Modeling the Longitudinal Effects of Insight on Depression, Quality of Life and Suicidality in Schizophrenia Spectrum Disorders: Results from the FACE-SZ Cohort

 ,
,  , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Design
2.2. Participants
2.3. Measures
2.4. Analyses
2.4.1. Models
2.4.2. Latent Variables and Longitudinal Invariance
2.5. Procedure
- Autoregressive model: only autoregressive paths (β)
- Expected model: autoregressive model + path XT0 → ΔY (β + γ1)
- Reverse model: autoregressive model + path YT0 → ΔX (β + γ2)
- Reciprocal model: expected + reverse model (β + γ1 and γ2)
3. Results
3.1. Participants and Evolution of the Measures
3.2. Model Comparisons
3.2.1. Bivariate Models
- Insight and quality of life, the best-fitting model was the expected model, suggesting that insight causes change in QoL.
- Quality of life and depression, the best-fitting model was the expected model, suggesting that QoL causes change in depression.
- Depression and suicidality, the best-fitting model was the reciprocal model. We estimated whether the two paths were significantly different by testing a constrained model, with coupling path coefficients fixed to equality. The constrained model did not fit the data significantly worse than the unconstrained model. Thus, we cannot conclude whether one link was significantly different than the other.
- Insight and depression, the best fitting model was the expected model, suggesting that insight causes change in depression.
- Insight and suicidality, the best fitting model was the expected model, suggesting that insight causes change in suicidality.
- Quality of life and suicidality, the best fitting model was the autoregressive model (no coupling path), suggesting that QoL and suicidality do not directly affect each other.
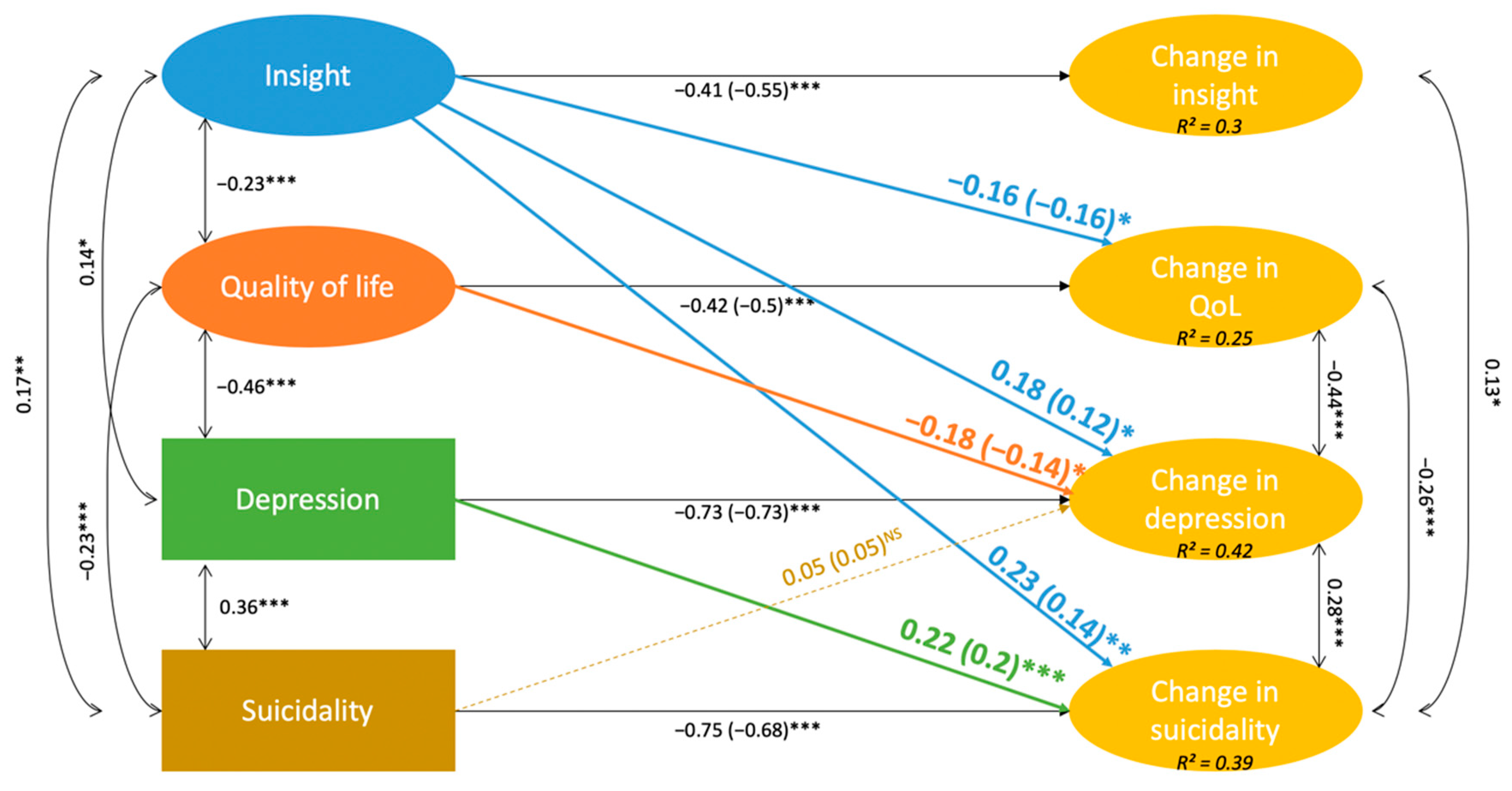
3.2.2. Final Multivariate Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harvey, P.D. Assessing disability in schizophrenia: Tools and contributors. J. Clin. Psychiatry 2014, 75, e27. [Google Scholar] [CrossRef] [PubMed]
- Hor, K.; Taylor, M. Suicide and schizophrenia: A systematic review of rates and risk factors. J. Psychopharmacol. (Oxf.) 2010, 24, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Nordentoft, M.; Mortensen, P.B.; Pedersen, C.B. Absolute risk of suicide after first hospital contact in mental disorder. Arch. Gen. Psychiatry 2011, 68, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H.Y. Treatment of suicidality in schizophrenia. Ann. N. Y. Acad. Sci. 2001, 932, 44–58; discussion 58–60. [Google Scholar] [CrossRef] [PubMed]
- David, A.S.; Amador, X.F. Insight and Psychosis: Awareness of Illness in Schizophrenia and Related Disorders; Oxford University Press: New York, NY, USA, 2004; ISBN 0-19-852568-0. [Google Scholar]
- Lysaker, P.H.; Vohs, J.; Hillis, J.D.; Kukla, M.; Popolo, R.; Salvatore, G.; Dimaggio, G. Poor insight into schizophrenia: Contributing factors, consequences and emerging treatment approaches. Expert Rev. Neurother. 2013, 13, 785–793. [Google Scholar] [CrossRef]
- Lincoln, T.M.; Lullmann, E.; Rief, W. Correlates and long-term consequences of poor insight in patients with schizophrenia. A systematic review. Schizophr. Bull. 2007, 33, 1324–1342. [Google Scholar] [CrossRef]
- Boyer, L.; Aghababian, V.; Richieri, R.; Loundou, A.; Padovani, R.; Simeoni, M.C.; Auquier, P.; Lançon, C. Insight into illness, neurocognition and quality of life in schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 2012, 36, 271–276. [Google Scholar] [CrossRef]
- Onwuameze, O.E.; Uga, A.; Paradiso, S. Longitudinal assessment of clinical risk factors for depression in schizophrenia spectrum disorders. Ann. Clin. Psychiatry Off. J. Am. Acad. Clin. Psychiatr. 2016, 28, 167–174. [Google Scholar]
- Misdrahi, D.; Denard, S.; Swendsen, J.; Jaussent, I.; Courtet, P. Depression in schizophrenia: The influence of the different dimensions of insight. Psychiatry Res. 2014, 216, 12–16. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Roe, D.; Yanos, P.T. Toward understanding the insight paradox: Internalized stigma moderates the association between insight and social functioning, hope, and self-esteem among people with schizophrenia spectrum disorders. Schizophr. Bull. 2007, 33, 192–199. [Google Scholar] [CrossRef]
- Belvederi Murri, M.; Respino, M.; Innamorati, M.; Cervetti, A.; Calcagno, P.; Pompili, M.; Lamis, D.A.; Ghio, L.; Amore, M. Is good insight associated with depression among patients with schizophrenia? Systematic review and meta-analysis. Schizophr. Res. 2015, 162, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Barrett, E.A.; Sundet, K.; Faerden, A.; Agartz, I.; Bratlien, U.; Romm, K.L.; Mork, E.; Rossberg, J.I.; Steen, N.E.; Andreassen, O.A.; et al. Suicidality in first episode psychosis is associated with insight and negative beliefs about psychosis. Schizophr. Res. 2010, 123, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.-C.; Liu, Y.-P. Suicidal behavior and insight into illness among patients with schizophrenia spectrum disorders. Psychiatr. Q. 2011, 82, 207–220. [Google Scholar] [CrossRef] [PubMed]
- López-Moríñigo, J.D.; Wiffen, B.; O’Connor, J.; Dutta, R.; Di Forti, M.; Murray, R.M.; David, A.S. Insight and suicidality in first-episode psychosis: Understanding the influence of suicidal history on insight dimensions at first presentation. Early Interv. Psychiatry 2014, 8, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Massons, C.; Lopez-Morinigo, J.-D.; Pousa, E.; Ruiz, A.; Ochoa, S.; Usall, J.; Nieto, L.; Cobo, J.; David, A.S.; Dutta, R. Insight and suicidality in psychosis: A cross-sectional study. Psychiatry Res. 2017, 252, 147–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, F.; Xiang, Y.-T.; Hou, Y.-Z.; Ungvari, G.S.; Dixon, L.B.; Chan, S.S.M.; Lee, E.H.M.; Li, W.-Y.; Li, W.-X.; Zhu, Y.-L.; et al. Suicide attempt and suicidal ideation and their associations with demographic and clinical correlates and quality of life in Chinese schizophrenia patients. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Roux, P.; Misdrahi, D.; Capdevielle, D.; Aouizerate, B.; Berna, F.; Brunel, L.; Chereau, I.; Dorey, J.-M.; Dubertret, C.; Dubreucq, J.; et al. Mediation Analyses of Insight, Quality of Life, Depression, and Suicidality: Results From the FACE-SZ Cohort. J. Clin. Psychiatry 2018, 79. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Morinigo, J.-D.; Di Forti, M.; Ajnakina, O.; Wiffen, B.D.; Morgan, K.; Doody, G.A.; Jones, P.B.; Ayesa-Arriola, R.; Canal-Rivero, M.; Crespo-Facorro, B. Insight and risk of suicidal behaviour in two first-episode psychosis cohorts: Effects of previous suicide attempts and depression. Schizophr. Res. 2019, 204, 80–89. [Google Scholar] [CrossRef]
- Bourgeois, M.; Swendsen, J.; Young, F.; Amador, X.; Pini, S.; Cassano, G.B.; Lindenmayer, J.-P.; Hsu, C.; Alphs, L.; Meltzer, H.Y. Awareness of disorder and suicide risk in the treatment of schizophrenia: Results of the international suicide prevention trial. Am. J. Psychiatry 2004, 161, 1494–1496. [Google Scholar] [CrossRef]
- van Rooijen, G.; van Rooijen, M.; Maat, A.; Vermeulen, J.M.; Meijer, C.J.; Ruhé, H.G.; de Haan, L.; Alizadeh, B.Z.; Bartels-Velthuis, A.A.; van Beveren, N.J.; et al. Longitudinal evidence for a relation between depressive symptoms and quality of life in schizophrenia using structural equation modeling. Schizophr. Res. 2019, 208, 82–89. [Google Scholar] [CrossRef]
- Cohen, C.I.; Vengassery, A.; Garcia Aracena, E.F. A Longitudinal Analysis of Quality of Life and Associated Factors in Older Adults with Schizophrenia Spectrum Disorder. Am. J. Geriatr. Psychiatry 2017, 25, 755–765. [Google Scholar] [CrossRef] [PubMed]
- McArdle, J.J.; Hamagami, F. Latent difference score structural models for linear dynamic analyses with incomplete longitudinal data. In New Methods for the Analysis of Change; Collins, L.M., Sayer, A.G., Eds.; American Psychological Association: Washington, DC, USA, 2001; pp. 139–175. ISBN 978-1-55798-754-9. [Google Scholar]
- Birchwood, M.; Smith, J.; Drury, V.; Healy, J.; Macmillan, F.; Slade, M. A self-report Insight Scale for psychosis: Reliability, validity and sensitivity to change. Acta Psychiatr. Scand. 1994, 89, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Cleary, S.D.; Bhatty, S.; Broussard, B.; Cristofaro, S.L.; Wan, C.R.; Compton, M.T. Measuring insight through patient self-report: An in-depth analysis of the factor structure of the Birchwood Insight Scale. Psychiatry Res. 2014, 216, 263–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michel, P.; Baumstarck, K.; Auquier, P.; Amador, X.; Dumas, R.; Fernandez, J.; Lancon, C.; Boyer, L. Psychometric properties of the abbreviated version of the Scale to Assess Unawareness in Mental Disorder in schizophrenia. BMC Psychiatry 2013, 13, 229. [Google Scholar] [CrossRef] [PubMed]
- Raffard, S.; Trouillet, R.; Capdevielle, D.; Gely-Nargeot, M.C.; Bayard, S.; Laroi, F.; Boulenger, J.P. French adaptation and validation of the scale to assess unawareness of mental disorder. Can. J. Psychiatry 2010, 55, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Jovanovski, D.; Zakzanis, K.K.; Atia, M.; Campbell, Z.; Young, D.A. A comparison between a researcher-rated and a self-report method of insight assessment in chronic schizophrenia revisited: A replication study using the SUMD and SAIQ. J. Nerv. Ment. Dis. 2007, 195, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Boyer, L.; Simeoni, M.C.; Loundou, A.; D’Amato, T.; Reine, G.; Lancon, C.; Auquier, P. The development of the S-QoL 18: A shortened quality of life questionnaire for patients with schizophrenia. Schizophr. Res. 2010, 121, 241–250. [Google Scholar] [CrossRef]
- Lancon, C.; Auquier, P.; Reine, G.; Bernard, D.; Addington, D. Relationships between depression and psychotic symptoms of schizophrenia during an acute episode and stable period. Schizophr. Res. 2001, 47, 135–140. [Google Scholar] [CrossRef]
- Addington, D.; Addington, J.; Maticka-Tyndale, E.; Joyce, J. Reliability and validity of a depression rating scale for schizophrenics. Schizophr. Res. 1992, 6, 201–208. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Taylor and Francis: Hoboken, NJ, USA, 2013; ISBN 978-1-134-74270-7. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Enders, C.K.; Bandalos, D.L. The Performance of the Full Information Maximum Likelihood Estimator in Multiple Regression Models with Missing Data. Educ. Psychol. Meas. 2001, 61, 713–740. [Google Scholar] [CrossRef]
- Satorra, A.; Bentler, P.M. Corrections to test statistics and standard errors in covariance structure analysis. In Latent Variables Analysis: Applications for Developmental Research; Sage Publications Inc.: Thousand Oaks, CA, USA, 1994; pp. 399–419. ISBN 0-8039-5330-5. [Google Scholar]
- Kievit, R.A.; Brandmaier, A.M.; Ziegler, G.; van Harmelen, A.-L.; de Mooij, S.M.M.; Moutoussis, M.; Goodyer, I.M.; Bullmore, E.; Jones, P.B.; Fonagy, P.; et al. Developmental cognitive neuroscience using latent change score models: A tutorial and applications. Dev. Cogn. Neurosci. 2018, 33, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Loehlin, J. Latent Variable Models: An Introduction to Factor, Path, and Structural Analysis, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1992. [Google Scholar]
- Pijnenborg, G.H.M.; Timmerman, M.E.; Derks, E.M.; Fleischhacker, W.W.; Kahn, R.S.; Aleman, A. Differential effects of antipsychotic drugs on insight in first episode schizophrenia: Data from the European First-Episode Schizophrenia Trial (EUFEST). Eur. Neuropsychopharmacol. 2015, 25, 808–816. [Google Scholar] [CrossRef]
- Yamauchi, K.; Aki, H.; Tomotake, M.; Iga, J.; Numata, S.; Motoki, I.; Izaki, Y.; Tayoshi, S.; Kinouchi, S.; Sumitani, S.; et al. Predictors of subjective and objective quality of life in outpatients with schizophrenia. Psychiatry Clin. Neurosci. 2008, 62, 404–411. [Google Scholar] [CrossRef]
- Zouari, L.; Thabet, J.B.; Elloumi, Z.; Elleuch, M.; Zouari, N.; Maâlej, M. Qualité de vie des malades atteints de schizophrénie: Étude de 100 cas. L’Encéphale 2012, 38, 111–117. [Google Scholar] [CrossRef]
- Donde, C.; Vignaud, P.; Poulet, E.; Brunelin, J.; Haesebaert, F. Management of depression in patients with schizophrenia spectrum disorders: A critical review of international guidelines. Acta Psychiatr. Scand. 2018, 138, 289–299. [Google Scholar] [CrossRef]
- Tiihonen, J.; Walhbeck, K.; Lönnqvist, J.; Klaukka, T.; Ioannidis, J.P.A.; Volavka, J.; Haukka, J. Effectiveness of antipsychotic treatments in a nationwide cohort of patients in community care after first hospitalisation due to schizophrenia and schizoaffective disorder: Observational follow-up study. Br. Med. J. 2006, 333, 224. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, M.; Lançon, C.; Fond, G.; Faget-Agius, C.; Richieri, R.; Faugere, M.; Metairie, E.; Boucekine, M.; Llorca, P.-M.; Auquier, P.; et al. A structural equation modelling approach to explore the determinants of quality of life in schizophrenia. Schizophr. Res. 2016, 171, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Aki, H.; Tomotake, M.; Kaneda, Y.; Iga, J.-I.; Kinouchi, S.; Shibuya-Tayoshi, S.; Tayoshi, S.-Y.; Motoki, I.; Moriguchi, K.; Sumitani, S.; et al. Subjective and objective quality of life, levels of life skills, and their clinical determinants in outpatients with schizophrenia. Psychiatry Res. 2008, 158, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Ponizovsky, A.M.; Grinshpoon, A.; Levav, I.; Ritsner, M.S. Life satisfaction and suicidal attempts among persons with schizophrenia. Compr. Psychiatry 2003, 44, 442–447. [Google Scholar] [CrossRef]
- Baumeister, R.F. Suicide as escape from self. Psychol. Rev. 1990, 97, 90–113. [Google Scholar] [CrossRef] [PubMed]
- Fulginiti, A.; Brekke, J.S. Escape from Discrepancy: Self-Esteem and Quality of Life as Predictors of Current Suicidal Ideation Among Individuals with Schizophrenia. Community Ment. Health J. 2015, 51, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Benaiges, I.; Prat, G.; Adan, A. Health-related quality of life in patients with dual diagnosis: Clinical correlates. Health Qual. Life Outcomes 2012, 10, 106. [Google Scholar] [CrossRef]
- Adan, A.; del Mar Capella, M.; Prat, G.; Forero, D.A.; López-Vera, S.; Navarro, J.F. Executive Functioning in Men with Schizophrenia and Substance Use Disorders. Influence of Lifetime Suicide Attempts. PLoS ONE 2017, 12, e0169943. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline | Follow-up | p | d | Statistics | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Age (years) | 32.4 | 9.4 | |||||
| Age at onset (years) | 21.6 | 6.4 | |||||
| Total duration of hospitalization (months) | 7.6 | 10 | |||||
| Insight latent score | 0 | 1.75 | 0.46 | 1.65 | <0.001 | 0.27 | t(343) = −5.35 |
| BIS (0–12) | 8.87 | 2.81 | 9.19 | 2.65 | 0.066 | 0.117 | t(290) = −1.84 |
| SUMD (0–100) | 30.46 | 32.03 | 22.91 | 29.98 | 0 | −0.242 | t(298) = 4.84 |
| PANSS G12 (1–7) | 3.13 | 1.52 | 2.82 | 1.55 | 0 | −0.201 | t(329) = 3.92 |
| Quality of life latent score | 0 | 21.27 | 7.95 | 20.94 | <0.001 | 0.37 | t(307) = −7.85 |
| Self-Esteem (0–100) | 46.76 | 30.21 | 56.88 | 26.31 | 0 | 0.352 | t(307) = −6.96 |
| Resilience (0–100) | 55.17 | 25.91 | 59.53 | 25.6 | 0.005 | 0.169 | t(307) = −2.85 |
| Autonomy (0–100) | 58.73 | 27.81 | 61.64 | 26.02 | 0.029 | 0.108 | t(307) = −2.2 |
| Physical well-being (0–100) | 45.29 | 27.84 | 51.33 | 26.06 | 0 | 0.223 | t(307) = −4.14 |
| Psychological well-being (0–100) | 51.41 | 27.31 | 58.72 | 26.4 | 0 | 0.27 | t(307) = −4.43 |
| Family relationships (0–100) | 69.16 | 25.51 | 71.99 | 23.57 | 0.034 | 0.115 | t(307) = −2.13 |
| Friends relationships (0–100) | 47.18 | 28.64 | 54.45 | 26.31 | 0 | 0.262 | t(307) = −4.27 |
| Sentimental life (0–100) | 33.85 | 28.75 | 37.77 | 28.66 | 0.018 | 0.136 | t(307) = −2.37 |
| CDS without suicide item (0–24) | 3.91 | 4.02 | 2.76 | 3.22 | 0 | −0.312 | t(327) = 6.12 |
| Calgary suicide item | 0.27 | 0.61 | 0.2 | 0.48 | 0.032 | −0.127 | t(328) = 2.15 |
| Risk of suicide (0–5) | 1.4 | 1.78 | 0.98 | 1.46 | 0 | −0.297 | t(313) = 5.07 |
| PANSS Positive (7–49) | 14.87 | 5.28 | 13.09 | 4.7 | 0 | −0.351 | t(329) = 6.54 |
| Negative (7–49) | 20.99 | 7.17 | 18.7 | 7.18 | 0 | −0.315 | t(329) = 6.57 |
| General without G12 (16–105) | 35.63 | 9.66 | 32.69 | 9.22 | 0 | −0.308 | t(329) = 5.96 |
| Chlorpromazine equivalent doses | 517.39 | 590.67 | 585.33 | 682.51 | 0.042 | 0.106 | t(262) = −2.04 |
| n | % | n | % | ||||
| Sex, male | 264 | 76.7 | |||||
| Schizophrenia/Scz-aff/Scz-form disorder | 269/72/3 | 78.2/20.9/0.9 | |||||
| Hospitalized the current year | 132 | 38.9 | |||||
| Suicide attempt over the past year, yes | 26 | 7.6 | 6 | 1.7 | |||
| Path | B (β) | SE | Z | p | |
|---|---|---|---|---|---|
| QoL and depression CFI = 0.951, TLI = 0.947, RMSEA < 0.05 (p = 1), SRMR = 0.05 | QoL → ΔQoL | −0.39 (−0.47) | 0.06 | −6.99 | <0.001 |
| Dep → ΔDep | −0.71 (−0.71) | 0.06 | −11.73 | <0.001 | |
| QoL → ΔDep | −0.21 (−0.17) | 0.08 | −2.51 | 0.01 | |
| QoL ←→ Dep | −0.28 (−0.46) | 0.05 | −6.22 | <0.001 | |
| ΔQoL ←→ ΔDep | −0.2 (−0.45) | 0.04 | −5.5 | <0.001 | |
| QoL and suicidality CFI = 0.952, TLI = 0.949, RMSEA < 0.05 (p = 1), SRMR = 0.049 | QoL → ΔQoL | −0.41 (−0.49) | 0.06 | −7.1 | <0.001 |
| Sui → ΔSui | −0.63 (−0.58) | 0.06 | −11.11 | <0.001 | |
| QoL ←→ Sui | −0.16 (−0.23) | 0.05 | −3.5 | <0.001 | |
| ΔQoL ←→ ΔSui | −0.14 (−0.26) | 0.04 | −3.58 | <0.001 | |
| Depression and suicidality CFI = 0.959, TLI = 0.912, RMSEA < 0.05 (p = 0.23), SRMR = 0.034 | Dep → ΔDep | −0.66 (−0.66) | 0.06 | −11.86 | <0.001 |
| Sui → ΔSui | −0.71 (−0.66) | 0.06 | −11.74 | <0.001 | |
| Dep → ΔSui | 0.22 (0.2) | 0.05 | 4.15 | <0.001 | |
| Sui → ΔDep | 0.1 (0.1) | 0.05 | 2.08 | 0.038 | |
| Dep ←→ Sui | 0.29 (0.36) | 0.05 | 5.61 | <0.001 | |
| ΔDep ←→ ΔSui | 0.2 (0.29) | 0.04 | 4.64 | <0.001 | |
| Insight and depression CFI = 0.933, TLI = 0.91, RMSEA = 0.065, SRMR = 0.047 | Ins → ΔIns | −0.39 (−0.52) | 0.09 | −4.4 | <0.001 |
| Dep → ΔDep | −0.64 (−0.64) | 0.05 | −12.1 | <0.001 | |
| Ins → ΔDep | 0.25 (0.16) | 0.08 | 3.13 | 0.002 | |
| Ins ←→ Dep | 0.07 (0.14) | 0.03 | 2.03 | 0.042 | |
| ΔIns ←→ ΔDep | 0 (0.01) | 0.02 | 0.15 | 0.88 | |
| Insight and QoL CFI = 0.928, TLI = 0.923, RMSEA < 0.05 (p = 0.97), SRMR = 0.056 | Ins → ΔIns | −0.4 (−0.54) | 0.05 | −7.4 | <0.001 |
| QoL → ΔQoL | −0.42 (−0.5) | 0.06 | −7.61 | <0.001 | |
| Ins → ΔQoL | −0.14 (−0.14) | 0.07 | −2.08 | 0.038 | |
| Ins ←→ QoL | −0.1 (−0.24) | 0.03 | −3.39 | 0.001 | |
| ΔIns ←→ ΔQoL | −0.02 (−0.11) | 0.02 | −1.23 | 0.22 | |
| Insight and suicidality CFI = 0.95, TLI = 0.932, RMSEA < 0.05 (p = 0.32), SRMR = 0.045 | Ins → ΔIns | −0.31 (−0.48) | 0.09 | −3.36 | 0.001 |
| Sui → ΔSui | −0.66 (−0.61) | 0.06 | −11.21 | <0.001 | |
| Ins → ΔSui | 0.24 (0.15) | 0.08 | 3.12 | 0.002 | |
| Ins ←→ Sui | 0.01 (0.17) | 0.03 | 2.89 | 0.004 | |
| ΔIns ←→ ΔSui | 0.05 (0.15) | 0.03 | 1.98 | 0.048 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ehrminger, M.; Urbach, M.; Passerieux, C.; Aouizerate, B.; Berna, F.; Bohec, A.-L.; Capdevielle, D.; Chereau, I.; Clauss, J.; Dubertret, C.; et al. Modeling the Longitudinal Effects of Insight on Depression, Quality of Life and Suicidality in Schizophrenia Spectrum Disorders: Results from the FACE-SZ Cohort. J. Clin. Med. 2019, 8, 1196. https://doi.org/10.3390/jcm8081196
Ehrminger M, Urbach M, Passerieux C, Aouizerate B, Berna F, Bohec A-L, Capdevielle D, Chereau I, Clauss J, Dubertret C, et al. Modeling the Longitudinal Effects of Insight on Depression, Quality of Life and Suicidality in Schizophrenia Spectrum Disorders: Results from the FACE-SZ Cohort. Journal of Clinical Medicine. 2019; 8(8):1196. https://doi.org/10.3390/jcm8081196
Chicago/Turabian StyleEhrminger, Mickaël, Mathieu Urbach, Christine Passerieux, Bruno Aouizerate, Fabrice Berna, Anne-Lise Bohec, Delphine Capdevielle, Isabelle Chereau, Julie Clauss, Caroline Dubertret, and et al. 2019. "Modeling the Longitudinal Effects of Insight on Depression, Quality of Life and Suicidality in Schizophrenia Spectrum Disorders: Results from the FACE-SZ Cohort" Journal of Clinical Medicine 8, no. 8: 1196. https://doi.org/10.3390/jcm8081196