Small-Diameter Subchondral Drilling Improves DNA and Proteoglycan Content of the Cartilaginous Repair Tissue in a Large Animal Model of a Full-Thickness Chondral Defect



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Animal Experiments
2.3. Biochemical Analyses
2.4. Statistical Analysis
3. Results
3.1. Biochemical Evaluation of the Original Articular Cartilage
3.2. Biochemical Analysis of the Adjacent Articular Cartilage
3.3. Correlation Analysis between the Biochemical Parameters and Structural Indices of Osteochondral Repair
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pridie, K.H. A method of resurfacing osteoarthritic knee Joints. J. Bone Jt. Surg. (Br.) 1959, 41, 618–619. [Google Scholar]
- Gomoll, A.H.; Farr, J.; Gillogly, S.D.; Kercher, J.; Minas, T. Surgical management of articular cartilage defects of the knee. J. Bone Jt. Surg. Am. 2010, 92, 2470–2490. [Google Scholar]
- Safran, M.R.; Seiber, K. The evidence for surgical repair of articular cartilage in the knee. J. Am. Acad. Orthop. Surg. 2010, 18, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, F.; Koide, S.; Glimcher, M.J. Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J. Bone Jt. Surg. Am. 1993, 75, 532–553. [Google Scholar] [CrossRef]
- Orth, P.; Gao, L.; Madry, H. Microfracture for cartilage repair in the knee: A systematic review of the contemporary literature. Knee Surg. Sports Traumatol. Arthrosc. 2019, 28, 670–706. [Google Scholar] [CrossRef]
- Schinhan, M.; Gruber, M.; Vavken, P.; Dorotka, R.; Samouh, L.; Chiari, C.; Gruebl-Barabas, R.; Nehrer, S. Critical-size defect induces unicompartmental osteoarthritis in a stable ovine knee. J. Orthop. Res. 2011, 30, 214–220. [Google Scholar] [CrossRef]
- Madry, H.; Luyten, F.P.; Facchini, A. Biological aspects of early osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 2011, 20, 407–422. [Google Scholar] [CrossRef]
- Orth, P.; Duffner, J.; Zurakowski, D.; Cucchiarini, M.; Madry, H. Small-diameter awls improve articular cartilage repair after microfracture treatment in a translational animal model. Am. J. Sports Med. 2015, 44, 209–219. [Google Scholar] [CrossRef]
- Eldracher, M.; Orth, P.; Cucchiarini, M.; Pape, D.; Madry, H. Small subchondral drill holes improve marrow stimulation of articular cartilage defects. Am. J. Sports Med. 2014, 42, 2741–2750. [Google Scholar] [CrossRef]
- Furukawa, T.; Eyre, D.R.; Koide, S.; Glimcher, M.J. Biochemical studies on repair cartilage resurfacing experimental defects in the rabbit knee. J. Bone Jt. Surg. Am. 1980, 62, 79–89. [Google Scholar] [CrossRef]
- Goodrich, L.R.; Hidaka, C.; Robbins, P.D.; Evans, C.H.; Nixon, A.J. Genetic modification of chondrocytes with insulin-like growth factor-1 enhances cartilage healing in an equine model. J. Bone Jt. Surg. Br. 2007, 89, 672–685. [Google Scholar] [CrossRef] [PubMed]
- Orth, P.; Peifer, C.; Goebel, L.; Cucchiarini, M.; Madry, H. Comprehensive analysis of translational osteochondral repair: Focus on the histological assessment. Prog. Histochem. Cytochem. 2015, 50, 19–36. [Google Scholar] [CrossRef] [PubMed]
- Hurtig, M.; Buschmann, M.D.; Fortier, L.A.; Hoemann, C.D.; Hunziker, E.B.; Jurvelin, J.S.; Mainil-Varlet, P.; McIlwraith, C.W.; Sah, R.L.; Whiteside, R.A.; et al. Preclinical studies for cartilage repair: Recommendations from the international cartilage repair society. Cartilage 2011, 2, 137–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortier, L.A.; Mohammed, H.O.; Lust, G.; Nixon, A.J. Insulin-like growth factor-I enhances cell-based repair of articular cartilage. J. Bone Jt. Surg. Br. 2002, 84, 276–288. [Google Scholar] [CrossRef]
- Griffin, D.; Ortved, K.; Nixon, A.; Bonassar, L. Mechanical properties and structure-function relationships in articular cartilage repaired using IGF-I gene-enhanced chondrocytes. J. Orthop. Res. 2015, 34, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Strauss, E.J.; Goodrich, L.R.; Chen, C.-T.; Hidaka, C.; Nixon, A.J. Biochemical and biomechanical properties of lesion and adjacent articular cartilage after Chondral defect repair in an equine model. Am. J. Sports Med. 2005, 33, 1647–1653. [Google Scholar] [CrossRef]
- Maroudas, A. Balance between swelling pressure and collagen tension in normal and degenerate cartilage. Nature 1976, 260, 808–809. [Google Scholar] [CrossRef]
- Orth, P.; Zurakowski, D.; Alini, M.; Cucchiarini, M.; Madry, H. Reduction of sample size requirements by bilateral versus unilateral research designs in animal models for cartilage tissue engineering. Tissue Eng. Part C Methods 2013, 19, 885–891. [Google Scholar] [CrossRef] [Green Version]
- Orth, P.; Goebel, L.; Wolfram, U.; Ong, M.F.; Gräber, S.; Kohn, D.; Cucchiarini, M.; Ignatius, A.; Pape, D.; Madry, H.; et al. Effect of subchondral drilling on the microarchitecture of subchondral bone: Analysis in a large animal model at 6 months. Am. J. Sports Med. 2012, 40, 828–836. [Google Scholar] [CrossRef]
- Orth, P.; Madry, H. A low morbidity surgical approach to the sheep femoral trochlea. BMC Musculoskelet. Disord. 2013, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Madry, H.; Cucchiarini, M.; Stein, U.; Remberger, K.; Menger, M.; Kohn, D.; Trippel, S.B. Sustained transgene expression in cartilage defectsin vivo after transplantation of articular chondrocytes modified by lipid-mediated gene transfer in a gel suspension delivery system. J. Gene Med. 2003, 5, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-J.; Sah, R.L.; Doong, J.-Y.H.; Grodzinsky, A.J. Fluorometric assay of DNA in cartilage explants using Hoechst 33258. Anal. Biochem. 1988, 174, 168–176. [Google Scholar] [CrossRef]
- Stöve, J.; Schöniger, R.; Huch, K.; Re, B.; Günther, K.-P.; Puhl, W.; Scharf, H.-P. Effects of dexamethasone on proteoglycan content and gene expression of IL-1ß-stimulated osteoarthrotic chondrocytes in vitro. Acta Orthop. Scand. 2002, 73, 562–567. [Google Scholar] [CrossRef]
- Müller, G.; Hanschke, M. Quantitative and qualitative analyses of proteoglycans in cartilage extracts by precipitation with 1,9-Dimethylmethylene blue. Connect. Tissue Res. 1996, 33, 243–248. [Google Scholar] [CrossRef]
- Sellers, R.S.; Peluso, D.; Morris, E.A. The effect of recombinant human bone morphogenetic protein-2 (rhBMP-2) on the healing of full-thickness defects of articular cartilage. J. Bone Jt. Surg. Am. 1997, 79, 1452–1463. [Google Scholar] [CrossRef] [PubMed]
- Hollander, A.P.; Heathfield, T.F.; Webber, C.; Iwata, Y.; Bourne, R.; Rorabeck, C.; Poole, A.R. Increased damage to type II collagen in osteoarthritic articular cartilage detected by a new immunoassay. J. Clin. Investig. 1994, 93, 1722–1732. [Google Scholar] [CrossRef] [Green Version]
- Kaul, G.; Cucchiarini, M.; Remberger, K.; Kohn, D.; Madry, H. Failed cartilage repair for early osteoarthritis defects: A biochemical, histological and immunohistochemical analysis of the repair tissue after treatment with marrow-stimulation techniques. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 2315–2324. [Google Scholar] [CrossRef]
- Dausse, Y.; Grossin, L.; Miralles, G.; Pelletier, S.; Mainard, D.; Hubert, P.; Baptiste, D.; Gillet, P.; Dellacherie, E.; Netter, P.; et al. Cartilage repair using new polysaccharidic biomaterials: Macroscopic, histological and biochemical approaches in a rat model of cartilage defect. Osteoarthr. Cartil. 2003, 11, 16–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orth, P.; Cucchiarini, M.; Wagenpfeil, S.; Menger, M.; Madry, H. PTH [1-34]-induced alterations of the subchondral bone provoke early osteoarthritis. Osteoarthr. Cartil. 2014, 22, 813–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiss, A.; Cucchiarini, M.; Menger, M.D.; Kohn, D.; Hannig, M.; Madry, H. Enamel matrix derivative inhibits proteoglycan production and articular cartilage repair, delays the restoration of the subchondral bone and induces changes of the synovial membrane in a lapine osteochondral defect modelin vivo. J. Tissue Eng. Regen. Med. 2012, 8, 41–49. [Google Scholar] [CrossRef]
- Bekkers, J.E.; Tsuchida, A.; Vonk, L.; Van Rijen, M.; Dhert, W.; Creemers, L.B.; Saris, D. Single-stage cell-based cartilage regeneration using a combination of chondrons and mesenchymal stromal cells: Comparison with microfracture. Am. J. Sports Med. 2013, 41, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Orth, P.; Meyer, H.-L.; Goebel, L.; Eldracher, M.; Ong, M.F.; Cucchiarini, M.; Madry, H. Improved repair of chondral and osteochondral defects in the ovine trochlea compared with the medial condyle. J. Orthop. Res. 2013, 31, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Nixon, A.J.; Fortier, L.A.; Williams, J.; Mohammed, H. Enhanced repair of extensive articular defects by insulin-like growth factor-I-laden fibrin composites. J. Orthop. Res. 1999, 17, 475–487. [Google Scholar] [CrossRef]
- Hidaka, C.; Goodrich, L.; Chen, C.-T.; Warren, R.F.; Crystal, R.G.; Nixon, A.J. Acceleration of cartilage repair by genetically modified chondrocytes over expressing bone morphogenetic protein-7. J. Orthop. Res. 2003, 21, 573–583. [Google Scholar] [CrossRef]
- Garcia-Seco, E.; Wilson, D.A.; Cook, J.L.; Kuroki, K.; Kreeger, J.M.; Keegan, K.G. Measurement of articular cartilage stiffness of the femoropatellar, tarsocrural, and metatarsophalangeal Joints in horses and comparison with biochemical data. Vet. Surg. 2005, 34, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Larsen, A.; Clausen, C.; Osther, K.; Everland, H. Cartilage repair with chondrocytes in fibrin hydrogel and MPEG polylactide scaffold: An in vivo study in goats. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 690–698. [Google Scholar] [CrossRef]
- Mithoefer, K.; McAdams, T.; Williams, R.J.; Kreuz, P.C.; Mandelbaum, B.R. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: An evidence-based systematic analysis. Am. J. Sports Med. 2009, 37, 2053–2063. [Google Scholar] [CrossRef]
- Knutsen, G.; Drogset, J.O.; Engebretsen, L.; Grontvedt, T.; Isaksen, V.; Ludvigsen, T.C.; Roberts, S.; Solheim, E.; Strand, T.; Johansen, O.; et al. A randomized trial comparing autologous chondrocyte implantation with microfracture: Findings at five years. J. Bone Jt. Surg. Am. 2007, 89, 2105–2112. [Google Scholar] [CrossRef]
- Vanlauwe, J.; Saris, D.; Victor, J.; Almqvist, K.F.; Bellemans, J.; Luyten, F.P.; Bohnsack, M.; Claes, T.; Fortems, Y.; Handelberg, F.; et al. Five-year outcome of characterized chondrocyte implantation versus microfracture for symptomatic cartilage defects of the knee: Early treatment matters. Am. J. Sports Med. 2011, 39, 2566–2574. [Google Scholar] [CrossRef]
- Pritzker, K.P.; Gay, S.; Jimenez, S.A.; Ostergaard, K.; Pelletier, J.-P.; Revell, P.; Salter, D.; Berg, W.V.D. Osteoarthritis cartilage histopathology: Grading and staging. Osteoarthr. Cartil. 2006, 14, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Mankin, H.J.; Dorfman, H.; Lippiello, L.; Zarins, A. Biochemical and metabolic abnormalities in articular cartilage from osteo-arthritic human hips. II. Correlation of morphology with biochemical and metabolic data. J. Bone Jt. Surg. Am. 1971, 53, 523–537. [Google Scholar] [CrossRef]
- Madry, H.; Kon, E.; Condello, V.; Peretti, G.M.; Steinwachs, M.; Seil, R.; Berruto, M.; Engebretsen, L.; Filardo, G.; Angele, P.; et al. Early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1753–1762. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.L.; Pareek, A.; Obey, M.R.; Johnson, N.R.; Carey, J.L.; Stuart, M.B.; Krych, A.J. High rate of osteoarthritis after osteochondritis dissecans fragment excision compared with surgical restoration at a mean 16-year follow-up. Am. J. Sports Med. 2017, 21, 1799–1805. [Google Scholar] [CrossRef] [PubMed]
- Perelli, S.; Romoli, A.R.M.; Costa-Paz, M.; Erquicia, J.I.; Gelber, P.E.; Monllau, J.C. Internal fixation of osteochondritis dissecans of the knee leads to good long-term outcomes and high degree of healing without differences between fixation devices. J. Clin. Med. 2019, 8, 1934. [Google Scholar] [CrossRef] [Green Version]
- Squires, G.R.; Okouneff, S.; Ionescu, M.; Poole, A.R. The pathobiology of focal lesion development in aging human articular cartilage and molecular matrix changes characteristic of osteoarthritis. Arthritis Rheum. 2003, 48, 1261–1270. [Google Scholar] [CrossRef]
- Orth, P.; Zurakowski, D.; Wincheringer, D.; Madry, H. Reliability, reproducibility, and validation of five major histological scoring systems for experimental articular cartilage repair in the rabbit model. Tissue Eng. Part C Methods 2012, 18, 329–339. [Google Scholar] [CrossRef]
- Orth, P.; Cucchiarini, M.; Zurakowski, D.; Menger, M.; Kohn, D.; Madry, H. Parathyroid hormone [1-34] improves articular cartilage surface architecture and integration and subchondral bone reconstitution in osteochondral defects in vivo. Osteoarthr. Cartil. 2013, 21, 614–624. [Google Scholar] [CrossRef] [Green Version]
- Orth, P.; Cucchiarini, M.; Kaul, G.; Ong, M.; Gräber, S.; Kohn, D.; Madry, H. Temporal and spatial migration pattern of the subchondral bone plate in a rabbit osteochondral defect model. Osteoarthr. Cartil. 2012, 20, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Lu, K. On efficiency of constrained longitudinal data analysis versus longitudinal analysis of covariance. Biometrics 2009, 66, 891–896. [Google Scholar] [CrossRef]
- Hartigan, E.; Lynch, A.; Logerstedt, D.S.; Chmielewski, T.L.; Snyder-Mackler, L. Kinesiophobia after anterior cruciate ligament rupture and reconstruction: Noncopers versus potential copers. J. Orthop. Sports Phys. Ther. 2013, 43, 821–832. [Google Scholar] [CrossRef]
- Garcia, T.P.; Marder, K. Statistical approaches to longitudinal data analysis in neurodegenerative diseases: Huntington’s disease as a Model. Curr. Neurol. Neurosci. Rep. 2017, 17, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Specimen | Unit | 1.0 mm | 1.8 mm | x-Fold Difference | p | |
|---|---|---|---|---|---|---|
| Original cartilage | DNA | [ng/μg] | 2.7−2 ± 0.9−2 | 3.3−2 ± 1.6−2 | 1.2 | 0.435 |
| Proteoglycans | [μg/μg] | 8.4−3 ± 3.3−3 | 10.5−3 ± 6.7−3 | 1.3 | 0.514 | |
| Proteoglycans/DNA | [μg/ng] | 3.2−1 ± 0.7−1 | 3.3−1 ± 1.5−1 | 1.0 | 0.878 | |
| Type II collagen | [μg/μg] | 6.7−4 ± 5.0−4 | 5.6−4 ± 2.7−4 | 1.2 | 0.644 | |
| Type II collagen/DNA | [μg/ng] | 2.6−2 ± 1.5−2 | 1.8−2 ± 0.6−2 | 1.4 | 0.261 | |
| Type I collagen | [μg/μg] | 0.8−4 ± 0.5−4 | 0.8−4 ± 0.3−4 | 1.1 | 0.741 | |
| Type I collagen/DNA | [μg/ng] | 0.3−2 ± 0.2−2 | 0.3−2 ± 0.1−2 | 1.2 | 0.455 | |
| Type I/Type II collagen | [μg/μg] | 1.3−1 ± 1.0−1 | 1.4−1 ± 0.7−1 | 0.9 | 0.688 | |
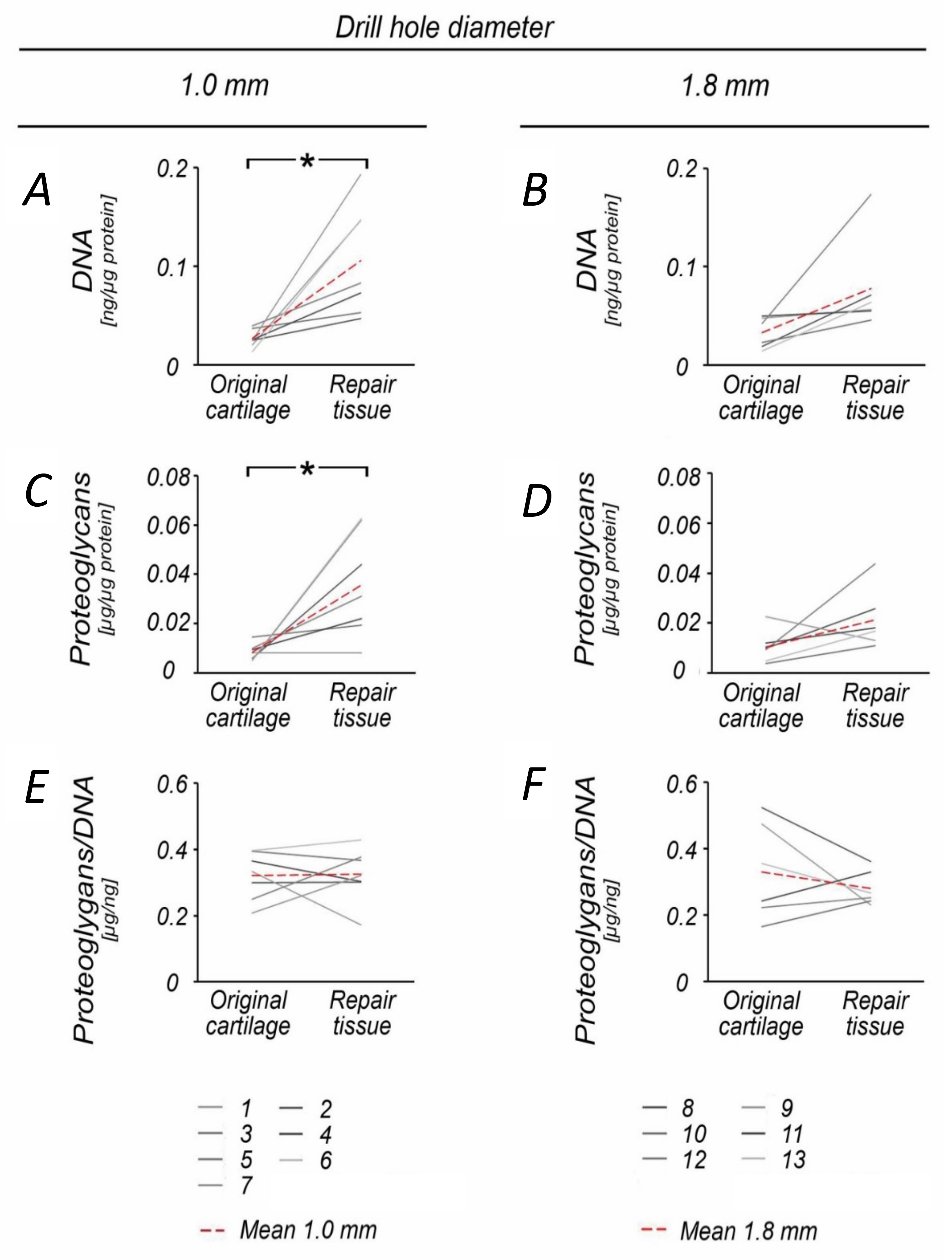
| Repair cartilage | DNA | [ng/μg] | 10.5−2 ± 5.6−2 | 7.7−2 ± 4.8−2 | 1.4 | 0.344 |
| Proteoglycans | [μg/μg] | 35.6−3 ± 21.3−3 | 21.4−3 ± 12.1−3 | 1.7 | 0.162 | |
| Proteoglycans/DNA | [μg/ng] | 3.2−1 ± 0.8−1 | 2.8−1 ± 0.5−1 | 1.2 | 0.271 | |
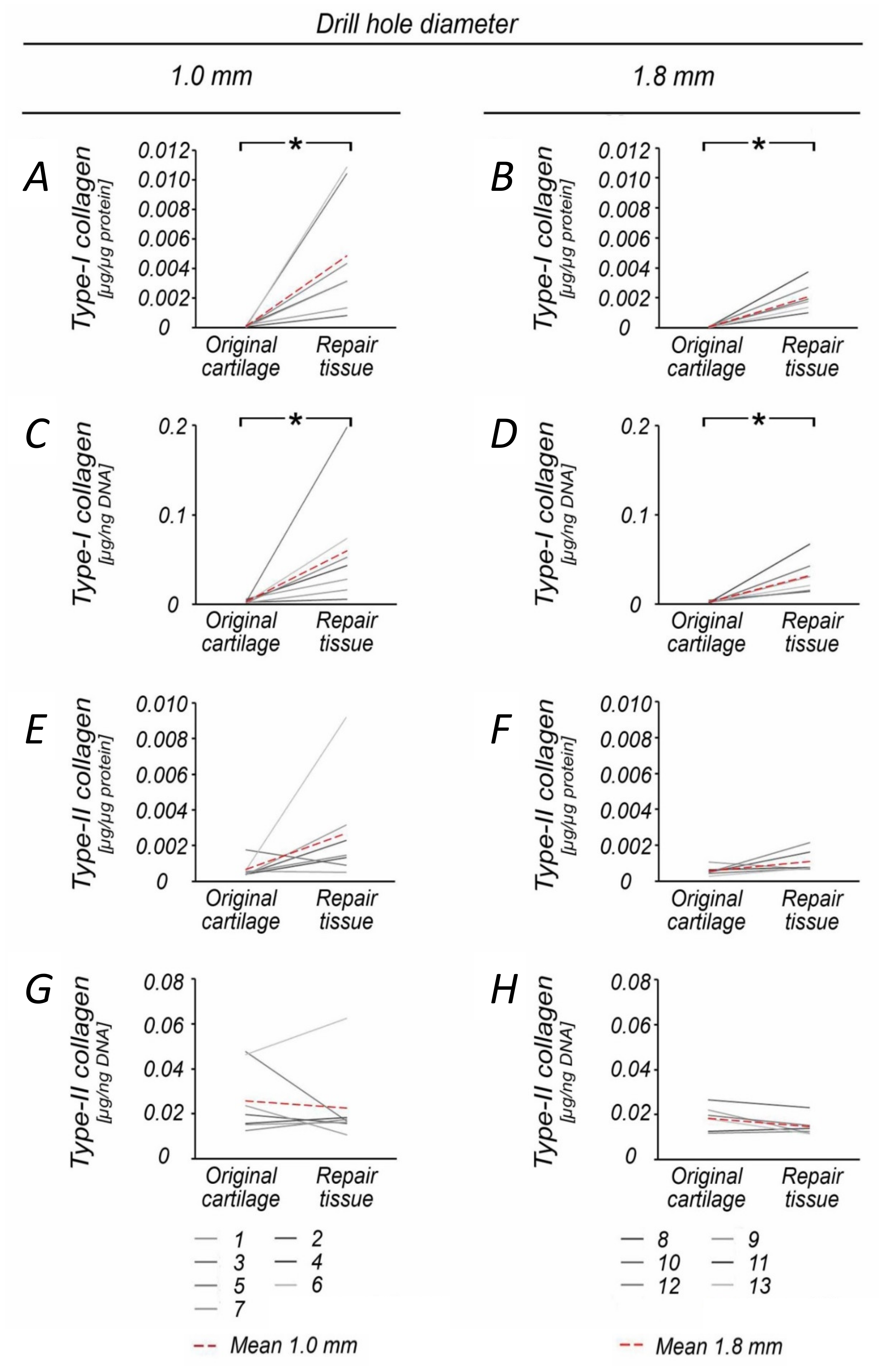
| Type II collagen | [μg/μg] | 26.9−4 ± 30.0−4 | 11.0−4 ± 6.4−4 | 2.4 | 0.215 | |
| Type II collagen/DNA | [μg/ng] | 2.3−2 ± 1.8−2 | 1.5−2 ± 0.4−2 | 1.5 | 0.287 | |
| Type I collagen | [μg/μg] | 48.6−4 ± 41.2−4 | 20.8−4 ± 9.9−4 | 2.3 | 0.127 | |
| Type I collagen/DNA | [μg/ng] | 6.0−2 ± 6.5−2 | 3.2−2 ± 2.0−2 | 1.9 | 0.324 | |
| Type I/Type II collagen | [μg/μg] | 1.8 ± 3.9 | 1.9 ± 1.5 | 1.0 | 0.505 | |
| Adjacent cartilage | DNA | [ng/μg] | 6.9−2 ± 1.2−2 | 6.6−2 ± 1.7−2 | 1.1 | 0.679 |
| Proteoglycans | [μg/μg] | 18.7−3 ± 3.3−3 | 18.6−3 ± 4.2−3 | 1.0 | 0.968 | |
| Proteoglycans/DNA | [μg/ng] | 2.8−1 ± 0.6−1 | 2.9−1 ± 0.6−1 | 1.1 | 0.668 | |
| Type II collagen | [μg/μg] | 8.7−4 ± 3.5−4 | 9.3−4 ± 3.4−4 | 1.1 | 0.752 | |
| Type II collagen/DNA | [μg/ng] | 2.3−2 ± 1.8−2 | 1.5−2 ± 0.4−2 | 1.5 | 0.287 | |
| Type I collagen | [μg/μg] | 38.3−4 ± 27.3−4 | 44.4−4 ± 28.0−4 | 1.2 | 0.701 | |
| Type I collagen/DNA | [μg/ng] | 5.5−2 ± 3.5−2 | 6.9−2 ± 4.2−2 | 1.3 | 0.532 | |
| Type I/Type II collagen | [μg/μg] | 4.4 ± 4.1 | 4.8 ± 4.0 | 0.9 | 0.787 |
| p | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Drill Hole Diameter | Specimen | DNA | Proteoglycans | Proteoglycans/DNA | Type II Collagen | Type II Collagen/DNA | Type I Collagen | Type I Collagen/DNA | Type I/ Type II Collagen | |
| [ng/μg] | [μg/μg] | [μg/ng] | [μg/μg] | [μg/ng] | [μg/μg] | [μg/ng] | [μg/μg] | |||
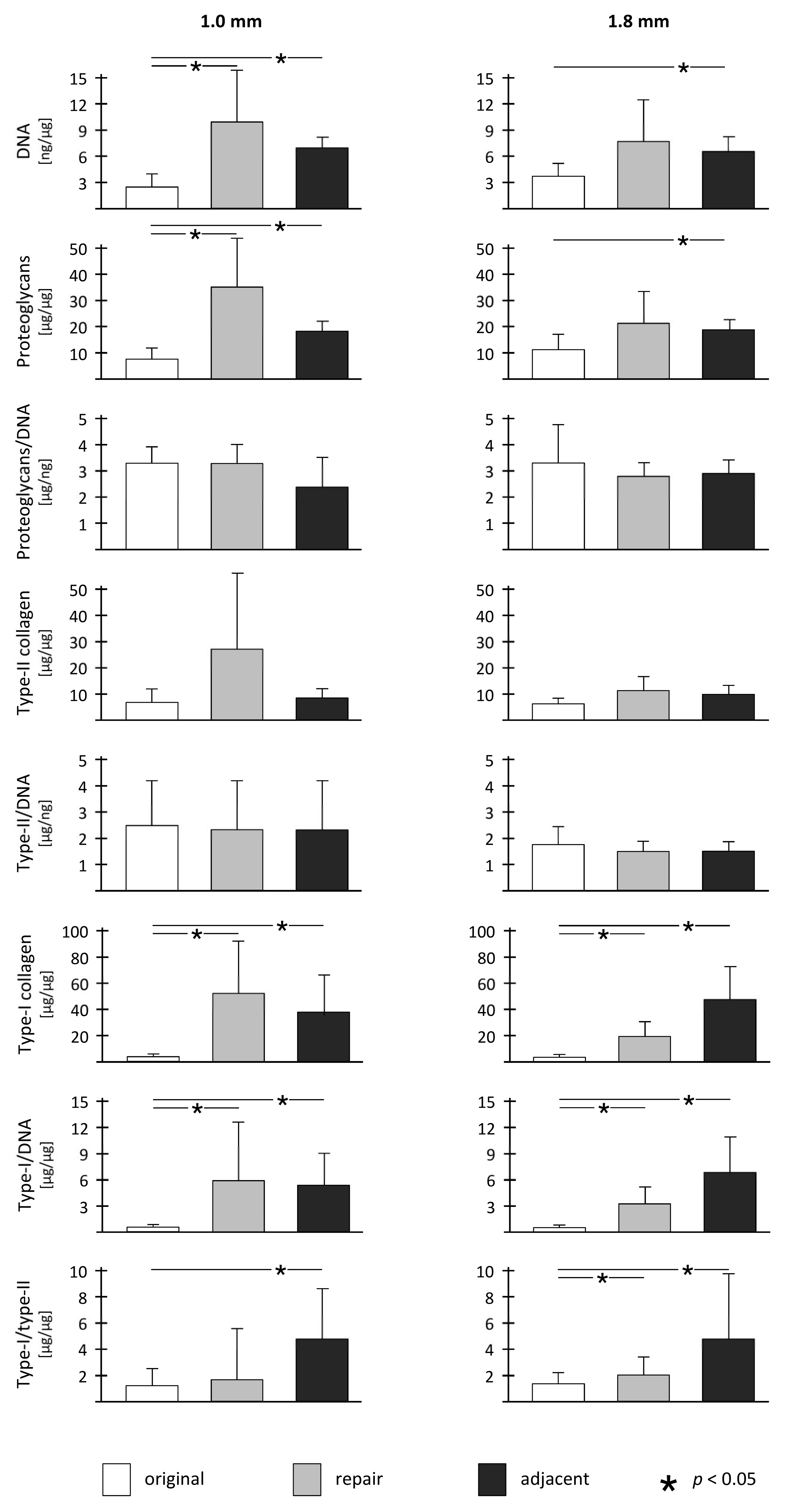
| 1.0 mm | Original cartilage | Repair cartilage | 0.010 | 0.015 | 0.935 | 0.128 | 0.722 | 0.022 | 0.020 | 0.062 |
| Original cartilage | Adjacent cartilage | <0.001 | <0.001 | 0.252 | 0.399 | 0.064 | 0.011 | 0.008 | 0.011 | |
| Repair cartilage | Adjacent cartilage | 0.136 | 0.082 | 0.250 | 0.161 | 0.208 | 0.595 | 0.877 | 0.447 | |
| 1.8 mm | Original cartilage | Repair cartilage | 0.072 | 0.089 | 0.452 | 0.096 | 0.223 | <0.001 | 0.016 | 0.005 |
| Original cartilage | Adjacent cartilage | 0.006 | 0.037 | 0.562 | 0.063 | 0.196 | 0.012 | 0.011 | 0.011 | |
| Repair cartilage | Adjacent cartilage | 0.596 | 0.610 | 0.737 | 0.565 | 0.920 | 0.099 | 0.092 | 0.133 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orth, P.; Eldracher, M.; Cucchiarini, M.; Madry, H. Small-Diameter Subchondral Drilling Improves DNA and Proteoglycan Content of the Cartilaginous Repair Tissue in a Large Animal Model of a Full-Thickness Chondral Defect. J. Clin. Med. 2020, 9, 1903. https://doi.org/10.3390/jcm9061903
Orth P, Eldracher M, Cucchiarini M, Madry H. Small-Diameter Subchondral Drilling Improves DNA and Proteoglycan Content of the Cartilaginous Repair Tissue in a Large Animal Model of a Full-Thickness Chondral Defect. Journal of Clinical Medicine. 2020; 9(6):1903. https://doi.org/10.3390/jcm9061903
Chicago/Turabian StyleOrth, Patrick, Mona Eldracher, Magali Cucchiarini, and Henning Madry. 2020. "Small-Diameter Subchondral Drilling Improves DNA and Proteoglycan Content of the Cartilaginous Repair Tissue in a Large Animal Model of a Full-Thickness Chondral Defect" Journal of Clinical Medicine 9, no. 6: 1903. https://doi.org/10.3390/jcm9061903