Calcium Orthophosphates as Bioceramics: State of the Art


Kudrinskaja sq. 1-155, Moscow 123242, Russia
J. Funct. Biomater. 2010, 1(1), 22-107; https://doi.org/10.3390/jfb1010022
Submission received: 21 October 2010
/
Revised: 16 November 2010
/
Accepted: 25 November 2010
/
Published: 30 November 2010
(This article belongs to the Special Issue Biomaterials for Bone Substitutes)
Abstract
:In the late 1960s, much interest was raised in regard to biomedical applications of various ceramic materials. A little bit later, such materials were named bioceramics. This review is limited to bioceramics prepared from calcium orthophosphates only, which belong to the categories of bioactive and bioresorbable compounds. There have been a number of important advances in this field during the past 30–40 years. Namely, by structural and compositional control, it became possible to choose whether calcium orthophosphate bioceramics were biologically stable once incorporated within the skeletal structure or whether they were resorbed over time. At the turn of the millennium, a new concept of calcium orthophosphate bioceramics—which is able to promote regeneration of bones—was developed. Presently, calcium orthophosphate bioceramics are available in the form of particulates, blocks, cements, coatings, customized designs for specific applications and as injectable composites in a polymer carrier. Current biomedical applications include artificial replacements for hips, knees, teeth, tendons and ligaments, as well as repair for periodontal disease, maxillofacial reconstruction, augmentation and stabilization of the jawbone, spinal fusion and bone fillers after tumor surgery. Exploratory studies demonstrate potential applications of calcium orthophosphate bioceramics as scaffolds, drug delivery systems, as well as carriers of growth factors, bioactive peptides and/or various types of cells for tissue engineering purposes.
1. Introduction
One of the most exciting and rewarding research areas of material science involves various applications to health care. Examples are sutures, catheters, heart valves, pacemakers, breast implants, fracture fixation plates, nails and screws in orthopedics, dental filling materials, orthodontic wires, as well as total joint replacement prostheses. Furthermore, during recent decades, both an ageing population and a democratization of high-risk sports have led to a surge of bone-related diseases and bone fractures, which must be treated. However, in order to be accepted by the living body, all implantable items must be prepared from a special class of materials, called biomedical materials or biomaterials, in short.
In general, all solids are divided into four major groups of materials: metals, polymers ceramics and composites thereof. Similarly, all biomaterials are also divided into the same major groups: biometals, biopolymers, bioceramics and biocomposites. All of them play very important roles in replacement and regeneration of human tissues. However, due to a great number of publications, this review is limited to bioceramics only. In general, the modern bioceramics comprise various polycrystalline materials, glasses, glass-ceramics, as well as ceramic-filled bioactive composites. All of them might be manufactured in both porous and dense forms in bulk, as well as in the forms of powders, granules and/or coatings. An expansion of bioceramics to health care has been characterized by a significant increase in the number of publications and patents in this field and an ever-increasing number of major international conferences and themed meetings [1,2,3,4,5].
Interestingly, the chemical elements used to manufacture bioceramics form just a small set of the Periodic Table. Namely, bioceramics might be prepared from alumina, zirconia, carbon, silica-contained and calcium-contained compounds, as well as some other chemicals [3]; however, this review is limited to calcium orthophosphates only. Calcium orthophosphate-based biomaterials and bioceramics are now used for a number of different applications throughout the body, covering all areas of the skeleton. Applications include dental implants, percutaneous devices and use in periodontal treatment, healing of bone defects, fracture treatment, total joint replacement (bone augmentation), orthopedics, cranio-maxillofacial reconstruction, otolaryngology and spinal surgery [2,3,4,5,6]. Depending upon the required properties, different calcium orthophosphates might be used. For example, Figure 1 shows some randomly chosen samples of the commercially available calcium orthophosphate bioceramics for bone graft applications.
In this review, the focus has been placed upon applications of calcium orthophosphates as medical implants to repair and reconstruct damaged or diseased hard tissues of the body (usually, those of the musculo-skeletal system, such as bones or teeth) and to describe some of the major developments in this field during the past ~40 years. To narrow the subject further, with a few important exceptions, bioceramics prepared from undoped and un-substituted calcium orthophosphates have been considered and discussed only. Furthermore, calcium orthophosphate bioceramics prepared from biological resources, such as bones, teeth, corals, etc., are not considered either. Readers interested in these topics are advised to read the original papers [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37].
Figure 1.
Several examples of the commercial calcium orthophosphate-based bioceramics.

2. General Knowledge on Biomaterials and Bioceramics
A number of definitions have been developed for the term “biomaterials”. Until recently, the consensus definition developed by the experts in this field has been the following: biomaterials are synthetic or natural materials used to replace parts of a living system or to function in intimate contact with living tissues [38]. However, in September 2009, a more advanced definition was introduced: “A biomaterial is a substance that has been engineered to take a form which, alone or as part of a complex system, is used to direct, by control of interactions with components of living systems, the course of any therapeutic or diagnostic procedure, in human or veterinary medicine” [39]. In any case, biomaterials are intended to interface with biological systems to evaluate, treat, augment or replace any tissue, organ or function of the body and are now used in a number of different applications throughout the body [4,5,40]. The major difference between biomaterials and other classes of materials is the ability of biomaterials to remain in a biological environment without damaging the surroundings and without being damaged themselves in the process. Thus, biomaterials are solely associated with the health care domain and must have an interface with tissues or tissue components. One should stress that any artificial materials that are simply in contact with skin, such as hearing aids and wearable artificial limbs, are not included in the definition of biomaterials since the skin acts as a protective barrier between the body and the external world.
The biomaterials discipline is founded in the knowledge of the synergistic interaction of material science, biological science, chemical science, medical science and mechanical science and requires input and comprehension from all these areas so that implanted biomaterials perform adequately in a living body and interrupt normal body functions as little as possible [41]. As biomaterials mainly deal with all aspects of material synthesis and processing, the knowledge in chemistry, material science and engineering is essential. On the other hand, as clinical applications are the main purposes of biomaterials, biomedical sciences become a key part of the research. These include cell and molecular biology, anatomy and animal and human physiology. The final aim is to achieve the ideal biological interaction of implanted biomaterials with living tissues of a host. In order to achieve these goals, several stages have to be performed, namely: material synthesis, design and manufacturing of prostheses, followed by various types of tests. Furthermore, any potential biomaterial must also pass all regulatory requirements before its clinical application [42].
Biomaterials must be distinguished from biological materials because the former are the materials that are accepted by living tissues and, therefore, they might be used for tissue replacements, while the latter are the materials being produced by various biological systems (wood, cotton, bones, chitin, etc.) [43]. In addition, there are biomimetic materials, which are not made by living organisms but have similar composition, structure and properties to biological materials. Further, bioceramics (or biomedical ceramics) might be defined as biomaterials of the ceramic origin [44]. In general, bioceramics can have structural functions as joint or tissue replacements, can be used as coatings to improve the biocompatibility [45] of metal implants, as well as function as resorbable lattices, providing temporary structures and frameworks those are dissolved and/or replaced as the body rebuilds the damaged tissues [46,47,48,49,50,51]. Some types of bioceramics even feature a drug-delivery capability [52,53].
A progressive deterioration of all tissues with age is the major contributor to the need for spare parts for the body. Bone is especially vulnerable to fracture in older people due to a loss of density and strength with age. This effect is especially severe in women due to the hormonal changes associated with menopause. A graphical representation of the effect of time on bone strength and density from the age of 30 years onward is available in literature [Ref. 48, Figure 1]. Bone density decreases because bone-growing cells (osteoblasts) become progressively less productive in making new bone and repairing micro-fractures. The lower density greatly deteriorates the strength of bones and an unfortunate consequence is that many old people fracture their hips or have collapsed vertebrae and spinal problems [48].
Surface reactivity is one of the common characteristics of bioceramics. It contributes to their bone bonding ability and their enhancing effect on bone tissue formation. During implantation, various reactions occur at the material/tissue interfaces that lead to time-dependent changes in the surface characteristics of the implanted bioceramics and the surrounding tissues [54]. Bioceramics are needed to alleviate pain and restore functions to diseased or damaged calcified tissues (bones and teeth) of the body. A great challenge facing the medical application of bioceramics is to replace old, deteriorating bone with a material that can function the remaining years of the patient’s life and, ideally, be replaced by a new mature bone without transient loss of mechanical support [1]. Because the average life span of humans is now 80+ years and the major need for spare parts begins at about 60 years of age, the implanted non-resorbable bioceramics need to last, at least, for 20+ years. This demanding requirement of survivability is under conditions of use that are especially harsh to implanted materials: corrosive saline solutions at 37 °C under variable, multiaxial and cyclical mechanical loads. The excellent performance of the specially designed bioceramics that have survived these clinical conditions represents one of the most remarkable accomplishments of research, development, production and quality assurance during the past century [48].

| Ca/P molar ratio | Compound | Formula | Solubility at 25 °C, −log(Ks) | Solubility at 25 °C, g/L | pH stability range in aqueous solutions at 25 °C |
|---|---|---|---|---|---|
| 0.5 | Monocalcium phosphate monohydrate (MCPM) | Ca(H2PO4)2·H2O | 1.14 | ~18 | 0.0–2.0 |
| 0.5 | Monocalcium phosphate anhydrous (MCPA) | Ca(H2PO4)2 | 1.14 | ~17 | [c] |
| 1.0 | Dicalcium phosphate dihydrate (DCPD), mineral brushite | CaHPO4·2H2O | 6.59 | ~0.088 | 2.0–6.0 |
| 1.0 | Dicalcium phosphate anhydrous (DCPA), mineral monetite | CaHPO4 | 6.90 | ~0.048 | [c] |
| 1.33 | Octacalcium phosphate (OCP) | Ca8(HPO4)2(PO4)4·5H2O | 96.6 | ~0.0081 | 5.5–7.0 |
| 1.5 | α-Tricalcium phosphate (α-TCP) | α-Ca3(PO4)2 | 25.5 | ~0.0025 | [a] |
| 1.5 | β-Tricalcium phosphate (β-TCP) | β-Ca3(PO4)2 | 28.9 | ~0.0005 | [a] |
| 1.0–2.2 | Amorphous calcium phosphate (ACP) | CaxHy(PO4)z·nH2O, n = 3–4.5; 15–20% H2O | [b] | [b] | ~5–12 [d] |
| 1.5–1.67 | Calcium-deficient hydroxyapatite (CDHA)[e] | Ca10-x(HPO4)x(PO4)6-x(OH)2-x[f] (0 < x < 1) | ~85.1 | ~0.0094 | 6.5–9.5 |
| 1.67 | Hydroxyapatite (HA, HAp or OHAp) | Ca10(PO4)6(OH)2 | 116.8 | ~0.0003 | 9.5–12 |
| 1.67 | Fluorapatite (FA or FAp) | Ca10(PO4)6F2 | 120.0 | ~0.0002 | 7–12 |
| 1.67 | Oxyapatite (OA or OAp) | Ca10(PO4)6O | ~69 | ~0.087 | [a] |
| 2.0 | Tetracalcium phosphate (TTCP or TetCP), mineral hilgenstockite | Ca4(PO4)2O | 38–44 | ~0.0007 | [a] |
[a] These compounds cannot be precipitated from aqueous solutions.[b] Cannot be measured precisely. However, the following values were found: 25.7 ± 0.1 (pH = 7.40), 29.9 ± 0.1 (pH = 6.00), 32.7 ± 0.1 (pH = 5.28). The comparative extent of dissolution in acidic buffer is: ACP >> α-TCP >> β-TCP > CDHA >> HA > FA.[c] Stable at temperatures above 100 °C.[d] Always metastable.[e] Occasionally CDHA is named as precipitated HA.[f] In the case x = 1 (the boundary condition with Ca/P = 1.5), the chemical formula of CDHA looks as follows: Ca9(HPO4)(PO4)5(OH).
3. General Knowledge on Calcium Orthophosphates
The main driving force behind the use of calcium orthophosphates as bone substitute materials is their chemical similarity to the mineral component of mammalian bones and teeth [55,56,57,58]. As a result, in addition to being non-toxic, they are biocompatible, not recognized as foreign materials in the body and, most importantly, exhibit both bioactive behavior [59] and integrate into living tissue by the same processes active in remodeling healthy bone. This leads to an intimate physicochemical bond between the implants and bones, termed osteointegration [60]. More to the point, calcium orthophosphates are also known to be osteoconductive (able to provide a scaffold or template for new bone formation) and support osteoblast adhesion and proliferation [61,62]. Even so, the major limitations to use calcium orthophosphates as load-bearing bioceramics are their mechanical properties; namely, they are brittle with a poor fatigue resistance [46,47,48,63]. The poor mechanical behavior is even more evident for highly porous bioceramics and scaffolds because porosity greater than ~100 µm is considered as the requirement for proper vascularization and bone cell colonization [64,65,66]. Thus, for biomedical applications, calcium orthophosphates are used primarily as fillers and coatings, rendering it impossible to use them for repair of large osseous defects [57,58].
The complete list of known calcium orthophosphates, including their standard abbreviations and the major properties, is given in Table 1, while detailed information on their synthesis, structure, chemistry, other properties and biomedical application has been comprehensively reviewed recently [57,58]; interested readers are referred here. Additional thorough information on various calcium orthophosphates can be found in books and monographs [67,68,69,70,71,72,73,74,75]. One should note that among the existing calcium orthophosphates (Table 1), only certain compounds are useful for biomedical applications, because those having a Ca/P ionic ratio less than 1 are not suitable for implantation due to their high solubility and acidity. Due to its basicity, TTCP is not suitable either. However, to be used in medicine, the “unsuitable” calcium orthophosphates might successfully be combined with either other calcium orthophosphates or other chemicals.
4. Bioceramics of Calcium Orthophosphates
4.1. History
The performance of living tissues is the result of millions of years of evolution, while the performance of acceptable artificial substitutions that humankind has designed to repair damaged tissues are only a few decades old. However, attempts to repair the human body with the use of implant materials are recorded in the early medical writings of the Hindu, Egyptian and Greek civilizations. The earliest successful implants were in the skeletal system. Historically, selection of the materials was based on their availability and an ingenuity of the individual making and applying the prosthetic [76]. Archaeological findings exhibited in museums showed that materials used to replace missing human bones and teeth included animal or human (from corpses) bones and teeth, shells, corals, ivory (elephant tusk), wood, as well as some metals (gold or silver). For instance, the Etruscans learned to substitute missing teeth with bridges made from artificial teeth carved from the bones of oxen, while in ancient Phoenicia loose teeth were bound together with gold wires, tying artificial ones to neighboring teeth. In the 17th century, a piece of dog skull was successfully transplanted into the damaged skull of a Dutch duke. The Chinese recorded the first use of dental amalgam to repair decayed teeth in the year 659 AD, while pre-Columbian civilizations used gold sheets to heal cranial cavities following trepanation [77]. Furthermore, in 1970, Amadeo Bobbio discovered Mayan skulls, some of then more than ~4000 years old, in which missing teeth had been replaced by nacre substitutes [78]. Unfortunately, due to the practice of cremation in many societies, little is known about prehistoric materials used to replace bone lost to accident or disease.
The first widely tested artificial bioceramic was plaster of Paris. However, in the past, many implantations failed due to infections, which tended to be exacerbated in the presence of implants, since they provided a region inaccessible to the body’s immunologically competent cells. Thus, the use of biomaterials did not become practical until the advent of an aseptic surgical technique developed by J. Lister in the 1860s. Furthermore, there was a lack of knowledge about the toxicity of selected materials. In this frame, application of calcium orthophosphates appears to be logical due to their similarity with the mineral phases of bones and teeth [55,56,69,79,80]. Calcium orthophosphates are not toxic and do not cause cell death in the surrounding tissues. However, according to available literature, the first attempt to use them (it was TCP) as an artificial material to repair surgically created defects in rabbits was performed in 1920 [81]. Although this may be the first scientific study on use of a calcium orthophosphate for bone defects repair, it remains unclear whether the calcium orthophosphate was a precipitated or a ceramic material and whether it was in a powder or granular form. The second clinical report was published 30 years later [82]. More than 20 years afterwards, the first dental application of a calcium orthophosphate (erroneously described as TCP) in surgically created periodontal defects [83] and the use of dense HA cylinders for immediate tooth root replacement [84] were reported. According to the available databases, the first paper with the term “bioceramics” in the abstract was published in 1971 [85], and with the term in the title in 1972 [86,87]. However, application of the ceramic materials as prostheses had been known before [88,89,90,91]. Further historical details might be found in literature [92,93]. On April 26, 1988, the first international symposium on bioceramics was held in Kyoto, Japan.
Commercialization of the dental and surgical applications of calcium orthophosphate (mainly, HA) bioceramics occurred in the 1980s, largely due to the pioneering efforts by Jarcho [94,95,96,97] in the USA, De Groot [67,98,99] in Europe and Aoki [100,101,102,103] in Japan. Shortly afterwards, HA became a bioceramic of reference in the field of calcium orthophosphates for biomedical applications. Preparation and biomedical applications of apatites derived from sea corals (coralline HA) [104,105,106] and bovine bone [107] were reported at the same time [108].
4.2. Chemical Composition and Preparation
Currently, calcium orthophosphate bioceramics can be prepared from various sources [109,110,111,112,113,114,115,116]. Unfortunately, up until now, all attempts to synthesize bone replacement materials for clinical applications featuring physiological tolerance, biocompatibility and a long-term stability have had only relative success; showing the superiority and a complexity of the natural structures [117].
In general, calcium orthophosphate bioceramics should be characterized from many viewpoints such as the chemical composition (stoichiometry and purity), homogeneity, phase distribution, morphology, grain sizes and shape, grain boundaries, crystallite size, crystallinity, pores, cracks, surface, etc. From the chemical point of view, the vast majority of calcium orthophosphate bioceramics is based on HA, β-TCP, α-TCP and/or biphasic calcium phosphate (BCP, which is an intimate mixture of either β-TCP + HA [118,119,120,121,122,123,124,125,126,127,128,129,130] or α-TCP + HA [7,8,9,10,11]) [131,132,133,134,135,136,137,138,139]. One should note that recently the concept of BCP has been extended by preparation and characterization of biphasic TCP, consisting of α-TCP and β-TCP phases [140,141,142,143,144]. The biphasic TCP is usually prepared by heating ACP precursors [142,143,144], in which the α-TCP/β-TCP ratio can be controlled by aging time and pH value during synthesis of the amorphous precursor [143]. Furthermore, very recently, a triphasic formulation, consisting of HA, α-TCP and β-TCP has been prepared [145]. The preparation techniques of various calcium orthophosphates have been extensively reviewed in literature [57,58,67,68,69,70,71,72,73,74,75] and references therein. When compared to both α- and β-TCP, HA is a more stable phase under the physiological conditions, as it has a lower solubility (Table 1) and, thus, a slower resorption kinetics [69,131,132]. Therefore, the BCP concept is determined by the optimum balance of a more stable phase of HA and a more soluble TCP. Due to a higher biodegradability of the α- or β-TCP component, the reactivity of BCP increases with increasing TCP/HA ratio. Thus, in vivo bioresorbability of BCP can be controlled through the phase composition [127]. Similar conclusions are also valid for both the biphasic TCP (in which α-TCP is a more soluble phase) and the triphasic (HA, α-TCP and β-TCP) formulation.
As implants made of calcined HA are found in bone defects for many years after implantation, bioceramics made of more soluble calcium orthophosphates [7,8,9,10,11,118,119,120,121,122,123,124,125,126,127,128,129,130,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147] are preferable for biomedical purposes. Furthermore, experimental results showed that BCP had a higher ability to adsorb fibrinogen, insulin or type I collagen than HA [148]. Thus, according to both observed and measured bone formation parameters, calcium orthophosphates have been ranked as follows: low sintering temperature BCP (rough and smooth) ≈medium sintering temperature BCP ≈ TCP > calcined low sintering temperature HA > non-calcined low sintering temperature HA > high sintering temperature BCP (rough and smooth) > high sintering temperature HA (calcined and non-calcined) [149]. This sequence was developed in 2000 and, thus, neither biphasic TCP, nor triphasic (HA, α-TCP and β-TCP) formulation have been included. Recent developments in processing and surface modification of HA have been reviewed elsewhere [150].
4.3. Forming and Shaping
In order to fabricate bioceramics in more and more complex shapes, scientists are investigating the use of old and new manufacturing techniques. These techniques range from an adaptation of age-old pottery techniques to the latest manufacturing methods for high-temperature ceramic parts for airplane engines. For example, reverse engineering and rapid prototyping technologies have revolutionized a generation of physical models, allowing an engineer to efficiently and accurately produce physical models and customized implants with high levels of geometric intricacy [151,152,153]. Combined with the computer-aided design and manufacturing (CAD/CAM), complex physical objects of the anatomical structure can be fabricated in a variety of sizes. In a typical application, an image of a bone defect in a patient can be taken and used to develop a three-dimensional (3D) CAD computer model [154,155,156]. A computer can then reduce the model to slices or layers. The 3D objects are constructed layer-by-layer using rapid prototyping techniques such as fused deposition modeling [157,158], selective laser sintering [159,160,161], 3D printing [162,163,164,165,166,167,168,169,170] or stereo lithography [171,172,173,174]. A custom-made implant of actual dimensions would reduce the time it takes to perform the medical implantation procedure and subsequently lower the risk to the patient. Another advantage of a prefabricated, exact-fitting implant is that it can be used more effectively and applied directly to the damaged site rather than a replacement that is formulated during surgery from a paste or granular material [175,176,177]. In some cases, laser processing can be applied as well [178].
The manufacturing technique depends greatly on the ultimate application of the bioceramic device, whether it is for a hard-tissue replacement or integration of the device within the surrounding tissues. In general, three types of processing technologies are used: (1) employment of a lubricant and a liquid binder with ceramic powders for shaping and subsequent firing; (2) application of self-setting and self-hardening properties of water-wet molded powders (cementation); (3) melting of materials to form a liquid and shaping during cooling and solidification [179,180,181,182]. Since calcium orthophosphates are either thermally unstable (MCPM, MCPA, DCPA, DCPD, OCP, ACP, CDHA) or have a melting point at temperatures exceeding ~1400 °C (α-TCP, β-TCP, HA, FA, TTCP), only the first and second consolidation approaches are used to prepare bulk bioceramics and scaffolds. The methods include uniaxial compaction [183,184], isostatic pressing (cold or hot) [185,186,187,188,189,190,191], granulation [192], loose packing [193], slip casting [194,195,196], gel casting [173,174,197,198,199,200,201,202], pressure mold forming [203], injection molding [204], polymer replication [205,206,207,208], extrusion [209,210,211], slurry dipping and spraying [212]. In addition, formation of ceramic sheets from slurries tape casting [130,199,213,214], doctor blade [215] and colander methods might be employed [63,179,180,181,182]. Furthermore, some of these processes might be performed under the magnetic field, which helps crystal aligning [216,217,218,219].
Powders are usually pressed damp in metal dies or dry in lubricated dies at pressures high enough to form sufficiently strong structures to hold together until they are sintered. An organic binder such as polyvinyl alcohol helps to bind the powder together [185]. Drying at about 100 °C is a critical step in preparing damp-formed pieces for firing. Too much or too little water in the compacts can lead to blowing apart the ware on heating or crumbling, respectively. The binder is removed by heating in air to oxidize the organic phases to carbon dioxide and water [179,180,181,182].
Furthermore, forming and shaping of any ceramic products require a proper selection of the raw materials in terms of particle sizes and size distribution. Namely, tough and strong bioceramics consist of pure, fine and homogeneous microstructures. To attain this, pure powders with small average size and high surface area must be used as the starting sources. However, for maximum packing and least shrinkage after firing, mixing of ~70% coarse and ~30% fine powders have been suggested [182]. Mixing is usually carried out in a ball mill for uniformity of properties and reaction during subsequent firing. Mechanical die forming, or sometimes extrusion through a die orifice, can be used to produce a fixed cross-section. Drying involves removal of water and subsequent shrinkage of the product. However, due to local variations in water content, warping and even cracks may be developed during drying. Dry pressing and hydrostatic molding can minimize these problems [182]. Afterwards, the manufactured green samples are sintered.
Finally, to produce the accurate shaping, necessary for the fine design of bioceramics, machine finishing might be essential [156,179,220]. Unfortunately, cutting tools developed for metals are usually useless for bioceramics due to their fragility; therefore, grinding and polishing appear to be the convenient finishing techniques [156,179]. Furthermore, the surface of bioceramics might be modified by various additional treatments [221].
4.4. Sintering and Firing
A sintering (or firing) procedure appears to be of a great importance to manufacture bulk bioceramics with the required properties. Usually, this stage is carried out according to controlled temperature programs of electric furnaces in adjusted ambience of air with necessary additional gasses; however, always at temperatures below the melting points of the materials. The firing step can include temporary holds at intermediate temperatures to burn out organic binders [179,180,181,182]. The heating rate, sintering temperature and holding time depend on the starting materials. For example, in the case of HA, these values are in the ranges of 0.5–3 °C/min, 1000–1250 °C and 2–5 h, respectively [222]. In the majority cases, sintering allows a structure to retain its shape. However, this process might be accompanied by a considerable degree of shrinkage [107], which must be accommodated in the fabrication process. The sintering mechanism is controlled by both surface and volume diffusion at grain boundaries. In general, when solids heat to high temperatures, the constituent ions or atoms are driven to move to fill up pores and open channels between the grains of powders, as well as to compensate for the surface energy differences among their convex and concave surfaces. At the initial stages, bottlenecks are formed and grow among the particles (Figure 2). Existing vacancies tend to flow away from the surfaces of sharply curved necks; this is an equivalent of a material flow towards the necks, which grow as the voids shrink. Small contact areas among the particles expand and, at the same time, a density of the compact increases and the total void volume decreases. As the pores and open channels are closed during a heat treatment, the particles become tightly bonded together and density, strength and fatigue resistance of the sintered object improve greatly. Grain-boundary diffusion was identified as the dominant mechanism for densification [223]. Furthermore, strong chemical bonds form among the particles and loosely compacted green bodies are hardened to denser materials [179,180,181,182].
Figure 2.
A schematic diagram representing the changes occurring with particles under sintering.

In the case of calcium orthophosphates, several specific processes occur during sintering. Firstly, moisture, carbonates and all other volatile chemicals remaining from the synthesis stage, such as ammonia, nitrates and any organic compounds, are removed as gaseous products. Secondly, unless powders are sintered, the removal of these gases facilitates production of denser ceramics with subsequent shrinkage of the samples (Figure 3). Thirdly, all chemical changes are accompanied by a concurrent increase in crystal size and a decrease in the specific surface area. Fourthly, a chemical decomposition of all acidic orthophosphates and their transformation into other phosphates (e.g., 2HPO42− → P2O74− + H2O↑) takes place.
Figure 3.
Linear shrinkage of the compacted ACP powders that were converted into β-TCP, BCP (50% HA + 50% β-TCP) and HA upon heating. According to the authors: “At 1300 °C, the shrinkage reached a maximum of approximately ~25, ~30 and ~35% for the compacted ACP powders that converted into HA, BCP 50/50 and β-TCP, respectively” [224]. Reprinted from [224] with permission.
Figure 3.
Linear shrinkage of the compacted ACP powders that were converted into β-TCP, BCP (50% HA + 50% β-TCP) and HA upon heating. According to the authors: “At 1300 °C, the shrinkage reached a maximum of approximately ~25, ~30 and ~35% for the compacted ACP powders that converted into HA, BCP 50/50 and β-TCP, respectively” [224]. Reprinted from [224] with permission.

In addition, sintering causes toughening [225], densification [226], as well as increasing the mechanical strength [227,228]. The latter events are due to presence of air and other gases filling gaps among the unsintered powders. At sintering, the gases move towards the outside of powders and green bodies shrink owing to decrease of distances among powders. However, in the case of FA sintering, a linear shrinkage was found to occur at ~715 °C and the material reached its final density at ~890 °C. Above this value, grain growth became important and induced an intra-granular porosity, which was responsible for density decrease. At ~1180 °C, a liquid phase forms due to formation of a binary eutectic between FA and fluorite contained in the powder as impurity. This liquid phase further promoted the coarsening process and induced formation of large pores at high temperatures [229]. Sintering of a biologically formed apatite has been investigated [230,231] as well, and the obtained products have been characterized [232,233]. In all cases, the numerical value of the Ca/P ratio in sintered apatites of biological origin was higher than that of the stoichiometric HA. One should mention that in the vast majority of cases, calcium orthophosphates with Ca/P ratio < 1.5 (Table 1) are not sintered, since these compounds are thermally unstable, while sintering of CDHA and ACP leads to their transformation into BCP (HA + β-TCP [234] or HA + α-TCP [235]).
An extensive study on the effects of sintering temperature and time on the properties of HA bioceramics revealed a correlation between these parameters and density, porosity, grain size, chemical composition and strength of the scaffolds [236]. Namely, sintering below ~1000 °C was found to result in initial particle coalescence, with little or no densification and a significant loss of the surface area and porosity. The degree of densification appeared to depend on the sintering temperature, whereas the degree of ionic diffusion was governed by the period of sintering [236]. Furthermore, various sintering additives might be added to calcium orthophosphate bioceramics to enhance sinterability [237,238,239,240]. Unexpectedly, a magnetic field during sintering was found to influence the growth of HA grains [241].
HA powders can be pressurelessly sintered up to the theoretical density at 1000–1200 °C. Processing at higher temperatures may lead to exaggerated grain growth and decomposition because HA becomes unstable at temperatures exceeding ~1300 °C [67,68,69,70,71,72,73,74,75,242]. The decomposition temperature of HA bioceramics is a function of the partial pressure of water vapor. Moreover, processing under vacuum leads to an earlier decomposition of HA, while processing under high partial pressure of water prevents the decomposition. On the other hand, the presence of water in the sintering atmosphere was reported to inhibit densification of HA and accelerate grain growth [63,243]. A definite correlation between hardness, density and grain size in sintered HA bioceramics was found: despite exhibiting high bulk density, hardness started to decrease at a certain critical grain size limit [244,245].
Hot pressing [245,246,247,248,249,250,251], hot isostatic pressing (HIP) [189,190] or hot pressing with post-sintering [252,253] processes make it possible to decrease the temperature of the densification process, diminish the grain size, as well as achieve higher densities. This leads to finer microstructures, higher thermal stability of calcium orthophosphates and subsequently better mechanical properties of bulk bioceramics. Microwave [254,255,256,257,258,259,260,261] and spark plasma [262,263,264,265,266,267,268,269,270] sintering techniques are alternative methods to the conventional sintering, hot pressing and HIP. Both techniques were found to be time and energy efficient densification methods. Recently, a hydrothermal hot pressing method was developed to fabricate OCP bioceramics without thermal dehydration and/or thermal decomposition [271]. Further details on the sintering and firing processes of calcium orthophosphate bioceramics are available in literature [47,63,69,70,272,273].
To conclude this part, one should mention an excellent recent review on various ceramic manufacturing techniques [274], to which interested readers are referred to extend their knowledge on ceramic processing.
5. The Major Properties
5.1. Mechanical Properties
Ideally, a bone substitute should be replaced by a mature bone without transient loss of mechanical support. Unfortunately for material scientists, a human body provides one of the most inhospitable environments for implanted materials. It is warm, wet and both chemically and biologically active. Furthermore, the body is capable of generating quite massive force concentrations and the variance in such characteristics among individuals might be enormous. Therefore, all types of potential biomaterials and bioceramics must sustain attacks of a great variety of aggressive conditions. Regrettably, there is presently no material fulfilling all these requirements.
On the other hand, any ceramics, when they fail, tend to do so in a dramatic manner. Namely, the brittle nature of calcium orthophosphate bioceramics is attributed to high strength ionic bonds. Thus, it is not possible for plastic deformation to happen prior to failure, as a slip cannot occur. Consequently, if a crack is initiated, its progress will not be hindered by the deformation of material ahead of the crack, as would be the case in a ductile material (e.g., a metal). The crack will continue to propagate, rapidly resulting in a catastrophic failure [180].
Accordingly, from the mechanical point of view, calcium orthophosphate bioceramics appear to be brittle polycrystalline materials for which the mechanical properties are governed by crystallinity, grain size, grain boundaries, porosity and composition [188]. It appears to be very sensitive to slow crack growth [275]. For dense bioceramics, the strength is a function of the grain size. Finer grain size materials have smaller flaws at the grain boundaries and thus are stronger than bioceramics with larger grain sizes. In general, the mechanical properties decrease significantly with increasing content of an amorphous phase, microporosity and grain size, while a high crystallinity, a low porosity and small grain size tend to give a higher stiffness, a higher compressive and tensile strength and a greater fracture toughness. Thus, calcium orthophosphate bioceramics possess poor mechanical properties (for instance, a low impact and fracture resistances) that do not allow use in load-bearing areas, such as artificial teeth or bones [46,47,48,49,50,51,52,276]. For example, fracture toughness [277] of HA bioceramics does not exceed ~1.2 MPa·m1/2 [278] (human bone: 2–12 MPa·m1/2). It decreases almost linearly with increasing porosity [63]. Generally, fracture toughness increases with decreasing grain size. However, in some materials, especially non-cubic ceramics, fracture toughness reaches the maximum and rapidly drops with decreasing grain size. For example, Halouani et al. investigated fracture toughness of pure hot pressed HA with grain sizes of 0.2–1.2 µm [251]. There appeared to be two distinct trends, where fracture toughness decreased with increasing grain size above ~0.4 µm and subsequently decreased with decreasing grain size. The maximum fracture toughness measured was 1.20 ± 0.05 MPa·m1/2 at ~0.4 µm [251]. Fracture energy of HA bioceramics is in the range of 2.3–20 J/m2, while the Weibull modulus [279] is low (~5–12) in wet environments, which means that HA behaves as a typical brittle ceramics and indicates low reliability of HA implants [63]. Interestingly, three peaks of internal friction were found at temperatures about −40, 80 and 130 °C for HA but no internal friction peaks were obtained for FA in the measured temperature range; this effect was attributed to the differences of the positions of F- and OH- in FA and HA, respectively [280].
Bending, compressive and tensile strengths of dense HA bioceramics are in the range of 38–250 MPa, 120–900 MPa and 38–300 MPa, respectively. Similar values for porous HA bioceramics are in the range of 2–11 MPa, 2–100 MPa and ~3 MPa, respectively [63]. These wide variations in the properties are due to both structural variations (e.g., an influence of remaining microporosity, grain sizes, presence of impurities, etc.) and manufacturing processes, as well as caused by a statistical nature of the strength distribution. Strength [281] was found to increase with increasing Ca/P ratio, reaching a maximum value around Ca/P ~1.67 (stoichiometric HA) and to decrease suddenly when Ca/P > 1.67 [63]. Furthermore, strength decreases almost exponentially with increasing porosity [119,120]. However, by changing the pore geometry, it is possible to influence the strength of porous bioceramics. It is also worth mentioning that porous HA bioceramics are considerably less fatigue [282] resistant than dense ones. Both grain sizes and porosity are reported to influence the fracture path, which itself has little effect on the fracture toughness of calcium orthophosphate bioceramics [188,283]. Furthermore, no obvious decrease in mechanical properties was found after calcium orthophosphate bioceramics had been aged in various solutions for different time periods [284].
Young’s (or elastic) modulus [285] of dense HA bioceramics is in the range of 35–120 GPa, which is more or less similar to those of the most resistant components of the natural calcified tissues (dental enamel: ~74 GPa, dentine: ~21 GPa, compact bone: ~18–22 GPa). Nevertheless, dense bulk compacts of HA have mechanical resistances of the order of 100 MPa versus ~300 MPa of human bones, diminishing drastically their resistance in the case of porous bulk compacts [286]. Young’s modulus measured in bending is between 44 and 88 GPa. Recently, a considerable anisotropy in the stress-strain behavior of the perfect HA crystals was found by ab initio calculations [287]. The crystals appeared to be brittle for tension along the z-axis with the maximum stress of ~9.6 GPa at 10% strain. Furthermore, the structural analysis of the HA crystal under various stages of tensile strain revealed that the deformation behavior manifested itself mainly in the rotation of PO4 tetrahedrons with concomitant movements of both the columnar and axial Ca ions [287]. Vickers hardness [288] of dense HA bioceramics is within 3–7 GPa, while the Poisson’s ratio [289] for the synthetic HA is about 0.27, which is close to that of bones (~0.3). At temperatures within 1000–1100 °C, dense HA bioceramics were found to exhibit superplasticity with a deformation mechanism based on grain boundary sliding. Furthermore, both the wear resistance and friction coefficient of dense HA bioceramics are comparable to those of dental enamel [63].
Due to high brittleness (associated to a low crack resistance), biomedical applications of calcium orthophosphate bioceramics are focused on production of non-load-bearing implants, such as pieces for middle ear surgery, filling of bone defects in oral or orthopedic surgery, as well as coating of dental implants and metallic prosthesis (see below) [117,290,291]. In order to improve the reliability of calcium orthophosphate bioceramics, diverse reinforcements (ceramics, metals or polymers) have been applied to manufacture various biocomposites and hybrid biomaterials [292], but that is another story. However, successful hybrid formulations consisting of calcium orthophosphates only should be mentioned [293,294,295,296,297,298]. For example, bulk HA bioceramics might be reinforced by HA whiskers [294,295,296,297]. Furthermore, a superior superplasticity of HA/β-TCP composites (i.e., BCP) to HA bioceramics has been detected [298].
Another approach to improve the mechanical properties of calcium orthophosphate bioceramics is to coat the items by a polymeric layer [299,300]; however, this is still other story. Interested readers are referred to further details on the mechanical properties of calcium orthophosphate bioceramics available elsewhere [63,301].
5.2. Electrical Properties
Occasionally, interest is expressed in the electrical properties of calcium orthophosphate bioceramics. For example, a surface ionic conductivity of both porous and dense HA bioceramics was examined for humidity sensor applications, since the room temperature conductivity was influenced by relative humidity [302]. Namely, the ionic conductivity of HA has been a subject of research for its possible use as an alcohol [303], carbon dioxide [303] or carbon monoxide [304] gas sensors. Electrical measurements have also been used as a characterization tool to study the evolution of microstructure in HA bioceramics [305]. More to the point, Valdes et al. examined the dielectric properties of HA to understand its decomposition to β-TCP [306]. In the case of CDHA, the electrical properties, in terms of ionic conductivity, were found to increase after compression of the samples at 15 t/cm2, which was attributed to establishment of some order within the apatitic network [307]. The conductivity mechanism of CDHA appeared to be multiple [308]. Furthermore, there is an attempt to develop CDHA whisker electrets for biomedical utilization [309].
Interestingly, the electrical properties of calcium orthophosphate bioceramics appear to influence their biomedical applications. For example, there is an interest in polarization of HA bioceramics to generate a surface charge by the application of electric fields at elevated temperatures [310,311]. The presence of surface charges on HA bioceramics was shown to have a significant effect on both in vitro and in vivo crystallization of biological apatite [312,313,314,315,316]. Furthermore, growth of both biomimetic calcium orthophosphates and bones was found to be accelerated on negatively charged surfaces and decelerated on positively charged surfaces [316,317,318,319,320,321,322,323,324,325]. In addition, the electrical polarization of HA bioceramics was found to accelerate a cytoskeleton reorganization of osteoblast-like cells [326,327,328], extend bioactivity [329] and enhance bone ingrowth through the pores of porous HA implants [330]. There is an interesting study on the interaction of a blood coagulation factor on electrically polarized HA surfaces [331]. Further details on the electrical properties of calcium orthophosphate-based bioceramics can be found in [258,332,333,334,335,336].
5.3. Possible Transparency
Single crystals of all calcium orthophosphates are optically transparent for visible light. As bioceramics of calcium orthophosphates have a polycrystalline nature with a random orientation of big amounts of small crystals they are opaque and of white color, unless colored dopants have been added. However, in some cases, transparency is convenient to provide some essential advantages (e.g., to enable direct viewing of living cells in a transmitted light). Thus, transparent calcium orthophosphate bioceramics have been prepared and investigated [189,191,267,270,337,338,339,340,341,342,343,344]. The preparation techniques, for example, include hot isostatic pressing [189,191], ambient-pressure sintering [337], gel casting coupled with a low-temperature sintering [340,343], pulse electric current sintering [341], as well as spark plasma sintering [267,270]. Fully dense, transparent calcium orthophosphate bioceramics were obtained at temperatures above ~800 °C. Depending on the preparation technique, the transparent calcium orthophosphate bioceramics have a uniform grain size ranging from ~0.2 μm [337] to ~250 μm [340] and are always pore-free; the latter is not good for biomedical applications.
5.4. Porosity
Porosity is defined as the percentage of void spaces in solids and it is a morphological property independent of the material. The surface area of porous bodies is much higher, which guarantees a good mechanical fixation in addition to providing sites on the surface that allow chemical bonding between the bioceramics and bones [345]. Furthermore, a porous material may have both closed (isolated) pores and open (connected) pores. Connected pores look like tunnels and are accessible by gases, liquids and particulate suspensions [346]. The open-cell nature of reticulated materials is a unique characteristic essential in many applications. Furthermore, dimensions of open pores are directly related to bone formation, since such pores grant both the surface and space for cell adhesion and bone ingrowth. On the other hand, pore interconnection provides the way for cell distribution and migration, as well as allowing efficient in vivo blood vessel formation suitable for sustaining bone tissue neo-formation and possibly remodeling [64,65,66,122,347,348,349,350,351,352,66,122,347]. Namely, porous HA bioceramics can be colonized by bone tissues [349,353,354,355,356,357,358,359,360,361,362,363]. Therefore, interconnecting macroporosity (pore size >100 μm) [118,345,349,364,365], which is defined by its capacity to be colonized by cells, is intentionally introduced in solid bioceramics (Figure 4). Macroporosity is usually formed due to a release of various volatile materials and, for that reason, incorporation of pore-creating additives (porogens) is the most popular technique to create macroporosity. The porogens are crystals or particles of either volatile (they evolve gases at elevated temperatures) or soluble substances, such as paraffin, naphthalene, sucrose, NaHCO3, gelatin, polymethylmethacrylate or even hydrogen peroxide [119,272,366,367,368,369,370,371,372,373]. Obviously, the ideal porogen should be nontoxic and be removed at ambient temperature, thereby allowing the ceramic/porogen mixture to be injected directly into a defect site and allowing the scaffold to fit the defect [374]. Sintering particles, preferably spheres of equal size, is a similar way to generate porous 3D bioceramics of calcium orthophosphates (Figure 5). However, pores resulting from this method are often irregular in size and shape and not fully interconnected with one another.
Figure 4.
Photographs of a commercially available porous calcium orthophosphate bioceramic with different porosity. Horizontal field width is 20 mm.
Figure 4.
Photographs of a commercially available porous calcium orthophosphate bioceramic with different porosity. Horizontal field width is 20 mm.

Several other techniques, such as replication of polymer foams by impregnation, dual-phase mixing, particulate leaching, freeze casting, slip casting, stereo lithography and foaming of gel casting suspensions, have been applied to fabricate porous calcium orthophosphate bioceramics [64,65,66,104,180,196,199,202,205,206,207,246,247,364,365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400,401,402,403,404,405,406,407,408]. Some are summarized in Table 2 [374]. Furthermore, natural porous materials, like coral skeletons made of CaCO3, can be converted into porous HA under hydrothermal conditions (250 °C, 24–48 h) with the microstructure undamaged [104,105,106]. Porous HA bioceramics can also be obtained by hydrothermal hot pressing. This technique allows solidification of the HA powder at 100–300 °C (30 MPa, 2 h) [381]. In another approach, bi-continuous water-filled microemulsions have been used as pre-organized systems for the fabrication of needle-like frameworks of crystalline HA (2 °C, three weeks) [382,383]. Porous HA bioceramics might be prepared by a combination of gel casting and foam burn out methods [202]. Lithography was used to print a polymeric material, followed by packing with HA and sintering [384]. A hot pressing technique can be applied as well [246,247]. In addition, an HA suspension can be cast into a porous CaCO3 skeleton, which is then dissolved, leaving a porous network [376]. 3D periodic macroporous frame of HA has been fabricated via a template-assisted colloidal processing technique [385]. Furthermore, porous HA bioceramics might be prepared by using different starting HA powders and sintering at various temperatures by pressureless-sintering method [391].
Figure 5.
β-TCP porous ceramics with different pore sizes prepared using polymethylmethacrylate balls with the diameters: (a) 100–200; (b) 300–400; (c) 500–600 and (d) 700–800 μm. Horizontal field width is 45 mm. Reprinted from [377] with permission.
Figure 5.
β-TCP porous ceramics with different pore sizes prepared using polymethylmethacrylate balls with the diameters: (a) 100–200; (b) 300–400; (c) 500–600 and (d) 700–800 μm. Horizontal field width is 45 mm. Reprinted from [377] with permission.

Table 2.
The procedures used to manufacture porous calcium orthophosphate scaffolds for tissue engineering [374].
| Year | Who and where | Process | Calcium orthophosphate | Sintering | Compressive strength | Pore sizes | Porosity |
|---|---|---|---|---|---|---|---|
| 2006 | Deville et al. Berkeley, CA | HA + ammonium methacrylate in PTFE mold, freeze dried and sintered. | HA | Yes: 1300 °C | 16 MPa, 65 MPa, 145 MPa | open unidirectional 50–150 μm | >60%, 56%, 47% |
| 2006 | Saiz et al. Berkeley, CA | Polymer foams coated, compressed after infiltration, then calcined. | HA powder | Yes: 700–1300 °C | – | 100–200 μm | – |
| 2006 | Murugan et al. Singapore + USA | Bovine bone cleaned, calcined. | Bovine bone | Yes: 500 °C | – | retention of nanopores | – |
| 2006 | Xu et al. Gaithersburg, MD | Directly injectable calcium orthophosphate cement, self hardens, mannitol as porogen. | Nanocrystalline HA | No | 2.2–4.2 MPa (flexural) | 0–50% macroporous | 65–82% |
| 2004 | Landi et al. Italy + Indonesia | Sponge impregnation, isotactic pressing, sintering of HA in simulated body fluid. | Calcium hydroxide + orthophosphoric acid | Yes: 1250 °C for 1 hr | 23 ± 3.8 MPa | closed 6%, open 60% | 66% |
| 2003 | Charriere et al. EPFL, Switzerland | Thermoplastic negative porosity by ink jet printing, slip casting process for HA | DCPD + Calcite | No: 90 °C for 1 day | 12.5 ± 4.6 MPa | – | 44% |
| 2003 | Almirall et al. Barcelona, Spain | α-TCP foamed with hydrogen peroxide at different conc., liq. ratios, poured in PTFE molds. | α-TCP + (10% and 20% peroxide) | No: 60 °C for 2 hr | 1.41 ± 0.27 MPa 2.69 ± 0.91 MPa | 35.7% macro 29.7% micro 26.8% macro 33.8% micro | 65.5% 60.7% |
| 2003 | Ramay et al. Seattle, WA | Slurries of HA prepared: gel-casting + polymer sponge technique. Sintered. | HA powder | Yes: 600 °C for 1 hr, 1350 °C for 2 hr | 0.5–5 MPa | 200–400 μm | 70–77% |
| 2003 | Miao et al. Singapore | TTCP to calcium orthophosphate cement. Slurry cast on polymer foam, sintered. | TTCP | Yes: 1200 °C for 2 hr | – | 1 mm macro, 5 μm micro | ~70% |
| 2003 | Uemura et al. China + Japan | Slurry of HA with polyoxyethylenelaurylether (crosslinked) and sintered. | HA powders | Yes: 1200 °C for 3 hr | 2.25 MPa (0 wk) 4.92 MPa (12 wks) 11.2 MPa (24 wks) | 500 micron 200 μm interconnects | ~77% |
| 2003 | Ma et al. Singapore + USA | Electrophoretic deposition of HA, sintering. | HA powders | Yes: 1200 °C for 2 hr | 860 MPa | 0.5 μm, 130 μm | ~20% |
| 2002 | Barralet et al. Birmingham, London | Calcium orthophosphate cement + sodium orthophosphate ice: evaporated. | Calcium carbonate + DCDP | 1st step: 1400 °C for 1 day | 0.6 ± 0.27 MPa | 2 μm | 62 ± 9% |
Porous bioceramics with an improved strength might be fabricated from calcium orthophosphate fibers or whiskers. In general, fibrous porous materials are known to exhibit improved strength due to fiber interlocking, crack deflection and/or pullout [386]. Namely, porous bioceramics with well-controlled open pores were processed by sintering of fibrous HA particles [387]. In another approach, porosity was achieved by firing apatite-fiber compacts mixed with carbon beads and agar. By varying the compaction pressure, firing temperature and carbon/HA ratio, the total porosity was controlled in the ranges from ~40% to ~85% [378]. Additional examples are available in literature [364,367,374,375,376,377,378,379,380,389,390,391,392,393,394,395,396,397,398,399,400,401,402,403,404,405,406,407,408].
In vivo response of calcium orthophosphate bioceramics of different porosity was investigated and hardly any effect of macropore dimensions (~150, ~260, ~510 and ~1220 μm) was observed [409]. In another study, a greater differentiation of mesenchymal stem cells was observed when cultured on ~200 μm pore size HA scaffolds when compared to those on ~500 μm pore size HA [410]. The latter finding was attributed to the fact that a higher pore volume in ~500 μm macropore scaffolds might contribute to a lack of cell confluency, leading to the cells proliferating before beginning differentiation. In addition, the authors hypothesized that bioceramics having less than optimal pore dimensions induced quiescence in differentiated osteoblasts due to reduced cell confluency [410]. Already in 1979, Holmes suggested that the optimal pore range was 200–400 μm with the average human osteon size of ~223 μm [105]. In 1997, Tsurga and coworkers implied that the optimal pore size of bioceramics that supported ectopic bone formation was 300–400 μm [411]. Thus, there is no need to create calcium orthophosphate bioceramics with very big pores; however, the pores must be interconnected [108,352,364,365]. Interconnectivity governs a depth of cells or tissue penetration into the porous bioceramics, as well as allowing development of blood vessels required for new bone nourishing and waste removal [412,413].
Bioceramic microporosity (pore size <10 μm), which is defined by its capacity to be impregnated by biological fluids [412], results from the sintering process, while the pore dimensions mainly depend on the material composition, thermal cycle and sintering time. The microporosity provides both a greater surface area for protein adsorption and increased ionic solubility. Nanoporous (average pore sizes of less than 100 nm) HA bioceramics might be fabricated as well [414]. Differences in porogens influence the macroporosity, while differences in sintering temperatures and conditions affect the percentage of microporosity. Usually, the higher the sintering temperature, the lower both the microporosity content and the specific surface area of bioceramics. Namely, HA bioceramics sintered at ~1200 °C shows significantly less microporosity and a dramatic change in crystal sizes, if compared with those sintered at ~1050 °C (Figure 6). Furthermore, the average shape of pores was found to transform from strongly oblate to round at higher sintering temperatures [416]. The total porosity (macroporosity + microporosity) of calcium orthophosphate bioceramics was reported to be about 70% of the bioceramic volume [417]. In the case of coralline HA or bovine-derived apatites, the porosity of the original biologic material (coral or bovine bone) is usually preserved during processing [107]. To conclude this topic, creation of the desired porosity in calcium orthophosphate bioceramics is a rather complicated engineering task and interested readers are referred to [65,119,368,382,418,419,420,421,422,423,424,425,426,427,428,429,430,431,432,433,434,435,436,437,438,439,440,441,442].
Studies revealed that increasing both the specific surface area and pore volume of bioceramics might greatly accelerate the in vivo process of apatite deposition and, therefore, enhance bone-forming bioactivity. More importantly, a precise control over the porosity, pore dimensions and internal pore architecture of bioceramics on different length scales is essential for understanding the structure-bioactivity relationship and the rational design of better bone-forming biomaterials [439,443,444]. Namely, in antibiotic charging experiments, a nanoporous calcium orthophosphate bioceramic showed a much higher charging capacity (1621 μg/g) than that of commercially available calcium orthophosphate (100 μg/g), which did not have any nanoporosity [434]. In other experiments, porous blocks of HA were found to be viable carriers with sustained release profiles for drugs [445] and antibiotics over 12 days [446] and 12 weeks [447], respectively. Unfortunately, the porosity significantly decreases the strength of implants [63,283,301]. Thus, porous calcium orthophosphate implants cannot be loaded and are used to fill only small bone defects. However, their strength increases gradually when bones ingrow into the porous network of calcium orthophosphate implants [448,449,450,451]. For example, Martin et al. reported bending strengths of 40–60 MPa for a porous HA implant filled with 50–60% of cortical bone [448], while in another study an ingrown bone increased strength of porous HA bioceramics by a factor of three to four [450].
To conclude this topic, filters for microbial filtration might be manufactured from porous HA [452].
Figure 6.
SEM pictures of HA bioceramics sintered at (a) 1050 °C and (b) 1200 °C. Note the presence of microporosity in (a) and not in (b). Reprinted from [415] with permission.
Figure 6.
SEM pictures of HA bioceramics sintered at (a) 1050 °C and (b) 1200 °C. Note the presence of microporosity in (a) and not in (b). Reprinted from [415] with permission.

6. Biomedical Applications
Since Levitt et al. described a method of preparing a FA bioceramics and suggested their possible use in medical applications in 1969 [453], calcium orthophosphate bioceramics have been widely tested for clinical applications. Namely, calcium orthophosphates in a number of forms and compositions (Table 3) are currently either in use or under a consideration in many areas of dentistry and orthopedics, with even more in development. For example, bulk materials, available in dense and porous forms, are used for alveolar ridge augmentation, immediate tooth replacement and maxillofacial reconstruction [65,69]. Other examples include orbital implants (Bio-Eye®) [458,459], increment of the hearing ossicles, spine fusion and repair of bone defects [460,461]. In order to permit growth of new bone into defects, a suitable bioresorbable material should fill these defects. Otherwise, ingrowth of fibrous tissue might prevent bone formation within the defects.
| Calcium orthophosphate | Trade name and producer | ||
|---|---|---|---|
| CDHA | Cementek (Teknimed, France) | ||
| Osteogen (Impladent, NY, USA) | |||
| HA | Actifuse (ApaTech, UK) | ||
| Apaceram (Pentax, Japan) | |||
| ApaPore (ApaTech, UK) | |||
| Bioroc (Depuy-Bioland, France) | |||
| Bonefil (Pentax, Japan) | |||
| Bonetite (Pentax, Japan) | |||
| Boneceram (Sumitomo Osaka Cement, Japan) | |||
| BoneSource (Stryker Orthopaedics, NJ, USA) | |||
| Calcitite (Zimmer, IN, USA) | |||
| Cerapatite (Ceraver, France) | |||
| Neobone (Toshiba Ceramics, Japan) | |||
| Ostegraf (Ceramed, CO, USA) | |||
| Ostim (Heraeus Kulzer, Germany) | |||
| Synatite (SBM, France) | |||
| HA/collagen | Bioimplant (Connectbiopharm, Russia) | ||
| Bonject (Koken, Japan) | |||
| CollapAn (Intermedapatite, Russia) | |||
| HAPCOL (Polystom, Russia) | |||
| LitAr (LitAr, Russia) | |||
| HA/sodium alginate | Bialgin (Biomed, Russia) | ||
| HA/Poly-L-Lactic Acid | SuperFIXSORB30 (Takiron, Japan) | ||
| HA/polyethylene | HAPEX (Gyrus, TN, USA) | ||
| HA/CaSO4 | Hapset (LifeCore, MIN, USA) | ||
| coralline HA | Interpore (Interpore, CA, USA) | ||
| ProOsteon (Interpore, CA, USA) | |||
| algae-derived HA | Algipore (Dentsply Friadent, Germany) | ||
| bovine bone apatite (unsintered) | BioOss (Geitslich, Switzerland) | ||
| Laddec (Ost-Developpement, France) | |||
| Lubboc (Ost-Developpement, France) | |||
| Oxbone (Bioland biomateriaux, France) | |||
| Tutoplast (IOP, CA, USA) | |||
| bovine bone apatite (sintered) | BonAP | ||
| Cerabone (aap Implantate, Germany) | |||
| Endobon (Merck, Germany) | |||
| Osteograf (Ceramed, CO, USA) | |||
| PepGen P-15 (Dentsply Friadent, Germany) | |||
| β-TCP | Bioresorb (Sybron Implant Solutions, Germany) | ||
| Biosorb (SBM S.A., France) | |||
| Calciresorb (Ceraver, France) | |||
| Cerasorb (Curasan, Germany) | |||
| Ceros (Thommen Medical, Switzerland) | |||
| ChronOS (Synthes, PA, USA) | |||
| Conduit (DePuy Spine, USA) | |||
| JAX (Smith and Nephew Orthopaedics, USA) | |||
| Osferion (Olympus Terumo Biomaterials, Japan) | |||
| OsSatura TCP (Integra Orthobiologics, CA, USA) | |||
| Vitoss (Orthovita, PA, USA) | |||
| BCP (HA + β-TCP) | 4Bone (MIS, Israel) | ||
| BCP (Medtronic, MN, USA) | |||
| Biosel (Depuy Bioland, France) | |||
| BoneSave (Stryker Orthopaedics, NJ, USA) | |||
| Calciresorb (Ceraver, France) | |||
| CellCeram (Scaffdex, Finland) | |||
| Ceraform (Teknimed, France) | |||
| Ceratite (NGK Spark Plug, Japan) | |||
| Eurocer (FH Orthopedics, France) | |||
| Graftys BCP (Graftys, France) | |||
| Hatric (Arthrex, Naples, FL, USA) | |||
| Indost (Polystom, Russia) | |||
| Kainos (Signus, Germany) | |||
| MBCP (Biomatlante, France) | |||
| OptiMX (Exactech, USA) | |||
| OsSatura BCP (Integra Orthobiologics, CA, USA) | |||
| Osteosynt (Einco, Brazil) | |||
| SBS (Expanscience, France) | |||
| TCH (Kasios, France) | |||
| Triosite (Zimmer, IN, USA) | |||
| Tribone (Stryker, Europe) | |||
| BCP (HA + α-TCP) | Skelite (Millennium Biologix, ON, Canada) | ||
| BCP/collagen | Allograft (Zimmer, IN, USA) | ||
| BCP/fibrin | TricOS (Baxter BioScience, France) | ||
| BCP/silicon | FlexHA (Xomed, FL, USA) | ||
| FA + BCP (HA + β-TCP) | FtAP (Polystom, Russia) | ||
| carbonateapatite | Healos (Orquest, CA, USA) |
In spite of the aforementioned serious mechanical limitations, bioceramics of calcium orthophosphates are available in various physical forms: powders, particles, granules (or granulates [11]), dense blocks, porous scaffolds, injectable formulations, self-setting cements and concretes, implant coatings and composite component of different origin (natural, biological or synthetic) often with specific shapes, such as implants, prostheses or prosthetic devices (Table 4) [1,108]. Furthermore, bone grafts are also proposed as non-hardening pastes (=“putty”). Generally, the latter materials consist of a mixture of calcium orthophosphate granules and a “glue”, typically a highly viscous hydrogel [1,292]. More to the point, custom-designed shapes like wedges for tibial opening osteotomy, cones for spine and knee and inserts for vertebral cage fusion are also available [417]. Various trademarks of the commercially available types of calcium orthophosphate-based bioceramics and biomaterials are summarized in Table 3.
6.1. Cements and Concretes
The need of bioceramics for minimal invasive surgery has induced the development of a concept of self-setting bone cements consisting of only calcium orthophosphates to be applied as injectable and/or mouldable bone substitutes [149,366,367,384,431,462,463,464,465,466,467,468,469,470]. In addition, there are reinforced formulations, which, in a certain sense, might be defined as calcium orthophosphate concretes [464]. Furthermore, porous formulations of both the cements and the concretes are available [367,384,465,466,467,468].
Calcium orthophosphate cements and concretes belong to low temperature bioceramics. They are divided into two major groups. The first one is a dry mixture of two different calcium orthophosphates (a basic one and an acidic one), in which, after being wetted, the setting reaction occurs according to an acid-base reaction. The second group of the cements contains only one calcium orthophosphate. Typical examples include ACP with Ca/P molar ratio within 1.50–1.67 and α-TCP: they form CDHA upon contact with an aqueous solution [149,463,464]. The setting reaction (= hardening, curing) of these materials is initiated by mixing the initial powder(s) with an aqueous solution. Chemically, hardening is due to the successive dissolution and precipitation reactions. Mechanically, hardening results from crystal entanglement and intergrowth (Figure 7) [1]. Setting of calcium orthophosphate cements and concretes occurs mostly within the initial ~6 h, yielding ~80% conversion to the final products and a compressive strength of 40–60 MPa. Hardening rate is strongly influenced by powder to liquid ratio, as well as by addition of other chemicals [149,462,463,464,465,466,467,468,469,470]. Despite a large number of formulations, all calcium orthophosphate cements can only form two different end products: CDHA and DCPD [149,463,464].
All calcium orthophosphate cements and concretes are biocompatible, bioactive and bioresorbable. The first animal study of a calcium orthophosphate cement was performed in 1991, where a cement consisting of TTCP and DCPA was investigated histologically by implanting disks made of this cement within the heads of nine cats [471,472]. In 1996, that formulation received an approval by the U.S. Food and Drug Administration, thus becoming the first commercially available calcium orthophosphate cement for use in humans [465]. As the structure and composition of the hardened cements is close to that of bone mineral, the material of the hardened cements can easily be used by bone remodeling cells for reconstruction of damaged parts of bones [149,462,463,464,465]. A possibility to be injected (a minimally invasive technique), a low setting temperature, an adequate stiffness, an easy shaping and a good adaptation to the defect geometry are the major advantages of calcium orthophosphate cements and concretes, when compared to the prefabricated bulk bioceramics and porous scaffolds. Further details on this subject are available in literature [463,464,465].
Table 4.
Specific features of the four most common forms of bone graft substitutes. The column “defect form” lists the types of defects that can be potentially filled with the listed bone graft substitute form. “Open” means that the defect has to be widely open, e.g., an open cancellous bone defect; “Defined shape” means that the defect has to have a well-defined shape, e.g., cylinder; “Closed” means that the material can be (potentially) injected into a closed defect, e.g., to reinforce an osteoporotic bone [1].
| Form | Defect form | Mechanical stability | Resorption/bone formation | Handling |
|---|---|---|---|---|
| Granules (0.1–5 mm in diameter) | Open | Negligible | Throughout the defect | Fair (granule migration during and after surgery) |
| Macroporous blocks | Open and defined shape | Fair provided there is press-fitting into the defect | Throughout the defect | Very good (problems might arise to fit the block within the defect) |
| Cement paste | Closed | Fair | Peripheral | Fair to good (the paste might set too fast or might be poorly injectable) |
| Putty | Open or closed | Negligible | Peripheral or throughout the defect depending on the composition | Very good for pastes that have to be mixed in the operating room to excellent for ready-mixed pastes (the paste might be poorly-injectable) |
Figure 7.
A typical microstructure of a calcium orthophosphate cement after hardening. The mechanical stability is provided by the physical entanglement of crystals. Reprinted from [1] with permission.
Figure 7.
A typical microstructure of a calcium orthophosphate cement after hardening. The mechanical stability is provided by the physical entanglement of crystals. Reprinted from [1] with permission.

6.2. Coatings
For many years, the clinical application of calcium orthophosphate-based bioceramics has been largely limited to non-load bearing parts of the skeleton due to their inferior mechanical properties. One of the major innovations in the last ~30 years has been to coat mechanically strong bioinert and/or biotolerant prostheses by calcium orthophosphates [60,473,474]. For example, metallic implants are encountered in endoprostheses (total hip joint replacements) and artificial teeth sockets. The requirement for a sufficient mechanical stability necessitates the use of a metallic body for such devices. As metals do not undergo bone bonding, i.e., do not form a mechanically stable link between the implant and bone tissue, methods have been sought to improve contacts at the interface. The major way is to coat metals with calcium orthophosphate bioceramics that exhibit a bone-bonding ability between the metal and bone [60,179,190,315,475,476,477,478,479,480]. Thickness of the coatings vary from submicron dimensions to several hundreds microns (Table 5) and this parameter appears to be very important. For example, if a calcium orthophosphate coating is too thick, it is easy to break. On the contrary, if the coating is too thin, it is easy to dissolve, because resorbability of HA, which is the second slowest to dissolve among calcium orthophosphates (Table 1), is about 15–30 μm per year [481]. One should stress that calcium orthophosphate coatings are not limited to metals only; they can be applied on carbon, bioinert ceramics and polymers as well [482]. Most important coating techniques are listed in Table 5, while the main advantages and drawbacks of each coating technique, as well as the major properties of the deposed calcium orthophosphates, are discussed in detail elsewhere [60,179,221,272,473,483,484,485,486,487,488,489,490,491,492,493,494,495,496,497]. Unfortunately, none of these methods can provide the perfect covering because each coating always contains cracks, pores, second phases and residual stresses that reduced their durability and might lead to a partial or complete disintegration of the coating in body fluids. The biomedical aspects of osteoconductive coatings for total joint arthroplasty have been reviewed elsewhere [498].
| Technique | Thickness | Advantages | Disadvantages |
|---|---|---|---|
| Thermal spraying | 30–200 μm | High deposition rates; low cost | Line of sight technique; high temperatures induce decomposition; rapid cooling produces amorphous coatings |
| Sputter coating | 0.5–3 μm | Uniform coating thickness on flat substrates; dense coating | Line of sight technique; expensive; time consuming; produces amorphous coatings |
| Pulsed laser deposition | 0.05–5 μm | Coating by crystalline and amorphous phases; dense and porous coating | Line of sight technique |
| Dynamic mixing method | 0.05–1.3 μm | High adhesive strength | Line of sight technique; expensive; produces amorphous coatings |
| Dip coating | 0.05–0.5 mm | Inexpensive; coatings applied quickly; can coat complex substrates | Requires high sintering temperatures; thermal expansion mismatch |
| Sol-gel technique | <1 μm | Can coat complex shapes; low processing temperatures; relatively cheap as coatings are very thin | Some processes require controlled atmosphere processing; expensive raw materials |
| Electrophoreticdeposition | 0.1–2.0 mm | Uniform coating thickness; rapid deposition rates; can coat complex substrates | Difficult to produce crack-free coatings; requires high sintering temperatures |
| Biomimetic coating | <30 μm | Low processing temperatures; can form bonelike apatite; can coat complex shapes; can incorporate bone growth stimulating factors | Time consuming; requires replenishment and a pH constancy of simulated body fluid |
| Hot isostatic pressing | 0.2–2.0 μm | Produces dense coatings | Cannot coat complex substrates; high temperature required; thermal expansion mismatch; elastic property differences; expensive; removal/interaction of encapsulation material |
| Electrochemical deposition | 0.05–0.5 mm | Uniform coating thickness; rapid deposition rates; can coat complex substrates; moderate temperature, low cost | Thecoating/substrate bonding is not strong enough |
All coatings must adhere satisfactorily to the underlying substrate irrespective of their intended function. Specifically, mechanical stability of calcium orthophosphate coatings should be high enough to maintain their bioactive functionality after a surgical implantation. Generally, tensile adhesion testing according to standards such as ASTM C633 is the most common procedure to determine the quantitative values for calcium orthophosphate coating adhesion to the underlying metallic substrates. Furthermore, fatigue [499,500] scratch [501] and pullout [501] testing are among the most valuable techniques to provide additional information on the mechanical behavior of calcium orthophosphate coatings [179].
Already in the 1980s, de Groot et al. [502] published on the development of plasma-sprayed HA coatings on metallic implants. A little bit later, Furlong and Osborn [503], two leading surgeons in the orthopedics field, began implanting plasma-sprayed HA stems in patients. Coated implants combine the surface biocompatibility and bioactivity of calcium orthophosphates with the core strength of strong substrates (Figure 8). Moreover, calcium orthophosphate coatings decrease a release of potentially hazardous chemicals from the core implant and shield the substrate surface from environmental attack. In the case of porous implants, calcium orthophosphate coatings enhance bone ingrowth into the pores [63]. Clinical results for calcium orthophosphate-coated implants reveal that they have much longer life times after implantation than uncoated devices and they are found to be particularly beneficial for younger patients. Studies concluded that there was significantly less pin loosening in the HA-coated groups [504]. HA coating as a system of fixation of hip implants was found to work well in the short to medium term (eight years [505], 10 to 15.5 years [506], 15 years [507], 16 years [508], 17 years [509], 19 years [510] and 15 to 21 years [511]). Similar data for HA-coated dental implants are also available [512,513]. Even longer-term clinical results are awaited with great interest.
Figure 8.
Plasma-sprayed HA coating on a porous titanium (dark bars) is dependent on the implantation time and will improve the interfacial bond strength compared to uncoated porous titanium (light bars). Reprinted from [46] with permission.
Figure 8.
Plasma-sprayed HA coating on a porous titanium (dark bars) is dependent on the implantation time and will improve the interfacial bond strength compared to uncoated porous titanium (light bars). Reprinted from [46] with permission.

A number of factors appear to influence the properties of calcium orthophosphate coatings, including coating thickness (this will influence coating adhesion and fixation—the agreed optimum now seems to be within 50–100 µm), crystallinity (affecting the dissolution and biological behavior), phase purity, chemical purity, porosity and adhesion [473,484]. Methods for the production of coatings and their properties are now largely standardized and, over recent years, calcium orthophosphate-coated implants have found highly successful clinical application, particularly in younger patients [514,515,516]. Further details on calcium orthophosphate coatings can be found in excellent reviews [517,518].
6.3. Functionally Graded Bioceramics
In general, functionally gradient materials (FGMs) are defined as materials having either a gradient of compositional or structural changes from their surface to the interior. The idea of FGMs allows one device to possess two different properties. One of the most important combinations for the biomedical field is that of mechanical strength and biocompatibility. Namely, only surface properties govern biocompatibility of the entire device. In contrast, the strongest material determines the mechanical strength of the entire device. Although, this subject belongs to the coatings section (above), in a certain sense, metallic implants covered by calcium orthophosphates can be considered as a FGM. The surface shows excellent biocompatibility because it consists of calcium orthophosphates, while the metallic core provides excellent mechanical strength. The gradient change from calcium orthophosphate to metal is important, for example, from the point of thermal expansion.
Functionally graded bioceramics consisting of calcium orthophosphates only [519] have been developed [377,438,440,522,523,524,525,526,527,528,529]. For example, dense sintered bodies with gradual compositional changes from α-TCP to HA were prepared by sintering diamond-coated HA compacts at 1280 °C under a reduced pressure, followed by heating under atmospheric conditions [522]. The content of α-TCP gradually decreased, while the content of HA increased with increasing depth from the surface. This functionally gradient bioceramic consisting of an HA core and α-TCP surface showed potential value as bone-substituting biomaterial [522]. Two types of functionally gradient FA/β-TCP biocomposites were prepared in another study [523]. As shown in Figure 9, one of the graded biocomposites was in the shape of a disk and contained four different layers of about 1 mm thickness. The other graded biocomposite was also in the shape of a disk but contained two sets of four layers, each layer being 0.5 mm thick, controlled by using a certain amount of the mixed powders. The final FA/β-TCP graded structures were formed at 100 MPa and sintered at 1300 °C for 2 h [523].
Furthermore, it is known that the bone cross-section from cancellous to cortical bone is non-uniform in porosity and pore dimensions. Thus, in various attempts to mimic the porous structure of bones, calcium orthophosphate bioceramics with graded porosity have been fabricated [377,438,440,522,523,524,525,526,527,528,529]. Since diverse biomedical applications require different configurations and shapes, the graded (or gradient) porous bioceramics can be grouped according to both the overall shape and the structural configuration [346]. The basic shapes include rectangular blocks and cylinders (or disks). For the cylindrical shape, there are configurations of dense core-porous layer, less porous core-more porous layer, dense layer-porous core and less porous layer-more porous core. For the rectangular shape, in the gradient direction i.e., the direction with varying porosity, pore size or composition, there are configurations of porous top-dense bottom (same as porous bottom-dense top), porous top-dense center-porous bottom, dense top-porous center-dense bottom, etc. Concerning biomedical applications, a dense core-porous layer structure is suitable for implants of a high mechanical strength and with bone ingrowth for stabilization, whereas a less porous layer-more porous core configuration can be used for drug delivery systems. Furthermore, a porous top-dense bottom structure can be shaped into implants of articulate surfaces for wear resistance and with porous ends for bone ingrowth fixation; while a dense top-porous center-dense bottom arrangement mimics the structure of head skull. Further details on bioceramics with graded porosity might be found in literature [346].
Figure 9.
A schematic diagram showing the arrangement of the FA/β-TCP biocomposite layers. (a) A non-symmetric functionally gradient material (FGM); (b) symmetric FGM. Reprinted from [523] with permission.
Figure 9.
A schematic diagram showing the arrangement of the FA/β-TCP biocomposite layers. (a) A non-symmetric functionally gradient material (FGM); (b) symmetric FGM. Reprinted from [523] with permission.

7. Biological Properties and In Vivo Behavior
The most important differences between bioactive bioceramics and all other implanted materials are: inclusion in metabolic processes of the organism; adaptation of either surface or the entire material to the biomedium; integration of a bioactive implant with bone tissues at the molecular level or the complete replacement of a resorbable bioceramic by healthy bone tissues. All of the enumerated processes are related to the effect of an organism on the implant. Nevertheless, another aspect of implantation is also important—the effect of the implant on the organism. For example, use of bone implants from corpses or animals, even after they have been treated in various ways, provokes a negative immune reaction in the organism, which substantially limits the application of such implants. In this connection, it is useful to dwell on the biological properties of bioceramic implants, particularly those of calcium orthophosphates, which in the course of time may be resorbed completely [530].
7.1. Interaction with the Surrounding Tissues and the Host Responses
An interaction between an implant and surrounding tissues is a dynamic process. Water, dissolved ions, biomolecules and cells surround the implant surface during initial few seconds after the implantation. It is accepted that no foreign material placed within a living body is completely compatible. The only substances that conform completely are those manufactured by the body itself (autogenous) and any other substance that is recognized as foreign, initiates some reactions (a host-tissue response). The reactions occurring at the biomaterial/tissue interface lead to time-dependent changes in the surface characteristics of both the implanted biomaterials and the surrounding tissues [54,531].
In order to develop new biomaterials, it is necessary to understand the in vivo host responses. Like any other species, biomaterials and bioceramics react chemically with their environment and, ideally, they should neither induce any changes nor provoke undesired reactions in the neighboring or distant tissues. In general, living organisms can treat artificial implants as biotoxic (or bioincompatible [50]), bioinert (or biostable [42]), biotolerant (or biocompatible [50]), bioactive and bioresorbable materials [3,4,5,6,38,39,40,46,47,48,49,50,91,478,530,531,532]. Biotoxic (e.g., alloys containing cadmium, vanadium, lead and other toxic elements) materials release substances to the body in toxic concentrations and/or trigger the formation of antigens that may cause immune reactions ranging from simple allergies to inflammation to septic rejection with the associated severe health consequences. They cause atrophy, pathological change or rejection of living tissue near the material due to chemical, galvanic or other processes. Bioinert [533] (e.g., zirconia, alumina, carbon and titanium) and biotolerant (e.g., polymethylmethacrylate, titanium and Co-Cr alloy) materials do not release any toxic constituents but also do not show positive interaction with living tissue. They evoke a physiological response to form a fibrous capsule, thus, isolating the material from the body. In such cases, thickness of the layer of fibrous tissue separating the material from other tissues of an organism can serve as a measure of bioinertness. Generally, both bioactivity and bioresorbability phenomena are fine examples of chemical reactivity and calcium orthophosphates (both non-substituted and ion-substituted ones) fall into these two categories of bioceramics [3,4,5,6,38,39,40,46,47,48,49,50,91,478,530,531,532]. A bioactive material will dissolve slightly but promote formation of a surface layer of biological apatite before interfacing directly with the tissue at the atomic level, which results in formation of a direct chemical bonds to bones. Such an implant provides good stabilization for materials that are subject to mechanical loading. A bioresorbable material will dissolve over time (regardless of the mechanism leading to the material removal) and allow a newly formed tissue to grow into any surface irregularities but may not necessarily interface directly with the material. Consequently, the functions of bioresorbable materials are to participate in dynamic processes of formation and re-absorption occurring in bone tissues; thus, bioresorbable materials are used as scaffolds or filling spacers allowing their infiltration and substitution to the tissues [47,272,534,535,536,537].
A distinction between bioactive and bioresorbable bioceramics might be associated with a structural factor only. For example, bioceramics made from non-porous, dense and highly crystalline HA behaves as a bioinert (but a bioactive) material and are retained in an organism for at least 5–7 years without noticeable changes, while a highly porous bioceramics of the same composition can be resorbed approximately within a year. Furthermore, submicron-sized HA powders are biodegraded even faster than the highly porous HA scaffolds. Other examples of bioresorbable materials include porous bioceramic scaffolds made of BCP (which is an intimate mixture of either β-TCP + HA [118,119,120,121,122,123,124,125,126,127,128,129,130], or α-TCP + HA [7,8,9,10,11]) or bone grafts (dense or porous) made of CDHA [538], TCP [377,539,540] and/or ACP [418,541]. One must stress that recently the concepts of bioactive and bioresorbable materials have converged and bioactive materials are made bioresorbable, while bioresorbable materials are made bioactive [542].
In certain in vivo experiments an inflammatory reaction was observed after implantation of calcium orthophosphate bioceramics [543,544,545]. Despite this, the general conclusion on using calcium orthophosphates with a Ca/P ionic ratio within 1.0–1.7 is that all types of implants (bioceramics of various porosities and structures, powders or granules) are not only nontoxic but also induce neither inflammatory nor foreign-body reactions [546]. The biological response to implanted calcium orthophosphates follows a similar cascade observed in fracture healing. This cascade includes hematoma formation, inflammation, neovascularization, osteoclastic resorption and new bone formation. An intermediate layer of fibrous tissue between the implants and bones has never been detected. Furthermore, calcium orthophosphate implants display the ability to directly bond to bones [2,3,4,5,6,38,42,46,47,48,49,50,51,52,54,60,530]. For further details, interested readers are referred to a good review on cellular perspectives of bioceramic scaffolds for bone tissue engineering [374].
One should note that the aforementioned rare cases of inflammatory reactions to calcium orthophosphate bioceramics were caused by “other” reasons. For example, a high rate of wound inflammation occurred when highly porous HA was used. In that particular case, the inflammation was explained by sharp implant edges, which irritated surrounding soft tissues [544]. Another reason for inflammation produced by porous HA could be due to micro movements of the implants, leading to simultaneous disruption of a large number of micro-vessels, which grow into the pores of the bioceramics. This would immediately produce an inflammatory reaction. Additionally, problems could arise in clinical tests connected with migration of granules used for alveolar ridge augmentation, because it might be difficult to achieve mechanical stability of implants at the implantation sites [544].
7.2. Osteoinduction
Until recently, it was generally considered, that alone, any type of synthetic bioceramics possessed neither osteogenic [547] nor osteoinductive [548] properties and demonstrated minimal immediate structural support. When attached to healthy bones, an osteoid [550] is produced directly onto the surfaces of bioceramics in the absence of a soft tissue interface. Consequently, the osteoid is mineralized and the resulting new bone undergoes remodeling [549]. However, several reports have already shown osteoinductive properties of certain types of calcium orthophosphate bioceramics [168,415,457,551,552,553,554,555,556,557,558,559,560,561,562,563]. Namely, bone formation was found to occur in dog muscle inside porous calcium orthophosphates with surface microporosity, while bone was not observed on the surface of dense bioceramics [559]. Furthermore, implantation of porous β-TCP bioceramics appeared to induce bone formation in soft tissues of dogs, while no bone formation was detected in any α-TCP implants [556]. More to the point, titanium implants coated by a microporous layer of OCP were found to induce ectopic bone formation in goat muscles, while a smooth layer of carbonated apatite on the same implants was not able to induce bone formation there [562,563].
Although the mechanisms of intrinsic osteoinduction of calcium orthophosphate bioceramics are not unraveled, the dissolution/precipitation behavior of calcium orthophosphates [479], as well as their microporosity [564,565] and specific surface area [565] have been pointed out as the relevant parameters. A positive effect of increased microporosity on ectopic bone formation could be direct and indirect. Firstly, an increased microporosity is directly related to the changes in surface topography, i.e., increases a surface roughness, which might affect cellular differentiation. Secondly, an increased microporosity indirectly means a larger surface is exposed to the body fluids, leading to elevated dissolution/precipitation phenomena as compared to non-microporous surfaces. Furthermore, other hypotheses are available. Namely, Reddi explained the apparent osteoinductive properties as an ability of particular bioceramics to concentrate bone growth factors, which are circulating in biological fluids, and that these growth factors induce bone formation [566]. Other researchers proposed a similar hypothesis that the intrinsic osteoinduction by calcium orthophosphate bioceramics is a result of adsorption of osteoinductive substances on their surface [561]. Moreover, Ripamonti [567] and Kuboki et al. [568] independently postulated that the geometry of calcium orthophosphate bioceramics is a critical parameter in bone induction. Specifically, bone induction by calcium orthophosphates was never observed on flat bioceramic surfaces. All osteoinductive cases were observed on either porous structures or structures contained well-defined concavities. Moreover, bone formation was never observed on the peripheries of porous implants and was always found inside the pores or concavities, aligning the surface [179]. Some researchers speculated that a low oxygen tension in the central region of implants might provoke a dedifferentiation of pericytes from blood micro-vessels into osteoblasts [569]. Finally, and importantly, both nano-structured rough surfaces and a surface charge on implants were found to cause an asymmetrical division of the stem cells into osteoblasts, which is important for osteoinduction [564].
7.3. Biodegradation
Shortly after implantation, a healing process is initiated by compositional changes of the surrounding bio-fluids and adsorption of biomolecules. Following this, various types of cells reach the bioceramic surface and the adsorbed layer dictates the ways the cells respond. Further, a biodegradation of the implanted bioceramics begins. This process can occur by either physicochemical dissolution with a possibility of phase transformation or cellular activity (so called, bioresorption), as well as by a combination of both processes. Dissolution is a physical chemistry process, which is controlled by some factors, such as solubility of the implant matrix (Table 1), surface area to volume ratio, local acidity, fluid convection and temperature. For HA, the dissolution process in acids has been described by a sequence of four successive chemical equations [570,571]:
Ca10(PO4)6(OH)2 + 2H+ → Ca10(PO4)6(H2O)22+
Ca10(PO4)6(H2O)22+ → 3Ca3(PO4)2 + Ca2+ + 2H2O
Ca3(PO4)2 + 2H+ → Ca2+ + 2CaHPO4
CaHPO4 + H+ → Ca2+ + H2PO4−
With few exceptions, dissolution rates of calcium orthophosphates are inversely proportional to the Ca/P ratio, phase purity and crystalline size, as well as being directly related to the porosity and surface area. Phase transformations might occur with OCP, DCPA, DCPD, α-TCP, β-TCP and ACP because they are unstable in aqueous environments under physiological conditions. Bioresorption is a biological process mediated by cells (mainly osteoclasts and to a lesser extent, macrophages). It depends on the response of cells to their environment. Osteoclasts attach firmly to the implant and dissolve calcium orthophosphates by secreting an enzyme carbonic anhydrase or any other acid, leading to a local pH drop to ~4–5 [572]. Furthermore, calcium orthophosphate particles can also be phagocyotosed by osteoclasts, i.e., they are incorporated into the cytoplasm and thereafter dissolved by acid attack and/or enzymatic processes. In any case, biodegradation of calcium orthophosphates is a combination of various non-equilibrium processes, occurring simultaneously and/or in competition with each other.
Usually, an in vitro biodegradation of calcium orthophosphate bioceramics is estimated by suspending the material in a slightly acidic (pH ~5) buffer and monitoring the release of Ca2+ ions with time. The acidic buffer, to some extent, mimics the acidic environment during osteoclastic activity. One study compared the in vivo behavior of porous β-TCP bioceramics prepared from rod-shaped particles and that prepared from non-rod-shaped particles in the rabbit femur. Although the porosities of both types of β-TCP bioceramics were almost the same, more active osteogenesis was preserved in the region where rod-shaped bioceramics was implanted [573]. This result implied that the microstructure affected the activity of bone cells and subsequent bone replacement.
Experimental results demonstrated that both the dissolution kinetics and in vivo biodegradation of biologically relevant calcium orthophosphates proceed in the following decreasing order: β-TCP > bovine bone apatite (unsintered) > bovine bone apatite (sintered) > coralline HA > HA. In the case of BCP bioceramics, the biodegradation kinetics depends on the HA/TCP ratio: the higher the ratio, the lower the degradation rate. Similarly, in vivo degradation rate of biphasic TCP (BTCP, consisting of α-TCP + β-TCP) bioceramics appeared to be lower than that of α-TCP and higher than that of β-TCP bioceramics, respectively [141]. Furthermore, incorporation of doping ions can either increase (e.g., CO32−, Mg2+ or Sr2+) or decrease (e.g., F−) the solubility (therefore, biodegradability) of CDHA and HA. Contrarily to apatites, solubility of β-TCP decreases due to incorporation of either Mg2+ or Zn2+ ions [415]. One should remember that ion-substituted calcium orthophosphates are not considered in this review; interested readers are advised to [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37].
7.4. Bioactivity
Generally, bioactive materials interact with surrounding bone resulting in formation of a chemical bond to this tissue (bone bonding). The bioactivity phenomenon is determined by both chemical factors, such as crystal phases and molecular structures of a biomaterial, and physical factors, such as surface roughness and porosity. Currently, it is agreed that the newly formed bone bonds directly to biomaterials through a carbonated CDHA layer precipitating at the bone/biomaterial interface. Strange enough, just a few publications are present in the literature [415,484,574,575] that briefly describe the bioactivity mechanism of calcium orthophosphates. For example, the chemical changes occurring after exposure of a synthetic HA bioceramics to both in vivo (implantation in human) and in vitro (cell culture) conditions were studied. A small amount of HA was phagocytozed but the major remaining part behaved as a secondary nucleator as evidenced by the appearance of newly formed mineral [574]. In vivo, cellular activity (e.g., of macrophages or osteoclasts) associated with an acidic environment were found to result in partial dissolution of calcium orthophosphates, causing liberation of calcium and orthophosphate ions to the microenvironment. The liberated ions increased the local supersaturation degree of the surrounding biologic fluids, causing precipitation of nanocrystals of biological apatite with simultaneous incorporation of various ions presented in the fluids. Infrared spectroscopic analyses demonstrated that these nanocrystals were intimately associated with bioorganic components (probably proteins), which might also have originated from the biologic fluids, such as serum [415].
Therefore, one should better rely on the bioactivity mechanism of other biomaterials, particularly of bioactive glasses—the concept introduced by Larry L. Hench [46,47,48]. The bonding mechanism of bioactive glasses to living tissues involves a sequence of 11 successive reaction steps. The initial five steps occurring on the surface of bioactive glasses are “chemistry” only, while the remaining six steps belong to “biology”; the latter including colonization by osteoblasts, followed by proliferation and differentiation of the cells to form a new bone that had a mechanically strong bond to the implant surface (Figure 10). Therefore, in the case of bioactive glasses, the border between “dead” and “alive” is postulated between stages five and six. According to Hench, all bioactive materials “form a bone-like apatite layer on their surfaces in the living body and bond to bone through this apatite layer. The formation of bone-like apatite on artificial material is induced by functional groups, such as Si-OH (in the case of biological glasses), Ti-OH, Zr-OH, Nb-OH, Ta-OH, -COOH and -H2PO4 (in the case of other materials). These groups have specific structures revealing negatively charge and induce apatite formation via formations of an amorphous calcium compound, e.g., calcium silicate, calcium titanate and ACP” [46,47,48].
Figure 10.
A sequence of interfacial reactions involved in forming a bond between tissue and bioactive ceramics. Reprinted from [46,47,48] with permission.

To extend the subject, it is important to refer to another set of 11 successive reaction steps for bonding mechanism of unspecified bioceramics, developed by Paul Ducheyne (Figure 11) [54]. One can see that the Ducheyne’s model is rather similar to that proposed by Hench; however, there are noticeable differences. For example, Ducheyne mentions ion exchange and structural rearrangement at the bioceramic/tissue interface (stage 3), as well as interdiffusion from the surface boundary layer into bioceramics (stage 4) and deposition with integration into the bioceramics (stage 7), which are absent in Hench’s model. On the other hand, Hench describes six biological stages (stages 6–11), while Ducheyne describes only four (stages 8–11). Both models were developed almost two decades ago and, to the best of my knowledge, remain unchanged since then. Presumably, both approaches have pro et contra of their own and, obviously, should be updated and/or revised. Furthermore, in literature there are at least two other descriptions of biological and cellular events occurring at the bone/implant interface [576,577]; however, they include less stages. One more hypothesis has been proposed recently (Figure 12), which for the first time, describes reasonable surface transformations happening with calcium orthophosphate bioceramics (in that case, HA) shortly after implantation [575].
Figure 11.
A schematic diagram representing the events taking place at the interface between bioceramics and the surrounding biological environment: (1) dissolution of bioceramics; (2) precipitation from solution into bioceramics; (3) ion exchange and structural rearrangement at the bioceramic/tissue interface; (4) interdiffusion from the surface boundary layer into the bioceramics; (5) solution-mediated effects on cellular activity; (6) deposition of either the mineral phase (a) or the organic phase (b) without integration into the bioceramic surface; (7) deposition with integration into the bioceramics; (8) chemotaxis to the bioceramic surface; (9) cell attachment and proliferation; (10) cell differentiation; (11) extracellular matrix formation. All phenomena, collectively, lead to the gradual incorporation of a bioceramic implant into developing bone tissue. Reprinted from [54] with permission.
Figure 11.
A schematic diagram representing the events taking place at the interface between bioceramics and the surrounding biological environment: (1) dissolution of bioceramics; (2) precipitation from solution into bioceramics; (3) ion exchange and structural rearrangement at the bioceramic/tissue interface; (4) interdiffusion from the surface boundary layer into the bioceramics; (5) solution-mediated effects on cellular activity; (6) deposition of either the mineral phase (a) or the organic phase (b) without integration into the bioceramic surface; (7) deposition with integration into the bioceramics; (8) chemotaxis to the bioceramic surface; (9) cell attachment and proliferation; (10) cell differentiation; (11) extracellular matrix formation. All phenomena, collectively, lead to the gradual incorporation of a bioceramic implant into developing bone tissue. Reprinted from [54] with permission.

An important study on formation of calcium orthophosphate precipitates on various types of bioceramic surfaces in both simulated body fluid (SBF) and rabbit muscle sites was performed [578]. The bioceramics were sintered porous solids, including bioglass, glass-ceramics, α-TCP, β-TCP and HA. An ability to induce calcium orthophosphate precipitation was compared among these types of bioceramics. The following conclusions were made: (1) OCP formation ubiquitously occurred on all types of bioceramic surfaces both in vitro and in vivo, except on β-TCP. (2) Apatite formation did not occur on every type of bioceramic surface; it was less likely to occur on the surfaces of HA and α-TCP. (3) Precipitation of calcium orthophosphates on the bioceramic surfaces was more difficult in vivo than in vitro. (4) Differences in calcium orthophosphate precipitation among the bioceramic surfaces were less noticeable in vitro than in vivo. (5) β-TCP bioceramics showed poor calcium orthophosphate precipitation both in vitro and in vivo [578]. These findings clearly revealed that apatite formation in the physiological environments could not be confirmed to be the common feature of bioceramics. Nevertheless, for want of anything better, currently the bioactivity mechanism of calcium orthophosphate bioceramics could be described by a reasonable combination of Figure 10, Figure 11 and Figure 12, e.g., by updating the Ducheyne’s and Hench’s models by the three initial stages taken from Figure 12.
Figure 12.
A schematic diagram representing the phenomena that occur on HA surface after implantation: (1) beginning of the implant procedure, where solubilization of the HA surface starts; (2) continuation of the solubilization of the HA surface; (3) the equilibrium between the physiological solutions and the modified surface of HA has been achieved (changes in the surface composition of HA does not mean that a new phase of DCPA or DCPD forms on the surface); (4) adsorption of proteins and/or other bioorganic compounds; (5) cell adhesion; (6) cell proliferation; (7) beginning of a new bone formation; (8) new bone has been formed. Reprinted from [575] with permission.
Figure 12.
A schematic diagram representing the phenomena that occur on HA surface after implantation: (1) beginning of the implant procedure, where solubilization of the HA surface starts; (2) continuation of the solubilization of the HA surface; (3) the equilibrium between the physiological solutions and the modified surface of HA has been achieved (changes in the surface composition of HA does not mean that a new phase of DCPA or DCPD forms on the surface); (4) adsorption of proteins and/or other bioorganic compounds; (5) cell adhesion; (6) cell proliferation; (7) beginning of a new bone formation; (8) new bone has been formed. Reprinted from [575] with permission.

Interestingly, bioactivity of HA bioceramics might be enhanced by high-energy ion irradiation [579]. The effect was attributed to formation of a unique 3D macroporous apatite layer of decreased crystallinity and crystal size on the irradiated surfaces. To conclude this topic, the atomic and molecular phenomena occurring at the bioceramic surface in aqueous solutions and their effects on the relevant reaction pathways of cells and tissues must be elucidated in more detail. Further investigation of this topic requires a careful analysis of the available experimental data, which is beyond the scope of this review.
7.5. Cellular Response
Fixation of an implant in the human body is a dynamic process that remodels the interface zone between the implant and living tissues at all dimensional levels, from the molecular up to the cell and tissue morphology level, and at all time scales, from the first second up to several years after implantation. Immediately following implantation, a space filled with bio-fluids appears next to the implant surface. With time, proteins adsorb at the bioceramic surface and gives rise to osteoinduction by cell proliferation and their differentiation towards bone cells, revascularization and eventual gap closing. Ideally, a strong bond forms between the implant and surrounding tissues [50]. A detailed study on interfacial interactions between calcined HA and substrates has been performed recently [580].
Osteoblasts cultured on HA bioceramics are generally reported to be completely flattened, leading to difficulties in distinguishing the cytoplasmic edge from the HA surfaces after ~2 hours incubation [581]. These observations underscore an expected bioactivity of HA and make HA bioceramics well suited for bone reconstruction. Osteoblasts cultured on porous HA bioceramics appeared to exhibit higher adhesion, enhanced differentiation and suppressed proliferation rates when compared to the non-porous controls [582,583]. Furthermore, formation of distinct resorption pits on HA [584] and β-TCP [573] surfaces in the presence of osteoclasts was observed. Moreover, a surface roughness of calcium orthophosphate bioceramics was reported to strongly influence the activation of mononuclear precursors to mature osteoclasts [584].
Cellular biodegradation of calcium orthophosphate bioceramics is known to depend on its phases. For example, a higher solubility of β-TCP prevented L-929 fibroblast cell adhesion, thereby leading to damage and rupture of the cells [585]. A mouse ectopic model study indicated the maximal bone growth for the 80:20 β-TCP:HA biphasic formulations preloaded with human mesenchymal stem cells when compared to other calcium orthophosphates [586]. The effects of substrate microstructure and crystallinity have been corroborated with an in vivo rabbit femur model, where rod-like crystalline β-TCP was reported to enhance osteogenesis when compared to non-rod like crystalline β-TCP [573]. Additionally, using a dog mandibular defect model, a higher bone formation on a scaffold surface coated by nano-dimensional HA was observed when compared to that coated by a micro-dimensional HA [587]. Furthermore, recent studies revealed a stronger stress signaling response by osteoblast precursor cells in 3D scaffolds when compared to 2D surfaces [588].
Mesenchymal stem cells are one of the most attractive cellular lines for application as bone grafts [589]. Early investigations by Okumura et al. indicated an adhesion, proliferation and differentiation, which ultimately became new bone and integrated with porous HA bioceramics [590]. Recently, Unger et al. showed a sustained co-culture of endothelial cells and osteoblasts on HA scaffolds for up to six weeks [591]. Furthermore, a release of factors by endothelial and osteoblast cells in co-culture supported proliferation and differentiation was suggested to ultimately result in microcapillary-like vessel formation and supported a neo-tissue growth within the scaffold [374]. More to the point, investigation of rat calvaria osteoblasts cultured on transparent HA bioceramics, as well as the analysis of osteogenic-induced human bone marrow stromal cells at different time points of culturing, indicated a good cytocompatibility of HA bioceramics and revealed favorable cell proliferation [343]. Positive results for other types of cells have been obtained in other studies [191,338,339,342].
Interestingly, HA scaffolds with marrow stromal cells in a perfused environment were reported to result in ~85% increase in mean core strength, a ~130% increase in failure energy and a ~355% increase in post-failure strength. The increase in mineral quantity and promotion of uniform mineral distribution in that study was suggested to attribute to the perfusion effect [449]. Additionally, other investigators indicated mechanical properties increased for other calcium orthophosphate scaffolds after induced osteogenesis [448,451].
Furthermore, the dimensions, extent and interconnectivity of pores in bioceramics are known to influence bone in-growth, blood vessels formation and canaliculi networks [409,410,457]. Initial reports have estimated a minimum pore size of ~50 μm for blood vessel formation and a minimum pore size of ~200 μm for osteonal in-growth [457]. Pore dimensions of ~100 μm and even ~50 μm [592] were reported in later studies to support bone in-growth. Additionally, vascularization, cell migration and nutrient diffusion required for sustained cell viability and tissue function are possible if pores within the scaffolds are well interconnected. For example, an essential mean pore interconnection size of ~10 μm was necessary to allow cell migration between the pores [593]. As such, both porosity and general architecture are critical in determining the rate of fluid transport through porous bioceramics, which, in turn, determines the rate and degree of bone ingrowth in vivo [122,412,413,594].
8. Calcium Orthophosphate Bioceramics in Tissue Engineering
8.1. Tissue Engineering
All modern orthopedic implants lack three of the most critical abilities of living tissues: (i) self-repairing; (ii) maintaining blood supply; (iii) self-modifying their structure and properties in response to external aspects such as a mechanical load [429]. Needless to mention, bones not only possess all of these properties but, in addition, are self-generating, hierarchical, multifunctional, nonlinear, composite and biodegradable; therefore, the ideal artificial bone grafts must possess similar properties [117].
The last decades have seen a surge in creative ideas and technologies developed to tackle the problem of repairing or replacing diseased and damaged tissues, leading to the emergence of a new field in healthcare technology now referred to as tissue engineering. This is an interdisciplinary field that exploits a combination of living cells, engineering materials and suitable biochemical factors to improve, replace, restore, maintain or enhance living tissues and whole organs [595,596]. However, as two of three major components (namely, cells and biochemical factors) of the tissue engineering subject appear to be far beyond the scope of this review, the topic of tissue engineering is limited to the engineering materials prepared from calcium orthophosphate bioceramics only.
Regeneration, rather than repair, is the central goal of any tissue engineering strategy [597]. Thus, tissue engineering has potential to create tissues and organs de novo. This field of science [599] started more than two decades ago [600,601] and a famous review article by Langer and Vacanti [602] has greatly contributed to the promotion of tissue engineering research worldwide. The field of tissue engineering, particularly when applied to bone substitutes where tissues often function in a mechanically demanding environment [603], requires a collaboration of excellence in cell and molecular biology, biochemistry, material sciences, bioengineering and clinical research. For the success, it is necessary that researchers with expertise in one area have an appreciation of the knowledge and challenges of the other areas. However, since the technical, regulatory and commercial challenges might be substantial, the introduction of new products is likely to be slow [598].
Nowadays tissue engineering is at full research potential due to the following key advantages: (i) the solutions it provides are long-term, much safer than other options and cost-effective as well; (ii) the need for a donor tissue is minimal, which eliminates the immuno-suppression problems; (iii) the presence of residual foreign material is eliminated as well.
8.2. Scaffolds and Their Properties
It would be very convenient to both patients and physicians if devastated tissues or organs of patients could be regenerated by simple cell injections to the target sites, but such cases are rare. The majority of large-sized tissues and organs with distinct 3D form require a support for their formation from cells. The support is named a scaffold [604], template and/or artificial extracellular matrix (ECM) [151,152,386,600,603,605,606,607,608]. The major function of scaffolds is similar to that of the natural ECM that assists proliferation, differentiation and biosynthesis of cells. In addition, scaffolds placed at the regeneration sites will prevent disturbing cells from invasion into the sites of action [609,610]. The role of scaffolds was perfectly described by Andrés Segovia (1893–1987), a Spanish classical guitarist: “When one puts up a building one makes an elaborate scaffold to get everything into its proper place. But when one takes the scaffold down, the building must stand by itself with no trace of the means by which it was erected. That is how a musician should work.”
The idea behind tissue engineering is to create or engineer autografts by either expanding autologous cells in vitro guided by a scaffold or implanting an acellular template in vivo and allowing the patient’s cells to repair the tissue guided by the scaffold. The first phase is the in vitro formation of a tissue construct by placing the chosen cells and scaffolds in a metabolically and mechanically supportive environment with growth media (in a bioreactor), in which the cells proliferate and elaborate extracellular matrix. It is expected that cells infiltrate into the porous matrix and consequently proliferate and differentiate therein. In the second phase, the construct is implanted in the appropriate anatomic location, where remodeling in vivo is intended to recapitulate the normal functional architecture of an organ or a tissue [611,612]. The key processes occurring during both in vitro and in vivo phases of tissue formation and maturation are: (1) cell proliferation, sorting and differentiation, (2) extracellular matrix production and organization, (3) biodegradation of the scaffold, (4) remodeling and potentially growth of the tissue.
To achieve the goal of tissue reconstruction, the scaffolds must meet several specific requirements [151,152,605]. A reasonable surface roughness is necessary to facilitate cell seeding and fixation [613,614]. A sufficient mechanical strength and stiffness are mandatory to oppose contraction forces and later for the remodeling of damaged tissues. A high porosity and adequate pore dimensions (Table 2 and Table 6) are very important to allow cell migration, vascularization, as well as diffusion of nutrients [352]. Namely, scaffolds should have a network of interconnected pores where more than ~60% of the pores should have a size ranging from ~150 μm to ~400 μm and at least ~20% should be smaller than ~20 μm [11,105,352,362,362,409,410,411,412,413,414,415,457,615,616,617,618,619,620,621]. Scaffolds must be manufactured from materials with controlled biodegradability and/or bioresorbability, such as calcium orthophosphate bioceramics, so that new bone will eventually replace the scaffold [622]. Furthermore, the resorption rate has to coincide as much as possible with the rate of bone formation (i.e., between a few months and about two years) [623]. This means that while cells are fabricating their own natural matrix structure around themselves, the scaffold is able to provide structural integrity within the body and eventually it will break down leaving the newly formed tissue that will take over the mechanical load. Besides, scaffolds should be easily fabricated into a variety of shapes and sizes [624] and be malleable to fit irregularly shaped defects. In many cases, ease of processability, such as an easiness of conformation, and injectability of calcium orthophosphate cements and concretes [149,463,464], can determine the choice of a certain biomaterial. Finally, sterilization with no loss of properties is a crucial step in scaffold production at both a laboratory and an industrial level [603]. In conclusion, since calcium and orthophosphate ions regulate bone metabolism, calcium orthophosphates appear to be among the few bone graft substitute materials that can be considered as a drug [1].
Table 6.
A hierarchical pore size distribution that an ideal scaffold should exhibit [11].
| Pore sizes of a 3D scaffold | Biochemical effect or function |
|---|---|
| <1 μm | Interaction with proteins |
| Responsible for bioactivity | |
| 1–20 μm | Type of cells attracted |
| Cellular development | |
| Orientation and directionality of cellular ingrowth | |
| 100–1000 μm | Cellular growth |
| Bone ingrowth | |
| Predominant function in the mechanical strength | |
| >1000 μm | Implant functionality |
| Implant shape | |
| Implant esthetics |
Many fabrication techniques are available to produce porous calcium orthophosphate scaffolds (Table 2) with varying architectural features (for details, see “Forming and shaping” and “Porosity” sections above). In order to achieve the desired properties at minimum expense, the production process should be optimized [625]. With the advent of tissue engineering, the search is on for the ultimate option—a “tissue engineered bone substitute”, consisting of a synthetic calcium orthophosphate scaffold impregnated with cells and growth factors. Figure 13 schematically depicts a possible fabrication process of such an item that, afterwards, will be implanted into a living organism to induce bone regeneration [42,52].
From the structural perspective, a degree of scaffold porosity is responsible for regulating the bioactivity of bone graft substitutes as a function of its influence on structural permeability, which controls the initial rate of bone regeneration and the local mechanical environment, which mediates the equilibrium volume of new bone within the repair site. Parameters such as pore interconnectivity, pore geometry, strut topography and strut porosity all contribute to modulate this process of osteogenesis and act synergistically to promote or screen the osteoconductive or osteoinductive potential of bone graft substitutes [412,626,627]. However, since bones have very different structures depending on their functions and locations, the same pore sizes and shapes may not be ideal for all potential uses. Therefore, bioceramic scaffolds of various porosities are required.

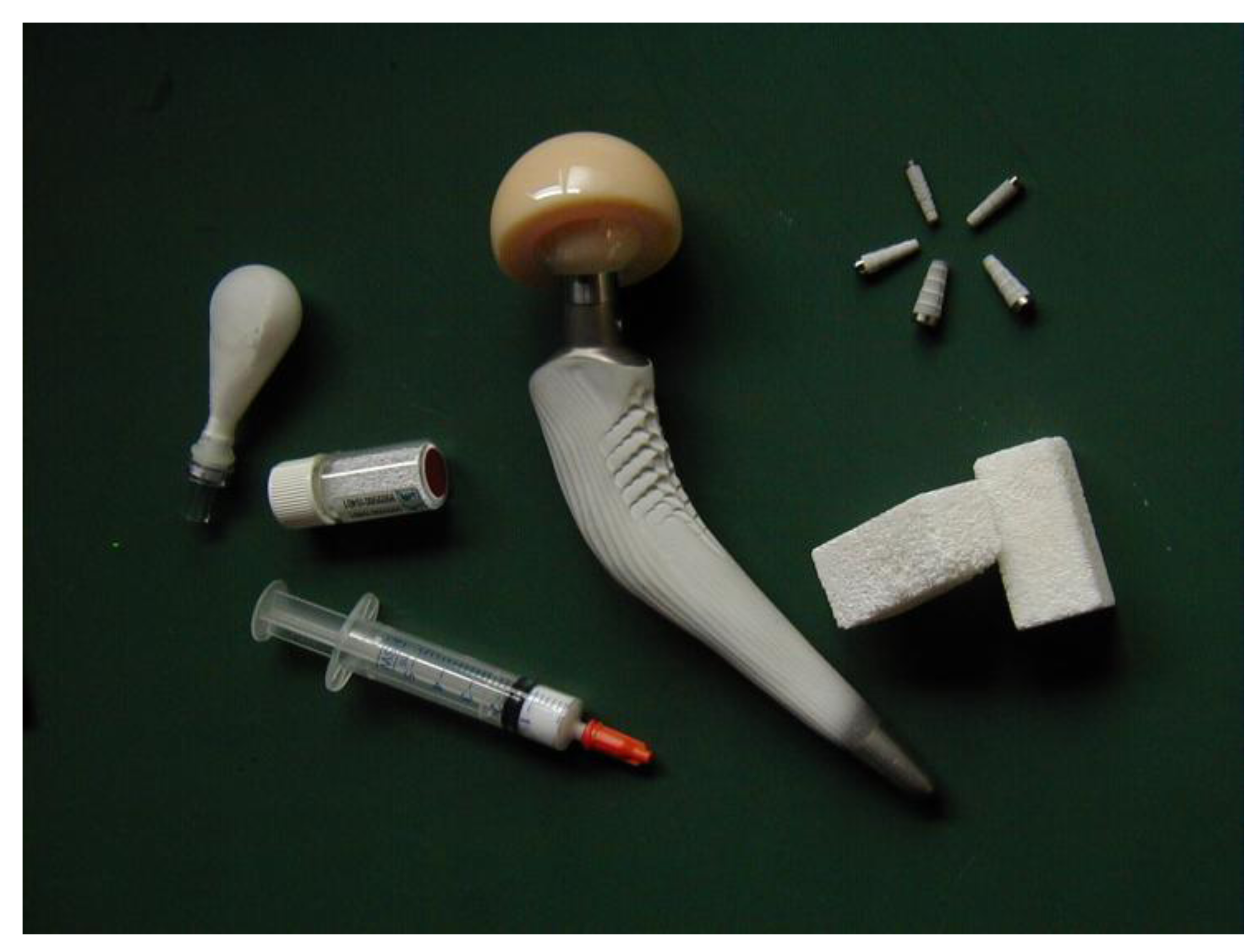{kind=link}
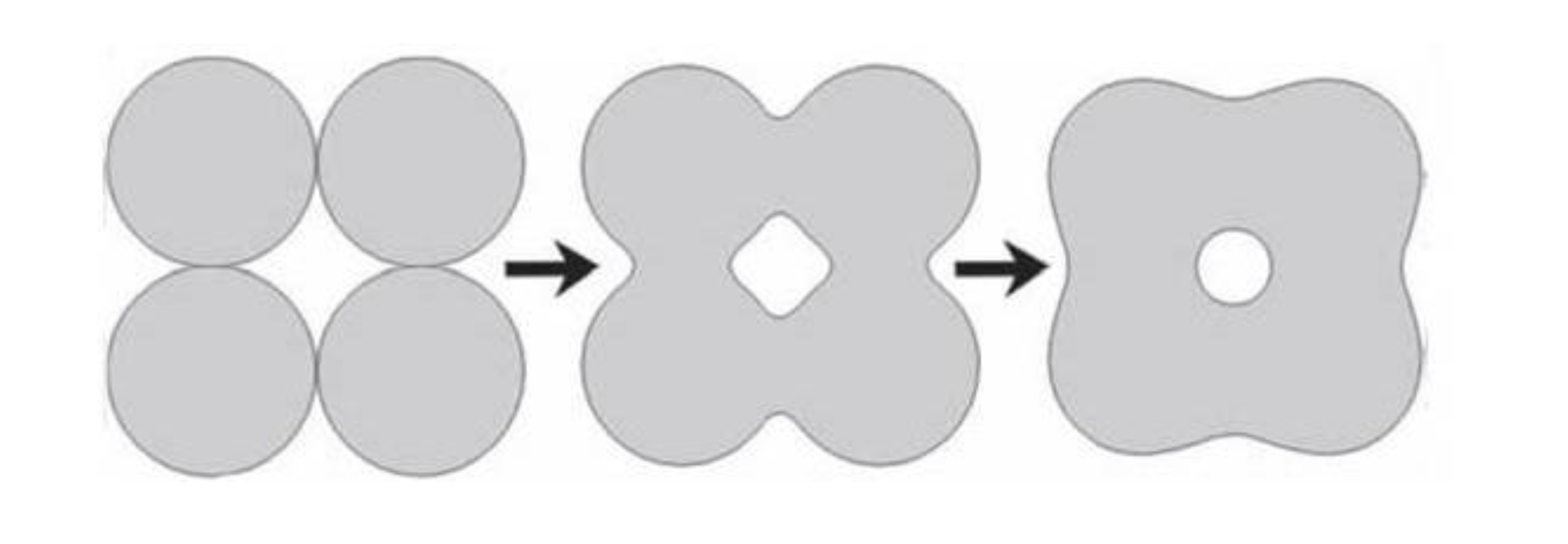{kind=link}
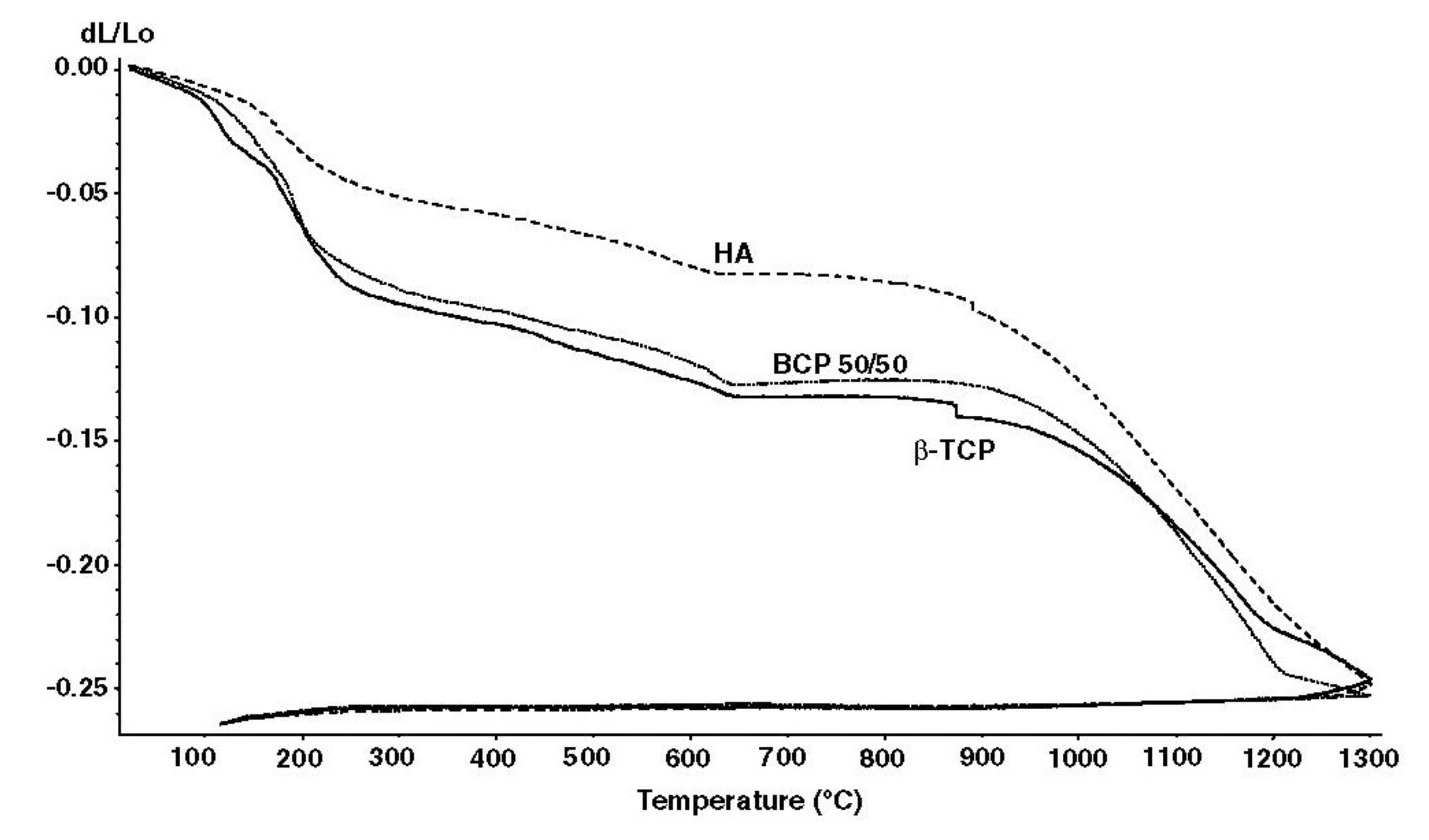{kind=link}
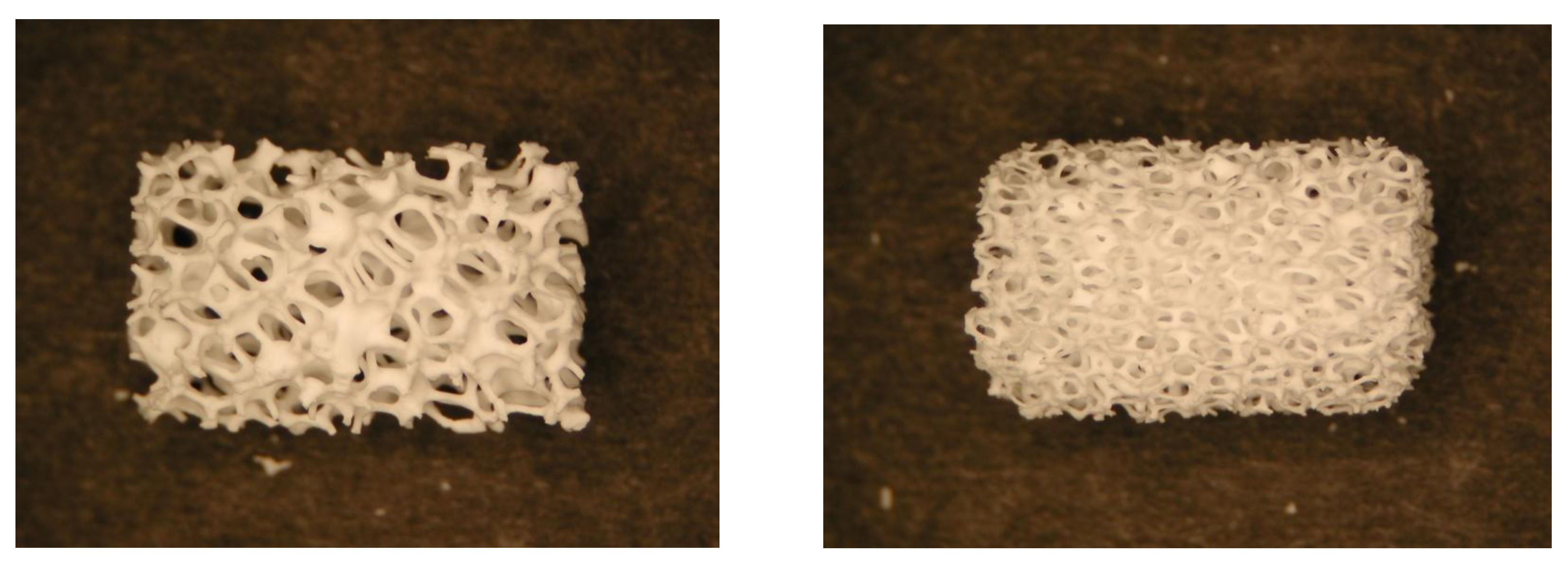{kind=link}
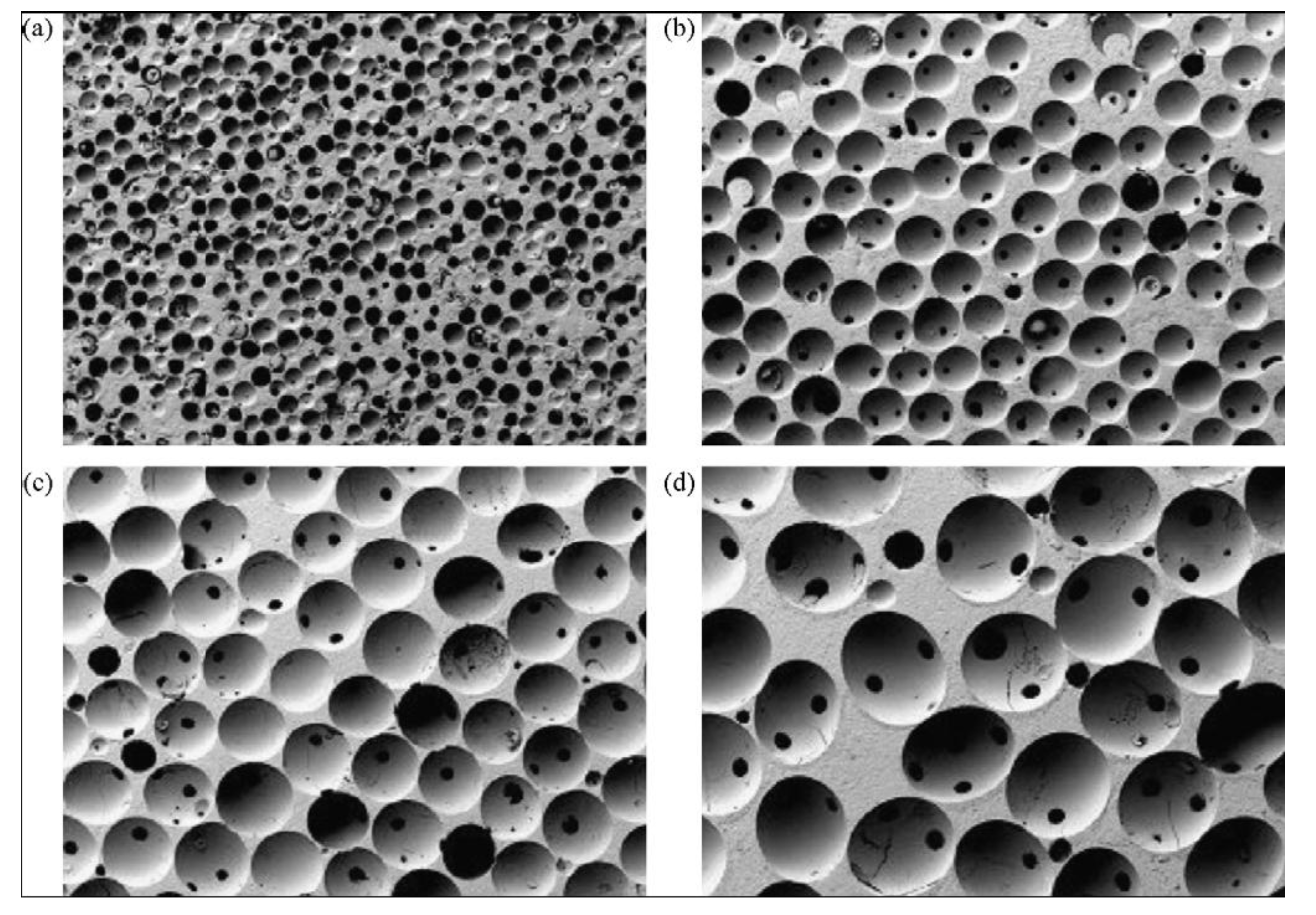{kind=link}
{kind=link}
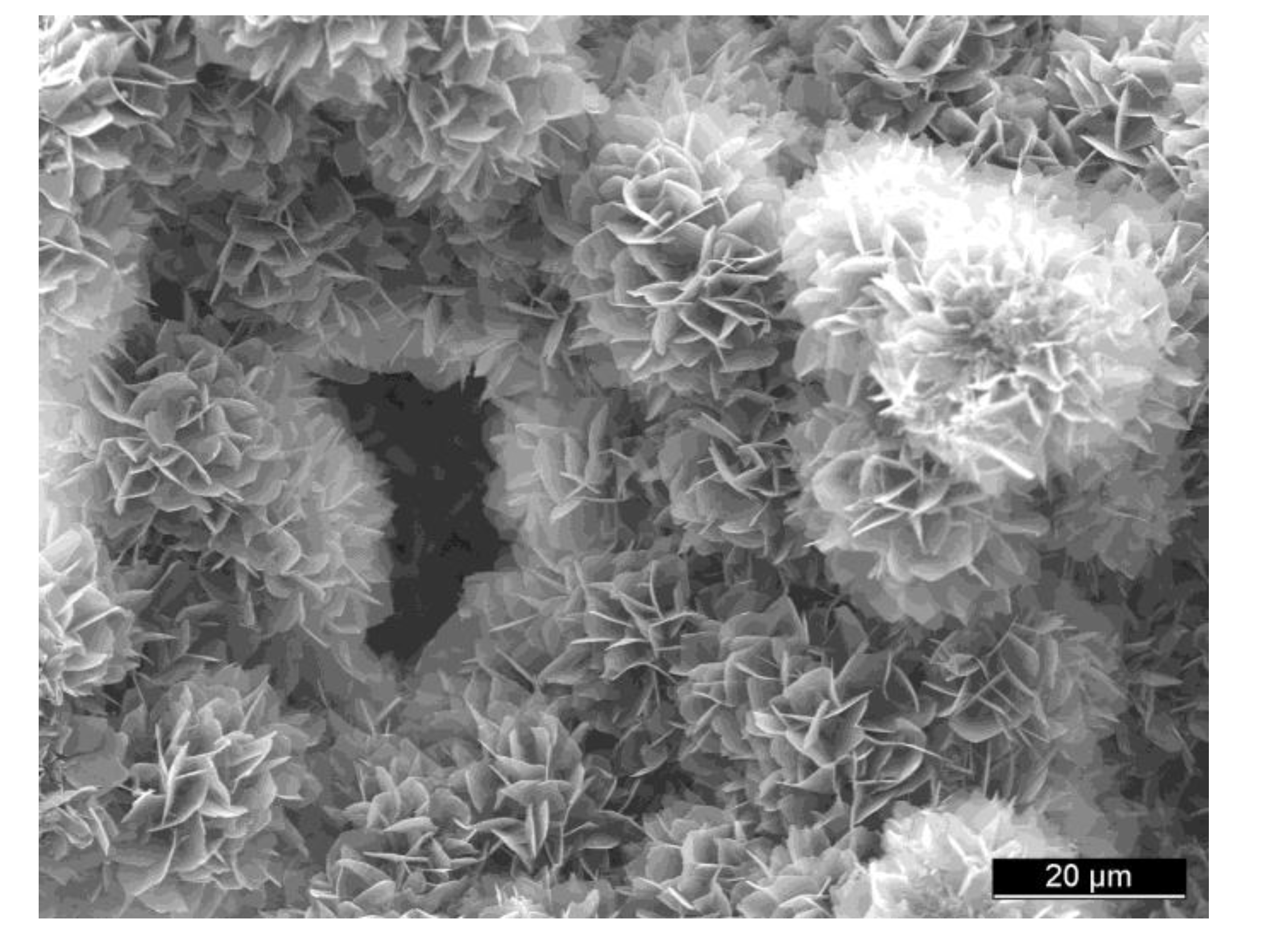{kind=link}
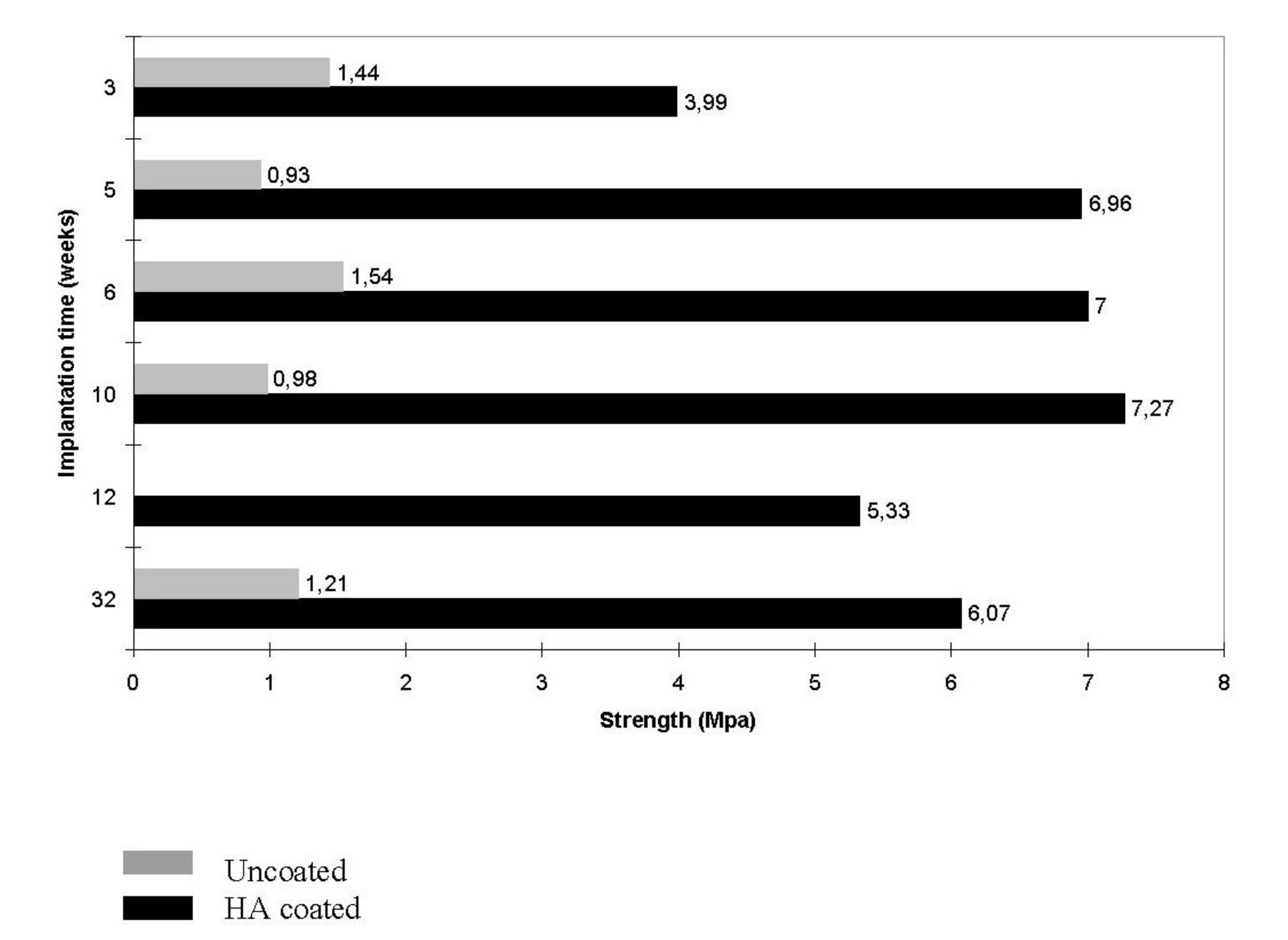{kind=link}
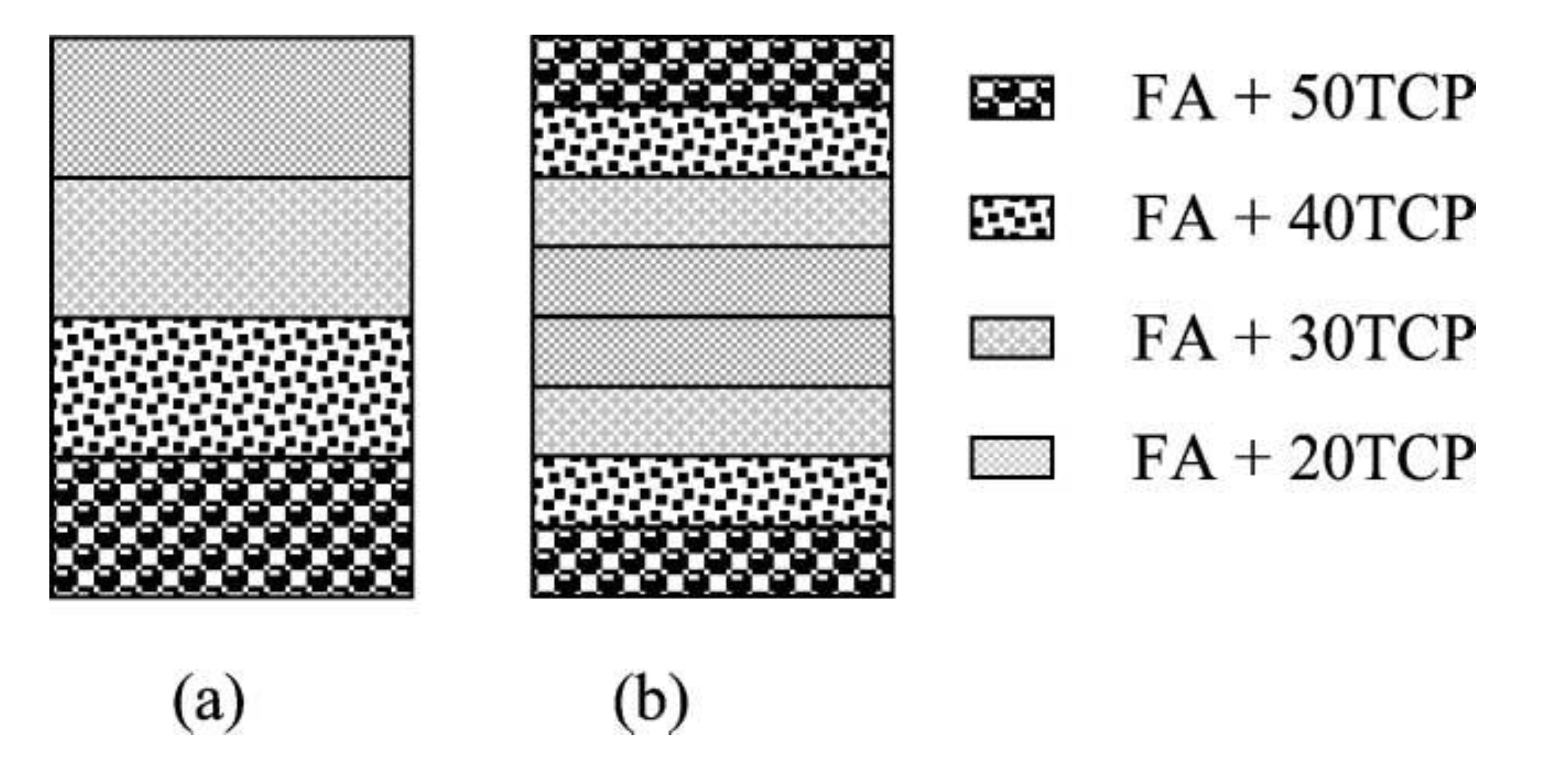{kind=link}
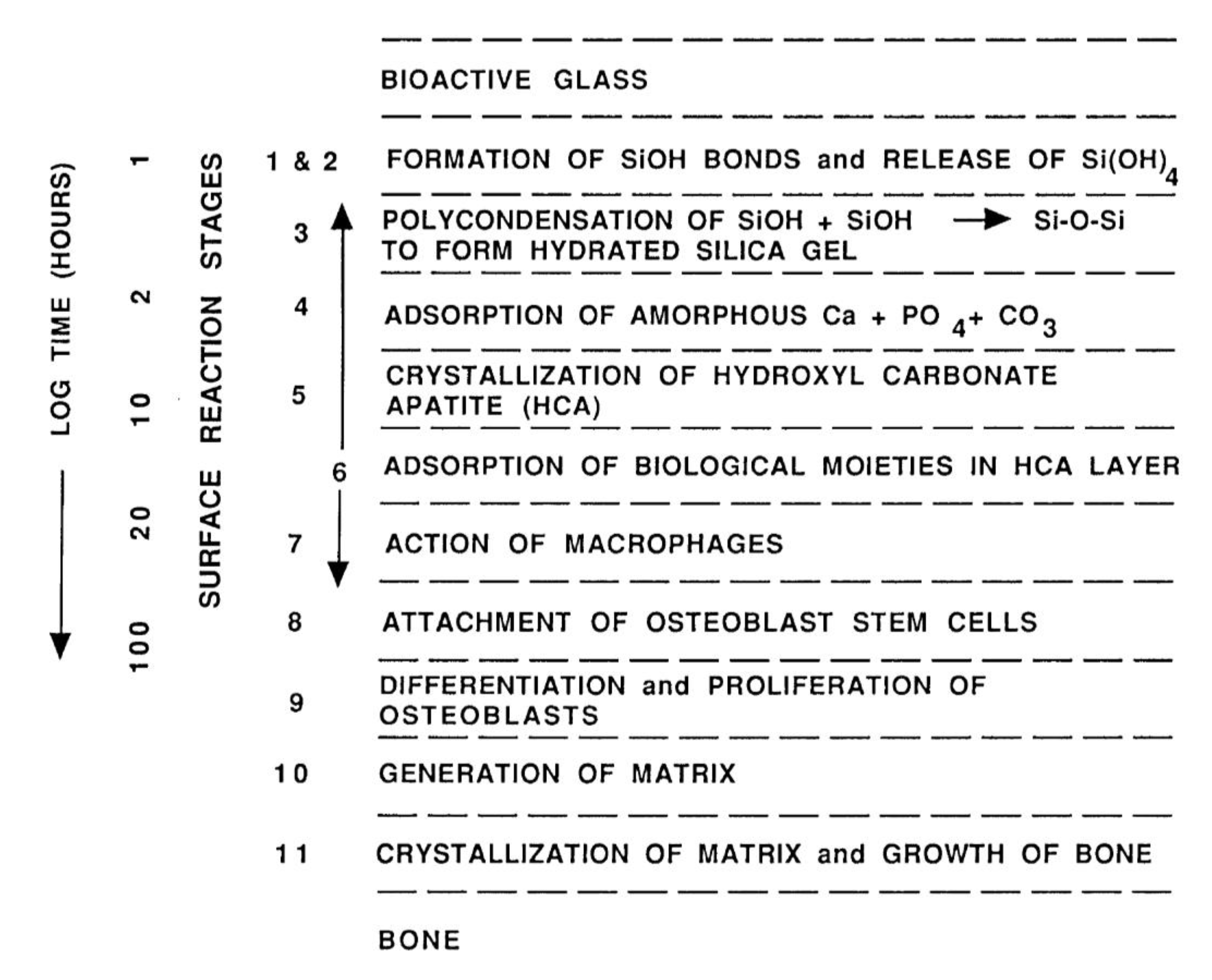{kind=link}
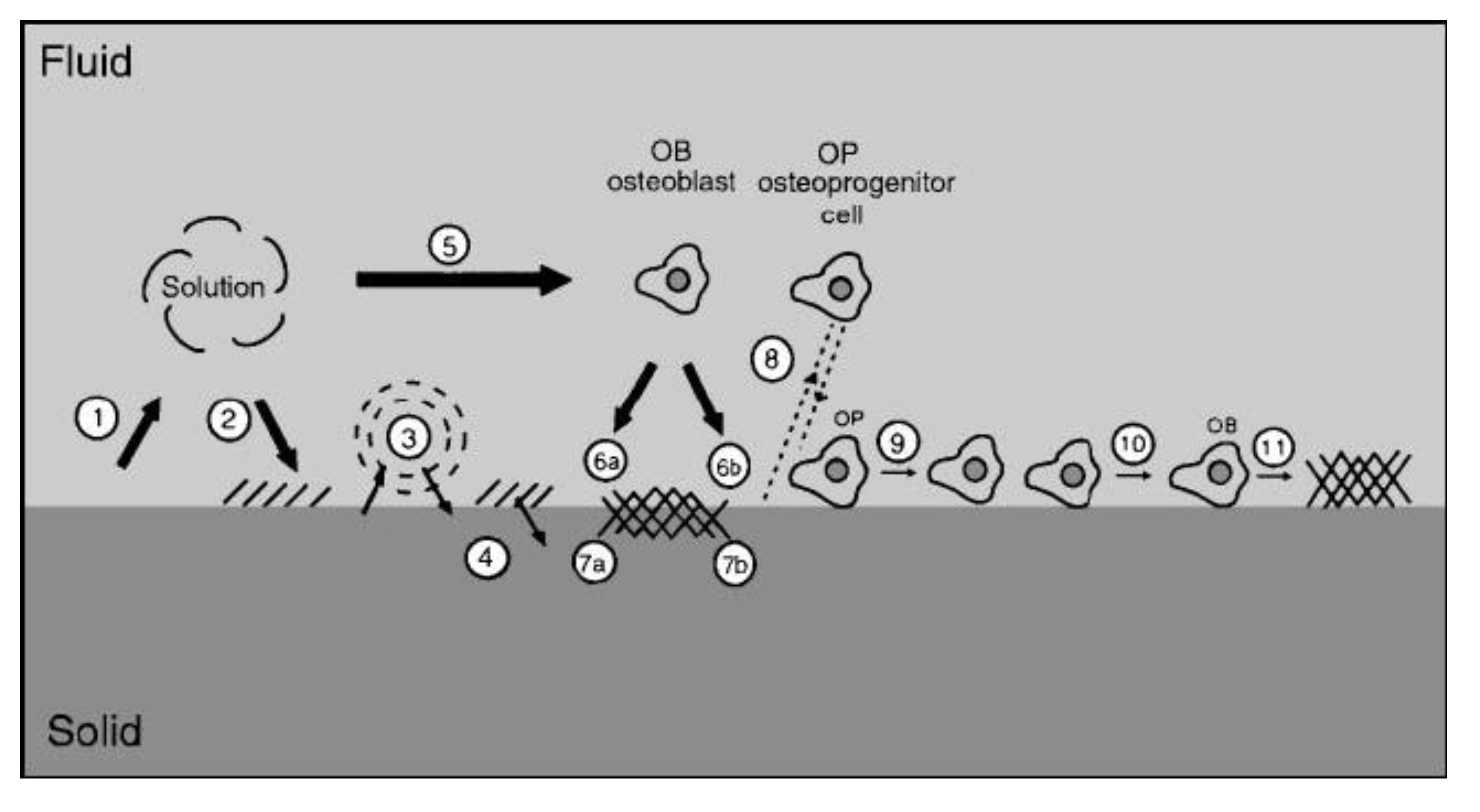{kind=link}
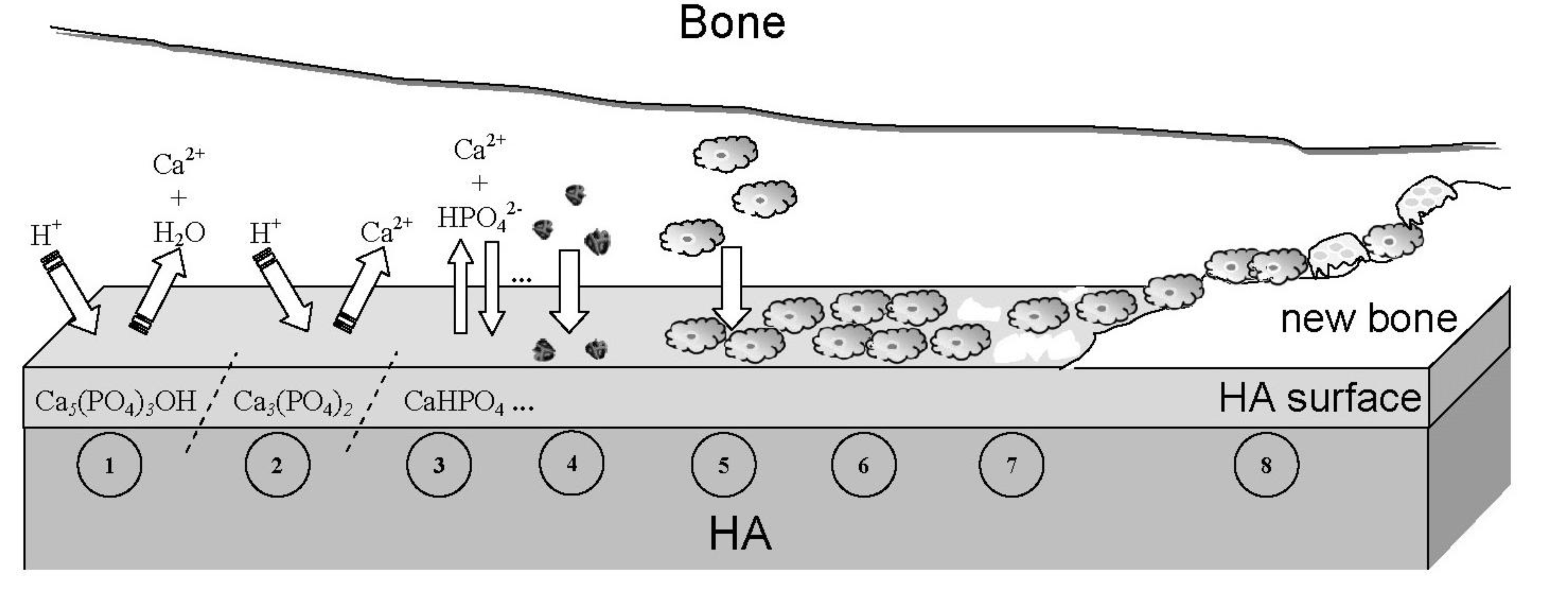{kind=link}
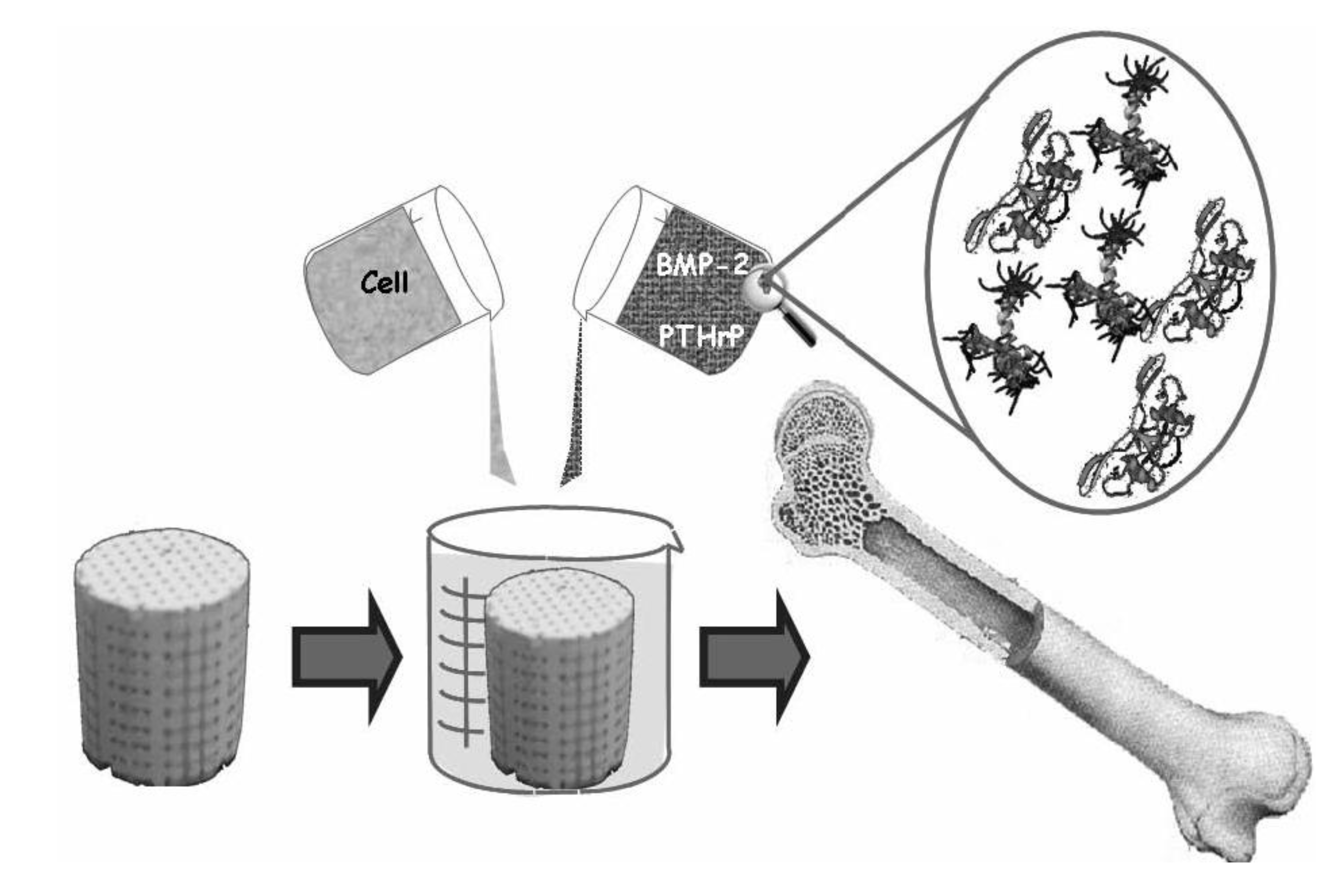{kind=link}
8.3. Scaffolds from Calcium Orthophosphate Bioceramics
Philosophically, the increase in life expectancy requires biological solutions to orthopedic problems previously managed with mechanical solutions. Therefore, since the end of 1990s, biomaterials research has focused on tissue regeneration instead of tissue replacement [628]. The alternatives include use of hierarchical bioactive scaffolds to engineer in vitro living cellular constructs for transplantation or use of bioresorbable bioactive particulates or porous networks to activate in vivo the mechanisms of tissue regeneration [629,630]. Thus, the aim of calcium orthophosphate bioceramics is to prepare artificial porous scaffolds able to provide the physical and chemical cues to guide cell seeding, differentiation and assembly into 3D tissues of a newly formed bone [587,631,632,633,634,635]. Particle sizes, shape and surface roughness of scaffolds are known to affect cellular adhesion, proliferation and phenotype. Additionally, the surface energy may play a role in attracting particular proteins to the bioceramic surface and, in turn, will affect the cells’ affinity to the material. More to the point, cells are exceedingly sensitive to chemical composition and their bone-forming functions can be dependent on grain morphology of the scaffolds. For example, osteoblast functions were found to increase on nanofiber structures if compared to nanospherical ones because nanofibers more closely approximate the shape of biological apatite in bones [636]. Besides, a significantly higher osteoblast proliferation on HA bioceramics sintered at 1200 °C as compared to that on HA bioceramics sintered at 800 °C and 1000 °C was reported [637]. Thus, to meet the tissue engineering requirements, much attention is devoted to further improvements of calcium orthophosphate bioceramics [638]. From the chemical point of view, the development includes synthesis of novel ion-substituted calcium orthophosphates [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37]. From the material point of view, the major research topics include nanodimensional and nanocrystalline structures [639,640,641,642,643], organic-inorganic biocomposites and hybrid biomaterials [292], fibers, whiskers and filaments [644,645,646,647,648,649,650,651,652,653,654,655,656], micro- and nanospheres and beads [656,657,658,659,660,661,662,663,664,665,666,667,668,669], porous 3D scaffolds made of ACP [418], TCP [396,397], HA [167,364,365,398,400,441,625,670,671,672,673,674,675] and various biphasic formulations [440,667,676,677,678,679,680], structures with graded porosity [377,438,440,524,525,526,527,528,529] and hierarchically organized ones [681,682]. Furthermore, an addition of defects through an intensive milling [683,684] or their removal by a thermal treatment [685] can be used to modify a chemical reactivity of calcium orthophosphates. In addition, more attention should be paid to crystallographically aligned calcium orthophosphate bioceramics [686].
There are three principal therapeutic strategies for treating diseased or injured tissues in patients: (i) implantation of freshly isolated or cultured cells; (ii) implantation of tissues assembled in vitro from cells and scaffolds; (iii) in situ tissue regeneration. For cellular implantation, individual cells or small cellular aggregates from the patient or a donor are either injected into the damaged tissue directly or are combined with a degradable scaffold in vitro and then implanted. For tissue implantation, a complete 3D tissue is grown in vitro using patient or donor cells and a bioresorbable scaffold and then is implanted into the patients to replace diseased or damaged tissues. For in situ regeneration, a scaffold implanted directly into the injured tissue stimulates the body’s own cells to promote local tissue repair [595,687]. In any case, simply trapping cells at the particular point on a surface is not enough: the cells must be encouraged to differentiate, which is impossible without the presence of suitable biochemical factors [688]. All the previously mentioned clearly indicate that for the purposes of tissue engineering, calcium orthophosphate bioceramics play an auxiliary role; namely, they act as a suitable material to manufacture the appropriate 3D templates, substrates or scaffolds to be colonized by living cells before the successive implantation. The in vitro evaluation of potential calcium orthophosphate scaffolds for tissue engineering has been described elsewhere [689], and data on the mechanical properties of calcium orthophosphate bioceramics for use in tissue engineering are also available [690,691]. The effect of a HA-based biomaterial on gene expression in osteoblast-like cells was reported as well [692]. To conclude, the excellent biocompatibility of calcium orthophosphate bioceramics, their possible osteoinductivity [168,415,457,551,552,553,554,555,556,557,558,559,560,561,562,563] and a high affinity for drugs, proteins and cells make them very functional for tissue engineering applications. The feasible production of scaffolds with tailored structures and properties opens up a spectacular future for calcium orthophosphates [692,693,694,695,696,697,698,699].
8.4. A Clinical Experience
During the last decade, several groups have made steps towards a clinical application of cell-seeded calcium orthophosphate bioceramics for bone tissue engineering of humans. For example, Quarto et al. [700] were the first to report treatment of large (4–7 cm) bone defects of the tibia, ulna and humerus in three patients from 16 to 41 years old, where conventional surgical therapies had failed. The authors implanted a custom-made unresorbable porous HA scaffold seeded with in vitro expanded autologous bone marrow stromal cells. In all three patients, radiographs and computed tomographic scans revealed abundant callus formation along the implants and good integration at the interfaces with the host bones by the second month after surgery [700]. In the same year, Vacanti et al. [701] reported the case of a man who had a traumatic avulsion of the distal phalanx of a thumb. The phalanx was replaced with a specially treated natural coral (porous HA; 500-pore ProOsteon (see Table 3)) implant that was previously seeded with in vitro expanded autologous periosteal cells. The procedure resulted in the functional restoration of a stable and biomechanically sound thumb of normal length, without the pain and complications that are usually associated with harvesting a bone graft.
Morishita et al. [702] treated a defect resulting from surgery of benign bone tumors in three patients using HA scaffolds seeded with in vitro expanded autologous bone marrow stromal cells after osteogenic differentiation of the cells. Two bone defects in a tibia and one defect in a femur were treated. Although ectopic implants in nude mice showed the osteogenicity of the cells, details such as the percentage of the implants containing bone and at what quantities were not reported. Furthermore, cell-seeded calcium orthophosphate scaffolds were found to be superior to autograft, allograft or cell-seeded allograft in terms of bone formation at ectopic implantation sites [703].
To conclude this part, one should mention that a cell seeding method for practical clinical experience is not enough. Although cell seeding into scaffolds at high density is closely associated with enhancement of tissue formation in 3D constructs (i.e., cartilage [704] and bone [705]), effective and high-density cell seeding into 3D scaffolds is difficult to achieve. Technical difficulties in cell seeding are caused by the complex structure of the scaffold and insufficient migration into the scaffolds due to pore size and material, which prolongs the culture period because of the shortage of initially seeded cells. Recently, Shimizu et al. [706] proposed a methodology for tissue engineering using magnetite nanoparticles and magnetic force. This method has been applied to a cell seeding process and attractive results have been reported.
9. Conclusions and Outlook
The available chronology of the search for a suitable bioceramic for bone substitutes is as follows: since the 1950s, the first aim was to use bioinert [533] bioceramics, which had no reaction with living tissues. Later on, in the 1980s, the trend changed towards the opposite: the idea was to implant bioceramics that reacted with the surrounding tissues by producing newly formed bone. These two stages have been referred to as the first and the second generations of bioceramics, respectively [707]. In the current century, we search for the third generation of bioceramics [687], which will be able to regenerate bone tissues by stimulating specific responses at the molecular level [42,52]. One should note that these three generations should not be interpreted as the chronological but the conceptual, since each generation represents an evolution on the requirements and properties of the biomaterials involved. This means that at present, research and development is still devoted to biomaterials and bioceramics that, according to their properties, could be considered to be of the first or the second generations, because the second generation of bioceramics with added porosity is one of the initial approaches in developing the third generation of bioceramics [708]. Furthermore, there is another classification of the history of biomaterials introduced by James M. Anderson. According to Anderson, between 1950–1975, researchers studied biomaterials, between 1975–2000 they studied biomaterials and since 2000 the time for biomaterials has been coming [709]; here, the italicized letters emphasize the major direction of the research efforts in the complex subject of biomaterials. As bioceramics are biomaterials of the ceramic origin (see Section 2), Anderson’s historical classification appears to be applicable to the bioceramics field.
The field of biomaterials is in the midst of a revolutionary change in which the life sciences are becoming equal in importance to materials science and engineering as the foundation of the field. Simultaneously, advances in engineering (for example nanotechnology) are greatly increasing the sophistication with which biomaterials can be designed, allowing fabrication of biomaterials with increasingly complex functions [76]. Specifically, during the last ~40 years, calcium orthophosphate bioceramics has become an integral and vital segment of our modern health care delivery system. In the modern fields of the third generation bioceramics (Hench) or BIOceramics (Anderson), the full potential of calcium orthophosphates has only begun to be recognized. Namely, calcium orthophosphates, which were intended as osteoconductive bioceramics in the past, stand for materials to fabricate osteoinductive implants nowadays [168,415,457,551,552,553,554,555,556,557,558,559,560,561,562,563]. The initial steps in this direction have been already made by both fabricating BCP-based scaffolds for bone tissue engineering through the design of controlled 3D-porous structures and increasing the biological activity through development of novel ion-substituted calcium orthophosphate bioceramics [11,417]. In the future, the composition, microstructure and molecular surface chemistry of various types of calcium orthophosphates will be tailored to match the specific biological and metabolic requirements of tissues or disease states. This new generation of calcium orthophosphate bioceramics should enhance the quality of life of millions of people as they grow older [710].
In spite of the great progress, there is still great potential for major advances to be made in the field of calcium orthophosphate bioceramics [4]. This includes requirements for:
- Improvement of the mechanical performance of existing types of bioceramics;
- Enhanced bioactivity in terms of gene activation;
- Improvement in the performance of biomedical coatings in terms of their mechanical stability and ability to deliver biological agents;
- Development of smart biomaterials capable of combining sensing with bioactivity;
- Development of improved biomimetic composites.
Furthermore, there is still need for a better understanding of the biological systems. For example, the bonding mechanism between the bone mineral and collagen remains unclear. It is also unclear whether a rapid repair that is elicited by the new generation of bioceramics results from the enhancement of mineralization per se or whether there is a more complex signaling process involving proteins in collagen. If we were able to understand the fundamentals of bone response to specific ions and the signals they activate, then we could design better bioceramics for the future [4].
To finalize this review, it is obvious that the present status of research and development in the field of calcium orthophosphate bioceramics is still at the starting point for the solution of new problems at the confluence of materials science, biology and medicine, concerned with the restoration of damaged functions in humans. A large increase in active elderly people has dramatically raised the need for load-bearing bone graft substitutes, for example for bone reconstruction during revision arthroplasty or for the reinforcement of osteoporotic bones. Strategies applied in the last four decades towards this goal have failed. New strategies, possibly based on self-assembling and/or nanofabrication, have to be proposed and developed [711]. Furthermore, it should be feasible to design a new generation of gene-activating calcium orthophosphate based scaffolds tailored for specific patients and disease states in the future. Perhaps, bioactive stimuli will be used to activate genes in a preventative treatment to maintain the health of aging tissues. Currently this concept seems impossible. However, we need to remember that only ~40 years ago the concept of a material that would not be rejected by living tissues also seemed impossible [542].
Acknowledgements
Many thanks to the contributors, who kindly agreed to permit reproducing the figures.
References and Notes
- Bohner, M. Resorbable biomaterials as bone graft substitutes. Mater. Today 2010, 13, 24–30. [Google Scholar] [CrossRef]
- Doremus, R.H. Bioceramics. J. Mater. Sci. 1992, 27, 285–297. [Google Scholar] [CrossRef]
- Vallet-Regí, M. Ceramics for medical applications. J. Chem. Soc. Dalton Trans. 2001, 97–108. [Google Scholar] [CrossRef]
- Best, S.M.; Porter, A.E.; Thian, E.S.; Huang, J. Bioceramics: Past, present and for the future. J. Eur. Ceram. Soc. 2008, 28, 1319–1327. [Google Scholar] [CrossRef]
- Vallet-Regí, M. Evolution of bioceramics within the field of biomaterials. C. R. Chimie 2010, 13, 174–185. [Google Scholar] [CrossRef]
- Rahaman, M.N.; Yao, A.; Bal, B.S.; Garino, J.P.; Ries, M.D. Ceramics for prosthetic hip and knee joint replacement. J. Am. Ceram. Soc. 2007, 90, 1965–1988. [Google Scholar] [CrossRef]
- Langstaff, S.D.; Sayer, M.; Smith, T.J.N.; Pugh, S.M.; Hesp, S.A.M.; Thompson, W.T. Resorbable bioceramics based on stabilized calcium phosphates. Part I: Rational design, sample preparation and material characterization. Biomaterials 1999, 20, 1727–1741. [Google Scholar] [CrossRef]
- Langstaff, S.D.; Sayer, M.; Smith, T.J.N.; Pugh, S.M. Resorbable bioceramics based on stabilized calcium phosphates. Part II: Evaluation of biological response. Biomaterials 2001, 22, 135–150. [Google Scholar] [CrossRef]
- Sayer, M.; Stratilatov, A.D.; Reid, J.W.; Calderin, L.; Stott, M.J.; Yin, X.; MacKenzie, M.; Smith, T.J.N.; Hendry, J.A.; Langstaff, S.D. Structure and composition of silicon-stabilized tricalcium phosphate. Biomaterials 2003, 24, 369–382. [Google Scholar] [CrossRef]
- Reid, J.W.; Pietak, A.M.; Sayer, M.; Dunfield, D.; Smith, T.J.N. Phase formation and evolution in the silicon substituted tricalcium phosphate/apatite system. Biomaterials 2005, 26, 2887–2897. [Google Scholar] [CrossRef]
- Sanchez-Sálcedo, S.; Arcos, D.; Vallet-Regí, M. Upgrading calcium phosphate scaffolds for tissue engineering applications. Key Eng. Mater. 2008, 377, 19–42. [Google Scholar] [CrossRef]
- Ito, A.; LeGeros, R.Z. Magnesium- and zinc-substituted beta-tricalcium phosphates as potential bone substitute biomaterials. Key Eng. Mater. 2008, 377, 85–98. [Google Scholar] [CrossRef]
- Ergun, C.; Webster, T.J.; Bizios, R.; Doremus, R.H. Hydroxylapatite with substituted magnesium, zinc, cadmium, and yttrium. I. Structure and microstructure. J. Biomed. Mater. Res. 2002, 59, 305–311. [Google Scholar] [CrossRef]
- Webster, T.J.; Ergun, C.; Doremus, R.H.; Bizios, R. Hydroxylapatite with substituted magnesium, zinc, cadmium, and yttrium. II. Mechanisms of osteoblast adhesion. J. Biomed. Mater. Res. 2002, 59, 312–317. [Google Scholar] [CrossRef]
- Kim, S.R.; Lee, J.H.; Kim, Y.T.; Riu, D.H.; Jung, S.J.; Lee, Y.J.; Chung, S.C.; Kim, Y.H. Synthesis of Si, Mg substituted hydroxyapatites and their sintering behaviors. Biomaterials 2003, 24, 1389–1398. [Google Scholar] [CrossRef]
- Patel, N.; Best, S.M.; Bonfield, W. Characterisation of hydroxyapatite and substituted-hydroxyapatites for bone grafting. J. Australas. Ceram. Soc. 2005, 41, 1–22. [Google Scholar]
- Vallet-Regí, M.; Arcos, D. Silicon substituted hydroxyapatites. A method to upgrade calcium phosphate based implants. J. Mater. Chem. 2005, 15, 1509–1516. [Google Scholar] [CrossRef]
- Landi, E.; Celotti, G.; Logroscino, G.; Tampieri, A. Carbonated hydroxyapatite as bone substitute. J. Eur. Ceram. Soc. 2003, 23, 2931–2937. [Google Scholar] [CrossRef]
- Gbureck, U.; Thull, R.; Barralet, J.E. Alkali ion substituted calcium phosphate cement formation from mechanically activated reactants. J. Mater. Sci. Mater. Med. 2005, 16, 423–427. [Google Scholar] [CrossRef]
- Kannan, S.; Ventura, J.M.; Ferreira, J.M.F. In situ formation and characterization of flourine-substituted biphasic calcium phosphate ceramics of varied F-HAP / β-TCP ratios. Chem. Mater. 2005, 17, 3065–3068. [Google Scholar] [CrossRef]
- Tas, A.C.; Bhaduri, S.B.; Jalota, S. reparation of Zn-doped β-tricalcium phosphate (β-Ca3(PO4)2) bioceramics. Mater. Sci. Eng. C 2007, 27, 394–401. [Google Scholar] [CrossRef]
- Gbureck, U.; Knappe, O.; Grover, L.M.; Barralet, J.E. Antimicrobial potency of alkali ion substituted calcium phosphate cements. Biomaterials 2005, 26, 6880–6886. [Google Scholar] [CrossRef]
- Tardei, C.; Grigore, F.; Pasuk, I.; Stoleriu, S. The study of Mg2+/Ca2+ substitution of β-tricalcium phosphate. J. Optoelectron. Adv. Mater. 2006, 8, 568–571. [Google Scholar]
- Pietak, A.M.; Reid, J.W.; Stott, M.J.; Sayer, M. Silicon substitution in the calcium phosphate bioceramics. Biomaterials 2007, 28, 4023–4032. [Google Scholar] [CrossRef]
- Yao, Z.P.; Liu, W.G.; Ni, G.X. Biology characteristics and clinical application of strontium substituted hydroxyapatite bone cement. J. Clin. Rehabil. Tissue Eng. Res. 2008, 12, 7151–7154. [Google Scholar]
- Landi, E.; Tampieri, A.; Mattioli-Belmonte, M.; Celotti, G.; Sandri, M.; Gigante, A.; Fava, P.; Biagini, G. Biomimetic Mg- and Mg,CO3-substituted hydroxyapatites: Synthesis characterization and in vitro behaviour. J. Eur. Ceram. Soc. 2006, 26, 2593–2601. [Google Scholar] [CrossRef]
- Landi, E.; Tampieri, A.; Celotti, G.; Sprio, S.; Sandri, M.; Logroscino, G. Sr-substituted hydroxyapatites for osteoporotic bone replacement. Acta Biomater. 2007, 3, 961–969. [Google Scholar] [CrossRef]
- Kannan, S.; Ventura, J.M.G.; Ferreira, J.M.F. Synthesis and thermal stability of potassium substituted hydroxyapatites and hydroxyapatite/β-tricalcium phosphate mixtures. Ceram. Int. 2007, 33, 1489–1494. [Google Scholar] [CrossRef]
- Kannan, S.; Rebelo, A.; Lemos, A.F.; Barba, A.; Ferreira, J.M.F. Synthesis and mechanical behaviour of chlorapatite and chlorapatite/β-TCP composites. J. Eur. Ceram. Soc. 2007, 27, 2287–2294. [Google Scholar] [CrossRef]
- Kannan, S.; Goetz-Neunhoeffer, F.; Neubauer, J.; Ferreira, J.M.F. Ionic substitutions in biphasic hydroxyapatite and β-tricalcium phosphate mixtures: Structural analysis by Rietveld refinement. J. Am. Ceram. Soc. 2008, 91, 1–12. [Google Scholar]
- Lafon, J.P.; Champion, E.; Bernache-Assollant, D. Processing of AB-type carbonated hydroxyapatite Ca10−x(PO4)6−x(CO3)x(OH)2−x−2y(CO3)y ceramics with controlled composition. J. Eur. Ceram. Soc. 2008, 28, 139–147. [Google Scholar] [CrossRef]
- Ren, F.; Xin, R.; Ge, X.; Leng, Y. An experimental and computational study on Zn-substituted hydroxyapatite. Adv. Mater. Res. 2008, 47-50, 1379–1382. [Google Scholar] [CrossRef]
- Meejoo, S.; Pon-On, W.; Charnchai, S.; Amornsakchai, T. Substitution of iron in preparation of enhanced thermal property and bioactivity of hydroxyapatite. Adv. Mater. Res. 2008, 55-57, 689–692. [Google Scholar] [CrossRef]
- Kannan, S.; Goetz-Neunhoeffer, F.; Neubauer, J.; Ferreira, J.M.F. Synthesis and structure refinement of zinc-doped β-tricalcium phosphate powders. J. Am. Ceram. Soc. 2009, 92, 1592–1595. [Google Scholar]
- Natasha, A.N.; Sopyan, I.; Zuraida, A. Fourier transform infrared study on sol-gel derived manganese-doped hydroxyapatite. Adv. Mater. Res. 2008, 47-50, 1185–1188. [Google Scholar] [CrossRef]
- Matsumoto, N.; Yoshida, K.; Hashimoto, K.; Toda, Y. Thermal stability of β-tricalcium phosphate doped with monovalent metal ions. Mater. Res. Bull. 2009, 44, 1889–1894. [Google Scholar] [CrossRef]
- Boanini, E.; Gazzano, M.; Bigi, A. Ionic substitutions in calcium phosphates synthesized at low temperature. Acta Biomater. 2010, 6, 1882–1894. [Google Scholar] [CrossRef]
- Williams, D.F. The Williams Dictionary of Biomaterials; Liverpool University Press: Liverpool, UK, 1999; p. 368. [Google Scholar]
- Williams, D.F. On the nature of biomaterials. Biomaterials 2009, 30, 5897–5909. [Google Scholar] [CrossRef]
- Jandt, K.D. Evolutions, revolutions and trends in biomaterials science—A perspective. Adv. Eng. Mater. 2007, 9, 1035–1050. [Google Scholar] [CrossRef]
- Biomimetic Materials Chemistry; Mann, S. (Ed.) Wiley-VCH: Weinheim, Germany, 1996; p. 400.
- Vallet-Regí, M. Bioceramics: Where do we come from and which are the future expectations. Key Eng. Mater. 2008, 377, 1–18. [Google Scholar] [CrossRef]
- Meyers, M.A.; Chen, P.Y.; Lin, A.Y.M.; Seki, Y. Biological materials: Structure and mechanical properties. Prog. Mater. Sci. 2008, 53, 1–206. [Google Scholar] [CrossRef]
- According to Wikipedia, the free encyclopedia: “The word ceramic comes from the Greek word κεραμικός (keramikos) meaning pottery, which is said to derive from the Indo-European word ker, meaning heat. A ceramic is an inorganic, non-metallic solid prepared by the action of heat and subsequent cooling. Ceramic materials may have a crystalline or partly crystalline structure, or may be amorphous (e.g., a glass). Because most common ceramics are crystalline, the definition of ceramic is often restricted to inorganic crystalline materials, as opposed to the non-crystalline glasses. Ceramic may be used as an adjective describing a material, product or process; or as a singular noun, or, more commonly, as a plural noun, ceramics.”. Available online: http://en.wikipedia.org/wiki/Ceramics (accessed on 11 November 2010).
- Biocompatibility is the ability of a material to perform with an appropriate host response in a specific application [46-48]
- Hench, L.L. Bioceramics: From concept to clinic. J. Am. Ceram. Soc. 1991, 74, 1487–1510. [Google Scholar] [CrossRef]
- Cao, W.; Hench, L.L. Bioactive materials. Ceram. Int. 1996, 22, 493–507. [Google Scholar] [CrossRef]
- Hench, L.L. Bioceramics. J. Am. Ceram. Soc. 1998, 81, 1705–1728. [Google Scholar] [CrossRef]
- Pinchuk, N.D.; Ivanchenko, L.A. Making calcium phosphate biomaterials. Powder Metall. Metal Ceram. 2003, 42, 357–371. [Google Scholar] [CrossRef]
- Heimann, R.B. Materials science of crystalline bioceramics: A review of basic properties and applications. CMU J. 2002, 1, 23–46. [Google Scholar]
- Dorozhkin, S.V. Bioceramics based on calcium orthophosphates. Glass Ceram. 2007, 64, 442–447. [Google Scholar] [CrossRef]
- Salinas, A.J.; Vallet-Regí, M. Evolution of ceramics with medical applications. Z. Anorg. Allg. Chem. 2007, 633, 1762–1773. [Google Scholar] [CrossRef]
- Tomoda, K.; Ariizumi, H.; Nakaji, T.; Makino, K. Hydroxyapatite particles as drug carriers for proteins. Colloids Surf. B Biointerfaces 2010, 76, 226–235. [Google Scholar] [CrossRef]
- Ducheyne, P.; Qiu, Q. Bioactive ceramics: The effect of surface reactivity on bone formation and bone cell function. Biomaterials 1999, 20, 2287–2303. [Google Scholar] [CrossRef]
- Lowenstam, H.A.; Weiner, S. On Biomineralization; Oxford University Press: Oxford, UK, 1989; p. 324. [Google Scholar]
- Weiner, S.; Wagner, H.D. Material bone: Structure-mechanical function relations. Ann. Rev. Mater. Sci. 1998, 28, 271–298. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphates. J. Mater. Sci. 2007, 42, 1061–1095. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphates in nature, biology and medicine. Materials 2009, 2, 399–498. [Google Scholar] [CrossRef]
- Bioactivity is defined as the property of the material to develop a direct, adherent and strong bonding with bone [46-48]
- Ong, J.L.; Chan, D.C.N. Hydroxyapatite and their use as coatings in dental implants: A review. Crit. Rev. Biomed. Eng. 1999, 28, 667–707. [Google Scholar]
- Davies, J.E. In vitro modeling of the bone/implant interface. Anat. Rec. 1996, 245, 426–445. [Google Scholar] [CrossRef]
- Anselme, K. Osteoblast adhesion on biomaterials. Biomaterials 2000, 21, 667–681. [Google Scholar] [CrossRef]
- Suchanek, W.L.; Yoshimura, M. Processing and properties of hydroxyapatite-based biomaterials for use as hard tissue replacement implants. J. Mater. Res. 1998, 13, 94–117. [Google Scholar] [CrossRef]
- Gauthier, O.; Bouler, J.M.; Weiss, P.; Bosco, J.; Daculsi, G.; Aguado, E. Kinetic study of bone ingrowth and ceramic resorption associated with the implantation of different injectable calcium-phosphate bone substitutes. J. Biomed. Mater. Res. 1999, 47, 28–35. [Google Scholar] [CrossRef]
- Hing, K.A.; Best, S.M.; Bonfield, W. Characterization of porous hydroxyapatite. J. Mater. Sci. Mater. Med. 1999, 10, 135–145. [Google Scholar] [CrossRef]
- Carotenuto, G.; Spagnuolo, G.; Ambrosio, L.; Nicolais, L. Macroporous hydroxyapatite as alloplastic material for dental applications. J. Mater. Sci. Mater. Med. 1999, 10, 671–676. [Google Scholar] [CrossRef]
- Bioceramics of Calcium Phosphate; De Groot, K. (Ed.) CRC Press: Boca Raton, FL, USA, 1983; p. 146.
- Narasaraju, T.S.B.; Phebe, D.E. Some physico-chemical aspects of hydroxylapatite. J. Mater. Sci. 1996, 31, 1–21. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Calcium Phosphates in Oral Biology and Medicine; Karger: Basel, Switzerland, 1991; p. 201. [Google Scholar]
- Elliott, J.C. Structure and chemistry of the apatites and other calcium orthophosphates. In Studies in Inorganic Chemistry; Elsevier: Amsterdam, The Netherlands, 1994; Volume 18, p. 389. [Google Scholar]
- Hydroxyapatite and Related Materials; Brown, P.W.; Constantz, B. (Eds.) CRC Press: Boca Raton, FL, USA, 1994; p. 343.
- Calcium Phosphates in Biological and Industrial Systems; Amjad, Z. (Ed.) Kluwer Academic Publishers: Boston, MA, USA, 1997; p. 529.
- Phosphates: Geochemical, Geobiological and Materials Importance; Hughes, J.M.; Kohn, M.; Rakovan, J. (Eds.) Mineralogical Society of America: Washington, DC, USA, 2002; p. 742.
- Octacalcium phosphate. In Monographs in Oral Science; Chow, L.C.; Eanes, E.D. (Eds.) S. Karger AG: Basel, Switzerland, 2001; Vol. 18, p. 168.
- Les Matériaux en Phosphate de Calcium. Aspects fondamentaux/Calcium Phosphate Materials. Fundamentals; Brès, E.; Hardouin, P. (Eds.) Sauramps Medical: Montpellier, France, 1998; p. 176.
- Huebsch, N.; Mooney, D.J. Inspiration and application in the evolution of biomaterials. Nature 2009, 462, 426–432. [Google Scholar] [CrossRef]
- Ring, M.E. Dentistry: An Illustrated History; Harry, N., Ed.; Abrams: New York, NY, USA, 1992; p. 320. [Google Scholar]
- Bobbio, A. The first endosseous alloplastic implant in the history of man. Bull. Hist. Dent. 1970, 20, 1–6. [Google Scholar]
- Weiner, S.; Dove, P.M. An overview of biomineralization processes and the problem of the vital effect. In Biomineralization, Series: Reviews in Mineralogy and Geochemistry; Dove, P.M., De Yoreo, J.J., Weiner, S., Eds.; Mineralogical Society of America: Washington, DC, USA, 2003; Volume 54, pp. 1–29. [Google Scholar]
- Weiner, S.; Traub, W.; Wagner, H.D. Lamellar bone: Structure-function relations. J. Struct. Biol. 1999, 126, 241–255. [Google Scholar] [CrossRef]
- Albee, F.H. Studies in bone growth: Triple calcium phosphate as a stimulus to osteogenesis. Ann. Surg. 1920, 71, 32–39. [Google Scholar] [CrossRef]
- Ray, R.D.; Ward, A.A., Jr. A preliminary report on studies of basic calcium phosphate in bone replacement. Surg. Form. 1951, 3, 429–434. [Google Scholar]
- Nery, E.B.; Lynch, K.L.; Hirthe, W.M.; Mueller, K.H. Bioceramic implants in surgically produced infrabony defects. J. Periodontol. 1975, 46, 328–347. [Google Scholar] [CrossRef]
- Denissen, H.W.; De Groot, K. Immediate dental root implants from synthetic dense calcium hydroxylapatite. J. Prosthet. Dent. 1979, 42, 551–556. [Google Scholar] [CrossRef]
- Blakeslee, K.C.; Condrate, R.A., Sr. Vibrational spectra of hydrothermally prepared hydroxyapatites. J. Am. Ceram. Soc. 1971, 54, 559–563. [Google Scholar] [CrossRef]
- Garrington, G.E.; Lightbody, P.M. Bioceramics and dentistry. J. Biomed. Mater. Res. 1972, 6, 333–343. [Google Scholar] [CrossRef]
- Cini, L.; Sandrolini, S.; Paltrinieri, M.; Pizzoferrato, A.; Trentani, C. Materiali bioceramici in funzione sostitutiva. Nota preventiva. (Bioceramic materials for replacement purposes. Preliminary note). Chir. Organi Mov. 1972, 60, 423–430. [Google Scholar]
- Rivault, M.A. Evolution, conception et technologie des travaux de prothèse fixe, réalisés en céramo-métallique. (Evolution, conception and technology of fixed prosthesis made of ceramic and metal). Rev. Fr. Odontostomatol. 1966, 13, 1367–1402. [Google Scholar]
- Dumont, A.; Appel, M.; Favard, E. Prothèses plurales en céramique sur métal. Soudage et artifices de jonction. (Multiple prostheses made of ceramics on metal. Soldering and artifacts of the junction). Ann. Odontostomatol. (Lyon) 1968, 25, 231–240. [Google Scholar]
- Hulbert, S.F.; Young, F.A.; Mathews, R.S.; Klawitter, J.J.; Talbert, C.D.; Stelling, F.H. Potential of ceramic materials as permanently implantable skeletal prostheses. J. Biomed. Mater. Res. 1970, 4, 433–456. [Google Scholar] [CrossRef]
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K. Bonding mechanisms at the interface of ceramic prosthetic materials. J. Biomed. Mater. Res. 1971, 2, 117–141. [Google Scholar]
- Hulbert, S.F.; Hench, L.L.; Forbers, D.; Bowman, L.S. History of bioceramics. Ceram. Int. 1982, 8, 131–140. [Google Scholar] [CrossRef]
- Hulbert, S.F.; Hench, L.L.; Forbers, D.; Bowman, L.S. History of bioceramics. In Ceramics in Surgery; Vincenzini, P., Ed.; Elsevier: Amsterdam, The Netherlands, 1983; pp. 3–29. [Google Scholar]
- Jarcho, M.; Bolen, C.H.; Thomas, M.B.; Bobick, J.; Kay, J.F.; Doremus, R.H. Hydroxylapatite synthesis and characterization in dense polycrystalline form. J. Mater. Sci. 1976, 11, 2027–2035. [Google Scholar] [CrossRef]
- Jarcho, M.; O’Connor, J.R.; Paris, D.A. Ceramic hydroxylapatite as a plaque growth and drug screening substrate. J. Dental Res. 1977, 56, 151–156. [Google Scholar] [CrossRef]
- Jarcho, M.; Salsbury, R.L.; Thomas, M.B.; Doremus, R.H. Synthesis and fabrication of β-tricalcium phosphate ceramics for potential prosthetic applications. J. Mater. Sci. 1979, 14, 142–150. [Google Scholar] [CrossRef]
- Jarcho, M. Calcium phosphate ceramics as hard tissue prosthetics. Clin. Orthop. Rel. Res. 1981, 157, 259–278. [Google Scholar]
- Rejda, B.V.; Peelen, J.G.J.; De Groot, K. Tricalcium phosphate as a bone substitute. J. Bioeng. 1977, 1, 93–97. [Google Scholar]
- De Groot, K. Bioceramics consisting of calcium phosphate salts. Biomaterials 1980, 1, 47–50. [Google Scholar] [CrossRef]
- Aoki, H.; Kato, K.M.; Ogiso, M.; Tabata, T. Studies on the application of apatite to dental materials. J. Dent. Eng. 1977, 18, 86–89. [Google Scholar]
- Kato, K.; Aoki, H.; Tabata, T.; Ogiso, M. Biocompatibility of apatite ceramics in mandibles. Biomater. Med. Dev. Artif. Organs 1979, 7, 291–297. [Google Scholar]
- Akao, M.; Aoki, H.; Kato, K. Mechanical properties of sintered hydroxyapatite for prosthetic applications. J. Mater. Sci. 1981, 16, 809–812. [Google Scholar] [CrossRef]
- Akao, M.; Aoki, H.; Kato, K.; Sato, A. Dense polycrystalline β-tricalcium phosphate for prosthetic applications. J. Mater. Sci. 1982, 17, 343–346. [Google Scholar] [CrossRef]
- Roy, D.M.; Linnehan, S.K. Hydroxyapatite formed from coral skeletal carbonate by hydrothermal exchange. Nature 1974, 247, 220–222. [Google Scholar] [CrossRef]
- Holmes, R.E. Bone regeneration within a coralline hydroxyapatite implant. Plast. Reconstr. Surg. 1979, 63, 626–633. [Google Scholar] [CrossRef]
- Elsinger, E.C.; Leal, L. Coralline hydroxyapatite bone graft substitutes. J. Foot Ankle Surg. 1996, 35, 396–399. [Google Scholar] [CrossRef]
- Shipman, P.; Foster, G.; Schoeninger, M. Burnt bones and teeth: An experimental study of color, morphology, crystal structure and shrinkage. J. Archaeol. Sci. 1984, 11, 307–325. [Google Scholar] [CrossRef]
- LeGeros, R.Z.; LeGeros, J.P. Calcium phosphate bioceramics: Past, present, future. Key Eng. Mater. 2003, 240-242, 3–10. [Google Scholar] [CrossRef]
- Rivera, E.M.; Araiza, M.; Brostow, W.; Castaño, V.M.; Díaz-Estrada, J.R.; Hernández, R.; Rodríguez, J.R. Synthesis of hydroxyapatite from eggshells. Mater. Lett. 1999, 41, 128–134. [Google Scholar] [CrossRef]
- Lee, S.J.; Oh, S.H. Fabrication of calcium phosphate bioceramics by using eggshell and phosphoric acid. Mater. Lett. 2003, 57, 4570–4574. [Google Scholar] [CrossRef]
- Balazsi, C.; Weber, F.; Kover, Z.; Horvath, E.; Nemeth, C. Preparation of calcium-phosphate bioceramics from natural resources. J. Eur. Ceram. Soc. 2007, 27, 1601–1606. [Google Scholar] [CrossRef]
- Murugan, R.; Ramakrishna, S. Crystallographic study of hydroxyapatite bioceramics derived from various sources. Cryst. Growth Des. 2005, 5, 111–112. [Google Scholar] [CrossRef]
- Ruksudjarit, A.; Pengpat, K.; Rujijanagul, G.; Tunkasiri, T. Synthesis and characterization of nanocrystalline hydroxyapatite from natural bovine bone. Curr. Appl. Phys. 2008, 8, 270–272. [Google Scholar] [CrossRef]
- Ooi, C.Y.; Hamdi, M.; Ramesh, S. Properties of hydroxyapatite produced by annealing of bovine bone. Ceram. Int. 2007, 33, 1171–1177. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, Y.C.; Yoon, Y.S. Characteristics of calcium phosphate powders synthesized from cuttlefish bone and phosphoric acid. J. Ceram. Proc. Res. 2007, 8, 427–430. [Google Scholar]
- Oktar, F.N. Microstructure and mechanical properties of sintered enamel hydroxyapatite. Ceram. Int. 2007, 33, 1309–1314. [Google Scholar] [CrossRef]
- Vallet-Regí, M.; González-Calbet, J.M. Calcium phosphates as substitution of bone tissues. Progr. Solid State Chem. 2004, 32, 1–31. [Google Scholar] [CrossRef]
- Lecomte, A.; Gautier, H.; Bouler, J.M.; Gouyette, A.; Pegon, Y.; Daculsi, G.; Merle, C. Biphasic calcium phosphate: A comparative study of interconnected porosity in two ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 84B, 1–6. [Google Scholar] [CrossRef]
- Tancret, F.; Bouler, J.M.; Chamousset, J.; Minois, L.M. Modelling the mechanical properties of microporous and macroporous biphasic calcium phosphate bioceramics. J. Eur. Ceram. Soc. 2006, 26, 3647–3656. [Google Scholar] [CrossRef]
- Bouler, J.M.; Trecant, M.; Delecrin, J.; Royer, J.; Passuti, N.; Daculsi, G. Macroporous biphasic calcium phosphate ceramics: Influence of five synthesis parameters on compressive strength. J. Biomed. Mater. Res. 1996, 32, 603–609. [Google Scholar] [CrossRef]
- Kivrak, N.; Tas, A.C. Synthesis of calcium hydroxyapatite—tricalcium phosphate (HA-TCP) composite bioceramic powders and their sintering behavior. J. Am. Ceram. Soc. 1998, 81, 2245–2252. [Google Scholar] [CrossRef]
- Gauthier, O.; Bouler, J.M.; Aguado, E.; Pilet, P.; Daculsi, G. Macroporous biphasic calcium phosphate ceramics: Influence of macropore diameter and macroporosity percentage on bone ingrowth. Biomaterials 1998, 19, 133–139. [Google Scholar] [CrossRef]
- Wang, J.; Chen, W.; Li, Y.; Fan, S.; Weng, J.; Zhang, X. Biological evaluation of biphasic calcium phosphate ceramic vertebral laminae. Biomaterials 1998, 19, 1387–1392. [Google Scholar] [CrossRef]
- Daculsi, G. Biphasic calcium phosphate concept applied to artificial bone, implant coating and injectable bone substitute. Biomaterials 1998, 19, 1473–1478. [Google Scholar] [CrossRef]
- Daculsi, G.; Weiss, P.; Bouler, J.M.; Gauthier, O.; Millot, F.; Aguado, E. Biphasic calcium phosphate/hydrosoluble polymer composites: A new concept for bone and dental substitution biomaterials. Bone 1999, 25 Suppl. 2, 59S–61S. [Google Scholar] [CrossRef]
- LeGeros, R.Z.; Lin, S.; Rohanizadeh, R.; Mijares, D.; LeGeros, J.P. Biphasic calcium phosphate bioceramics: Preparation, properties and applications. J. Mater. Sci. Mater. Med. 2003, 14, 201–209. [Google Scholar] [CrossRef]
- Daculsi, G.; Laboux, O.; Malard, O.; Weiss, P. Current state of the art of biphasic calcium phosphate bioceramics. J. Mater. Sci. Mater. Med. 2003, 14, 195–200. [Google Scholar]
- Alam, I.; Asahina, I.; Ohmamiuda, K.; Enomoto, S. Comparative study of biphasic calcium phosphate ceramics impregnated with rhBMP-2 as bone substitutes. J. Biomed. Mater. Res. 2001, 54, 129–138. [Google Scholar] [CrossRef]
- Daculsi, G. Biphasic calcium phosphate granules concept for injectable and mouldable bone substitute. Adv. Sci. Technol. 2006, 49, 9–13. [Google Scholar] [CrossRef]
- Tanimoto, Y.; Shibata, Y.; Murakami, A.; Miyazaki, T.; Nishiyama, N. Effect of varying HAP/TCP ratios in tape-cast biphasic calcium phosphate ceramics on responcce in vitro. J. Hard Tissue Biology 2009, 18, 71–76. [Google Scholar] [CrossRef]
- O’Neill, W.C. The fallacy of the calcium—phosphorus product. Kidney Int. 2007, 72, 792–796. [Google Scholar] [CrossRef]
- da Silva, R.V.; Bertran, C.A.; Kawachi, E.Y.; Camilli, J.A. Repair of cranial bone defects with calcium phosphate ceramic implant or autogenous bone graft. J. Craniofac. Surg. 2007, 18, 281–286. [Google Scholar] [CrossRef]
- Metsger, D.S.; Driskell, T.D.; Paulsrud, J.R. Tricalcium phosphate ceramic—a resorbable bone implant: Review and current status. J. Am. Dent. Assoc. 1982, 105, 1035–1038. [Google Scholar]
- Reid, J.W.; Tuck, L.; Sayer, M.; Fargo, K.; Hendry, J.A. Synthesis and characterization of single-phase silicon substituted α-tricalcium phosphate. Biomaterials 2006, 27, 2916–2925. [Google Scholar] [CrossRef]
- Yin, X.; Stott, M.J.; Rubio, A. α- and β-tricalcium phosphate: A density functional study. Phys. Rev. B 2003, 68, 205205–205211. [Google Scholar] [CrossRef]
- Yin, X.; Stott, M.J. Theoretical insights into bone grafting Si-stabilized α-tricalcium phosphate. J. Chem. Phys. 2005, 122, 024709–024717. [Google Scholar] [CrossRef]
- Ruan, J.M.; Zou, J.P.; Zhou, J.N.; Hu, J.Z. Porous hydroxyapatite—tricalcium phosphate bioceramics. Powder Metall. 2006, 49, 66–69. [Google Scholar] [CrossRef]
- Yin, X.; Stott, M.J. Surface and adsorption properties of α-tricalcium phosphate. J. Chem. Phys. 2006, 124, 124701–124709. [Google Scholar] [CrossRef]
- Kamitakahara, M.; Ohtsuki, C.; Miyazaki, T. Review paper: Behavior of ceramic biomaterials derived from tricalcium phosphate in physiological condition. J. Biomater. Appl. 2008, 23, 197–212. [Google Scholar] [CrossRef]
- Oishi, M.; Ohtsuki, C.; Kitamura, M.; Kamitakahara, M.; Ogata, S.; Miyazaki, T.; Tanihara, M. Fabrication and chemical durability of porous bodies consisting of biphasic tricalcium phosphates. Phosphorus Res. Bull. 2004, 17, 95–100. [Google Scholar]
- Kamitakahara, M.; Ohtsuki, C.; Oishi, M.; Ogata, S.; Miyazaki, T.; Tanihara, M. Preparation of porous biphasic tricalcium phosphate and its in vivo behavior. Key Eng. Mater. 2005, 284-286, 281–284. [Google Scholar] [CrossRef]
- Wang, R.; Weng, W.; Deng, X.; Cheng, K.; Liu, X.; Du, P.; Shen, G.; Han, G. Dissolution behavior of submicron biphasic tricalcium phosphate powders. Key Eng. Mater. 2006, 309-311, 223–226. [Google Scholar] [CrossRef]
- Li, Y.; Weng, W.; Tam, K.C. Novel highly biodegradable biphasic tricalcium phosphates composed of α-tricalcium phosphate and β-tricalcium phosphate. Acta Biomater. 2007, 3, 251–254. [Google Scholar] [CrossRef]
- Li, Y.; Li, D.; Weng, W. In vitro dissolution behavior of biphasic tricalcium phosphate composite powders composed of α-tricalcium phosphate and β-tricalcium phosphate. Key Eng. Mater. 2008, 368-372, 1206–1208. [Google Scholar] [CrossRef]
- Vani, R.; Girija, E.K.; Elayaraja, K.; Prakash Parthiban, S.; Kesavamoorthy, R.; Narayana Kalkura, S. Hydrothermal synthesis of porous triphasic hydroxyapatite/(α and β) tricalcium phosphate. J. Mater. Sci. Mater. Med. 2009, 20 Suppl. 1, 43–48. [Google Scholar]
- Daculsi, G.; Bouler, J.M.; LeGeros, R.Z. Adaptive crystal formation in normal and pathological calcifications in synthetic calcium phosphate and related biomaterials. Int. Rev. Cytol. 1997, 172, 129–191. [Google Scholar] [CrossRef]
- Astala, R.; Calderin, L.; Yin, X.; Stott, M.J. Ab initio simulation of Si-doped hydroxyapatite. Chem. Mater. 2006, 18, 413–422. [Google Scholar] [CrossRef]
- Zhu, X.D.; Zhang, H.J.; Fan, H.S.; Li, W.; Zhang, X.D. Effect of phase composition and microstructure of calcium phosphate ceramic particles on protein adsorption. Acta Biomater. 2010, 6, 1536–1541. [Google Scholar] [CrossRef]
- Bohner, M. Calcium orthophosphates in medicine: From ceramics to calcium phosphate cements. Injury 2000, 31 Suppl. 4, D37–D47. [Google Scholar] [CrossRef]
- Norton, J.; Malik, K.R.; Darr, J.A.; Rehman, I. Recent developments in processing and surface modification of hydroxyapatite. Adv. Appl. Ceram. 2006, 105, 113–139. [Google Scholar] [CrossRef]
- Yang, S.; Leong, K.F.; Du, Z.; Chua, C.K. The design of scaffolds for use in tissue engineering. Part II. Rapid prototyping techniques. Tissue Eng. 2002, 8, 1–11. [Google Scholar] [CrossRef]
- Yeong, W.Y.; Chua, C.K.; Leong, K.F.; Chandrasekaran, M. Rapid prototyping in tissue engineering: Challenges and potential. Trends Biotechnol. 2004, 22, 643–652. [Google Scholar] [CrossRef]
- Hieu, L.C.; Zlatov, N.; Sloten, J.V.; Bohez, E.; Khanh, L.; Binh, P.H.; Oris, P.; Toshev, Y. Medical rapid prototyping applications and methods. Assembly Autom. 2005, 25, 284–292. [Google Scholar] [CrossRef]
- Eufinger, H.; Wehniöller, M.; Machtens, E.; Heuser, L.; Harders, A.; Kruse, D. Reconstruction of craniofacial bone defects with individual alloplastic implants based on CAD/CAM-manipulated CT-data. J. Craniomaxillofac. Surg. 1995, 23, 175–181. [Google Scholar] [CrossRef]
- Klein, M.; Glatzer, C. Individual CAD/CAM fabricated glass-bioceramic implants in reconstructive surgery of the bony orbital floor. Plast. Reconstr. Surg. 2006, 117, 565–570. [Google Scholar] [CrossRef]
- Yin, L.; Song, X.F.; Song, Y.L.; Huang, T.; Li, J. An overview of in vitro abrasive finishing & CAD/CAM of bioceramics in restorative dentistry. Int. J. Mach. Tools Manuf. 2006, 46, 1013–1026. [Google Scholar] [CrossRef]
- Yardimci, M.A.; Guceri, S.I.; Danforth, S.C. Process modeling for fused deposition of ceramics. Ceram. Eng. Sci. Proc. 1996, 17, 78–82. [Google Scholar] [CrossRef]
- Bellini, A.; Shor, L.; Guceri, S.I. New developments in fused deposition modeling of ceramics. Rapid Prototyping J. 2005, 11, 214–220. [Google Scholar] [CrossRef]
- Tan, K.H.; Chua, C.K.; Leong, K.F.; Cheah, C.M.; Cheang, P.; Abu Bakar, M.S.; Cha, S.W. Scaffold development using selective laser sintering of polyetheretherketone-hydroxyapatite biocomposite blends. Biomaterials 2003, 24, 3115–3123. [Google Scholar] [CrossRef]
- Wiria, F.E.; Leong, K.F.; Chua, C.K.; Liu, Y. Poly-ε-caprolactone/hydroxyapatite for tissue engineering scaffold fabrication via selective laser sintering. Acta Biomater. 2007, 3, 1–12. [Google Scholar]
- Zhou, W.Y.; Lee, S.H.; Wang, M.; Cheung, W.L.; Ip, W.Y. Selective laser sintering of porous tissue engineering scaffolds from poly(L-lactide)/carbonated hydroxyapatite nanocomposite microspheres. J. Mater. Sci. Mater. Med. 2008, 19, 2535–2540. [Google Scholar] [CrossRef]
- Sachs, E.; Cima, M.; Williams, P.; Brancazio, D.; Cornie, J. Three dimensional printing. Rapid tooling and prototypes directly from a CAD model. J. Eng. Ind. 1992, 114, 481–488. [Google Scholar] [CrossRef]
- Gbureck, U.; Hölzel, T.; Doillon, C.J.; Müller, F.A.; Barralet, J.E. Direct printing of bioceramic implants with spatially localized angiogenic factors. Adv. Mater. 2007, 19, 795–800. [Google Scholar] [CrossRef]
- Gbureck, U.; Hölzel, T.; Klammert, U.; Würzler, K.; Müller, F.A.; Barralet, J.E. Resorbable dicalcium phosphate bone substitutes prepared by 3D powder printing. Adv. Funct. Mater. 2007, 17, 3940–3945. [Google Scholar] [CrossRef]
- Vorndran, E.; Klarner, M.; Klammert, U.; Grover, L.M.; Patel, S.; Barralet, J.E.; Gbureck, U. 3D powder printing of β-tricalcium phosphate ceramics using different strategies. Adv. Eng. Mater. 2008, 10, B67–B71. [Google Scholar] [CrossRef]
- Seitz, H.; Rieder, W.; Irsen, S.; Leukers, B.; Tille, C. Three-dimensional printing of porous ceramic scaffolds for bone tissue engineering. J. Biomed. Mater. Res. B 2005, 74B, 782–788. [Google Scholar] [CrossRef]
- Leukers, B.; Gülkan, H.; Irsen, S.H.; Milz, S.; Tille, C.; Schieker, M.; Seitz, H. Hydroxyapatite scaffolds for bone tissue engineering made by 3D printing. J. Mater. Sci. Mater. Med. 2005, 16, 1121–1124. [Google Scholar] [CrossRef]
- Habibovic, P.; Gbureck, U.; Doillon, C.J.; Bassett, D.C.; Van Blitterswijk, C.A.; Barralet, J.E. Osteoconduction and osteoinduction of low-temperature 3D printed bioceramic implants. Biomaterials 2008, 29, 944–953. [Google Scholar]
- Fierz, F.C.; Beckmann, F.; Huser, M.; Irsen, S.H.; Leukers, B.; Witte, F.; Degistirici, O.; Andronache, A.; Thie, M.; Müller, B. The morphology of anisotropic 3D-printed hydroxyapatite scaffolds. Biomaterials 2008, 29, 3799–3806. [Google Scholar] [CrossRef]
- Seitz, H.; Deisinger, U.; Leukers, B.; Detsch, R.; Ziegler, G. Different calcium phosphate granules for 3-D printing of bone tissue engineering scaffolds. Adv. Eng. Mater. 2009, 11, B41–B46. [Google Scholar] [CrossRef]
- Chu, T.M.G.; Halloran, J.W.; Hollister, S.J.; Feinberg, S.E. Hydroxyapatite implants with designed internal architecture. J. Mater. Sci. Mater. Med. 2001, 12, 471–478. [Google Scholar] [CrossRef]
- Li, X.; Li, D.; Lu, B.; Tang, Y.; Wang, L.; Wang, Z. Design and fabrication of CAP scaffolds by indirect solid free form fabrication. Rapid Prototyping J. 2005, 11, 312–318. [Google Scholar] [CrossRef]
- Woesz, A.; Rumpler, M.; Stampfl, J.; Varga, F.; Fratzl-Zelman, N.; Roschger, P.; Klaushofer, K.; Fratzl, P. Towards bone replacement materials from calcium phosphates via rapid prototyping and ceramic gel casting. Mater. Sci. Eng. C 2005, 25, 181–186. [Google Scholar] [CrossRef]
- Li, X.; Li, D.; Lu, B.; Wang, C. Fabrication of bioceramic scaffolds with pre-designed internal architecture by gel casting and indirect stereolithography techniques. J. Porous Mater. 2008, 15, 667–671. [Google Scholar] [CrossRef]
- Leong, K.F.; Cheah, C.M.; Chua, C.K. Solid freeform fabrication of three-dimensional scaffolds for engineering replacement tissues and organs. Biomaterials 2003, 24, 2363–2378. [Google Scholar] [CrossRef]
- Bone Grafts and Bone Substitutes: Basic Science and Clinical Applications; Nather, A. (Ed.) World Scientific: Singapore, 2005; p. 592.
- Bio-Materials and Prototyping Applications in Medicine; Bártolo, P.; Bidanda, B. (Eds.) Springer: New York, NY, USA, 2008; p. 216.
- Narayan, R.J.; Jin, C.; Doraiswamy, A.; Mihailescu, I.N.; Jelinek, M.; Ovsianikov, A.; Chichkov, B.; Chrisey, D.B. Laser processing of advanced bioceramics. Adv. Eng. Mater. 2005, 7, 1083–1098. [Google Scholar] [CrossRef]
- Bioceramics and Their Clinical Applications; Kokubo, T. (Ed.) Woodhead Publishing: Sawston, UK, 2008; p. 784.
- Biomedical Materials; Narayan, R. (Ed.) Springer: New York, NY, USA, 2009; p. 566.
- Raksujarit, A.; Pengpat, K.; Rujijanagul, G.; Tunkasiri, T. Processing and properties of nanoporous hydroxyapatite ceramics. Mater. Des. 2010, 31, 1658–1660. [Google Scholar] [CrossRef]
- Park, J. Bioceramics: Properties, Characterizations, and Applications; Springer: Berlin, Germany, 2008; p. 364. [Google Scholar]
- Rodríguez-Lorenzo, L.M.; Vallet-Regí, M.; Ferreira, J.M.F. Fabrication of hydroxyapatite bodies by uniaxial pressing from a precipitated powder. Biomaterials 2001, 22, 583–588. [Google Scholar] [CrossRef]
- Nazarpak, M.H.; Solati-Hashjin, M.; Moztarzadeh, F. Preparation of hydroxyapatite ceramics for biomedical applications. J. Ceram. Proc. Res. 2009, 10, 54–57. [Google Scholar]
- Itoh, H.; Wakisaka, Y.; Ohnuma, Y.; Kuboki, Y. A new porous hydroxyapatite ceramic prepared by cold isostatic pressing and sintering synthesized flaky powder. Dental Mater. 1994, 13, 25–35. [Google Scholar] [CrossRef]
- Gautier, H.; Merle, C.; Auget, J.L.; Daculsi, G. Isostatic compression, a new process for incorporating vancomycin into biphasic calcium phosphate: Comparison with a classical method. Biomaterials 2000, 21, 243–249. [Google Scholar] [CrossRef]
- Tadic, D.; Epple, M. Mechanically stable implants of synthetic bone mineral by cold isostatic pressing. Biomaterials 2003, 24, 4565–4571. [Google Scholar] [CrossRef]
- Pecqueux, F.; Tancret, F.; Payraudeau, N.; Bouler, J.M. Influence of microporosity and macroporosity on the mechanical properties of biphasic calcium phosphate bioceramics: Modelling and experiment. J. Eur. Ceram. Soc. 2010, 30, 819–829. [Google Scholar] [CrossRef]
- Uematsu, K.; Takagi, M.; Honda, T.; Uchida, N.; Saito, K. Transparent hydroxyapatite prepared by hot isostatic pressing of filter cake. J. Am. Ceram. Soc. 1989, 72, 1476–1478. [Google Scholar] [CrossRef]
- Onoki, T.; Hashida, T. New method for hydroxyapatite coating of titanium by the hydrothermal hot isostatic pressing technique. Surf. Coat. Technol. 2006, 200, 6801–6807. [Google Scholar] [CrossRef]
- Takikawa, K.; Akao, M. Fabrication of transparent hydroxyapatite and application to bone marrow derived cell/hydroxyapatite interaction observation in-vivo. J. Mater. Sci. Mater. Med. 1996, 7, 439–445. [Google Scholar] [CrossRef]
- Viana, M.; Désiré, A.; Chevalier, E.; Champion, E.; Chotard, R.; Chulia, D. Interest of high shear wet granulation to produce drug loaded porous calcium phosphate pellets for bone filling. Key Eng. Mater. 2009, 396-398, 535–538. [Google Scholar] [CrossRef]
- Reikerås, O.; Johansson, C.B.; Sundfeldt, M. Bone ingrowths to press-fit and loose-fit implants: Comparisons between titanium and hydroxyapatite. J. Long. Term. Eff. Med. Implants 2006, 16, 157–164. [Google Scholar] [CrossRef]
- Rao, R.R.; Kannan, T.S. Dispersion and slip casting of hydroxyapatite. J. Am. Ceram. Soc. 2001, 84, 1710–1716. [Google Scholar]
- Sakka, Y.; Takahashi, K.; Matsuda, N.; Suzuki, T.S. Effect of milling treatment on texture development of hydroxyapatite ceramics by slip casting in high magnetic field. Mater. Trans. 2007, 48, 2861–2866. [Google Scholar] [CrossRef]
- Zhang, Y.; Yokogawa, Y.; Feng, X.; Tao, Y.; Li, Y. Preparation and properties of bimodal porous apatite ceramics through slip casting using different hydroxyapatite powders. Ceram. Int. 2010, 36, 107–113. [Google Scholar] [CrossRef]
- Sepulveda, P.; Ortega, F.S.; Innocentini, M.D.M.; Pandolfelli, V.C. Properties of highly porous hydroxyapatite obtained by the gel casting of foams. J. Am. Ceram. Soc. 2000, 83, 3021–3024. [Google Scholar] [CrossRef]
- Padilla, S.; Vallet-Regí, M.; Ginebra, M.P.; Gil, F.J. Processing and mechanical properties of hydroxyapatite pieces obtained by the gel-casting method. J. Eur. Ceram. Soc. 2005, 25, 375–383. [Google Scholar]
- Sánchez-Salcedo, S.; Werner, J.; Vallet-Regí, M. Hierarchical pore structure of calcium phosphate scaffolds by a combination of gel-casting and multiple tape-casting methods. Acta Biomater. 2008, 4, 913–922. [Google Scholar] [CrossRef]
- Chen, B.; Zhang, T.; Zhang, J.; Lin, Q.; Jiang, D. Microstructure and mechanical properties of hydroxyapatite obtained by gel-casting process. Ceram. Int. 2008, 34, 359–364. [Google Scholar] [CrossRef]
- Marcassoli, P.; Cabrini, M.; Tirillò, J.; Bartuli, C.; Palmero, P.; Montanaro, L. Mechanical characterization of hydroxiapatite micro/macro-porous ceramics obtained by means of innovative gel-casting process. Key Eng. Mater. 2010, 417-418, 565–568. [Google Scholar]
- Padilla, S.; Roman, J.; Vallet-Regí, M. Synthesis of porous hydroxyapatites by combination of gel casting and foams burn out methods. J. Mater. Sci. Mater. Med. 2002, 13, 1193–1197. [Google Scholar]
- Fomin, A.S.; Barinov, S.M.; Ievlev, V.M.; Smirnov, V.V.; Mikhailov, B.P.; Belonogov, E.K.; Drozdova, N.A. Nanocrystalline hydroxyapatite ceramics produced by low-temperature sintering after high-pressure treatment. Dokl. Chem. 2008, 418, 22–25. [Google Scholar]
- Kankawa, Y.; Kaneko, Y.; Saitou, K. Injection molding of highly-purified hydroxylapatite and TCP utilizing solid phase reaction method. J. Ceram. Soc. Jpn. 1991, 99, 438–442. [Google Scholar]
- Kwon, S.H.; Jun, Y.K.; Hong, S.H.; Lee, I.S.; Kim, H.E.; Won, Y.Y. Calcium phosphate bioceramics with various porosities and dissolution rates. J. Am. Ceram. Soc. 2002, 85, 3129–3131. [Google Scholar]
- Fooki, A.C.B.M.; Aparecida, A.H.; Fideles, T.B.; Costa, R.C.; Fook, M.V.L. Porous hydroxyapatite scaffolds by polymer sponge method. Key Eng. Mater. 2009, 396-398, 703–706. [Google Scholar] [CrossRef]
- Sopyan, I.; Kaur, J. Preparation and characterization of porous hydroxyapatite through polymeric sponge method. Ceram. Int. 2009, 35, 3161–3168. [Google Scholar] [CrossRef]
- Bellucci, D.; Cannillo, V.; Sola, A. Shell scaffolds: A new approach towards high strength bioceramic scaffolds for bone regeneration. Mater. Lett. 2010, 64, 203–206. [Google Scholar]
- Velayudhan, S.; Ramesh, P.; Sunny, M.C.; Varma, H.K. Extrusion of hydroxyapatite to clinically significant shapes. Mater. Lett. 2000, 46, 142–146. [Google Scholar]
- Yang, H.Y.; Thompson, I.; Yang, S.F.; Chi, X.P.; Evans, J.R.G.; Cook, R.J. Dissolution characteristics of extrusion freeformed hydroxyapatite—tricalcium phosphate scaffolds. J. Mater. Sci. Mater. Med. 2008, 19, 3345–3353. [Google Scholar]
- Yang, S.; Yang, H.; Chi, X.; Evans, J.R.G.; Thompson, I.; Cook, R.J.; Robinson, P. Rapid prototyping of ceramic lattices for hard tissue scaffolds. Mater. Des. 2008, 29, 1802–1809. [Google Scholar] [CrossRef]
- Muthutantri, A.I.; Huang, J.; Edirisinghe, M.J.; Bretcanu, O.; Boccaccini, A.R. Dipping and electrospraying for the preparation of hydroxyapatite foams for bone tissue engineering. Biomed. Mater. 2008, 3, 25009–25022. [Google Scholar] [CrossRef]
- Roncari, E.; Galassi, C.; Pinasco, P. Tape casting of porous hydroxyapatite ceramics. J. Mater. Sci. Lett. 2000, 19, 33–35. [Google Scholar] [CrossRef]
- Tian, T.; Jiang, D.; Zhang, J.; Lin, Q. Aqueous tape casting process for hydroxyapatite. J. Eur. Ceram. Soc. 2007, 27, 2671–2677. [Google Scholar] [CrossRef]
- Suzuki, S.; Itoh, K.; Ohgaki, M.; Ohtani, M.; Ozawa, M. Preparation of sintered filter for ion exchange by a doctor blade method with aqueous slurries of needlelike hydroxyapatite. Ceram. Int. 1999, 25, 287–291. [Google Scholar] [CrossRef]
- Inoue, K.; Sassa, K.; Yokogawa, Y.; Sakka, Y.; Okido, M.; Asai, S. Control of crystal orientation of hydroxyapatite by imposition of a high magnetic field. Mater. Trans. 2003, 44, 1133–1137. [Google Scholar]
- Iwai, K.; Akiyama, J.; Asai, S. Structure control of hydroxyapatite using a magnetic field. Mater. Sci. Forum 2007, 561-565, 1565–1568. [Google Scholar] [CrossRef]
- Iwai, K.; Akiyama, J.; Tanase, T.; Asai, S. Alignment of HAp crystal using a sample rotation in a static magnetic field. Mater. Sci. Forum 2007, 539-543, 716–719. [Google Scholar] [CrossRef]
- Sakka, Y.; Takahashi, K.; Suzuki, T.S.; Ito, S.; Matsuda, N. Texture development of hydroxyapatite ceramics by colloidal processing in a high magnetic field followed by sintering. Mater. Sci. Eng. A 2008, 475, 27–33. [Google Scholar]
- Kang, J.; Hadfield, M. Parameter optimization by Taguchi methods for finishing advanced ceramic balls using a novel eccentric lapping machine. Proc. Inst. Mech. Eng. B 2001, 215, 69–78. [Google Scholar] [CrossRef]
- Kurella, A.; Dahotre, N.B. Surface modification for bioimplants: The role of laser surface engineering. J. Biomater. Appl. 2005, 20, 5–50. [Google Scholar] [CrossRef]
- Oktar, F.N.; Genc, Y.; Goller, G.; Erkmen, E.Z.; Ozyegin, L.S.; Toykan, D.; Demirkiran, H.; Haybat, H. Sintering of synthetic hydroxyapatite compacts. Key Eng. Mater. 2004, 264-268, 2087–2090. [Google Scholar] [CrossRef]
- He, Z.; Ma, J.; Wang, C. Constitutive modeling of the densification and the grain growth of hydroxyapatite ceramics. Biomaterials 2005, 26, 1613–1621. [Google Scholar] [CrossRef]
- Fellah, B.H.; Layrolle, P. Sol-gel synthesis and characterization of macroporous calcium phosphate bioceramics containing microporosity. Acta Biomater. 2009, 5, 735–742. [Google Scholar] [CrossRef]
- Khalil, K.A.; Kim, S.W.; Dharmaraj, N.; Kim, K.W.; Kim, H.Y. Novel mechanism to improve toughness of the hydroxyapatite bioceramics using high-frequency induction heat sintering. J. Mater. Proc. Technol 2007, 187-188, 417–420. [Google Scholar]
- Landi, E.; Tampieri, A.; Celotti, G.; Sprio, S. Densification behaviour and mechanisms of synthetic hydroxyapatites. J. Eur. Ceram. Soc. 2000, 20, 2377–2387. [Google Scholar] [CrossRef]
- Ruys, A.J.; Wei, M.; Sorrell, C.C.; Dickson, M.R.; Brandwood, A.; Milthorpe, B.K. Sintering effect on the strength of hydroxyapatite. Biomaterials 1995, 16, 409–415. [Google Scholar] [CrossRef]
- Van Landuyt, P.; Li, F.; Keustermans, J.P.; Streydio, J.M.; Delannay, F.; Munting, E. The influence of high sintering temperatures on the mechanical properties of hydroxylapatite. J. Mater. Sci. Mater. Med. 1995, 6, 8–13. [Google Scholar] [CrossRef]
- Ben Ayed, F.; Bouaziz, J.; Bouzouita, K. Pressureless sintering of fluorapatite under oxygen atmosphere. J. Eur. Ceram. Soc. 2000, 20, 1069–1076. [Google Scholar] [CrossRef]
- Haberko, K.; Bućko, M.M.; Brzezińska-Miecznik, J.; Haberko, M.; Mozgawa, W.; Panz, T.; Pyda, A.; Zarebski, J. Natural hydroxyapatite—its behaviour during heat treatment. J. Eur. Ceram. Soc. 2006, 26, 537–542. [Google Scholar] [CrossRef]
- Haberko, K.; Bućko, M.M.; Mozgawa, W.; Pyda, A.; Brzezińska-Miecznik, J.; Carpentier, J. Behaviour of bone origin hydroxyapatite at elevated temperatures and in O2 and CO2 atmospheres. Ceram. Int. 2009, 35, 2537–2540. [Google Scholar] [CrossRef]
- Janus, A.M.; Faryna, M.; Haberko, K.; Rakowska, A.; Panz, T. Chemical and microstructural characterization of natural hydroxyapatite derived from pig bones. Mikrochim. Acta 2008, 161, 349–353. [Google Scholar] [CrossRef]
- Bahrololoom, M.E.; Javidi, M.; Javadpour, S.; Ma, J. Characterisation of natural hydroxyapatite extracted from bovine cortical bone ash. J. Ceram. Proc. Res. 2009, 10, 129–138. [Google Scholar]
- Dorozhkina, E.I.; Dorozhkin, S.V. Mechanism of the solid-state transformation of a calcium-deficient hydroxyapatite (CDHA) into biphasic calcium phosphate (BCP) at elevated temperatures. Chem. Mater. 2002, 14, 4267–4272. [Google Scholar] [CrossRef]
- Li, Y.; Kong, F.; Weng, W. Preparation and characterization of novel biphasic calcium phosphate powders (α-TCP/HA) derived from carbonated amorphous calcium phosphates. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 89B, 508–517. [Google Scholar] [CrossRef]
- Mostafa, N.Y. Characterization, thermal stability and sintering of hydroxyapatite powders prepared by different routes. Mater. Chem. Phys. 2005, 94, 333–341. [Google Scholar] [CrossRef]
- Suchanek, W.; Yashima, M.; Kakihana, M.; Yoshimura, M. Hydroxyapatite ceramics with selected sintering additives. Biomaterials 1997, 18, 923–933. [Google Scholar] [CrossRef]
- Kalita, S.J.; Bose, S.; Bandyopadhyay, A.; Hosick, H.L. Oxide based sintering additives for HAp ceramics. Ceram. Trans. 2003, 147, 63–72. [Google Scholar]
- Kalita, S.J.; Bose, S.; Hosick, H.L.; Bandyopadhyay, A. CaO-P2O5-Na2O-based sintering additives for hydroxyapatite (HAp) ceramics. Biomaterials 2004, 25, 2331–2339. [Google Scholar] [CrossRef]
- Safronova, T.V.; Putlyaev, V.I.; Shekhirev, M.A.; Tretyakov, Y.D.; Kuznetsov, A.V.; Belyakov, A.V. Densification additives for hydroxyapatite ceramics. J. Eur. Ceram. Soc. 2009, 29, 1925–1932. [Google Scholar] [CrossRef]
- Chen, S.; Wang, W.; Kono, H.; Sassa, K.; Asai, S. Abnormal grain growth of hydroxyapatite ceramic sintered in a high magnetic field. J. Cryst. Growth 2010, 312, 323–326. [Google Scholar]
- Muralithran, G.; Ramesh, S. Effects of sintering temperature on the properties of hydroxyapatite. Ceram. Int. 2000, 26, 221–230. [Google Scholar] [CrossRef]
- Bernache-Assollant, D.; Ababou, A.; Champion, E.; Heughebaert, M. Sintering of calcium phosphate hydroxyapatite Ca10(PO4)6(OH)2 I. Calcination and particle growth. J. Eur. Ceram. Soc. 2003, 23, 229–241. [Google Scholar] [CrossRef]
- Ramesh, S.; Tan, C.Y.; Bhaduri, S.B.; Teng, W.D. opyan I. Densification behaviour of nanocrystalline hydroxyapatite bioceramics. J. Mater. Proc. Technol. 2008, 206, 221–230. [Google Scholar]
- Kobayashi, S.; Kawai, W.; Wakayama, S. The effect of pressure during sintering on the strength and the fracture toughness of hydroxyapatite ceramics. J. Mater. Sci. Mater. Med. 2006, 17, 1089–1093. [Google Scholar] [CrossRef]
- Kasuga, T.; Ota, Y.; Tsuji, K.; Abe, Y. Preparation of high-strength calcium phosphate ceramics with low modulus of elasticity containing β-Ca(PO3)2 fibers. J. Am. Ceram. Soc. 1996, 79, 1821–1824. [Google Scholar] [CrossRef]
- Suchanek, W.L.; Yoshimura, M. Preparation of fibrous, porous hydroxyapatite ceramics from hydroxyapatite whiskers. J. Am. Ceram. Soc. 1998, 81, 765–767. [Google Scholar] [CrossRef]
- Kim, Y.; Kim, S.R.; Song, H.; Yoon, H. Preparation of porous hydroxyapatite/TCP composite block using a hydrothermal hot pressing method. Mater. Sci. Forum 2005, 486-487, 117–120. [Google Scholar] [CrossRef]
- Li, J.G.; Hashida, T. Preparation of hydroxyapatite ceramics by hydrothermal hot-pressing method at 300 °C. J. Mater. Sci. 2007, 42, 5013–5019. [Google Scholar] [CrossRef]
- Li, J.G.; Hashida, T. In situ formation of hydroxyapatite-whisker ceramics by hydrothermal hot-pressing method. J. Am. Ceram. Soc. 2006, 89, 3544–3546. [Google Scholar] [CrossRef]
- Halouani, R.; Bernache-Assolant, D.; Champion, E.; Ababou, A. Microstructure and related mechanical properties of hot pressed hydroxyapatite ceramics. J. Mater. Sci. Mater. Med. 1994, 5, 563–568. [Google Scholar] [CrossRef]
- Nakahira, A.; Murakami, T.; Onoki, T.; Hashida, T.; Hosoi, K. Fabrication of porous hydroxyapatite using hydrothermal hot pressing and post-sintering. J. Am. Ceram. Soc. 2005, 88, 1334–1336. [Google Scholar] [CrossRef]
- Auger, M.A.; Savoini, B.; Muñoz, A.; Leguey, T.; Monge, M.A.; Pareja, R.; Victoria, J. Mechanical characteristics of porous hydroxyapatite/oxide composites produced by post-sintering hot isostatic pressing. Ceram. Int. 2009, 35, 2373–2380. [Google Scholar] [CrossRef]
- Fang, Y.; Agrawal, D.K.; Roy, D.M.; Roy, R. Microwave sintering of hydroxyapatite ceramics. J. Mater. Res. 1994, 9, 180–187. [Google Scholar] [CrossRef]
- Yang, Y.; Ong, J.L.; Tian, J. Rapid sintering of hydroxyapatite by microwave processing. J. Mater. Sci. Lett. 2002, 21, 67–69. [Google Scholar] [CrossRef]
- Nath, S.; Basu, B.; Sinha, A. A comparative study of conventional sintering with microwave sintering of hydroxyapatite synthesized by chemical route. Trends Biomater. Artif. Organs 2006, 19, 93–98. [Google Scholar]
- Ramesh, S.; Tan, C.Y.; Bhaduri, S.B.; Teng, W.D. Rapid densification of nanocrystalline hydroxyapatite for biomedical applications. Ceram. Int. 2007, 33, 1363–1367. [Google Scholar] [CrossRef]
- Silva, C.C.; Graça, M.P.F.; Sombra, A.S.B.; Valente, M.A. Structural and electrical study of calcium phosphate obtained by a microwave radiation assisted procedure. Phys. Rev. B—Condens. Matter. 2009, 404, 1503–1508. [Google Scholar] [CrossRef]
- Chanda, A.; Dasgupta, S.; Bose, S.; Bandyopadhyay, A. Microwave sintering of calcium phosphate ceramics. Mater. Sci. Eng. C 2009, 29, 1144–1149. [Google Scholar] [CrossRef]
- Veljović, D.; Zalite, I.; Palcevskis, E.; Smiciklas, I.; Petrović, R.; Janaćković, D. Microwave sintering of fine grained HAP and HAP/TCP bioceramics. Ceram. Int. 2010, 36, 595–603. [Google Scholar] [CrossRef]
- Kalita, S.J.; Verma, S. Nanocrystalline hydroxyapatite bioceramic using microwave radiation: Synthesis and characterization. Mater. Sci. Eng. C 2010, 30, 295–303. [Google Scholar] [CrossRef]
- Gu, Y.W.; Loh, N.H.; Khor, K.A.; Tor, S.B.; Cheang, P. Spark plasma sintering of hydroxyapatite powders. Biomaterials 2002, 23, 37–43. [Google Scholar] [CrossRef]
- Guo, X.; Xiao, P.; Liu, J.; Shen, Z. Fabrication of nanostructured hydroxyapatite via hydrothermal synthesis and spark plasma sintering. J. Am. Ceram. Soc. 2005, 88, 1026–1029. [Google Scholar] [CrossRef]
- Drouet, C.; Largeot, C.; Raimbeaux, G.; Estournès, C.; Dechambre, G.; Combes, C.; Rey, C. Bioceramics: Spark plasma sintering (SPS) of calcium phosphates. Adv. Sci. Technol. 2006, 49, 45–50. [Google Scholar] [CrossRef]
- Li, H.; Khor, K.A.; Chow, V.; Cheang, P. Nanostructural characteristics, mechanical properties and osteoblast response of spark plasma sintered hydroxyapatite. J. Biomed. Mater. Res. A 2007, 82A, 296–303. [Google Scholar]
- Nakamura, T.; Fukuhara, T.; Izui, H. Mechanical properties of hydroxyapatites sintered by spark plasma sintering. Ceram. Trans. 2006, 194, 265–272. [Google Scholar]
- Kawagoe, D.; Ioku, K.; Fujimori, H.; Goto, S. Transparent β-tricalcium phosphate ceramics prepared by spark plasma sintering. J. Ceram. Soc. Jpn. 2004, 112, 462–463. [Google Scholar] [CrossRef]
- Zhang, F.; Lin, K.; Chang, J.; Lu, J.; Ning, C. Spark plasma sintering of macroporous calcium phosphate scaffolds from nanocrystalline powders. J. Eur. Ceram. Soc. 2008, 28, 539–545. [Google Scholar] [CrossRef]
- Grossin, D.; Rollin-Martinet, S.; Estournès, C.; Rossignol, F.; Champion, E.; Combes, C.; Rey, C.; Geoffroy, C.; Drouet, C. Biomimetic apatite sintered at very low temperature by spark plasma sintering: Physico-chemistry and microstructure aspects. Acta Biomater. 2010, 6, 577–585. [Google Scholar] [CrossRef] [Green Version]
- Chesnaud, A.; Bogicevic, C.; Karolak, F.; Estournès, C.; Dezanneau, G. Preparation of transparent oxyapatite ceramics by combined use of freeze-drying and spark-plasma sintering. Chem. Comm. 2007, 1550–1552. [Google Scholar]
- Ishihara, S.; Matsumoto, T.; Onoki, T.; Sohmura, T.; Nakahira, A. New concept bioceramics composed of octacalcium phosphate (OCP) and dicarboxylic acid-intercalated OCP via hydrothermal hot-pressing. Mater. Sci. Eng. C 2009, 29, 1885–1888. [Google Scholar]
- Gross, K.A.; Berndt, C.C. Biomedical application of apatites. In Phosphates: Geochemical, Geobiological And Materials Importance; Series: Reviews in Mineralogy and Geochemistry; Hughes, J.M., Kohn, M., Rakovan, J., Eds.; Mineralogical Society of America: Washington, DC, USA, 2002; Volume 48, pp. 631–672. [Google Scholar]
- LeGeros, R.Z.; LeGeros, J.P. Dense hydroxyapatite. In An Introduction to Bioceramics; Hench, L.L., Wilson, J., Eds.; World Scientific: London, UK, 1993; pp. 139–180. [Google Scholar]
- Evans, J.R.G. Seventy ways to make ceramics. J. Eur. Ceram. Soc. 2008, 28, 1421–1432. [Google Scholar] [CrossRef]
- Benaqqa, C.; Chevalier, J.; Saädaoui, M.; Fantozzi, G. Slow crack growth behaviour of hydroxyapatite ceramics. Biomaterials 2005, 26, 6106–6112. [Google Scholar] [CrossRef]
- Linhart, W.; Briem, D.; Amling, M.; Rueger, J.M.; Windolf, J. Mechanical failure of porous hydroxyapatite ceramics 7.5 years after implantation in the proximal tibial. Unfallchirurg. 2004, 107, 154–157. [Google Scholar]
- In materials science, fracture toughness is a property, which describes the ability of a material containing a crack to resist fracture and is one of the most important properties of any material for virtually all design applications
- Ramesh, S.; Tan, C.Y.; Sopyan, I.; Hamdi, M.; Teng, W.D. Consolidation of nanocrystalline hydroxyapatite powder. Sci. Technol. Adv. Mater. 2007, 8, 124–130. [Google Scholar] [CrossRef]
- The nature of flaws in most ceramics is statistical. As such, the strength of ceramics is not one specific value, but a distribution of strengths. The Weibull modulus is a measure of the distribution of flaws, usually for a brittle material. The modulus is a dimensionless number corresponding to the ability in measured strength and reflects the distribution of flaws in the material
- Suzuki, S.; Sakamura, M.; Ichiyanagi, M.; Ozawa, M. Internal friction of hydroxyapatite and fluorapatite. Ceram. Int. 2004, 30, 625–627. [Google Scholar] [CrossRef]
- Strength can be defined as the maximum tensile stresses that a material can endure before fracture occurs. It might also be defined as force per unit area required to initiate and propagate a crack to the fracture point [179]
- In materials science, fatigue is the progressive and localized structural damage that occurs when a material is subjected to cyclic loading
- le Huec, J.C.; Schaeverbeke, T.; Clement, D.; Faber, J.; le Rebeller, A. Influence of porosity on the mechanical resistance of hydroxyapatite ceramics under compressive stress. Biomaterials 1995, 16, 113–118. [Google Scholar] [CrossRef]
- Hsu, Y.H.; Turner, I.G.; Miles, A.W. Mechanical properties of three different compositions of calcium phosphate bioceramic following immersion in Ringer’s solution and distilled water. J. Mater. Sci. Mater. Med. 2009, 20, 2367–2374. [Google Scholar] [CrossRef]
- The elastic modulus is the ratio of stress to strain below the proportional limit. It represents the magnitude of the interatomic stiffness of a material within the elastic range when tensile or compressive forces are applied. It is also an indication of the amount of reversible deformation that will ur in a structure when a load is applied [179]
- De Aza, P.N.; De Aza, A.H.; De Aza, S. Crystalline bioceramic materials. Bol. Soc. Esp. Ceram. V. 2005, 44, 135–145. [Google Scholar] [CrossRef]
- Ching, W.Y.; Rulis, P.; Misra, A. Ab initio elastic properties and tensile strength of crystalline hydroxyapatite. Acta Biomater. 2009, 5, 3067–3075. [Google Scholar] [CrossRef]
- Hardness of a material usually is considered as a measure of the resistance to permanent indentation. A standardized force or weight is applied to an indenter pressing into the surface of a material to create a symmetrical shaped indentation [179]
- Poisson’s ratio (ν), named after Siméon Poisson, is the ratio, when a sample object is stretched, of the contraction or transverse strain (perpendicular to the applied load), to the extension or axial strain (in the direction of the applied load)
- Burger, E.L.; Patel, V. Calcium phosphates as bone graft extenders. Orthopedics 2007, 30, 939–942. [Google Scholar]
- Rodriguez-Lorenzo, L.M.; Vallet-Regí, M.; Ferreira, J.M.F.; Ginebra, M.P.; Aparicio, C.; Planell, J. A hydroxyapatite ceramic bodies with tailored mechanical properties for different applications. J. Biomed. Mater. Res. 2002, 60, 159–166. [Google Scholar]
- Dorozhkin, S.V. Calcium orthophosphate-based biocomposites and hybrid biomaterials. J. Mater. Sci. 2009, 44, 2343–2387. [Google Scholar] [CrossRef]
- Bouslama, N.; Ben Ayed, F.; Bouaziz, J. Sintering and mechanical properties of tricalcium phosphate – fluorapatite composites. Ceram. Int. 2009, 35, 1909–1917. [Google Scholar] [CrossRef]
- Suchanek, W.; Yashima, M.; Kakihana, M.; Yoshimura, M. Processing and mechanical properties of hydroxyapatite reinforced with hydroxyapatite whiskers. Biomaterials 1996, 17, 1715–1723. [Google Scholar] [CrossRef]
- Suchanek, W.; Yashima, M.; Kakihana, M.; Yoshimura, M. Hydroxyapatite/hydroxyapatite-whisker composites without sintering additives: Mechanical properties and microstructural evolution. J. Am. Ceram. Soc. 1997, 80, 2805–2813. [Google Scholar]
- Simsek, D.; Ciftcioglu, R.; Guden, M.; Ciftcioglu, M.; Harsa, S. Mechanical properties of hydroxyapatite composites reinforced with hydroxyapatite whiskers. Key Eng. Mater. 2004, 264-268, 1985–1988. [Google Scholar] [CrossRef]
- Bose, S.; Banerjee, A.; Dasgupta, S.; Bandyopadhyay, A. Synthesis, processing, mechanical, and biological property characterization of hydroxyapatite whisker-reinforced hydroxyapatite composites. J. Am. Ceram. Soc. 2009, 92, 323–330. [Google Scholar] [CrossRef]
- Shiota, T.; Shibata, M.; Yasuda, K.; Matsuo, Y. Influence of β-tricalcium phosphate dispersion on mechanical properties of hydroxyapatite ceramics. J. Ceram. Soc. Jpn. 2009, 116, 1002–1005. [Google Scholar]
- Dorozhkin, S.V.; Ajaal, T. Toughening of porous bioceramic scaffolds by bioresorbable polymeric coatings. Proc. Inst. Mech. Eng. Part H: J. Eng. Med. 2009, 223, 459–470. [Google Scholar] [CrossRef]
- Dorozhkin, S.V.; Ajaal, T. Strengthening of dense bioceramic samples using bioresorbable polymers—A statistical approach. J. Biomim. Biomater. Tissue Eng. 2009, 4, 27–39. [Google Scholar] [CrossRef]
- He, L.H.; Standard, O.C.; Huang, T.T.; Latella, B.A.; Swain, M.V. Mechanical behaviour of porous hydroxyapatite. Acta Biomater. 2008, 4, 577–586. [Google Scholar] [CrossRef]
- Nagai, M.; Nishino, T. Surface conduction of porous hydroxyapatite ceramics at elevated temperatures. Solid State Ionics 1988, 28-30, 1456–1461. [Google Scholar] [CrossRef]
- Yamashita, K.; Owada, H.; Umegaki, T.; Kanazawa, T.; Futagamu, T. Ionic conduction in apatite solid solutions. Solid State Ionics 1988, 28-30, 660–663. [Google Scholar] [CrossRef]
- Mahabole, M.P.; Aiyer, R.C.; Ramakrishna, C.V.; Sreedhar, B.; Khairnar, R.S. Synthesis, characterization and gas sensing property of hydroxyapatite ceramic. Bull. Mater. Sci. 2005, 28, 535–545. [Google Scholar]
- Fanovich, M.A.; Castro, M.S.; Lopez, J.M.P. Analysis of the microstructural evolution in hydroxyapatite ceramics by electrical characterisation. Ceram. Int. 1999, 25, 517–522. [Google Scholar] [CrossRef]
- Valdes, J.J.P.; Rodriguez, A.V.; Carrio, J.G. Dielectric properties and structure of hydroxyapatite ceramics sintered by different conditions. J. Mater. Res. 1995, 10, 2174–2177. [Google Scholar] [CrossRef]
- Bensaoud, A.; Bouhaouss, A.; Ferhat, M. Electrical properties in compressed poorly crystalline apatite. J. Solid State Electrochem. 2001, 5, 362–365. [Google Scholar] [CrossRef]
- Tanaka, Y.; Nakamura, M.; Nagai, A.; Toyama, T.; Yamashita, K. Ionic conduction mechanism in Ca-deficient hydroxyapatite whiskers. Mater. Sci. Eng. B 2009, 161, 115–119. [Google Scholar] [CrossRef]
- Tanaka, Y.; Takata, S.; Shimoe, K.; Nakamura, M.; Nagai, A.; Toyama, T.; Yamashita, K. Conduction properties of non-stoichiometric hydroxyapatite whiskers for biomedical use. J. Ceram. Soc. Jpn. 2008, 116, 815–821. [Google Scholar] [CrossRef]
- Nakamura, S.; Takeda, H.; Yamashita, K. Proton transport polarization and depolarization of hydroxyapatite ceramics. J. Appl. Phys. 2001, 89, 5386–5392. [Google Scholar] [CrossRef]
- Gittings, J.P.; Bowen, C.R.; Turner, I.G.; Baxter, F.R.; Chaudhuri, J.B. Polarisation behaviour of calcium phosphate based ceramics. Mater. Sci. Forum 2008, 587-588, 91–95. [Google Scholar] [CrossRef]
- Itoh, S.; Nakamura, S.; Kobayashi, T.; Shinomiya, K.; Yamashita, K.; Itoh, S. Effect of electrical polarization of hydroxyapatite ceramics on new bone formation. Calcif. Tissue Int. 2006, 78, 133–142. [Google Scholar] [CrossRef]
- Iwasaki, T.; Tanaka, Y.; Nakamura, M.; Nagai, A.; Hashimoto, K.; Toda, Y.; Katayama, K.; Yamashita, K. Rate of bonelike apatite formation accelerated on polarized porous hydroxyapatite. J. Am. Ceram. Soc. 2008, 91, 3943–3949. [Google Scholar] [CrossRef]
- Itoh, S.; Nakamura, S.; Kobayashi, T.; Shinomiya, K.; Yamashita, K. Enhanced bone ingrowth into hydroxyapatite with interconnected pores by electrical polarization. Biomaterials 2006, 27, 5572–5579. [Google Scholar] [CrossRef]
- Kobayashi, T.; Itoh, S.; Nakamura, S.; Nakamura, M.; Shinomiya, K.; Yamashita, K. Enhanced bone bonding of hydroxyapatite-coated titanium implants by electrical polarization. J. Biomed. Mater. Res. A 2007, 82A, 145–151. [Google Scholar] [CrossRef]
- Bodhak, S.; Bose, S.; Bandyopadhyay, A. Role of surface charge and wettability on early stage mineralization and bone cell-materials interactions of polarized hydroxyapatite. Acta Biomater. 2009, 5, 2178–2188. [Google Scholar] [CrossRef]
- Yamashita, K.; Oikawa, N.; Umegaki, T. Acceleration and deceleration of bone-like crystal growth on ceramic hydroxyapatite by electric poling. Chem. Mater. 1996, 8, 2697–2700. [Google Scholar] [CrossRef]
- Teng, N.C.; Nakamura, S.; Takagi, Y.; Yamashita, Y.; Ohgaki, M.; Yamashita, K. A new approach to enhancement of bone formation by electrically polarized hydroxyapatite. J. Dental Res. 2001, 80, 1925–1929. [Google Scholar] [CrossRef]
- Kobayashi, T.; Nakamura, S.; Yamashita, K. Enhanced osteobonding by negative surface charges of electrically polarized hydroxyapatite. J. Biomed. Mater. Res. 2001, 57, 477–484. [Google Scholar] [CrossRef]
- Park, Y.J.; Hwang, K.S.; Song, J.E.; Ong, J.L.; Rawls, H.R. Growth of calcium phosphate on poling treated ferroelectric BaTiO3 ceramics. Biomaterials 2002, 23, 3859–3864. [Google Scholar]
- Hwang, K.S.; Song, J.E.; Jo, J.W.; Yang, H.S.; Park, Y.J.; Ong, J.L.; Rawls, H.R. Effect of poling conditions on growth of calcium phosphate crystal in ferroelectric BaTiO3 ceramics. J. Mater. Sci. Mater. Med. 2002, 13, 133–138. [Google Scholar] [CrossRef]
- Yamashita, K. Enhanced bioactivity of electrically poled hydroxyapatita ceramics and coatings. Mater. Sci. Forum 2003, 426-432, 3237–3242. [Google Scholar]
- Nakamura, S.; Kobayashi, T.; Yamashita, K. Highly orientated calcification in newly formed bones on negatively charged hydroxyapatite electrets. Key Eng. Mater. 2005, 284-286, 897–900. [Google Scholar] [CrossRef]
- Kato, R.; Nakamura, S.; Katayama, K.; Yamashita, K. Electrical polarization of plasma-spray-hydroxyapatite coatings for improvement of osteoconduction of implants. J. Biomed. Mater. Res. A 2005, 74A, 652–658. [Google Scholar] [CrossRef]
- Nakamura, S.; Kobayashi, T.; Nakamura, M.; Itoh, S.; Yamashita, K. Electrostatic surface charge acceleration of bone ingrowth of porous hydroxyapatite/β-tricalcium phosphate ceramics. J. Biomed. Mater. Res. A 2010, 92A, 267–275. [Google Scholar] [CrossRef]
- Itoh, S.; Nakamura, S.; Nakamura, M.; Shinomiya, K.; Yamashita, K. Enhanced bone regeneration by electrical polarization of hydroxyapatite. Artif. Organs 2006, 30, 863–869. [Google Scholar]
- Nakamura, M.; Nagai, A.; Ohashi, N.; Tanaka, Y.; Sekilima, Y.; Nakamura, S. Regulation of osteoblast-like cell behaviors on hydroxyapatite by electrical polarization. Key Eng. Mater. 2008, 361-363, 1055–1058. [Google Scholar] [CrossRef]
- Nakamura, M.; Nagai, A.; Tanaka, Y.; Sekilima, Y.; Yamashita, K. Polarized hydroxyapatite promotes spread and motility of osteoblastic cells. J. Biomed. Mater. Res. A 2010, 92A, 783–790. [Google Scholar]
- Nakamura, S.; Kobayashi, T.; Yamashita, K. Extended bioactivity in the proximity of hydroxyapatite ceramic surfaces induced by polarization charges. J. Biomed. Mater. Res. 2002, 61, 593–599. [Google Scholar] [CrossRef]
- Wang, W.; Itoh, S.; Tanaka, Y.; Nagai, A.; Yamashita, K. Comparison of enhancement of bone ingrowth into hydroxyapatite ceramics with highly and poorly interconnected pores by electrical polarization. Acta Biomater. 2009, 5, 3132–3140. [Google Scholar] [CrossRef]
- Nakamura, M.; Niwa, K.; Nakamura, S.; Sekijima, Y.; Yamashita, K. Interaction of a blood coagulation factor on electrically polarized hydroxyapatite surfaces. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 82B, 29–36. [Google Scholar]
- Nagai, M.; Shibuya, Y.; Nishino, T.; Saeki, T.; Owada, H.; Yamashita, K.; Umegaki, T. Electrical conductivity of calcium phosphate ceramics with various Ca/P ratios. J. Mater. Sci. 1991, 26, 2949–2953. [Google Scholar] [CrossRef]
- Laghzizil, A.; Elherch, N.; Bouhaouss, A.; Lorente, G.; Coradin, T.; Livage, J. Electrical behavior of hydroxyapatites M10(PO4)6(OH)2 (M = Ca, Pb, Ba). Mater. Res. Bull. 2001, 36, 953–962. [Google Scholar]
- Louati, B.; Guidara, K.; Gargouri, M. Dielectric and ac ionic conductivity investigations in the monetite. J. Alloys Compd. 2009, 472, 347–351. [Google Scholar] [CrossRef]
- Gittings, J.P.; Bowen, C.R.; Dent, A.C.; Turner, I.G.; Baxter, F.R.; Chaudhuri, J.B. Electrical characterization of hydroxyapatite-based bioceramics. Acta Biomater. 2009, 5, 743–754. [Google Scholar] [CrossRef]
- Tofail, S.A.M.; Baldisserri, C.; Haverty, D.; McMonagle, J.B.; Erhart, J. Pyroelectric surface charge in hydroxyapatite ceramics. J. Appl. Phys. 2009, 106, 106104. [Google Scholar] [CrossRef]
- Fang, Y.; Agrawal, D.K.; Roy, D.M.; Roy, R. Fabrication of transparent hydroxyapatite ceramics by ambient-pressure sintering. Mater. Lett. 1995, 23, 147–151. [Google Scholar] [CrossRef]
- Kotobuki, N.; Kawagoe, D.; Fujimori, H.; Goto, S.; Loku, K.; Ohgushi, H. In vitro osteogenic activity of rat bone marrow derived mesenchymal stem cells cultured on transparent hydroxyapatite ceramics. Key Eng. Mater. 2004, 254-256, 1055–1058. [Google Scholar] [CrossRef]
- Kotobuki, N.; Ioku, K.; Kawagoe, D.; Nomura, D.; Fujimori, H.; Goto, S.; Ohgushi, H. In vitro osteogenic activity of rat mesenchymal cells cultured on transparent β-tricalcium phosphate ceramics. Key Eng. Mater. 2005, 284-286, 663–666. [Google Scholar] [CrossRef]
- Varma, H.; Vijayan, S.P.; Babu, S.S. Transparent hydroxyapatite ceramics through gel-casting and low-temperature sintering. J. Am. Ceram. Soc. 2002, 85, 493–495. [Google Scholar] [CrossRef]
- Watanabe, Y.; Ikoma, T.; Monkawa, A.; Suetsugu, Y.; Yamada, H.; Tanaka, J.; Moriyoshi, Y. Fabrication of transparent hydroxyapatite sintered body with high crystal orientation by pulse electric current sintering. J. Am. Ceram. Soc. 2005, 88, 243–245. [Google Scholar]
- Kotobuki, N.; Ioku, K.; Kawagoe, D.; Fujimori, H.; Goto, S.; Ohgushi, H. Observation of osteogenic differentiation cascade of living mesenchymal stem cells on transparent hydroxyapatite ceramics. Biomaterials 2005, 26, 779–785. [Google Scholar]
- John, A.; Varma, H.K.; Vijayan, S.; Bernhardt, A.; Lode, A.; Vogel, A.; Burmeister, B.; Hanke, T.; Domaschke, H.; Gelinsky, M. In vitro investigations of bone remodeling on a transparent hydroxyapatite ceramic. Biomed. Mater. 2009, 4, 015007–015015. [Google Scholar]
- Kotobuki, N.; Kawagoe, D.; Nomura, D.; Katou, Y.; Muraki, K.; Fujimori, H.; Goto, S.; Ioku, K.; Ohgushi, H. Observation and quantitative analysis of rat bone marrow stromal cells cultured in vitro on newly formed transparent β-tricalcium phosphate. J. Mater. Sci. Mater. Med. 2006, 17, 33–41. [Google Scholar] [CrossRef]
- Tancred, D.C.; McCormack, B.A.; Carr, A.J. A synthetic bone implant macroscopically identical to cancellous bone. Biomaterials 1998, 19, 2303–2311. [Google Scholar] [CrossRef]
- Miao, X.; Sun, D. Graded/gradient porous biomaterials. Materials 2010, 3, 26–47. [Google Scholar] [CrossRef]
- Bucholz, R.W.; Carlton, A.; Holmes, R. Interporous hydroxyapatite as a bone graft substitute in tibial plateau fractures. Clin. Orthop. 1989, 240, 53–62. [Google Scholar]
- Cavagna, R.; Daculsi, G.; Bouler, J.M. Macroporous calcium phosphate ceramic: A prospective study of 106 cases in lumbar spinal fusion. J. Long Term Eff. Med. Implants 1999, 9, 403–412. [Google Scholar]
- Lu, J.X.; Flautre, B.; Anselme, K.; Hardouin, P.; Gallur, A.; Descamps, M.; Thierry, B. Role of interconnections in porous bioceramics on bone recolonization in vitro and in vivo. J. Mater. Sci. Mater. Med. 1999, 10, 111–120. [Google Scholar] [CrossRef]
- Ayers, R.A.; Simske, S.J.; Nunes, C.R.; Wolford, L.M. Long-term bone ingrowth and residual microhardness of porous block hydroxyapatite implants in humans. J. Oral Maxillof. Surg. 1998, 56 Suppl. 5, 1297–1302. [Google Scholar] [CrossRef]
- Jones, A.C.; Arns, C.H.; Sheppard, A.P.; Hutmacher, D.W.; Milthorpe, B.K.; Knackstedt, M.A. Assessment of bone ingrowth into porous biomaterials using MICRO-CT. Biomaterials 2007, 28, 2491–2504. [Google Scholar]
- Karageorgiou, V.; Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 2005, 26, 5474–5491. [Google Scholar] [CrossRef]
- Ohgushi, H.; Goldberg, V.M.; Caplan, A.I. Heterotopic osteogenesis in porous ceramics induced by marrow cells. J. Orthop. Res. 1989, 7, 568–578. [Google Scholar] [CrossRef]
- Cheung, H.S.; Haak, M.H. Growth of osteoblasts on porous calcium phosphate ceramic: An in vitro model for biocompatibility study. Biomaterials 1989, 10, 63–67. [Google Scholar] [CrossRef]
- Zyman, Z.; Ivanov, I.; Glushko, V.; Dedukh, N.; Malyshkina, S. Inorganic phase composition of remineralisation in porous CaP ceramics. Biomaterials 1998, 19, 1269–1273. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Ohgushi, H.; Tamai, S. Immediate bone forming capability of prefabricated osteogenic hydroxyapatite. J. Biomed. Mater. Res. 1996, 32, 481–492. [Google Scholar] [CrossRef]
- Chang, B.S.; Lee, C.K.; Hong, K.S.; Youn, H.J.; Ryu, H.S.; Chung, S.S.; Park, K. Osteoconduction at porous hydroxyapatite with various pore configurations. Biomaterials 2000, 21, 1291–1298. [Google Scholar]
- Flautre, B.; Descamps, M.; Delecourt, C.; Blary, M.C.; Hardouin, P. Porous HA ceramic for bone replacement: Role of the pores and interconnections-experimental study in the rabbits. J. Mater. Sci. Mater. Med. 2001, 12, 679–682. [Google Scholar] [CrossRef]
- McAfee, P.C.; Cunningham, B.W.; Orbegoso, D.O.; Sefter, J.C.; Dmitriev, A.E.; Fedder, I.L. Analysis of porous ingrowth in intervertebral disc prostheses. Spine 2003, 28, 332–340. [Google Scholar]
- Tamai, N.; Myoui, A.; Tomita, T.; Nakase, T.; Tanaka, J.; Ochi, T.; Yoshikawa, H. Novel hydroxyapatite ceramics with an interconnective porous structure exhibit superior osteoconduction in vivo. J. Biomed. Mater. Res. 2002, 59, 110–117. [Google Scholar]
- Mastrogiacomo, M.; Scaglione, S.; Martinetti, R.; Dolcini, L.; Beltrame, F.; Cancedda, R.; Quarto, R. Role of scaffold internal structure on in vivo bone formation in macroporous calcium phosphate bioceramics. Biomaterials 2006, 27, 3230–3237. [Google Scholar]
- Okamoto, M.; Dohi, Y.; Ohgushi, H.; Shimaoka, H.; Ikeuchi, M.; Matsushima, A.; Yonemasu, K.; Hosoi, H. Influence of the porosity of hydroxyapatite ceramics on in vitro and in vivo bone formation by cultured rat bone marrow stromal cells. J. Mater. Sci. Mater. Med. 2006, 17, 327–336. [Google Scholar] [CrossRef]
- Zhang, L.; Hanagata, N.; Maeda, M.; Minowa, T.; Ikoma, T.; Fan, H.; Zhang, X. Porous hydroxyapatite and biphasic calcium phosphate ceramics promote ectopic osteoblast differentiation from mesenchymal stem cells. Sci. Technol. Adv. Mater. 2009, 10, 025003–025011. [Google Scholar] [CrossRef]
- Omae, H.; Mochizuki, Y.; Yokoya, S.; Adachi, N.; Ochi, M. Effects of interconnecting porous structure of hydroxyapatite ceramics on interface between grafted tendon and ceramics. J. Biomed. Mater. Res. A 2006, 79A, 329–337. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Tamai, N.; Murase, T.; Myoui, A. Interconnected porous hydroxyapatite ceramics for bone tissue engineering. J. R. Soc. Interface 2009, 6, S341–S348. [Google Scholar] [CrossRef]
- Takagi, S.; Chow, L.C. Formation of macropores in calcium phosphate cement implants. J. Biomed. Mater. Res. 2001, 12, 135–139. [Google Scholar]
- Walsh, D.; Tanaka, J. Preparation of a bone-like apatite foam cement. J. Mater. Sci. Mater. Med. 2001, 12, 339–344. [Google Scholar] [CrossRef]
- Chevalier, E.; Chulia, D.; Pouget, C.; Viana, M. Fabrication of porous substrates: A review of processes using pore forming agents in the biomaterial field. J. Pharm. Sci. 2008, 97, 1135–1154. [Google Scholar] [CrossRef]
- Komlev, V.S.; Barinov, S.M. Porous hydroxyapatite ceramics of bi-modal pore size distribution. J. Mater. Sci. Mater. Med. 2002, 13, 295–299. [Google Scholar] [CrossRef]
- Sepulveda, P.; Binner, J.G.; Rogero, S.O.; Higa, O.Z.; Bressiani, J.C. Production of porous hydroxyapatite by the gel-casting of foams and cytotoxic evaluation. J. Biomed. Mater. Res. 2000, 50, 27–34. [Google Scholar] [CrossRef]
- Hsu, Y.H.; Turner, I.G.; Miles, A.W. Mechanical characterization of dense calcium phosphate bioceramics with interconnected porosity. J. Mater. Sci. Mater. Med. 2007, 18, 2319–2329. [Google Scholar] [CrossRef]
- Zhang, H.G.; Zhu, Q. Preparation of porous hydroxyapatite with interconnected pore architecture. J. Mater. Sci. Mater. Med. 2007, 18, 1825–1829. [Google Scholar] [CrossRef]
- le Ray, A.M.; Gautier, H.; Bouler, J.M.; Weiss, P.; Merle, C. A new technological procedure using sucrose as porogen compound to manufacture porous biphasic calcium phosphate ceramics of appropriate micro- and macrostructure. Ceram. Int. 2010, 36, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Guda, T.; Appleford, M.; Oh, S.; Ong, J.L. A cellular perspective to bioceramic scaffolds for bone tissue engineering: The state of the art. Curr. Topics Med. Chem. 2008, 8, 290–299. [Google Scholar] [CrossRef]
- Ota, Y.; Kasuga, T.; Abe, Y. Preparation and compressive strength behaviour of porous ceramics with β-Ca3(PO3)2 fiber skeletons. J. Am. Ceram. Soc. 1997, 80, 225–231. [Google Scholar] [CrossRef]
- White, E.; Shors, E.C. Biomaterial aspects of Interpore-200 porous hydroxyapatite. Dent. Clin. North Am. 1986, 30, 49–67. [Google Scholar]
- Descamps, M.; Duhoo, T.; Monchau, F.; Lu, J.; Hardouin, P.; Hornez, J.C.; Leriche, A. Manufacture of macroporous β-tricalcium phosphate bioceramics. J. Eur. Ceram. Soc. 2008, 28, 149–157. [Google Scholar] [CrossRef]
- Engin, N.O.; Tas, A.C. Manufacture of macroporous calcium hydroxyapatite bioceramics. J. Eur. Ceram. Soc. 1999, 19, 2569–2572. [Google Scholar]
- Liu, D.M. Fabrication of hydroxyapatite ceramic with controlled porosity. J. Mater. Sci. Mater. Med. 1997, 8, 227–232. [Google Scholar] [CrossRef]
- Rivera-Munoz, E.; Diaz, J.R.; Rodriguez, J.R.; Brostow, W.; Castano, V.M. Hydroxyapatite spheres with controlled porosity for eye ball prosthesis: Processing and characterization. J. Mater. Sci. Mater. Med. 2001, 12, 305–311. [Google Scholar] [CrossRef]
- Hosoi, K.; Hashida, T.; Takahashi, H.; Yamasaki, N.; Korenaga, T. New processing technique for hydroxyapatite ceramics by the hydrothermal hot-pressing method. J. Am. Ceram. Soc. 1996, 79, 2771–2774. [Google Scholar]
- Walsh, D.; Hopwood, J.D.; Mann, S. Crystal tectonics: Construction of reticulated calcium phosphate frameworks in bicontinuous reverse microemulsions. Science 1994, 264, 1576–1578. [Google Scholar]
- Walsh, D.; Mann, S. Chemical synthesis of microskeletal calcium phosphate in bicontinuous microemulsions. Chem. Mater. 1996, 8, 1944–1953. [Google Scholar] [CrossRef]
- Charriere, E.; Lemaitre, J.; Zysset, P. Hydroxyapatite cement scaffolds with controlled macroporosity: Fabrication protocol and mechanical properties. Biomaterials 2003, 24, 809–817. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, D.; Huang, W.; Yao, A.; Kamitakahara, M.; Ioku, K. Preparation and characterization of periodic porous frame of hydroxyapatite. J. Ceram. Soc. Jpn. 2009, 117, 521–524. [Google Scholar] [CrossRef]
- Moroni, L.; De Wijn, J.R.; Van Blitterswijk, C.A. Integrating novel Technologies to fabricate smart scaffolds. J. Biomater. Sci. Polymer Ed. 2008, 19, 543–572. [Google Scholar] [CrossRef]
- Aizawa, M.; Howell, S.F.; Itatani, K.; Yokogawa, Y.; Nishizawa, K.; Toriyama, M.; Kameyama, T. Fabrication of porous ceramics with well-controlled open pores by sintering of fibrous hydroxyapatite particles. J. Ceram. Soc. Jpn. 2000, 108, 249–253. [Google Scholar] [CrossRef]
- Kawata, M.; Uchida, H.; Itatani, K.; Okada, I.; Koda, S.; Aizawa, M. Development of porous ceramics with well-controlled porosities and pore sizes from apatite fibers and their evaluations. J. Mater. Sci. Mater. Med. 2004, 15, 817–823. [Google Scholar] [CrossRef]
- Li, S.H.; De Wijn, J.R.; Layrolle, P.; De Groot, K. Novel method to manufacture porous hydroxyapatite by dual-phase mixing. J. Am. Ceram. Soc. 2003, 86, 65–72. [Google Scholar] [CrossRef]
- Koh, Y.H.; Kim, H.W.; Kim, H.E.; Halloran, J.W. Fabrication of macrochannelled-hydroxyapatite bioceramic by a coextrusion process. J. Am. Ceram. Soc. 2002, 85, 2578–2580. [Google Scholar] [CrossRef]
- Nakahira, A.; Tamai, M.; Sakamoto, K.; Yamaguchi, S. Sintering and microstructure of porous hydroxyapatite. J. Ceram. Soc. Jpn. 2000, 108, 99–104. [Google Scholar] [CrossRef]
- De Sousa, F.C.G.; Evans, J.R.G. Tubular hydroxyapatite scaffolds. Adv. Appl. Ceram. 2005, 104, 30–34. [Google Scholar] [CrossRef]
- Kitamura, M.; Ohtsuki, C.; Ogata, S.I.; Kamitakahara, M.; Tanihara, M.; Miyazaki, T. Mesoporous calcium phosphate via post-treatment of α-TCP. J. Am. Ceram. Soc. 2005, 88, 822–826. [Google Scholar] [CrossRef]
- Walsh, D.; Boanini, E.; Tanaka, J.; Mann, S. Synthesis of tri-calcium phosphate sponges by interfacial deposition and thermal transformation of self-supporting calcium phosphate films. J. Mater. Chem. 2005, 15, 1043–1048. [Google Scholar] [CrossRef]
- Gonzalez-McQuire, R.; Green, D.; Walsh, D.; Hall, S.; Chane-Ching, J.Y.; Oreffo, R.O.C.; Mann, S. Fabrication of hydroxyapatite sponges by dextran sulphate/amino acid templating. Biomaterials 2005, 26, 6652–6656. [Google Scholar] [CrossRef] [Green Version]
- Ioku, K.; Kawachi, G.; Nakahara, K.; Ishida, E.H.; Minagi, H.; Okuda, T.; Yonezawa, I.; Kurosawa, H.; Ikeda, T. Porous granules of β-tricalcium phosphate composed of rod-shaped particles. Key Eng. Mater. 2006, 309-311, 1059–1062. [Google Scholar]
- Kitamura, M.; Ohtsuki, C.; Ogata, S.; Kamitakahara, M.; Tanihara, M. Microstructure and bioresorbable properties of α-TCP ceramic porous body fabricated by direct casting method. Mater. Trans. 2004, 45, 983–988. [Google Scholar] [CrossRef]
- Ramay, H.R.; Zhang, M. Preparation of porous hydroxyapatite scaffolds by combination of the gel-casting and polymer sponge methods. Biomaterials 2003, 24, 3293–3302. [Google Scholar] [CrossRef]
- Potoczek, M.; Zima, A.; Paszkiewicz, Z.; Ślósarczyk, A. Manufacturing of highly porous calcium phosphate bioceramics via gel-casting using agarose. Ceram. Int. 2009, 35, 2249–2254. [Google Scholar] [CrossRef]
- Xu, S.; Li, D.; Lu, B.; Tang, Y.; Wang, C.; Wang, Z. Fabrication of a calcium phosphate scaffold with a three dimensional channel network and its application to perfusion culture of stem cells. Rapid Prototyping J. 2007, 13, 99–106. [Google Scholar] [CrossRef]
- Li, S.H.; De Wijn, J.R.; Layrolle, P.; De Groot, K. Synthesis of macroporous hydroxyapatite scaffolds for bone tissue engineering. J. Biomed. Mater. Res. 2002, 61, 109–120. [Google Scholar] [CrossRef]
- Almirall, A.; Larrecq, G.; Delgado, J.A.; Martínez, S.; Planell, J.A.; Ginebra, M.P. Fabrication of low temperature macroporous hydroxyapatite scaffolds by foaming and hydrolysis of an α-TCP paste. Biomaterials 2004, 25, 3671–3680. [Google Scholar] [CrossRef]
- Kamitakahara, M.; Ohtsuki, C.; Kawachi, G.; Wang, D.; Ioku, K. Preparation of hydroxyapatite porous ceramics with different porous structures using a hydrothermal treatment with different aqueous solutions. J. Ceram. Soc. Jpn. 2008, 116, 6–9. [Google Scholar] [CrossRef]
- Peña, J.; Román, J.; Cabañas, M.V.; Vallet-Regí, M. An alternative technique to shape scaffolds with hierarchical porosity at physiological temperature. Acta Biomater. 2010, 6, 1288–1296. [Google Scholar] [CrossRef]
- Marcassoli, P.; Cabrini, M.; Tirillò, J.; Bartuli, C.; Palmero, P.; Montanaro, L. Mechanical characterization of hydroxyapatite micro/macro-porous ceramics obtained by means of innovative gel-casting process. Key Eng. Mater. 2010, 417-418, 565–568. [Google Scholar]
- Nakamura, S.; Nakahira, A. Synthesis and evaluation of porous hydroxyapatite prepared by hydrothermal treatment and subsequent sintering method. J. Ceram. Soc. Jpn. 2008, 116, 42–45. [Google Scholar] [CrossRef]
- Song, H.Y.; Islam, S.; Lee, B.T. A novel method to fabricate unidirectional porous hydroxyapatite body using ethanol bubbles in a viscous slurry. J. Am. Ceram. Soc. 2008, 91, 3125–3127. [Google Scholar] [CrossRef]
- Impens, S.; Schelstraete, R.; Luyten, J.; Mullens, S.; Thijs, I.; Van Humbeeck, J.; Schrooten, J. Production and characterisation of porous calcium phosphate structures with controllable hydroxyapatite/β-tricalcium phosphate ratios. Adv. Appl. Ceram. 2009, 108, 494–500. [Google Scholar] [CrossRef]
- Von Doernberg, M.C.; Von Rechenberg, B.; Bohner, M.; Grünenfelder, S.; Van Lenthe, G.H.; Müller, R.; Gasser, B.; Mathys, R.; Baroud, G.; Auer, J. In vivo behavior of calcium phosphate scaffolds with four different pore sizes. Biomaterials 2006, 27, 5186–5198. [Google Scholar] [CrossRef]
- Mygind, T.; Stiehler, M.; Baatrup, A.; Li, H.; Zou, X.; Flyvbjerg, A.; Kassem, M.; Bunger, C. Mesenchymal stem cell ingrowth and differentiation on coralline hydroxyapatite scaffolds. Biomaterials 2007, 28, 1036–1047. [Google Scholar] [CrossRef]
- Tsuruga, E.; Takita, H.; Wakisaka, Y.; Kuboki, Y. Pore size of porous hydoxyapatite as the cell-substratum controls BMP-induced osteogenesis. J. Biochem. 1997, 121, 317–324. [Google Scholar] [CrossRef]
- Hing, K.; Annaz, B.; Saeed, S.; Revell, P.; Buckland, T. Microporosity enhances bioactivity of synthetic bone graft substitutes. J. Mater. Sci. Mater. Med. 2005, 16, 467–475. [Google Scholar] [CrossRef]
- Woodard, J.R.; Hilldore, A.J.; Lan, S.K.; Park, C.J.; Morgan, A.W.; Eurell, J.A.C.; Clark, S.G.; Wheeler, M.B.; Jamison, R.D.; Wagoner, J.A.J. The mechanical properties and osteoconductivity of hydroxyapatite bone scaffolds with multi-scale porosity. Biomaterials 2007, 28, 45–54. [Google Scholar] [CrossRef]
- Ruksudjarit, A.; Pengpat, K.; Rujijanagul, G.; Tunkasiri, T. The fabrication of nanoporous hydroxyapatite ceramics. Adv. Mater. Res. 2008, 47-50, 797–800. [Google Scholar] [CrossRef]
- LeGeros, R.Z. Calcium phosphate-based osteoinductive materials. Chem. Rev. 2008, 108, 4742–4753. [Google Scholar] [CrossRef]
- Prokopiev, O.; Sevostianov, I. Dependence of the mechanical properties of sintered hydroxyapatite on the sintering temperature. Mater. Sci. Eng. A 2006, 431, 218–227. [Google Scholar] [CrossRef]
- Daculsi, G.; Jegoux, F.; Layrolle, P. The micro macroporous biphasic calcium phosphate concept for bone reconstruction and tissue engineering. In Advanced Biomaterials: Fundamentals, Processing and Applications; Basu, B., Katti, D.S., Kumar, A., Eds.; Wiley-American Ceramic Society: oken, NJ, USA, 2009; p. 768. [Google Scholar]
- Tadic, D.; Beckmann, F.; Schwarz, K.; Epple, M. A novel method to produce hydroxylapatite objects with interconnecting porosity that avoids sintering. Biomaterials 2004, 25, 3335–3340. [Google Scholar] [CrossRef]
- Woyansky, J.S.; Scott, C.E.; Minnear, W.P. Processing of porous ceramics. Am. Ceram. Soc. Bull. 1992, 71, 1674–1682. [Google Scholar]
- Vaz, L.; Lopes, A.B.; Almeida, M. Porosity control of hydroxyapatite implants. J. Mater. Sci. Mater. Med. 1999, 10, 239–242. [Google Scholar] [CrossRef]
- Yao, X.; Tan, S.; Jiang, D. Improving the properties of porous hydroxyapatite ceramics by fabricating methods. J. Mater. Sci. 2005, 40, 4939–4942. [Google Scholar] [CrossRef]
- Zhang, J.; Fujiwara, M.; Xu, Q.; Zhu, Y.; Iwasa, M.; Jiang, D. Synthesis of mesoporous calcium phosphate using hybrid templates. Micropor. Mesopor. Mater. 2008, 111, 411–416. [Google Scholar] [CrossRef]
- Simske, S.J.; Ayers, R.A.; Bateman, T.A. Porous materials for bone engineering. Mater. Sci. Forum 1997, 250, 151–182. [Google Scholar] [CrossRef]
- Wang, H.; Zhai, L.; Li, Y.; Shi, T. Preparation of irregular mesoporous hydroxyapatite. Mater. Res. Bull. 2008, 43, 1607–1614. [Google Scholar] [CrossRef]
- Cyster, L.A.; Grant, D.M.; Howdle, S.M.; Rose, F.R.A.J.; Irvine, D.J.; Freeman, D.; Scotchford, C.A.; Shakesheff, K.M. The influence of dispersant concentration on the pore morphology of hydroxyapatite ceramics for bone tissue engineering. Biomaterials 2005, 26, 697–702. [Google Scholar] [CrossRef]
- Tian, J.; Tian, J. Preparation of porous hydroxyapatite. J. Mater. Sci. 2001, 36, 3061–3066. [Google Scholar] [CrossRef]
- Rodriguez-Lorenzo, L.M.; Vallet-Regí, M.; Ferreira, J.M.F. Fabrication of porous hydroxyapatite bodies by a new direct consolidation method: Starch consolidation. J. Biomed. Mater. Res. 2002, 60, 232–240. [Google Scholar] [CrossRef]
- Lee, E.J.; Koh, Y.H.; Yoon, B.H.; Kim, H.E.; Kim, H.W. Highly porous hydroxyapatite bioceramics with interconnected pore channels using camphene-based freeze casting. Mater. Lett. 2007, 61, 2270–2273. [Google Scholar] [CrossRef]
- Jones, J.R.; Hench, L.L. Regeneration of trabecular bone using porous ceramics. Curr. Opin. Solid State Mater. Sci. 2003, 7, 301–307. [Google Scholar] [CrossRef]
- Ota, T.; Eitsuka, T.; Yoshida, H.; Adachi, N. Porous apatite ceramics derived from woods. Adv. Mater. Res. 2006, 11-12, 247–250. [Google Scholar] [CrossRef]
- Tas, A.C. Preparation of porous apatite granules from calcium phosphate cement. J. Mater. Sci. Mater. Med. 2008, 19, 2231–2239. [Google Scholar] [CrossRef]
- Fu, Q.; Rahaman, M.N.; Dogan, F.; Bal, B.S. Freeze casting of porous hydroxyapatite scaffolds. I. Processing and general microstructure. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 86B, 125–135. [Google Scholar] [CrossRef]
- Tang, Y.J.; Tang, Y.F.; Lv, C.T.; Zhou, Z.H. Preparation of uniform porous hydroxyapatite biomaterials by a new method. Appl. Surf. Sci. 2008, 254, 5359–5362. [Google Scholar] [CrossRef]
- Fan, J.; Lei, J.; Yu, C.; Tu, B.; Zhao, D. Hard-templating synthesis of a novel rod-like nanoporous calcium phosphate bioceramics and their capacity as antibiotic carriers. Mater. Chem. Phys. 2007, 103, 489–493. [Google Scholar] [CrossRef]
- Sopyan, I.; Mel, M.; Ramesh, S.; Khalid, K.A. Porous hydroxyapatite for artificial bone applications. Sci. Technol. Adv. Mater. 2007, 8, 116–123. [Google Scholar] [CrossRef]
- Rice, R.W. Porosity of ceramics. Marcel Dekker: New York, NY, USA, 1998; 560 pp. [Google Scholar]
- Fu, Y.C.; Ho, M.L.; Wu, S.C.; Hsieh, H.S.; Wang, C.K. Porous bioceramic bead prepared by calcium phosphate with sodium alginate gel and PE powder. Mater. Sci. Eng. C 2008, 28, 1149–1158. [Google Scholar] [CrossRef]
- Hsu, Y.H.; Turner, I.G.; Miles, A.W. Fabrication of porous bioceramics with porosity gradients similar to the bimodal structure of cortical and cancellous bone. J. Mater. Sci. Mater. Med. 2007, 18, 2251–2256. [Google Scholar] [CrossRef]
- Munch, E.; Franco, J.; Deville, S.; Hunger, P.; Saiz, E.; Tomsia, A.P. Porous ceramic scaffolds with complex architectures. JOM 2008, 60, 54–59. [Google Scholar]
- Macchetta, A.; Turner, I.G.; Bowen, C.R. Fabrication of HA/TCP scaffolds with a graded and porous structure using a camphene-based freeze-casting method. Acta Biomater. 2009, 5, 1319–1327. [Google Scholar] [CrossRef]
- Deville, S.; Saiz, E.; Tomsia, A.P. Freeze casting of hydroxyapatite scaffolds for bone tissue engineering. Biomaterials 2006, 27, 5480–5489. [Google Scholar] [CrossRef]
- Zuo, K.H.; Zeng, Y.P.; Jiang, D. Effect of polyvinyl alcohol additive on the pore structure and morphology of the freeze-cast hydroxyapatite ceramics. Mater. Sci. Eng. C 2010, 30, 283–287. [Google Scholar] [CrossRef]
- Yan, X.; Yu, C.; Zhou, X.; Tang, J.; Zhao, D. Highly ordered mesoporous bioactive glasses with superior in vitro bone-forming bioactivities. Angew. Chem. Int. Ed. Engl. 2004, 43, 5980–5984. [Google Scholar] [CrossRef]
- Izquierdo-Barba, I.; Ruiz-González, L.; Doadrio, J.C.; González-Calbet, J.M.; Vallet-Regí, M. Tissue regeneration: A new property of mesoporous materials. Solid State Sci. 2005, 7, 983–989. [Google Scholar] [CrossRef]
- Cosijns, A.; Vervaet, C.; Luyten, J.; Mullens, S.; Siepmann, F.; Van Hoorebeke, L.; Masschaele, B.; Cnudde, V.; Remon, J.P. Porous hydroxyapatite tablets as carriers for low-dosed drugs. Eur. J. Pharm. Biopharm. 2007, 67, 498–506. [Google Scholar] [CrossRef]
- Uchida, A.; Shinto, Y.; Araki, N.; Ono, K. Slow release of anticancer drugs from porous calcium hydroxyapatite ceramic. J. Orthop. Res. 1992, 10, 440–445. [Google Scholar] [CrossRef]
- Shinto, Y.; Uchida, A.; Korkusuz, F.; Araki, N.; Ono, K. Calcium hydroxyapatite ceramic used as a delivery system for antibiotics. J. Bone. Joint. Surg. Br. 1992, 74, 600–604. [Google Scholar]
- Martin, R.B.; Chapman, M.W.; Sharkey, N.A.; Zissimos, S.L.; Bay, B.; Shors, E.C. Bone ingrowth and mechanical properties of coralline hydroxyapatite 1 yr after implantation. Biomaterials 1993, 14, 341–348. [Google Scholar] [CrossRef]
- Kazakia, G.J.; Nauman, E.A.; Ebenstein, D.M.; Halloran, B.P.; Keaveny, T.M. Effects of in vitro bone formation on the mechanical properties of a trabeculated hydroxyapatite bone substitute. J. Biomed. Mater. Res. A 2006, 77A, 688–699. [Google Scholar] [CrossRef]
- Hing, K.A.; Best, S.M.; Tanner, K.E.; Bonfield, W.; Revell, P.A. Mediation of bone ingrowth in porous hydroxyapatite bone graft substitutes. J. Biomed. Mater. Res. A 2004, 68A, 187–200. [Google Scholar] [CrossRef]
- Vuola, J.; Taurio, R.; Goransson, H.; Asko-Seljavaara, S. Compressive strength of calcium carbonate and hydroxyapatite implants after bone marrow induced osteogenesis. Biomaterials 1998, 19, 223–227. [Google Scholar] [CrossRef]
- Yang, L.; Ning, X.; Chen, K.; Zhou, H. Preparation and properties of hydroxyapatite filters for microbial filtration. Ceram. Int. 2007, 33, 483–489. [Google Scholar] [CrossRef]
- Levitt, G.E.; Crayton, P.H.; Monroe, E.A.; Condrate, R.A. Forming methods for apatite prosthesis. J. Biomed. Mater. Res. 1969, 3, 683–685. [Google Scholar] [CrossRef]
- Tadic, D.; Epple, M. A thorough physicochemical characterization of 14 calcium phosphate-based bone substitution materials in comparison to natural bone. Biomaterials 2004, 25, 987–994. [Google Scholar] [CrossRef]
- Bodde, E.W.H.; Wolke, J.G.C.; Kowalski, R.S.Z.; Jansen, J.A. Bone regeneration of porous β-tricalcium phosphate (Conduit™ TCP) and of biphasic calcium phosphate ceramic (Biosel®) in trabecular defects in sheep. J. Biomed. Mater. Res. A 2007, 82A, 711–722. [Google Scholar] [CrossRef]
- le Guéhennec, L.; Layrolle, P.; Daculsi, G. A review of bioceramics and fibrin sealant. Eur. Cell Mater. 2004, 8, 1–11. [Google Scholar]
- LeGeros, R.Z. Properties of osteoconductive biomaterials: Calcium phosphates. Clin. Orthop. Rel. Res. 2002, 395, 81–98. [Google Scholar] [CrossRef]
- Jordan, D.R.; Gilberg, S.; Bawazeer, A. Coralline hydroxyapatite orbital implant (Bio-Eye): Experience with 158 patients. Ophthal. Plast. Reconstr. Surg. 2004, 20, 69–74. [Google Scholar] [CrossRef]
- Yoon, J.S.; Lew, H.; Kim, S.J.; Lee, S.Y. Exposure rate of hydroxyapatite orbital implants a 15-year experience of 802 cases. Ophthalmology 2008, 115, 566–572. [Google Scholar] [CrossRef]
- Schnettler, R.; Stahl, J.P.; Alt, V.; Pavlidis, T.; Dingeldein, E.; Wenisch, S. Calcium phosphate-based bone substitutes. Eur. J. Trauma 2004, 4, 219–229. [Google Scholar]
- Zyman, Z.Z.; Glushko, V.; Dedukh, N.; Malyshkina, S.; Ashukina, N. Porous calcium phosphate ceramic granules and their behaviour in differently loaded areas of skeleton. J. Mater. Sci. Mater. Med. 2008, 19, 2197–2205. [Google Scholar] [CrossRef]
- Constantz, B.R.; Ison, I.C.; Fulmer, M.T.; Poser, R.D.; Smith, S.T.; Vanwagoner, M.; Ross, J.; Goldstein, S.A.; Jupiter, J.B.; Rosenthal, D.I. Skeletal repair by in situ formation of the mineral phase of bone. Science 1995, 267, 1796–1799. [Google Scholar]
- Dorozhkin, S.V. Calcium orthophosphate cements for biomedical application. J. Mater. Sci. 2008, 43, 3028–3057. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphate cements and concretes. Materials 2009, 2, 221–291. [Google Scholar] [CrossRef]
- Chow, L.C. Next generation calcium phosphate-based biomaterials. Dent. Mater. J. 2009, 28, 1–10. [Google Scholar] [CrossRef]
- Del Real, R.P.; Wolke, J.G.C.; Vallet-Regí, M.; Jansen, J.A. A new method to produce macropores in calcium phosphate cements. Biomaterials 2002, 23, 3673–3680. [Google Scholar] [CrossRef]
- Victor, S.P.; Kumar, T.S.S. Processing and properties of injectable porous apatitic cements. J. Ceram. Soc. Jpn. 2008, 116, 105–107. [Google Scholar] [CrossRef]
- Hesaraki, S.; Nemati, R.; Nosoudi, N. Preparation and characterisation of porous calcium phosphate bone cement as antibiotic carrier. Adv. Appl. Ceram. 2009, 108, 231–240. [Google Scholar] [CrossRef]
- Weiss, D.D.; Sachs, M.A.; Woodard, C.R. Calcium phosphate bone cements: A comprehensive review. J. Long Term Eff. Med. Implants 2003, 13, 41–47. [Google Scholar] [CrossRef]
- Ambard, A.J.; Mueninghoff, L. Calcium phosphate cement: Review of mechanical and biological properties. J. Prosthodont. 2006, 15, 321–328. [Google Scholar] [CrossRef]
- Costantino, P.D.; Friedman, C.D.; Jones, K.; Chow, L.C.; Pelzer, H.J.; Sisson, G.A. Hydroxyapatite cement. I—Basic chemistry and histologic properties. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 379–384. [Google Scholar] [CrossRef]
- Costantino, P.D.; Friedman, C.D.; Jones, K.; Chow, L.C.; Pelzer, H.J.; Sisson, G.A. Hydroxyapatite cement. II—Obliteration and reconstruction of the cat frontal sinus. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 385–389. [Google Scholar] [CrossRef]
- De Groot, K.; Wolke, J.G.C.; Jansen, J.A. Calcium phosphate coatings for medical implants. Proc. Inst. Mech. Eng. Part H: J. Eng. Med. 1998, 212, 137–147. [Google Scholar] [CrossRef]
- Campbell, A.A. Bioceramics for implant coatings. Mater. Today 2003, 6, 26–30. [Google Scholar] [CrossRef]
- Epinette, J.A.M.D.; Geesink, R.G.T. Hydroxyapatite Coated Hip and Knee Arthroplasty; Elsevier: Amsterdam, The Netherlands, 1995; p. 394. [Google Scholar]
- Willmann, G. Coating of implants with hydroxyapatite—Material connections between bone and metal. Adv. Eng. Mater. 1999, 1, 95–105. [Google Scholar] [CrossRef]
- Schliephake, H.; Scharnweber, D.; Roesseler, S.; Dard, M.; Sewing, A.; Aref, A. Biomimetic calcium phosphate composite coating of dental implants. Int. J. Oral Max. Impl. 2006, 21, 738–746. [Google Scholar]
- Kokubo, T.; Kim, H.M.; Kawashita, M. Novel bioactive materials with different mechanical properties. Biomaterials 2003, 24, 2161–2175. [Google Scholar] [CrossRef]
- Habibovic, P.; Li, J.; Van der Valk, C. M.; Meijer, G.; Layrolle, P.; Van Blitterswijk, C.A.; De Groot, K. Biological performance of uncoated and octacalcium phosphate-coated Ti6Al4V. Biomaterials 2005, 26, 23–36. [Google Scholar] [CrossRef]
- Hahn, B.D.; Park, D.S.; Choi, J.J.; Ryu, J.; Yoon, W.H.; Kim, K.H.; Park, C.; Kim, H.E. Dense nanostructured hydroxyapatite coating on titanium by aerosol deposition. J. Am. Ceram. Soc. 2009, 92, 683–687. [Google Scholar] [CrossRef]
- Gineste, L.; Gineste, M.; Ranz, X.; Ellefterion, A.; Guilhem, A.; Rouquet, N.; Frayssinet, P. Degradation of hydroxylapatite, fluorapatite, and fluorhydroxyapatite coatings of dental implants in dogs. J. Biomed. Mater. Res. 1999, 48, 224–234. [Google Scholar] [CrossRef]
- Okada, M.; Furuzono, T. Hydroxyapatite nanocrystal coating on biodegradable microspheres. Mater. Sci. Eng. B 2010, 173, 199–203. [Google Scholar] [CrossRef]
- Habibovic, P.; Barrère, F.; Van Blitterswijk, C.A.; De Groot, K.; Layrolle, P. Biomimetic hydroxyapatite coating on metal implants. J. Am. Ceram. Soc. 2002, 85, 517–522. [Google Scholar]
- Sun, L.; Berndt, C.C.; Gross, K.A.; Kucuk, A. Review: Material fundamentals and clinical performance of plasma sprayed hydroxyapatite coatings. J. Biomed. Mater. Res. Appl. Biomater. 2001, 58, 570–592. [Google Scholar] [CrossRef]
- Yang, Y.; Kim, K.H.; Ong, J.L. A review on calcium phosphate coatings produced using a sputtering process—An alternative to plasma spraying. Biomaterials 2005, 26, 327–337. [Google Scholar] [CrossRef]
- Oliveira, A.L.; Mano, J.F.; Reis, R.L. Nature-inspired calcium phosphate coatings: Present status and novel advances in the science of mimicry. Curr. Opin. Solid State Mater. Sci. 2003, 7, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Manso, M.; Jiménez, C.; Morant, C.; Herrero, P.; Martínez-Duart, J. Electrodeposition of hydroxyapatite coatings in basic conditions. Biomaterials 2000, 21, 1755–1761. [Google Scholar] [CrossRef]
- Kuo, M.C.; Yen, S.K. The process of electrochemical deposited hydroxyapatite coatings on biomedical titanium at room temperature. Mater. Sci. Eng. C 2002, 20, 153–160. [Google Scholar] [CrossRef]
- Eliaz, N.; Sridhar, T.M.; Mudali, U.K.; Raj, B. Electrochemical and electrophoretic deposition of hydroxyapatite for orthopaedic applications. Surf. Eng. 2005, 21, 238–242. [Google Scholar] [CrossRef]
- Ma, M.; Ye, W.; Wang, X.X. Effect of supersaturation on the morphology of hydroxyapatite crystals deposited by electrochemical deposition on titanium. Mater. Lett. 2008, 62, 3875–3877. [Google Scholar] [CrossRef]
- Ong, J.L.; Appleford, M.; Oh, S.; Yang, Y.; Chen, W.H.; Bumgardner, J.D.; Haggard, W.O. The characterization and development of bioactive hydroxyapatite coatings. JOM 2006, 58, 67–69. [Google Scholar]
- Qu, H.; Wei, M. The effect of temperature and initial pH on biomimetic apatite coating. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 87B, 204–212. [Google Scholar] [CrossRef]
- Esfehanian, M.; Raissi-Dehkordi, B.; Moztarzadeh, F. Electrophoretic deposition of hydroxyapatite on metal implants. Inter. Ceram. 2005, 54, 92–98. [Google Scholar]
- Narayanan, R.; Seshadri, S.K.; Kwon, T.Y.; Kim, K.H. Calcium phosphate-based coatings on titanium and its alloys. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 85B, 279–299. [Google Scholar] [CrossRef]
- Sugino, A.; Tsuru, K.; Hayakawa, S.; Kikuta, K.; Kawachi, G.; Osaka, A.; Ohtsuki, C. Induced deposition of bone-like hydroxyapatite on thermally oxidized titanium substrates using a spatial gap in a solution that mimics a body fluid. J. Ceram. Soc. Jpn. 2009, 117, 515–520. [Google Scholar] [CrossRef]
- Ye, G.; Troczynski, T. Hydroxyapatite coatings by pulsed ultrasonic spray pyrolysis. Ceram. Int. 2008, 34, 511–516. [Google Scholar] [CrossRef]
- Zheng, M.; Fan, D.; Li, X.K.; Zhang, J.B.; Liu, Q.B. Microstructure and in vitro bioactivity of laser-cladded bioceramic coating on titanium alloy in a simulated body fluid. J. Alloys Compd. 2010, 489, 211–214. [Google Scholar] [CrossRef]
- Geesink, R.G.T. Osteoconductive coating for total joint arthroplasty. Clin. Orthop. Rel. Res. 2002, 395, 53–65. [Google Scholar] [CrossRef]
- Mukherjee, D.P.; Dorairaj, N.R.; Mills, D.K.; Graham, D.; Krauser, J.T. Fatigue properties of hydroxyapatite-coated dental implants after exposure to a periodontal pathogen. J. Biomed. Mater. Res. 2000, 53, 467–474. [Google Scholar] [CrossRef]
- Gledhill, H.C.; Turner, I.G.; Doyle, C. In vitro fatigue behaviour of vacuum plasma and detonation gun sprayed hydroxyapatite coatings. Biomaterials 2001, 22, 1233–1240. [Google Scholar] [CrossRef]
- Cheng, K.; Ren, C.; Weng, W.; Du, P.; Shen, G.; Han, G.; Zhang, S. Bonding strength of fluoridated hydroxyapatite coatings: A comparative study on pull-out and scratch analysis. Thin Solid Films 2009, 517, 5361–5364. [Google Scholar] [CrossRef]
- De Groot, K.; Geesink, R.G.T.; Klein, C.P.A.T.; Serekian, P. Plasma sprayed coatings of hydroxylapatite. J. Biomed. Mater. Res. 1987, 21, 1375–1381. [Google Scholar] [CrossRef]
- Furlong, R.J.; Osborn, J.F. Fixation of hip prostheses by hydroxyapatite ceramic coating. J. Bone Joint Surg. B 1991, 73, 741–745. [Google Scholar]
- Saithna, A. The influence of hydroxyapatite coating of external fixator pins on pin loosening and pin track infection: A systematic review. Injury 2010, 41, 128–132. [Google Scholar] [CrossRef]
- Chang, J.K.; Chen, C.H.; Huang, K.Y.; Wang, G.J. Eight-year results of hydroxyapatite-coated hip arthroplasty. J. Arthroplasty 2006, 21, 541–546. [Google Scholar] [CrossRef]
- Matsumine, A.; Myoui, A.; Kusuzaki, K.; Araki, N.; Seto, M.; Yoshikawa, H.; Uchida, A. Calcium hydroxyapatite ceramic implants in bone tumor surgery. A long-term follow-up study. J. Bone Joint Surg. B 2004, 86, 719–725. [Google Scholar]
- Shetty, A.A.; Slack, R.; Tindall, A.; James, K.D.; Rand, C. 1 Results of a hydroxyapatite-coated (Furlong) total hip replacement. A 13- to 15-year follow-up. J. Bone Joint Surg. B 2005, 87, 1050–1054. [Google Scholar]
- Buchanan, J.M. 16 year review of hydroxyapatite ceramic coated hip implants—A clinical and histological evaluation. Key Eng. Mater. 2005, 284-286, 1049–1052. [Google Scholar] [CrossRef]
- Buchanan, J.M. 17 year review of hydroxyapatite ceramic coated hip implants—A clinical and histological evaluation. Key Eng. Mater. 2006, 309-311, 1341–1344. [Google Scholar] [CrossRef]
- Buchanan, J.M.; Goodfellow, S. Nineteen years review of hydroxyapatite ceramic coated hip implants: A clinical and histological evaluation. Key Eng. Mater. 2008, 361-363, 1315–1318. [Google Scholar] [CrossRef]
- Rajaratnam, S.S.; Jack, C.; Tavakkolizadeh, A.; George, M.D.; Fletcher, R.J.; Hankins, M.; Shepperd, J.A.N. Long-term results of a hydroxyapatite-coated femoral component in total hip replacement: A 15- to 21-year follow-up study. J. Bone Joint Surg. B 2008, 90, 27–30. [Google Scholar] [CrossRef]
- Binahmed, A.; Stoykewych, A.; Hussain, A.; Love, B.; Pruthi, V. Long-term follow-up of hydroxyapatite-coated dental implants—A clinical trial. Int. J. Oral Max. Impl. 2007, 22, 963–968. [Google Scholar]
- Iezzi, G.; Scarano, A.; Petrone, G.; Piattelli, A. Two human hydroxyapatite-coated dental implants retrieved after a 14-year loading period: A histologic and histomorphometric case report. J. Periodontol. 2007, 78, 940–947. [Google Scholar] [CrossRef]
- Bauer, T.W.; Geesink, R.G.T.; Zimmerman, R.; McMahon, J.T. Hydroxyapatite-coated femoral stems. Histological analysis of components retrieved at autopsy. J. Bone Joint Surg. A 1991, 73, 1439–1452. [Google Scholar]
- Buma, P.; Gardeniers, J.W. Tissue reactions around a hydroxyapatite-coated hip prostheses: Case report of a retrieveal specimen. J. Arthroplasty 1995, 10, 389–395. [Google Scholar] [CrossRef]
- Capello, W.D.; D’Antonio, J.A.; Feinberg, J.R.; Manley, M.T. Hydroxyapatite-coated total hip femoral components in patients less than fifty years old. Clinical and radiographic results after five to eight years of follow-up. J. Bone Joint Surg. A 1997, 79, 1023–1029. [Google Scholar]
- Paital, S.R.; Dahotre, N.B. Calcium phosphate coatings for bio-implant applications: Materials, performance factors, and methodologie. Mater. Sci. Eng. R 2009, 66, 1–70. [Google Scholar] [CrossRef]
- Thin Calcium Phosphate Coatings for Medical Implants; León, B.; Jansen, J.A. (Eds.) Springer: Berlin, Germany, 2009; p. 326.
- To narrow the subject of this review, functionally graded bioceramics prepared from calcium orthophosphates with various dopants is not considered. The interested readers are advised to read the original papers [292,520,521]
- Manjubala, I.; Kumar, T.S.S. Effect of TiO2—Ag2O additives on the formation of calcium phosphate based functionally graded bioceramics. Biomaterials 2000, 21, 1995–2002. [Google Scholar] [CrossRef]
- Wei, T.; Ruys, A.; Milthorpe, B. Hydroxyapatite-zirconia functionally graded bioceramics prepared by hot isostatic pressing. Key Eng. Mater. 2003, 240-242, 591–594. [Google Scholar] [CrossRef]
- Kon, M.; Ishikawa, K.; Miyamoto, Y.; Asaoka, K. Development of calcium phosphate based functional gradient bioceramics. Biomaterials 1995, 16, 709–714. [Google Scholar] [CrossRef]
- Wong, L.H.; Tio, B.; Miao, X. Functionally graded tricalcium phosphate/fluoroapatite composites. Mater. Sci. Eng. C 2002, 20, 111–115. [Google Scholar] [CrossRef]
- Tampieri, A.; Celotti, G.; Sprio, S.; Delcogliano, A.; Franzese, S. Porosity-graded hydroxyapatite ceramics to replace natural bone. Biomaterials 2001, 22, 1365–1370. [Google Scholar] [CrossRef]
- Lu, W.W.; Zhao, F.; Luk, K.D.K.; Yin, Y.J.; Cheung, K.M.C.; Cheng, G.X.; Yao, K.D.; Leong, J.C.Y. Controllable porosity hydroxyapatite ceramics as spine cage: Fabrication and properties evaluation. J. Mater. Sci. Mater. Med. 2003, 14, 1039–1046. [Google Scholar] [CrossRef]
- Werner, J.; Linner-Krcmar, B.; Friess, W.; Greil, P. Mechanical properties and in vitro cell compatibility of hydroxyapatite ceramics with graded pore structure. Biomaterials 2002, 23, 4285–4294. [Google Scholar] [CrossRef]
- Kaito, T.; Mukai, Y.; Nishikawa, M.; Ando, W.; Yoshikawa, H.; Myoui, A. Dual hydroxyapatite composite with porous and solid parts: Experimental study using canine lumbar interbody fusion model. J. Biomed. Mater. Res. B 2006, 78B, 378–384. [Google Scholar] [CrossRef]
- Rodriguez-Lorenzo, L.M.; Ferreira, J.M.F. Development of porous ceramic bodies for applications in tissue engineering and drug delivery systems. Mater. Res. Bull. 2004, 39, 83–91. [Google Scholar] [CrossRef]
- Lu, W.W.; Zhao, F.; Luk, K.D.K.; Yin, Y.J.; Cheung, K.M.C.; Cheng, G.X.; Yao, K.D.; Leong, J.C.Y. Controllable porosity hydroxyapatite ceramics as spine cage: Fabrication and properties evaluation. J. Mater. Sci. Mater. Med. 2003, 14, 1039–1046. [Google Scholar] [CrossRef]
- Dubok, V.A. Bioceramics—Yesterday, today, tomorrow. Powder Metallurgy Metal Ceram. 2000, 39, 381–394. [Google Scholar] [CrossRef]
- Heness, G.; Ben-Nissan, B. Innovative bioceramics. Mater. Forum 2004, 27, 104–114. [Google Scholar]
- Ohtsuki, C.; Kamitakahara, M.; Miyazaki, T. Bioactive ceramic-based materials with designed reactivity for bone tissue regeneration. J. R. Soc. Interface 2009, 6, S349–S360. [Google Scholar] [CrossRef]
- The term “bioinert” should be used with care, since it is clear that any material introduced into the physiological environment will induce a response. However, for the purposes of biomedical implants, the term can be defined as a minimal level of response from the host tissue [4]
- Yuan, H.; Fernandes, H.; Habibovic, P.; De Boer, J.; Barradas, A.M.C.; De Ruiter, A.; Walsh, W.R.; Van Blitterswijk, C.A.; De Bruijn, J.D. Osteoinductive ceramics as a synthetic alternative to autologous bone grafting. Proc. Natl. Acad. Sci. USA 2010, 107, 13614–13619. [Google Scholar] [CrossRef]
- Greenspan, D.C. Bioactive ceramic implant materials. Curr. Opin. Solid State Mater. Sci. 1999, 4, 389–393. [Google Scholar] [CrossRef]
- Blokhuis, T.J.; Termaat, M.F.; Den Boer, F.C.; Patka, P.; Bakker, F.C.; Haarman, H.J.T.M. Properties of calcium phosphate ceramics in relation to their in vivo behavior. J. Trauma 2000, 48, 179–189. [Google Scholar] [CrossRef]
- Kim, H.M. Bioactive ceramics: Challenges and perspectives. J. Ceram. Soc. Jpn. 2001, 109, S49–S57. [Google Scholar] [CrossRef]
- Okuda, T.; Ioku, K.; Yonezawa, I.; Minagi, H.; Gonda, Y.; Kawachi, G.; Kamitakahara, M.; Shibata, Y.; Murayama, H.; Kurosawa, H.; Ikeda, T. The slow resorption with replacement by bone of a hydrothermally synthesized pure calcium-deficient hydroxyapatite. Biomaterials 2008, 29, 9–2728. [Google Scholar]
- Seeley, Z.; Bandyopadhyay, A.; Bose, S. Tricalcium phosphate based resorbable ceramics: Influence of NaF and CaO addition. Mater. Sci. Eng. C 2008, 28, 11–17. [Google Scholar] [CrossRef]
- Descamps, M.; Richart, O.; Hardouin, P.; Hornez, J.C.; Leriche , A. Synthesis of macroporous β-tricalcium phosphate with controlled porous architectural. Ceram. Int. 2008, 34, 1131–1137. [Google Scholar] [CrossRef]
- Cushnie, E.K.; Khan, Y.M.; Laurencin, C.T. Amorphous hydroxyapatite-sintered polymeric scaffolds for bone tissue regeneration: Physical characterization studies. J. Biomed. Mater. Res. A 2008, 84A, 54–62. [Google Scholar] [CrossRef]
- Hench, L.L. Challenges for bioceramics in the 21st century. Am. Ceram. Soc. Bull. 2005, 84, 18–21. [Google Scholar]
- Nagase, M.; Baker, D.G.; Schumacher, H.R. Prolonged inflammatory reactions induced by artificial ceramics in the rat pouch model. J. Rheumatol. 1988, 15, 1334–1338. [Google Scholar]
- Rooney, T.; Berman, S.; Indersano, A.T. Evaluation of porous block hydroxylapatite for augmentation of alveolar ridges. J. Oral Maxillof. Surg. 1988, 46, 15–18. [Google Scholar] [CrossRef]
- Prudhommeaux, F.; Schiltz, C.; Lioté, F.; Hina, A.; Champy, R.; Bucki, B.; Ortiz-Bravo, E.; Meunier, A.; Rey, C.; Bardin, T. Variation in the inflammatory properties of basic calcium phosphate crystals according to crystal type. Arthritis Rheum. 1996, 39, 1319–1326. [Google Scholar] [CrossRef]
- Uchida, A.; Araki, N.; Shinto, Y.; Yoshikawa, H.; Kurisaki, E.; Ono, K. The use of calcium hydroxyapatite ceramic in bone tumour surgery. J. Bone Joint Surg. B 1990, 72, 298–302. [Google Scholar]
- Osteogenesis is the process of laying down new bone material by osteoblasts
- Osteoinduction is the property of the material to induce bone formation de novo or ectopically (i.e., in non-bone forming sites). It happens due to a stimulation and activation of host mesenchymal stem cells from the surrounding tissues, which differentiate into bone-forming osteoblasts [549]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone substitutes: An update. Injury 2005, 36 Suppl. 1, S20–S27. [Google Scholar] [CrossRef]
- Osteoid is a bioorganic portion of the matrix of bone tissue. Osteoblasts begin the process of forming bone tissue by secreting the osteoid as several specific proteins. When the osteoid becomes mineralized, it and the adjacent bone cells have developed into new bone tissues
- Yamasaki, H.; Sakai, H. Osteogenic response to porous hydroxyapatite ceramics under the skin of dogs. Biomaterials 1992, 13, 308–312. [Google Scholar] [CrossRef]
- Klein, C.; De Groot, K.; Chen, W.; Li, Y.; Zhang, X. Osseous substance formation induced in porous calcium phosphate ceramics in soft tissues. Biomaterials 1994, 15, 31–34. [Google Scholar] [CrossRef]
- Yuan, H.; Yang, Z.; Li, Y.; Zhang, Z.; De Bruijn, J.D.; De Groot, K. Osteoinduction by calcium phosphate biomaterials. J. Mater. Sci. Mater. Med. 1998, 9, 723–726. [Google Scholar] [CrossRef]
- Ripamonti, U. Osteoinduction in porous hydroxyapatite implanted in heterotopic sites of different animal models. Biomaterials 1996, 17, 31–35. [Google Scholar] [CrossRef]
- Ripamonti, U.; Crooks, J.; Kirkbride, A.N. Sintered porous hydroxyapatites with intrinsic osteoinductive activity: Geometric induction of bone formation. S. Afr. J. Sci. 1999, 95, 335–343. [Google Scholar]
- Yuan, H.P.; De Bruijn, J.D.; Li, Y.B.; Feng, J.Q.; Yang, Z.J.; De Groot, K.; Zhang, X.D. Bone formation induced by calcium phosphate ceramics in soft tissue of dogs: A comparative study between porous α-TCP and β-TCP. J. Mater. Sci. Mater. Med. 2001, 12, 7–13. [Google Scholar] [CrossRef]
- Matsushita, N.; Terai, H.; Okada, T.; Nozaki, K.; Inoue, H.; Miyamoto, S.; Takaoka, K. A new bone-inducing biodegradable porous β-tricalcium phosphate. J. Biomed. Mater. Res. A 2004, 70A, 450–458. [Google Scholar] [CrossRef]
- Le Nihouannen, D.; Daculsi, G.; Saffarzadeh, A.; Gauthier, O.; Delplace, S.; Pilet, P.; Layrolle, P. Ectopic bone formation by microporous calcium phosphate ceramic particles in sheep muscles. Bone 2005, 36, 1086–1093. [Google Scholar] [CrossRef]
- Yuan, H.; Kurashina, K.; De Bruijn, D.J.; Li, Y.; De Groot, K.; Zhang, X. A preliminary study of osteoinduction of two kinds of calcium phosphate bioceramics. Biomaterials 1999, 20, 1799–1806. [Google Scholar] [CrossRef]
- Gosain, A.K.; Song, L.; Riordan, P.; Amarante, M.T.; Nagy, P.G.; Wilson, C.R.; Toth, J.M.; Ricci, J.L. A 1-year study of osteoinduction in hydroxyapatite-derived biomaterials in an adult sheep model: Part I. Plast. Reconstr. Surg. 2002, 109, 619–630. [Google Scholar] [CrossRef]
- Cheng, L.; Ye, F.; Yang, R.; Lu, X.; Shi, Y.; Li, L.; Fan, H.; Bu, H. Osteoinduction of hydroxyapatite/β-tricalcium phosphate bioceramics in mice with a fractured fibula. Acta Biomater. 2010, 6, 1569–1574. [Google Scholar]
- Barrere, F.; Van der Valk, C.M.; Dalmeijer, R.A.; Meijer, G.; Van Blitterswijk, C.A.; De Groot, K.; Layrolle, P. Osteogenecity of octacalcium phosphate coatings applied on porous titanium. J. Biomed. Mater. Res. A 2003, 66A, 779–788. [Google Scholar] [CrossRef]
- Habibovic, P.; Van der Valk, C.M.; Van Blitterswijk, C.A.; De Groot, K.; Meijer, G. Influence of octacalcium phosphate coating on osteoinductive properties of biomaterials. J. Mater. Sci. Mater. Med. 2004, 15, 373–380. [Google Scholar]
- Habibovic, P.; Yuan, H.; Van der Valk, C.M.; Meijer, G.; Van Blitterswijk, C.A.; De Groot, K. 3D microenvironment as essential element for osteoinduction by biomaterials. Biomaterials 2005, 26, 3565–3575. [Google Scholar] [CrossRef]
- Habibovic, P.; Sees, T.M.; Van den Doel, M.A.; Van Blitterswijk, C.A.; De Groot, K. Osteoinduction by biomaterials—physicochemical and structural influences. J. Biomed. Mater. Res. A 2006, 77A, 747–762. [Google Scholar] [CrossRef]
- Reddi, A.H. Morphogenesis and tissue engineering of bone and cartilage: Inductive signals, stem cells and biomimetic biomaterials. Tissue Eng. 2000, 6, 351–359. [Google Scholar] [CrossRef]
- Ripamonti, U. The morphogenesis of bone in replicas of porous hydroxyapatite obtained by conversion of calcium carbonate exoskeletons of coral. J. Bone Joint Surg. A 1991, 73, 692–703. [Google Scholar]
- Kuboki, Y.; Takita, H.; Kobayashi, D. BMP-induced osteogenesis on the surface of hydroxyapatite with geometrically feasible and nonfeasible structures: Topology of osteogenesis. J. Biomed. Mater. Res. 1998, 39, 190–199. [Google Scholar] [CrossRef]
- Diaz-Flores, L.; Gutierrez, R.; Lopez-Alonso, A.; Gonzalez, R.; Varela, H. Pericytes as a supplementary source of osteoblasts in periosteal osteogenesis. Clin. Orthop. Relat. Res. 1992, 275, 280–286. [Google Scholar]
- Dorozhkin, S.V. Inorganic chemistry of the dissolution phenomenon, the dissolution mechanism of calcium apatites at the atomic (ionic) level. Comment Inorg. Chem. 1999, 20, 285–299. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. A review on the dissolution models of calcium apatites. Prog. Cryst. Growth Charact. 2002, 44, 45–61. [Google Scholar] [CrossRef]
- Teitelbaum, S.L. Bone resorption by osteoclasts. Science 2000, 289, 1504–1508. [Google Scholar] [CrossRef]
- Okuda, T.; Ioku, K.; Yonezawa, I.; Minagi, H.; Kawachi, G.; Gonda, Y.; Murayama, H.; Shibata, Y.; Minami, S.; Kamihara, S.; Kurosawa, H.; Ikeda, T. The effect of the microstructure of β-tricalcium phosphate on the metabolism of subsequently formed bone tissue. Biomaterials 2007, 28, 2–2621. [Google Scholar]
- Orly, I.; Gregoire, M.; Menanteau, J.; Heughebaert, M.; Kerebel, B. Chemical changes in hydroxyapatite biomaterial under in vivo and in vitro biological conditions. Calcif. Tissue Int. 1989, 45, 20–26. [Google Scholar] [CrossRef]
- Bertazzo, S.; Zambuzzi, W.F.; Campos, D.D.P.; Ogeda, T.L.; Ferreira, C.V.; Bertran, C.A. Hydroxyapatite surface solubility and effect on cell adhesion. Colloids Surf. B Biointerfaces 2010, 78, 177–184. [Google Scholar] [CrossRef]
- Schwartz, Z.; Boyan, B.D. Underlying mechanisms at the bone-biomaterial interface. J. Cell. Biochem. 1994, 56, 340–347. [Google Scholar] [CrossRef]
- Puleo, D.A.; Nanci, A. Understanding and controlling the bone-implant interface. Biomaterials 1999, 20, 2311–2321. [Google Scholar] [CrossRef]
- Xin, R.; Leng, Y.; Chen, J.; Zhang, Q. A comparative study of calcium phosphate formation on bioceramics in vitro and in vivo. Biomaterials 2005, 26, 6477–6486. [Google Scholar] [CrossRef]
- Girija, E.K.; Parthiban, S.P.; Suganthi, R.V.; Elayaraja, K.; Joshy, M.I.A.; Vani, R.; Kularia, P.; Asokan, K.; Kanjilal, D.; Yokogawa, Y.; Narayana Kalkura, S. High energy irradiation—A tool for enhancing the bioactivity of hydroxyapatite. J. Ceram. Soc. Jpn. 2008, 116, 320–324. [Google Scholar] [CrossRef]
- Okada, M.; Furukawa, K.; Serizawa, T.; Yanagisawa, Y.; Tanaka, H.; Kawai, T.; Furuzono, T. Interfacial interactions between calcined hydroxyapatite nanocrystals and substrates. Langmuir 2009, 25, 6300–6306. [Google Scholar]
- Malik, M.A.; Puleo, D.A.; Bizios, R.; Doremus, R.H. Osteoblasts on hydroxyapatite, alumina and bone surfaces in vitro: Morphology during the first 2 h of attachment. Biomaterials 1992, 13, 123–128. [Google Scholar] [CrossRef]
- Norman, M.E.; Elgendy, H.M.; Shors, E.C.; El-Amin, S.F.; Laurencin, C.T. An in-vitro evaluation of coralline porous hydroxyapatite as a scaffold for osteoblast growth. Clin. Mater. 1994, 17, 85–91. [Google Scholar] [CrossRef]
- Shu, R.; McMullen, R.; Baumann, M.J.; McCabe, L.R. Hydroxyapatite accelerates differentiation and suppresses growth of MC3T3-E1 osteoblasts. J. Biomed. Mater. Res. A 2003, 67A, 1196–1204. [Google Scholar] [CrossRef]
- Gomi, K.; Lowenberg, B.; Shapiro, G.; Davies, J.E. Resorption of sintered synthetic hydroxyapatite by osteoclasts in vitro. Biomaterials 1992, 20, 91–96. [Google Scholar]
- Suzuki, T.; Ohashi, R.; Yokogawa, Y.; Nishizawa, K.; Nagata, F.; Kawamoto, Y.; Kameyama, T.; Toriyama, M. Initial anchoring and proliferation of fibroblast L-929 cells on unstable surface of calcium phosphate ceramics. J. Biosci. Bioeng. 1999, 87, 320–327. [Google Scholar] [CrossRef]
- Arinzeh, T.L.; Tran, T.; McAlary, J.; Daculsi, G. A comparative study of biphasic calcium phosphate ceramics for human mesenchymal stem-cell-induced bone formation. Biomaterials 2005, 26, 3631–3638. [Google Scholar] [CrossRef]
- Oh, S.; Oh, N.; Appleford, M.; Ong, J.L. Bioceramics for tissue engineering applications—A review. Am. J. Biochem. Biotechnol. 2006, 2, 49–56. [Google Scholar] [CrossRef]
- Appleford, M.; Oh, S.; Cole, J.A.; Carnes, D.L.; Lee, M.; Bumgardner, J.D.; Haggard, W.O.; Ong, J.L. Effects of trabecular calcium phosphate scaffolds on stress signaling in osteoblast precursor cells. Biomaterials 2007, 28, 2747–2753. [Google Scholar] [CrossRef]
- Ohgushi, H.; Caplan, A.I. Stem cell technology and bioceramics: From cell to gene engineering. J. Biomed. Mater. Res. 1999, 48, 913–927. [Google Scholar] [CrossRef]
- Okumura, M.; Ohgushi, H.; Tamai, S. Bonding osteogenesis in coralline hydroxyapatite combined with bone marrow cells. Biomaterials 1990, 12, 28–37. [Google Scholar]
- Unger, R.E.; Sartoris, A.; Peters, K.; Motta, A.; Migliaresi, C.; Kunkel, M.; Bulnheim, U.; Rychly, J.; Kirkpatrick, C.J. Tissue-like self-assembly in cocultures of endothelial cells and osteoblasts and the formation of microcapillary like structures on three-dimensional porous biomaterials. materials 2007, 28, 3965–3976. [Google Scholar]
- Saiz, E.; Gremillard, L.; Menendez, G.; Miranda, P.; Gryn, K.; Tomsia, A.P. Preparation of porous hydroxyapatite scaffolds. Mater. Sci. Eng. C 2007, 27, 546–550. [Google Scholar] [CrossRef]
- Tamai, N.; Myoui, A.; Hirao, M.; Kaito, T.; Ochi, T.; Tanaka, J.; Takaoka, K.; Yoshikawa, H. A new biotechnology for articular cartilage repair: Subchondral implantation of a composite of interconnected porous hydroxyapatite, synthetic polymer (PLAPEG), and bone morphogenetic protein-2 (rhBMP-2). Osteoarthritis Cartilage 2005, 13, 405–417. [Google Scholar] [CrossRef]
- Bignon, A.; Chouteau, J.; Chevalier, J.; Fantozzi, G.; Carret, J.P.; Chavassieux, P.; Boivin, G.; Melin, M.; Hartmann, D. Effect of micro- and macroporosity of bone substitutes on their mechanical properties and cellular response. J. Mater. Sci. Mater. Med. 2003, 14, 1089–1097. [Google Scholar] [CrossRef]
- Griffith, L.G.; Naughton, G. Tissue engineering—Current challenges and expanding opportunities. Science 2002, 295, 1009–1014. [Google Scholar] [CrossRef]
- Tissue Engineering; Van Blitterswijk, C.A.; Thomsen, P.; Hubbell, J.; Cancedda, R.; De Bruijn, J.D.; Lindahl, A.; Sohier, J.; Williams, D.F. (Eds.) Academic Press: Burlington, MA, USA, 2008; p. 760.
- Repair is usually a rapid occurrence that is required for the survival of the individual but is not necessary for its optimal function. It usually results in a dense connective tissue scar that fills the space; however, it may not be responsive to the highly loaded mechanical environment required of culoskeletal tissue. Regeneration is a slow process that is usually characterized by the recapitulation of aspects of embryonic development [598]
- Goldberg, V.M.; Caplan, A.I. Orthopedic Tissue Engineering Basic Science and Practice; Marcel Dekker: New York, NY, USA, 2004; p. 338. [Google Scholar]
- In 2003, the NSF published a report titled: “The emergence of tissue engineering as a research field”, which provides a thorough description of the history of this field. Available online: http://www.nsf.gov/pubs/2004/nsf0450/start.htm (accessed on October 2010).
- Ikada, Y. Challenges in tissue engineering. J. R. Soc. Interface 2006, 3, 589–601. [Google Scholar] [CrossRef]
- Cima, L.G.; Langer, R. Engineering human tissue. Chem. Eng. Prog. 1993, 89, 46–54. [Google Scholar]
- Langer, R.; Vacanti, J.P. Tissue engineering. Science 1993, 260, 920–926. [Google Scholar]
- El-Ghannam, A. Bone reconstruction: From bioceramics to tissue engineering. Expert Rev. Med. Dev. 2005, 2, 87–101. [Google Scholar] [CrossRef]
- In general, a scaffold is a temporary structure used to support people and material in the construction or repair of buildings and other large structures. It is usually a modular system of metal pipes (termed tubes in Britain), although it can be made out of other materials
- Yang, S.; Leong, K.F.; Du, Z.; Chua, C.K. The design of scaffolds for use in tissue engineering. Part I—Traditional factors. Tissue Eng. 2001, 7, 679–689. [Google Scholar] [CrossRef]
- Hutmacher, D.W. Scaffolds in tissue engineering bone and cartilage. Biomaterials 2000, 21, 2529–2543. [Google Scholar] [CrossRef]
- Ma, P.X. Scaffolds for tissue fabrication. Mater. Today 2004, 7, 30–40. [Google Scholar]
- Yasuhiko, T. Biomaterial Technology for tissue engineering applications. J. R. Soc. Interface 2009, 6, S311–S324. [Google Scholar] [CrossRef]
- Scaffolding in Tissue Engineering; Ma, P.X.; Elisseeff, J. (Eds.) CRC Press: Boca Raton, FL, USA, 2006; p. 638.
- Schieker, M.; Seitz, H.; Drosse, I.; Seitz, S.; Mutschler, W. Biomaterials as scaffold for bone tissue engineering. Eur. J. Trauma 2006, 32, 114–124. [Google Scholar] [CrossRef]
- Okumura, M.; Ohgushi, H.; Dohi, Y.; Katuda, T.; Tamai, S.; Koerten, H.K.; Tabata, S. Osteoblastic phenotype expression on the surface of hydroxyapatite ceramics. J. Biomed. Mater. Res. 1997, 37, 122–129. [Google Scholar] [CrossRef]
- Service, R.F. Tissue engineers build new bone. Science 2000, 289, 1498–1500. [Google Scholar] [CrossRef]
- Fini, M.; Giardino, R.; Borsari, V.; Torricelli, P.; Rimondini, L.; Giavaresi, G.; Aldini, N.N. In vitro behaviour of osteoblasts cultured on orthopaedic biomaterials with different surface roughness, uncoated and fluorohydroxyapatite-coated, relative to the in vivo osteointegration rate. Int. J. Artif. ans 2003, 26, 520–528. [Google Scholar]
- Sato, M.; Webster, T.J. Designing orthopedic implant surfaces: Harmonization of nanotopographical and chemical aspects. Nanomedicine 2006, 1, 351–354. [Google Scholar] [CrossRef]
- Annaz, B.; Hing, K.A.; Kayser, M.; Buckland, T.; Di Silvio, L. Porosity in phase-pure hydroxyapatite. J. Microscopy 2004, 216, 97–109. [Google Scholar] [CrossRef]
- Li, S.; De Wijn, J.R.; Li, J.; Layrolle, P.; De Groot, K. Macroporous biphasic calcium phosphate scaffold with high permeability/porosity ratio. Tissue Eng. 2003, 9, 535–548. [Google Scholar] [CrossRef]
- Ebaretonbofa, E.; Evans, J.R. High porosity hydroxyapatite foam scaffolds for bone substitute. J. Porous Mater. 2002, 9, 257–263. [Google Scholar] [CrossRef]
- Specchia, N.; Pagnotta, A.; Cappella, M.; Tampieri, A.; Greco, F. Effect of hydroxyapatite porosity on growth and differentiation of human osteoblast-like cells. J. Mater. Sci. 2002, 37, 577–584. [Google Scholar] [CrossRef]
- Malmström, J.; Adolfsson, E.; Arvidsson, A.; Thomsen, P. Bone response inside free-form fabricated macroporous hydroxyapatite scaffolds with and without an open microporosity. Clin. Implant Dentistry Rel. Res. 2007, 9, 79–88. [Google Scholar] [CrossRef]
- Teixeira, C.C.; Nemelivsky, Y.; Karkia, C.; LeGeros, R.Z. Biphasic calcium phosphate: A scaffold for growth plate chondrocyte maturation. Tissue Eng. 2006, 12, 2283–2289. [Google Scholar] [CrossRef]
- Teixeira, S.; Oliveira, S.; Ferraz, M.P.; Monteiro, F.J. Three dimensional macroporous calcium phosphate scaffolds for bone tissue engineering. Key Eng. Mater. 2008, 361-363, 947–950. [Google Scholar] [CrossRef]
- Stevens, M.M. Biomaterials for bone tissue engineering. Mater. Today 2008, 11, 18–25. [Google Scholar] [CrossRef]
- Artzi, Z.; Weinreb, M.; Givol, N.; Rohrer, M.D.; Nemcovsky, C.E.; Prasad, H.S.; Tal, H. Biomaterial resorbability and healing site morphology of inorganic bovine bone and beta tricalcium phosphate in the canine: A 24-month longitudinal histologic study and morphometric analysis. Int. J. Oral. Impl. 2004, 19, 357–368. [Google Scholar]
- Burg, K.J.L.; Porter, S.; Kellam, J.F. Biomaterial developments for bone tissue engineering. Biomaterials 2000, 21, 2347–2359. [Google Scholar] [CrossRef]
- Ajaal, T.T.; Smith, R.W. Employing the Taguchi method in optimizing the scaffold production process for artificial bone grafts. J. Mater. Proc. Technol. 2009, 209, 1521–1532. [Google Scholar] [CrossRef]
- Boyde, A.; Corsi, A.; Quarto, R.; Cancedda, R.; Bianco, P. Osteoconduction in large macroporous hydroxyapatite ceramic implants: Evidence for a complementary integration and disintegration mechanism. Bone 1999, 24, 579–589. [Google Scholar] [CrossRef]
- Hing, K.A. Bioceramic bone graft substitutes: Influence of porosity and chemistry. Int. J. Appl. Ceram. Technol. 2005, 2, 184–199. [Google Scholar] [CrossRef]
- Peppas, N.A.; Langer, R. New challenges in biomaterials. Science 1994, 263, 1715–1720. [Google Scholar]
- Hench, L.L. Biomaterials: A forecast for the future. Biomaterials 1998, 19, 1419–1423. [Google Scholar] [CrossRef]
- Barrère, F.; Mahmood, T.A.; De Groot, K.; Van Blitterswijk, C.A. Advanced biomaterials for skeletal tissue regeneration: Instructive and smart functions. Mater. Sci. Eng. R 2008, 59, 38–71. [Google Scholar] [CrossRef]
- Dellinger, J.G.; Eurell, J.A.C.; Jamison, R.D. Bone response to 3D periodic hydroxyapatite scaffolds with and without tailored microporosity to deliver bone morphogenetic protein 2. J. Biomed. Mater. Res. A 2006, 76A, 366–376. [Google Scholar] [CrossRef]
- Pal, K.; Pal, S. Development of porous hydroxyapatite scaffolds. Mater. Manuf. Proc. 2006, 21, 325–328. [Google Scholar] [CrossRef]
- Bae, C.J.; Kim, H.W.; Koh, Y.H.; Kim, H.E. Hydroxyapatite (HA) bone scaffolds with controlled macrochannel pores. J. Mater. Sci. Mater. Med. 2006, 17, 517–521. [Google Scholar] [CrossRef]
- Guo, H.; Wei, J.; Kong, H.; Liu, C.; Pan, K. Biocompatibility and osteogenesis of calcium phosphate cement scaffolds for bone tissue engineering. Adv. Mater. Res. 2008, 47-50, 1383–1386. [Google Scholar] [CrossRef]
- Guo, H.; Su, J.; Wei, J.; Kong, H.; Liu, C. Biocompatibility and osteogenicity of degradable Ca-deficient hydroxyapatite scaffolds from calcium phosphate cement for bone tissue engineering. Acta Biomater. 2009, 5, 268–278. [Google Scholar] [CrossRef]
- Liu, H.; Webster, T.J. Nanomedicine for implants: A review of studies and necessary experimental tools. Biomaterials 2007, 28, 354–369. [Google Scholar] [CrossRef]
- Wang, C.; Duan, Y.; Markovic, B.; Barbara, J.; Howlett, C.R.; Zhang, X.; Zreiqat, H. Proliferation and bone-related gene expression of osteoblasts grown on hydroxyapatite ceramics sintered at different temperature. Biomaterials 2004, 25, 2949–2956. [Google Scholar] [CrossRef]
- Matsumoto, T.; Okazaki, M.; Nakahira, A.; Sasaki, J.; Egusa, H.; Sohmura, T. Modification of apatite materials for bone tissue engineering and drug delivery carriers. Curr. Med. Chem. 2007, 14, 2726–2733. [Google Scholar] [CrossRef]
- Traykova, T.; Aparicio, C.; Ginebra, M.P.; Planell, J.A. Bioceramics as nanomaterials. Nanomedicine 2006, 1, 91–106. [Google Scholar] [CrossRef]
- Kalita, S.J.; Bhardwaj, A.; Bhatt, H.A. Nanocrystalline calcium phosphate ceramics in biomedical engineering. Mater. Sci. Eng. C 2007, 27, 441–449. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Nano-sized and nanocrystalline calcium orthophosphates in biomedical engineering. J. Biomimetics Biomaterials Tissue Eng. 2009, 3, 59–92. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Nanodimensional and nanocrystalline apatites and other calcium orthophosphates in biomedical engineering, biology and medicine. Materials 2009, 2, 1975–2045. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Nanosized and nanocrystalline calcium orthophosphates. Acta Biomater. 2010, 6, 715–734. [Google Scholar] [CrossRef]
- Aizawa, M.; Porter, A.E.; Best, S.M.; Bonfield, W. Ultrastructural observation of single-crystal apatite fibres. Biomaterials 2005, 26, 3427–3433. [Google Scholar] [CrossRef]
- Park, Y.M.; Ryu, S.C.; Yoon, S.Y.; Stevens, R.; Park, H.C. Preparation of whisker-shaped hydroxyapatite/β-tricalcium phosphate composite. Mater. Chem. Phys. 2008, 109, 440–447. [Google Scholar] [CrossRef]
- Morisue, H.; Matsumoto, M.; Chiba, K.; Matsumoto, H.; Toyama, Y.; Aizawa, M.; Kanzawa, N.; Fujimi, T.J.; Uchida, H.; Okada, I. A novel hydroxyapatite fiber mesh as a carrier for recombinant human bone morphogenetic protein-2 enhances bone union in rat posterolateral fusion model. Spine 2006, 31, 1194–1200. [Google Scholar]
- Matsuda, A.; Ikoma, T.; Kobayashi, H.; Tanaka, J. Preparation and mechanical property of core-shell type chitosan/calcium phosphate composite fiber. Mater. Sci. Eng. C 2004, 24, 723–728. [Google Scholar] [CrossRef]
- Tas, A.C. Molten salt synthesis of calcium hydroxyapatite whiskers. J. Am. Ceram. Soc. 2001, 84, 295–300. [Google Scholar] [CrossRef]
- Aizawa, M.; Ueno, H.; Itatani, K.; Okada, I. Syntheses of calcium-deficient apatite fibres by a homogeneous precipitation method and their characterizations. J. Eur. Ceram. Soc. 2006, 26, 501–507. [Google Scholar] [CrossRef]
- Wu, Y.; Hench, L.L.; Du, J.; Choy, K.L.; Guo, J. Preparation of hydroxyapatite fibers by electrospinning technique. J. Am. Ceram. Soc. 2004, 87, 1988–1991. [Google Scholar]
- Ramanan, S.R.; Venkatesh, R. A study of hydroxyapatite fibers prepared via sol-gel route. Mater. Lett. 2004, 58, 3320–3323. [Google Scholar] [CrossRef]
- Seo, D.S.; Lee, J.K. Synthesis of hydroxyapatite whiskers through dissolution-reprecipitation process using EDTA. J. Cryst. Growth 2008, 310, 2162–2167. [Google Scholar] [CrossRef]
- Tas, A.C. Formation of calcium phosphate whiskers in hydrogen peroxide (H2O2) solutions at 90 °C. J. Am. Ceram. Soc. 2007, 90, 2358–2362. [Google Scholar] [CrossRef]
- Neira, I.S.; Guitián, F.; Taniguchi, T.; Watanabe, T.; Yoshimura, M. Hydrothermal synthesis of hydroxyapatite whiskers with sharp faceted hexagonal morphology. J. Mater. Sci. 2008, 43, 2171–2178. [Google Scholar] [CrossRef]
- Yang, H.Y.; Yang, S.F.; Chi, X.P.; Evans, J.R.G.; Thompson, I.; Cook, R.J.; Robinson, P. Sintering behaviour of calcium phosphate filaments for use as hard tissue scaffolds. J. Eur. Ceram. Soc. 2008, 28, 159–167. [Google Scholar] [CrossRef]
- Zhang, H.; Zhu, Q. Synthesis of nanospherical and ultralong fibrous hydroxyapatite and reinforcement of biodegradable chitosan/hydroxyapatite composite. Modern Phys. Lett. B 2009, 23, 3967–3976. [Google Scholar] [CrossRef]
- Ribeiro, C.C.; Barrias, C.C.; Barbosa, M.A. Preparation and characterisation of calcium-phosphate porous microspheres with a uniform size for biomedical applications. J. Mater. Sci. Mater. Med. 2006, 17, 455–463. [Google Scholar] [CrossRef]
- Ribeiro, C.C.; Barrias, C.C.; Barbosa, M.A. Calcium phosphate-alginate microspheres as enzyme delivery matrices. Biomaterials 2004, 25, 4363–4373. [Google Scholar] [CrossRef]
- Zhou, W.Y.; Wang, M.; Cheung, W.L.; Guo, B.C.; Jia, D.M. Synthesis of carbonated hydroxyapatite nanospheres through nanoemulsion. J. Mater. Sci. Mater. Med. 2008, 19, 103–110. [Google Scholar]
- Kim, H.W.; Gu, H.J.; Lee, H.H. Microspheres of collagen-apatite nanocomposites with osteogenic potential for tissue engineering. Tissue Eng. 2007, 13, 965–973. [Google Scholar] [CrossRef]
- Kawai, T.; Sekikawa, H.; Unuma, H. Preparation of hollow hydroxyapatite microspheres utilizing poly(divinylbenzene) as a template. J. Ceram. Soc. Jpn. 2009, 117, 340–343. [Google Scholar] [CrossRef]
- Descamps, M.; Hornez, J.C.; Leriche, A. Manufacture of hydroxyapatite beads for medical applications. J. Eur. Ceram. Soc. 2009, 29, 369–375. [Google Scholar] [CrossRef]
- Cho, J.S.; Jung, D.S.; Han, J.M.; Kang, Y.C. Spherical shape hydroxyapatite powders prepared by flame spray pyrolysis. J. Ceram. Proc. Res. 2008, 9, 348–352. [Google Scholar]
- Kimura, I.; Honma, T.; Riman, R.E. Preparation of hydroxyapatite microspheres by interfacial reaction in a multiple emulsion. J. Ceram. Soc. Jpn. 2007, 115, 888–893. [Google Scholar] [CrossRef]
- Yao, A.; Ai, F.; Liu, X.; Wang, D.; Huang, W.; Xu, W. Preparation of hollow hydroxyapatite microspheres by the conversion of borate glass at near room temperature. Mater. Res. Bull. 2010, 45, 25–28. [Google Scholar] [CrossRef]
- Jiang, D.; Chen, M.; Li, D.; Zhu, J.; Lü, X.; Xie, J. One-pot synthesis of hierarchical fluorapatite hollow microparticles. Mater. Lett. 2009, 63, 2639–2642. [Google Scholar] [CrossRef]
- Lim, J.H.; Park, J.H.; Park, E.K.; Kim, H.J.; Park, I.K.; Shin, H.Y.; Shin, H.I. Fully interconnected globular porous biphasic calcium phosphate ceramic scaffold facilitates osteogenic repair. Key Eng. Mater. 2008, 361-363, 119–122. [Google Scholar] [CrossRef]
- Cho, J.S.; Ko, Y.N.; Koo, H.Y.; Kang, Y.C. Synthesis of nano-sized biphasic calcium phosphate ceramics with spherical shape by flame spray pyrolysis. J. Mater. Sci. Mater. Med. 2010, 21, 1143–1149. [Google Scholar] [CrossRef]
- Ye, F.; Guo, H.; Zhang, H.; He, X. Polymeric micelle-templated synthesis of hydroxyapatite hollow nanoparticles for a drug delivery system. Acta Biomater. 2010, 6, 2212–2218. [Google Scholar] [CrossRef]
- Simon, J.L.; Michna, S.; Lewis, J.A.; Rekow, E.D.; Thompson, V.P.; Smay, J.E.; Yampolsky, A.; Parsons, J.R.; Ricci, J.L. In vivo bone response to 3D periodic hydroxyapatite scaffolds assembled by direct ink writing. J. Biomed. Mater. Res. A 2007, 83A, 747–758. [Google Scholar] [CrossRef]
- Chu, T.M.; Orton, D.G.; Hollister, S.J.; Feinberg, S.E.; Halloran, J.W. Mechanical and in vivo performance of hydroxyapatite implants with controlled architectures. Biomaterials 2002, 23, 1283–1293. [Google Scholar] [CrossRef]
- Yoshikawa, H.; Myoui, A. Bone tissue engineering with porous hydroxyapatite ceramics. J.Artif. Organs 2005, 8, 131–136. [Google Scholar] [CrossRef]
- Detsch, R.; Uhl, F.; Deisinger, U.; Ziegler, G. In vitro-studies of cell growth on three differently fabricated hydroxyapatite ceramic scaffolds for bone tissue engineering. Key Eng. Mater. 2008, 361-363, 1181–1184. [Google Scholar] [CrossRef]
- Min, S.H.; Jin, H.H.; Park, H.Y.; Park, I.M.; Park, H.C.; Yoon, S.Y. Preparation of porous hydroxyapatite scaffolds for bone tissue engineering. Mater. Sci. Forum 2006, 510-511, 754–757. [Google Scholar] [CrossRef]
- Deville, S.; Saiz, E.; Nalla, R.K.; Tomsia, A.P. Strong biomimetic hydroxyapatite scaffolds. Adv. Sci. Technol. 2006, 49, 148–152. [Google Scholar] [CrossRef]
- Yang, W.; Zhou, D.; Yin, G.; Chen, H. Progress of biphasic calcium phosphate bioceramic as scaffold materials of bone tissue engineering. J. Chinese Ceram. Soc. 2004, 32, 1143–1149. [Google Scholar]
- Ramay, H.R.R.; Zhang, M. Biphasic calcium phosphate nanocomposite porous scaffolds for load-bearing bone tissue engineering. Biomaterials 2004, 25, 5171–5180. [Google Scholar] [CrossRef]
- Yuan, H.; Van Blitterswijk, C.A.; De Groot, K.; De Bruijn, J.D. Cross-species comparison of ectopic bone formation in biphasic calcium phosphate (BCP) and hydroxyapatite (HA) scaffolds. Tissue Eng. 2006, 12, 1607–1615. [Google Scholar] [CrossRef]
- Chen, G.; Li, W.; Zhao, B.; Sun, K. A novel biphasic bone scaffold: β-calcium phosphate and amorphous calcium polyphosphate. J. Am. Ceram. Soc. 2009, 92, 945–948. [Google Scholar] [CrossRef]
- Guo, D.; Xu, K.; Han, Y. The in situ synthesis of biphasic calcium phosphate scaffolds with controllable compositions, structures, and adjustable properties. J. Biomed. Mater. Res. A 2009, 88A, 43–52. [Google Scholar] [CrossRef]
- Furuichi, K.; Oaki, Y.; Ichimiya, H.; Komotori, J.; Imai, H. Preparation of hierarchically organized calcium phosphate-organic polymer composites by calcification of hydrogel. Sci. Technol. Adv. Mater. 2006, 7, 219–225. [Google Scholar] [CrossRef]
- Wei, J.; Jia, J.; Wu, F.; Wei, S.; Zhou, H.; Zhang, H.; Shin, J.W.; Liu, C. Hierarchically microporous/macroporous scaffold of magnesium-calcium phosphate for bone tissue regeneration. Biomaterials 2010, 31, 1260–1269. [Google Scholar] [CrossRef]
- Gbureck, U.; Grolms, O.; Barralet, J.E.; Grover, L.M.; Thull, R. Mechanical activation and cement formation of β-tricalcium phosphate. Biomaterials 2003, 24, 4123–4131. [Google Scholar] [CrossRef]
- Gbureck, U.; Barralet, J.E.; Hofmann, M.; Thull, R. Mechanical activation of tetracalcium phosphate. J. Am. Ceram. Soc. 2004, 87, 311–313. [Google Scholar] [CrossRef]
- Bohner, M.; Luginbühl, R.; Reber, C.; Doebelin, N.; Baroud, G.; Conforto, E. A physical approach to modify the hydraulic reactivity of α-tricalcium phosphate powder. Acta Biomater. 2009, 5, 3524–3535. [Google Scholar] [CrossRef]
- Hagio, T.; Tanase, T.; Akiyama, J.; Iwai, K.; Asai, S. Formation and biological affinity evaluation of crystallographically aligned hydroxyapatite. J. Ceram. Soc. Jpn. 2008, 116, 79–82. [Google Scholar] [CrossRef]
- Hench, L.L.; Polak, J.M. Third-generation biomedical materials. Science 2002, 295, 1014–1017. [Google Scholar] [CrossRef]
- Blawas, A.S.; Reichert, W.M. Protein patterning. Biomaterials 1998, 19, 595–609. [Google Scholar] [CrossRef]
- Sánchez-Salcedo, S.; Izquierdo-Barba, I.; Arcos, D.; Vallet-Regí, M. In vitro evaluation of potential calcium phosphate scaffolds for tissue engineering. Tissue Eng. 2006, 12, 279–290. [Google Scholar] [CrossRef]
- Meganck, J.A.; Baumann, M.J.; Case, E.D.; McCabe, L.R.; Allar, J.N. Biaxial flexure testing of calcium phosphate bioceramics for use in tissue engineering. J. Biomed. Mater. Res. A 2005, 72A, 115–126. [Google Scholar] [CrossRef]
- Case, E.D.; Smith, I.O.; Baumann, M.J. Microcracking and porosity in calcium phosphates and the implications for bone tissue engineering. Mater. Sci. Eng. A 2005, 390, 246–254. [Google Scholar] [CrossRef]
- Sibilla, P.; Sereni, A.; Aguiari, G.; Banzi, M.; Manzati, E.; Mischiati, C.; Trombelli, L.; Del Senno, L. Effects of a hydroxyapatite-based biomaterial on gene expression in osteoblast-like cells. J. Dent. Res. 2006, 85, 354–358. [Google Scholar] [CrossRef]
- Ono, I.; Ohura, T.; Murata, M.; Yamaguchi, H.; Ohnuma, Y.; Kuboki, Y. A study on bone induction in hydroxyapatite combined with bone morphogenetic protein. Plast. Reconstr. Surg. 1992, 90, 870–879. [Google Scholar] [CrossRef]
- Ono, I.; Yamashita, T.; Jin, H.Y.; Ito, Y.; Hamada, H.; Akasaka, Y.; Nakasu, M.; Ogawa, T.; Jimbow, K. Combination of porous hydroxyapatite and cationic liposomes as a vector for BMP-2 gene therapy. Biomaterials 2004, 25, 4709–4718. [Google Scholar] [CrossRef]
- Sawyer, A.A.; Hennessy, K.M.; Bellis, S.L. The effect of adsorbed serum proteins, RGD and proteoglycan-binding peptides on the adhesion of mesenchymal stem cells to hydroxyapatite. Biomaterials 2007, 28, 383–392. [Google Scholar] [CrossRef]
- Mastrogiacomo, M.; Muraglia, A.; Komlev, V.; Peyrin, F.; Rustichelli, F.; Crovace, A.; Cancedda, R. Tissue engineering of bone: Search for a better scaffold. Orthod. Craniofac. Res. 2005, 8, 277–284. [Google Scholar] [CrossRef]
- Schek, R.M.; Taboas, J.M.; Hollister, S.J.; Krebsbach, P.H. Tissue engineering osteochondral implants for temporomandibular joint repair. Orthod. Craniofac. Res. 2005, 8, 313–319. [Google Scholar] [CrossRef]
- Krylova, E.A.; Ivanov, A.A.; Krylov, S.E.; Plashchina, I.G.; Grigorjan, A.S.; Goldstein, D.V.; Pulin, A.A.; Fatkhudinov, T.H. Hydroxyapatite—Alginate structure as living cells supporting system. Minerva Biotecnol. 2006, 18, 17–22. [Google Scholar]
- Nishikawa, M.; Myoui, A.; Ohgushi, H.; Ikeuchi, M.; Tamai, N.; Yoshikawa, H. Bone tissue engineering using novel interconnected porous hydroxyapatite ceramics combined with marrow mesenchymal cells: Quantitative and three-dimensional image analysis. Cell Transplant. 2004, 3, 367–376. [Google Scholar]
- Quarto, R.; Mastrogiacomo, M.; Cancedda, R.; Kutepov, S.M.; Mukhachev, V; Lavroukov, A.; Kon, E.; Marcacci, M. Repair of large bone defects with the use of autologous bone marrow stromal cells. N. Engl. J. Med. 2001, 344, 385–386. [Google Scholar] [CrossRef]
- Vacanti, C.A.; Bonassar, L.J.; Vacanti, M.P.; Shufflebarger, J. Replacement of an avulsed phalanx with tissue-engineered bone. N. Engl. J. Med. 2001, 344, 1511–1514. [Google Scholar] [CrossRef]
- Morishita, T.; Honoki, K.; Ohgushi, H.; Kotobuki, N.; Matsushima, A.; Takakura, Y. Tissue engineering approach to the treatment of bone tumors: Three cases of cultured bone grafts derived from patients’ mesenchymal stem cells. Artif. Organs 2006, 30, 115–118. [Google Scholar] [CrossRef]
- Eniwumide, J.O.; Yuan, H.; Cartmell, S.H.; Meijer, G.J.; De Bruijn, J.D. Ectopic bone formation in bone marrow stem cell seeded calcium phosphate scaffolds as compared to autograft and (cell seeded) allograft. Eur. Cell Mater. 2007, 14, 30–39. [Google Scholar]
- Freed, L.E.; Langer, R.; Martin, I.; Pellis, N.R.; Vunjak-Novakovic, G. Tissue engineering of cartilage in space. Proc. Natl. Acad. Sci. USA 1997, 94, 13885–13890. [Google Scholar] [CrossRef]
- Holy, C.E.; Shoichet, M.S.; Davies, J.E. Engineering three-dimensional bone tissue in vitro using biodegradable scaffolds: Investigating initial cell-seeding density and culture period. J. Biomed. Mater. Res. 2000, 51, 376–382. [Google Scholar] [CrossRef]
- Shimizu, K.; Ito, A.; Honda, H. Enhanced cell-seeding into 3D porous scaffolds by use of magnetite nanoparticles. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 77B, 265–272. [Google Scholar] [CrossRef]
- Hench, L.L.; Wilson, J. Surface-active biomaterials. Science 1984, 226, 630–636. [Google Scholar]
- Navarro, M.; Michiardi, A.; Castano, O.; Planell, J.A. Biomaterials in orthopaedics. J. R. Soc. Interface 2008, 5, 1137–1158. [Google Scholar] [CrossRef]
- Anderson, J.M. The future of biomedical materials. J. Mater. Sci. Mater. Med. 2006, 17, 1025–1028. [Google Scholar] [CrossRef]
- Chevalier, J.; Gremillard, L. Ceramics for medical applications: A picture for the next 20 years. J. Eur. Ceram. Soc. 2009, 29, 1245–1255. [Google Scholar] [CrossRef]
- Hartgerink, J.D.; Beniash, E.; Stupp, S.I. Self-assembly and mineralization of peptide-amphiphile nanofibers. Science 2001, 294, 1684–1688. [Google Scholar] [CrossRef]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
MDPI and ACS Style
Dorozhkin, S.V. Calcium Orthophosphates as Bioceramics: State of the Art. J. Funct. Biomater. 2010, 1, 22-107. https://doi.org/10.3390/jfb1010022
AMA Style
Dorozhkin SV. Calcium Orthophosphates as Bioceramics: State of the Art. Journal of Functional Biomaterials. 2010; 1(1):22-107. https://doi.org/10.3390/jfb1010022
Chicago/Turabian StyleDorozhkin, Sergey V. 2010. "Calcium Orthophosphates as Bioceramics: State of the Art" Journal of Functional Biomaterials 1, no. 1: 22-107. https://doi.org/10.3390/jfb1010022