New Cardiovascular Biomarkers in Ischemic Heart Disease—GDF-15, A Probable Predictor for Ejection Fraction

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Subjects and Patient Population
2.2. Echocardiographic Analysis
2.3. Laboratory Analysis
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
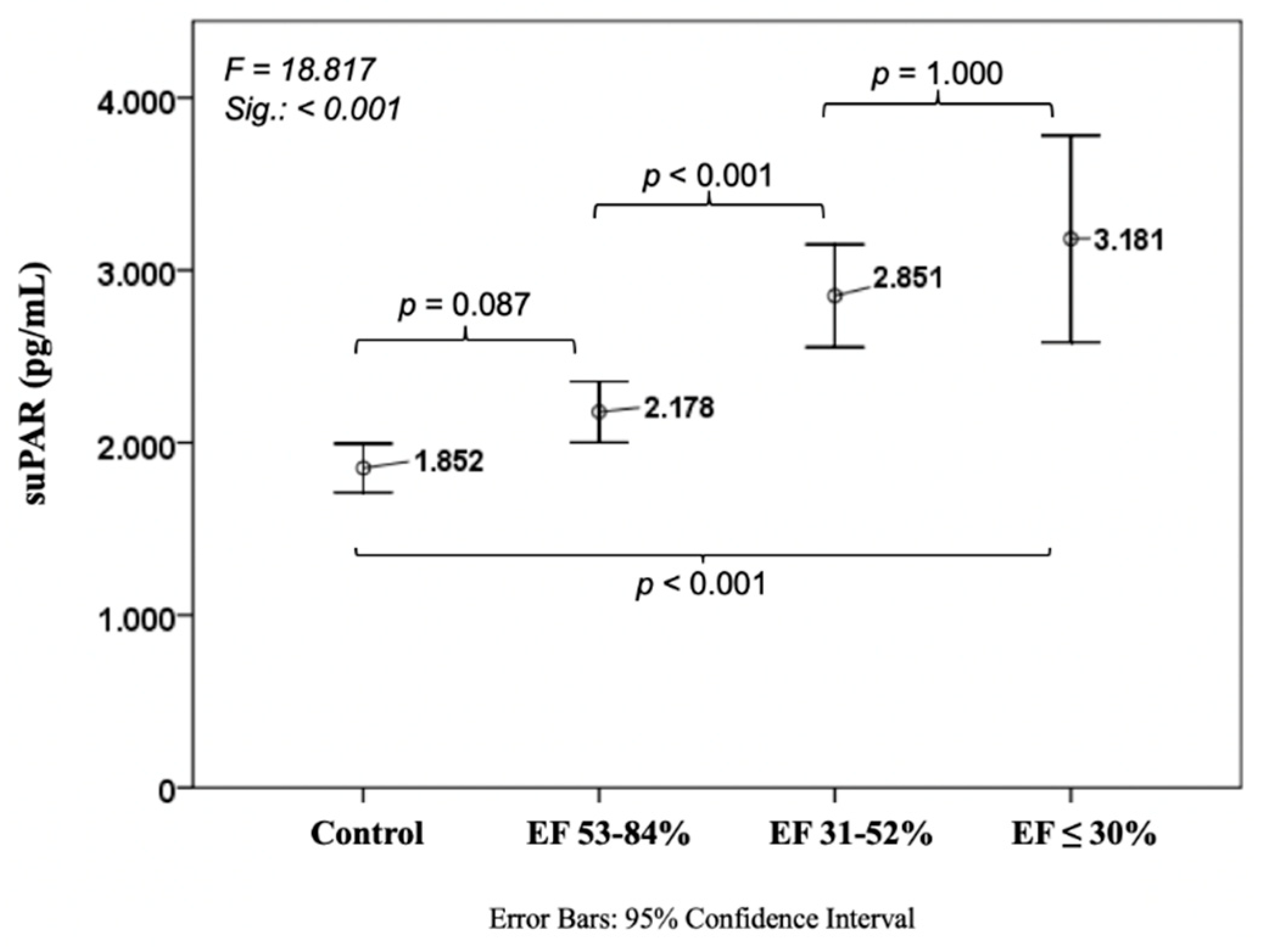
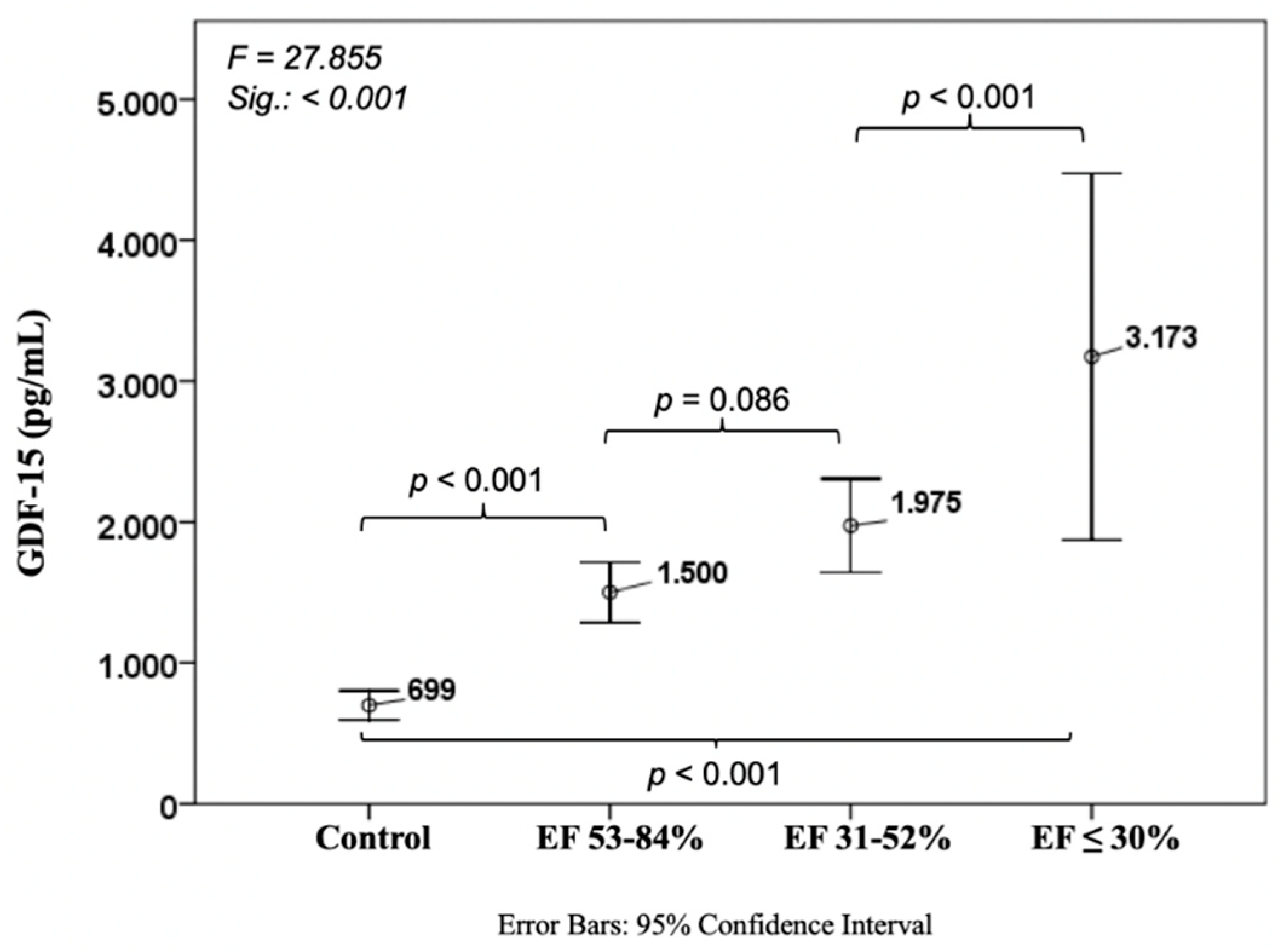
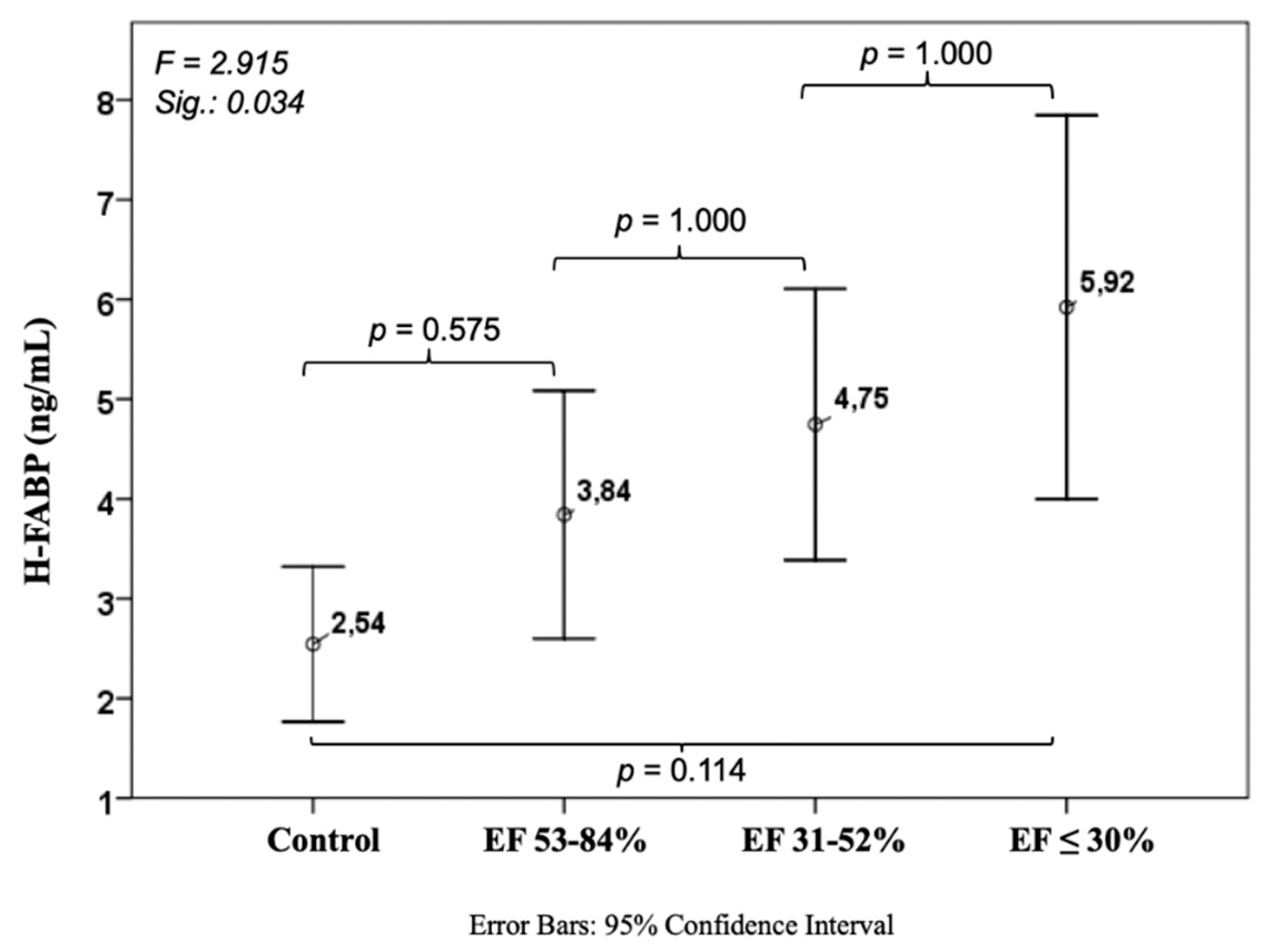
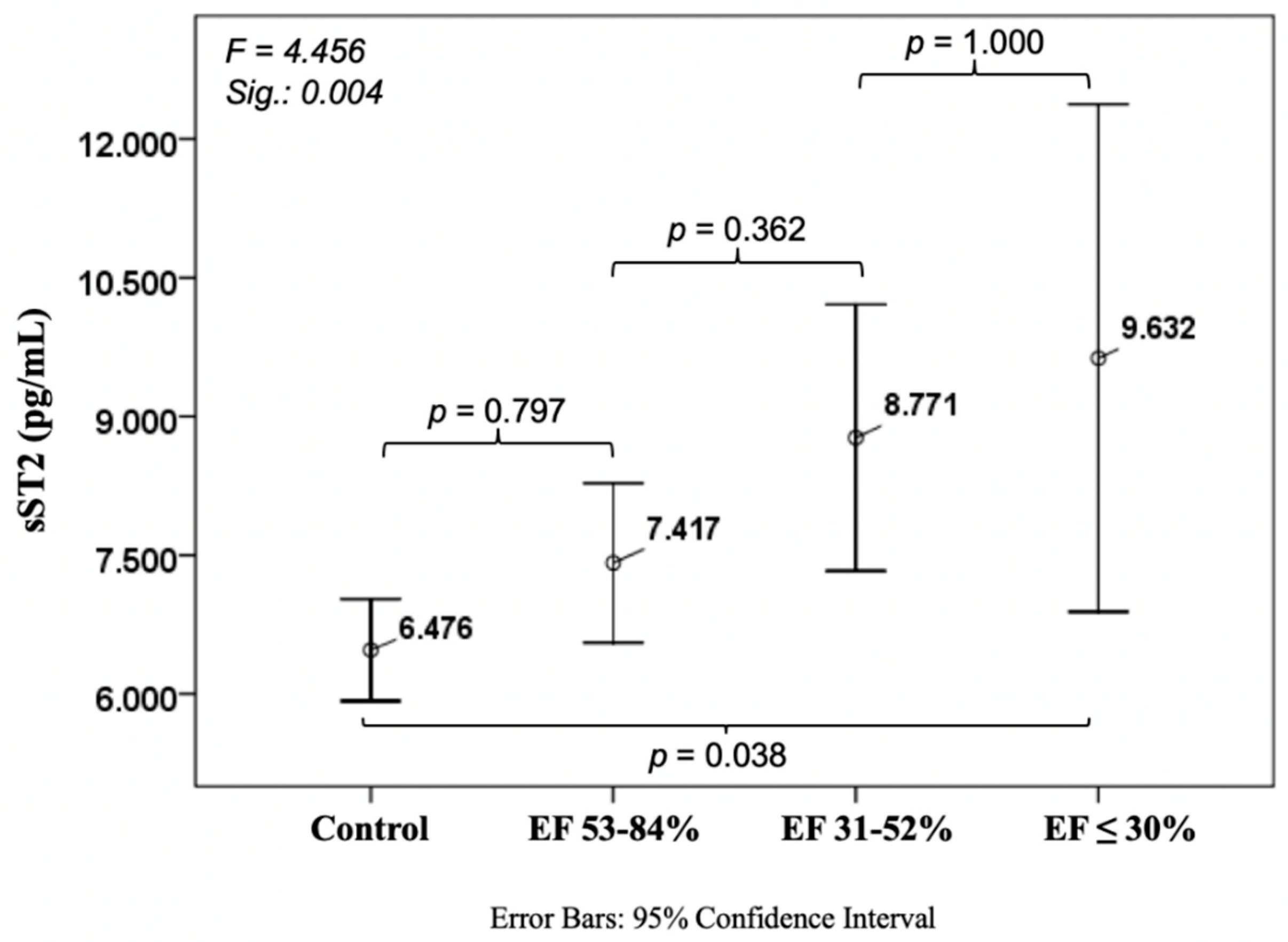
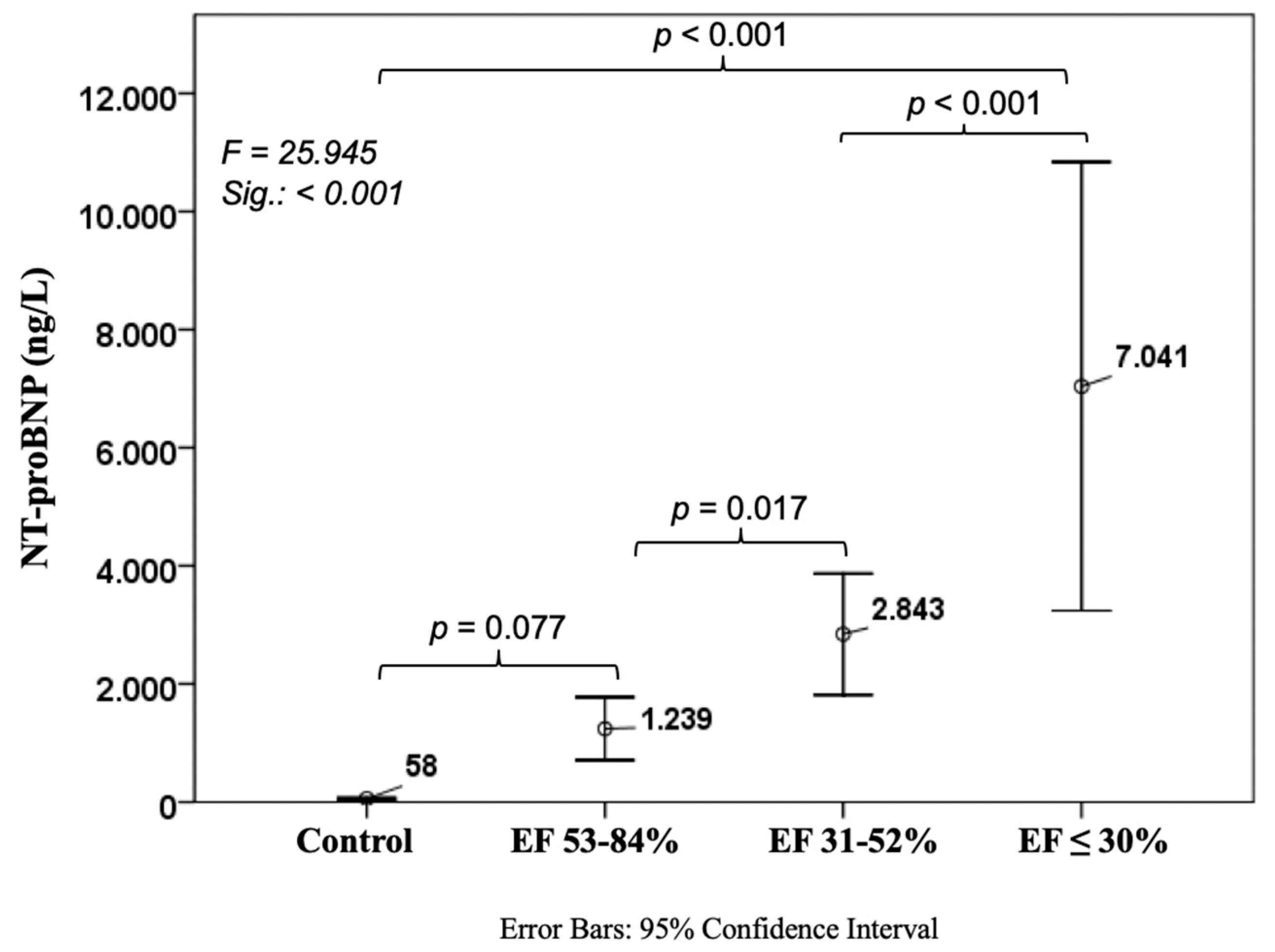
3.2. Biomarkers
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sorensen, M.H.; Gerke, O.; Eugen-Olsen, J.; Munkholm, H.; Lambrechtsen, J.; Sand, N.P.; Mickley, H.; Rasmussen, L.M.; Olsen, M.H.; Diederichsen, A. Soluble urokinase plasminogen activator receptor is in contrast to high-sensitive C-reactive-protein associated with coronary artery calcifications in healthy middle-aged subjects. Atherosclerosis 2014, 237, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Lyngbaek, S.; Marott, J.L.; Sehestedt, T.; Hansen, T.W.; Olsen, M.H.; Andersen, O.; Linneberg, A.; Haugaard, S.B.; Eugen-Olsen, J.; Hansen, P.R.; et al. Cardiovascular risk prediction in the general population with use of suPAR, CRP, and Framingham Risk Score. Int. J. Cardiol. 2013, 167, 2904–2911. [Google Scholar] [CrossRef] [PubMed]
- Borne, Y.; Persson, M.; Melander, O.; Smith, J.G.; Engstrom, G. Increased plasma level of soluble urokinase plasminogen activator receptor is associated with incidence of heart failure but not atrial fibrillation. Eur. J. Heart Fail. 2014, 16, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bootcov, M.R.; Bauskin, A.R.; Valenzuela, S.M.; Moore, A.G.; Bansal, M.; He, X.Y.; Zhang, H.P.; Donnellan, M.; Mahler, S.; Pryor, K.; et al. MIC-1, a novel macrophage inhibitory cytokine, is a divergent member of the TGF-beta superfamily. Proc. Natl. Acad. Sci. USA 1997, 94, 11514–11519. [Google Scholar] [CrossRef] [PubMed]
- Kempf, T.; Eden, M.; Strelau, J.; Naguib, M.; Willenbockel, C.; Tongers, J.; Heineke, J.; Kotlarz, D.; Xu, J.; Molkentin, J.D.; et al. The transforming growth factor-beta superfamily member growth-differentiation factor-15 protects the heart from ischemia/reperfusion injury. Circ. Res. 2006, 98, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Wollert, K.C.; Kempf, T.; Wallentin, L. Growth differentiation factor 15 as a biomarker in cardiovascular disease. Clin. Chem. 2017, 63, 140–151. [Google Scholar] [CrossRef]
- Kempf, T.; von Haehling, S.; Peter, T.; Allhoff, T.; Cicoira, M.; Doehner, W.; Ponikowski, P.; Filippatos, G.S.; Rozentryt, P.; Drexler, H.; et al. Prognostic utility of growth differentiation factor-15 in patients with chronic heart failure. J. Am. Coll. Cardiol. 2007, 50, 1054–1060. [Google Scholar] [CrossRef]
- Zschiesche, W.; Kleine, A.H.; Spitzer, E.; Veerkamp, J.H.; Glatz, J.F. Histochemical localization of heart-type fatty-acid binding protein in human and murine tissues. Histochem. Cell Biol. 1995, 103, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Bathia, D.P.; Carless, D.R.; Viswanathan, K.; Hall, A.S.; Barth, J.H. Serum 99th centile values for two heart-type fatty acid binding protein assays. Ann. Clin. Biochem. 2009, 46, 464–467. [Google Scholar] [CrossRef] [Green Version]
- Martin, N.T.; Martin, M.U. Interleukin 33 is a guardian of barriers and a local alarmin. Nat. Immunol. 2016, 17, 122–131. [Google Scholar] [CrossRef]
- Lassus, J.; Gayat, E.; Mueller, C.; Peacock, W.F.; Spinar, J.; Harjola, V.P.; van Kimmenade, R.; Pathak, A.; Mueller, T.; Disomma, S.; et al. Incremental value of biomarkers to clinical variables for mortality prediction in acutely decompensated heart failure: The Multinational Observational Cohort on Acute Heart Failure (MOCA) study. Int. J. Cardiol. 2013, 168, 2186–2194. [Google Scholar] [CrossRef] [PubMed]
- Kohli, P.; Bonaca, M.P.; Kakkar, R.; Kudinova, A.Y.; Scirica, B.M.; Sabatine, M.S.; Murphy, S.A.; Braunwald, E.; Lee, R.T.; Morrow, D.A. Role of ST2 in non-ST-elevation acute coronary syndrome in the MERLIN-TIMI 36 trial. Clin. Chem. 2012, 58, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Anand, I.S.; Rector, T.S.; Kuskowski, M.; Snider, J.; Cohn, J.N. Prognostic value of soluble ST2 in the Valsartan Heart Failure Trial. Circ. Heart Fail. 2014, 7, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Dieplinger, B.; Januzzi, J.L., Jr.; Steinmair, M.; Gabriel, C.; Poelz, W.; Haltmayer, M.; Mueller, T. Analytical and clinical evaluation of a novel high-sensitivity assay for measurement of soluble ST2 in human plasma—The presage ST2 assay. Clin. Chim. Acta 2009, 409, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.E.; Lyass, A.; Courchesne, P.; Chen, G.; Liu, C.; Yin, X.; Hwang, S.J.; Massaro, J.M.; Larson, M.G.; Levy, D. Protein biomarkers of cardiovascular disease and mortality in the community. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Kazimierczyk, E.; Kazimierczyk, R.; Harasim-Symbor, E.; Kaminski, K.; Sobkowicz, B.; Chabowski, A.; Tycinska, A. Persistently elevated plasma heart-type fatty acid binding protein concentration is related with poor outcome in acute decompensated heart failure patients. Clin. Chim. Acta 2018, 487, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Koller, L.; Stojkovic, S.; Richter, B.; Sulzgruber, P.; Potolidis, C.; Liebhart, F.; Mortl, D.; Berger, R.; Goliasch, G.; Wojta, J.; et al. Soluble urokinase-type plasminogen activator receptor improves risk prediction in patients with chronic heart failure. JACC Heart Fail. 2017, 5, 268–277. [Google Scholar] [CrossRef]
- Li, J.; Cui, Y.; Huang, A.; Li, Q.; Jia, W.; Liu, K.; Qi, X. Additional diagnostic value of growth differentiation factor-15 (GDF-15) to N-Terminal B-type natriuretic peptide (NT-proBNP) in patients with different stages of heart failure. Med. Sci. Monit. 2018, 24, 4992–4999. [Google Scholar] [CrossRef]
- Vorovich, E.; French, B.; Ky, B.; Goldberg, L.; Fang, J.C.; Sweitzer, N.K.; Cappola, T.P. Biomarker predictors of cardiac hospitalization in chronic heart failure: A recurrent event analysis. J. Card. Fail. 2014, 20, 569–576. [Google Scholar] [CrossRef]
- Weinberg, E.O.; Shimpo, M.; Hurwitz, S.; Tominaga, S.; Rouleau, J.L.; Lee, R.T. Identification of serum soluble ST2 receptor as a novel heart failure biomarker. Circulation 2003, 107, 721–726. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging. 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, K.; Hall, A.S.; Barth, J.H. An evidence-based approach to the assessment of heart-type Fatty Acid binding protein in acute coronary syndrome. Clin. Biochem. Rev. 2012, 33, 3–11. [Google Scholar] [PubMed]
- Lippi, G.; Schena, F.; Montagnana, M.; Salvagno, G.L.; Guidi, G.C. Influence of acute physical exercise on emerging muscular biomarkers. Clin. Chem. Lab. Med. 2008, 46, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Sponder, M.; Lichtenauer, M.; Wernly, B.; Paar, V.; Hoppe, U.; Emich, M.; Fritzer-Szekeres, M.; Litschauer, B.; Strametz-Juranek, J. Serum heart-type fatty acid-binding protein decreases and soluble isoform of suppression of tumorigenicity 2 increases significantly by long-term physical activity. J. Investig. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Shirazi, L.F.; Bissett, J.; Romeo, F.; Mehta, J.L. Role of inflammation in heart failure. Curr. Atheroscler. Rep. 2017, 19, 27. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.J.; Ladelund, S.; Haupt, T.H.; Ellekilde, G.; Poulsen, J.H.; Iversen, K.; Eugen-Olsen, J.; Andersen, O. Soluble urokinase plasminogen activator receptor (suPAR) in acute care: A strong marker of disease presence and severity, readmission and mortality. A retrospective cohort study. Emerg. Med. J. 2016, 33, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Filipovic, Z.; Brown, D.; Breit, S.N.; Vassilev, L.T. Macrophage inhibitory cytokine-1: A novel biomarker for p53 pathway activation. Mol. Cancer Ther. 2003, 2, 1023–1029. [Google Scholar]
- Vousden, K.H.; Lane, D.P. p53 in health and disease. Nat. Rev. Mol. Cell Biol. 2007, 8, 275–283. [Google Scholar] [CrossRef]
- Li, J.; Yang, L.; Qin, W.; Zhang, G.; Yuan, J.; Wang, F. Adaptive induction of growth differentiation factor 15 attenuates endothelial cell apoptosis in response to high glucose stimulus. PLoS ONE 2013, 8, e65549. [Google Scholar] [CrossRef]
- Schillaci, G.; Verdecchia, P.; Porcellati, C.; Cuccurullo, O.; Cosco, C.; Perticone, F. Continuous relation between left ventricular mass and cardiovascular risk in essential hypertension. Hypertension 2000, 35, 580–586. [Google Scholar] [CrossRef]
- Xu, X.Y.; Nie, Y.; Wang, F.F.; Bai, Y.; Lv, Z.Z.; Zhang, Y.Y.; Li, Z.J.; Gao, W. Growth differentiation factor (GDF)-15 blocks norepinephrine-induced myocardial hypertrophy via a novel pathway involving inhibition of epidermal growth factor receptor transactivation. J. Biol. Chem. 2014, 289, 10084–10094. [Google Scholar] [CrossRef] [PubMed]
- Ding, Q.; Mracek, T.; Gonzalez-Muniesa, P.; Kos, K.; Wilding, J.; Trayhurn, P.; Bing, C. Identification of macrophage inhibitory cytokine-1 in adipose tissue and its secretion as an adipokine by human adipocytes. Endocrinology 2009, 150, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Schlittenhardt, D.; Schober, A.; Strelau, J.; Bonaterra, G.A.; Schmiedt, W.; Unsicker, K.; Metz, J.; Kinscherf, R. Involvement of growth differentiation factor-15/macrophage inhibitory cytokine-1 (GDF-15/MIC-1) in oxLDL-induced apoptosis of human macrophages in vitro and in arteriosclerotic lesions. Cell Tissue Res. 2004, 318, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Lok, S.I.; Winkens, B.; Goldschmeding, R.; van Geffen, A.J.; Nous, F.M.; van Kuik, J.; van der Weide, P.; Klopping, C.; Kirkels, J.H.; Lahpor, J.R.; et al. Circulating growth differentiation factor-15 correlates with myocardial fibrosis in patients with non-ischaemic dilated cardiomyopathy and decreases rapidly after left ventricular assist device support. Eur. J. Heart Fail. 2012, 14, 1249–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kempf, T.; Sinning, J.M.; Quint, A.; Bickel, C.; Sinning, C.; Wild, P.S.; Schnabel, R.; Lubos, E.; Rupprecht, H.J.; Munzel, T.; et al. Growth-differentiation factor-15 for risk stratification in patients with stable and unstable coronary heart disease: Results from the AtheroGene study. Circ. Cardiovasc. Genet. 2009, 2, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Schopfer, D.W.; Ku, I.A.; Regan, M.; Whooley, M.A. Growth differentiation factor 15 and cardiovascular events in patients with stable ischemic heart disease (The Heart and Soul Study). Am. Heart J. 2014, 167, 186–192. [Google Scholar] [CrossRef]
- Bonaca, M.P.; Morrow, D.A.; Braunwald, E.; Cannon, C.P.; Jiang, S.; Breher, S.; Sabatine, M.S.; Kempf, T.; Wallentin, L.; Wollert, K.C. Growth differentiation factor-15 and risk of recurrent events in patients stabilized after acute coronary syndrome: Observations from PROVE IT-TIMI 22. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Eggers, K.M.; Kempf, T.; Lagerqvist, B.; Lindahl, B.; Olofsson, S.; Jantzen, F.; Peter, T.; Allhoff, T.; Siegbahn, A.; Venge, P.; et al. Growth-differentiation factor-15 for long-term risk prediction in patients stabilized after an episode of non-ST-segment-elevation acute coronary syndrome. Circ. Cardiovasc. Genet. 2010, 3, 88–96. [Google Scholar] [CrossRef]
- Anand, I.S.; Kempf, T.; Rector, T.S.; Tapken, H.; Allhoff, T.; Jantzen, F.; Kuskowski, M.; Cohn, J.N.; Drexler, H.; Wollert, K.C. Serial measurement of growth-differentiation factor-15 in heart failure: Relation to disease severity and prognosis in the Valsartan Heart Failure Trial. Circulation 2010, 122, 1387–1395. [Google Scholar] [CrossRef]
- Chan, M.M.; Santhanakrishnan, R.; Chong, J.P.; Chen, Z.; Tai, B.C.; Liew, O.W.; Ng, T.P.; Ling, L.H.; Sim, D.; Leong, K.T.; et al. Growth differentiation factor 15 in heart failure with preserved vs. reduced ejection fraction. Eur. J. Heart Fail. 2016, 18, 81–88. [Google Scholar] [CrossRef]
- Paulus, W.J.; Tschope, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll. Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, T.; Wang, T.; O’Brien, E.C.; Samsky, M.D.; Pura, J.A.; Lokhnygina, Y.; Rogers, J.G.; Hernandez, A.F.; Craig, D.; Bowles, D.E.; et al. Effects of left ventricular assist device support on biomarkers of cardiovascular stress, fibrosis, fluid homeostasis, inflammation, and renal injury. JACC Heart Fail. 2015, 3, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jiang, T.; Jiang, M.; Gu, S. Appraising growth differentiation factor 15 as a promising biomarker in digestive system tumors: A meta-analysis. BMC Cancer 2019, 19, 177. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.A.; Wu, S.; Juang, J.J.; Chiang, F.T.; Teng, M.S.; Lin, J.F.; Huang, H.L.; Ko, Y.L. Growth differentiation factor 15 may predict mortality of peripheral and coronary artery diseases and correlate with their risk factors. Mediators Inflamm. 2017, 2017, 9398401. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 112) | EF 53–84% (n = 155) | EF 31–52% (n = 71) | EF ≤ 30% (n = 23) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | 51.3 ± 9.0 | 62.1 ± 10.9 | 65.2 ± 10.1 | 66.6 ± 8.2 | <0.001 |
| Female sex (%) | 44.6 | 29.0 | 29.6 | 13.0 | 0.006 |
| Hypertension (%) | 38.4 | 92.9 | 93.0 | 95.7 | <0.001 |
| Family history of CAD (%) | 42.0 | 59.4 | 56.3 | 52.2 | 0.040 |
| Diabetes (%) | 5.4 | 21.9 | 25.2 | 34.8 | <0.001 |
| Dyslipidemia (%) | 34.8 | 92.3 | 91.5 | 73.9 | <0.001 |
| BMI (kg/m2) | 27.4 ± 4.2 | 27.8 ± 4.8 | 28.6 ± 5.7 | 29.5 ± 6.4 | 0.226 |
| SBP (mmHg) | 138 ± 16 | 131 ± 16 | 128 ± 16 | 129 ± 19 | 0.004 |
| DBP (mmHg) | 84 ± 12 | 76 ± 10 | 74 ± 10 | 79 ± 17 | <0.001 |
| HR (bpm) | 67 ± 9 | 68 ± 12 | 71 ± 15 | 77 ± 13 | 0.003 |
| Cholesterol (mg/dL) | 200 ± 40 | 180 ± 52 | 164 ± 41 | 163 ± 56 | <0.001 |
| Triglycerides (mg/dL) | 129 ± 78 | 153 ± 88 | 149 ± 83 | 148 ± 72 | 0.605 |
| LDL (mg/dL) | 117 ± 35 | 107 ± 40 | 94 ± 41 | 96 ± 35 | 0.495 |
| HDL (mg/dL) | 58 ± 18 | 48 ± 14 | 43 ± 12 | 37 ± 10 | 0.005 |
| Creatinine (mg/dL) | 0.9 ± 0.2 | 1.1 ± 0.8 | 1.2 ± 0.4 | 1.4 ± 0.5 | 0.003 |
| ASAT (U/L) | 26 ± 13 | 52 ± 61 | 52 ± 78 | 35 ± 25 | 0.311 |
| ALAT (U/L) | 27 ± 15 | 37 ± 27 | 43 ± 12 | 31 ± 25 | 0.569 |
| Gamma GT (U/L) | 30 ± 40 | 56 ± 100 | 89 ± 133 | 78 ± 88 | 0.076 |
| HbA1c (rel%) | 5.4 ± 0.6 | 6.0 ± 0.9 | 6.6 ± 1.7 | 7.1 ± 2.4 | <0.001 |
| Erythrocytes (T/L) | 4.7 ± 0.5 | 4.5 ± 0.6 | 4.4 ± 0.6 | 4.6 ± 0.7 | 0.028 |
| Hemoglobin (g/dL) | 13.8 ± 1.4 | 13.3 ± 1.8 | 12.8 ± 1.8 | 12.8 ± 2.4 | 0.012 |
| Hematocrit (%) | 40 ± 3 | 39 ± 5 | 39 ± 5 | 39 ± 7 | 0.392 |
| Platelet count (G/L) | 243 ± 56 | 236 ± 74 | 250 ± 101 | 217 ± 89 | 0.040 |
| Leukocytes (G/L) | 6.6 ± 1.7 | 12.7 ± 2.0 | 8.0 ± 2.5 | 7.2 ± 2.1 | 0.494 |
| Parameters | Regression Coefficient B | Standard Error | Beta | T | p-Value |
|---|---|---|---|---|---|
| Constant | −2.056 | 0.334 | −6.149 | <0.001 | |
| Age (years) | 0.029 | 0.004 | 0.379 | 7888 | <0.001 |
| Sex | 0.351 | 0.083 | 0.188 | 2.614 | <0.001 |
| BMI (kg/m2) | 0.020 | 0.008 | 0.115 | 2.584 | 0.010 |
| GDF-15 (pg/mL) | 9.177 × 10−5 | 0.001 | 0.158 | 2.614 | 0.009 |
| NT-proBNP (pg/mL) | 3.702 × 10−5 | 0.001 | 0.172 | 2.983 | 0.003 |
| F = 38.0; p < 0.001; r2adj:0.346 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalos, D.; Spinka, G.; Schneider, M.; Wernly, B.; Paar, V.; Hoppe, U.; Litschauer, B.; Strametz-Juranek, J.; Sponder, M. New Cardiovascular Biomarkers in Ischemic Heart Disease—GDF-15, A Probable Predictor for Ejection Fraction. J. Clin. Med. 2019, 8, 924. https://doi.org/10.3390/jcm8070924
Dalos D, Spinka G, Schneider M, Wernly B, Paar V, Hoppe U, Litschauer B, Strametz-Juranek J, Sponder M. New Cardiovascular Biomarkers in Ischemic Heart Disease—GDF-15, A Probable Predictor for Ejection Fraction. Journal of Clinical Medicine. 2019; 8(7):924. https://doi.org/10.3390/jcm8070924
Chicago/Turabian StyleDalos, Daniel, Georg Spinka, Matthias Schneider, Bernhard Wernly, Vera Paar, Uta Hoppe, Brigitte Litschauer, Jeanette Strametz-Juranek, and Michael Sponder. 2019. "New Cardiovascular Biomarkers in Ischemic Heart Disease—GDF-15, A Probable Predictor for Ejection Fraction" Journal of Clinical Medicine 8, no. 7: 924. https://doi.org/10.3390/jcm8070924