Coronary Artery Bypass in Young Patients—On or Off-Pump?
by
 , ,
, ,
Ryoi Okano
1,2 ,
,
Yi-Jia Liou
3,
Hsi-Yu Yu
1,
I-Hui Wu
1,
Nai-Kuan Chou
1,
Yih-Sharng Chen
1 and
Nai-Hsin Chi
1,* 1
Department of Surgery, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei 10002, Taiwan
2
Department of Cardiovascular Surgery, Ageo Central General Hospital, Saitama 362-8588, Japan
3
Department of Life Science, National Dong Hwa University, Hualien 97401, Taiwan
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2019, 8(2), 128; https://doi.org/10.3390/jcm8020128
Submission received: 24 December 2018
/
Revised: 12 January 2019
/
Accepted: 20 January 2019
/
Published: 22 January 2019
(This article belongs to the Special Issue New Technologies for the Treatment of Coronary and Structural Heart Diseases)
Abstract
:A definitive conclusion regarding whether on-pump or off-pump coronary artery bypass is preferable in young patients is lacking. The aim of our study was to perform a long-term comparison of the two approaches in young patients. We analyzed the National Health Insurance Research Database, using data for patients between 18 and 45 years of age who had undergone isolated coronary artery bypass between 2001 and 2011. The study endpoints were: all-cause death, major adverse cardiac and cerebrovascular events, and repeat revascularization within 30 days, 1 year, 5 years, and the entire 10-year follow-up period. A total of 344 patients received off-pump surgery and 741 patients received on-pump surgery. Preoperative characteristics and comorbidities were similar in both groups, and all-cause mortality was almost equal (p = 0.716). The 5-year survival rates were 93.9% and 92.2% in the off-pump and on-pump groups, respectively, and the 10-year survival rates were 86.3% and 82.1%, respectively. The repeat revascularization rate was significantly lower in the on-pump group (p = 0.0407). Both the on-pump and off-pump methods offer equally good long-term outcomes in terms of mortality and major adverse cardiac and cerebrovascular events. However, the need for repeat revascularization is a concern in the long term after off-pump surgery.
1. Introduction
The efficacy and appropriate indications for off-pump coronary artery bypass grafting (CABG) have been a source of contention since its enthusiastic re-emergence in the 1990s [1]. Recently, several large randomized trials have compared on-pump with off-pump CABG [2,3,4,5,6]. They showed the superiority, or at least non-inferiority, of on-pump CABG to off-pump CABG for most patients and in the hands of most surgeons [7]. However, the main participants in these trials were elderly patients. In most of the trials the average age was approximately 60 years, and in some trials patients under 45 years were even excluded [2,3,4,5,6].
Young patients account for 3% of all patients with coronary artery disease (CAD) and have a different background and propensity to elderly patients [8]. They are more likely to be male, smokers, obese, have a family history, and some of them have non-atherosclerotic diseases [8,9,10,11,12,13,14,15,16,17]. Although the appropriateness of CABG in young patients is currently being considered [8,9,10,11,12,13,14,16], there is insufficient data to form a definitive conclusion. In particular, there have been no studies comparing long-term outcomes between on-pump and off-pump CABG in young patients.
The aim of our study was to perform the first long-term, high-volume comparison of on-pump versus off-pump CABG in young patients using the Taiwan Nationwide Database.
2. Experimental Section
2.1. Materials and Methods
The Taiwanese National Health Insurance (NHI) program has been operating since 1995. By 2014, approximately 99.9% of the Taiwanese population was enrolled in the NHI program [18]. For the current analysis, we used a data subset of the NHI Research Database, namely the registry for patients with catastrophic illness, which contains the records of all prevalent cases of patients who have major illnesses.
From the database, we included patients between 18 and 45 years of age who had undergone isolated on-pump or off-pump CABG between 2001 and 2011, as shown in Figure 1. We searched the database to determine the presence of comorbidities such as hypertension, diabetes mellitus, peripheral vascular disease, chronic obstructive pulmonary disease stroke, myocardial infarction (MI), implanted cardiac pacemaker, or atrial fibrillation. The extent of CAD (single, double, or triple vessel disease) and renal function were also compared. The study endpoints were all-cause death, major adverse cardiac and cerebrovascular events (MACCE; defined as all-cause death, MI, and stroke); and repeat revascularization within 30 days, 1 year, 5 years, and over the entire follow-up period.
2.2. Statistical Analysis
The characteristics of patients were analyzed using the chi-square test for categorical variables and t-tests for continuous variables to identify potential differences between the two groups. We used standardized difference to measure the balance of covariates, whereby an absolute standardized difference of greater than 10% represented meaningful imbalance.
The survival was compared between the groups of patients using Kaplan–Meier survival curves and log-rank tests. The factors affecting survival were analyzed by univariate and multivariate Cox’s proportional hazard models to estimate the hazard ratio (HR) with a 95% confidence interval (95% CI). All the analyses were performed with SAS 9.3 software (SAS Institute Inc, Cary, NC, USA). A p-value <0.05 was considered statistically significant.
3. Results
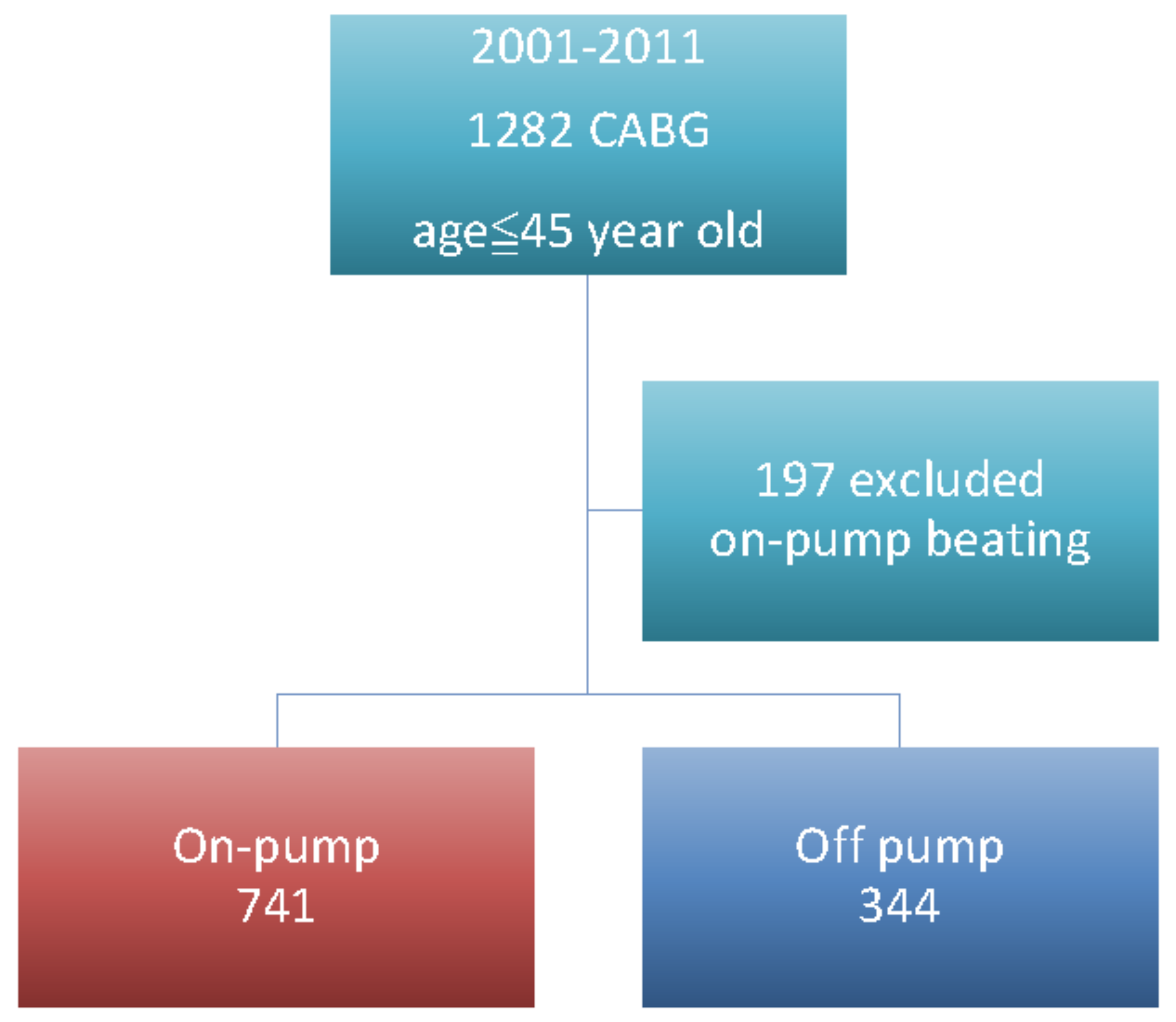
There were 31,448 patients that had undergone CABG in the database. From these, we included 1282 patients who were 45 years old or younger and had isolated on-pump or off-pump CABG. Among these, 197 patients were excluded due the use of an on-pump beating heart technique, as shown in Figure 1. The average overall follow-up time was 5.3 years and the longest was 16 years, with 100% complete follow up. The mean follow-up times were 4.79 years for off-pump CABG and 5.53 years for on-pump CABG.
A total of 344 patients received off-pump surgery and 741 patients received on-pump surgery, as shown in Table 1. Both groups were comprised of predominantly male patients, and mean age was similar in both groups (approximately 41 years in both; p = 0.18). The distribution of one-vessel disease was greater in the off-pump group (15.99% off-pump vs. 6.34% on-pump). Before the operation, both groups had a similar incidence of diabetes mellitus, hyperlipidemia, familial hypercholesterolemia, chronic obstructive pulmonary disease, stroke, peripheral vascular disease, hypertension, previous myocardial infarction, atrial fibrillation, implanted pacemaker, and presence of renal dysfunction, as shown in Table 1. In the off-pump group, there were 28.19% of them that received previous percutaneous coronary intervention and in the on-pump group it was 26.85% (p = 0.63). The emergent operations of both groups were similar; they accounted for 13.95% in the off-pump and 13.76% in the on-pump group (p = 0.41).
Regarding the completeness of revascularization, we used graft number/disease vessels as a marker; if the number is more than 1, we deem this as complete revascularization in our database. By doing so, the completeness of revascularization in one vessel disease was 100% in both groups. The completeness of revascularization in two-vessel disease was 93% in the off-pump group and 95% in the on-pump group. The completeness of revascularization in three-vessel disease was 91% in the off-pump group and 92% in the on-pump group.
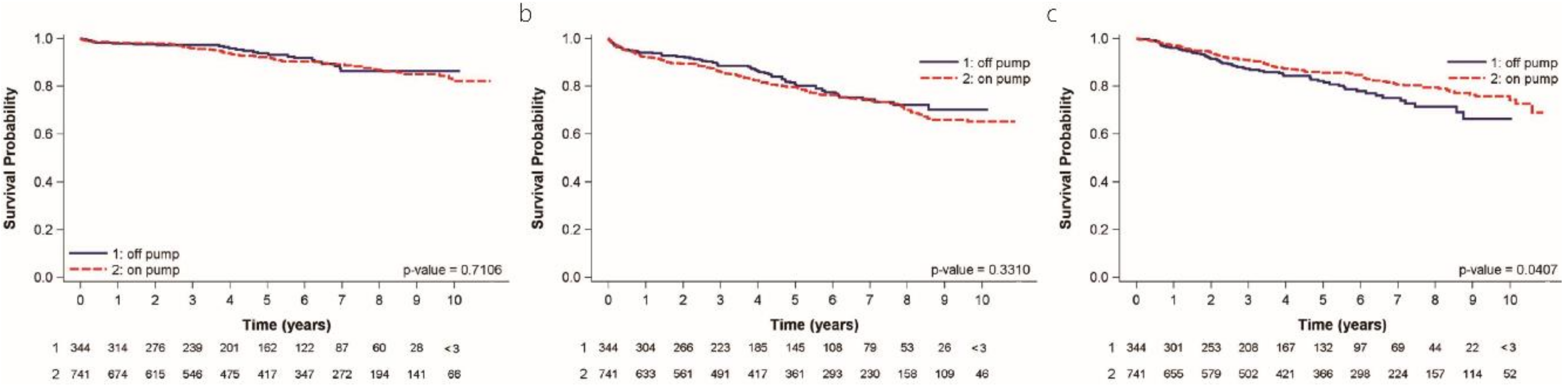
The 30-day outcomes, as shown in Table 2, and the 1-year outcomes, as shown in Table 3, in terms of death, myocardial infarction, and stroke were not different between the groups. The operative outcome, as shown in Table 2, including transfusion amount, post-operative atrial fibrillation, ICU (intensive care unit) stay, and hospital stay were no different. The incidence of post-operative atrial fibrillation was 10.46% in the off-pump and 13.76% in the on-pump groups (p = 0.535). Further, at 5 years and 10 years, there were no differences in death, MI, stroke, and MACCE, as shown in Table 4 and Table 5. The Kaplan–Meier curve shows that the rates of all-cause mortality were almost equal in both groups (p = 0.716), as shown in Figure 2A. The 5-year survival rate was 93.9% in the off-pump group and 92.2% in the on-pump group and the 10-year survival rates were 86.3% and 82.1%, respectively. There was no significant difference in freedom from MACCE at 5 and 10 years in patients receiving on-pump versus off-pump surgery (79.1% vs. 81.8% and 64.8% vs. 70.0%, respectively; p = 0.3310), as shown in Figure 2B.
Repeat revascularization was defined by further admission intervention of coronary artery or repeat coronary artery bypass surgery 6 months after first operation. The reason we defined repeat revisualization by 6 months after first operation was to eliminate the scheduled hybrid procedures, because most of the hybrid procedures were performed within 3 months.
The repeat revascularization rate was significantly lower in the on-pump group (p = 0.0407), as shown in Figure 2C. Freedom from revascularization at 5 years was 86.2% in the on-pump versus 80.8% in the off-pump group, and at 10 years was 76.1% versus 65.9%, respectively.
4. Discussion
In our study, we compared the outcomes of on-pump and off-pump CABG in 1085 young patients. There was no difference in the 30-day, 1-year, and 5-year outcomes in terms of death, MI, stroke, and new renal failure. Kaplan–Meier and long-rank analysis showed that all-cause mortality and MACCE were not significantly different. Off-pump surgery was not inferior to on-pump surgery in terms of death, MI, and MACCE. However, the repeat revascularization rate was significantly higher in the off-pump group. The long-term survival was excellent in both groups.
For young coronary artery bypass patients, the long-term durability of the vascular graft and the long-term survival benefit are the major concerns. Young patients have less comorbidities than older patients. They have better renal function, less incidence of diabetes, and less renal impairment compared with older patients. Therefore, in both groups, young patients have less surgical risk [19].
The characteristics of coronary artery disease in young patients are different from older patients: 80% is atherosclerotic and 20% is non-atherosclerotic (e.g., coronary embolism, thrombosis, congenital anomalies, vessel inflammation, spasm) [9,10,11,12,13,14,15,16,17].
Compared with older patients, coronary heart disease in young patients is more closely associated with male sex, smoking, obesity, and family history. Conversely, the proportion of patients with diabetes mellitus and hypertension is smaller [8,9,10,11,12,13,17]. In our patients, the prevalence of diabetes was 33.72% and 31.85% in the off-pump and on-pump groups, respectively; in contrast, in our previous nationwide study where the mean age of patients was 62 years, the incidence was approximately 70% [19]. The overall prevalence of hypertension was 55%, and 90% of the cohort were males.
Young patients with coronary artery disease have fewer comorbidities than older patients [10,12]. In our study, the incidence of stroke, peripheral vascular disease, chronic obstructive pulmonary disease, and atrial fibrillation were low, and renal function was preserved in most patients.
Triple vessel disease was the predominant pathology in our cohort, in accordance with similar findings reported recently by Saraiva et al. [10].
Kaplan–Meier analysis in this study revealed excellent survival in young patients, and there were no significant differences between on-pump and off-pump CABG. However, the repeat revascularization rate was significantly higher after off-pump CABG. As recognized in the European Society of Cardiology/European Association for Cardiothoracic Surgery 2014 guidelines, there is substantial evidence indicating that on-pump CABG provides superior or equal short-and-long term outcomes compared with off-pump CABG in elderly patients [2,3,4,5,6,7]. However, the more frequent need for revascularization may be a major concern when treating younger patients who would be expected to live longer, and their rates of revascularization may keep rising in parallel to their follow-up.
Previous studies had suggested that the higher rate of repeat revascularization in off-pump CABG patients was related to incomplete revascularization and the surgeon’s experience [20]. In addition, the rapid progression of atherosclerosis in young patients [15] might also have precipitated the high rate of repeat revascularization in our study. Regarding the completeness of revascularization, we used graft number/disease vessels as a marker; if the number is more than 1, we deem this is complete revascularization in our database. By doing so, the completeness of revascularization in one vessel disease was 100% in both groups. The completeness of revascularization in two-vessel disease was 93% in the off-pump group and 95% in the on-pump group. The completeness of revascularization in three-vessel disease was 91% in the off-pump group and 92% in the on-pump group. In our national database, the completeness of revascularization in coronary artery patients was more than 91% in all, and there were no differences in both groups. However, we cannot trace specific surgeon’s experience in the registry database. Presuming that both groups have an equal completeness revascularization rate, we could say that the repeat revascularization was not due to incomplete surgery at the first operation. The differences might come from the procedure itself.
Actually, both methods offer good immediate results and provide also good long-term outcomes in terms of death, myocardial infarction, and stroke. We thought the choice of off-pump and on-pump procedures in the young patient should be decided by the patient’s lesion anatomy, and the surgeon’s experience and preference.
Several possible limitations to our study must be addressed. Because the study analysis was retrospective and only clinical events and services regulated by reimbursement were recorded, factors such as the extension of diseased coronary arteries and the completeness of revascularization, left ventricular ejection fraction or patients’ functional capacity, choice of conduit (percentage of bilateral internal mammary arteries or total arterial grafting), conversion between on-pump and off-pump, and surgeon experience were not evaluated. The decision to perform off-pump versus on-pump CABG was dependent on the patients’ clinical characteristics and the surgeons’ preferences. Unmeasured confounders or detection bias may thus have affected our results.
5. Conclusions
We compared on-pump and off-pump CABG in young patients using a nationwide database. There was no significant difference in short-and-long term outcomes in terms of death and MACCE. However, the need for repeat revascularization might be a concern over the long term after off-pump surgery.
Author Contributions
Conceptualization, R.O., Y.-S.C., and N.-H.C.; Formal analysis, H.-Y.Y. and N.-H.C.; Investigation, N.-H.C.; Methodology, R.O. and N.-H.C.; Resources, I-H.W., N.-K.C., and Y.-S.C.; Supervision, N.-H.C.; Validation, R.O.; Visualization, Y.-J.L.; Writing—original draft, R.O.; Writing—review & editing, N.-H.C.
Funding
This research received no external funding.
Acknowledgments
The authors thank the staff at the Seventh Core Laboratory, Department of Medical Research, National Taiwan University Hospital for their technical support. We thank members of the Department of Medical Research at National Taiwan University Hospital for helpful discussions during manuscript preparation. We would especially like to thank Yi-Jia Liou for preparing the figures. The authors would also like to acknowledge the statistical assistance provided by the Taiwan Clinical Trial Statistical Center, Training Center, and Pharmacogenomics Laboratory (founded by the National Research Program for Biopharmaceuticals) at the Ministry of Science and Technology of Taiwan. (MOST 104-2325-B-002-032, MOST 105-2314-B-002-128).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Benetti, F.J.; Naselli, G.; Wood, M.; Geffner, L. Direct Myocardial Revascularization without Extracorporeal Circulation: Experience in 700 Patients. Chest 1991, 100, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Paolasso, E.; Straka, Z.; Piegas, L.S.; Akar, A.R.; Jain, A.R.; et al. Effects of Off-Pump and On-Pump Coronary-Artery Bypass Grafting at 1 Year. N. Engl. J. Med. 2013, 368, 1179–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamy, A.; Devereaux, P.J.; Prabhakaran, D.; Taggart, D.P.; Hu, S.; Straka, Z.; Piegas, L.S.; Avezum, A.; Akar, A.R.; Lanas Zanetti, F.; et al. Five-Year Outcomes after Off-Pump or On-Pump Coronary-Artery Bypass Grafting. N. Engl. J. Med. 2016, 375, 2359–2368. [Google Scholar] [CrossRef] [PubMed]
- Shroyer, A.L.; Hattler, B.; Wagner, T.H.; Collins, J.F.; Baltz, J.H.; Quin, J.A.; Almassi, G.H.; Kozora, E.; Bakaeen, F.; Cleveland, J.C., Jr.; et al. Five-Year Outcomes after On-Pump and Off-Pump Coronary-Artery Bypass. N. Engl. J. Med. 2017, 377, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Diegeler, A.; Börgermann, J.; Kappert, U.; Breuer, M.; Böning, A.; Ursulescu, A.; Rastan, A.; Holzhey, D.; Treede, H.; Rieß, F.C.; et al. Off-Pump versus On-Pump Coronary-Artery Bypass Grafting in Elderly Patients. N. Engl. J. Med. 2013, 368, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Houlind, K.; Kjeldsen, B.J.; Madsen, S.N.; Rasmussen, B.S.; Holme, S.J.; Nielsen, P.H.; Mortensen, P.E.; DOORS Study, Group. On-pump versus off-pump coronary artery bypass surgery in elderly patients: results from the Danish on-pump versus off-pump randomization study. Circulation 2012, 125, 2431–2439. [Google Scholar] [CrossRef] [PubMed]
- Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.-P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; Jüni, P.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [CrossRef] [PubMed]
- Alkhawam, H.; Zaiem, F.; Sogomonian, R.; El-Hunjul, M.; Al-kateb, M.; Umair Bakhsh, M.; Madanieh, R. Coronary Artery Disease in Young Adults. Am. J. Med. Sci. 2015, 350, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Rubin, J.B.; Borden, W.B. Coronary Heart Disease in Young Adults. Curr. Atheroscler. Rep. 2012, 14, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, J.; Antunes, P.E.; Antunes, M.J. Coronary artery bypass surgery in young adults: excellent perioperative results and long-term survival. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, Y.; Ehara, N.; Kita, T.; Kimura, T. Abstract: P1356 CORONARY RISK FACTOR PROFILE AND PROGNOSTIC FACTORS FOR YOUNG JAPANESE PATIENTS UNDERGOING CORONARY REVASCULARIZATION. Atheroscler. Suppl. 2009, 10, e325. [Google Scholar] [CrossRef]
- Trzeciak, P.; Karolak, W.; Gąsior, M.; Zembala, M. In-hospital and long-term outcomes of coronary artery bypass graft surgery in patients ≤ 45 years of age and older (from the KROK registry). Kardiol. Pol. 2017, 75, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Tini, G.; Proietti, G.; Casenghi, M.; Colopi, M.; Bontempi, K.; Autore, C.; Volpe, M.; Musumeci, B. Long-Term Outcome of Acute Coronary Syndromes in Young Patients. High Blood Press. Cardiovasc. Prev. 2017, 24, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Fleissner, F.; Warnecke, G.; Cebotari, S.; Rustum, S.; Haverich, A.; Ismail, I. Coronary artery bypass grafting in young patients—insights into a distinct entity. J. Cardiothorac. Surg. 2015, 10, 65. [Google Scholar] [CrossRef] [PubMed]
- Rohrer-Gubler, I.; Niederhauser, U.; Turina, M.I. Late outcome of coronary artery bypass grafting in young versus older patients. Ann. Thorac. Surg. 1998, 65, 377–382. [Google Scholar] [CrossRef]
- Cole, J.H.; Miller, J.I.; Sperling, L.S.; Weintraub, W.S. Long-term follow-up of coronary artery disease presenting in young adults. J. Am. Coll. Cardiol. 2003, 41, 521–528. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, L.; Marsh, J.D. Myocardial infarction in young patients. Am. J. Med. 1999, 107, 254–261. [Google Scholar] [CrossRef]
- National Health Insurance Annual Report 2014–2015. Ministry of Health and Welfare: Taiwan, R.O.C., 2014. Available online: https://goo.gl/xrKWwj (accessed on 12 December 2013).
- Chen, J.-J.; Lin, L.-Y.; Yang, Y.-H.; Hwang, J.-J.; Chen, P.-C.; Lin, J.-L.; Chi, N.-H. On pump versus off pump coronary artery bypass grafting in patients with end-stage renal disease and coronary artery disease—A nation-wide, propensity score matched database analyses. Int. J. Cardiol. 2017, 227, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Puskas, J.D.; Mack, M.J.; Smith, C.R. On-pump versus off-pump CABG. N. Engl. J. Med. 2010, 362, 851–854. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of patient enrollment. We included 1282 patients, who were 45 years old or younger, and had isolated on-pump arrest or off-pump coronary artery bypass grafting (CABG). Among them, 197 patients were excluded for the surgeons’ adopted on-pump beating techniques. Mean follow up time was 5.53 years and longest follow up time was 16 years, with 100% complete follow up.
Figure 1.
Flowchart of patient enrollment. We included 1282 patients, who were 45 years old or younger, and had isolated on-pump arrest or off-pump coronary artery bypass grafting (CABG). Among them, 197 patients were excluded for the surgeons’ adopted on-pump beating techniques. Mean follow up time was 5.53 years and longest follow up time was 16 years, with 100% complete follow up.

Figure 2.
Kaplan–Meier survival curve. (a) All cause of death in both groups. The 5-year survival rate was 93.9% in the off-pump and 92.2% in on-pump groups; the 10-year survival rate was 86.3% in the off-pump and 82.1% in the on-pump groups. (b) Major cardiac and cerebrovascular events (death, myocardial infarction, and stoke). The 5-year free from major adverse cardiac and cerebrovascular events (MACCE) rate was 79.1% in the off-pump and 81.8% in the on-pump groups; the 10-year free from MACCE rate was 64.8% in the off-pump and 70.0% in the on-pump groups. (c) Kaplan–Meier survival curve of repeat revascularization. Off-pump carries concern of repeat revascularization in the long term. Free from revascularization at 5 years was 86.2% in on-pump vs. 80.8% in off-pump, and at 10 years, 76.1% vs. 65.9%, respectively.
Figure 2.
Kaplan–Meier survival curve. (a) All cause of death in both groups. The 5-year survival rate was 93.9% in the off-pump and 92.2% in on-pump groups; the 10-year survival rate was 86.3% in the off-pump and 82.1% in the on-pump groups. (b) Major cardiac and cerebrovascular events (death, myocardial infarction, and stoke). The 5-year free from major adverse cardiac and cerebrovascular events (MACCE) rate was 79.1% in the off-pump and 81.8% in the on-pump groups; the 10-year free from MACCE rate was 64.8% in the off-pump and 70.0% in the on-pump groups. (c) Kaplan–Meier survival curve of repeat revascularization. Off-pump carries concern of repeat revascularization in the long term. Free from revascularization at 5 years was 86.2% in on-pump vs. 80.8% in off-pump, and at 10 years, 76.1% vs. 65.9%, respectively.


{kind=link}
{kind=link}
Table 1.
Baseline characteristics of the patients.
| Characteristic | Age ≤ 45 Year (N = 1282) | |||||
|---|---|---|---|---|---|---|
| Off-Pump CABG | On-Pump CABG | P Value | Standardized Difference (%) | |||
| N | % | N | % | |||
| Patients, total No.—no. (%) | 344 | 741 | ||||
| Female sex | 34 | 9.88 | 94 | 12.69 | 0.18 | 8.86 |
| Age—year Mean/Std. Dev. | 41.04 ± 4.15 | 40.95 ± 4.13 | 2.17 | |||
| Extent of coronary artery disease | ||||||
| One-vessel disease | 55 | 15.99 | 47 | 6.34 | <0.0001 | 30.99 |
| Two-vessel disease | 72 | 20.93 | 113 | 15.25 | 14.80 | |
| Three-vessel disease | 217 | 63.08 | 581 | 78.41 | 34.18 | |
| Number of grafting | ||||||
| 1 | 57 | 16.56 | 45 | 6.07 | <0.0001 | 25.14 |
| 2 | 42 | 12.20 | 61 | 8.23 | 9.63 | |
| 3 and >3 | 245 | 71.22 | 635 | 85.69 | 8.14 | |
| Comorbidity | ||||||
| Diabetes Mellitus | 116 | 33.72 | 236 | 31.85 | 0.54 | 3.99 |
| Hyperlipidemia | 65 | 18.89 | 131 | 17.67 | 0.62 | 4.21 |
| Familial hypercholesterolemia | 6 | 1.74 | 15 | 2.02 | 0.31 | 5.11 |
| Insulin-dependent diabetes mellitus | 8 | 2.33 | 7 | 0.94 | 0.07 | 10.90 |
| Chronic obstructive pulmonary disease | 8 | 2.33 | 16 | 2.16 | 0.86 | 1.12 |
| Previous stroke | 23 | 6.69 | 45 | 6.07 | 0.70 | 2.51 |
| Peripheral vascular disease | 9 | 2.62 | 19 | 2.56 | 0.96 | 0.33 |
| Hypertension | 195 | 56.69 | 400 | 53.98 | 0.40 | 5.44 |
| History of myocardial infarction | 107 | 31.10 | 214 | 28.88 | 0.45 | 4.86 |
| History of atrial fibrillation | 5 | 1.45 | 6 | 0.81 | 0.32 | 6.09 |
| Implanted pacemaker | 7 | 2.03 | 8 | 1.08 | 0.21 | 7.72 |
| Normal renal function | 322 | 93.60 | 698 | 94.20 | 0.70 | 2.48 |
| Chronic kidney disease | 5 | 1.45 | 8 | 1.08 | 0.60 | 3.34 |
| Renal-replacement therapy | 17 | 4.94 | 36 | 4.86 | 0.95 | 0.39 |
| Prior percutaneous coronary intervention | 97 | 28.19 | 199 | 26.85 | 0.63 | 5.23 |
| Surgical Timing—emergency | 48 | 13.95 | 102 | 13.76 | 0.91 | 0.41 |
CABG: coronary artery bypass grafting; Std. Dev.: Standard Deviation.
Table 2.
Outcomes at 30 days.
| Outcome | Off-Pump CABG | On-Pump CABG | Adjusted Gender and Age and Other Variables (with Stepwise Selection) | |||
|---|---|---|---|---|---|---|
| Hazard Ratio (On:off) | P Value | |||||
| HR | 95% C.I. | |||||
| Low | Up | |||||
| Operative outcome | ||||||
| Transfusion—pRBC (unit) | 2.56 ± 1.45 | 3.12 ± 1.63 | 0.93 | 0.34 | 2.42 | 0.672 |
| Post-OP atrial fibrillation—no. (%) | 36 (10.46) | 102 (13.76) | 1.32 | 0.41 | 2.16 | 0.535 |
| ICU stay (days) | 1.4 ± 0.82 | 1.5 ± 0.93 | 1.02 | 0.81 | 1.32 | 0.812 |
| Hospital stay (days) | 8.2 ± 3.58 | 9.1 ± 4.21 | 1.15 | 0.36 | 4.21 | 0.781 |
| Components of primary outcome—no. (%) | ||||||
| Death | 2 (0.58%) | 3 (0.4%) | 1.43 | 0.15 | 13.75 | 0.7581 |
| Myocardial infarction | 4 (0.11%) | 7 (0.94%) | 0.84 | 0.25 | 2.87 | 0.7805 |
| Stroke | 2 (0.58%) | 2 (0.28%) | 0.41 | 0.03 | 6.63 | 0.5266 |
| New renal failure requiring dialysis | 5 (1.45%) | 12 (1.62%) | 1.10 | 0.39 | 3.14 | 0.8596 |
| Other specified outcomes—no. (%) | ||||||
| Cardiovascular-related death | 1 (0.29%) | 1 (0.13%) | 0.46 | 0.03 | 7.29 | 0.5781 |
pRBC: Red blood cell; ICU: intensive care unit; CABG: coronary artery bypass grafting; HR: hazard ratio; C.I.: confidence interval.
Table 3.
Outcomes at 1 year.
| Outcome | Off-Pump CABG | On-Pump CABG | Adjusted Gender and Age and Other Variables (with Stepwise Selection) | |||
|---|---|---|---|---|---|---|
| Hazard Ratio (On:off) | P Value | |||||
| HR | 95% C.I. | |||||
| Low | Up | |||||
| Components of primary outcome—no. (%) | ||||||
| Death | 7 (2.03%) | 12 (1.62%) | 0.80 | 0.32 | 2.03 | 0.6392 |
| Myocardial infarction | 11 (3.2%) | 36 (4.86%) | 1.46 | 0.73 | 2.89 | 0.2819 |
| Stroke | 6 (1.74%) | 11 (1.48%) | 0.87 | 0.31 | 2.41 | 0.7879 |
| New renal failure requiring dialysis | 13 (3.78%) | 35 (4.72%) | 1.59 | 0.83 | 3.05 | 0.1622 |
| Other specified outcomes—no. (%) | ||||||
| Cardiovascular-related death | 13 (3.78%) | 11 (1.48%) | 0.98 | 0.23 | 4.22 | 0.9738 |
Table 4.
Outcomes at 5 years.
| Outcome | Off-Pump CABG | On-Pump CABG | Adjusted Gender and Age and Other Variables (with Stepwise Selection) | |||
|---|---|---|---|---|---|---|
| Hazard Ratio (On:off) | P Value | |||||
| HR | 95% C.I. | |||||
| Low | Up | |||||
| Components of primary outcome—no. (%) | ||||||
| Death | 16 (4.65%) | 45 (6.07%) | 1.27 | 0.72 | 2.25 | 0.4109 |
| Myocardial infarction | 28 (8.14%) | 67 (9.04%) | 1.11 | 0.71 | 1.74 | 0.6420 |
| Stroke | 18 (5.23%) | 37 (4.99%) | 1.00 | 0.56 | 1.77 | 0.9909 |
| New renal failure requiring dialysis | 29 (8.43%) | 68 (9.18%) | 1.18 | 0.76 | 1.84 | 0.4650 |
| Other specified outcomes—no. (%) | ||||||
| Cardiovascular-related death | 5 (1.45%) | 13 (1.75%) | 1.14 | 0.41 | 3.21 | 0.7996 |
| Cerebrovascular disease death | 2 (0.58%) | 2 (0.27%) | 1.18 | 0.10 | 13.64 | 0.8945 |
Table 5.
Outcomes followed by death.
| Outcome | Off-Pump CABG | On-Pump CABG | Adjusted Gender and Age and other Variables (with Stepwise Selection) | |||
|---|---|---|---|---|---|---|
| Hazard Ratio (On:off) | P Value | |||||
| HR | 95% C.I. | |||||
| Low | Up | |||||
| Components of primary outcome—no. (%) | ||||||
| Death | 25 (7.27%) | 70 (9.45%) | 1.15 | 0.73 | 1.83 | 0.5492 |
| Myocardial infarction | 35 (10.17%) | 90 (12.15%) | 1.12 | 0.75 | 1.67 | 0.5737 |
| Stroke | 22 (6.4%) | 48 (6.48%) | 0.99 | 0.60 | 1.65 | 0.9731 |
| New renal failure requiring dialysis | 32 (9.3%) | 79 (10.66%) | 1.14 | 0.75 | 1.72 | 0.5533 |
| Other specified outcomes—no. (%) | ||||||
| Cardiovascular-related death | 5 (1.45%) | 15 (2.02%) | 1.30 | 0.47 | 3.58 | 0.6113 |
| Cerebrovascular disease death | 2 (0.58%) | 2 (0.27%) | 1.18 | 0.10 | 13.64 | 0.8945 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Okano, R.; Liou, Y.-J.; Yu, H.-Y.; Wu, I.-H.; Chou, N.-K.; Chen, Y.-S.; Chi, N.-H. Coronary Artery Bypass in Young Patients—On or Off-Pump? J. Clin. Med. 2019, 8, 128. https://doi.org/10.3390/jcm8020128
AMA Style
Okano R, Liou Y-J, Yu H-Y, Wu I-H, Chou N-K, Chen Y-S, Chi N-H. Coronary Artery Bypass in Young Patients—On or Off-Pump? Journal of Clinical Medicine. 2019; 8(2):128. https://doi.org/10.3390/jcm8020128
Chicago/Turabian StyleOkano, Ryoi, Yi-Jia Liou, Hsi-Yu Yu, I-Hui Wu, Nai-Kuan Chou, Yih-Sharng Chen, and Nai-Hsin Chi. 2019. "Coronary Artery Bypass in Young Patients—On or Off-Pump?" Journal of Clinical Medicine 8, no. 2: 128. https://doi.org/10.3390/jcm8020128
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.