; Hwang, N.-K. The effect of neuromuscular electrical stimulation with different electrode positions on swallowing in stroke patients with oropharyngeal dysphagia: A randomized trial. J. Back Musculoskelet. Rehabil. 2020, 33, 637–644. [Google Scholar] [CrossRef]
- Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716. [Google Scholar] [CrossRef]
- Park, J.-W.; Kim, Y.; Oh, J.C.; Lee, H.-J. Effortful Swallowing Training Combined with Electrical Stimulation in Post-Stroke Dysphagia: A Randomized Controlled Study. Dysphagia 2012, 27, 521–527. [Google Scholar] [CrossRef]
- Park, J.-S.; Oh, D.-H.; Hwang, N.-K.; Lee, J.H. Effects of neuromuscular electrical stimulation combined with effortful swallowing on post-stroke oropharyngeal dysphagia: A randomised controlled trial. J. Oral Rehabil. 2016, 43, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Oh, D.H.; Hwang, N.K.; Lee, J.H. Effects of neuromuscular electrical stimulation in patients with Parkinson’s disease and dysphagia: A ran-domized, single-blind, placebo-controlled trial. Neurorehabilitation 2018, 42, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Permsirivanich, W.; Tipchatyotin, S.; Wongchai, M.; Leelamanit, V.; Setthawatcharawanich, S.; Sathirapanya, P.; Boonmeeprakob, A. Comparing the effects of rehabilitation swallowing therapy vs. neuromuscular electrical stimu-lation therapy among stroke Pptients with persistent pharyngeal dysphagia: A randomized controlled study. Med. J. Med. Assoc. Thail. 2009, 92, 259. [Google Scholar]
- Ryu, J.S.; Kang, J.Y.; Park, J.Y.; Nam, S.Y.; Choi, S.H.; Roh, J.L.; Kim, S.Y.; Choi, K.H. The effect of electrical stimulation therapy on dysphagia following treatment for head and neck cancer. Oral Oncol. 2009, 45, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Simonelli, M.; Ruoppolo, G.; Iosa, M.; Morone, G.; Fusco, A.; Grasso, M.G.; Gallo, A.; Paolucci, S. A stimulus for eating. The use of neuromuscular transcutaneous electrical stimulation in patients affected by severe dysphagia after subacute stroke: A pilot randomized controlled trial. Neurorehabilitation 2019, 44, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Song, W.J.; Park, J.H.; Lee, J.H.; Kim, M.Y. Effects of Neuromuscular Electrical Stimulation on Swallowing Functions in Children with Cerebral Palsy: A Pilot Randomised Controlled Trial. Hong Kong J. Occup. Ther. 2015, 25, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Sproson, L.; Pownall, S.; Enderby, P.; Freeman, J. Combined electrical stimulation and exercise for swallow rehabilitation post-stroke: A pilot randomized control trial. Int. J. Lang. Commun. Disord. 2018, 53, 405–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terré, R.; Mearin, F. A randomized controlled study of neuromuscular electrical stimulation in oropharyngeal dysphagia secondary to acquired brain injury. Eur. J. Neurol. 2015, 22, 687-e44. [Google Scholar] [CrossRef]
- Umay, E.K.; Yaylaci, A.; Saylam, G.; Gundogdu, I.; Gurcay, E.; Akcapinar, D.; Kirac, Z. The effect of sensory level electrical stimulation of the masseter muscle in early stroke patients with dysphagia: A randomized controlled study. Neurol. India 2017, 65, 734. [Google Scholar] [CrossRef]
- Umay, E.; Gurcay, E.; Ozturk, E.A.; Akyuz, E.U. Is sensory-level electrical stimulation effective in cerebral palsy children with dysphagia? A randomized controlled clinical trial. Acta Neurol. Belg. 2020, 120, 1097–1105. [Google Scholar] [CrossRef]
- Xia, W.; Zheng, C.; Lei, Q.; Tang, Z.; Hua, Q.; Zhang, Y.; Zhu, S. Treatment of post-stroke dysphagia by vitalstim therapy coupled with conventional swallowing training. J. Huazhong Univ. Sci. Technol. 2011, 31, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Yip, J.; Cui, H.; Guan, L.; Zhu, H.; Zhang, W.; Du, H.; Geng, X. Efficacy of neuromuscular electrical stimulation in improving the negative psychological state in patients with cerebral infarction and dysphagia. Neurol. Res. 2018, 40, 473–479. [Google Scholar] [CrossRef]
- Zhang, M.; Tao, T.; Zhang, Z.-B.; Zhu, X.; Fan, W.-G.; Pu, L.-J.; Chu, L.; Yue, S.-W. Effectiveness of Neuromuscular Electrical Stimulation on Patients with Dysphagia with Medullary Infarction. Arch. Phys. Med. Rehabil. 2016, 97, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Bath, P.M.; Scutt, P.; Love, J.; Clavé, P.; Cohen, D.; Dziewas, R.; Hamdy, S. Pharyngeal electrical stimulation for treatment of dysphagia in subacute stroke: A randomised controlled trial. Stroke 2016, 47, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Dziewas, R.; Stellato, R.; van der Tweel, I.; Walther, E.; Werner, C.J.; Braun, T.; Citerio, G.; Jandl, M.; Friedrichs, M.; Nötzel, K.; et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST-TRAC): A prospective, single-blinded, randomised trial. Lancet Neurol. 2018, 17, 849–859. [Google Scholar] [CrossRef]
- Essa, H.; Vasant, D.H.; Raginis-Zborowska, A.; Payton, A.; Michou, E.; Hamdy, S. The BDNF polymorphism Val66Met may be predictive of swallowing improvement post pharyngeal electrical stimulation in dysphagic stroke patients. Neurogastroenterol. Motil. 2017, 29, e13062. [Google Scholar] [CrossRef] [PubMed]
- Fraser, C.; Power, M.; Hamdy, S.; Rothwell, J.; Hobday, D.; Hollander, I.; Tyrell, P.; Hobson, A.; Williams, S.; Thompson, D. Driving Plasticity in Human Adult Motor Cortex Is Associated with Improved Motor Function after Brain Injury. Neuron 2002, 34, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Jayasekeran, V.; Singh, S.; Tyrrell, P.; Michou, E.; Jefferson, S.; Mistry, S.; Gamble, E.; Rothwell, J.; Thompson, D.; Hamdy, S. Adjunctive functional pharyngeal elctrical stimulation reverses swallowing disability after brain lesions. Gastroentrology 2010, 138, 1737–1746. [Google Scholar] [CrossRef] [Green Version]
- Restivo, D.A.; Casabona, A.; Centonze, D.; Ragona, R.M.; Maimone, D.; Pavone, A. Pharyngeal Electrical Stimulation for Dysphagia Associated with Multiple Sclerosis: A Pilot Study. Brain Stimul. 2013, 6, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Suntrup, S.; Marian, T.; Schröder, J.B.; Suttrup, I.; Muhle, P.; Oelenberg, S.; Hamacher, C.; Minnerup, J.; Warnecke, T.; Dziewas, R. Electrical pharyngeal stimulation for dysphagia treatment in tracheotomized stroke patients: A randomized controlled trial. Intensiv. Care Med. 2015, 41, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Vasant, D.H.; Michou, E.; O’Leary, N.; Vail, A.; Mistry, S.; Hamdy, S.; Greater Manchester Stroke Research Network. Pharyngeal electrical stimulation in dysphagia poststroke: A prospective, randomized single-blinded interventional study. Neurorehabilit. Neural Repair 2016, 30, 866–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabib, C.; Nascimento, W.; Rofes, L.; Arreola, V.; Tomsen, N.; Mundet, L.; Palomeras, E.; Michou, E.; Clavé, P.; Ortega, O. Short-term neurophysiological effects of sensory pathway neurorehabilitation strategies on chronic post-stroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.-B.; Lee, H.-J.; Yoo, J.; Kwon, Y.-G. Effect of Low-Frequency rTMS and NMES on Subacute Unilateral Hemispheric Stroke with Dysphagia. Ann. Rehabil. Med. 2014, 38, 592–602. [Google Scholar] [CrossRef]
- Michou, E.; Mistry, S.; Jefferson, S.; Tyrrell, P.; Hamdy, S. Characterizing the Mechanisms of Central and Peripheral Forms of Neurostimulation in Chronic Dysphagic Stroke Patients. Brain Stimul. 2014, 7, 66–73. [Google Scholar] [CrossRef]
- Zhang, C.; Zheng, X.; Lu, R.; Yun, W.; Yun, H.; Zhou, X. Repetitive transcranial magnetic stimulation in combination with neuromuscular electrical stimulation for treatment of post-stroke dysphagia. J. Int. Med. Res. 2019, 47, 662–672. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database and Search Terms | Number of Records |
|---|---|
| Cinahl: ((MH “Deglutition”) OR (MH “Deglutition Disorders”)) AND (MH “Randomized Controlled Trials”) | 239 |
| Embase: (swallowing/OR dysphagia/) AND (randomization/or randomized controlled trial/OR “randomized controlled trial (topic)”/OR controlled clinical trial/) | 4550 |
| PsycINFO: (swallowing/OR dysphagia/) AND (RCT OR (Randomised AND Controlled AND Trial) OR (Randomized AND Clinical AND Trial) OR (Randomised AND Clinical AND Trial) OR (Controlled AND Clinical AND Trial)).af. | 231 |
| PubMed: (“Deglutition”[Mesh] OR “Deglutition Disorders”[Mesh]) AND (“Randomized Controlled Trial” [Publication Type] OR “Randomized Controlled Trials as Topic”[Mesh] OR “Controlled Clinical Trial” [Publication Type] OR “Pragmatic Clinical Trials as Topic”[Mesh]) | 3039 |
Study
| Inclusion/Exclusion Criteria | Sample (N)
| Group Descriptives (Mean ± SD) Age, Gender, Medical Diagnoses |
|---|---|---|---|
| NeuroMuscular Electrical Stimulation (NMES) a—n = 30 | |||
Beom, et al. [28]
|
| n = 132
| Treatment group 1: Age 64.4 ± 12.0 50% male Location of lesion: cortex (29), subcortex (20), brainstem (16), cerebellum (1) Treatment group 2: Age 59.8 ± 15.9 66.6% male Location of lesion: cortex (29), subcortex (14), brainstem (19), cerebellum (4) NS difference between groups |
Bülow, et al. [29]
|
| n = 25
| Combined treatment groups data: 64% male Treatment group 1: Age 71 (SD not reported) Treatment group 2: Age 70 Statistical difference between groups = NR |
El-Tamawy, et al. [30]
|
| n = 30
| Treatment group 1: Age 61.5 ± 7.3 Control group 2: Age 61.3 ± 6.6 No further details on subjects within the groups. |
Guillén-Solà, et al. [31]
|
| n = 62
| Treatment 1: Age = 68.9 ± 7 Male = 57.1% Treatment 2: Age = 67.9 ± 10.6 Male = 76.2% Treatment 3: Age = 70.3 ± 8.4 Male = 47.6% NS differences between groups |
Heijnen, et al. [32]
|
| n = 85
| Treatment group 1: median age 69 78.6% male Treatment group 2: median age 65 74.1% male Treatment group 3: median age 66 76.7% male NS differences between groups |
Huang, et al. [33]
|
| n = 29
| Treatment group 1: Age 67.0 ± 10.1 54.5% male Infarction (9); haemorrhage (2) Treatment group 2: Age 64.5 ± 14.4 62.5% male Infarction (6); haemorrhage (2) Treatment group 3: Age 68.9 ± 9.8 90% male Infarction (9); haemorrhage (1) NS differences between groups |
Huh, et al. [34]
|
| n = 31
| Treatment group 1: Age 64.8 ± 14.1 90% male Infarction 6, haemorrhage 4 Treatment group 2: Age 60.45 ± 16.2 72.7% male Infarction 4, haemorrhage 7 Treatment group 3: Age 62.40 ± 12.7 50% male Infarction 4, haemorrhage 6 NS differences between groups |
Jing, et al. [35]
|
| n = 60
| Treatment group 1: Age 67.9 ± 11.4 63.3% male 63% unilateral, 47% bilateral stroke, 70% infarction, 30% haemorrhage Treatment group 2: Age 68.6 ± 12.5 53.3% male 70% unilateral, 30% bilateral stroke, 77% infarction, 23% haemorrhage Statistical difference between groups = NR |
Langmore, et al. [36]
|
| n = 127
| Treatment group 1: Age 62.1 + 9.2 86.2% male RT site: Oral—9.5%, Nasopharynx—8.6%, Oropharynx—47.4%, Hypopharynx—12.1%, Larynx—11.2%, Other—12.1% Stage: 1—7.4% 2—7.4% 3—21.1% 4—64.2% Sham/Treatment group 2: Age 61.5 + 10.6 84.6% male RT site: Oral—5.9%, Nasopharynx—13.7%, Oropharynx—45.1%, Hypopharynx—17.6%, Larynx—17.6%, Other—7.8% Stage: 1—0% 2—15.2% 3—13% 4—71.7% NS difference between groups |
Lee, et al. [37]
|
| n = 57
| Treatment group 1: Age 63.5 ± 11.4 years 71% male Lesion location: right (13), left (18) Cortical (5), subcortical (26) Treatment group 2: Age: 66.7 ± 9.5 years 77% male Lesion location: right (11), left (15) Cortical (4), subcortical (22) NS difference between groups |
Li, et al. [38]
|
| n = 135
38, 40 and 40 patients in groups 1–3 respectively, completed the treatment. All descriptive data about groups given based on originally enrolled numbers. | Treatment group 1: Age 66.7 ± 14.6 53% male 44% haemorrhage, 56% infarct. Treatment group 2: Age 65.8 ± 13.2 49% male 49% haemorrhage, 51% infarct. Treatment group 3: Age 66.1 ± 13.1 51% male 47% haemorrhage, 53% infarct. NS differences between groups |
Maeda, et al. [39]
|
| n = 43
| Treatment group: Age 82.7 ± 8.0 45.5% male Primary reason for admission: Dysphagia rehabilitation 63.6%; aspiration pneumonia 27.3%; other 9.1% Sham group 2: Age 86.0 ± 6.7 38.1% male Primary reason for admission: Dysphagia rehabilitation 42.9%; aspiration pneumonia 33.3%; other 23.8% NS differences between groups |
Meng, et al. [40]
|
| n = 30
| Treatment group 1: Age 65.2 ± 10.7 70% male 80% infarction, 20% haemorrhage. Treatment group 2: Age 67.2 ± 15.8 60% male 70% infarction, 30% haemorrhage. Treatment group 3: Age 64.4 ± 9.0 70% male 70% infarction, 30% haemorrhage. NS differences between groups |
Nam, et al. [41]
|
| n = 50
| Treatment group 1: Age 62.3 ± 11.4 52% male Location of lesion: cortex 13, subcortex 6, brainstem 5, cerebellum 1 Treatment group 2: Age 60.9 ± 12.3 56% male Location of lesion: cortex 10, subcortex 8, brainstem 6, cerebellum 1 NS differences between groups |
Oh, et al. [42]
|
| n = 26
| Treatment group 1: Age 56.3 ± 13.3 50% male Site of stroke lesion: middle cerebral artery (8), midbrain (1), frontal lobe (2), internal capsule (2), corona radiate (1) Treatment group 2: Age 58.7 ± 14.8 41.7% male Site of stroke lesion: middle cerebral artery (7), midbrain (1), frontal lobe (1), internal capsule (2), corona radiate (1) NS differences between groups |
Ortega, et al. [43]
|
| n = 38
| Treatment group 1: Age 81.2 ± 5.6 42.1% male Dysphagia cause: elderly (8), stroke (8), neurodegenerative disease (3) Treatment group 2: Age 79.8 ± 4.8 47.4% male Dysphagia cause: elderly (7), stroke (8), neurodegenerative disease (3) NS difference between groups. |
Park, et al. [44]
|
| n = 18
| Treatment group 1: Age 68.7 ± 12.8 56% intracranial haemorrhage (ICH), 44% infarct. Treatment group 2: Age 62.0 ± 17.2 78% ICH, 22% infarct. Gender reported at cohort level: 88% male. NS differences between groups |
Park, et al. [45]
|
| n = 50
| Treatment group 1: Age 54 ± 11.93 48% male Infarct = 14, haemorrhage = 11 Treatment group 2: Age 55.8 ± 12.23 56% male Infarct = 12, haemorrhage = 13 NS differences between groups |
Park, et al. [46]
|
| n = 18
| Treatment group: Age 63.44 ± 13.55 55% male Treatment group 2: 54.67 ± 13.82 33% male NB. Patients’ medical diagnosis: stroke (Table 1) [Error?] NS differences between groups |
Permsirivanich, et al. [47]
|
| n = 23
| Treatment group 1: Age 64.7 ± 9.4 36.4% male Type of stroke: infarction 81.8%, haemorrhage 18.2% Treatment group 2: Age 64.5 ± 8.8 41.7% male Type of stroke: infarction 75%, haemorrhage 25% NS differences between groups |
Ryu, et al. [48]
|
| n = 26
| Treatment group 1: Age 63.4 ± 7.3 100% male Larynx ca = 6 Hypopharynx ca = 3 Oropharynx = 4 Oral =1 T1-T2 = 6 T3-T4 = 8 Sham/Treatment group 2: Age 60.8 ± 12.0 92% male Larynx ca = 5 Hypopharynx ca = 1 Oropharynx = 4 Oral =2 T1-T2 = 7 T3-T4 = 4 Unknown = 1 Statistical difference between groups = NR |
Simonelli, et al. [49]
|
| n = 33
| Treatment group 1: Age 67.2 ± 16.2 62.5% male (10?) Left CVA (4), right CVA (6), Other (6) Treatment group 2: Age 72.4 ± 12.3 37.5% male (6) Left CVA (6), right CVA (6), Other (3) NS differences between groups. |
Song, et al. [50]
|
| n = 20
| Treatment group 1: Age = 6.20 ± 2.78 70% male CP type: Hemiplegia = 2 Diplegia = 5 Quadriplegia = 3 Flaccid = 0 Sham/Treatment group 2: Age = 6.00 ± 2.40 60% male CP type: Hemiplegia = 4 Diplegia = 3 Quadriplegia = 2 Flaccid = 1 NS differences between groups. |
Sproson, et al. [51]
|
| n = 24
| Treatment group 1: Age 76 ± 11.4 67% male 33% >1 stroke event Time post-stroke 17.3 months ± 25.0 Usual care group 2: Age 79 ± 11.4 66.7% male 33% >1 stroke event Time post-stroke 9.1 months ± 20.5 Significant difference between groups = NR. |
Terré and Mearin [52]
|
| n = 20
| Treatment group 1: Age 46.0 ± 16 60% male 70% stroke, (haemorrhagic = 5, ischaemic = 2) 30% TBI Sham/Treatment group 2: Age 51 ± 23 60% male 70% stroke (haemorrhagic = 6, ischaemic = 1) 30% TBI Significant difference between groups = NR. |
Umay, et al. [53]
|
| n = 98
| Treatment group 1: Age 61.03 ± 10.05 70.7% male 87.9% middle cerebral artery (MCA) stroke, 12.1% posterior inferior cerebellar (PICA) stroke Sham/Treatment group 2: Age 62.40 ± 9.93 87.5% male 87.5% middle cerebral artery (MCA) stroke, 12.5% posterior inferior cerebellar (PICA) stroke NS difference between groups. |
Umay, et al. [54]
|
| n = 102
| Treatment group 1: Age 51.97 ± 24.46 months 56% male Motor function status as per GMFCS (I = walks with no limitations, V = wheelchair). I = 0 II = 7 III = 10 IV = 22 V = 13 Sham/Treatment group 2: Age 47.95 ± 23.18 months 46% male I = 0 II = 11 III = 11 IV = 16 V = 12 NS difference between groups. |
Xia, et al. [55]
|
| n = 120
| Treatment group 1: Age 65.32 ± 14.29 62.5% male 42.5% haemorrhage, 45% infarct, 12.5% other stroke. Treatment group 2: Age 66.40 ± 15.63 57.5% male 35% haemorrhage, 55% infarct, 10% other stroke. Treatment group 3: Age 65.85 ± 14.63 70% male 32.5% haemorrhage, 62.5% infarct, 0.5% other stroke. NS difference between groups. |
Zeng, et al. [56]
|
| n = 112
| Treatment group 1: Age 66.13 ± 13.03 73.5% male NIHSS score = 4.25 ± 2.45 Treatment group 2: Age 67.92 ± 12.31 69.4% male NIHSS score = 5.02 ± 2.32 NS differences between groups at baseline. |
Zhang, et al. [57]
|
| n = 82
| Treatment group 1: Age 62.6 ± 8.7 62.9% male Time since infarct: 21.3 ± 4.1 days Treatment group 2: Age 61.3 ± 7.1 57.1% male Time since infarct: 22.1 ± 4.0 days Treatment group 3: Age 62.2 ± 9.2 70.3% male Time since infarct: 20.6 ± 4.3 days NS differences between groups. |
| Pharyngeal Electrical Stimulation (PES)—n = 8 | |||
Bath, et al. [58]
|
| n = 162
| Treatment group: Age = 74.4 ±11.2 Male = 55.2% Ischaemic stroke = 89.5% Haemorrhagic = 10.5% PAS >2 in 90.8% Sham group: Age = 74.9 ± 12.6 Male = 61.3% Ischaemic stroke = 88% Haemorrhagic = 10.7% (Non-stroke = 1.3%) PAS > 2 in 92% NS difference between groups |
Dziewas, et al. [59]
|
| n = 69
2nd open label treatment: Delayed group (n = 30) - Sham group still with a tracheostomy received late treatment; Retreat group (n = 16) PES group still with a tracheostomy received a 2nd treatment | Treatment group: Age = 61.7 ± 13 Male = 69% Sham group: Age = 66.8 ± 10.3 Male = 59% NS differences between groups |
Essa, et al. [60]
|
| n = 16
| Treatment group: Age 58.6 ± 13.4 62.5% male Stroke type: infarct (7), bleed (1) Sham group: Age 70.5 ± 11.8 62.5% male Stroke type: infarct (7), bleed (1) NS differences between groups. |
Fraser, et al. [61]
|
| n = 16
| Descriptive statistics only Treatment group: Age range 65–93 60% male Sham group: Age range 56–78 66.6% male Statistical difference between groups = NR |
Jayasekeran, et al. [62]
|
| Protocol 1 (active or sham PES on virtual lesion) n = 11 (+2 for reversal of swallowing behaviour) Patients their own controls. Protocol 2 (PES with varying dose) n = 22
n = 28
| Protocol 1: Age range 24–47 yrs 45.5% male (no data on treatment and sham groups separately) Protocols 2 and 3: Age 74 ± 10 68% male (No consistent data on treatment and sham groups separately for both protocols) Difference between groups NS |
Restivo, et al. [63]
|
| n = 20
| Cohort demographics supplied, no group descriptives given. Mean age = 39.7 ± 6.5 years 35% male Relapsing-remitting MS = 14, Secondary progressive MS = 6 Mean EDSS = 5.7 ± 0.8; mean disease duration = 9.8 ± 2.4 years; mean dysphagia duration = 22.0 ± 7.4 months Statistical difference between groups = NR |
Suntrup, et al. [64]
|
| n = 30
| Treatment group: Age 63.0 ± 14.5 years 45% male 90% ischaemic, 10% haemorrhagic stroke. 70% supratentorial, 30% infratentorial Sham group: Age: 66.7 ± 14.5 years 60% male 80% ischaemic, 20% haemorrhagic stroke. 90% supratentorial, 10% infratentorial Difference between groups NS |
Vasant, et al. [65]
|
| n = 35 at 2 weeks post treatment, n = 33 at 3 months post treatment.
| Treatment group: (median) age = 71 Interquartile range (IQR) =56–79. 50% male NIHSS: median score = 10.0 (IQR= 5.2, 18.5) Sham group: (median) age = 71 (IQR = 61–78) 72% male NIHSS: median score = 12.5 (IQR = 9.2, 16.8) No other stroke, site of lesion details reported. NS differences between groups. |
| Combined Neurostimulation Interventions—n = 4 | |||
Cabib, et al. [66]
|
| n = 36
| Treatment group 1: Age 70.0 ± 8.6 75% male 0% haemorrhage, 100% infarct. Treatment group 2: Age 74.3 ± 7.8 58% male 8% haemorrhage, 92% infarction Treatment group 3: Age 70.0 ± 14.2 92% male 25% haemorrhage, 75% infarction Difference between groups NS |
Lim, et al. [67]
|
| n = 47
| Treatment group 1: Age 62.5 ± 8.2 60% male 34% haemorrhage, 66% infarction Treatment group 2: Age 59.8 ± 11.8 43% male 71% haemorrhage, 29% infarction Treatment group 3: Age 66.3 ± 15.4 67% male 66% haemorrhage, 44% infarction Difference between groups NS |
Michou, et al. [68]
|
| n = 18
| Treatment group: Avg age 60.3 83% male Treatment group 2: Avg age 67.3 100% male Treatment group 3: Avg age 67.8 66.7% male Overall: 63 ± 15 weeks post stroke with 7.6 ± 1 on NIHHS Statistical difference between groups = NR |
Zhang, et al. [69]
|
| n = 64
| Treatment group 1: Age 55.9 ± 8.9 43% male 61.5% subcortical, 38.5% brainstem Treatment group 2: Age 56.8 ± 9.7 54% male 30.8% subcortical, 69.2% brainstem Treatment group 3: Age 56.5 ± 10.1 50% male 58.3% subcortical, 41.7% brainstem Treatment group 4: Age 53.1 ± 10.6 31% male 61.5% subcortical, 38.5% brainstem * All data given on participants that finished the trial and follow-up period (n = 52) |
| Study | Intervention Goal | Procedure, Delivery and Dosage Per Intervention Group | Outcome Measures | Intervention Outcomes/Conclusions |
|---|---|---|---|---|
| NeuroMuscular Electrical Stimulation (NMES) a—n = 30 | ||||
| Beom, et al. [28] | To investigate the effectiveness of NMES to suprahyoid muscle compared with NMES to infrahyoid muscle in brain-injured (stroke) patients with dysphagia | Procedure:
| Primary outcomes: FDS b; SFS; aspiration/penetration based off VFSS pre and post treatment. Secondary outcome: N/R |
|
| Bülow, et al. [29] | To evaluate and compare the outcome of NMES versus traditional swallowing therapy (TT) in stroke patients | Procedure:
| Primary outcomes: Patient reported VAS (swallowing complaints); VFSS measure b (performed day of last treatment). Secondary outcome: N/R |
|
| El-Tamawy, et al. [30] | Assess the effect of NMES and physical therapy program on severe poststroke dysphagia | Treatment group 1:
Standard medical treatment only | Primary outcomes: Swallowing variables (OTT, hyoid elevation, laryngeal elevation, oesophageal sphincter opening, aspiration/penetration) as per VFSS. Secondary outcome: N/R |
|
| Guillén-Solà, et al. [31] | Assess the therapeutic effectiveness of NMES and inspiratory and expiratory muscle training (IEMT) in dysphagic subacute stroke patients, compared to standard swallow therapy (DT) |
IEMT: 5 sets of 10 respirations twice a day 5 days per week for 3 weeks. Loads were set to 30% of max insp and exp pressures, increased weekly by 10 cm H2O Sham IEMT: same frequency, but with set workloads of 10 cm H2O NMES: 40 min a day 5 days per week for 3 weeks at 80 Hz on suprahyoid muscles | Primary outcomes: Max inspiratory + expiratory muscle function (MicroRPM), dysphagia severity (VFSS, PAS), respiratory complications. Secondary outcomes: Swallowing parameter changes as per voice changes, coughing, desaturation (>3%), piecemeal deglutition, oropharyngeal residue (V-VST), FOIS, DOSS. (Not reported in study) Assessed at baseline, 3 weeks post (by V-VST), and 3 months post intervention (VFSS). | Respiratory muscle strength:
|
| Heijnen, et al., [32] | To compare the effects of traditional speech therapy exercises to those combined with NMES on motor or sensory level on dysphagia and quality of life of patients with Parkinson’s Disease | Procedure:
| Primary outcomes: Health related quality of life (SWAL-QOL; MDADI). Secondary outcomes: Dysphagia severity (single-item Dysphagia Severity Scale) |
|
| Huang, et al. [33] | To compare functional dysphagia recovery in acute stroke patients using traditional dysphagia therapy, NMES or the two combined | Procedure:
| Primary outcomes: FOIS, PAS, FDS as per VFSS before and after treatment. Secondary outcome: N/R |
|
| Huh, et al. [34] | To investigate the effect of different electrode placement in NMES in poststroke dysphagia rehabilitation | Procedure:
| Primary outcomes: VFSS performed at baseline and post treatment.
Secondary outcome: N/R |
|
| Jing, et al. [35] | To investigate the effect of NMES on post stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
| Primary outcomes: Swallow efficacy, swallow function scores, laryngeal elevation, severity of aspiration, amount of food intake, residue scores. All based on Rattans dysphagia classification criteria. Secondary outcome: N/R |
|
| Langmore, et al. [36] | To investigate the efficacy of NMES combined with swallow exercises in improving dysphagia post radiotherapy for head & neck cancer | Procedure:
Sham/Treatment group:
| Primary outcome: Swallowing function as measured by PAS on VFSS. Secondary outcomes: OPSE, hyoid excursion, diet measured by the PSS, and quality of life as measured by HNCI. Assessments were performed prior to, midway through (week 7) and at the end of the treatment (week 13). |
Treatment group:
Sham/Treatment group:
|
| Lee, et al. [37] | To compare early NMES combined with DT versus DT only on dysphagia outcomes in acute/subacute ischaemic stroke patients with moderate to severe dysphagia | Procedure:
Treatment group 1:
Treatment group 2:DT only, as per above | Primary outcome: FOIS b as per VFSS at 3, 6, and 12 weeks post treatment. Secondary outcome: N/R |
|
| Li, et al. [38] | To assess whether adding NMES to the conventional swallow therapy improves post-stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
Treatment group 3:
| Primary outcomes: VAS to compare the differences of muscle pain pre and post treatment; SSA, sEMG, OTT, PTT, LCD and Standardised swallowing PAS were measured using VFSS. Secondary outcome: N/R |
|
| Maeda, et al. [39] | To investigate the effect of transcutaneous electrical sensory stimulation (TESS) without muscle contraction in patients undergoing dysphagia rehabilitation | Procedure:
Treatment group:
Sham group:
| Primary outcomes: Cough latency time against 1% citric acid mist. Secondary outcomes: FOIS, oral nutritional intake outcomes measured at study entry, and after the 2nd and 3rd week following treatment initiation |
|
| Meng, et al. [40] | To assess the effectiveness of surface NMES with various electrode placements on patients with post-stroke dysphagia | Procedure:
Treatment Group 1: Electrode placement: 1 pair of electrodes on the surface of both sides of suprahyoid, and another pair on surface of upper and lower edge of thyroid cartilage Treatment Group 2: Electrode placement: 2 pairs of electrodes on the surface of suprahyoid (geniohyoid + mylohyoid) Treatment Group 3: DT | Primary outcomes: VFSS pre and post treatment. Hyoid excursion, DOSS b, WST and RSST. Secondary outcome: N/R |
|
| Nam, et al. [41] | To assess the effect of repeated sessions of NMES with two different electrode placements on dysphagia following brain injury | Procedure:
Treatment Group 1:
Treatment Group 2:
| Primary outcomes: Motion analysis of the hyolaryngeal excursion according to VFSS conducted before and after the treatment Secondary outcome: N/R |
|
| Oh, et al. [42] | To identify the effects of NMES with two different electrode placements on post-stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
| Primary outcomes: VDS, PAS b and FOIS Secondary outcome: N/R |
|
| Ortega, et al. [43] | To evaluate the effectiveness of two different sensory stimulation treatments on oropharyngeal dysphagia in the elderly | Procedure:
Treatment group 1:
Treatment group 2:
| Primary outcome: VFSS measurements, PAS (measured before and 5 days after the treatment) Secondary outcomes: EAT-10, V-VST, |
|
| Park, et al. [44] | To determine whether effortful swallow training combined with surface electrical stimulation as a form of resistance training has an effect on post-stroke dysphagia | Procedure: NMES with VitalStim, 2 sets of electrodes placed on infrahyoid muscles (working against resistance)
Treatment group 1:
Treatment group 2: Effortful swallow + NMES (non-treatment level) | Primary outcome: Hyolaryngeal excursion (max anterior hyoid displacement, max vertical hyoid displacement), maximum vertical laryngeal displacement, UES opening (width), PAS (as per VFSS), pre and post treatment. Secondary outcome: N/R |
Treatment group 1:
Treatment group 2:
|
| Park, et al. [45] | To investigate the effects of effortful swallowing combined with NMES on hyoid bone movement and swallowing function in stroke patients | Procedure: NMES (VitalStim, as per protocol), electrodes placed on infrahyoid muscles (targeting sternohyoid muscle, working against resistance) Delivery and dosage: 30 min per session, 5 sessions a week for 6 weeks. Treatment group 1:
Treatment group 2:
| Primary outcomes: As per VDS pre and post treatment (6 weeks). Kinematics of the hyoid bone (analysed with Image J Program); swallow function (as per VDS and PAS b); VDS measures: Oral phase (lip closure, bolus formation, mastication, apraxia, tongue to palate contact, premature bolus loss and OTT); Pharyngeal phase (pharyngeal triggering, vallecular residues, pyriform sinus resides, laryngeal elevation, pharyngeal wall coating, pharyngeal transit time and aspiration). Secondary outcome: N/R |
Treatment group 1:
Treatment group 2:
|
| Park, et al. [46] | To identify the effect of effortful swallowing combined with neuromuscular electrical stimulation NMES in treating dysphagia in Parkinson’s disease | Procedure: NMES (VitalStim) 5 days/week, for 4 weeks, 30 min each session
Treatment group 1:
Treatment group 2:
| Primary outcome: Kinematics of the hyoid bone (analysed with Image J Program); swallow function (as per VDS and PAS b) Secondary outcomes: VDS measures: Oral phase (lip closure, bolus formation, mastication, apraxia, tongue to palate contact, premature bolus loss and OTT); Pharyngeal phase (pharyngeal triggering, vallecular residues, pyriform sinus resides, laryngeal elevation, pharyngeal wall coating, pharyngeal transit time and aspiration) |
|
| Permsirivanich, et al. [47] | To compare the treatment outcomes between dysphagia rehabilitation exercises and NMES in post-stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
| Primary outcomes: Changes in FOIS b, complications related to treatment and number of therapy sessions. VFSS only performed pre-treatment. Secondary outcome: N/R |
|
| Ryu, et al. [48] | To evaluate the effect of NMES on dysphagia following treatment for head and neck cancer | Procedure:
Sham/Treatment group 2: Sham stimulation using low intensity TENS | Primary outcome measures: FDS, CDS, ASHA-NOMS and MDADI Secondary outcome: N/R |
|
| Simonelli, et al. [49] | To investigate the effect of laryngopharyngeal NMES on poststroke dysphagia | Procedure: NMES and/or DT. Treatment 30 min twice daily, 5 days/week for 8 weeks, by SLTs Treatment group 1: NMES (VitalStim) plus DT. Electrode placement 3B (two electrodes were placed just at or above the level of the thyroid notch over the thyrohyoid muscle) Treatment group 2: DT included oral-facial, lingual, laryngeal adduction-elevation exercises, effortful swallow maneuver, Mendelsohn maneuver, Masako maneuver, Shaker exercises and thermal stimulation plus compensatory strategies | Primary outcome: FOIS, PAS b, the Pooling score and the presence of oropharyngeal secretion as per FEES. Secondary outcomes: Diet taken by mouth; the need for postural compensations and the duration of the dysphagia training. |
|
| Song, et al. [50] | To investigate the effects of NMES and oral sensorimotor treatment (OST) on dysphagia in children with CP | Procedure: OST followed by NMES (20min) with thickened fluid, delivered by occupational therapist
Sham/Treatment group:
| Primary outcomes: (1) BASOFF: jaw closure, lip closure over a spoon, tongue control, lip closure while swallowing, swallowing food without excess loss, chewing food (tongue/jaw control), sipping liquids, swallowing liquids without excess loss, and swallowing food without coughing; (2) ASHA-NOMS. Secondary outcome: N/R |
|
| Sproson, et al. [51] | To investigate the efficacy of the Ampcare Effective Swallowing Protocol (ESP), combining NMES with swallow-strengthening exercises, compared with usual care in the treatment of dysphagia post-stroke | Procedure: NMES to suprahyoid muscles via AmpCare ESP Treatment group 1:
Usual Care Group 2:
| Primary outcomes: (1) FOIS and PAS b immediately post treatment as per VFSS; (2) FOIS, PAS and SWAL-QOL 1 month follow-up. Secondary outcome: N/R |
|
| Terré, et al. [52] | To evaluate the effectiveness of neuromuscular electrical stimulation NMES treatment in patients with oropharyngeal dysphagia secondary to acquired brain injury | Procedure: NMES (VitalStim), or sham, + traditional dysphagia therapy,
Sham/Treatment group 2: Sham NMES + DT
| Primary outcome: FOIS Secondary outcomes: VFSS parameters, pharyngo-esophageal manometry Assessed at 1 month (immediately post therapy) and at 3 months. |
|
| Umay, et al. [53] | To evaluate the effects of sensory electrical stimulation (SES) to bilateral masseter muscles in early stroke patients with dysphagia | Procedure: Sensory level electrical stimulation (Intelect Advanced) with galvanic stimulation to bilateral masseter muscles for 60 min, 5 days/week, for 4 weeks Treatment group 1:
| Primary outcomes: Bedside dysphagia score (from water swallow test, pulse oximetry), total dysphagia score, MASA, NEDS. Secondary outcome: N/R |
|
| Umay, et al. [54] | To investigate the effects of sensory-level electrical stimulation NMES treatment applied to bilateral masseter muscles at the lowest current level combined with conventional dysphagia rehabilitation in children with CP who had any oropharyngeal dysphagia symptoms | Procedure:
Treatment group 1:
and dietary modification. Oral motor exercises included for children who could participate. Sham/Treatment group 2:
| Primary outcome: Ped EAT-10, FEES; Secondary outcomes: Clinical Feeding Evaluation. |
|
| Xia, et al. [55] | To investigate the effects of VitalStim therapy coupled with conventional swallowing training on recovery of post-stroke dysphagia | Treatment group 1:
Treatment group 2:
Treatment group 3:
| Primary outcome: Dysphagia Rating Scale b (as per VFSS); Secondary outcomes: Maximum amplitude of surface electromyography (sEMG) signals of hyoid muscles; SWAL-QOL. |
|
| Zeng, et al. [56] | To observe the improvement of swallow function and negative affect disorders in patients with cerebral infarction and dysphagia by NMES | Procedure:
Treatment group 1:
Treatment group 2:
| Primary outcome: Swallow function as per Kubota water-drinking test; Secondary outcomes: Negative affect disorders as per Hamilton anxiety scale and depression scale test. |
|
| Zhang, et al. [57] | To evaluate and compare the effects of NMES acting on the sensory input versus motor muscle in treating patients with dysphagia with medullary infarction | Procedure:
Treatment group 1:
Treatment group 2, DT + sensory NMES:
Treatment group 3, DT + motor NMES:
| Primary outcomes: WST, FOIS, SWAL-QOL, SSA. Secondary outcome: N/R |
|
| Pharyngeal Electrical Stimulation (PES)—n = 8 | ||||
| Bath, et al. [58] | Assess the efficacy of PES in treating subacute poststroke dysphagia | Procedure: PES (Phagenyx) catheter + standard stroke care
Treatment group:
Sham:
| Primary outcome: PAS b (via VFSS), assessed at 2 and 12 weeks post treatment. 3–7 bolus per VFSS. Secondary outcome: At 2, 6 and 12 weeks = DSRS, function (Barthel Index), dependency (modified Rankin Scale), impairment (NIHSS), quality of life (EQ-5D), nutritional measures and serious adverse events (chest infections, pneumonia, death). |
|
| Dziewas, et al. [59] | Assess the safety and efficacy of PES in accelerating dysphagia rehabilitation and enabling decannulation of tracheostomised stroke patients | Procedure: PES (Phagenyx)
Treatment group:
Sham group:
Open label PES group:
| Primary outcome: Readiness for decannulation 24–72 h after treatment (determined by FEES protocol) Secondary outcomes: delayed improvement in Open label group; recannulations (between 2–30 days post decannulation/discharge); DSRS; FOIS; stroke severity as per modified Rankin Scale and NIHSS; LOS, SLT plan, number and type of adverse events. | Primary outcomes: 17/35 patients (49%) ready for decannulation versus sham 3/34 (9%) patients. Significant difference (p < 0.001) between groups Secondary outcomes: Open-label PES (a) Retreated group = 4/15 (27%) ready for decannulation (b) Sham/delayed treatment group = 16/30 (53%) ready for decannulation. No significant differences between groups. |
| Essa, et al. [60] | Assess if The Brain Derived Neurotrophic Factor (BDNF) genotype can influence swallowing recovery post PES in stroke patients | Procedure:
Sham group Sham PES | Primary outcome: DSRS. Assessed at baseline, 2 weeks and 3 months post treatment. Secondary outcome: N/R |
|
| Fraser, et al. [61] | To assess the effect of PES on swallow function in hemispheric stroke patients | Procedure:
| Primary outcomes: PTT, swallowing response time, PAS Secondary outcome: N/R | Between group statistics = NR
|
| Jayasekeran, et al. [62] | To examine the role of PES in expediting human swallowing recovery after experimental (virtual) and actual (stroke) lesions | Agent: PES Protocol 1—active or sham PES with virtual lesion Patients their own controls. The two studies (active or sham) took place at least 1 week apart. Protocol 2—PES with varying treatment intensity (times/day) and dose (total number of days)
Protocol 3—active or sham PES with acute stroke. Once daily on three consecutive days. | Primary outcomes: Protocol 1 Cortical excitability, swallow timeliness Protocol 2 PAS b Protocol 3 PAS b, swallow timing, DSRS, LOS at hospital, Barthel Index. For protocols 2 and 3, VFSS conducted before treatment, and again weeks later. Secondary outcome: N/R | Protocol 1
Protocol 2
Protocol 3
|
| Restivo, et al. [63] | To investigate whether intraluminal electrical pharyngeal stimulation facilitates swallowing recovery in dysphagic multiple sclerosis (MS) patients | Procedure: PES (bipolar platinum pharyngeal ring electrodes built into 3 mm-diameter intraluminal catheter) using constant/current electrical simulator (DS7)
Treatment group:
Sham:
| Primary outcome: PAS via VFSS at pre-treatment (T0), immediately after treatment (T1), after two (T2), and four (T3) weeks of PES. Secondary outcomes: sEMG measure of: (1) duration of laryngeal excursion; (2) duration of the sEMG activity of suprahyoid/submental muscles; (3) duration of the inhibition of the CP muscle; and (4) interval between onset of suprahyoid/submental muscles and onset of laryngeal elevation. |
|
| Suntrup, et al. [64] | To assess the effectiveness of PES on swallowing function of severely dysphagic tracheostomised patients | Procedure: PES (Phagenyx) catheter system and base station, stimuli of 0.2 ms pulse duration at a frequency of 5 Hz with 280 V
Treatment group:
Sham:
Another treatment session was offered to participants who were not eligible for tracheostomy decannulation post the first treatment session. | Primary outcome: Eligibility for decannulation Secondary outcomes:FOIS at discharge; mRS; LOS in ICU and hospital; time from stimulation to discharge. |
|
| Vasant, et al. [65] | To assess the effectiveness of PES on swallowing in poststroke dysphagia, with clinical effects in longer-term follow-up | Procedure: PES (Gaeltec catheter) inserted nasally or orally (patient preference)
Treatment group:
Sham:
| Primary outcome: DSRS at 2 weeks post treatment. Secondary outcomes: DSRS at 3 months, feeding method, PAS b (as per MBS/FEES), number of adverse events (chest infections, death). |
|
| Combined Neurostimulation Interventions—n = 4 | ||||
| Cabib et al. [66] | To investigate the effect of repetitive transcranial magnetic stimulation (rTMS) of the primary sensory cortex (A), oral capsaicin (B) and intra-pharyngeal electrical stimulation (IPES; C) on post stroke dysphagia | Procedure: All patients received both treatment and sham, cross over active/sham in visits 1 week apart (randomised). Assessment occurred immediately prior to treatment and within 2 h post treatment. Treatment group 1: rTMS (Magstim rapid stimulator)
Treatment group 2: Capsaicin stimulus (10−5 M) or placebo (potassium sorbate) were administered once in a 100 mL solution Treatment group 3: PES via two-ring electrode naso-pharyngeal catheter (Gaeltec Ltd)
| Primary outcomes: Effect size pre-post treatment for neurophysiological variables (pharyngeal and thenar RMT and MEP). Secondary outcomes: Effects on the biomechanics of swallow (PAS b, impaired efficiency + more) VFSS before and after treatment |
Primary outcomes:
Secondary outcomes: (VFSS)
|
| Lim, et al. [67] | To investigate the effect of low-frequency repetitive transcranial magnetic stimulation (rTMS) and neuromuscular electrical stimulation (NMES) on post-stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
Treatment group 3:
| Primary outcomes: VFSS baseline, 2 weeks + 4 weeks post treatment (for semi-solids and liquids) FDS, PTT, PAS. Secondary outcome: N/R |
|
| Michou, et al. [68] | To compare the effects of a single application of one of three neurostimulation techniques (PES, paired stimulation, rTMS) on swallow safety and neurophysiological mechanisms in chronic post-stroke dysphagia | Procedure:
Treatment group 1:
Treatment group 2:
Treatment group 3:
| Primary Outcome: VFSS before and after treatment (PAS b) Secondary outcomes: Percentage change in cortical excitability; OTT, pharyngeal response time, PTT, airway closure time and upper oesophageal opening time as per VFSS |
Corticobulbar excitability of pharyngeal motor cortex was beneficially modulated by PES, Paired Stimulation and to a lesser extent by rTMS |
| Zhang, et al. [69] | To determine whether repetitive transcranial magnetic stimulation (rTMS) combined with neuromuscular electrical stimulation (NMES) effectively ameliorates dysphagia and how rTMS protocols (bilateral vs. unilateral) combined with NMES can be optimized | Procedure:
Treatment group 1: Sham rTMS + NMES
Treatment group 2: Ipsilateral rTMS + NMES 10 Hz real rTMS was delivered to the hot spot for the mylohyoid muscle at the ipsilesional hemisphere followed by 1 Hz sham rTMS over the corresponding position of the contralesional hemisphere. Treatment group 3: Contralateral rTMS + NMES 10 Hz sham rTMS was delivered to the hot spot for the mylohyoid muscle at the ipsilesional hemisphere followed by 1-Hz real rTMS over the corresponding position of the contralesional hemisphere Treatment group 4: Bilateral rTMS + NMES 10 Hz real rTMS was delivered to the hot spot for the mylohyoid muscle at the ipsilesional hemisphere followed by 1-Hz real rTMS over the corresponding position of the contralesional hemisphere | Primary outcome: cortical excitability (amplitude of the motor evoked potential) Secondary outcomes: SSA and DD. | Compared with group 2 or 3 in the affected hemisphere, group 4 displayed a significantly greater % change (p.0.017 and p.0.024, respectively). All groups displayed significant improvements in SSA and DD scores after treatment and at 1-month follow-up. The % change in cortical excitability increased over time in either the affected or unaffected hemisphere in treatment groups 1, 2 and 4 (p < 0.05). In Group 3, the % change in cortical excitability in the unaffected hemisphere significantly decreased after the stimulation course (p < 0.05). Change in SSA and DD scores in group 4 was markedly higher than that in the other three groups at the end of stimulation (p.0.02, p.0.03, and p.0.005) and still higher than that in group 1 at the 1-month follow-up (p.0.01). |
| Neurostimulation | Subgroup | Hedges’ g | Lower Limit CI | Upper Limit CI | Z-Value | p-Value |
|---|---|---|---|---|---|---|
| NMES | Diagnostic groups | |||||
| Aged dysphagia [>65 yrs] (n = 1) | 0.291 | −0.299 | 0.881 | 0.966 | 0.334 | |
| Cerebral palsy (children) (N = 2) | 0.264 | −0.088 | 0.616 | 1.470 | 0.142 | |
| Head and neck cancer (n = 2) | 0.281 | −0.610 | 1.172 | 0.618 | 0.536 | |
| Parkinson’s disease (n = 2) | 0.000 | −0.359 | 0.359 | 0.000 | 1.000 | |
| Stroke (n = 9) | 0.433 | 0.105 | 0.760 | 2.589 | 0.010 * | |
| Intervention types | ||||||
| NMES (n = 2) | 0.134 | −0.247 | 0.515 | 0.688 | 0.492 | |
| NMES + DT (n = 7) | 0.648 | 0.398 | 0.897 | 5.086 | <0.001 * | |
| Time between pre-post (days) | ||||||
| 14 (n = 1) | −0.099 | −0.888 | 0.690 | −0.246 | 0.806 | |
| 21 (n = 1) | 1.013 | 0.466 | 1.559 | 3.631 | <0.001 * | |
| 28 (n = 6) | 0.342 | −0.062 | 0.746 | 1.657 | 0.098 | |
| 56 (n = 1) | 0.751 | 0.040 | 1.462 | 2.069 | 0.039 * | |
| Outcome measures | ||||||
| DOSS (n = 2) | 0.188 | −0.407 | 0.784 | 0.621 | 0.535 | |
| FOIS (n = 2) | 0.805 | 0.268 | 1.343 | 2.937 | 0.003 * | |
| PAS (n = 2) | 0.235 | −0.799 | 1.269 | 0.446 | 0.656 | |
| VFSS-scale 1 (n = 1) | −0.099 | −0.888 | 0.690 | −0.246 | 0.806 | |
| VFSS-scale 2 (n = 2) | 0.611 | −0.193 | 1.415 | 1.489 | 0.137 | |
| Total stimulation time (min) | ||||||
| Low [< 500 min] (N = 4) | 0.317 | −0.304 | 0.938 | 0.999 | 0.318 | |
| Medium [500–100 min] (N = 1) | −0.099 | −0.888 | 0.690 | −0.246 | 0.806 | |
| High [>100 min] (N = 4) | 0.607 | 0.176 | 1.038 | 2.761 | 0.006 * | |
| Electrodes configuration | ||||||
| Infrahyoid (N = 3) | 0.771 | 0.041 | 1.501 | 2.069 | 0.039 * | |
| Mixed (patient-dependent) (N = 2) | 0.617 | −0.195 | 1.429 | 1.489 | 0.137 | |
| Suprahyoid and infrahyoid (N = 2) | 0.056 | −0.0544 | 0.655 | 0.182 | 0.856 | |
| Suprahyoid (N = 2) | −0.100 | −0.694 | 0.493 | −0.331 | 0.740 | |
| Pulse duration (μs) | ||||||
| 300 (N = 1) | 0.751 | 0.040 | 1.462 | 2.069 | 0.039 * | |
| 350 (N = 3) | 0.084 | −0.391 | 0.559 | 0.348 | 0.728 | |
| 700 (N = 4) | 0.680 | 0.227 | 1.133 | 2.944 | 0.003 * | |
| Pulse rates (Hz) | ||||||
| 30 (N = 1) | −0.304 | −1.082 | 0.473 | −0.768 | 0.433 | |
| 80 (N = 8) | 0.519 | 0.202 | 0.836 | 3.206 | 0.001 * | |
| PES | Total stimulation time (min) | |||||
| 10 (N = 2) | 0.300 | −0.325 | 0.925 | 0.940 | 0.347 | |
| 30 (N = 3) | 0.053 | 0.245 | 0.351 | 0.348 | 0.728 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Speyer, R.; Sutt, A.-L.; Bergström, L.; Hamdy, S.; Heijnen, B.J.; Remijn, L.; Wilkes-Gillan, S.; Cordier, R. Neurostimulation in People with Oropharyngeal Dysphagia: A Systematic Review and Meta-Analyses of Randomised Controlled Trials—Part I: Pharyngeal and Neuromuscular Electrical Stimulation. J. Clin. Med. 2022, 11, 776. https://doi.org/10.3390/jcm11030776
Speyer R, Sutt A-L, Bergström L, Hamdy S, Heijnen BJ, Remijn L, Wilkes-Gillan S, Cordier R. Neurostimulation in People with Oropharyngeal Dysphagia: A Systematic Review and Meta-Analyses of Randomised Controlled Trials—Part I: Pharyngeal and Neuromuscular Electrical Stimulation. Journal of Clinical Medicine. 2022; 11(3):776. https://doi.org/10.3390/jcm11030776
Chicago/Turabian StyleSpeyer, Renée, Anna-Liisa Sutt, Liza Bergström, Shaheen Hamdy, Bas Joris Heijnen, Lianne Remijn, Sarah Wilkes-Gillan, and Reinie Cordier. 2022. "Neurostimulation in People with Oropharyngeal Dysphagia: A Systematic Review and Meta-Analyses of Randomised Controlled Trials—Part I: Pharyngeal and Neuromuscular Electrical Stimulation" Journal of Clinical Medicine 11, no. 3: 776. https://doi.org/10.3390/jcm11030776