A Culture-Independent Analysis of the Microbiota of Female Interstitial Cystitis/Bladder Pain Syndrome Participants in the MAPP Research Network

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Specimens
2.2. Specimen Handling
2.3. DNA Extraction and Ibis Eubacterial and Fungal Domain Assays on the PLEX-ID
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Clinical Data
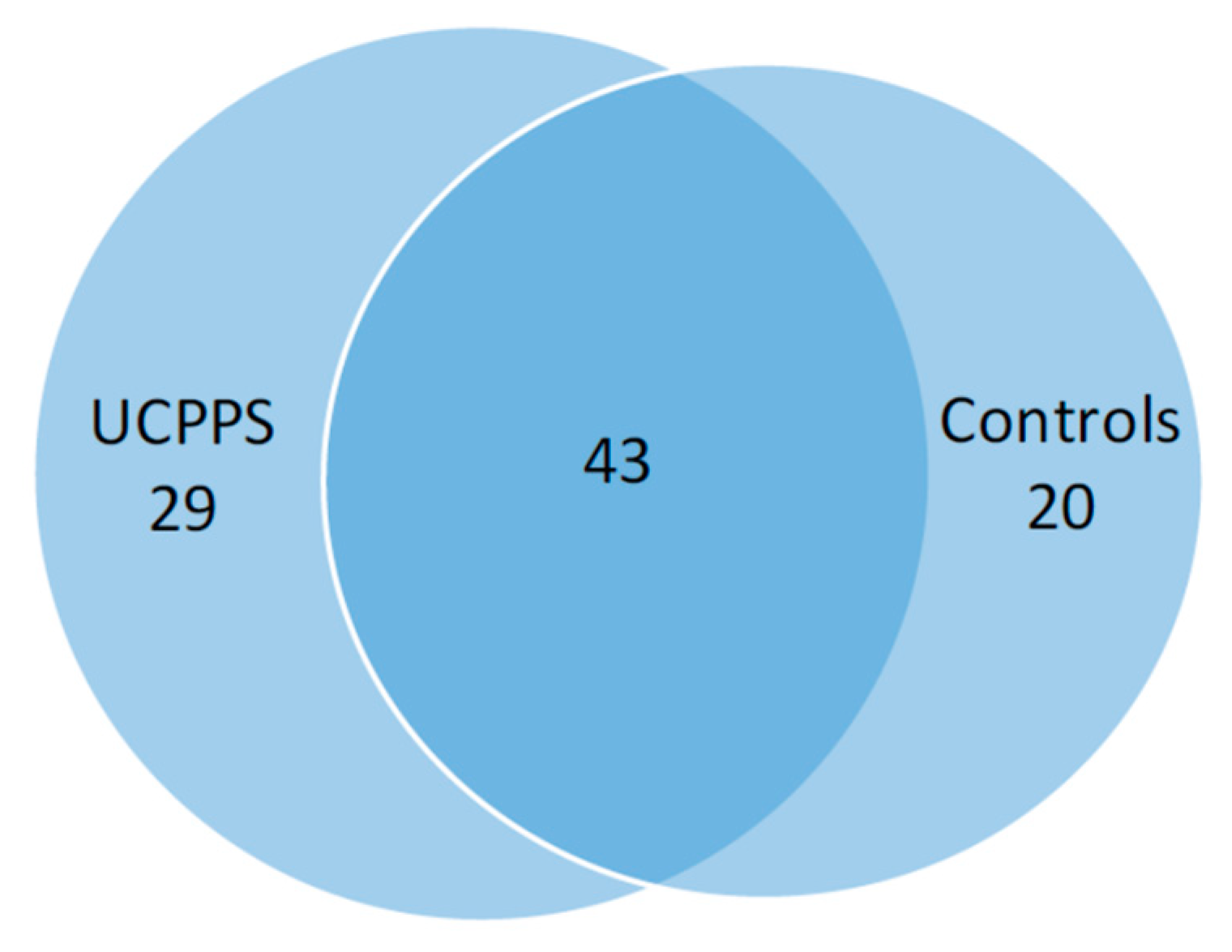
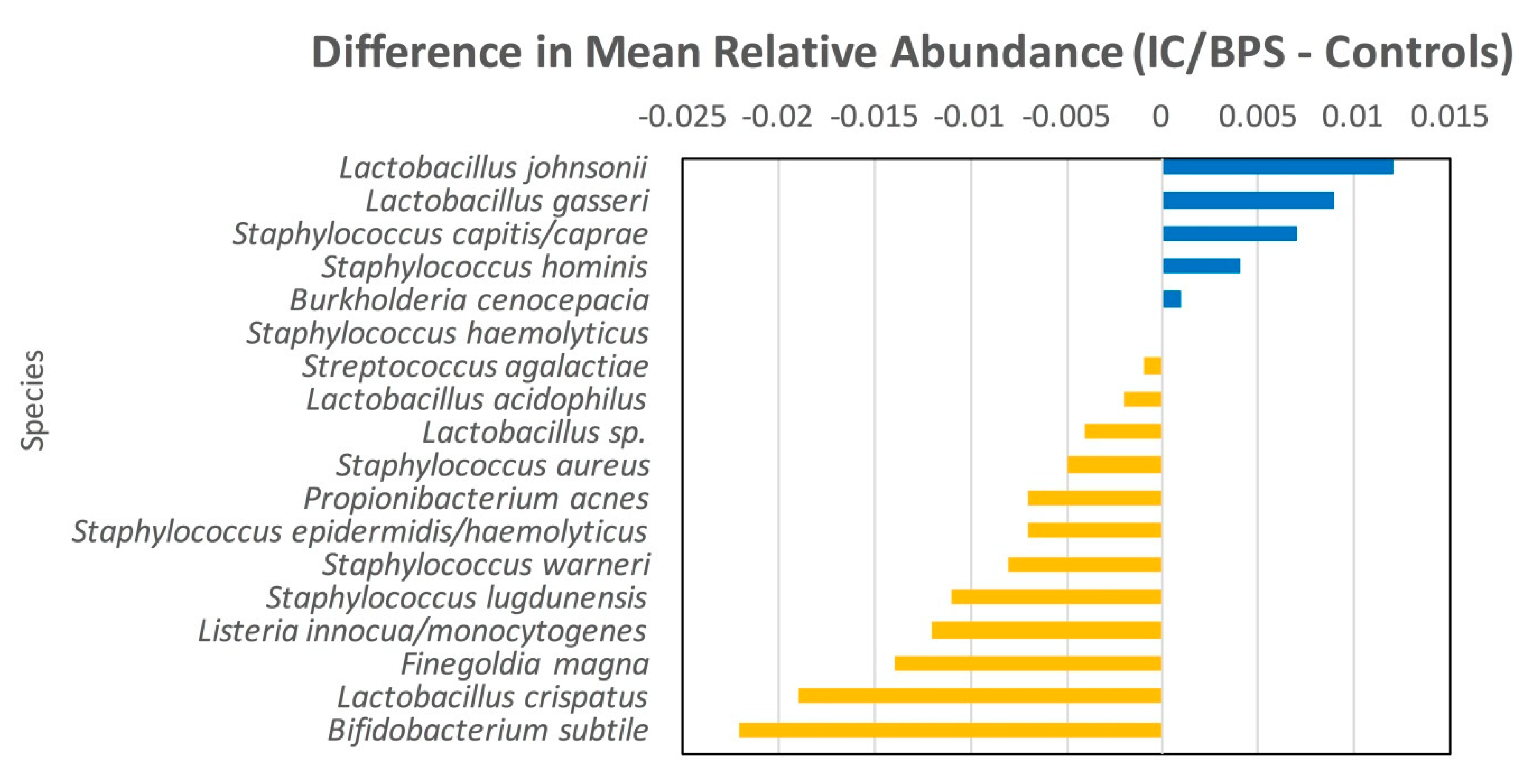
3.3. Species Data
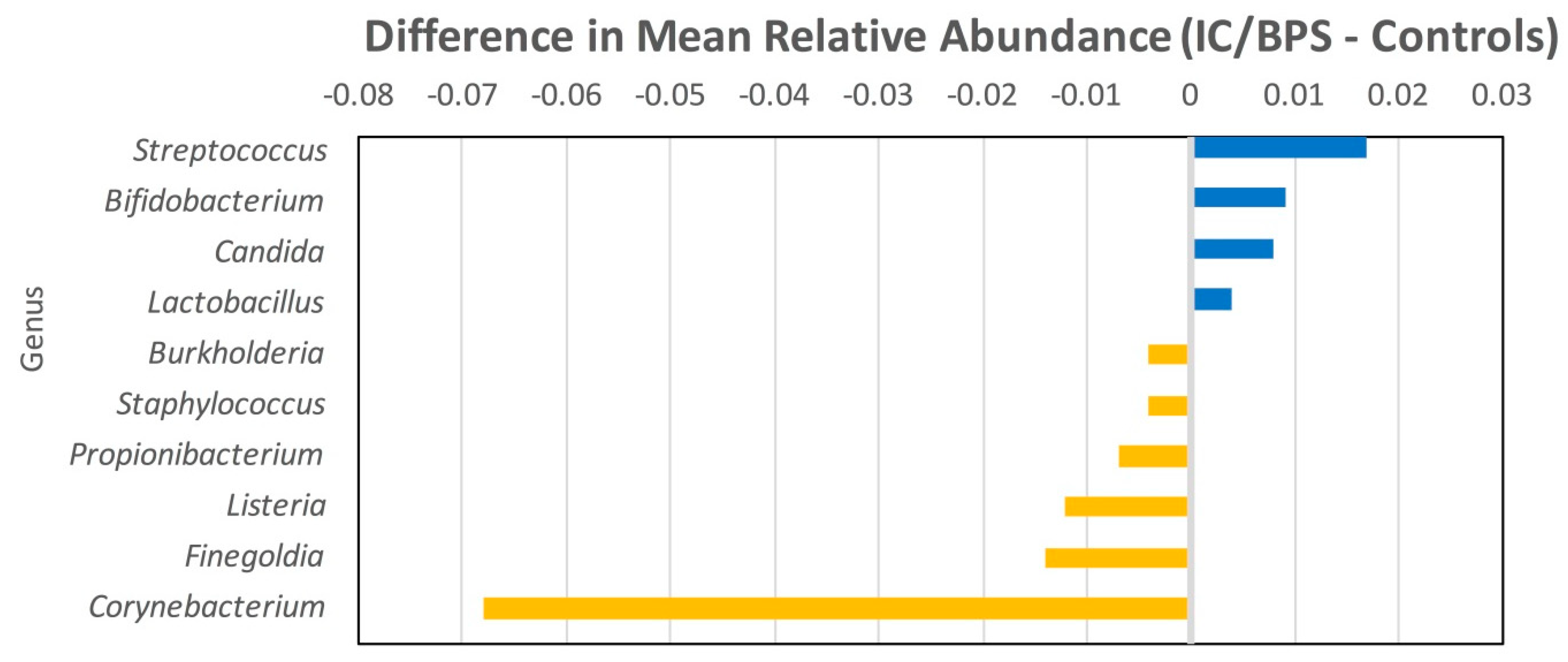
3.4. Genus Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. NIH/NIDDK MAPP Network

Appendix B. Inclusion and Exclusion Criteria for MAPP 1. Adapted from [24]
Appendix B.1. Inclusion Criteria
Appendix B.2. Exclusion Criteria
Appendix B.3. Eligibility Criteria for Controls
Appendix C. Details of Methodology in Regard to PLEX-ID Analysis
References
- Hanno, P.M.; Burks, D.A.; Clemens, J.Q.; Dmochowski, R.R.; Erickson, D.; Fitzgerald, M.P.; Forrest, J.B.; Gordon, B.; Gray, M.; Mayer, R.D.; et al. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J. Urol. 2011, 185, 2162–2170. [Google Scholar] [CrossRef]
- Clemens, J.Q.; Meenan, R.T.; O’Keeffe Rosetti, M.C.; Brown, S.O.; Gao, S.Y.; Calhoun, E.A. Prevalence of interstitial cystitis symptoms in a managed care population. J. Urol. 2005, 174, 576–580. [Google Scholar] [CrossRef]
- Nickel, J.C.; Tripp, D.A.; Beiko, D.; Tolls, V.; Herschorn, S.; Carr, L.K.; Kelly, K.; Golda, N. The Interstitial Cystitis/Bladder Pain Syndrome Clinical Picture: A Perspective from Patient Life Experience. Urol. Pract. 2018, 5, 286–292. [Google Scholar] [CrossRef]
- Giannantoni, A.; Bini, V.; Dmochowski, R.; Hanno, P.; Nickel, J.C.; Proietti, S.; Wyndaele, J.J. Contemporary Management of the Painful Bladder. Eur. Urol. 2012, 61, 29–53. [Google Scholar] [CrossRef] [PubMed]
- Domingue, G.J.; Ghoniem, G.M. Dormant microbes in interstitial cystitis. J. Urol. 1995, 153, 1321–1326. [Google Scholar] [CrossRef]
- Heritz, D.M.; Lacroix, J.M.; Batra, S.D.; Jarvi, K.A.; Beheshti, B.; Mittelman, M.W. Detection of eubacteria in interstitial cystitis by 16S rDNA amplification. J. Urol. 1997, 158, 2291–2297. [Google Scholar] [CrossRef]
- Haarala, M.; Kiilholma, P.; Lehtonen, O.P. Urinary bacterial flora of women with urethral syndrome and interstitial cystitis. Gynecol. Obstet. Investig. 1999, 47, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Haarala, M.; Kiiholma, P.; Nurmi, M.; Uksila, J.; Alanen, A. The role of Borrelia burgdorferi in interstitial cystitis. Eur. Urol. 2000, 37, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.; Dixon, R.A. A study to detect Helicobacter pylori in fresh and archival specimens from patients with interstitial cystitis, using amplification methods. BJU Int. 2003, 91, 814–816. [Google Scholar] [CrossRef]
- Atug, F.; Turkeri, L.; Atug, O.; Cal, C. Detection of Helicobacter pylori in bladder biopsy specimens of patients with interstitial cystitis by polymerase chain reaction. Urol. Res. 2004, 32, 346–349. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, G.D.; Greenberg, S.J. PCR-Based Diagnostics in Infectious Disease; Blackwell Scientific Publications: Boston, MA, USA, 1994; 697p. [Google Scholar]
- Khasriya, R.; Sathiananthamoothy, S.; Ismail, S.; Kelsey, M.; Wilson, M.; Rohn, J.L.; Malone-Lee, J. Spectrum of bacterial colonization associated with urothelial cells from patients with chronic lower urinary tract symptoms. J. Clin. Microbiol. 2013, 51, 2054–2062. [Google Scholar] [CrossRef] [PubMed]
- Hilt, E.E.; McKinley, K.; Pearce, M.M.; Rosenfeld, A.B.; Zilliox, M.J.; Mueller, E.R.; Brubaker, L.; Gai, X.; Wolfe, A.J.; Schreckenberger, P.C. Bacterial Flora in the Adult Female Bladder Culture Techniques to Detect Resident Urine Is Not Sterile: Use of Enhanced Urine. J. Clin. Microbiol. 2014, 52, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, S.A.; Razvi, H.; Dave, S.; Reid, G.; Burton, J.P. The microbiome of the urinary tract—A role beyond infection. Nat. Rev. Urol. 2015, 12, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Thomas-White, K.; Brady, M.; Wolfe, A.J.; Mueller, E.R. The bladder is not sterile: History and current discoveries on the urinary microbiome. Curr. Bladder Dysfunct. Rep. 2016, 11, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, M.M.; Hilt, E.E.; Rosenfeld, A.B.; Zilliox, M.J.; Thomas-White, K.; Fok, C.; Kliethermes, S.; Schreckenberger, P.C.; Brubaker, L.; Gai, X.; et al. The female urinary microbiome: A comparison of women with and without urgency urinary incontinence. mBio 2014, 8, e01283-14. [Google Scholar] [CrossRef] [PubMed]
- Karstens, L.; Asquith, M.; Davin, S. Does the urinary microbiome play a role in urgency urinary incontinence and its severity. Front. Cell. Infect. Microbiol. 2016, 27, 78. [Google Scholar] [CrossRef] [PubMed]
- Thomas-White, K.J.; Kliethermes, S.; Rickey, L.; Lukacz, E.S.; Richter, H.E.; Moalli, P.; Zimmern, P.; Norton, P.; Kusek, J.W.; Wolfe, A.J.; et al. Evaluation of the urinary microbiota of women with uncomplicated stress urinary incontinence. Am. J. Obstet. Gynecol. 2017, 216, 55.e1–55.e16. [Google Scholar] [CrossRef] [PubMed]
- Al-Hadithi, H.N.; Williams, H.; Hart, C.A.; Frazer, M.; Adams, E.J.; Richmond, D.H.; Tincello, D.G. Absence of bacterial and viral DNA in bladder biopsies from patients with interstitial cystitis/chronic pelvic pain syndrome. J. Urol. 2005, 174, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Ecker, D.J.; Sampath, R.; Massire, C.; Blyn, L.B.; Hall, T.A.; Eshoo, M.W.; Hofstadler, S.A. Ibis T5000: A universal biosensor approach for microbiology. Nat. Rev. Microbiol. 2008, 6, 553–558. [Google Scholar] [CrossRef]
- Nickel, J.C.; Stephens, A.; Landis, J.R.; Chen, J.; Mullins, C.; van Bokhoven, A.; Lucia, M.S.; Melton-Kreft, R.; Ehrlich, G.D.; MAPP Research Network. Search for Microorganisms in Men with Urologic Chronic Pelvic Pain Syndrome: A Culture-Independent Analysis in the MAPP Research Network. J. Urol. 2015, 194, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Nickel, J.C.; Stephens, A.; Landis, J.R.; Mullins, C.; van Bokhoven, A.; Lucia, M.S.; Ehrlich, G.D.; MAPP Research Network. Assessment of the Lower Urinary Tract Microbiota during Symptom Flare in Women with Urologic Chronic Pelvic Pain Syndrome: A MAPP Network Study. J. Urol. 2016, 195, 356–362. [Google Scholar] [CrossRef]
- Clemens, J.Q.; Mullins, C.; Kusek, J.W.; Kirkali, Z.; Mayer, E.A.; Rodríguez, L.V.; Klumpp, D.J.; Schaeffer, A.J.; Kreder, K.J.; Buchwald, D.; et al. The MAPP research network: A novel study of urologic chronic pelvic pain syndromes. BMC Urol. 2014, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Williams, D.A.; Lucia, M.S.; Clauw, D.J.; Naliboff, B.D.; Robinson, N.A.; van Bokhoven, A.; Sutcliffe, S.; Schaeffer, A.J.; Rodriguez, L.V.; et al. The MAPP research network: Design, patient characterization and operations. BMC Urol. 2014, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Chao, A. Non-parametric estimation of the number of classes in a population. Scand. J. Stat. 1984, 11, 265–270. [Google Scholar]
- Shannon, C.E.; Weaver, W. The Mathematical Theory of Communication; The University of Illinois Press: Urbana, IL, USA, 1949; 117p. [Google Scholar]
- Anderson, M.J. A new method for non-parametric multivariate analysis of variance. Aust. Ecol. 2001, 26, 32–46. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Siddiqui, H.; Lagesen, K.; Nederbragt, A.J.; Jeansson, S.L.; Jakobsen, K.S. Alterations of microbiota in urine from women with interstitial cystitis. BMC Microbiol. 2012, 12, 205. [Google Scholar] [CrossRef]
- Brauundmeier-Fleming, A.; Russell, N.T.; Nas, M.Y.; Yaggie, R.E.; Berry, M.; Bachrach, L.; Flury, S.C.; Marko, D.S.; Bushell, C.B.; et al. Stool-based biomarkers of interstitial cystitis/bladder pain syndrome. Sci. Rep. 2016, 6, 26083. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Category | *IC/BPS | Controls | Total | p |
|---|---|---|---|---|---|
| Number of Participants | n (%) | 181 | 182 | 363 | |
| Clinical Site | Northwestern U | 17 (9.4%) | 22 (12.1%) | 39 (10.7%) | 0.906 |
| UCLA | 25 (13.8%) | 24 (13.2%) | 49 (13.5%) | ||
| U of Iowa | 36 (19.9%) | 29 (15.9%) | 65 (17.9%) | ||
| U of Michigan | 33 (18.2%) | 33 (18.1%) | 66 (18.2%) | ||
| U of Washington | 23 (12.7%) | 29 (15.9%) | 52 (14.3%) | ||
| Wash U St. Louis | 39 (21.5%) | 37 (20.3%) | 76 (20.9%) | ||
| Stanford U | 8 (4.4%) | 8 (4.4%) | 16 (4.4%) | ||
| Age Group | <35 years | 76 (42.0%) | 81 (44.5%) | 157 (43.3%) | 0.869 |
| 35–50 years | 50 (27.6%) | 50 (27.5%) | 100 (27.5%) | ||
| 50+ years | 55 (30.4%) | 51 (28.0%) | 106 (29.2%) | ||
| Race | White | 165 (91.2%) | 137 (75.3%) | 302 (83.2%) | <0.001 |
| Black | 5 (2.8%) | 25 (13.7%) | 30 (8.3%) | ||
| Asian | 2 (1.1%) | 10 (5.5%) | 12 (3.3%) | ||
| Multi Race | 3 (1.7%) | 5 (2.7%) | 8 (2.2%) | ||
| Other | 5 (2.8%) | 4 (2.2%) | 9 (2.5%) | ||
| Unknown | 1 (0.6%) | 1 (0.5%) | 2 (0.6%) | ||
| Ethnicity | Hispanic | 11 (6.1%) | 11 (6.0%) | 22 (6.1%) | 1.000 |
| Non-Hispanic | 170 (93.9%) | 171 (94.0%) | 341 (93.9%) |
| Parameter | Category | IC/BPS | Controls | Total | p |
|---|---|---|---|---|---|
| Number of Participants | n (%) | 181 | 182 | 363 | |
| Self-reported IC diagnosis | No | 24 (13.3%) | 169 (92.9%) | 193 (53.2%) | <0.001 |
| Yes | 157 (86.7%) | 2 (1.1%) | 159 (43.8%) | ||
| Missing | 11 (6.0%) | 11 (3.0%) | |||
| Meet MAPP IC/BPS Criteria | Yes | 181 (100.0%) | 181 (49.9%) | ||
| Missing | 182 (100.0%) | 182 (50.1%) | |||
| IC diagnosis from Rice form | No | 64 (35.4%) | 172 (94.5%) | 236 (65.0%) | <0.001 |
| Yes | 117 (64.6%) | 10 (5.5%) | 127 (35.0%) | ||
| Associated Chronic Pain Syndrome | None | 105 (58.0%) | 110 (60.4%) | 215 (59.2%) | 0.670 |
| Any Syndrome | 76 (42.0%) | 72 (39.6%) | 148 (40.8%) | ||
| Interstitial Cystitis Symptom Index (ICSI) | 10.9 (4.4) | 3.0 (3.2) | 7.0 (5.5) | <0.001 | |
| Genitourinary Pain Index (GUPI) | 26.6 (8.7) | 4.7 (7.4) | 15.7 (13.6) | <0.001 | |
| Meds for urologic or pelvic pain symptoms | No | 37 (20.4%) | 176 (96.7%) | 213 (58.7%) | <0.001 |
| Yes | 144 (79.6%) | 6 (3.3%) | 150 (41.3%) | ||
| Pain medication class | None | 36 (19.9%) | 121 (66.5%) | 157 (43.3%) | <0.001 |
| Peripheral | 42 (23.2%) | 24 (13.2%) | 66 (18.2%) | ||
| Central | 81 (44.8%) | 28 (15.4%) | 109 (30.0%) | ||
| Opioid | 22 (12.2%) | 9 (4.9%) | 31 (8.5%) |
| Species unique to IC/BPS | Species unique to Controls | Species found in both: |
|---|---|---|
| 1. Acinetobacter grimontii | 1. Bordetella parapertussis | 1. Bacteroides ureolyticus |
| 2. Akkermansia muciniphila | 2. Burkholderia sp. | 2. Bifidobacterium inopinatum |
| 3. Bacillus sp. | 3. Clostridium sp. | 3. Bifidobacterium longum |
| 4. Bifidobacterium bifidum | 4. Enterococcus faecium | 4. Bifidobacterium subtile |
| 5. Bifidobacterium infantis | 5. Haemophilus influenzae | 5. Bordetella bronchiseptica |
| 6. Borrelia turicatae | 6. Klebsiella oxytoca | 6. Burkholderia cenocepacia |
| 7. Candida dubliniensis | 7. Klebsiella pneumoniae | 7. Candida albicans |
| 8. Clostridium perfringens | 8. Lactobacillus collinoides | 8. Candida glabrata |
| 9. Escherichia coli | 9. Ochrobactrum anthropi | 9. Corynebacterium diphtheriae |
| 10. Helicobacter hepaticus | 10. Pasteurella multocida | 10. Corynebacterium jeikeium |
| 11. Lactobacillus casei | 11. Pediococcus pentosaceus | 11. Corynebacterium pseudodiphtheriticum |
| 12. Lactobacillus helveticus | 12. Pseudomonas stutzeri | |
| 13. Lactobacillus reuteri | 13. Serratia marcescens | |
| 14. Lactococcus lactis | 14. Streptococcus mutans | |
| 15. Proteus mirabilis | 15. Streptococcus sanguinis | |
| 16. Pseudomonas aeruginosa | 16. Treponema denticola | |
| 17. Salmonella enterica | 17. Ureaplasma urealyticum | |
| 18. Staphylococcus intermedius | 18. Francisella philomiragia | |
| 19. Streptococcus dysgalactiae | 19. Corynebacterium striatum | |
| 20. Streptococcus porcinus | 20. Microbacterium sp. | |
| 21. Streptococcus pyogenes | ||
| 22. Bacteroides vulgatus | ||
| 23. Bifidobacterium pseudocatenulatum | ||
| 24. Francisella tularensis | ||
| 25. Mycoplasma hyorhinis | ||
| 26. Paracoccus denitrificans | ||
| 27. Staphylococcus sp. | ||
| 28. Micrococcus lylae | ||
| 29. Tetragenococcus halophilus |
| Taxonomic Level | Index | Controls | UCPPS | p1 | ||
|---|---|---|---|---|---|---|
| n | Mean (SD) | n | Mean (SD) | |||
| Species | Chao1 | 182 | 2.3 (1.3) | 181 | 2.5 (1.5) | 0.18 |
| Shannon | 182 | 0.2 (0.3) | 181 | 0.3 (0.3) | 0.15 | |
| Genus | Chao1 | 182 | 1.9 (1.1) | 181 | 2 (1.1) | 0.41 |
| Shannon | 182 | 0.2 (0.3) | 181 | 0.2 (0.3) | 0.38 | |
| Controls | UCPPS | Associate: Prevalence | Association: Relative Abundance | |||||
|---|---|---|---|---|---|---|---|---|
| taxa | Prevalence | Mean (SD) Relative Abundance | Prevalence | Mean (SD) Relative Abundance | OR (95% CI) | p1 | Mean Difference | p2 |
| Staphylococcus hominis | 20/182 (11%) | 0.01 (0.055) | 29/181 (16%) | 0.014 (0.091) | 1.55 (0.84,2.85) | 0.163 | 0.004 | 0.216 |
| Staphylococcus lugdunensis | 6/182 (3.3%) | 0.012 (0.106) | 6/181 (3.3%) | 0.002 (0.016) | 1.01 (0.32,3.18) | 0.992 | −0.011 | 0.996 |
| Staphylococcus warneri | 10/182 (5.5%) | 0.011 (0.091) | 4/181 (2.2%) | 0.003 (0.043) | 0.39 (0.12,1.26) | 0.116 | −0.008 | 0.098 |
| Streptococcus agalactiae | 11/182 (6%) | 0.009 (0.068) | 11/181 (6.1%) | 0.008 (0.078) | 1.01 (0.42,2.38) | 0.989 | −0.001 | 0.972 |
| Bifidobacterium subtile | 26/182 (14.3%) | 0.128 (0.322) | 26/181 (14.4%) | 0.106 (0.282) | 1.01 (0.56,1.81) | 0.982 | −0.022 | 0.872 |
| Burkholderia cenocepacia | 12/182 (6.6%) | 0.018 (0.128) | 8/181 (4.4%) | 0.019 (0.128) | 0.66 (0.26,1.64) | 0.367 | 0.001 | 0.389 |
| Finegoldia magna | 10/182 (5.5%) | 0.018 (0.113) | 12/181 (6.6%) | 0.004 (0.029) | 1.22 (0.51,2.9) | 0.651 | −0.014 | 0.703 |
| Lactobacillus acidophilus | 21/182 (11.5%) | 0.062 (0.223) | 20/181 (11%) | 0.06 (0.22) | 0.95 (0.5,1.82) | 0.883 | −0.002 | 0.878 |
| Lactobacillus crispatus | 54/182 (29.7%) | 0.277 (0.434) | 51/181 (28.2%) | 0.258 (0.419) | 0.93 (0.59,1.46) | 0.753 | −0.019 | 0.415 |
| Lactobacillus gasseri | 5/182 (2.7%) | 0.015 (0.11) | 12/181 (6.6%) | 0.024 (0.122) | 2.51 (0.87,7.29) | 0.090 | 0.009 | 0.084 |
| Lactobacillus johnsonii | 45/182 (24.7%) | 0.027 (0.127) | 51/181 (28.2%) | 0.038 (0.146) | 1.19 (0.75,1.91) | 0.456 | 0.012 | 0.329 |
| Lactobacillus sp. | 11/182 (6%) | 0.059 (0.233) | 11/181 (6.1%) | 0.055 (0.218) | 1.01 (0.42,2.38) | 0.989 | −0.004 | 0.96 |
| Listeria innocua/monocytogenes | 8/182 (4.4%) | 0.013 (0.098) | 5/181 (2.8%) | 0.001 (0.016) | 0.62 (0.2,1.93) | 0.407 | −0.012 | 0.39 |
| Propionibacterium acnes | 10/182 (5.5%) | 0.036 (0.173) | 12/181 (6.6%) | 0.03 (0.145) | 1.22 (0.51,2.9) | 0.651 | −0.007 | 0.686 |
| Staphylococcus aureus | 6/182 (3.3%) | 0.006 (0.051) | 4/181 (2.2%) | 0.001 (0.008) | 0.66 (0.18,2.39) | 0.560 | −0.005 | 0.524 |
| Staphylococcus capitis/caprae | 8/182 (4.4%) | 0.009 (0.077) | 7/181 (3.9%) | 0.016 (0.108) | 0.88 (0.31,2.47) | 0.801 | 0.007 | 0.814 |
| Staphylococcus epidermidis/haemolyticus | 57/182 (31.3%) | 0.05 (0.184) | 61/181 (33.7%) | 0.042 (0.171) | 1.11 (0.72,1.73) | 0.628 | −0.007 | 0.816 |
| Staphylococcus haemolyticus | 10/182 (5.5%) | 0.004 (0.037) | 11/181 (6.1%) | 0.004 (0.031) | 1.11 (0.46,2.69) | 0.812 | 0.000 | 0.819 |
| Controls | UCPPS | Associate: Prevalence | Association: Relative Abundance | |||||
|---|---|---|---|---|---|---|---|---|
| Taxa | Prevalence | Mean (SD) Relative Abundance | Prevalence | Mean (SD) Relative Abundance | OR (95% CI) | p1 | Mean Difference | p2 |
| Bifidobacterium | 28/182 (15.4%) | 0.138 (0.333) | 35/181 (19.3%) | 0.148 (0.327) | 1.32 (0.76,2.28) | 0.321 | 0.009 | 0.461 |
| Burkholderia | 13/182 (7.1%) | 0.023 (0.147) | 8/181 (4.4%) | 0.019 (0.128) | 0.6 (0.24,1.49) | 0.271 | −0.004 | 0.283 |
| Candida | 5/182 (2.7%) | 0 (0.004) | 11/181 (6.1%) | 0.009 (0.078) | 2.29 (0.78,6.73) | 0.132 | 0.008 | 0.119 |
| Corynebacterium | 23/182 (12.6%) | 0.08 (0.248) | 6/181 (3.3%) | 0.012 (0.085) | 0.24 (0.09,0.6) | 0.002* | −0.068 | 0.001 * |
| Finegoldia | 10/182 (5.5%) | 0.018 (0.113) | 12/181 (6.6%) | 0.004 (0.029) | 1.22 (0.51,2.9) | 0.651 | −0.014 | 0.703 |
| Lactobacillus | 104/182 (57.1%) | 0.457 (0.473) | 109/181 (60.2%) | 0.461 (0.461) | 1.14 (0.75,1.72) | 0.552 | 0.004 | 0.822 |
| Listeria | 8/182 (4.4%) | 0.013 (0.098) | 5/181 (2.8%) | 0.001 (0.016) | 0.62 (0.2,1.93) | 0.407 | −0.012 | 0.39 |
| Propionibacterium | 10/182 (5.5%) | 0.036 (0.173) | 12/181 (6.6%) | 0.03 (0.145) | 1.22 (0.51,2.9) | 0.651 | −0.007 | 0.686 |
| Staphylococcus | 101/182 (55.5%) | 0.107 (0.258) | 99/181 (54.7%) | 0.103 (0.263) | 0.97 (0.64,1.46) | 0.879 | −0.004 | 0.511 |
| Streptococcus | 17/182 (9.3%) | 0.018 (0.099) | 26/181 (14.4%) | 0.035 (0.156) | 1.63 (0.85,3.12) | 0.141 | 0.017 | 0.141 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nickel, J.C.; Stephens-Shields, A.J.; Landis, J.R.; Mullins, C.; van Bokhoven, A.; Lucia, M.S.; Henderson, J.P.; Sen, B.; Krol, J.E.; Ehrlich, G.D.; et al. A Culture-Independent Analysis of the Microbiota of Female Interstitial Cystitis/Bladder Pain Syndrome Participants in the MAPP Research Network. J. Clin. Med. 2019, 8, 415. https://doi.org/10.3390/jcm8030415
Nickel JC, Stephens-Shields AJ, Landis JR, Mullins C, van Bokhoven A, Lucia MS, Henderson JP, Sen B, Krol JE, Ehrlich GD, et al. A Culture-Independent Analysis of the Microbiota of Female Interstitial Cystitis/Bladder Pain Syndrome Participants in the MAPP Research Network. Journal of Clinical Medicine. 2019; 8(3):415. https://doi.org/10.3390/jcm8030415
Chicago/Turabian StyleNickel, J. Curtis, Alisa J. Stephens-Shields, J. Richard Landis, Chris Mullins, Adrie van Bokhoven, M. Scott Lucia, Jeffrey P. Henderson, Bhaswati Sen, Jaroslaw E. Krol, Garth D. Ehrlich, and et al. 2019. "A Culture-Independent Analysis of the Microbiota of Female Interstitial Cystitis/Bladder Pain Syndrome Participants in the MAPP Research Network" Journal of Clinical Medicine 8, no. 3: 415. https://doi.org/10.3390/jcm8030415