Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
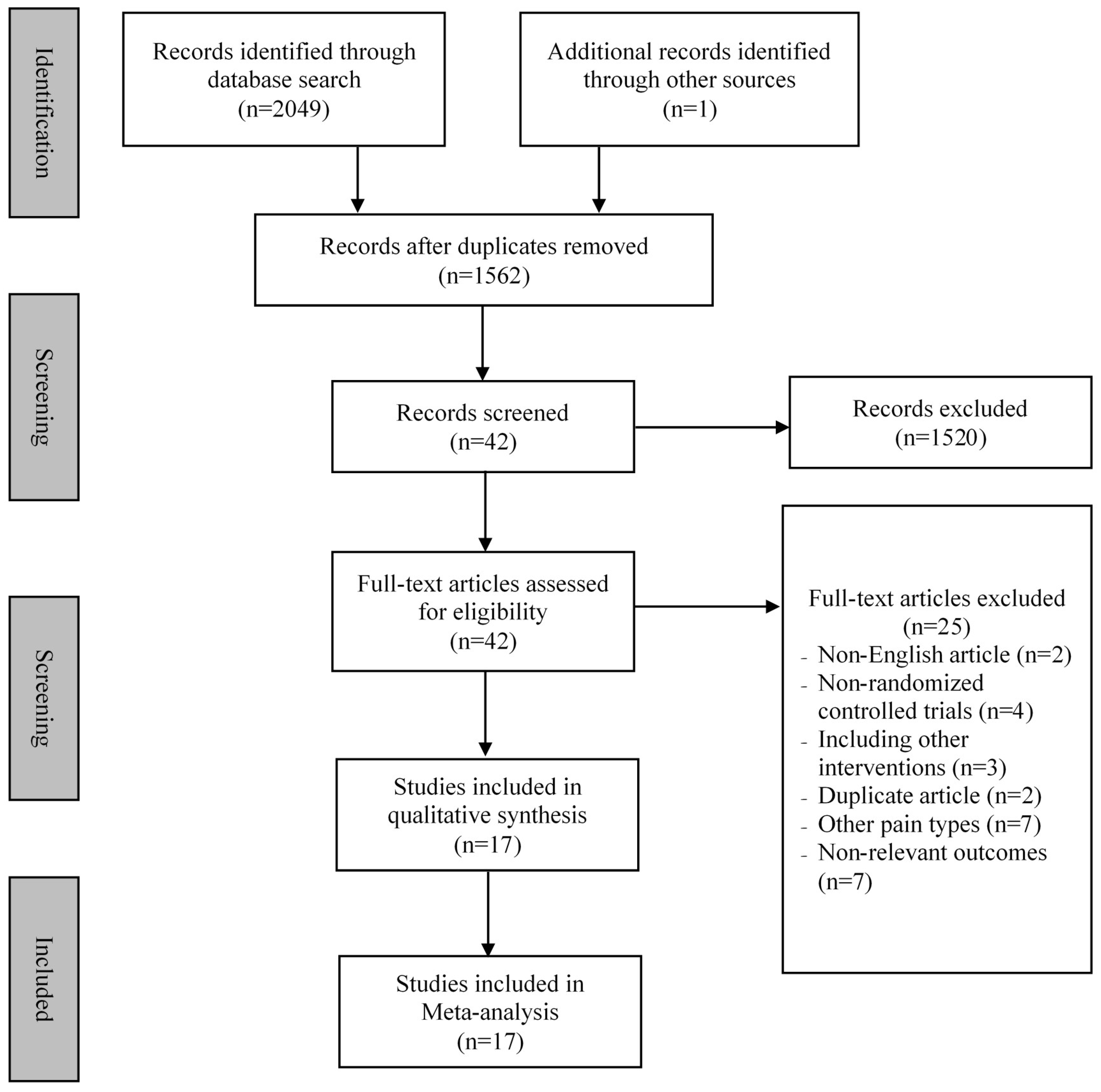
3.1. Search Results
3.2. Characteristics of Included Studies
3.3. Study Quality Assessment
3.4. Meta-Analysis of Outcome Measured
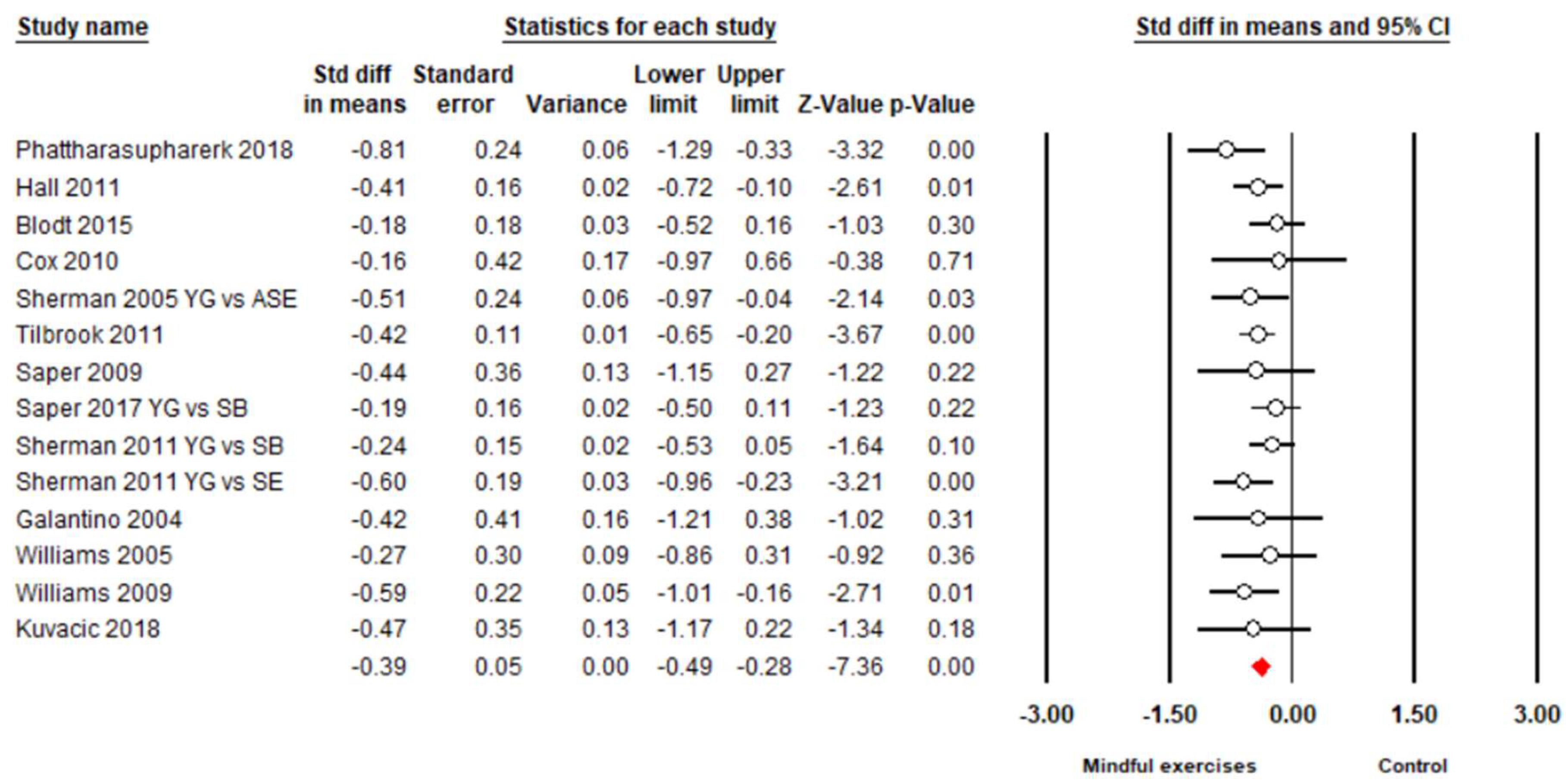
3.4.1. Pain Intensity
3.4.2. Back-Specific Disability
4. Discussion
4.1. Pain Intensity
4.2. Back-Specific Disability
4.3. Strengths and Limitations for Future Research
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Shmagel, A.; Foley, R.; Ibrahim, H. Epidemiology of chronic low back pain in US adults: Data from the 2009–2010 national health and nutrition examination survey. Arthritis Care Res. 2016, 68, 1688–1694. [Google Scholar] [CrossRef]
- Murray, C.J.; Atkinson, C.; Bhalla, K.; Birbeck, G.; Burstein, R. The state of US health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–608. [Google Scholar] [CrossRef]
- Taimela, S.; Kujala, U.M.; Salminen, J.J.; Viljanen, T. The prevalence of low back pain among children and adolescents: A nationwide, cohort-based questionnaire survey in Finland. Spine 1997, 22, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Balague, F.; Troussier, B.; Salminen, J.J. Non-specific low back pain in children and adolescents: Risk factors. Eur. Spine J. 1999, 8, 429–438. [Google Scholar] [CrossRef]
- Richard, G.; David, W. The Adult Spine: Principles and Practice-Second Edition. Neurosurgery 1997, 41, 1208–1209. [Google Scholar] [CrossRef]
- Enthoven, W.; Roelofs, P.; Deyo, R. Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst. Rev. 2016, 2, 012087. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, K.A.; Alsop, J.A.; Albertson, T.E. Tramadol exposures reported to statewide poison control system. Ann. Pharmacother. 2005, 39, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Shipton, E.A. Physical Therapy Approaches in the Treatment of Low Back Pain. Pain Ther. 2018, 7, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Burns, S.A.; Cleland, J.A.; Rivett, D.A.; Snodgrass, S.J. Effectiveness of physical therapy interventions for low back pain targeting the low back only or low back plus hips: A randomized controlled trial protocol. Braz. J. Phys. Ther. 2018, 22, 424–430. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; Cortés-Amador, S.; Espí-López, G.V. Effectiveness of classic physical therapy proposals for chronic non-specific low back pain: A literature review. Phys. Ther. Res. 2018, 21, 16–22. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef] [PubMed]
- Gordon, R.; Bloxham, S. A Systematic Review of the Effects of Exercise and Physical Activity on Non-Specific Chronic Low Back Pain. Healthcare 2016, 4, 22. [Google Scholar] [CrossRef]
- Miyamoto, G.C.; Lin, C.C.; Cabral, C.M.; Van-Dongen, J.M.; Van-Tulder, M.W. Costeffectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: A systematic review with meta-analysis. Br. J. Sports Med. 2019, 53, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Zhang, Y.; Kong, Z.; Loprinzi, P.D.; Hu, Y.; Ye, J.; Liu, S.; Yu, J.J.; Zou, L. The Effects of tai chi on markers of atherosclerosis, lower-limb physical function, and cognitive ability in adults aged over 60: A randomized controlled trial. Int. J. Environ. Res. Public Health 2019, 16, 753. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Zeng, N.; Huang, T.; Yeung, A.S.; Wei, G.X.; Liu, S.J.; Zhou, J.; Hu, R.; Hui, S.S. The Beneficial Effects of Mind-body Exercises for People with Mild Cognitive Impairment: A Systematic Review with Meta-Analysis. Arch. Phys. Med. Rehabil. 2019, in press. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.C. Effects of mind–body exercises (Tai Chi/Yoga) on heart rate variability parameters and perceived stress: A systematic review with meta-analysis of randomized controlled trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.; Chen, K.; Kinser, P.; Chan, J.; Ren, Z. Effects of meditative movements on major depressive disorder: A systematic Review and meta-analysis of randomized controlled trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Han, J.; Tsang, W.; Yeung, A. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review ad meta-analysis. Arch. Phys. Med. Rehabil. 2018, in press. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L.A. Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among post-stroke patients. Arch. Phys. Med. Rehabil. 2018, 9, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Chiou, S.; Zeng, N.; Tzeng, H. Effects of mind-body movement on balance function in stroke survivors: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 1292. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.; Wang, H. Effects of Mind-Body Exercises for Mood and Functional Capabilities in Post-Stroke Patients: An Analytical Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and Musculoskeletal Flexibility in Healthy Chinese Older Women. Sports 2017, 5, 52. [Google Scholar] [CrossRef]
- Zhang, Y.; Loprinzi, P.D.; Yang, L.; Liu, J.; Liu, S.; Zou, L. The Beneficial Effects of Traditional Chinese Exercises for Adults with Low Back Pain: A Meta-Analysis of Randomized Controlled Trials. Medicina 2019, 55, 118. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Albert, Y.; Quan, X.; Wang, H. A Systematic review and meta-analysis of mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; SasaKi, J.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid. Based Complement. Altern. Med. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Xiao, Z.; Wang, H.; Wang, C.; Hu, X.; Shu, Y. Asian martial arts for Children with Autism Spectrum Disorder: A Systematic Review. Arch. Budo 2017, 13, 79–92. [Google Scholar]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener. Dis. 2017, 2, 46–52. [Google Scholar]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The effect of Taichi practice on attenuating bone mineral density loss: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef]
- Zou, L.; Wang, H.; Li, T.; Lu, L. Effect of traditional Chinese mind-body exercise on disease activity, spinal mobility, and quality of life in patients with ankylosing spondylitis. Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Wang, C.; Yeung, A.; Liu, Y.; Pan, Z. A Review Study on the beneficial effects of baduanjin. J. Altern. Complement. Med. 2018, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X. Mindfulness-based baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Chen, X.; Wang, H. Baduanjin Exercise for Stroke Rehabilitation: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Theadom, A.; Cropley, M.; Smith, H.E.; Feigin, V.L.; Mcpherson, K. Mind and body therapy for fibromyalgia. Cocrane Database Syst. Rev. 2015, 9, CD001980. [Google Scholar] [CrossRef] [PubMed]
- Selfe, T.K.; Innes, K.E. Mind-body therapies and osteoarthritis of the knee. Curr. Rheumatol. Rev. 2009, 5, 204–211. [Google Scholar] [CrossRef]
- Holtzman, S.; Beggs, R.T. Yoga for chronic low back pain: A meta-analysis of randomized controlled trials. Pain Res. Manag. 2013, 18, 267–272. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Haller, H.; Dobos, G. A systematic review and meta-analysis of yoga for low back pain. Clin. J. Pain 2013, 29, 450–460. [Google Scholar] [CrossRef]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.; Benoliel, R.; Wang, S.J. Chronic pain as a symptom or a disease: The IASP classification of chronic pain for the international classification of disease (ICD-11). Pain 2019, 160, 19–27. [Google Scholar] [CrossRef]
- Maher, C.; Sherrington, C.; Herbert, R.; Moseley, A.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: New York, NY, USA, 2011; ISBN 9780470057964. [Google Scholar]
- Hall, A.M.; Maher, C.G.; Lam, P.; Ferreira, M.; Latimer, J. Tai chi exercise for treatment of pain and disability in people with persistent low back pain: A randomized controlled trial. Arthritis Care Res. 2011, 63, 1576–1583. [Google Scholar] [CrossRef] [Green Version]
- Blödt, S.; Pach, D.; Kaster, T.; Lüdtke, R.; Icke, K.; Reisshauer, A.; Witt, C.M. Qigong versus exercise therapy for chronic low back pain in adults—A randomized controlled non-inferiority trial. Eur. J. Pain (UK) 2015, 19, 123–131. [Google Scholar] [CrossRef]
- Teut, M.; Knilli, J.; Daus, D.; Roll, S.; Witt, C.M. Qigong or Yoga Versus No Intervention in Older Adults with Chronic Low Back Pain—A Randomized Controlled Trial. J. Pain 2016, 17, 796–805. [Google Scholar] [CrossRef]
- Phattharasupharerk, S.; Purepong, N.; Eksakulkla, S.; Siriphorn, A. Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial. J. Bodyw. Mov. Ther. 2018. [Google Scholar] [CrossRef]
- Liu, J.; Yeung, A.; Xiao, T.; Tian, X.; Kong, Z.; Zou, L.; Wang, X. Chen-Style Tai Chi for Individuals (Aged 50 Years Old or Above) with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 517. [Google Scholar] [CrossRef]
- Galantino, M.L.; Bzdewka, T.M.; Eissler-Russo, J.L.; Holbrook, M.L.; Mogck, E.P.; Geigle, P.; Farrar, J.T. The impact of modified hatha yoga on chronic low back pain: A pilot study. Altern. Ther. Health Med. 2004, 10, 56–59. [Google Scholar] [CrossRef]
- Sherman, K.J.; Cherkin, D.C.; Erro, J.; Miglioretti, D.L.; Deyo, R.A. Comparing yoga, exercise, and a self-care book for chronic low back pain: A randomized, controlled trial. Ann. Intern. Med. 2005, 143, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.A.; Petronis, J.; Smith, D.; Goodrich, D.; Wu, J.; Ravi, N.; Doyle, E.J.; Juckett, R.G.; Kolar, M.M.; Gross, R. Effect of Iyengar yoga therapy for chronic low back pain. Pain 2005, 115, 107–117. [Google Scholar] [CrossRef]
- Tekur, P.; Singphow, C.; Nagendra, H.R.; Raghuram, N. Effect of Short-Term Intensive Yoga Program on Pain, Functional Disability and Spinal Flexibility in Chronic Low Back Pain: A Randomized Control Study. J. Altern. Complement. Med. 2008, 14, 637–644. [Google Scholar] [CrossRef]
- Williams, K.; Ph, D.; Abildso, C.; Ph, D.; Steinberg, L.; Ph, D.; Doyle, E.; Epstein, B.; Pt, M.D.; Smith, D. Evaluation of the effectiveness and efficacy of Iyengar Yoga Therapy on Chronic Low Back Pain. Spine 2009, 34, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Sherman, K.J.; Cullum-Dugan, D.; Davis, R.B.; Phillips, R.S.; Culpepper, L. Yoga for chronic low back pain in a predominantly minority population: A pilot randomized controlled trial. Altern. Ther. Health Med. 2009, 15, 18–27. [Google Scholar] [CrossRef]
- Cox, H.; Torgerson, D.; Semlyen, A.; Tilbrook, H.; Watt, I.; Aplin, J.; Trewhela, A. A randomised controlled trial of yoga for the treatment of chronic low back pain: Results of a pilot study. Complement. Ther. Clin. Pract. 2010, 16, 187–193. [Google Scholar] [CrossRef]
- Tilbrook, H.E.; Cox, H.; Hewitt, C.E.; Kangombe, A.R.; Chuang, L.H.; Jayakody, S.; Aplin, J.D. Yoga for Chronic Low Back Pain. Ann. Intern. Med. 2011, 155, 569–578. [Google Scholar] [CrossRef]
- Sherman, K.J.; Cherkin, D.C.; Wellman, R.D.; Cook, A.J.; Hawkes, R.J.; Delaney, K.; Deyo, R.A. A randomized trial comparing yoga, stretching, and a self-care book for chronic low back pain. Arch. Intern. Med. 2011, 171, 2019–2026. [Google Scholar] [CrossRef] [PubMed]
- Nambi, G.S.; Inbasekaran, D.; Khuman, R.; Devi, S. Changes in pain intensity and health related quality of life with Iyengar yoga in nonspecific chronic low back pain: A randomized controlled study. Int. J. Yoga 2014, 7, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Lemaster, C.; Delitto, A.; Sherman, K.J.; Herman, P.M.; Sadikova, E.; Stevans, J.; Keosaian, J.E.; Cerrada, C.J.; Femia, A.L. Yoga, Physical Therapy, or Education for Chronic Low Back Pain. Ann. Intern. Med. 2017, 167, 85. [Google Scholar] [CrossRef] [PubMed]
- Kuvačić, G.; Fratini, P.; Padulo, J.; Antonio, D.I.; De Giorgio, A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: A randomized controlled trial. Complement. Ther. Clin. Pract. 2018, 31, 262–267. [Google Scholar] [CrossRef]
- Hall, A.M.; Kamper, S.J.; Emsley, R.; Maher, C.G. Does pain-catestrophising mediate the effects of tai Chi on treatment outcomes ofr people with low back pain? Complement. Ther. Med. 2016, 25, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Enghauser, R. Motor learning and the dance technique class: Science, tradition and pedagogy. J. Dance Educ. 2003, 3, 87–95. [Google Scholar] [CrossRef]
- Wayne, P.M.; Berkowitz, D.L.; Litrownik, D.E.; Buring, J.E.; Yeh, G.Y. What do we really know about the safety of tai chi? A systematic review of adverse event reports in randomized trials. Arch. Phys. Med. Rehabil. 2014, 95, 2470–2483. [Google Scholar] [CrossRef]
- Zou, L.; Zhang, Y.; Liu, Y.; Tian, X.; Xiao, T.; Liu, X.; Yeung, A.S.; Liu, J.; Wang, X. The effects of tai chi chuan versus core stability training on lower-limb neuromuscular function in aging individuals with non-specific chronic lower back pain. Medicina 2019, 55, 60. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Tao, J.; Liu, W.; Huang, J.; Xue, X.; Li, M.; Yang, M.; Zhu, J.; Lang, C.; Park, J.; et al. Different modulation effects of tai chi chuan and baduanjin on resting state functional connectivity of the default mode network in older adults. Soc. Cogn. Affect. Neurosci. 2019, 14, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Chen, X.; Liu, J.; Egorova, N.; Xue, X.; Liu, W.; Zheng, G.; Li, M.; Wu, J.; Hu, K.; et al. Tai Chi Chuan and Baduanjin mind-body training changes resting-state low-frequency fluctuations in the frontal lobe of older adults: A resting-state fmri study. Front. Hum. Neurosci. 2017, 11, 514. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Intervention Protocol | Outcome Measured | Safety | ||||
|---|---|---|---|---|---|---|---|---|
| Sample Size | MA (years) | Mindful Exercise (Qualified Instructor) | Control | DR (wk) | Control Type | Pain and Disability | Adverse Events | |
| Hall et al., (2011) [41] | 160 CLBP TC = 80; C = 80 | 44 | 2 × 40 min/wk, TC | Wait-list | 10 | Passive | Pain intensity (NRS), disability (RMDQ) | No adverse event |
| Blödt et al., (2015) [42] | 127 CLBP QG = 64; C = 63 | 47 | 1 × 90 min/wk, QG | 1 × 60 min/wk Strengthening | 12 | Active | Pain intensity (VAS), disability (RMDQ) | No adverse event |
| Teut et al., (2016) [43] | 176 CLBP QG = 58; YG = 61 C = 57 | 73 | 1 × 90 min/wk, QG; 2 × 45 min/wk, YG | Waitlist | 12 | Passive | Pain intensity (VAS) | No adverse event |
| Phattharasupharerk et al., (2018) [44] | 72 CLBP QG = 36; C = 36 | 35 | 1 × 60 min/wk plus daily practice, YG | Waitlist | 6 | Passive | Pain intensity (VAS), disability (RMDQ) | No adverse event |
| Liu et al., (2019) [45] | 43 CLBP TC = 15; C1 = 15; C2 = 13 | 74 | 3 × 60 min/wk, TC | C1: Core training C2: No intervention | 12 | C1: Active C2: Passive | Pain intensity (VAS) | No adverse event |
| Galantino et al., (2004) [46] | 22 CLBP YG = 11; C = 11 | 30–65 | 2 × 60 min/wk plus 7 × 60 min/wk (home), YG | No treatment | 6 | Passive | disability (ODI) Depression (BDI) | No adverse event |
| Sherman et al., (2005) [47] | 101 CLBP YG = 36; C1 = 35; C2 = 30 | 44 | 1 × 75 min/wk plus daily practice (home), YG | C1: 1 × 75min/wk + Daily practice, aerobic exercises and strength exercise C2: Self-care book | 12 | C1: Active C2: Passive | disability (RMDQ) | No adverse event |
| Williams et al., (2005) [48] | 60 CLBP YG = 30; C = 30 | 48 | 1 × 90 min/wk plus 5 × 30 min/wk (home), YG | Newsletters on back pain | 16 | Passive | Pain intensity (VAS), disability (ODI) | 1 participant diagnosed with a herniated disc in YG |
| Tekur et al., (2008) [49] | 80 CLBP YG = 40; C = 40 | 48 | 7 × 120 min/wk, YG | Daily physical movements + education | 1 | Active | disability (ODI) | No adverse event |
| Williams et al., (2009) [50] | 90 CLBP YG = 43; C = 47 | 48 | 2 × 90 min/wk plus 7 × 30 min/wk (home), YG | Waitlist | 24 | Passive | Pain intensity (VAS), disability (ODI) | No adverse event |
| Saper et al., (2009) [51] | 30 CLBP YG = 15; C = 15 | 44 | 1 × 75 min/wk plus 7 × 30 min/wk (home), YG | Self-care book | 12 | Passive | Pain intensity (VAS), disability (RMDQ) | No adverse event |
| Cox et al., (2010) [52] | 20 CLBP YG = 10; C = 10 | 45 | 1 × 75 min/wk plus home practice, YG | Self-care book | 12 | Passive | Pain intensity (ABPS), disability (RMDQ) | No adverse event |
| Tilbrook et al., (2011) [53] | 313 CLBP YG = 156; C = 157 | 46 | 1 × 75min/wk plus 7 × 30 min/wk (home), YG | Self-care book | 12 | Passive | Pain intensity (ABPS), disability (RMDQ) | 8 participants (increased pain) in YG |
| Sherman et al., (2011) [54] | 228 CLBP YG = 92; C1 = 9 1; C2 = 45 | 48 | 1 × 75 min/wk plus 6 × 20 min/wk (home),YG | C1: 1 × 75min/wk + 20 min/wk (home) Stretching exercise C2: Self-care book | 12 | C1: Active C2: Passive | Pain intensity (NRS) disability (RMDQ) | 13 participants (increased pain) and 1 herniated disc in yoga |
| Nambi et al., (2014) [55] | 60 CLBP YG = 30; C = 30 | 44 | 1 × 60 min/wk plus 5 × 30 min/wk (home), YG | 35days/wk, Exercise (strengthening and stretching) | 4 | Active | Pain intensity (VAS) | 1 herniated disc in YG |
| Saper et al., (2017) [56] | 320 CLBP YG = 127; C1 = 129; C2 = 64 | 46 | 1 × 75 min/wk plus 7 × 30 min/wk (home), YG | C1: 1 x 60min/wk, PT (stabilization and aerobic exercise) C2: Self-care book | 12 | C1: Active C2: Passive | Pain intensity (NRS) disability (RMDQ) | 9 and 14 participants (mild self-limited joint and back pain) in YG and PT, respectively |
| Kuvačić et al., (2018) [57] | 30 CLBP YG = 15; C = 15 | 34 | 2 × 75 min/wk, YG | Pamphlet program | 8 | Passive | Pain intensity (NRS), disability (ODI), depression (SDS) | Not reported |
| Study | Score | Methodological Quality | PEDro Item Number | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Hall et al., 2011 [41] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Blödt et al., 2015 [42] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Teut et al., 2016 [43] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Phattharasupharerk et al., 2018 [44] | 7 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||||
| Liu et al., 2019 [45] | 7 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||||
| Galantino et al., 2004 [46] | 7 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||||
| Sherman et al., 2005 [47] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Williams et al., 2005 [48] | 6 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| Tekur et al., 2008 [49] | 7 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||||
| Williams et al., 2009 [50] | 6 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| Saper et al., 2009 [51] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Cox et al., 2010 [52] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Tilbrook et al., 2011 [53] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Sherman et al., 2011 [54] | 8 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||
| Nambi et al., 2014 [55] | 6 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | |||||
| Saper et al., 2017 [56] | 9 | Excellent | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||
| Kuvačić et al., 2018 [57] | 7 | Good | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ||||
| Studies were classified as having excellent (9–10), good (6–8), fair (4–5) or poor (<4) | |||||||||||||
| Categorical Moderator | Outcome | Covariates | No. of Studies/Comparisons | SMD | 95% Confidence Interval | I2% | Test for Between-Group Hoterogeneity | ||
|---|---|---|---|---|---|---|---|---|---|
| Q-Value | df(Q) | p-Value | |||||||
| Control Type | Pain intensity | Active | 7 | −0.40 | -0.48 to -0.20 | 53.2 % | 0.08 | 1 | 0.78 |
| Passive | 7 | -0.35 | −0.46 to −0.21 | 46.5% | |||||
| Disability | Active | 4 | −0.28 | −0.47 to −0.09 | 0% | 1.62 | 1 | 0.20 | |
| Passive | 10 | −0.43 | −0.55 to −0.31 | 0% | |||||
| Mindful Type | Pain intensity | Yoga | 10 | −0.33 | −0.47 to −0.19 | 33.7% | 8.46 | 2 | 0.01* |
| TC | 2 | −0.75 | −1.05 to −0.46 | 0% | |||||
| Qigong | 2 | −0.21 | −0.48 to 0.06 | 10.0% | |||||
| Disability | Yoga | 11 | −0.38 | −0.50 to −0.26 | 0% | 0.16 | 2 | 0.92 | |
| TC | 1 | −0.41 | −0.72 to −0.10 | 0% | |||||
| Qigong | 2 | −0.47 | −1.09 to 0.14 | 77.2% | |||||
| Instruments | Pain intensity | ABPS | 2 | −0.21 | −0.42 to 0.01 | 0% | 2.1 | 2 | 0.35 |
| VAS | 7 | −0.43 | −0.68 to −0.18 | 50.5% | |||||
| NRS | 5 | −0.38 | −0.59 to −0.17 | 60.1% | |||||
| Disability | RMDQ | 10 | −0.38 | −0.49 to −0.27 | 0% | 0.36 | 1 | 0.55 | |
| ODI | 4 | −0.47 | −0.76 to −0.18 | 0% | |||||
| Allocation Concealment | Pain intensity | Yes | 11 | −0.33 | −0.46 to −0.19 | 39.5% | 1.19 | 1 | 0.28 |
| No | 3 | −0.59 | 1.05 to −0.13 | 50.9% | |||||
| Disability | Yes | 9 | −0.35 | −0.46 to −0.24 | 0% | 2.27 | 1 | 0.13 | |
| No | 5 | −0.56 | −0.80 to −0.31 | 0% | |||||
| Continuous moderator | Outcome | No. of studies/comparisons | β | 95% Confidence Interval | Q-value | df(Q) | p-value | ||
| Age | Pain intensity | 14 | −0.00108 | −0.01080 to 0.00865 | 0.05 | 1 | 0.83 | ||
| Disability | 14 | 0.02454 | −0.00706 to 0.05614 | 2.32 | 1 | 0.13 | |||
| Total Time | Pain intensity | 14 | 0.00002 | −0.00007 to 0.00012 | 0.22 | 1 | 0.64 | ||
| Disability | 14 | −0.00002 | −0.00012 to 0.00009 | 0.10 | 1 | 0.75 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Zhang, Y.; Yang, L.; Loprinzi, P.D.; Yeung, A.S.; Kong, J.; Chen, K.W.; Song, W.; Xiao, T.; Li, H. Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 628. https://doi.org/10.3390/jcm8050628
Zou L, Zhang Y, Yang L, Loprinzi PD, Yeung AS, Kong J, Chen KW, Song W, Xiao T, Li H. Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2019; 8(5):628. https://doi.org/10.3390/jcm8050628
Chicago/Turabian StyleZou, Liye, Yanjie Zhang, Lin Yang, Paul D. Loprinzi, Albert S. Yeung, Jian Kong, Kevin W Chen, Wook Song, Tao Xiao, and Hong Li. 2019. "Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 8, no. 5: 628. https://doi.org/10.3390/jcm8050628