Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis

 , ,
, ,  ,
,  , , , , , , , , ,
, , , , , , , , ,  , ,
, ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Experimental Section
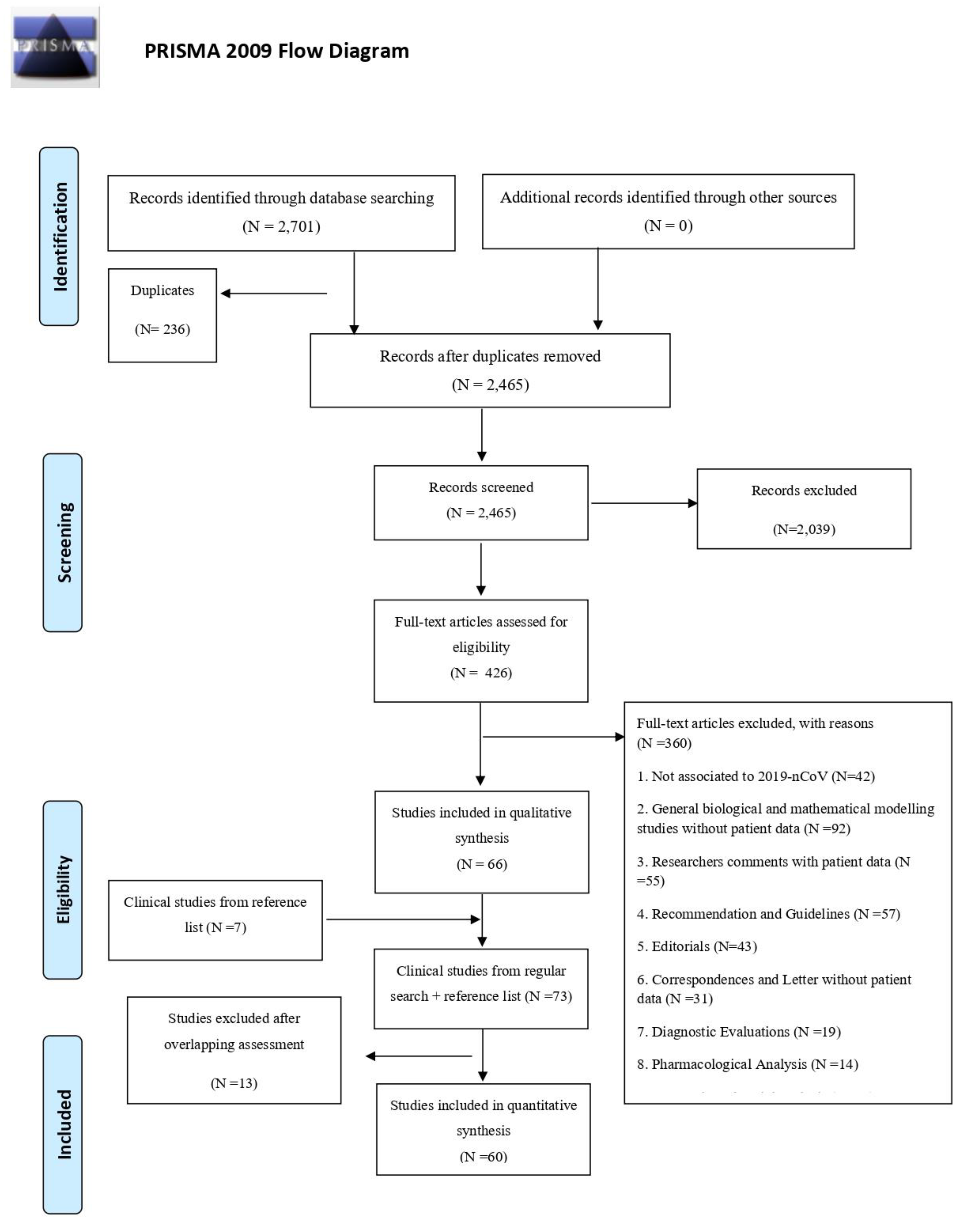
2.1. Literature Search and Selection Criteria
2.2. Outcomes
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Study and Patient Characteristics
3.2. Risk of Bias
3.3. Clinical Symptoms
3.4. Chest Imaging Findings
3.5. Laboratory Findings
3.6. Management and Mortality
3.7. Epidemiological Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lu, H.; Stratton, C.W.; Tang, Y.W. Outbreak of pneumonia of unknown etiology in Wuhan China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report—38; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005); Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Naming the Coronavirus Disease (COVID-2019) and the Virus that Causes It. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 1 March 2020).
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Chen, P.; Wang, J.; Feng, J.; Zhou, H.; Li, X.; Hao, P. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci. China Life Sci. 2020, 63, 457–460. [Google Scholar] [CrossRef] [Green Version]
- Hu, B.; Zeng, L.-P.; Yang, X.-L.; Ge, X.Y.; Zhang, W.; Li, B.; Xie, J.-Z.; Shen, X.-R.; Zhang, Y.-Z.; Wang, N.; et al. Discovery of a rich gene pool of bat SARS-related coronaviruses provides new insights into the origin of SARS coronavirus. PLoS Pathog. 2017, 13, e1006698. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Shi, Z.; Yu, M.; Ren, W.; Smith, C.; Epstein, J.H.; Wang, H.; Crameri, G.; Hu, Z.; Zhang, H.; et al. Bats are natural reservoirs of SARS-like coronaviruses. Science 2005, 310, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Sun, P.; Qie, S.; Liu, Z.; Ren, J.; Xi, J.J. Clinical characteristics of 50466 patients with SARS-CoV-2 infection. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based. Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- University of Bristol CfRSaDA. The ROBINS-E tool (Risk of Bias in Non-Randomized Studies-of Exposures). 2018. Available online: https://www.bristol.ac.uk/population-health-sciences/centres/cresyda/barr/riskofbias/robins-e/ (accessed on 25 March 2020).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Liu, H.; Liu, W.; Liu, J.; Liu, K.; Shang, J.; Deng, Y.; Wei, S. Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 203–208. [Google Scholar] [PubMed]
- Feng, K.; Yun, Y.; Wang, X.; Yang, G.D.; Zheng, Y.J.; Lin, C.M.; Wang, L. Analysis of CT features of 15 children with 2019 novel coronavirus infection. Zhonghua Er Ke Za Zhi 2020, 58, E007. [Google Scholar] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Y.; Guan, H.; Zhou, S.; Wang, Y.; Li, Q.; Zhu, T.; Hu, Q.; Xia, L. Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): A study of 63 patients in Wuhan, China. Eur. Radiol. Available online: https://link.springer.com/content/pdf/10.1007/s00330-020-06731-x.pdf (accessed on 25 March 2020). [CrossRef] [PubMed] [Green Version]
- Hu, J.; He, G.; Liu, T.; Xiao, J.P.; Rong, Z.H.; Guo, L.C.; Zeng, W.; Zhu, Z.; Gond, D.; Yin, L.; et al. Risk assessment of exported risk of novel coronavirus pneumonia from Hubei Province. Zhonghua Yu Fang Yi Xue Za Zhi 2020, 54, E017. [Google Scholar] [PubMed]
- Novel CPERE. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 2020, 41, 145–151. [Google Scholar]
- Sun, K.; Chen, J.; Viboud, C. Early epidemiological analysis of the coronavirus disease 2019 outbreak based on crowdsourced data: A population-level observational study. Lancet Digital Health. 2020. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Zhang, C.; Huang, F.; Wang, F.; Yuan, J.; Wang, Z.; Li, J.; Feng, C.; Zhang, Z.; et al. Clinical and biochemical indexes from SARS-CoV-2 infected patients linked to viral loads and lung injury. Sci. China Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Dias, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT findings in coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology 2020, 200463. [Google Scholar] [CrossRef] [Green Version]
- Team C-NIRS. COVID-19, Australia: Epidemiology Report 3 (Reporting week ending 19:00 AEDT 15 February 2020). Commun. Dis. Intell. (2018) 2020, 44. [Google Scholar] [CrossRef]
- Bai, S.; Wang, J.; Zhou, Y.; Yu, D.S.; Gao, X.M.; Li, L.L.; Yang, F. Analysis of the first cluster of cases in a family of novel coronavirus pneumonia in Gansu Province. Zhonghua Yu Fang Yi Xue Za Zhi 2020, 54, E005. [Google Scholar] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Yang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastola, A.; Sah, R.; Rodriguez-Morales, A.J.; Lal, B.; Jha, R.; Ojha, H.; Shrestha, B.; Chu, D.; Poon, L.; Costello, A.; et al. The first 2019 novel coronavirus case in Nepal. Lancet Infect. Dis. 2020, 20, 279–280. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Wang, X.; Ge, Y.; Xia, A.; Chang, H.; Tian, H.; Zhu, Y.; Wang, Q.; Zeng, J. First case of 2019 novel coronavirus infection in children in Shanghai. Zhonghua Er Ke Za Zhi 2020, 58, E002. [Google Scholar]
- Chang, D.; Lin, M.; Wei, L.; Xie, L.; Zhu, G.; Dela Cruz, C.S.; Sharma, L. Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA 2020. [Google Scholar] [CrossRef]
- Chen, F.; Liu, Z.; Zhang, F.; Xiong, R.H.; Chen, Y.; Cheng, X.F.; Wang, W.; Ren, J. First case of severe childhood novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 2020, 58, E005. [Google Scholar]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Yang, Y.; Fayad, Z.; Jacobi, A.; et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Duan, Y.-N.; Qin, J. Pre-and posttreatment chest CT findings: 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 21. [Google Scholar] [CrossRef]
- Fang, X.; Zhao, M.; Li, S.; Yang, L.; Wu, B. Changes of CT Findings in a 2019 Novel Coronavirus (2019-nCoV) pneumonia patient. QJM 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 200432. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Zhang, H.; Xu, Y.; Xie, J.; Pang, P.; Ji, W. CT manifestations of two cases of 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 208–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovanetti, M.; Benvenuto, D.; Angeletti, S.; Ciccozzi, M. The first two cases of 2019-nCoV in Italy: Where they come from? J. Med. Virol. 2020, 92, 518–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, W.; Li, M.; Huang, X. First atypical case of 2019 novel coronavirus in Yan’an, China. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Huang, P.; Liu, T.; Huang, L.; Liu, H.; Lei, M.; Xu, W.; Hu, X.; Chen, J.; Liu, B. Use of chest CT in combination with negative RT-PCR assay for the 2019 novel coronavirus but high clinical suspicion. Radiology 2020, 200330. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Ki, M. Epidemiologic characteristics of early cases with 2019 novel coronavirus (2019-nCoV) disease in Korea. Epidemiol. Health 2020, 42, e2020007. [Google Scholar] [CrossRef]
- Lei, J.; Li, J.; Li, X.; Qi, X. CT imaging of the 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 18. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.; Lau, E.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Gong, Z.; Xiao, Z.; Xiong, J.; Fan, B.; Liu, J. Novel coronavirus pneumonia outbreak in 2019: Computed tomographic findings in two cases. Korean J. Radiol. 2020, 21, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Jiang, Z.; Shao, C.; Zhang, H.G.; Yue, H.M.; Chen, Z.H.; Ma, B.; Liu, W.; Huang, H.; Yang, J.; et al. Preliminary study of the relationship between novel coronavirus pneumonia and liver function damage: A multicenter study. Zhonghua Gan Zang Bing Za Zhi 2020, 28, 148–152. [Google Scholar]
- Kui, L.; Fang, Y.-Y.; Deng, Y.; Liu, W.; Wang, M.F.; Ma, J.P.; Xiao, W.; Wang, Y.; Zhong, M.; Li, C.; et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin. Med. J. 2020. [Google Scholar] [CrossRef]
- Liu, M.; He, P.; Liu, H.; Wang, X.J.; Li, F.J.; Chen, S.; Liu, J.; Li, C. Clinical characteristics of 30 medical workers infected with new coronavirus pneumonia. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 209–214. [Google Scholar]
- Liu, P.; Tan, X.-Z. 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 19. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health Labour and Welfare—Japan. Novel Coronavirus—Japan (ex-China). 2020. Available online: https://www.who.int/csr/don/17-january-2020-novel-coronavirus-japan-ex-china/en/ (accessed on 21 March 2020).
- Ministry of Public Health (MoPH) T. Novel Coronavirus—Thailand (ex-China). 2020. Available online: https://www.who.int/csr/don/14-january-2020-novel-coronavirus-thailand-ex-china/en/ (accessed on 21 March 2020).
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.; Yang, L.; et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020, 200370. [Google Scholar] [CrossRef] [Green Version]
- Phan, L.T.; Nguyen, T.V.; Luong, Q.C.; Nguyen, T.V.; Nguyen, H.T.; Le, H.Q. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N. Engl. J. Med. 2020, 382, 872–874. [Google Scholar] [CrossRef] [Green Version]
- Pongpirul, W.A.; Pongpirul, K.; Ratnarathon, A.C.; Prasithsirikul, W. Journey of a Thai taxi driver and novel coronavirus. N. Engl. J. Med. 2020, 382, 1067–1068. [Google Scholar] [CrossRef]
- Ren, L.-L.; Wang, Y.-M.; Wu, Z.-Q.; Xiang, Z.C.; Guo, L.; Xu, T.; Jiang, Y.; Xiong, Y.; Li, Y.; Li, X.W.; et al. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, H.; Han, X.; Zheng, C. Evolution of CT manifestations in a patient recovered from 2019 novel coronavirus (2019-nCoV) pneumonia in Wuhan, China. Radiology 2020, 295, 20. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, W.K.; Stroud, L.; Cleghorn, G.E.; Leis, J.A. First imported case of 2019 novel coronavirus in Canada, presenting as mild pneumonia. Lancet 2020, 395, 734. [Google Scholar] [CrossRef]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging coronavirus 2019-nCoV pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Tang, J.; Wei, F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wei, M.; Yuan, J.; Liu, Y.; Fu, T.; Yu, X.; Zhang, Z.-J. Novel coronavirus infection in hospitalized infants under 1 year of age in China. JAMA 2020. [Google Scholar] [CrossRef]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.; Hiu, D.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for typical 2019-nCoV pneumonia: Relationship to negative RT-PCR testing. Radiology 2020, 200343. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Yu, C.; Zhang, L.; Luo, L.; Liu, J. Imaging features of 2019 novel coronavirus pneumonia. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.-W.; Wu, X.-X.; Jiang, X.-G.; Xu, K.J.; Ying, L.J.; Ma, C.L.; Wang, H.; Zhang, S.; Gao, H.; Sheng, J.F.; et al. Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. BMJ 2020, 368, m606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, L.; Tao, X.; Yuan, W.; Wang, J.; Liu, X.; Liu, Z. First case of neonate infected with novel coronavirus pneumonia in China. Zhonghua Er Ke Za Zhi 2020, 58, E009. [Google Scholar] [PubMed]
- Zhang, J.j.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.; Gao, Y. Clinical characteristics of 140 patients infected by SARS-CoV-2 in Wuhan, China. Allergy 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wang, X.; Chen, Y.; Zhao, K.L.; Cai, Y.Q.; An, C.L.; Lin, M.; Mu, X. Clinical features of 2019 novel coronavirus pneumonia in the early stage from a fever clinic in Beijing. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, E013. [Google Scholar] [PubMed]
- Zhang, Y.; Lin, D.; Xiao, M.; Wang, J.C.; Wei, Y.; Lei, Z.X.; Zeng, Z.; Li, L.; Li, H.; Xiang, W. 2019-novel coronavirus infection in a three-month-old baby. Zhonghua Er Ke Za Zhi 2020, 58, E006. [Google Scholar] [PubMed]
- Zhang, Z.; Li, X.; Zhang, W.; Shi, Z.-L.; Zheng, Z.; Wang, T. Clinical features and treatment of 2019-nCoV pneumonia patients in Wuhan: Report of a couple cases. Virol. Sin. 2020, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Park, W.B.; Kwon, N.-J.; Choi, S.-J.; Kang, C.K.; Choe, P.G.; Kim, J.Y.; Yun, J.; Lee, G.; Seong, M.; Kim, N.; et al. Virus isolation from the first patient with SARS-CoV-2 in Korea. J. Korean Med. Sci. 2019, 35, e84. [Google Scholar] [CrossRef]
- Lim, J.; Jeon, S.; Shin, H.-Y.; Kim, M.J.; Seong, Y.M.; Lee, W.J.; Choe, K.; Kang, Y.; Lee, B.; Park, S. Case of the index patient who caused tertiary transmission of COVID-19 infection in Korea: The application of lopinavir/ritonavir for the treatment of COVID-19 infected pneumonia monitored by quantitative RT-PCR. J. Korean Med. Sci. 2020, 35, e79. [Google Scholar] [CrossRef]
- Kim, J.Y.; Choe, P.G.; Oh, Y.; Oh, K.J.; Kim, J.; Park, S.J.; Na, H.; Oh, M. The first case of 2019 novel coronavirus pneumonia imported into Korea from Wuhan, China: Implication for infection prevention and control measures. J. Korean Med. Sci. 2020, 35, e61. [Google Scholar] [CrossRef]
- Yang, Y.; Qingbin, L.; Mingjin, L.; Wang, Y.; Zhang, A.; Jalali, N.; Dean, N.; Longini, I.; Halloran, E.; Xu, B.; et al. Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China. medRxiv 2020. Preprint article. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Robles, A.; San Gil, A.; Pascual, V.; Calbo, E.; Viladot, E.; Benet, S.; Bienvenido, B.; Cuchi, E.; Torrer, J.; Canales, L.; et al. Viral vs bacterial community-acquired pneumonia: Radiologic features. Eur. Respir. J. 2011, 38, 2507. [Google Scholar]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Healthc. J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCall, B. COVID-19 and artificial intelligence: Protecting health-care workers and curbing the spread. Lancet Digital Health. 2020. [Google Scholar] [CrossRef]
- Stempniak, M. Artificial Intelligence Reads CT Images to Diagnose Coronavirus in Seconds. 2020. Available online: https://www.radiologybusiness.com/topics/artificial-intelligence/artificial-intelligence-ct-images-coronavirus-diagnosis (accessed on 1 March 2020).
- Namendyz-Silva, S. Respiratory support for patients with COVID-19 infection. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Cuomo, A.; Dulebohn, S.; Napolli, R. Features, Evaluation and Treatment Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar] [PubMed]
- Cao, Y.; Li, L.; Feng, Z.; Wan, S.; Huang, P.; Sun, X.; Wen, F.; Huang, X.; Ning, G.; Wang, W. Comparative genetic analysis of the novel coronavirus (SARS-CoV-2/SARS-CoV-2) receptor ACE2 in different populations. Cell Discov. 2020, 6, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Ma, Z.; Peppelenbosch, M.P.; Pan, Q. Potential association between COVID-19 mortality and health-care resource availability. Lancet Glob. Health 2020, 8, PE480. [Google Scholar] [CrossRef] [Green Version]
- Djulbegovic, B.; Guyatt, G.H. Progress in evidence-based medicine: A quarter century on. Lancet 2017, 390, 415–423. [Google Scholar] [CrossRef]


{kind=link}
| Laboratory Test | No. of Studies | Total Patient No. | Values in Physiologic Range n (%) | Values > Physiologic Range n (%) | Values < Physiologic Range n (%) | Lost to Follow up n (%) |
|---|---|---|---|---|---|---|
| Inflammatory markers | ||||||
| C-RP | 25 | 1637 | 427 (26.1%) | 900 (55.0%) | - | 310 (18.9%) |
| ESR | 7 | 105 | NA | 88 (83.8%) | - | NA |
| PCT | 12 | 1463 | NA | 98 (6.7%) | NA | NA |
| IL-6 | 1 | 99 | NA | 51 (52.0%) | NA | NA |
| Peripheral blood profile | ||||||
| Total WBC | 32 | 1747 | 1109 (63.5%) | 155 (8.9%) | 469 (26.8%) | 14 (0.8%) |
| Neutrophils | 20 | 204 | 143 (70.1%) | 48 (23.5%) | 6 (2.9%) | 7 (3.4%) |
| Lymphocytes | 25 | 464 | 159 (34.3%) | 47 (10.3%) | 256 (55.2%) | 2 (0.4%) |
| Platelets | 11 | 218 | NA | 64 (29.4%) | 25 (11.5%) | NA |
| Blood biochemistry | ||||||
| ALT | 12 | 1316 | NA | 211 (16.0%) | NA | NA |
| AST | 18 | 1420 | NA | 254 (17.9%) | NA | NA |
| LDH | 11 | 283 | NA | 157 (55.5%) | NA | NA |
| D-dimer | 16 | 1573 | NA | 527 (33.5%) | NA | NA |
| Outcome | Study Population | Incidence (95%CI) | Higgins I2-Test | Certainty of the Evidence (GRADE) |
|---|---|---|---|---|
| All patients | 31 studies (53,631 patients) | 0.3 (0.0–1.0) | 83% | (+) very low |
| Chinese patients | 28 studies (5632 patients) | 0.5 (0.0–1.4) | 85% | (+) very low |
| Patients from other countries | 3 studies (41 patients) | 0.0 (0.0–1.4) | 0% | (+) very low |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borges do Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; von Groote, T.C.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marusic, A.; Jeroncic, A.; et al. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. J. Clin. Med. 2020, 9, 941. https://doi.org/10.3390/jcm9040941
Borges do Nascimento IJ, Cacic N, Abdulazeem HM, von Groote TC, Jayarajah U, Weerasekara I, Esfahani MA, Civile VT, Marusic A, Jeroncic A, et al. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(4):941. https://doi.org/10.3390/jcm9040941
Chicago/Turabian StyleBorges do Nascimento, Israel Júnior, Nensi Cacic, Hebatullah Mohamed Abdulazeem, Thilo Caspar von Groote, Umesh Jayarajah, Ishanka Weerasekara, Meisam Abdar Esfahani, Vinicius Tassoni Civile, Ana Marusic, Ana Jeroncic, and et al. 2020. "Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 4: 941. https://doi.org/10.3390/jcm9040941