Investigation on the Use of Traditional Chinese Medicine for Polycystic Ovary Syndrome in a Nationwide Prescription Database in Taiwan


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
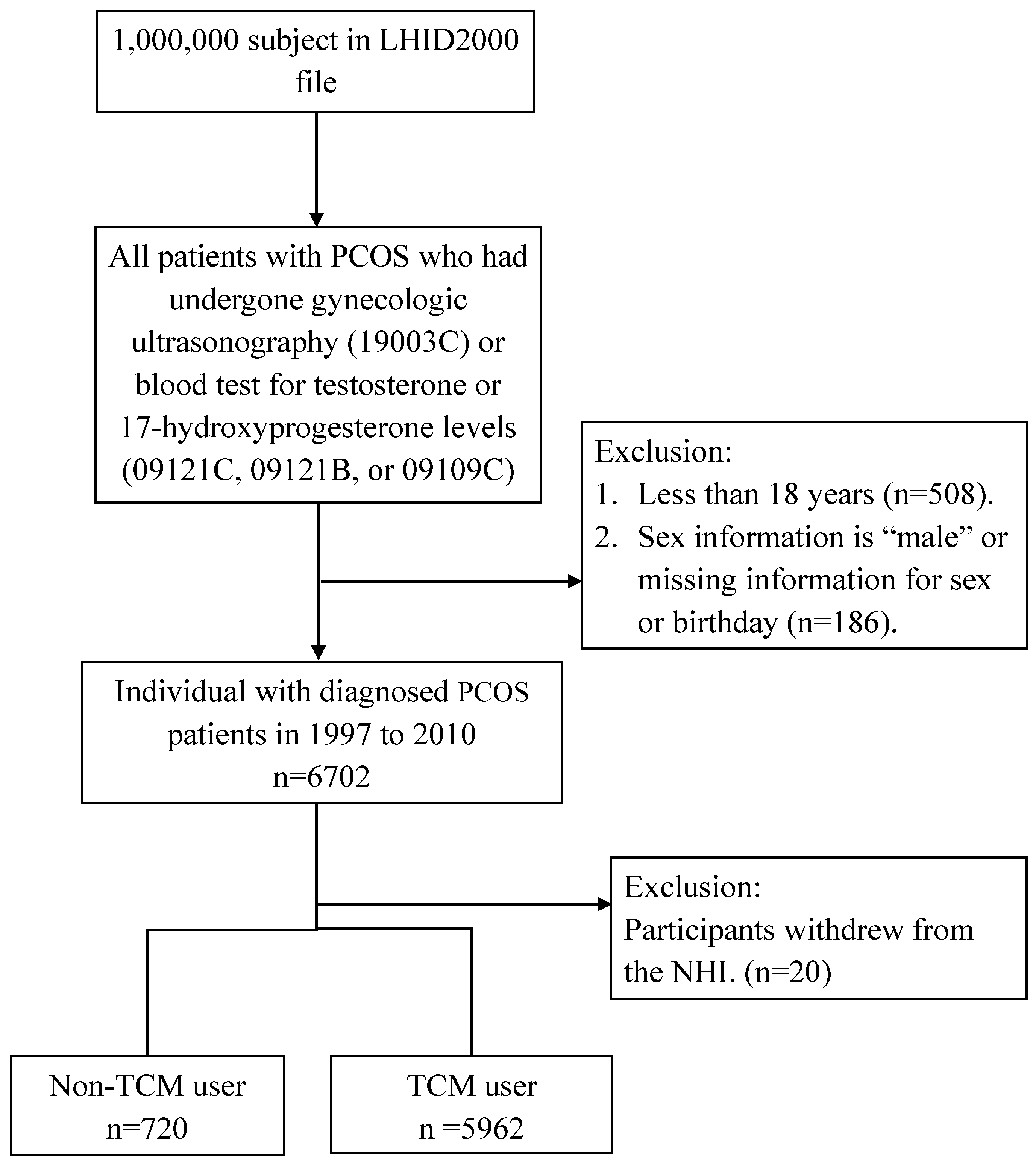
2.2. Study Design and Population
2.3. Potential Confounders
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristics
3.2. Distribution of Types of TCM
3.3. TCM Prescription Patterns for PCOS
3.4. Frequency Distribution of Disease Categories in TCM and Non-TCM Visits
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre-Amione, G. The syndrome of heart failure: Emerging concepts in the understanding of its pathogenesis and treatment. Curr. Opin. Cardiol. 1999, 14, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Franks, S. Polycystic ovary syndrome. N. Engl. J. Med. 1995, 333, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, J.; Wang, X.; Xu, L.; Wu, T.; Kang, D. Antidepressants for polycystic ovary syndrome. Cochrane Database Syst. Rev. 2013, CD008575. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.; Hickey, M.; Franks, S. Definitions, prevalence and symptoms of polycystic ovaries and polycystic ovary syndrome. Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Solomon, C.G. The epidemiology of polycystic ovary syndrome. Prevalence and associated disease risks. Endocrinol. Metab. Clin. N. Am. 1999, 28, 247–263. [Google Scholar] [CrossRef]
- Cerda, C.; Perez-Ayuso, R.M.; Riquelme, A.; Soza, A.; Villaseca, P.; Sir-Petermann, T.; Espinoza, M.; Pizarro, M.; Solis, N.; Miquel, J.F.; et al. Nonalcoholic fatty liver disease in women with polycystic ovary syndrome. J. Hepatol. 2007, 47, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.B.; Khorram, O.; Chiu, V.; Schwimmer, W.B. Abnormal aminotransferase activity in women with polycystic ovary syndrome. Fertil. Steril. 2005, 83, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Hutchison, S.K.; Norman, R.J.; Teede, H.J. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst. Rev. 2011, CD007506. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Misso, M.L.; Deeks, A.A.; Moran, L.J.; Stuckey, B.G.; Wong, J.L.; Norman, R.J.; Costello, M.F. Assessment and management of polycystic ovary syndrome: Summary of an evidence-based guideline. Med. J. Aust. 2011, 195, S65–S112. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.A.; Anderson, R.R.; Chang, R.J.; Ehrmann, D.A.; Lobo, R.A.; Murad, M.H.; Pugeat, M.M.; Rosenfield, R.L. Evaluation and Treatment of Hirsutism in Premenopausal Women: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2018, 103, 1233–1257. [Google Scholar] [CrossRef] [PubMed]
- Legro, R.S.; Arslanian, S.A.; Ehrmann, D.A.; Hoeger, K.M.; Murad, M.H.; Pasquali, R.; Welt, C.K. Diagnosis and treatment of polycystic ovary syndrome: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2013, 98, 4565–4592. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Baillargeon, J.P.; Iuorno, M.J.; Jakubowicz, D.J.; Nestler, J.E. A modern medical quandary: Polycystic ovary syndrome, insulin resistance, and oral contraceptive pills. J. Clin. Endocrinol. Metab. 2003, 88, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Polson, D.W.; Kiddy, D.S.; Mason, H.D.; Franks, S. Induction of ovulation with clomiphene citrate in women with polycystic ovary syndrome: The difference between responders and nonresponders. Fertil. Steril. 1989, 51, 30–34. [Google Scholar] [CrossRef]
- Kousta, E.; White, D.M.; Franks, S. Modern use of clomiphene citrate in induction of ovulation. Hum. Reprod. Update 1997, 3, 359–365. [Google Scholar] [CrossRef] [Green Version]
- Messinis, I.E. Ovulation induction: A mini review. Hum. Reprod. 2005, 20, 2688–2697. [Google Scholar] [CrossRef] [PubMed]
- Sepilian, V.; Nagamani, M. Effects of rosiglitazone in obese women with polycystic ovary syndrome and severe insulin resistance. J. Clin. Endocrinol. Metab. 2005, 90, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Lord, J.M.; Norman, R.J.; Yasmin, E.; Balen, A.H. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst. Rev. 2010, CD003053. [Google Scholar] [CrossRef]
- Nesto, R.W.; Bell, D.; Bonow, R.O.; Fonseca, V.; Grundy, S.M.; Horton, E.S.; Le Winter, M.; Porte, D.; Semenkovich, C.F.; Smith, S.; et al. Thiazolidinedione use, fluid retention, and congestive heart failure: A consensus statement from the American Heart Association and American Diabetes Association. October 7, 2003. Circulation 2003, 108, 2941–2948. [Google Scholar] [CrossRef] [PubMed]
- Lago, R.M.; Singh, P.P.; Nesto, R.W. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: A meta-analysis of randomised clinical trials. Lancet 2007, 370, 1129–1136. [Google Scholar] [CrossRef]
- Ma, K.; Yu, X.Y.; Peng, Y.F. Clinical observation on combination of compound xuanju capsule and clomiphene citrate in treating ovulatory dysfunctional infertility patients of Shen-yang deficiency. Zhongguo Zhong Xi Yi Jie He Za Zhi 2012, 32, 882–884. [Google Scholar] [PubMed]
- Liang, R.N.; Liu, J.; Lu, J. Treatment of refractory polycystic ovary syndrome by bushen huoxue method combined with ultrasound-guided follicle aspiration. Zhongguo Zhong Xi Yi Jie He Za Zhi 2008, 28, 314–317. [Google Scholar] [PubMed]
- Yao, X.Q.; Yang, H.E. Clinical observation on integrated traditional Chinese and Western medicine therapy in treating patients with pelvic inflammatory disease: A report of 28 cases. Zhong Xi Yi Jie He Xue Bao 2006, 4, 199–201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.J.; Chen, P.; Cheng, H.J. Clinical observation on treatment of chronic prostatitis with integrated traditional Chinese and Western medicine therapy: A report of 167 cases. Zhong Xi Yi Jie He Xue Bao 2006, 4, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Jedel, E.; Labrie, F.; Oden, A.; Holm, G.; Nilsson, L.; Janson, P.O.; Lind, A.K.; Ohlsson, C.; Stener-Victorin, E. Impact of electro-acupuncture and physical exercise on hyperandrogenism and oligo/amenorrhea in women with polycystic ovary syndrome: A randomized controlled trial. Am. J. Physiol. Endocrinol. Metab. 2011, 300, E37–E45. [Google Scholar] [CrossRef] [PubMed]
- Stener-Victorin, E.; Holm, G.; Janson, P.O.; Gustafson, D.; Waern, M. Acupuncture and physical exercise for affective symptoms and health-related quality of life in polycystic ovary syndrome: Secondary analysis from a randomized controlled trial. BMC Complement. Altern. Med. 2013, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- Johansson, J.; Redman, L.; Veldhuis, P.P.; Sazonova, A.; Labrie, F.; Holm, G.; Johannsson, G.; Stener-Victorin, E. Acupuncture for ovulation induction in polycystic ovary syndrome: A randomized controlled trial. Am. J. Physiol. Endocrinol. Metab. 2013, 304, E934–E943. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.C.; Choo, C.Y.; Tan, K.T. A randomised controlled trial of ultrasound-assisted spinal anaesthesia. Anaesth. Intensiv. Care 2014, 42, 191–198. [Google Scholar]
- Pastore, L.M.; Williams, C.D.; Jenkins, J.; Patrie, J.T. True and sham acupuncture produced similar frequency of ovulation and improved LH to FSH ratios in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2011, 96, 3143–3150. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.C.; Tsai, Y.T.; Lai, J.N.; Wu, C.T.; Lin, S.K.; Huang, C.Y. Integrating traditional Chinese medicine healthcare into diabetes care by reducing the risk of developing kidney failure among type 2 diabetic patients: A population-based case control study. J. Ethnopharmacol. 2014, 156, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.L.; Chen, B.C.; Mou, C.H.; Sun, M.F.; Yen, H.R. Association of Traditional Chinese Medicine Therapy and the Risk of Vascular Complications in Patients With Type II Diabetes Mellitus: A Nationwide, Retrospective, Taiwanese-Registry, Cohort Study. Medicine 2016, 95, e2536. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.S.; Peng, Y.I.; Lee, P.C.; Liu, T.C. The effectiveness of preventive care at reducing curative care risk for the Taiwanese elderly under National Health Insurance. Health Policy 2015, 119, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.P.; Liu, P.H.; Lien, A.S.; Yang, S.L.; Chang, H.H.; Yen, H.R. A nationwide population-based study of traditional Chinese medicine usage in children in Taiwan. Complement. Ther. Med. 2014, 22, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Yen, H.; Huang, T.; Sun, M. Chinese Medicine Usage in Taiwan: A Nationwide Population-Based Study. Available online: https://www.researchgate.net/publication/284799987_Chinese_medicine_usage_in_Taiwan_A_nationwide_population-based_study (accessed on 21 July 2018).
- Ma, R.J.; Zhou, J.; Fang, J.Q.; Yang, D.H.; Qu, F. Combination of acupuncture and chinese medicinal herbs in treating model rats with polycystic ovary syndrome. Afr. J. Tradit. Complement. Altern. Med. AJTCAM 2011, 8, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Huang, B.S.; Lin, Y.H.; Su, I.H.; Yang, S.H.; Chen, J.L.; Huang, J.W.; Chen, Y.C. Identifying Chinese herbal medicine for premenstrual syndrome: Implications from a nationwide database. BMC Complement. Altern. Med. 2014, 14, 206. [Google Scholar] [CrossRef] [PubMed]
- Washio, M. Kami-shoyo-san is usually used for women. Psychiatry Clin. Neurosci. 2003, 57, 345. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Kim, Y.K.; Lee, J.G.; Kim, S.H.; Kim, J.M.; Yoon, J.S.; Park, Y.K.; Lee, Y.K.; Kim, Y.H. Antidepressant-like effects of the traditional Chinese medicine kami-shoyo-san in rats. Psychiatry Clin. Neurosci. 2007, 61, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Ushiroyama, T.; Ikeda, A.; Sakuma, K.; Ueki, M. Changes in serum tumor necrosis factor (TNF-alpha) with kami-shoyo-san administration in depressed climacteric patients. Am. J. Chin. Med. 2004, 32, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Park, D.M.; Kim, S.H.; Park, Y.C.; Kang, W.C.; Lee, S.R.; Jung, I.C. The comparative clinical study of efficacy of Gamisoyo-San (Jiaweixiaoyaosan) on generalized anxiety disorder according to differently manufactured preparations: Multicenter, randomized, double blind, placebo controlled trial. J. Ethnopharmacol. 2014, 158 Pt A, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, P.; Dellarco, M.; Dearry, A. A major milestone for the National Children’s Study. Environ. Health Perspect. 2009, 117, A13. [Google Scholar] [CrossRef] [PubMed]
- Goto, H.; Shimada, Y.; Sekiya, N.; Yang, Q.; Kogure, T.; Mantani, N.; Hikiami, H.; Shibahara, N.; Terasawa, K. Effects of Keishi-bukuryo-gan on vascular function and hemorheological factors in spontaneously diabetic (WBN/kob) rats. Phytomed. Int. J. Phytother. Phytopharmacol. 2004, 11, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Goto, H.; Hussein, G.; Hikiami, H.; Shibahara, N.; Shimada, Y. Keishibukuryogan ameliorates glucose intolerance and hyperlipidemia in Otsuka Long-Evans Tokushima Fatty (OLETF) rats. Diabetes Res. Clin. Pract. 2008, 80, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Yokozawa, T.; Terasawa, K.; Nakanishi, K. Therapeutic usefulness of Keishi-bukuryo-gan for diabetic nephropathy. J. Pharm. Pharmacol. 2003, 55, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, M.; Tsuneyama, K.; Kinoshita, H.; Goto, H.; Takano, Y.; Selmi, C.; Keen, C.L.; Gershwin, M.E.; Shimada, Y. The traditional Japanese formula keishibukuryogan reduces liver injury and inflammation in patients with nonalcoholic fatty liver disease. Ann. N. Y. Acad. Sci. 2010, 1190, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.S.; Yang, J.K.; Yang, L.L. Effect of “Dang-Qui-Shao-Yao-San” a Chinese medicinal prescription for dysmenorrhea on uterus contractility in vitro. Phytomed. Int. J. Phytother. Phytopharmacol. 2006, 13, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Ushiroyama, T.; Ikeda, A.; Sakai, M.; Hosotani, T.; Suzuki, Y.; Tsubokura, S.; Ueki, M. Effects of unkei-to, an herbal medicine, on endocrine function and ovulation in women with high basal levels of luteinizing hormone secretion. J. Reprod. Med. 2001, 46, 451–456. [Google Scholar] [PubMed]
- Sun, W.S.; Imai, A.; Tagami, K.; Sugiyama, M.; Furui, T.; Tamaya, T. In vitro stimulation of granulosa cells by a combination of different active ingredients of unkei-to. Am. J. Chin. Med. 2004, 32, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Bian, Z.X.; Cheng, C.W.; Zhu, L.Z. Chinese herbal medicine for functional constipation: A randomised controlled trial. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2013, 19 (Suppl. 9), 44–46. [Google Scholar] [PubMed]
- Zhong, L.L.; Cheng, C.W.; Chan, Y.; Chan, K.H.; Lam, T.W.; Chen, X.R.; Wong, C.T.; Wu, J.C.; Bian, Z.X. Chinese herbal medicine (Ma Zi Ren Wan) for functional constipation: Study protocol for a prospective, double-blinded, double-dummy, randomized controlled trial. Trials 2013, 14, 366. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.W.; Bian, Z.X.; Zhu, L.X.; Wu, J.C.; Sung, J.J. Efficacy of a Chinese herbal proprietary medicine (Hemp Seed Pill) for functional constipation. Am. J. Gastroenterol. 2011, 106, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Han, J.; Seog, D.H.; Chung, J.Y.; Kim, N.; Hong Park, Y.; Lee, S.K. Antidepressant effect of Chaihu-Shugan-San extract and its constituents in rat models of depression. Life Sci. 2005, 76, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Liu, Y.; Sun, Y.; Chen, C.; Qi, Y.; Zhang, Y. AZT and emodin exhibit synergistic growth-inhibitory effects on K562/ADM cells by inducing S phase cell cycle arrest and suppressing MDR1 mRNA/p-gp protein expression. Pharm. Biol. 2013, 51, 1586–1591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Jia, L.; Liu, Z.C.; Zhang, H.; Zhang, P.J.; Wan, Q.; Wang, R. Emodin ameliorates high-glucose induced mesangial p38 over-activation and hypocontractility via activation of PPARgamma. Exp. Mol. Med. 2009, 41, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Kim, J.H.; Ghim, J.; Yoon, J.H.; Lee, A.; Kwon, Y.; Hyun, H.; Moon, H.Y.; Choi, H.S.; Berggren, P.O.; et al. Emodin regulates glucose utilization by activating AMP-activated protein kinase. J. Biol. Chem. 2013, 288, 5732–5742. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Ding, W.; Liu, Y. Anti-diabetic effects of emodin involved in the activation of PPARgamma on high-fat diet-fed and low dose of streptozotocin-induced diabetic mice. Fitoterapia 2010, 81, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Shang, W.; Zhou, L.; Jiang, B.; Jin, H.; Chen, M. Emodin with PPARgamma ligand-binding activity promotes adipocyte differentiation and increases glucose uptake in 3T3-Ll cells. Biochem. Biophys. Res. Commun. 2007, 353, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, R.; Lv, P.; Yang, J.; Deng, Y.; Xu, J.; Zhu, R.; Zhang, D.; Yang, Y. Emodin up-regulates glucose metabolism, decreases lipolysis, and attenuates inflammation in vitro. J. Diabetes 2015, 7, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.J.; Huang, S.L.; Feng, Y.; Ning, M.M.; Leng, Y. Emodin, an 11beta-hydroxysteroid dehydrogenase type 1 inhibitor, regulates adipocyte function in vitro and exerts anti-diabetic effect in ob/ob mice. Acta Pharmacol. Sin. 2012, 33, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ji, J.; Song, Z.; Zhang, W.; He, X.; Li, F.; Zhang, C.; Guo, C.; Wang, C.; Yuan, C. Hypocholesterolemic effect of emodin by simultaneous determination of in vitro and in vivo bile salts binding. Fitoterapia 2016, 110, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Xin, H.; Liu, X.; Xu, Y.; Wen, D.; Zhang, Y.; Zhu, Y.Z. Novel anti-diabetic effect of SCM-198 via inhibiting the hepatic NF-kappaB pathway in db/db mice. Biosci. Rep. 2012, 32, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, W.; Wen, Y.; Xiong, Q.; Liu, H.; Wu, J.; Zou, Y.; Zhu, Y. SCM-198 attenuates early atherosclerotic lesions in hypercholesterolemic rabbits via modulation of the inflammatory and oxidative stress pathways. Atherosclerosis 2012, 224, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Jia, M.; Li, C.; Zheng, Y.; Ding, X.; Chen, M.; Ding, J.; Du, R.; Lu, M.; Hu, G. Leonurine Exerts Antidepressant-Like Effects in the Chronic Mild Stress-Induced Depression Model in Mice by Inhibiting Neuroinflammation. Int. J. Neuropsychopharmacol. 2017, 20, 886–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, C.S.; Mehendale, S.R.; Wang, C.Z.; Aung, H.H.; Jiang, T.; Guan, X.; Shoyama, Y. Effects of Corydalis yanhusuo and Angelicae dahuricae on cold pressor-induced pain in humans: A controlled trial. J. Clin. Pharmacol. 2004, 44, 1323–1327. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Lin, Y.H.; Su, I.H.; Chen, Y.C.; Yang, S.H.; Chen, J.L. Investigation on Chinese herbal medicine for primary dysmenorrhea: Implication from a nationwide prescription database in Taiwan. Complement. Ther. Med. 2014, 22, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, C.; Wang, L.; Parks, G.S.; Zhang, X.; Guo, Z.; Ke, Y.; Li, K.W.; Kim, M.K.; Vo, B.; et al. A novel analgesic isolated from a traditional Chinese medicine. Curr. Biol. CB 2014, 24, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.L.; Cui, M.; He, Y.; Yu, H.L.; Guo, D.A. Chemical fingerprint and metabolic fingerprint analysis of Danshen injection by HPLC-UV and HPLC-MS methods. J. Pharm. Biomed. Anal. 2005, 36, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.Q.; Zhou, C.J.; Zhang, Y.P.; Zhang, X.Q.; Xu, W.; Lin, J.; Wang, P.J. Salvianolic Acid B Ameliorates Hyperglycemia and Dyslipidemia in db/db Mice through the AMPK Pathway. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2016, 40, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Xie, Y.; Chen, L.; Chu, K.; Wu, S.; Lu, J.; Chen, X.; Wang, Y.; Lai, X. Antidiabetic effect of the total polyphenolic acids fraction from Salvia miltiorrhiza Bunge in diabetic rats. Phytother. Res. PTR 2012, 26, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Xu, S.; Li, W.; Wang, F.; Yang, Z.; Jiang, L.; Wang, Q.; Huang, M.; Zhou, P. Salvianolic acid B inhibited PPARgamma expression and attenuated weight gain in mice with high-fat diet-induced obesity. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2014, 34, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Wang, P.; Xu, S.; Xu, W.; Chu, K.; Lu, J. Biological activities of salvianolic acid B from Salvia miltiorrhiza on type 2 diabetes induced by high-fat diet and streptozotocin. Pharm. Biol. 2015, 53, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Raoufi, S.; Baluchnejadmojarad, T.; Roghani, M.; Ghazanfari, T.; Khojasteh, F.; Mansouri, M. Antidiabetic potential of salvianolic acid B in multiple low-dose streptozotocin-induced diabetes. Pharm. Biol. 2015, 53, 1803–1809. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Shan, W.; Gao, L.; Gao, D.; Hu, Y.; Wang, G.; Zhang, N.; Li, Z.; Tian, X.; Xu, W.; et al. Inhibition of HMGB1 release via salvianolic acid B-mediated SIRT1 up-regulation protects rats against non-alcoholic fatty liver disease. Sci. Rep. 2015, 5, 16013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Chen, M.L.; Zhou, Y.; Yi, L.; Gao, Y.X.; Ran, L.; Chen, S.H.; Zhang, T.; Zhou, X.; Zou, D.; et al. Resveratrol improves hepatic steatosis by inducing autophagy through the cAMP signaling pathway. Mol. Nutr. Food Res. 2015, 59, 1443–1457. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Zhao, Y.; Shi, X.; Zhang, N.; Zu, G.; Li, Z.; Zhou, J.; Gao, D.; Lv, L.; Tian, X.; et al. New insights into salvianolic acid A action: Regulation of the TXNIP/NLRP3 and TXNIP/ChREBP pathways ameliorates HFD-induced NAFLD in rats. Sci. Rep. 2016, 6, 28734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, W.; Gao, L.; Zeng, W.; Hu, Y.; Wang, G.; Li, M.; Zhou, J.; Ma, X.; Tian, X.; Yao, J. Activation of the SIRT1/p66shc antiapoptosis pathway via carnosic acid-induced inhibition of miR-34a protects rats against nonalcoholic fatty liver disease. Cell Death Dis. 2015, 6, e1833. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; He, Y.; Zheng, G.; Zhang, W.; Yao, Z.; Xie, W. Meta-analysis of traditional herbal medicine in the treatment of nonalcoholic fatty liver disease. Cell. Mol. Biol. 2016, 62, 88–95. [Google Scholar] [PubMed]
- Liao, H.H.; Yeh, C.C.; Lin, C.C.; Chen, B.C.; Yeh, M.H.; Chang, K.M.; Sun, M.F.; Yen, H.R. Prescription patterns of Chinese herbal products for patients with fractures in Taiwan: A nationwide population-based study. J. Ethnopharmacol. 2015, 173, 11–19. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Without TCM | With TCM | p Value | ||
|---|---|---|---|---|---|
| n = 720 (10.78%) | n = 5962 (89.22%) | ||||
| n | % | n | % | ||
| Age at baseline | 0.0654 * | ||||
| 18–29 | 395 | 54.86 | 3539 | 59.36 | |
| 30–39 | 265 | 36.81 | 1991 | 33.39 | |
| Older than 40 | 60 | 8.33 | 432 | 7.25 | |
| Mean(SD) | 29.77(6.93) | 29.09(6.67) | 0.0094 ‡ | ||
| Urbanization | 0.7906 * | ||||
| 1 (highest) | 236 | 32.78 | 1972 | 33.08 | |
| 2 | 230 | 31.94 | 1824 | 30.59 | |
| 3 | 116 | 16.11 | 984 | 16.5 | |
| 4 | 89 | 12.36 | 707 | 11.86 | |
| 4+ (lowest) | 49 | 6.81 | 475 | 7.97 | |
| Hospital level (where diagnosed with PCOS) | 0.2209 * | ||||
| Medical center | 170 | 23.64 | 1326 | 22.24 | |
| Regional hospital | 281 | 39.08 | 2172 | 36.43 | |
| District hospital | 118 | 16.41 | 1070 | 17.95 | |
| Physician clinics | 150 | 20.86 | 1394 | 23.38 | |
| Baseline comorbidity | |||||
| Diabetes mellitus | 43 | 5.97 | 441 | 7.4 | 0.1636 * |
| Infertility female | 129 | 17.92 | 1362 | 22.84 | 0.0027 * |
| Hirsutism | 1 | 0.14 | 27 | 0.45 | 0.3567 * |
| Acne varioliformis | 227 | 31.53 | 1950 | 32.71 | 0.5236 * |
| Obesity | 14 | 1.94 | 159 | 2.67 | 0.2489 * |
| Disorders of lipoid metabolism | 42 | 5.83 | 294 | 4.93 | 0.2954 * |
| Major depression | 16 | 2.22 | 137 | 2.3 | 0.898 * |
| Anxiety | 60 | 8.33 | 786 | 13.18 | 0.0002 * |
| Amenorrhea | 218 | 30.28 | 2630 | 44.11 | <0.0001 * |
| Interval between onset of PCOS disease and the first TCM consultation, days mean (median) | 530.88(246) | ||||
| Number of TCM Visits (Times/per Year) | Only Chinese Herbal Remedies | Only Acupuncture or Traumatology | Combination of Both Treatments | Total of TCM (n = 5962) |
|---|---|---|---|---|
| n = 3003 (50.37%) | n = 11 (0.18%) | n = 2948 (49.45%) | ||
| n (%) | n (%) | n (%) | n (%) | |
| 1–3 | 2016 (67.13) | 11 (100) | 1569 (53.22) | 3596 (60.32) |
| 4–6 | 361 (12.02) | 0 | 461 (15.64) | 822 (13.79) |
| >6 | 626 (20.85) | 0 | 918 (31.14) | 1544 (25.90) |
| Herbal Formula | Frequency | Number of Person-Days | Average Daily Dose | Average Duration for Prescription |
|---|---|---|---|---|
| (g) | (Days) | |||
| Single Chinese herb | ||||
| Xiang-Fu (Cyperus rotundus L.) | 12,375 | 86,491 | 1.0 | 7.0 |
| Da-Huang (Rheum officinale Baill.) | 11,350 | 83,520 | 0.7 | 7.4 |
| Yi-Mu-Cao (Leonurus artemisia (Lour.) S. Y. Hu) | 10,824 | 77,687 | 1.1 | 7.2 |
| Yan-hu-suo (Corydalis yanhusuo W. T. Wang) | 9889 | 68,526 | 1.1 | 6.9 |
| Dan-shen (Salvia miltiorrhiza Bge.) | 8072 | 61,438 | 1.1 | 7.6 |
| Gan-Cao (Glycyrrhiza uralensis Fisch.) | 7818 | 53,026 | 0.9 | 6.8 |
| Tu-Si-Zi (Cuscuta chinensis Lam.) | 7178 | 52,268 | 1.3 | 7.3 |
| Huang-Qin (Scutellaria baicalensis Georgi) | 7616 | 52,213 | 1.2 | 6.9 |
| Bei-Mu (Fritillaria thunbergii Miq.) | 5860 | 39,858 | 1.1 | 6.8 |
| Du-Zhong (Eucommia ulmoides Oliv.) | 5414 | 39,649 | 1.1 | 7.3 |
| Combined Chinese herb | ||||
| Jia-Wei-Xiao-Yao-San | 21,305 | 15,3952 | 4.3 | 7.2 |
| Gui-Zhi-Fu-Ling-Wan | 8779 | 62,294 | 3.9 | 7.1 |
| Dang-Gui-Shao-Yao-San | 8470 | 58,510 | 4.4 | 6.9 |
| Wen-Jing-Tang | 7970 | 58,018 | 4.2 | 7.3 |
| Ma-Zi-Ren-Wan | 6850 | 51,079 | 2.7 | 7.5 |
| Chuan-Xiong-Cha-Tiao-San | 5643 | 36,836 | 3.9 | 6.5 |
| Gui-Pi-Tang | 4895 | 36,050 | 4.3 | 7.4 |
| Ger-Gen-Tang | 5471 | 35,096 | 4.3 | 6.4 |
| Shao-Fu-ZhuYu-Tang | 4994 | 34,233 | 3.8 | 6.9 |
| Xue-Fu-Zhu-Yu-Tang | 4473 | 33,638 | 3.8 | 7.5 |
| List according to person-days |
| Disease (ICD-9-CM) | Without TCM (n = 720) | With TCM (n = 5962) | p Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Infectious and parasitic disease (001–139) | 439 | 60.97 | 4433 | 74.35 | <0.0001 |
| Neoplasms (140–239) | 324 | 45.00 | 3384 | 56.76 | <0.0001 |
| Malignant (140–208) | 19 | 2.64 | 257 | 4.31 | 0.0332 |
| Benign (210–229) | 313 | 43.47 | 3242 | 54.38 | <0.0001 |
| Endocrine, nutritional, and metabolic disease and immunity disorder (240–279) | 720 | 100.00 | 5962 | 100.00 | - |
| Blood and blood-forming organs (280–289) | 136 | 18.89 | 1482 | 24.86 | 0.0004 |
| Mental disorder (290–319) | 156 | 21.67 | 2243 | 37.62 | <0.0001 |
| Nervous system (320–389) | 532 | 73.89 | 5232 | 87.76 | <0.0001 |
| Circulatory system (390–459) | 200 | 27.78 | 2415 | 40.51 | <0.0001 |
| Respiratory system (460–519) | 680 | 94.44 | 5904 | 99.03 | <0.0001 |
| Digestive system (520–579) | 687 | 95.42 | 5911 | 99.14 | <0.0001 |
| Genitourinary system (580–629) | 681 | 94.58 | 5915 | 99.21 | <0.0001 |
| Complications of pregnancy, childbirth, and the puerperium (630–676) | 309 | 42.92 | 3015 | 50.57 | 0.0001 |
| Skin and subcutaneous tissue (680–709) | 595 | 82.64 | 5553 | 93.14 | <0.0001 |
| Musculoskeletal system and connective tissue (710–739) | 394 | 54.72 | 4964 | 83.26 | <0.0001 |
| Congenital anomalies (740–759) | 30 | 4.17 | 455 | 7.63 | 0.0007 |
| Certain conditions originating in the perinatal period (760–779) | 122 | 16.94 | 1053 | 17.66 | 0.6329 |
| Symptoms, signs, and ill-defined conditions (780–799) | 607 | 84.31 | 5772 | 96.81 | <0.0001 |
| Injury and poisoning (800–999) | 422 | 58.61 | 5129 | 86.03 | <0.0001 |
| Chinese Herbal Products | Model/Design | Possible Pharmacological Effects or Mechanism | |
|---|---|---|---|
| Herbal formulas | |||
| Jia-Wei-Xiao-Yao-San | Multicenter, Double blind, Placebo controlled RCT | Antidepressant effects | Improve quality of life, reduce depressive, obsessive-compulsive, somatic symptoms of generalized anxiety disorder |
| Stressed rats | Antidepressant effects | Reverse the impairment of neurogenesis in the hippocampus | |
| Gui-Zhi-Fu-Ling-Wan | Retrospective study | Anti-inflammation Hypolipidemic effects | Reduction in liver injury tests and blood cholesterol |
| Diabetic rats | Anti-diabetic effects Hypolipidemic effects | Improve glucose intolerance, decrease in serum total cholesterol and TG levels Delay the development of diabetic nephropathy | |
| Dang-Gui-Shao-Yao-San | Rats | Analgesic effect | Suppress uterine contraction through antagonistic action on both prostaglandin F2α and acetylcholine |
| Wen-Jing-Tang | Clinical Trial | Decrease in plasma LH level in anovulatory patients including those with PCOS | |
| Human granulosa cells | Enhancing 17β-estradiol and progesterone secretion | ||
| Ma-Zi-Ren-Wan | Double blind, Placebo controlled RCT | Increase complete spontaneous bowel movement and decrease straining at evacuation | |
| Single herbs | |||
| Xiang-Fu | Rats | Antidepressant | Had antidepressant activity in the forced swimming test |
| Da-Huang | Mice | Hypocholesterolemic effects | Activation of the PPAR-γ and AMPK signaling pathways |
| Yi-Mu-Cao | Mice | Potential to treat insulin resistance, and type-2 diabetes | Through inhibition of the NF-κB/IκB kinase pathway |
| Yan-hu-suo | Mice | Analgesic effects | Antinociceptive effect due to interaction with D2 receptors |
| Dan-shen | Rats | Potential to treat insulin resistance, obesity, and type-2 diabetes | SalB: Increased phosphorylated AMPK protein expression, GLUT 4 and glycogen synthase protein expressions |
| Rats | Hepatoprotective effects | SalA: Suppressing ROS, MDA; preventing the decreased expression of SOD SalB: Through SIRT1-mediated HMGB1 deacetylation | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, W.-T.; Chiang, J.-H.; Li, C.-J.; Lee, M.-T.; Su, C.-C.; Yen, H.-R. Investigation on the Use of Traditional Chinese Medicine for Polycystic Ovary Syndrome in a Nationwide Prescription Database in Taiwan. J. Clin. Med. 2018, 7, 179. https://doi.org/10.3390/jcm7070179
Liao W-T, Chiang J-H, Li C-J, Lee M-T, Su C-C, Yen H-R. Investigation on the Use of Traditional Chinese Medicine for Polycystic Ovary Syndrome in a Nationwide Prescription Database in Taiwan. Journal of Clinical Medicine. 2018; 7(7):179. https://doi.org/10.3390/jcm7070179
Chicago/Turabian StyleLiao, Wan-Ting, Jen-Huai Chiang, Chia-Jung Li, Ming-Tsung Lee, Cheng-Chiung Su, and Hung-Rong Yen. 2018. "Investigation on the Use of Traditional Chinese Medicine for Polycystic Ovary Syndrome in a Nationwide Prescription Database in Taiwan" Journal of Clinical Medicine 7, no. 7: 179. https://doi.org/10.3390/jcm7070179