The Impact of the Extent of Surgery on the Long-Term Outcomes of Patients with Low-Risk Differentiated Non-Medullary Thyroid Cancer: A Systematic Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Extraction
2.2. Risk of Bias Assessment
2.3. Pre-Intervention
- Domain 1: Bias due to confounding (see below)
- Domain 2: Bias in selection of participants into the study
- Inclusion of patients (consecutive inclusion of all patients eligible or a random sample is considered low risk of bias).
- Definition of low risk thyroid cancer?
2.4. At Intervention
- Domain 3: Bias in classification of intervention.
- Were intervention groups clearly defined?
2.5. Post Intervention
- Domain 4: Bias due to missing data
- TNM-stage available (see below)
- Reporting of high-risk patients (see below)
- Reporting of RAI treatment (see below)
- Reporting number of patients included per treatment arm (see below)
- Domain 5: Bias in measurement of outcomes
- Loss to follow-up (<5% is considered low risk of bias)
- Criteria for extent of surgery (see below)
- Reporting of outcome definition
2.6. Statistical Analysis
3. Results
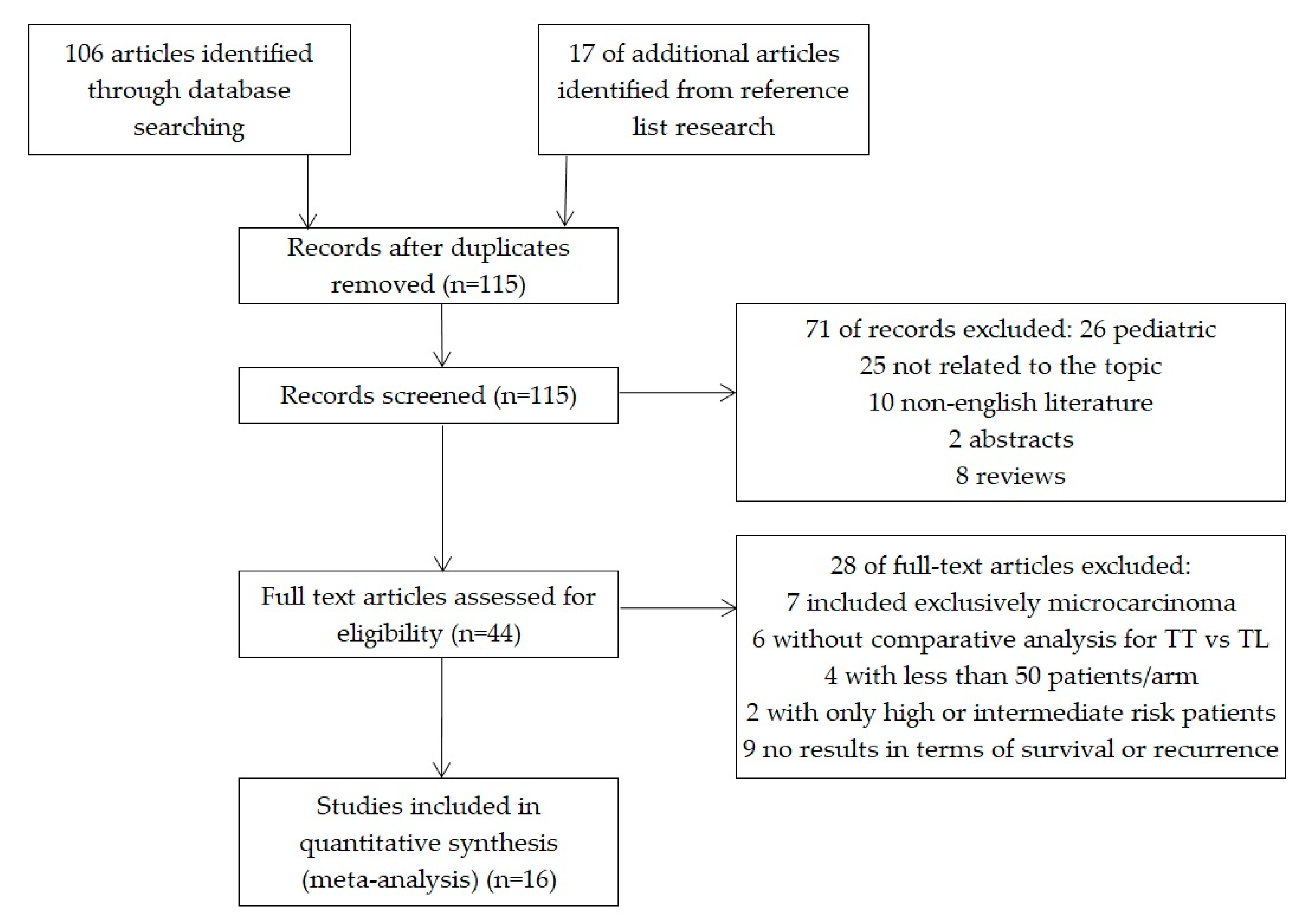
3.1. Characteristics of the Selected Studies
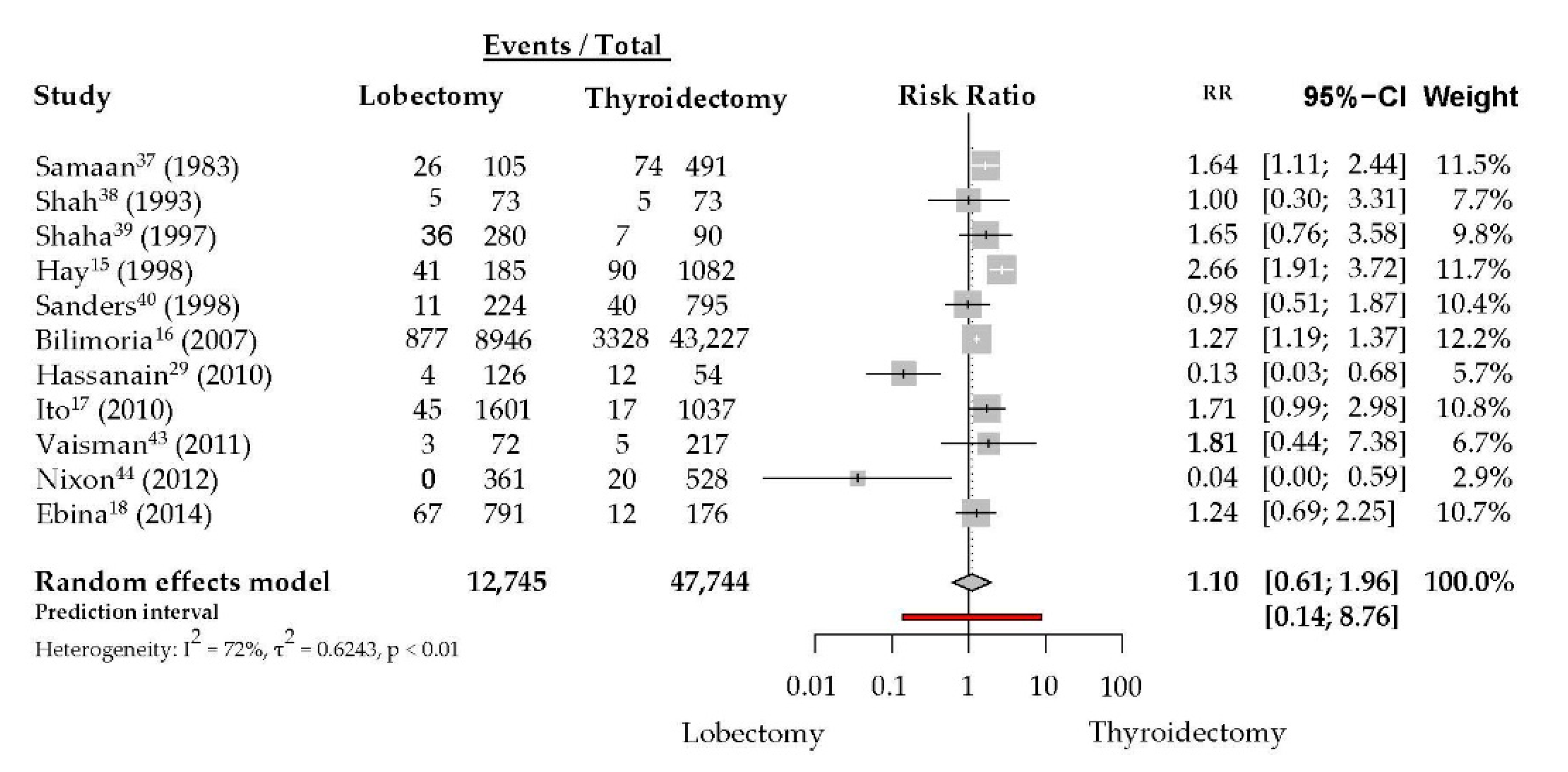
3.2. Any Thyroid Cancer-Related Recurrence
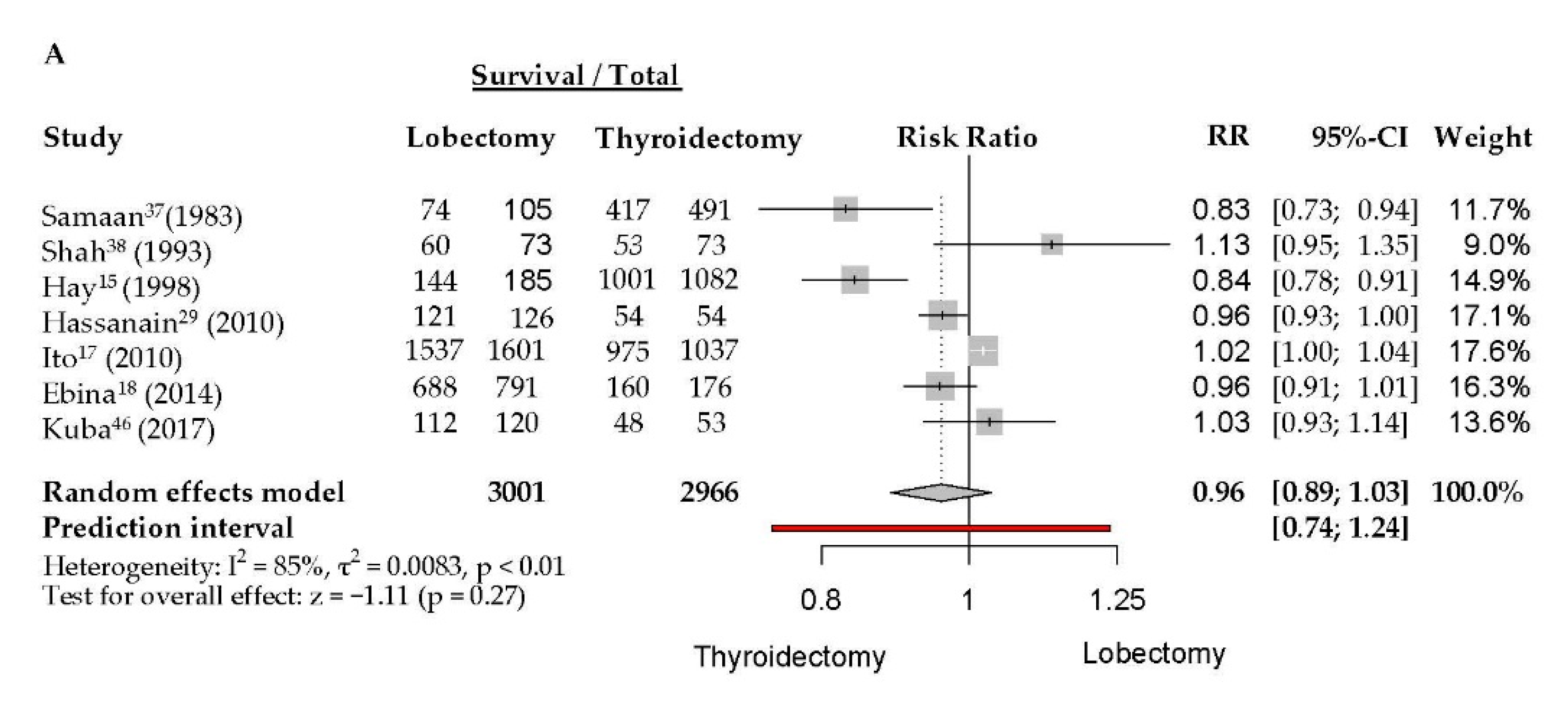
3.3. Survival Outcomes
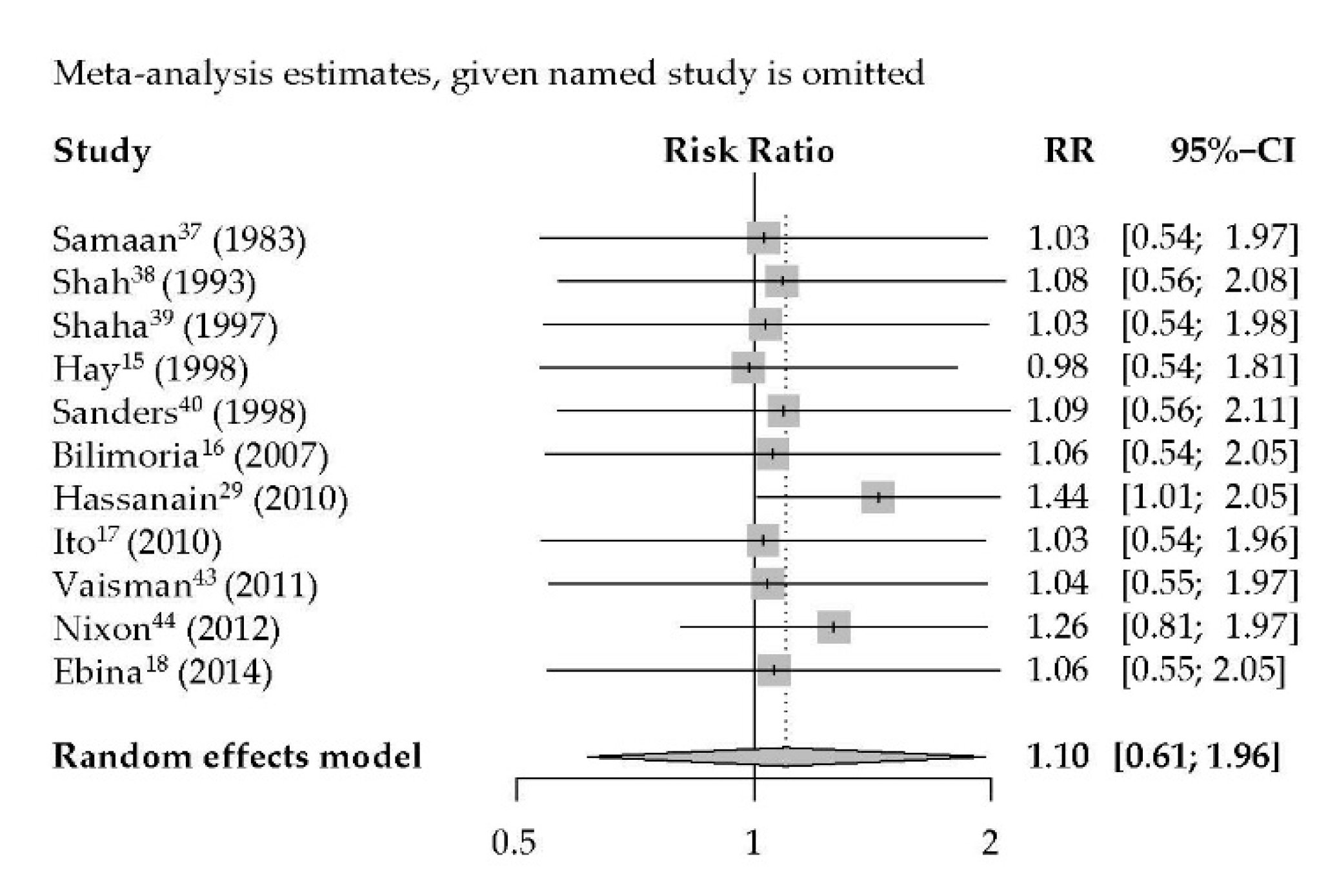
3.4. Sensitivity Analysis
3.5. Risk of Bias Assessment
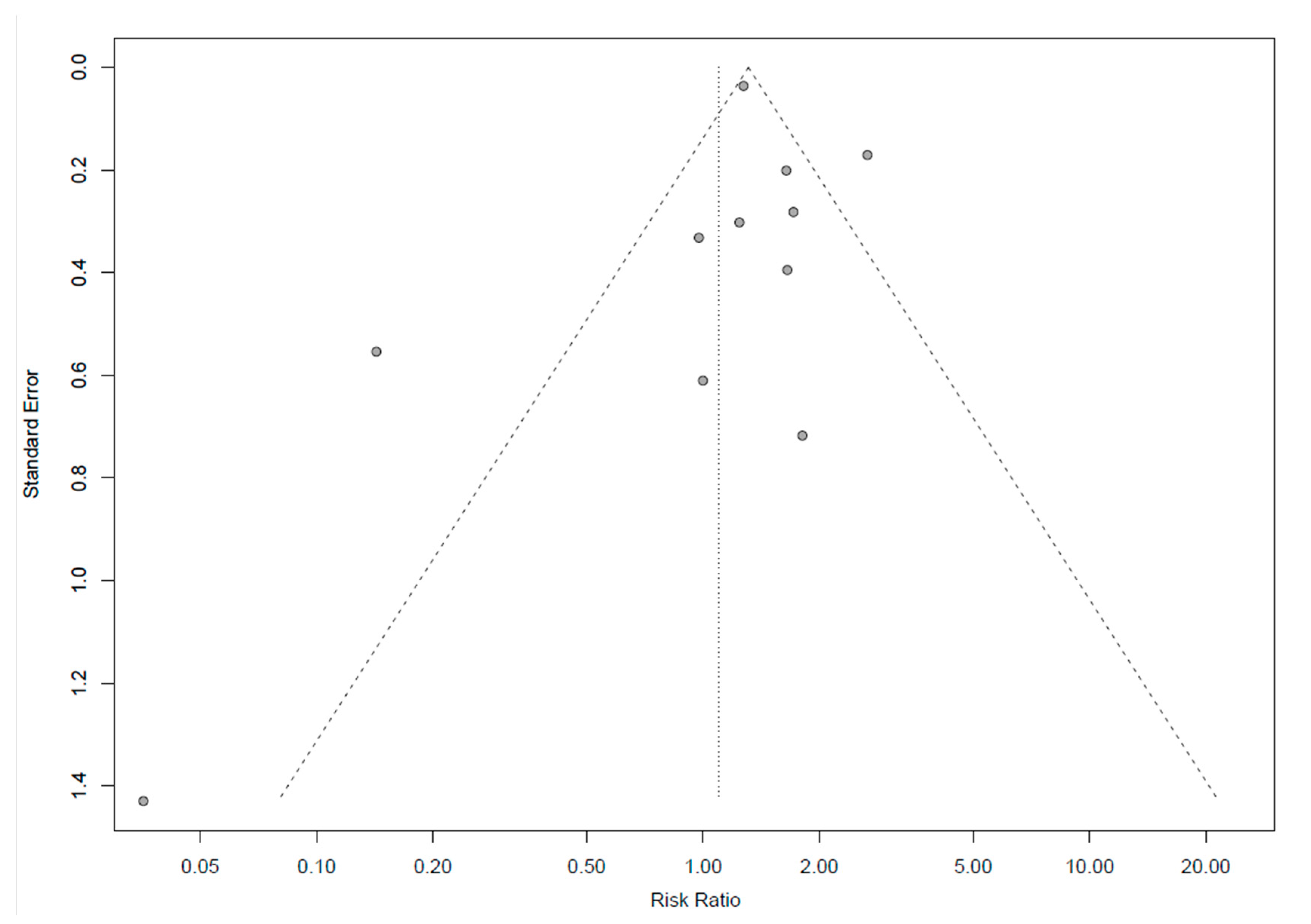
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Barney, B.M.; Hitchcock, Y.; Sharma, P.; Shrieve, D.C.; Tward, J.D. Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck 2010, 33, 645–649. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Morris, L.G.; Myssiorek, D. Improved detection does not fully explain the rising incidence of well-differentiated thyroid cancer: A population-based analysis. Am. J. Surg. 2010, 200, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, H.G.; Black, W.C. Overdiagnosis in cancer. J. Natl. Cancer Inst. 2010, 102, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harach, H.R.; Franssila, K.O.; Wasenius, V.-M. Occult papillary carcinoma of the thyroid. A “normal” finding in Finland. A systematic autopsy study. Cancer 1985, 56, 531–538. [Google Scholar] [CrossRef]
- Byrd, J.K.; Yawn, R.J.; Wilhoit, C.S.T.; Sora, N.D.; Meyers, L.; Fernandes, J.; Day, T. Well Differentiated Thyroid Carcinoma: Current Treatment. Curr. Treat. Options Oncol. 2012, 13, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Sosa, J.A.; Udelsman, R. Total thyroidectomy for differentiated thyroid cancer. J. Surg. Oncol. 2006, 94, 701–707. [Google Scholar] [CrossRef]
- Murthy, S.P.; Balasubramanian, D.; Anand, A.; Limbachiya, S.V.; Subramaniam, N.; Nair, V.; Thankappan, K.; Iyer, S. Extent of Thyroidectomy in Differentiated Thyroid Cancers—Review of Evidence. Indian J. Surg. Oncol. 2017, 9, 90–96. [Google Scholar] [CrossRef]
- Kim, S.H.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Differences in the recurrence and survival of patients with symptomatic and asymptomatic papillary thyroid carcinoma: An observational study of 11.265 person-years of follow-up. Thyroid 2016, 26, 1472–1479. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Thyroid Cancer Survival in the United States. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 440–444. [Google Scholar] [CrossRef] [Green Version]
- Nixon, I.; Shah, J.P. Well differentiated thyroid cancer: Are we over treating our patients? Eur. J. Surg. Oncol. 2014, 40, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Tarasova, V.; Tuttle, R.M. Current Management of Low Risk Differentiated Thyroid Cancer and Papillary Microcarcinoma. Clin. Oncol. 2017, 29, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Higashiyama, T.; Kobayashi, K.; Miya, A. Patient age is significantly related to the progression of papillary microcarcinoma of the thyroid under observation. Thyroid 2013, 24, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugitani, I.; Fujimoto, Y. Management of low-risk papillary thyroid carcinoma: Unique conventional policy in Japan and our efforts to improve the level of evidence. Surg. Today 2010, 40, 199–215. [Google Scholar] [CrossRef]
- Hay, I.D.; Grant, C.S.; Bergstrahl, E.J.; Thompson, G.B.; van Heerden, J.A.; Goellner, J.R. Unilateral total lobectomy: Is it sufficient surgical treatment for patients with AMES low-risk papillary thyroid carcinoma? Surgery 1998, 124, 958–966. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Stewart, A.K.; Winchester, D.P.; Talamonti, M.S.; Sturgeon, C. Extent of surgery affects survival for papillary thyroid cancer. Ann. Surg. 2007, 246, 375–384. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A. Excellent Prognosis for Patients with Solitary T1N0M0 Papillary Thyroid Carcinoma Who Underwent Thyroidectomy and Elective Lymph Node Dissection without Radioiodine Therapy: Reply to Letter. World J. Surg. 2010, 35, 233–234. [Google Scholar] [CrossRef]
- Ebina, A.; Sugitani, I.; Fujimoto, Y.; Yamada, K. Risk-adapted management of papillary thyroid carcinoma according to our own risk group classification system: Is thyroid lobectomy the treatment of choice for low-risk patients? Surgery 2014, 156, 1579–1589. [Google Scholar] [CrossRef]
- Udelsman, R.; Lakatos, E.; Ladenson, P. Optimal Surgery for Papillary Thyroid Carcinoma. World J. Surg. 1996, 20, 88–93. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef]
- Nixon, I. The Surgical Approach to Differentiated Thyroid Cancer. F1000Research 2015, 4, 1366. [Google Scholar] [CrossRef] [PubMed]
- Gibelli, B.; Dionisio, R.; Ansarin, M.; Mohssen, A. Role of hemithyroidectomy in differentiated thyroid cancer. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Cady, B.; Rossi, R. An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery 1988, 104, 947–953. [Google Scholar] [PubMed]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef]
- Bearhs, O.H.; Henson, D.E. AJCC Manual for Staging Cancer, 3rd ed.; J.B. Lippincott Company: Philadelphia, PA, USA, 1988; pp. 61–62. [Google Scholar]
- Greene, F.I.; Page, D.L. AJCC Manual for Staging Cancer, 6th ed.; Springer: New York, NY, USA, 2002; pp. 77–79. [Google Scholar]
- Hassanain, M.; Wexler, M.J. Conservative management of well-differentiated thyroid cancer. Can. J. Surg. 2010, 53, 109–118. [Google Scholar]
- Sterne, J.A.C.; Hernan, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Broersen, L.H.A.; Jha, M.; Biermasz, N.R.; Pereira, A.M.; Dekkers, O.M. Effectiveness of medical treatment for Cushing’s syndrome: A systematic review and meta-analysis. Pituitary 2018, 21, 631–641. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: http://www.R-project.org (accessed on 28 May 2019).
- Schwarzer, G. Meta: An R package for meta-analysis. R News 2007, 7, 40–45, version 4.9-5, 2007. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaan, N.A.; Maheshwari, Y.K.; Nader, S.; Hill, C.S.; Schultz, P.N.; Haynie, T.P.; Hickey, R.C.; Clark, R.L.; Goepfert, H.; Ibanez, M.L.; et al. Impact of therapy for differentiated carcinoma of the thyroid: An analysis of 706 cases. J. Clin. Endocrinol. Metab. 1983, 56, 1131–1138. [Google Scholar] [CrossRef]
- Shah, J.P.; Loree, T.R.; Dharker, D.; Strong, E.W. Lobectomy versus total thyroidectomy for differentiated carcinoma of the thyroid: A matched-pair analysis. Am. J. Surg. 1993, 166, 331–335. [Google Scholar] [CrossRef]
- Shaha, A.R.; Shah, J.P.; Loree, T.R. Low-risk differentiated thyroid cancer: The need for selective treatment. Ann. Surg. Oncol. 1997, 4, 328–333. [Google Scholar] [CrossRef]
- Sanders, L.E.; Cady, B. Differentiated thyroid cancer: Reexamination of risk groups and outcome of treatment. Arch. Surg. 1998, 133, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Haigh, P.I.; Urbach, D.R.; Rotstein, L.E. Extent of Thyroidectomy Is Not a Major Determinant of Survival in Low- or High-Risk Papillary Thyroid Cancer. Ann. Surg. Oncol. 2004, 12, 81–89. [Google Scholar] [CrossRef]
- Mendelsohn, A.H.; Elashoff, D.A.; Abemayor, E.; St John, M.A. Surgery for papillary thyroid cancer: Is lobectomy enough? Arch. Otolaryngol. Head Neck Surg. 2010, 136, 1055–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaisman, F.; Shaha, A.; Fish, S.; Tuttle, R.M. Initial therapy with either thyroid lobectomy or total thyroidectomy without radioactive iodine remnant ablation is associated with very low rates of structural disease recurrence in properly selected patients with differentiated thyroid cancer. Clin. Endocrinol. 2011, 75, 112–119. [Google Scholar] [CrossRef]
- Nixon, I.J.; Ganly, I.; Patel, S.G.; Palmer, F.L.; Whitcher, M.M.; Tuttle, R.M.; Shaha, A.; Shah, J.P. Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery 2012, 151, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.A.; Pura, J.; Gu, L.; Dinan, M.A.; Tyler, D.S.; Reed, S.D.; Scheri, R.; Roman, S.A.; Sosa, J.A. Extent of Surgery for Papillary Thyroid Cancer Is Not Associated With Survival. Ann. Surg. 2014, 260, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuba, S.; Yamanouchi, K.; Hayashida, N.; Maeda, S.; Adachi, T.; Sakimura, C.; Kawakami, F.; Yano, H.; Matsumoto, M.; Otsubo, R.; et al. Total thyroidectomy versus thyroid lobectomy for papillary thyroid cancer: Comparative analysis after propensity score matching: A multicenter study. Int. J. Surg. 2017, 38, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.; Smart, L.; Fielding, S.; Ramsay, C.; Krukowski, Z.H. Long term outcomes of simple clinical risk stratification in management of differentiated thyroid cancer. Surgeon 2018, 16, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferri, E.L.; Young, R.L.; Oertel, J.E.; Kemmerer, W.T.; Page, C.P. Papillary thyroid carcinoma: The impact of therapy in 576 patients. Medicine (Baltimore) 1977, 56, 171–196. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.B.; Lee, S.G.; Kim, M.J.; Kim, T.H.; Ban, E.J.; Lee, C.R.; Lee, J.; Kang, S.-W.; Jeong, J.J.; Nam, K.-H.; et al. Oncologic outcomes in patients with 1-cm to 4-cm differentiated thyroid carcinoma according to extent of thyroidectomy. Head Neck 2018, 41, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Momesso, D.P.; Vaisman, F.; Caminha, L.S.C.; Pessoa, C.H.C.N.; Corbo, R.; Vaisman, M. Surgical approach and radioactive iodine therapy for small well-differentiated thyroid cancer. J. Endocrinol. Investig. 2014, 37, 57–64. [Google Scholar] [CrossRef]
- Matsuzu, K.; Sugino, K.; Masudo, K.; Nagahama, M.; Kitagawa, W.; Shibuya, H.; Ohkuwa, K.; Uruno, T.; Suzuki, A.; Magoshi, S.; et al. Thyroid Lobectomy for Papillary Thyroid Cancer: Long-term Follow-up Study of 1,088 Cases. World J. Surg. 2013, 38, 68–79. [Google Scholar] [CrossRef]
- Chow, T.L.; Choi, C.Y.; Lam, S.H. Disease control of differentiated thyroid carcinomas by hemithyroidectomy. Singap. Med. J. 2010, 51, 311–314. [Google Scholar]
- Cady, B.; Sedgwick, C.E.; Meissner, W.A.; Bookwalter, J.R.; Romagosa, V.; Werber, J. Changing Clinical, Pathologic, Therapeutic, and Survival Patterns in Differentiated Thyroid Carcinoma. Ann. Surg. 1976, 184, 541–553. [Google Scholar] [CrossRef]
- Pitt, S.C.; Sippel, R.S.; Chen, H. Contralateral papillary thyroid cancer: Does size matter? Am. J. Surg. 2009, 197, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Liu, S.; Xu, Z.; Ni, S.; Zhang, Z.; Wang, X. Long-term outcome of thyroid lobectomy for unilateral multifocal papillary carcinoma. Medicine (Baltimore) 2017, 96, e7461. [Google Scholar] [CrossRef] [PubMed]
- DeGroot, L.J.; Kaplan, E.L.; McCormick, M.; Straus, F.H. Natural History, Treatment, and Course of Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 1990, 71, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Grigsby, P.W.; Reddy, R.M.; Moley, J.F.; Hall, B.L. Contralateral papillary thyroid cancer at completion thyroidectomy has no impact on recurrence or survival after radioiodine treatment. Surgery 2006, 140, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Schvartz, C.; Bonnetain, F.; Dabakuyo, S.; Gauthier, M.; Cueff, A.; Fieffe, S.; Cochet, I.; Crevisy, E.; Dalac, A.; Papathanassiou, D.; et al. Impact on Overall Survival of Radioactive Iodine in Low-Risk Differentiated Thyroid Cancer Patients. J. Clin. Endocrinol. Metab. 2012, 97, 1526–1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawka, A.M.; Thephamongkhol, K.; Brouwers, M.; Thabane, L.; Browman, G.; Gerstein, H.C. Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2004, 89, 3668–3676. [Google Scholar] [CrossRef] [Green Version]
- Peiris, A.N.; Medlock, D.; Gavin, M. Thyroglobulin for Monitoring for Thyroid Cancer Recurrence. JAMA 2019, 321, 1228. [Google Scholar] [CrossRef]
- Park, S.; Jeon, M.J.; Oh, H.-S.; Lee, Y.-M.; Sung, T.-Y.; Han, M.; Han, J.M.; Kim, T.Y.; Chung, K.-W.; Kim, W.B.; et al. Changes in Serum Thyroglobulin Levels After Lobectomy in Patients with Low-Risk Papillary Thyroid Cancer. Thyroid 2018, 28, 997–1003. [Google Scholar] [CrossRef]
- Harvey, R.D.; Matheson, N.A.; Grabowski, P.S.; Rodger, A.B. Measurement of serum thyroglobulin is of value in detecting tumour recurrence following treatment of differentiated thyroid carcinoma by lobectomy. Br. J. Surg. 1990, 77, 324–326. [Google Scholar] [CrossRef]
- Duren, M.; Yavuz, N.; Bukey, Y.; Ozyegin, M.A.; Gundogdu, S.; Açbay, O.; Hatemi, H.; Uslu, I.; Onsel, C.; Aksoy, F.; et al. Impact of initial surgical treatment on survival of patients with differentiated thyroid cancer: Experience of an endocrine surgery center in an iodine-deficient region. World J. Surg. 2000, 24, 1290–1294. [Google Scholar] [CrossRef]
- Friedman, M.; Pacella, B.L. Total versus subtotal thyroidectomy. Arguments, approaches, and recommendations. Otolaryngol. Clin. N. Am. 1990, 23, 413–427. [Google Scholar] [CrossRef]
- Verburg, F.; Flux, G. Differentiated Thyroid Cancer Patients Potentially Benefitting From Postoperative I-131 Therapy: A Review of the Literature of the Past Decade. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 78–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asimakopoulos, P.; Nixon, I. Surgical management of primary thyroid tumours. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 321–326. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year of Publication | Country | Female (%) | Mean Age (Y) | Time of Surgery Stated | Study Design | Surgical Approach | Follow-Up | Outcomes Assessed | RAI Given (%) | Histological Subtypes Included | High Risk Patients Included (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TL | TT | |||||||||||
| Samaan 1983 [36] | USA | 73 | NA | 1951–1975 | Retrospective cohort study | 105 | 491 | 6–30 Y | Recurrence, OS | yes (34%) | PTC, FTC, HCC | yes |
| Shah 1993 [37] | USA | 62 | 57 | 1930–1980 | Retrospective matched cohort study | 73 | 73 | 20 Y | Recurrence, DFS | yes * | PTC, FTC | yes |
| Shaha 1997 [38] | USA | 74 | 31 | 1930–1985 | Retrospective cohort study | 280 | 90 | 20 Y | Recurrence, DSS | NA | PTC, FTC | no |
| Hay 1998 [15] | USA | NA | 43 | 1940–1991 | Retrospective cohort study | 185 | 1082 | 16 Y | Recurrence, DFS, DSS | yes | PTC | no |
| Sanders 1998 [39] | USA | 72 | 44 | 1940–1990 | Retrospective cohort study | 224 | 795 | 0–47 Y | Recurrence, OS, DSS | NA | PTC, FTC, HCC | yes |
| Haigh 2004 [40] | USA | 77 | NA | 1988–1995 | Retrospective population-based cohort | 739 | 3663 | 1 mo–12 Y | OS | yes | PTC | Yes ** |
| Bilimoria 2007 [16] | USA | 76 | 43 | 1985–1998 | Retrospective population-based cohort | 8946 | 43,227 | 5.8 Y | Recurrence, OS | yes | PTC | yes |
| Mendelsohn 2010 [41] | USA | 78 | 44 | 1988–2001 | Retrospective population-based cohort | 5964 | 16,760 | 9.1 Y | OS, DSS | yes | PTC | yes |
| Hassanain 2010 [29] | Canada | 73 | NA | 1982–2002 | Retrospective cohort study | 126 | 54 | 4–25 Y | Recurrence, DFS | yes (28.3%) | PTC, FTC | yes |
| Ito 2010 [17] | Japan | 94 | 51.1 ± 12.4 | 1987–2005 | Retrospective cohort study | 1601 | 1037 | 0.5–34 Y | Recurrence, DSS | yes (0.1%) | PTC | no |
| Barney 2010 [1] | USA | NA | NA | 1983–2002 | Retrospective population-based cohort | 3266 | 12,598 | 2 mo–19.9 Y | OS, DSS | yes | PTC, FTC | yes |
| Vaisman 2011 [42] | USA | 84 | 45 ± 13 | 1986–2005 | Retrospective cohort study | 72 | 217 | 0.5–34 Y | Recurrence, DSS | no | PTC, HCC | no |
| Nixon 2012 [43] | USA | 79 | 46 | 1986–2005 | Retrospective cohort study | 361 | 528 | 13 mo–24.3 Y | Recurrence, OS, DSS | yes | PTC, FTC, HCC | yes |
| Ebina 2014 [18] | Japan | 76 | 54 ± 14 | 1993–2010 | Retrospective cohort study | 791 | 176 | 3–20 Y | Recurrence, DFS, DSS | yes | PTC | yes *** |
| Adam 2014 [44] | USA | 80 | NA | 1998–2011 | Retrospective population-based cohort | 6849 | 54,926 | 5–14.9 Y | OS | yes | PTC | yes |
| Kuba 2017 [45] | Japan | 86 | 53 | 1994–2008 | Retrospective matched cohort study | 120 | 53 | 11 mo–20.8 Y | OS, DFS | yes | PTC | yes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bojoga, A.; Koot, A.; Bonenkamp, J.; de Wilt, J.; IntHout, J.; Stalmeier, P.; Hermens, R.; Smit, J.; Ottevanger, P.; Netea-Maier, R. The Impact of the Extent of Surgery on the Long-Term Outcomes of Patients with Low-Risk Differentiated Non-Medullary Thyroid Cancer: A Systematic Meta-Analysis. J. Clin. Med. 2020, 9, 2316. https://doi.org/10.3390/jcm9072316
Bojoga A, Koot A, Bonenkamp J, de Wilt J, IntHout J, Stalmeier P, Hermens R, Smit J, Ottevanger P, Netea-Maier R. The Impact of the Extent of Surgery on the Long-Term Outcomes of Patients with Low-Risk Differentiated Non-Medullary Thyroid Cancer: A Systematic Meta-Analysis. Journal of Clinical Medicine. 2020; 9(7):2316. https://doi.org/10.3390/jcm9072316
Chicago/Turabian StyleBojoga, Andreea, Anna Koot, Johannes Bonenkamp, Johannes de Wilt, Joanna IntHout, Peep Stalmeier, Rosella Hermens, Johannes Smit, Petronella Ottevanger, and Romana Netea-Maier. 2020. "The Impact of the Extent of Surgery on the Long-Term Outcomes of Patients with Low-Risk Differentiated Non-Medullary Thyroid Cancer: A Systematic Meta-Analysis" Journal of Clinical Medicine 9, no. 7: 2316. https://doi.org/10.3390/jcm9072316